Embed Size (px)
Citation preview
Vol. 10, No. 6JOURNAL OF CLINICAL MICROBIOLOGY, DeC. 1979, p. 861-8750096-1137/79/12-0861/15$02.00/0
Microbiology Subsystem of a Total, Dedicated LaboratoryComputer System
D. JAMES LAWRIE,t* RONALD J. ELIN, VEE J. GILL, THOMAS L. LEWIS, JAMES D.MACLOWRY, AND FRANK G. WITEBSKY
Clinical Pathology Department, National Institutes ofHealth, Bethesda, Maryland 20205
Received for publication 29 May 1979
The computer system used by the Microbiology Service of the Clinical Pathol-ogy Department, Clinical Center, National Institutes of Health is discussed. Thismicrobiology subsystem is a part of a dedicated on-line laboratory computersystem used by the entire department. The laboratory computer is connected on-line to a hospital computer which provides patient admission, transfer, anddischarge data. Mark sense worksheets and cathode ray tube terminals are usedfor result entry and correction. Cumulative patient reports are printed. Resultsfor both active and completed accessions can be easily retrieved on cathode rayterminals in the laboratory. All laboratory data are archived on magnetic tapefrom which a research data base and microfiched laboratory records are generated.The manner in which the system is integrated in the routine operation of themicrobiology laboratory is emphasized. In addition, some of the costs, benefits,liabilities, and pitfalls associated with the introduction of the computer in thelaboratory are reviewed. Finally, we have presented our concept of some of thefuture enhancements to our present system and some of the directions in whichany future microbiology system might develop.
The Clinical Pathology Department of theNational Institutes of Health (NIH) provideslaboratory services for inpatients and outpa-tients seen in the Clinical Center, a 541-bedresearch hospital and clinic. The chemistry andhematology services of the department havebeen using computers to report laboratory re-sults since 1965. In contrast, the microbiologyservice began to use computers to support thedaily operation of the laboratory in July 1976.
In June 1974 the Clinical Center signed acontract with Honeywell Inc. for a "turn-key"laboratory computer system. Honeywell, like theother vendors competing in the laboratory com-puter system market at that time, did not havea fully developed microbiology subsystem whichcould be readily adapted for use in our labora-tory. (The microbiology laboratory in the Clini-cal Center is staffed by 25 technologists andperforms routine and special microbiological andserological studies on approximately 50,000 spec-imens per year.) The contract, therefore, re-quired that a usable system be developed. How-ever, the requirements for a microbiology sub-system were not completely defined at the timethe contract was signed; the extent to whichthese requirements were defined before selecting
t Present address: Department of Pathology, University ofCalifornia-Davis, Sacramento Medical Center, Sacramento,CA 95817.
the Honeywell computer system have been de-scribed elsewhere (9). This made it difficult forboth Honeywell and the Clinical Pathology De-partment to agree on precisely what functionsthe microbiology subsystem should perform andhow they should be implemented. It was even-tually agreed that a workable system from thelaboratory's point of view should be provided,and a cooperative development effort ensued.The result of that development effort was amicrobiology subsystem which we have usedeffectively since July 1976 and which Honeywellfelt it could market to other customers. It doesnot have all of the features which we believewould be valuable in a microbiology system, andthe method of implementation of some featurescould be improved.The system differs from most previously de-
scribed systems in several respects (2-6, 8, 10,11). It is an integrated part of a total, stand-alone, laboratory computer system. The datastructures for the storage ofmicrobiology cultureresults are basically the same as those for otherlaboratory data. They differ only in some detailsof record format and the use of two accessoryfiles for the storage of antibiotic susceptibilityresults and the results of procedures such as aGram stain which may have multiple observa-tions. The system is quite flexible and is adapt-able to a variety of different operating environ-
861
on May 8, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
862 LAWRIE ET AL.
ments. This flexibility is achieved through theuse of easily modified tables that describe thetests which the laboratory will perform, the an-tibiotics used in sensitivity testing, the orga-nisms which will be reported, the body sourcesfrom which a specimen might be obtained, etc.The description of the system which follows
presents the details of the way in which thesystem is used in our laboratory. There are anumber of features and options which we haveelected not to use and which we have not at-tempted to describe. Specifically, although thesystem can generate patient billing information,we have not discussed this aspect of the systembecause our patients are not billed.
MATERIALS AND METHODSSystem hardware and software. The Honeywell
laboratory computer system is run on a Honeywell 716minicomputer. (The reader may obtain some help withthe specialized vocabulary of computer science in thereference provided [10], or from several other special-ized dictionaries.) The Clinical Pathology Departmenthardware configuration includes 64K of 16-bit/wordmemory, four 15-megabyte moving head disk drives,two 1,600-bpi (bits per inch) tape drives, a 650-line/min line printer, analog to digital converter, and com-munications equipment for 17 cathode ray terminals(CRT), 11 keyboard printers (Texas Instruments Si-lent 700), four label printers (Terminet T1200), twomedium speed printers (Texas Instruments 810), threemark document readers (MDRs; Bell and Howell),and numerous instrument interfaces. The peripheralequipment required by the microbiology service in-cludes three CRTs, one label printer, one Silent 700,and one MDR.The real-time operating system is unique to Hon-
eywell's laboratory system and is not used in other 716computer applications. All application programs arewritten in FORTRAN IV, and there is an extensivesubroutine library for special laboratory functions, e.g.,for interfaced instruments, for programs using a CRT,etc. All programs must be compiled and loadedthrough an off-line batch operating system which can-not be used simultaneously with the real-time execu-tive, which operates the laboratory system. This hasbeen a relatively minor inconvenience since there isalso a real-time executive compatible on-line batchoperating system which permits editing of tables andprograms while the laboratory is in operation.
RESULTS AND DISCUSSIONFunctional description of the microbiol-
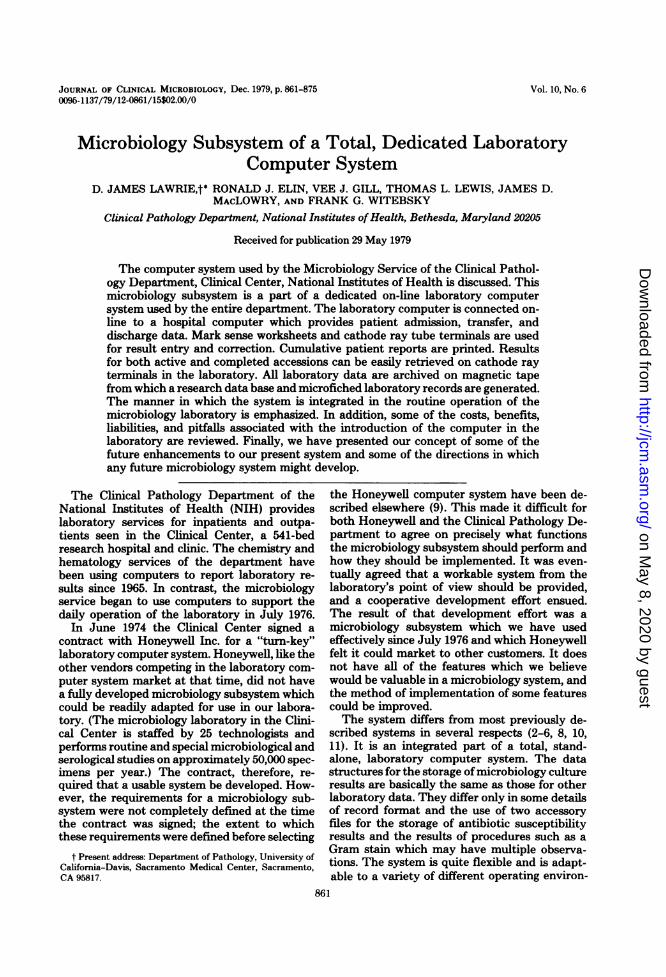
ogy subsystem. Figures 1 and 2 present anoverview of the interactions between the com-puter system functions and laboratory workflow. We will now examine in greater detail eachstep in the process.Accessioning. At the initial visit to the Clin-
ical Center, each patient is assigned a uniqueseven-digit, check-digited, hospital identification
number. On the first visit, and on every subse-quent visit either as an inpatient or an outpa-tient, the patient is admitted to the ClinicalCenter's total hospital information system,Technicon Medical Information System(TMIS). This admission is automatically com-municated to the Honeywell laboratory com-puter system via an on-line communications linkbetween the TMIS computer and the Honeywellcomputer. This same link keeps the laboratorycomputer up to date on all transfers and dis-charges from the Clinical Center. Informationtransferred at the time of admission includespatient name, hospital number, birth date, sex,race, nursing unit or clinic, attending physician,and Institute. There are nine Institutes whichadmit patients to the Clinical Center to be stud-ied under specific research protocols. Knowledgeof the Institute which is studying a particularpatient is necessary for proper routing of certainlaboratory reports.The TMIS is used by physicians to request
laboratory services. A physician may direct anurse or laboratory technologist to request lab-oratory services on TMIS as his "agent." Suchrequests appear in the patients' charts and arecountersigned by the physician. Studies may berequested for immediate action, e.g., "stat," tobe performed at some future time, or on a recur-ring basis. At the appropriate time and in theappropriate location(s) TMIS prints a labora-tory request document which accompanies thespecimen to the laboratory. In addition to pa-tient identification and tests requested, the re-quest document contains the laboratory acces-sion number assigned by TMIS. A preprintedlabel containing patient identification but notthe laboratory accession number is attached tothe specimen by the person responsible for col-lecting the specimen.When the specimen and request form arrive
in the microbiology laboratory, the request isentered in the laboratory computer on a CRT.(We are presently implementing a direct TMISto Honeywell laboratory test request and resultlink but this is not yet fully operational.) Theinformation entered on a formatted screen (Fig.3) includes the patient hospital identificationnumber, the TMIS-assigned laboratory acces-sion number, the collection date and time if thecurrent date and time are not appropriate, thebody source from which the specimen was ob-tained, the tests requested, and any additionaltextual information which may be of help to thetechnologist working with the specimen or tothe doctor interpreting the results. After the testrequest information is entered into Honeywell,a label (Fig. 4) containing the laboratory acces-
