Embed Size (px)
Citation preview

Microsatellite Instability and Loss ofHeterozygosity in Prostatic Carcinomas:Comparison of Primary Tumors, and of
Corresponding Recurrences AfterAndrogen-Deprivation Therapy and
Lymph-Node Metastases
Helmut Rohrbach,* Christian J. Haas, Gustavo B. Baretton,Astrid Hirschmann, Joachim Diebold, Ralf-Peter Behrendt, and Udo Lohrs
Institute of Pathology, Ludwig-Maximilians-University, Munich, Germany
BACKGROUND. The molecular mechanisms leading to prostate cancer progression arepoorly understood. In particular, those changes which are responsible for androgen-independent growth and metastatic spread in prostate cancer are an issue of current inves-tigations.METHODS. To gain more insight into these processes, paired microdissected samples fromboth untreated, locally advanced primary tumors (n = 20) and recurrences (n = 20) afterconventional androgen-deprivation therapy (ADT) were analyzed retrospectively for micro-satellite instability (MSI) and loss of heterozygosity (LOH) at nine loci on chromosomes 8, 18,and X by polymerase chain reaction. In parallel, 12 prostatic carcinomas treated by radicalprostatectomy and nine corresponding lymph-node metastases were analyzed in the sameway.RESULTS. The group treated with ADT showed a total of 10 MSI in 7 of the primary tumors(35%): 4 of these (20%) at one locus, and 3 of these (15%) at two loci. In the recurrences, MSIwas observed in 4 cases (20%): 3 of these at one locus (15%), and 1 of these (5%) at two loci.LOH was found in 8 cases (40%) before as well as after ADT. In the radically resectedcarcinomas, MSI could be detected at two chromosomal loci in one of the primary tumors (8%)and in one of the metastases (11%); LOH was found in 2 primaries (16%) and 3 metastases(33%).CONCLUSIONS. Although MSI can be found in advanced prostatic carcinomas, it appar-ently does not play a major role in the progression of prostate cancer regarding androgen-independent growth or lymphogenous spread. Prostate 40:20–27, 1999.© 1999 Wiley-Liss, Inc.
KEY WORDS: prostatic carcinoma; tumor progression; androgen-independence; micro-satellite instability; LOH; polymerase chain reaction
INTRODUCTION
Carcinoma of the prostate is one of the most com-mon malignancies in men in the Western Hemisphere[1]. Androgens (testosterone and 5a-dihydrotestoster-one) are required for embryonal development, differ-entiation, and growth of the prostatic gland. Under
Grant sponsor: Deutsche Forschungsgemeinschaft; Grant number:BA 1458/2-1.*Correspondence to: Dr. Helmut Rohrbach, Institute of Pathology,Ludwig-Maximilians-University-Munich, Thalkirchnerstr. 36,D-80337 Munchen, Germany. E-mail: [email protected] 24 June 1998; Accepted 10 December 1998
The Prostate 40:20–27 (1999)
© 1999 Wiley-Liss, Inc.

conditions of androgen withdrawal, programmed celldeath/apoptosis is induced physiologically. Thus, an-drogen-deprivation therapy (ADT) performed eitherby castration or by other forms of endocrine manipu-lation (e.g., antiandrogens, luteinizing hormone re-leasing hormone (LHRH) analogues) has been used aspalliative therapy for locally advanced or metasta-sized prostatic carcinomas for more than five decades[2]. In spite of favorable clinical response to ADT inabout 80% of cases, however, nearly all tumors prog-ress to androgen-independent growth within a fewyears [3,4].
The molecular mechanisms underlying androgen-independent growth are poorly understood. One hy-pothesis focuses on the androgen receptor (AR). Theandrogen receptor is a key element of the androgensignal transduction cascade in androgen-responsivetissues. Mutations of the AR gene, located on the longarm of chromosome X, have been described in theliterature [4–7]. Recently an amplification of the ARgene was found in 30% of cases after ADT [8]. Thus,mutant or amplified androgen receptor moleculesmight contribute to a growth advantage of tumor cellpopulations. However, these changes could be de-tected only in a subset of prostatic carcinomas.
