Embed Size (px)
Citation preview

Microprosthetic Implant for the Treatment of Erectile Dysfunction
Matt Schwartz and Robert DouglasAdvisor – Dr. Franz Baudenbacher

Thesis
• A microprosthetic drug delivery implant has the potential to provide a biomimetic treatment option for erectile dysfunction. –Minimally invasive– Patient compliance– Targeted drug release and control

Erectile Dysfunction Background
• Erectile Dysfunction (ED)– Prevalence in men 40-70 = 52%1
– Current treatment options• Prescription oral pills• Injection therapy• Penile prosthetics
– Drug therapy market size• $3.1 billion in 2005• Estimated growth of 6.5% annually through 20102

Pathophysiology• Physiology of erection
• Erectile tissue – cavernous smooth muscles– Low blood flow in flaccid state– Stimulation causes arterioles to dilate3
• Neurophysiologoy– Cavernous nerves – neurovascular control of erection/detumescence– Dorsal nerve – sensory function
• Pathology of ED– Psychogenic– Neurogenic
• Estimated at 10-19%• Iatrogenic
– Arteriogenic– Combination
Problem and Solution
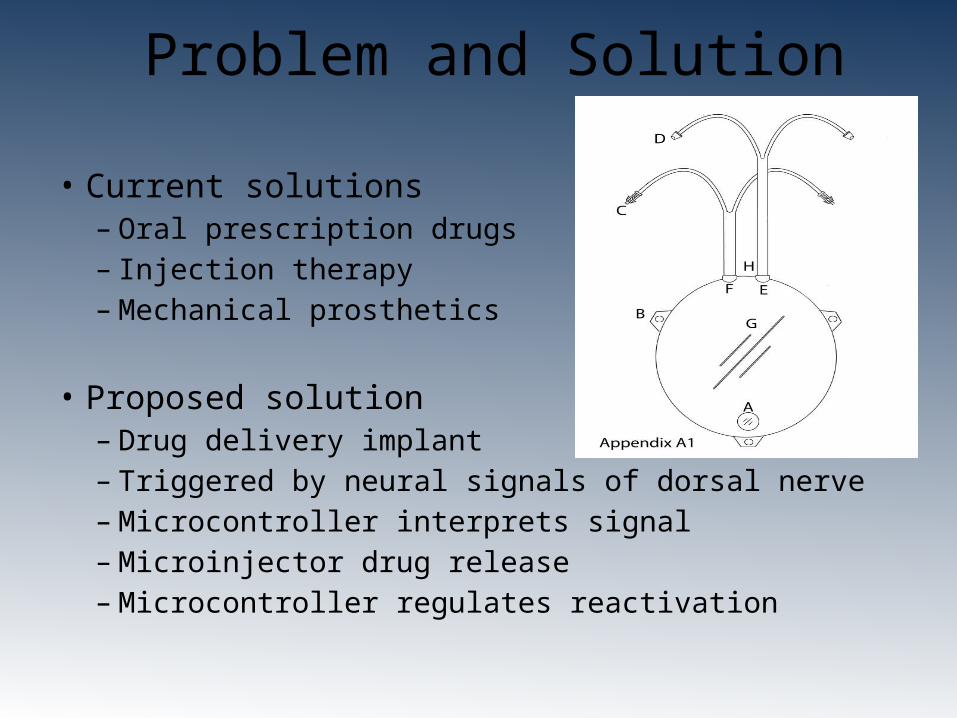
• Current solutions– Oral prescription drugs– Injection therapy– Mechanical prosthetics
• Proposed solution– Drug delivery implant– Triggered by neural signals of dorsal nerve– Microcontroller interprets signal– Microinjector drug release– Microcontroller regulates reactivation

Design Parameters• Dorsal nerve input interface• Drug reservoir, microprocessor, power supply, microinjector
– Refillable reservoir– Power saving sleep mode
• Candidates for drug release– Papaverine– Prostaglandin E1– Affects reservoir size and flow specifications
• Surgical Technique and Implantation– Site – Anterior face of pubic bone– Proximity to anatomical targets– Minimally invasive

System Flow Chart

Microprocessor Flow Chart

Timeline of Future Work• Week ending 2/6/10 – Finalize list of components needed for proof
of concept, consult with Dr. Doug Milam on device parameters • Week ending 2/13/10 – Order/fabricate proof of concept components• Week ending 2/20/10 – Contact pharmacologist and companies
involved with related technologies• Week ending 2/27/10 – Assemble proof of concept device, change
specifications with Dr. Doug Milam’s recommendations• Week ending 3/6/10 – Finalize specifications and component list for
scaled up prototype device, order/fabricate components • Week ending 3/20/10 – Setup testing scenarios for prototype device • Week ending 3/27/10 – Begin assembly of prototype device• Week ending 4/3/10 – Complete prototype device assembly, begin
device testing• Week ending 4/10/10 – Complete device testing, calculate
specifications for to-scale device

References
1. Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: Results of the Massachusetts Male Aging Study. Urology 1994; 151: 54-61.
2. Elder, Melissa. Men’s Health: The Worldwide Market for Current and Emerging Drug Therapies, 2nd ed. Kalorma Information. May 2006.
3. Robert C. Dean, MD and Tom F. Lue, MD. Physiology of penile erection and pathophysiology of erectile dysfunction. Urol Clin North Am. 2005 November; 32(4): 379-v.
4. “Codman 3000.” Codman Pumps. 15 Oct. 2009. Web. <http://www.codman.com/DePuy/products/Products/neuromodulation/pump/index.html>.
5. Sacral Plexus of the Right Side. Gray’s Anatomy.