J. CLIN. MICROBIOL.
on May 8, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
COMPUTERIZATION IN CLINICAL MICROBIOLOGY 863
FIG. 1. Interactions between computer system functions and laboratory work flow showing (A) initialspecimen handling, (B) worksheet generation, result entry, and verification, and (C) specimen handling forroutine (except blood cultures) and anaerobic bacteriology.
sion number is printed on the microbiology labelprinter. The same accession number is assignedto all cultures to be performed on a given spec-imen.Mark sense worksheets. Mark sense work-
sheets are printed at about 6:00 p.m. each eve-ning and 5:00 a.m. the next morning. Worksheetsare printed for all specimens which have beenaccessioned in the laboratory since the previoustime worksheets were printed. Although theworksheets are not needed by the technologistsuntil the day after the specimen arrives in thelaboratory, the 6:00 p.m. printing insures that
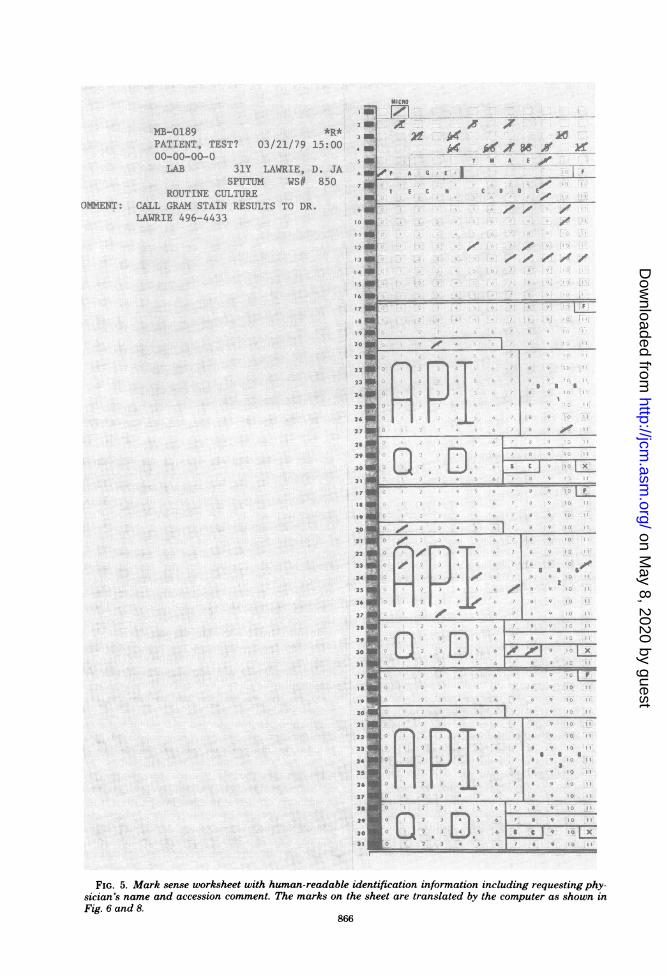
most of the needed worksheets will be availableif there is a computer malfunction which pre-vents timely printing of worksheets in the morn-ing. A separate worksheet is printed for each testrequested, e.g., routine bacterial culture, anaer-obe culture, tuberculosis culture, etc. If neces-sary, worksheets can be reprinted on demand.A sample worksheet is pictured in Fig. 5. The
computer prints human-readable specimen andpatient identification on the left side of the marksense worksheet. Computer interpretable iden-tification information is printed on the right sideof the page. This information is used by the
VOL. 10, 1979
on May 8, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
864 LAWRIE ET AL.
(4) handling of specimens which wareautomatically finalized by thecomputer if there was no growth.
continue organismidentificationaccording tolaboratoryprotocol
TB nd Mycology
'culture age in days since the specimenwas collected.
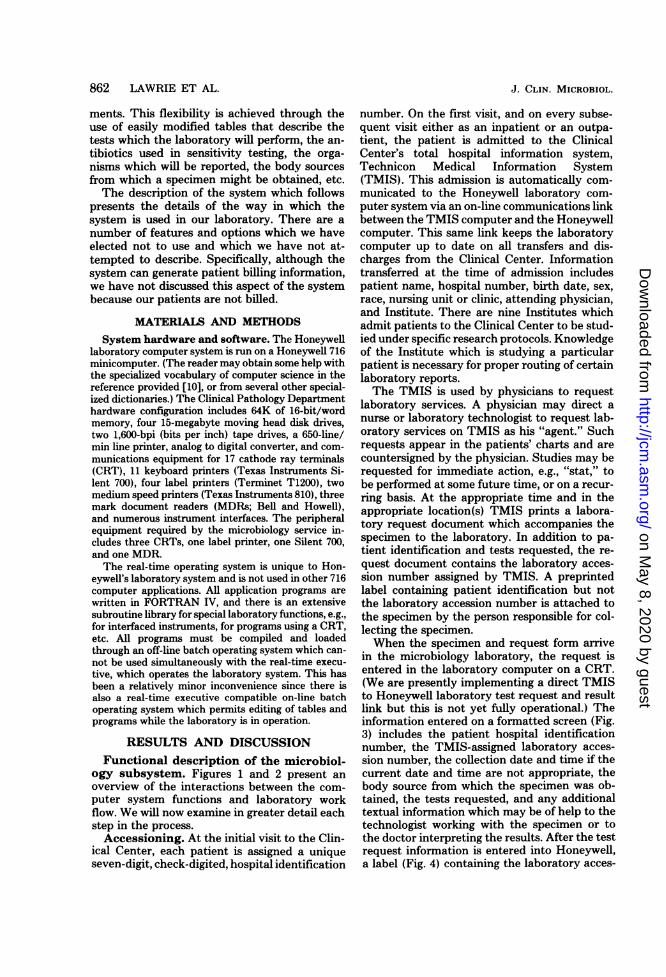
FIG. 2. Interactions between computer system functions and laboratory work flow for mycobacteriology,mycology, and routine blood cultures, which are automatically finalized when there is no growth.