Alternately, the regular androgen-dependentgrowth control might be overruled by the activation of“classical” oncogenes or the loss of tumor suppressorgenes. Nonrandom losses of parts of chromosomescan be observed in different genetic locations [9,10] inprostate cancer and may give clues to the location oftumor suppressor genes. One “hot spot” of geneticalterations in prostate cancer is the short arm of chro-mosome 8. Numerous authors were able to find dele-tions of chromosomal material in this location in up to80% of cases [11–20]. Several regions on 8p were de-leted, suggesting the location of still unknown tumor-suppressor genes at these sites.
Losses of centromeric regions of chromosome 18were detected in 58% of prostate cancers in a previousinterphase-cytogenetic study by our group [21]. Otherstudies revealed chromosomal losses on the long armof chromosome 18 in up to 45% [22], involving genessuch as the DCC (deleted in colorectal carcinoma) tu-mor-suppressor gene and the apoptosis-inhibitingBCL2 protooncogene.
Another hypothesis, concerning multiple mutationsfound in tumors, postulates mutations in mismatchrepair genes. This mechanism of tumorigenesis hasbeen demonstrated recently in hereditary nonpolypo-sis colonic carcinomas (HNPCC); [23–25]. Mutationsin the mismatch repair genes hMSH2 and hMLH1 areassociated with microsatellite instability (MSI), i.e., in-creased variability in lengths of microsatellites. Mi-crosatellites are highly repetitive mono-, di-, tri-, or
tetranucleotide sequences spread over the whole hu-man genome and are located between and withingenes. Physiologically, they show high interindividualpolymorphism in length relative to different chromo-somal loci and exhibit intraindividually differentlengths in corresponding alleles on homologous chro-mosomes. Therefore, microsatellites are genetic mark-ers suitable for the investigation of both microsatelliteinstability (MSI) and loss of heterozygosity (LOH).
In this study, we investigated paired specimensfrom primary prostatic carcinomas and from corre-sponding recurrences after ADT or from lymph-nodemetastases without ADT for genetic alterations in mi-crosatellites on the short arm of chromosome 8 (8p),on the short and long arms of chromosome 18 (18pand 18q), and on the short and long arms of chromo-some X (Xp and Xq). By comparison of the results, wehoped to gain more insight into the genetic changesleading to prostate cancer progression.
MATERIALS AND METHODS
Tumor Samples
In the first group, paired specimens of transurethralresections of the prostate gland from patients withhormonally untreated primary carcinomas (n = 20)and corresponding androgen-independent recur-rences (n = 20) up to 9 years after conventional ADTwere analyzed retrospectively in comparison withnormal prostatic tissue of the patients. The age of pa-tients treated palliatively with transurethral resectionof prostate carcinoma ranged between 47–82 years(average, 71.5 years) at the time of operation. All caseswere revised and graded according to the Gleasonscheme [26]. Accordingly, 80% of these carcinomaswere classified as high-grade tumors with Gleasonscores between 7–10 (mean Gleason score, 7.65).
In the second group, specimens of 12 patients withprostate cancer treated primarily with radical prosta-tectomy were analyzed in the same way, includinglymph-node metastases which were present in 9 ofthese 12 cases. The mean age of these patients rangedbetween 47–76 years (average, 63 years) at time ofresection. Ninety-two percent of the tumors werehigh-grade, with Gleason scores between 7–9 (meanGleason score, 8). In 83% of cases, a locally advancedtumor stage (pT3b) and lymph-node metastases (pN1)were diagnosed postoperatively according to theUICC classification [27]. In 9 cases, tumor tissue in thelymph-node metastases was sufficient for moleculargenetic investigations.
DNA Extraction and Polymorphism Analysis
Tumor tissue was routinely formalin-fixed and par-affin-embedded. In order to study representative tu-
Microsatellite Instability in Prostate Cancer 21
mor areas in close correlation to histomorphology, mi-crodissection was performed in the group of transure-thrally resected tumors from 8-mm sections which hadbeen mounted on lysin-treated slides, deparaffinizedby standard procedures, and briefly stained with eo-sin. For DNA extraction from the group of radical re-sected prostates, tumor tissue sections were trans-ferred directly into reaction tubes before deparaf-finization.
DNA was extracted with the QIAamp Tissue Kit(Quiagen, Hilden, Germany) according to the manu-facturer’s protocol. Polymorphism analysis was per-formed for the microsatellites on 8p (D8S265 andD8S560), on 18p (D18S59), on 18q (D18S60, D18S64,and D18S499), on Xp (DXS1060), and on Xq (DXS1215and DXS1213). They were amplified by polymerasechain reaction (PCR) with primers as described byGyapay et al. [28] and van Kessel et al. [29]. For thePCR reaction, 1 ml of extracted DNA was used per 50ml reaction mix. Amplification was performed on aGeneAmp PCR system 2400 (Perkin-Elmer, Norwalk,CT) with annealing temperatures between 52–60°C,depending on the primers used. PCR products wereseparated on a 10% native polyacrylamide gel and vi-sualized by silver staining [30].
RESULTS
Prostatic Carcinomas Before and AfterAndrogen-Deprivation Therapy
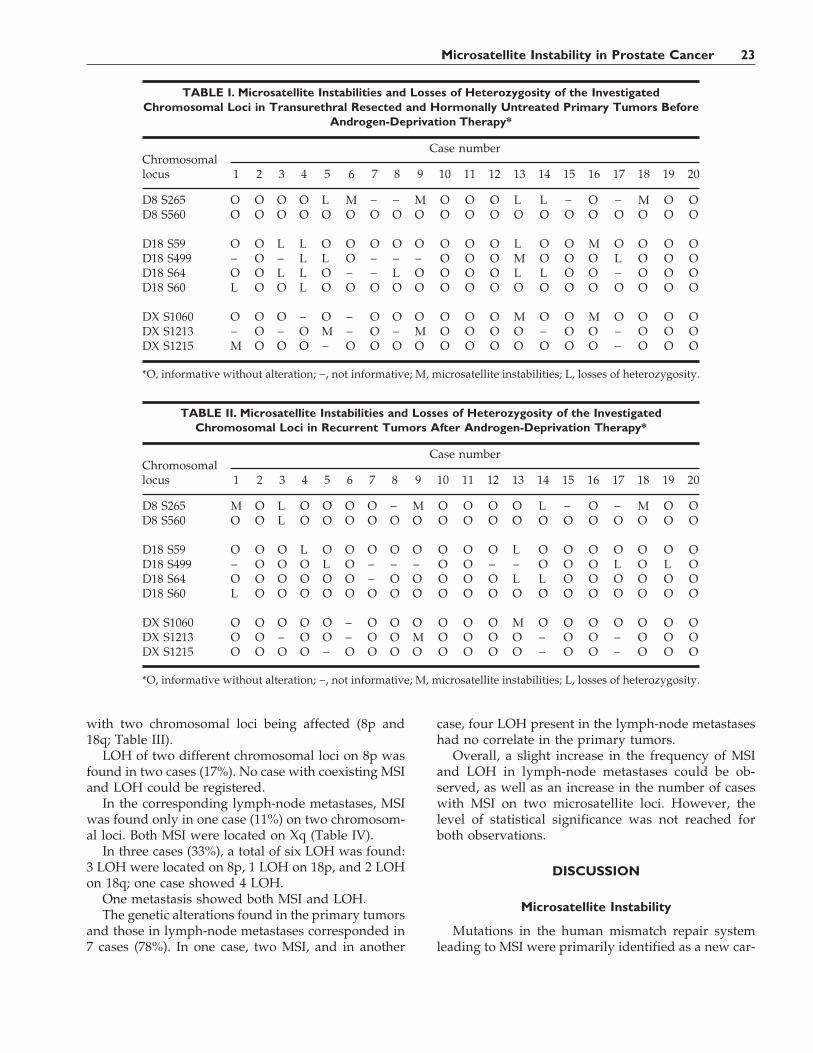
A total of 10 MSI was found in 7 cases (35%) of the20 prostate cancer specimens before ADT. In 4 cases(20%), MSI could be detected at one locus; 3 cases(15%) showed MSI on two chromosomal loci. ThreeMSI were revealed on 8p, 1 MSI on 18p, 1 MSI on 18q,2 MSI on Xp, and 3 MSI on Xq (Table I).
In the same group, 16 LOH were found: 3 LOH on8p and on 18p, and 10 LOH on 18q; 8 cases (40%)showed LOH on 1–4 chromosomal loci.