J. CLIN. MICROBIOL.
on May 8, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
COMPUTERIZATION IN CLINICAL MICROBIOLOGY
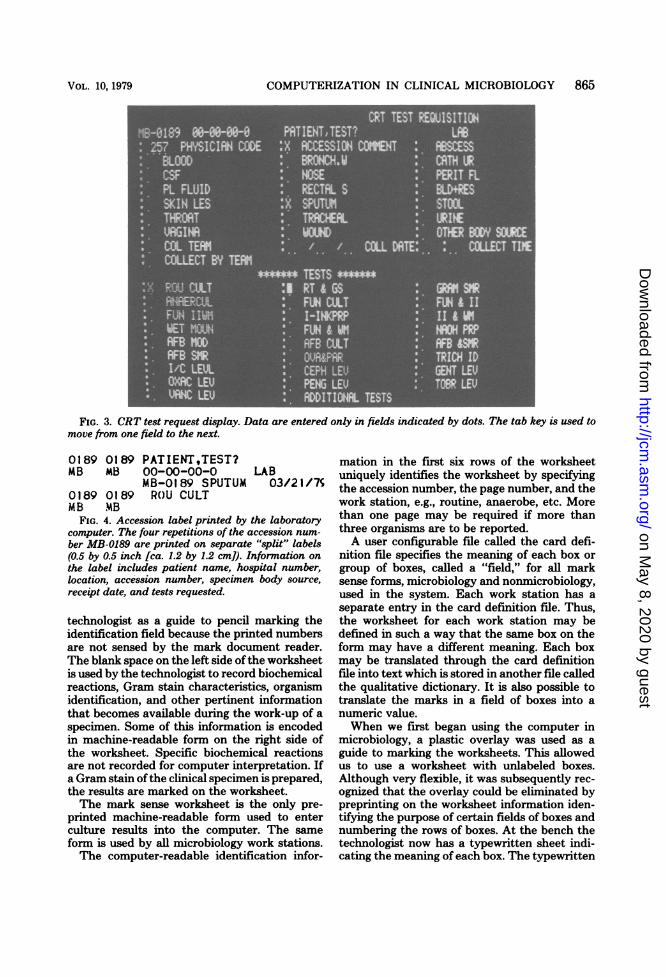
FIG. 3. CRT test request display. Data are entered only in fields indicated by dots. The tab key is used tomove from one field to the next.
0189 0189 PATIENT,TEST?MB MB 00-00-00-0 LAB
MB-0189 SPUTUM 03/21/7S0189 0189 ROU CULTMB MB
FIG. 4. Accession label printed by the laboratorycomputer. The four repetitions of the accession num-ber MB-0189 are printed on separate "split" labels(0.5 by 0.5 inch [ca. 1.2 by 1.2 cm]). Information onthe label includes patient name, hospital number,location, accession number, specimen body source,receipt date, and tests requested.
technologist as a guide to pencil marking theidentification field because the printed numbersare not sensed by the mark document reader.The blank space on the left side of the worksheetis used by the technologist to record biochemicalreactions, Gram stain characteristics, organismidentification, and other pertinent informationthat becomes available during the work-up of aspecimen. Some of this information is encodedin machine-readable form on the right side ofthe worksheet. Specific biochemical reactionsare not recorded for computer interpretation. Ifa Gram stain ofthe clinical specimen is prepared,the results are marked on the worksheet.The mark sense worksheet is the only pre-
printed machine-readable form used to enterculture results into the computer. The sameform is used by all microbiology work stations.The computer-readable identification infor-
mation in the first six rows of the worksheetuniquely identifies the worksheet by specifyingthe accession number, the page number, and thework station, e.g., routine, anaerobe, etc. Morethan one page may be required if more thanthree organisms are to be reported.A user configurable file called the card defi-
nition file specifies the meaning of each box orgroup of boxes, called a "field," for all marksense forms, microbiology and nonmicrobiology,used in the system. Each work station has aseparate entry in the card definition file. Thus,the worksheet for each work station may bedefined in such a way that the same box on theform may have a different meaning. Each boxmay be translated through the card definitionfile into text which is stored in another file calledthe qualitative dictionary. It is also possible totranslate the marks in a field of boxes into anumeric value.When we first began using the computer in
microbiology, a plastic overlay was used as aguide to marking the worksheets. This allowedus to use a worksheet with unlabeled boxes.Although very flexible, it was subsequently rec-ognized that the overlay could be eliminated bypreprinting on the worksheet information iden-tifying the purpose of certain fields of boxes andnumbering the rows of boxes. At the bench thetechnologist now has a typewritten sheet indi-cating the meaning of each box. The typewritten
865VOL. 10, 1979
on May 8, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
1B-01.89 *R*PATIENT, TEST? 03/21/79 15:0000-00-00-0
LAB 31Y LAWRIE, D. JASPUTUM WS# 850
ROUTINE CULTUREJMM:ENT: CALL GRAM STAIN RESULTS TO DR.
LAWRIE 496-4433
S41
71|8
91
12 1
1 1
14 1
I5
14 4
8 1
1920 j
211
224
23
24 I
2 1
26
29
30
3 1
riI911
20
2
222223
324
25
2':
2?
26
29
30.
3 1
20
21
24
20
2123
UUUUmlUtI
MtCRO
F71A: A1- o4
x k//& v x /I N A f .O F
A 5 0
U1 [-
9 C (10tD
ml -
* 0
S Im_ ,,,------='-'F-
S ___________
o0fT g?c
~~~~~...._. . .
-. XLT....- .......,,..... ^ ...,,
a..mlUI D..E..
C D 4 I~~~~~~~~~~~~~~~~~~
-I _
g~~~~~~~~~~~~~IPInRI.i __4FIG. 5. Mark sense worksheet with human-readable identification information including requesting phy-
sician's name and accession comment. The marks on the sheet are translated by the computer as shown inFig. 6 and 8.
866
on May 8, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
COMPUTERIZATION IN CLINICAL MICROBIOLOGY 867
sheets are different for each work station; how-ever, each work station uses the same preprintedform.The types ofinformation which can be entered
in the machine-readable portion of the work-sheet will now be discussed. The technologistmay record general observations that apply tothe culture as a whole, e.g., Gram stain results,colony counts on urine cultures, the number ofpositive bottles in a blood culture set, no growth,free text when desired, etc. For routine bacterialcultures, organisms which are considered to be"normal flora" in the body site from which thespecimen was obtained may be recorded. Infor-mation unique to each organism not identifiedas "normal flora" is recorded. Three organismsper page and up to 15 organisms, not counting''normal flora," may be reported on the marksense worksheets by copying the computer-read-able header to a blank worksheet, and markingthe appropriate page number box. Individualorganism information includes the following: (i)preliminary observations, statements about anorganism which are automatically deleted by thecomputer when the final organism identificationis recorded; (ii) quantitation of growth on aculture plate, e.g., scant, light, moderate, orheavy; (iii) a seven-digit octal API (AnalytabProducts, Inc.) profile number when appropri-ate; (iv) organism identification; (v) antibioticsusceptibility request; and (vi) for each organismup to 580 characters of free text may be enteredon a CRT.
If, for example, a fungus is encountered duringthe routine bacteriological work-up of a speci-men, a preprinted referral slip is filled out by thetechnologist working up the specimen. When thefinal identification is completed by the mycologylaboratory, the referral slip is returned to thebacteriology laboratory and the identification isentered on the mark sense worksheet on whichthe routine bacteriological identifications wererecorded. The increased amount of time whichmay be required to identify a fungus does notaffect the timely reporting of bacteriological re-sults. As the work-up of a specimen proceeds,the technologist will make appropriate notes onthe left side of the worksheet and record theinformation in machine-readable form on theright side of the worksheet. Each time importantnew information becomes available the work-sheet is read through the mark document reader.Thus, most worksheets are submitted for read-ing several times before the final identificationof all isolated organisms is complete.Worksheet processing errors. Like Wil-
liams et al. (11) we have experienced a low errorrate associated with the machine reading ofmark sense forms. Over a recent 2-week period
we measured our MDR read error rate. A totalof 1,073 worksheets were read. Errors were de-tected in 8% of the worksheets. Of the work-sheets, 6% had errors that were immediatelydetected by the computer, and most of thesecould be corrected by the clerk and immediatelyreread through the MDR. The remaining 2% ofthe errors occurred because the technologistmarked the wrong box in a result field and laterrecognized the error during the verification proc-ess which will be discussed next. The MDRmisread only one worksheet. MDR misreadshave occurred with occasional increase in fre-quency in the past. At these times the fieldengineer was called in to adjust the alignmentand sensitivity of the MDR, usually with im-mediate resolution of the problem. Such servicehas been required approximately once every 3 to4 months.Worksheet verification. After a batch of
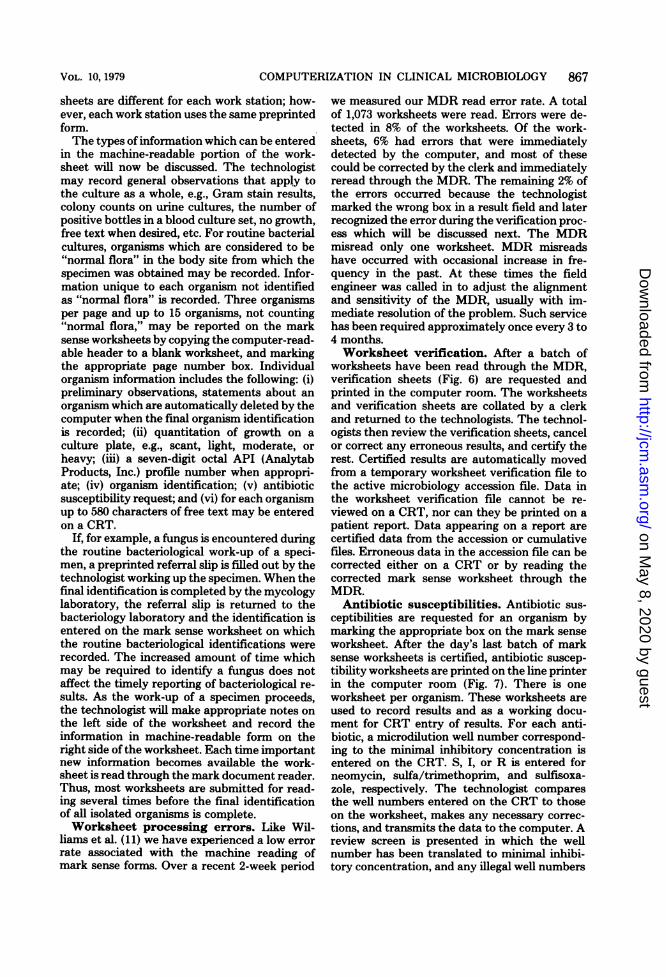
worksheets have been read through the MDR,verification sheets (Fig. 6) are requested andprinted in the computer room. The worksheetsand verification sheets are collated by a clerkand returned to the technologists. The technol-ogists then review the verification sheets, cancelor correct any erroneous results, and certify therest. Certified results are automatically movedfrom a temporary worksheet verification file tothe active microbiology accession file. Data inthe worksheet verification file cannot be re-viewed on a CRT, nor can they be printed on apatient report. Data appearing on a report arecertified data from the accession or cumulativefiles. Erroneous data in the accession file can becorrected either on a CRT or by reading thecorrected mark sense worksheet through theMDR.Antibiotic susceptibilities. Antibiotic sus-
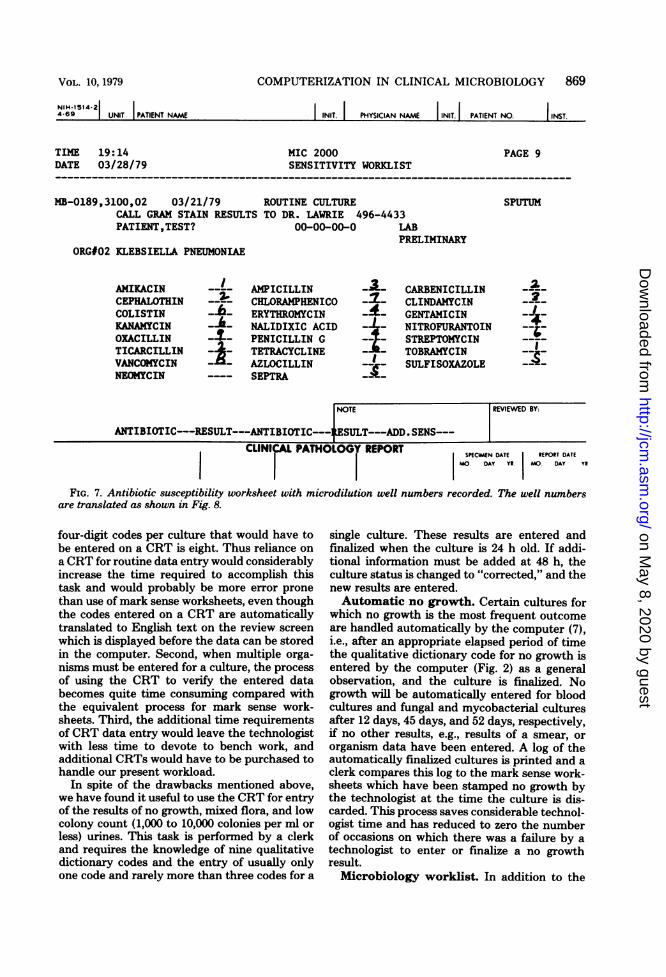
ceptibilities are requested for an organism bymarking the appropriate box on the mark senseworksheet. After the day's last batch of marksense worksheets is certified, antibiotic suscep-tibility worksheets are printed on the line printerin the computer room (Fig. 7). There is oneworksheet per organism. These worksheets areused to record results and as a working docu-ment for CRT entry of results. For each anti-biotic, a microdilution well number correspond-ing to the minimal inhibitory concentration isentered on the CRT. S, I, or R is entered forneomycin, sulfa/trimethoprim, and sulfisoxa-zole, respectively. The technologist comparesthe well numbers entered on the CRT to thoseon the worksheet, makes any necessary correc-tions, and transmits the data to the computer. Areview screen is presented in which the wellnumber has been translated to minimal inhibi-tory concentration, and any illegal well numbers
VOL. 10, 1979
on May 8, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
868 LAWRIE ET AL.
TIN 11:04DATE 03/28/79
BATCH 1 SEQUENCE 36
MICROBIOLOGY VUIFICATIONWORKSTATION 850 - MAIN LAD
J. CLIN. MICROBIOL.
PAGE 38MDR 2
TECH 99
PATIENT, TZST? 00-00-00-0 LABMB-0189 REQSTED 03/21 15:00 IT 257-LAWRIE, D. JAMESCOLLECTED 03/21 15:00 BY 0 ROUTINE
3100-ROUTINE CULTURE SPUTUM
OBSERVATIONSSTATUS PRELIKINART
4003-GRAM POSITIVE COCCI IN CHAINS5111-GRAM POSITIVE DIPLOCOCCI5112-GRAM POSITIVE BACILLI5087-GRAM NEGATIVE DIPLOCOCCI5095-CLUIIAR EPITHELLAL CELLS5098-GRANULOCYTES-MANY4036-NORMAL FLORA IDENTIFIED AS:1441-STREPTOCOCCUS - ALPHA HENDLYTIC1065-STREPTOCOCCUS, NONHEDLYTIC (GAMA)1024-NEISSERIA SPECIES1445-CORTNEBACTERIUM SPECIES4064- **SENSITIVITY RSULTS CODE**
ORG#0011052-STREPTOCOCCUS PNEUMONIU7078-HEAVY
ORG#OO20513-KLEBSIELLA PNEUMONIAE0248-LIGHTAPI NUMBER 1215753BATTERY MIC 2000SENSITIVITIES AMIKACIN
AMPICILLINCARBENICILLINCEPHALOTHINCHLORAMPHENICOLCLINDAMYCINCOLISTINERYTHROMYCINGENTAMICINKANANYCINNALIDIXIC ACIDNITROFURANTOINOXACILLINPENICILLIN GSTREPTOMYCINTICARCILLINTETRACYCLINETOBRAMYCINVANCOMYCINAZLOCILLINSULFISOXAZOLENEOMYCIN
FIG. 6. Verification sheet corresponding to the worksheet shown in Fig. 5. The word "*ADDED" indicatesthat a particular result is a new result. Other possibilities include "*CHANGED," "*DELETED," or blank,indicating no change.
not corrected previously are noted. If correct,the data on the review screen are certified.Culture finalization and result correc-
tion. When all organisms in a culture have beenidentified and all other data have been entered,the culture is finalized. Ten days after a cultureis finalized the results are transferred in thecomputer from the active, or accession, file tothe historical, cumulative file. All results of a
culture can be easily corrected or modified be-fore they are transferred to the cumulative file.Although microbiology data in the cumulativefile can be corrected, it has been made somewhatdifficult to do and is necessary for at most one
culture per month.
CRT data entry. Use of a CRT in the Hon-eywell system for entry of culture and organismdata other than antibiotic susceptibilities hasbeen mentioned. In fact, any data which can beentered on a mark sense worksheet can also beentered on a CRT. There are several reasons
why we have elected not to use a CRT routinelyfor all microbiology data entry. First, a mark ina single box on a mark sense worksheet maytranslate to a phrase of English language text,e.g., organism name, which is identified in thequalitative dictionary by a four-digit code. Thisfour-digit code must be entered on a CRT tocommunicate the same information to the com-
puter. In our laboratory the average number of
SEX-M AGE 31
WORK SHEET PAGE 1
*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED
*ADDED*ADDED
*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDEDD*ADDECD*ADDED*ADDED*ADDED*AIDDE£D*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED*ADDED
on May 8, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
VOL. 10, 1979
NIH-1514 214-69 | UNIT PATIENT NAME
COMPUTERIZATION IN CLINICAL MICROBIOLOGY 869
NIT. PHYSICIAN NAME I INIT. PATIENT NO. I INST.
TIME 19:14 MIC 2000 PAGE 9DATE 03/28/79 SENSITIVITY WORKLIST
MB-0189,3100,02 03/21/79 ROUTINE CULTURE SPUTUMCALL GRAM STAIN RESULTS TO DR. LAWRIE 496-4433PATIENT,TEST? 00-00-00-0 LAB
PRELIMINARYORG#02 KLEBSIELLA PNEUMONIAE
AMIKACIN - AMPICILLIN CARBENICILLIN 2-CEPHALOTHIN CHLORAMPHENICO CLINDAMYCIN 2-COLISTIN ERYTHROMYCIN -4- GENTAMICIN -J.KANAMYACIN - ^- NALIDIXIC ACID - - NITROOINANTOIOXACILLIN PENICILLIN G - N-STREPTOFYCINTICARCILLIN -i- TETRACYCLINE - TOBRAMYCINVANCOMYCIN - - AZLOCILLIN --- SULFISOXAZOLENEOMYCIN S---SULIRASOAZL
NOTE REVIEWED BY:
ANTIBIOTIC---RESULT---ANTIBIOTIC---4.ESULT---ADD.SENS---r1 lUIr-| MATU^l ^&'-V DCMID
SPECIMEN DATE REPORT DATEMO. DAY Y. MO. DAY YR
FIG. 7. Antibiotic susceptibility worksheet with microdilution well numbers recorded. The well numbersare translated as shown in Fig. 8.
four-digit codes per culture that would have tobe entered on a CRT is eight. Thus reliance ona CRT for routine data entry would considerablyincrease the time required to accomplish thistask and would probably be more error pronethan use of mark sense worksheets, even thoughthe codes entered on a CRT are automaticallytranslated to English text on the review screenwhich is displayed before the data can be storedin the computer. Second, when multiple orga-nisms must be entered for a culture, the processof using the CRT to verify the entered databecomes quite time consuming compared withthe equivalent process for mark sense work-sheets. Third, the additional time requirementsof CRT data entry would leave the technologistwith less time to devote to bench work, andadditional CRTs would have to be purchased tohandle our present workload.
In spite of the drawbacks mentioned above,we have found it useful to use the CRT for entryof the results of no growth, mixed flora, and lowcolony count (1,000 to 10,000 colonies per ml orless) urines. This task is performed by a clerkand requires the knowledge of nine qualitativedictionary codes and the entry of usually onlyone code and rarely more than three codes for a
single culture. These results are entered andfinalized when the culture is 24 h old. If addi-tional information must be added at 48 h, theculture status is changed to "corrected," and thenew results are entered.Automatic no growth. Certain cultures for
which no growth is the most frequent outcomeare handled automatically by the computer (7),i.e., after an appropriate elapsed period of timethe qualitative dictionary code for no growth isentered by the computer (Fig. 2) as a generalobservation, and the culture is finalized. Nogrowth will be automatically entered for bloodcultures and fungal and mycobacterial culturesafter 12 days, 45 days, and 52 days, respectively,if no other results, e.g., results of a smear, ororganism data have been entered. A log of theautomatically finalized cultures is printed and aclerk compares this log to the mark sense work-sheets which have been stamped no growth bythe technologist at the time the culture is dis-carded. This process saves considerable technol-ogist time and has reduced to zero the numberof occasions on which there was a failure by atechnologist to enter or finalize a no growthresult.Microbiology worklist. In addition to the
%.Lglllq.AL rAlrlVLV%* KtrUKI
on May 8, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
870 LAWRIE ET AL.
mark sense worksheets described above, the my-cology and mycobacteriology laboratories useanother type of working document, a microbi-ology worklist. This document is printed on theline printer on plain paper (8.5 by 11 inches [ca.21.6 by 27.9 cm]) once a day. There are nineaccessions per page organized in ascendingaccession number order. Only accessions whichhave not appeared on a previous worklist areprinted. Between each accession there is suffi-cient space for the technologist to make notesabout the progress of the culture. The worklistsoffer several advantages to the technologistworking with tuberculosis or fungus cultures.Because the incubation times are frequently 6 to8 weeks, there are often several hundred tuber-culosis or fungus cultures in progress. Therefore,instead of having to manage 200 to 300 pages ofindividual mark sense worksheets, all of theactive work will be contained in 20 to 30 pagesof worklists. The technologist need only use themark sense worksheets for cultures on which
14: 5703/29/79
PATIENT, TEST?00-00-00-0
J. CLIN. MICROBIOL.
there are positive results to report, a relativelysmall percentage of the total. Those cultures forwhich there was no growth are handled auto-matically by the computer as noted above.Patient reports. Three types of patient re-
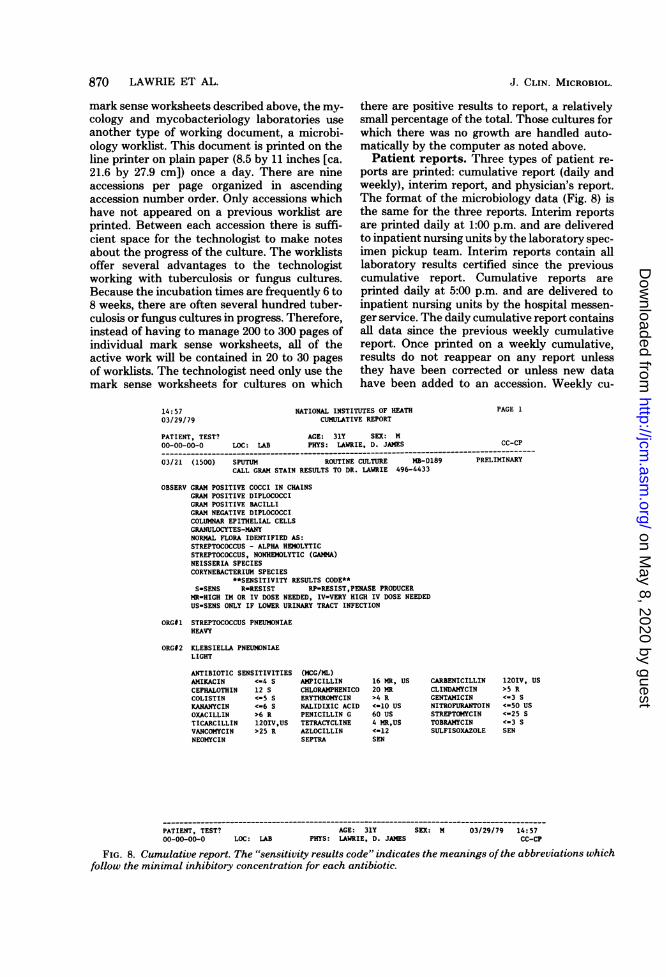
ports are printed: cumulative report (daily andweekly), interim report, and physician's report.The format of the microbiology data (Fig. 8) isthe same for the three reports. Interim reportsare printed daily at 1:00 p.m. and are deliveredto inpatient nursing units by the laboratory spec-imen pickup team. Interim reports contain alllaboratory results certified since the previouscumulative report. Cumulative reports areprinted daily at 5:00 p.m. and are delivered toinpatient nursing units by the hospital messen-ger service. The daily cumulative report containsall data since the previous weekly cumulativereport. Once printed on a weekly cumulative,results do not reappear on any report unlessthey have been corrected or unless new datahave been added to an accession. Weekly cu-
NATIONAL INSTITUTES OF HEATHCUMULATIVE REPORT
AGE: 31Y SEX: MLOC: LAB PHYS: LAWRIE, D. JAMES
03/21 (1500) SPUTUM ROUTINE CULTURE MB-0189CALL GRAM STAIN RESULTS TO DR. LAWRIE 496-4433
OBSERV GRAM POSITIVE COCCI IN CHAINSGRAM POSITIVE DIPLOCOCCIGRAM POSITIVE BACILLIGRAM NEGATIVE DIPLOCOCCICOLUMNAR EPITHELIAL CELLSGRANULOCYTES-MANYNORMAL FLORA IDENTIFIED AS:STREPTOCOCCUS - ALPHA HEMOLYTICSTREPTOCOCCUS, NONHEMOLYTIC (GAMMA)NEISSERIA SPECIESCORYNERACTERIUM SPECIES
**SENSITIVITY RESULTS CODE**S-SENS R-RESIST RP-RESIST,PENASE PRODUCER
MR-HIGH IM OR IV DOSE NEEDED, IV-VERY HIGH IV DOSE NEEDEDUS-SENS ONLY IF LOWER URINARY TRACT INFECTION
ORG#1 STREPTOCOCCUS PNEUMONIAEHEAVY
ORG#2 KLEBSIELLA PNEUMONIAELIGHT
ANTIBIOTIC SENSITIVITIESAMIKACIN <-4 SCEPHALOTHIN 12 SCOLISTIN <-5 SKANANYCIN <-6 SOXACILLIN >6 RTICARCILLIN 120IV,USVANCOMYCIN >25 RNEOMYCIN
(MCG/ML)AMPICILLINCHLORAMPHENICOERYTHROMYCINNALIDIXIC ACIDPENICILLIN GTETRACYCLINEAZLOCILLINSEPTRA
16 MR, US20 MR>4 R<-10 US60 US4 MR,US<-12SEN
PAGE 1
Cc-CP
PRELIMINARY
CARBENICILLINCLINDAMYCINGENTAMICINNITROFURANTOINSTREPTOMYCINTOBRAMYCINSULFISOXAZOLE
1201V, US>5 R<-3 S<-50 US<-25 S<-3 SSEN
PATIENT, TEST? AGE: 31Y SEX: M 03/29/79 14:5700-00-00-0 LOC: LAB PHYS: LAWRIE, D. JAMES CC-CP
FIG. 8. Cumulative report. The "sensitivity results code" indicates the meanings ofthe abbreviations whichfollow the minimal inhibitory concentration for each antibiotic.
on May 8, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

COMPUTERIZATION IN CLINICAL MICROBIOLOGY 871
mulatives are printed for both inpatients andoutpatients. Outpatient reports are delivered tomedical records and filed in the patient's chart.Physician's reports are printed daily after cu-mulative reports and include all data not printedon a previous physician's report. Physician's re-ports are printed only for outpatients unless aphysician specifically requests that his inpa-tients be included as well. The morning afterbeing printed, physicians' reports are deliveredto physicians' offices in the hospital.The format of the microbiology report is the
same for each culture type, e.g., routine, fungus,etc., and begins with general observations. Gen-eral observations are followed by specific orga-nism identifications with antibiotic susceptibili-ties where appropriate. Results are sorted in thefollowing manner: first by date, within date bybody source, and within body source by acces-sion number.CRT data retrieval. In addition to the "hard
copy" provided by patient reports, it is possibleto use a CRT in the laboratory for retrieval of apatient's results. The data are displayed in re-verse chronological order, and it is possible tolook up the results of all active accessions, aspecific accession, or to scan the cumulative filewithin a specified date range. The data displayedon the CRT are the same as the data printed onpatient reports. The CRT retrieval is used rou-tinely by technologists to answer telephone in-quiries. The CRT is also used routinely by theinfectious disease consultant physician for thehospital because the data for many patients ina variety of locations in the hospital can bereviewed in one place.Additional reports. An incomplete work re-
port is printed weekly. This report identifies allcultures which have not been finalized. A routineculture more than 3 to 4 weeks old or a myco-bacterial culture more than 10 weeks old, forexample, would be reviewed, and the reason itwas not finalized would be identified.Each day a specimen log which lists all speci-
mens accessioned in microbiology during theprevious 6 days is printed. This list is printedalphabetically by patient, within patient by bodysource, and within body source by date. The 6-day specimen log provides a quick reference foridentification of patients from whom specimensare being obtained for culture more often thanclinically necessary.An infection control, epidemiology report can
be printed weekly, biweekly, or monthly to pro-vide a summary of all cultures positive for anyone or more of up to 100 specific organisms. Atable of organism versus patient location isprinted for each body source. The body of thereport is the count of the number of times a
given organism was isolated from a given bodysource at a particular location in the hospital. Inpractice this report has not been particularlyuseful for several reasons. First, the patientswhose organisms are counted in the report arenot specifically identified. Second, the data inthe infections control report are retrospectiveand do not provide day-to-day informationabout infection in the hospital. To provide thenurse epidemiologist with timely information, areport, printed nightly, summarizes all culturesto which new results have been added duringthe previous day.A workload summary available for daily,
monthly, or yearly statistics is printed. It pro-vides raw counts of the number of cultures, e.g.,routine or anaerobe, performed during the pe-riod of interest. The workload summary wouldbe more useful if cultures were enumerated bybody source.Long-term data storage. Data are stored
on computer output microfiche for long-termlaboratory records. Once a week all certifiedresults in the cumulative file not previously ar-chived are written on tape, taken to the NIHcentral computer facility, the Division of Com-puter Research and Technology, and incorpo-rated in the large central laboratory data base.The processing of the archive tapes results inthe generation of microfiche for chemistry andhematology data and the transfer of all data intodisk files for three different data bases; chemis-try and hematology, bone marrow results, andmicrobiology. Once every 3 months data in themicrobiology data base are transferred to mi-crofiche. The mark sense worksheets for themost recent 3 to 6 months are filed in the labo-ratory and are discarded once the data havebeen microfiched. Two years' worth of data rep-resenting approximately 90,000 cultures havebeen stored on 85 sheets of microfilm (4 by 6inches [10.1 by 15.2 cm]).Although laboratory results are archived on
tape weekly, all laboratory data for a patient arepurged from the laboratory computer only if thefollowing conditions are met: (i) the patient musthave been discharged from the hospital, i.e., thepatient is in outpatient status; (ii) all pendingresults must have been certified at least 30 daysbefore purge; and (iii) all data must have beenarchived on tape. Certified results in the cumu-lative file may be partially purged if a particularpatient is using a large amount of space in thecumulative file. If patient data are partiallypurged, the most recent 6 weeks of data willalways be maintained.Microbiology research data base. The mi-
crobiology data base, the data bases mentionedabove, and other data bases are all part of a
VOL. 10, 1979
on May 8, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
872 LAWRIE ET AL.
larger system called the Clinical InformationUtility. Anyone who is permitted access tocharts in the medical records department maybe given access to the Clinical Information Util-ity data. The research potential for both retro-spective and prospective data analysis is signifi-cant. The data have been used to support theresearch of clinical investigators at NIH and bythe Microbiology Service to determine policyregarding the laboratory work-up of certaintypes of specimens and to support research.System down time. When a decision has
been made to install a computer system in alaboratory, it must be recognized that there willbe periods of time during which the computerwill be unavailable due to malfunction or powerfailure. One must be prepared with a carefullyorganized plan which will permit the laboratoryto continue to function without the computer. Itmust be possible to implement the plan flexiblyto appropriately accommodate a variety of situ-ations which can arise, e.g., a mark documentreader is unavailable but the rest of the systemcontinues to function, or the entire computer isdown for 1 h or for 8 h, etc.The reliance of the laboratory on the hospital
computer system, TMIS, for assignment ofaccession numbers slightly complicates ourdown-time planning. However, all specimens ar-riving in the laboratory can be accessioned onthe laboratory computer by using accessionnumbers in the laboratory system which willnever be assigned by TMIS.Costs, benefits, and liabilities. In discuss-
ing the costs, benefits, and liabilities associatedwith our use of a computer system in microbi-ology we will identify some of the elementsinvolved without attempting to assign a dollarcost, except to say that the microbiology subsys-tem represents one-third of a system the originaltotal cost of which was approximately $620,000,including 24-h/day, 7-day/week maintenance onall hardware for 5 years. The peripheral com-puter hardware required to operate the micro-biology system have been described above. Indetermining the cost of hardware one must in-clude maintenance and, depending upon theavailability of maintenance personnel, the costof backup hardware for crucial devices. Each of18 technologists spends an average of about 25min per day (range: 5 to 60 min/day) on com-puter-related functions, e.g., marking work-sheets, reviewing verification sheets, and enter-ing data on CRTs. These functions replace anal-ogous functions from our previous manual op-eration, but the technologist time required hasincreased by a factor of about 1.3. The modestincrease in work required to enter data into thecomputer is justified in our setting since, as a
byproduct of routine daily patient care-relatedoperations of the laboratory, we are now captur-ing data for our research data base. In additionto the technologists, there are two other peoplewho perform computer-related functions. First,a clerk spends 3 h/day putting mark sense work-sheets through the MDR, entering results on aCRT, and performing other tasks describedabove. The second person is a former technolo-gist who spends about 4 h/day performing awide variety of computer-related tasks, some ofwhich include training new microbiology person-nel in the use of the computer, reviewing theweekly incomplete work report and resolving allproblems raised by the incomplete work report,helping technologists with difficulties they mayexperience in their routine use of the computer,identifying and documenting hardware and soft-ware problems, and preparing file change re-quests, e.g., for adding a new organism to thequalitative dictionary, adding a new test to thetest file, etc.The cost of all preprinted documents and com-
puter paper must also be considered. Because allcultures are reported on the same mark sensedocument, our expenditure for preprinted formsis relatively small. The only other form usedexclusively by the microbiology section is theworksheet (5.5 by 8.5 inches [13.9 by 21.6 cm])used for antibiotic susceptibilities.The savings directly attributable to the com-
puter will now be described. First, our previousmanual system required one full-time secretarydevoted to typing reports. Second, 3 to 4 h/weekwere spent reporting no-growth mycobacterialand mycological cultures. A secretary is nolonger involved with reports, and no growth formycology and mycobacteriology are automati-cally handled by the computer. Report distri-bution for microbiology is now integrated withdistribution for the rest of the department,thereby eliminating about 2 h spent by a clerkperforming this function per day.There are a number of additional benefits
attributable to the computer which enhance theservice provided by the department. (i) Anti-biotic susceptibility result recording has beensimplified so that the technologist need onlyrecord the microdilution well number. Previ-ously, the well number had to be converted toantibiotic concentration by the technologist be-fore recording the result. The computer nowautomatically performs the conversion, resultingin some savings of time and reduction of error,particularly for inexperienced technologists. (ii)Patient demographic data including hospital lo-cation and attending physician are immediatelyavailable in the laboratory. This is particularlyvaluable in the specimen accessioning area
J. CLIN. MICROBIOL.
on May 8, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

COMPUTERIZATION IN CLINICAL MICROBIOLOGY 873
where it is frequently necessary to contact some-one caring for the patient regarding a variety ofquestions which may arise concerning specimenssent to the laboratory. (iii) When a physiciancalls the laboratory with a question about aparticular culture, it is no longer necessary tolocate the results by searching through a numberof worksheets belonging to the technologistworking on the specimen in question. Most in-quiries can be answered by retrieval of the in-formation on a CRT. (iv) Archived data are nowkept on microfiche, resulting in a very substan-tial saving in filing space and frequently simpli-fying retrieval of old results. (v) The value of thesystem for creating a research data base whichis a byproduct of routine laboratory operationhas been discussed. (vi) The system generates areadable, standardized report for the medicalrecord.
It should be emphasized that some of thebenefits noted above could be realized in a well-designed manual system and that others thatare important in the environment of our labo-ratory would not be important in a differentsetting. Such potential benefits must be weighedcarefully against the liabilities of introducing acomputer system in the laboratory.The installation of a computer system can be
a very traumatic experience for people at alllevels in the laboratory and for those caring forpatients. The installation of the system in ourmicrobiology laboratory was quite smooth, amarked contrast to the installation of the systemin the chemistry and hematology departments.The relative ease of the installation in the mi-crobiology laboratory is attributable to severalfactors: (i) the system had been operating inchemistry and hematology departments for 9months, so most of the initial hardware andoperating system software problems had beenresolved; (ii) the microbiology applications soft-ware was very completely checked out by Hon-eywell, and there were no serious deficienciesdetected after installation; (iii) the computer hadbeen used for accessioning and for reportingserology results since its original installation inthe chemistry and hematology laboratories; (iv)more time was devoted to teaching the technol-ogists how to use the system before they had touse it in daily operation in the microbiology lab;and (v) the computer did not substantiallychange the relationship of the technologist tothe bench work, i.e., there were no instrumentsdirectly on-line to the computer, and the hand-written aspect of recording the work-up of aculture was unchanged.Once a computer has been installed, the lab-
oratory becomes dependent upon it in manyrespects. Therefore, when the computer is down,
as occasionally it will most certainly be, thedisruptions of daily routine and of the level ofservice which we all have come to expect can besignificant. Such disruptions can be minimizedonly with careful planning and careful review ofthe manner in which the laboratory has dealtwith previous periods of computer down time.The other major liability associated with the
use of the computer is the limitations whicheven the most flexibly designed systems canimpose on the reporting of new types of data.We have emphasized the flexibility of the Hon-eywell system in permitting the routine types ofchanges the laboratory usually needs to make.It is not always possible to anticipate new typesof results which one may wish to report. There-fore, the types and characteristics of data whichare permitted by the system must be carefullystudied. For example, API has recently enlargedtheir numeric scheme from seven to nine digitsfor nonfermentative gram-negative rods. Al-though we do not print the API number onpatient reports, the data are entered and storedfor research purposes. The manner in which theAPI number is stored in the computer precludesthe possibility of storing a larger API number.Although a larger API number could be enteredas free text, it would then appear on patientreports. It would not be distinct from any otherfree text comment, and the data could not beeasily identified and archived for our research.In addition, the program which processes themark sense worksheets does not recognize anAPI number of more than seven digits. Thelimitation just discussed could be corrected at aconsiderable expense of reprogramiing, not tomention the changes which would be requiredto add two more digits of API number for eachorganism on the mark sense worksheet.
Thus, in the process of selecting a computersystem for a laboratory or any other environ-ment, one must clearly delineate the functionsthe system must perform, attempt to anticipatethe future uses of the system, and analyze thelimitations of the system. Finally, it must berecognized that any system cannot be all thingsto all people and that most decisions must bemade balancing benefits and liabilities.
Potential enhancements to clinical mi-crobiology computer systems. There are anumber of areas in which we believe substantialenhancements could be made to our microbiol-ogy system. Some of these enhancements arespecific to the Honeywell system, and somewould be desirable in any system and are not toour knowledge presently available.There are two features that would improve
the mark sense worksheets. First, considerableflexibility in the design of the worksheets could
VOL. 10, 1979
on May 8, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
874 LAWRIE ET AL.
be achieved if more than three organisms couldbe reported on a single page. Second, it mightbe desirable to have more extensive error check-ing of the final organism identification. For ex-ample, one might check the organism identifi-cation against the API number or compare thesensitivity pattern of the organism against thesensitivities of other isolates of the same orga-nism. It must be emphasized that although it isoften possible to implement sophisticated errorchecking and other complicated procedures, thismay be done at considerable expense in terms ofsystem performance or programming time. Thepotential benefits must be weighed against thecost.
In our laboratory the computer could be help-ful in facilitating intralaboratory referral. Forexample, if the routine bacteriology laboratoryisolated a yeast, a box on the worksheet wouldbe marked which automatically causes the com-puter to generate a mycology worksheet, and togenerate on the patient report a comment suchas "yeastlike cells isolated, identification to fol-low." Data collection for some of our researchprojects would be facilitated if the system couldbe easily modified to uniquely recognize newtypes of data, e.g., staphylococcal phage types,pseudomonal grouping, a nine-digit API num-ber, etc. In addition, there may be new types ofinformation of clinical utility which should beprinted on a patient report and which should beidentifiably separate from existing data types inthe computer. The system as presently designedhas little flexibility for the introduction of newdata types which do not correspond to existingcategories.Workload reporting in microbiology could be
substantially improved. It would be possible toimplement a system based on organism identi-fication, rather than the number of cultures per-formed regardless of growth. Since the path bywhich the fmal identification of an organismfrom a specimen of a given source is usuallyknown, it is possible in most cases to assign aweighting factor which accurately reflects theamount of work required to make the identifi-cation. Only a computer could make such aworkload reporting system economically feasi-ble.The present CRT data entry scheme is cum-
bersome and can be time consuming to use,especially as the number of organisms identifiedin a culture increases. A redesign of the CRTdata entry scheme would result in some im-provement. However, any scheme which de-pends upon the entry of code numbers or evenmnemonic abbreviations is difficult for the newuser to learn. The use of a very fast CRTequipped with a light pen would avoid the ne-
J. CLIN. MICROBIOL.
cessity of using codes or abbreviations if thescreens presented lists of organisms, minimalinhibitory concentrations, etc., which would beselected with the light pen. Such a system, ifproperly designed, could be a considerable im-provement on the use of mark sense documents.However, to function smoothly, a CRT-basedsystem might require one device per technolo-gist, an expensive proposition at this time. Inaddition, there would be considerable idle timefor each device, thereby requiring such a termi-nal to be very inexpensive for it to be cost-effective.Instrumentation for the automatic identifica-
tion of microbial organisms is being developed.One must anticipate the time when it will bedesirable to interface such devices with a labo-ratory computer system.The ability to perform cross-patient retrieval
of laboratory data might be a useful function toincorporate into a dedicated laboratory system.There are several major obstacles to this appli-cation. First, the mass storage required to main-tain the total output from the laboratory rapidlybecomes very large. Retrieval of data acrosspatients from a data base stored on magnetictape, relatively inexpensive mass storage, is veryslow and cumbersome. Second, the minicompu-ters used in most laboratory systems simplycould not perform efficiently for the laboratoryand simultaneously search a large data base.
Archival of purged patient data presents an-other problem for the minicomputer-based lab-oratory system. Although the Honeywell systemprovides the capability to transfer data to mag-netic tape, it is very difficult to retrieve the datafrom tape for a single patient or for a group ofpatients using the programs provided with thesystem. In addition, the output does not providea readable report. These problems could be cor-rected; however, it would become necessary tomaintain a computerized indexing system tohelp locate the tapes on which the desired dataare stored.There is a growing interest in the use of com-
puters to provide interpretative reports of labo-ratory data (1) based on a synthesis of a varietyof discrete parameters. It might be possible toprovide a physician with therapeutic recommen-dations based on the body site from which wasisolated an organism with a given antibiotic sus-ceptibility pattern. Similarly, through integra-tion of laboratory and medication data onemight provide the clinician with an early warn-ing of possible harmful side effects of antibioticsor other drugs the patient was receiving. Inte-gration of drug and laboratory data would notbe practical without a hospital information sys-tem. However, a dedicated laboratory system
on May 8, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

COMPUTERIZATION IN CLINICAL MICROBIOLOGY 875
could provide the capability of retrieving anddisplaying laboratory data relating to organ sys-tems or diseases, e.g., a meningitis profile mightinclude cerebrospinal fluid cell count, differen-tial, protein, glucose, culture, etc.
It should be noted that Honeywell is no longeractively marketing the system we have de-scribed. However, there is an active users group,and the possibility exists that Honeywell willdevelop a laboratory system for use on their newgeneration of minicomputers.
ACKNOWLEDGMENTSWe acknowledge the very fine work of the Honeywell
programming staff, particularly Robert Wilson and PamelaBraunschweig.
LITERATURE CITED1. Ackerman, V. P., D. J. Groot Obbink, R. C. Pritchard,
and R. Bradbury. 1979. Consumer survey on micro-biology reports. Lancet 1:199-202.
2. Andrews, H. J., and M. Vickers. 1974. An assessmentof one year of computer-assisted microbiology reportingat Charing Cross Hospital. J. Clin. Pathol. 27:185-191.
3. Ayliffe, P. F., and R. Chalke. 1973. A computer systemto perform record handling and reporting for a hospitalmicrobiology laboratory. Med. Lab. Technol. 30:363-371.
4. Farrar, J. L., T. D. Brogan, T. Moulding, R. Taylor,
and M. Page. 1975. Use of a computer for producingmicrobiological reports and for data storage and proc-essing. J. Clin. Pathol. 28:580-586.
5. Goodwin, C. S., and B. Clare Smith. 1976. Computerprinting and filing of microbiology reports; 1 descriptionof the system. J. Clin. Pathol. 29:543-552.
6. Jorgensen, J. H., P. Holmes, W. L. Williams, and J.L. Harris. 1978. Computerization of a hospital clinicalmicrobiology laboratory. Am. J. Clin. Pathol. 69:605-614.
7. Kunz, L J., J. W. Poitras, J. Kissling, B. A. Mercier,M. Cameron, C. Lazarus, R. C. Moellering, Jr., andG. 0. Barnett. 1975. The role of the computer inmicrobiology, p. 181-193. In J. E. Prier, J. Bartola, andH. Friedman (ed.), Modem methods in medical micro-biology: systems and trends. University Park Press,Baltimore.
8. Mitchison, D. A., J. H. Darrell, and R. Mitchison.1978. A computer-assisted bacteriology reporting andinformation system. J. Clin. Pathol. 31:673-680.
9. National Institutes of Health. 1974. Request for pro-posals, clinical laboratory information system, RFPNIH-CC-74-4. National Institutes of Health, Bethesda,Md.
10. Sindak, N., and E. Sindak. 1973. The laymans dictionaryof computer terminology. Hawthorn, New York.
11. Vermenlen, G. D., J. W. Genster, V. M. Young, andR. K. C. Hsieth. 1974. A computerized data storageand retrieval system for clinical microbiology. Am. J.Clin. Pathol. 61:209-215.
12. Williams, K. N., J. M. F. Davidson, R. Lynn, E. Rice,and I. Phillips. 1978. A computer system for clinicalmicrobiology. J. Clin. Pathol. 31:1193-1201.
VOL. 10, 1979
on May 8, 2020 by guest
http://jcm.asm
.org/D
ownloaded from





