In 3 cases (15%), both MSI and LOH were present.After ADT, 5 MSI were observed in 4 cases (20%),
located 3 times on 8p, and once on Xp and once on Xq(Table II). In 3 of the cases (15%), an MSI was found onone locus, and in one case (5%) on two chromosomalloci.
Eleven LOH were diagnosed after ADT: 3 LOH on8p, 2 LOH on 18p, and 6 LOH on 18q. Eight cases(40%) showed LOH on 1–2 chromosomal loci. Twocases (10%) showed both MSI and LOH.
The comparison of genetic alterations detected inthe specimens from the hormonally untreated primarytumors and from tumor tissue after ADT showed cor-responding results in 10 cases (50%). In 7 cases (35%),
less MSI and LOH were present in the recurrencesafter ADT as compared to the primary tumors. Twocases (10%) exhibited a different mutation pattern inregard to localization of MSI and LOH. In one case(5%), a new LOH was detected in the recurrence.Overall, a trend towards a decrease in the frequency ofMSI and LOH could be observed in the recurrent tu-mors as well as a decrease of cases with MSI on twomicrosatelite loci.
Prostatic Carcinomas and RegionalLymph-Node Metastases
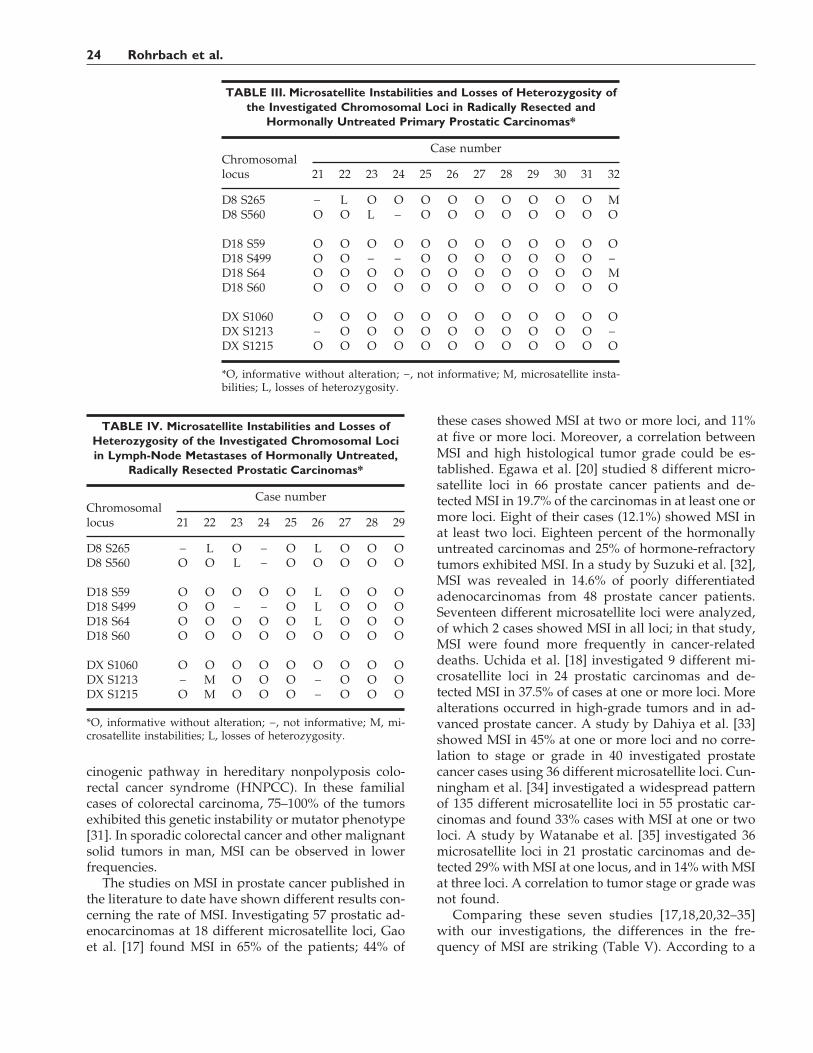
The group of 12 primary tumors found in prosta-tectomy specimens showed MSI only in one case (8%),
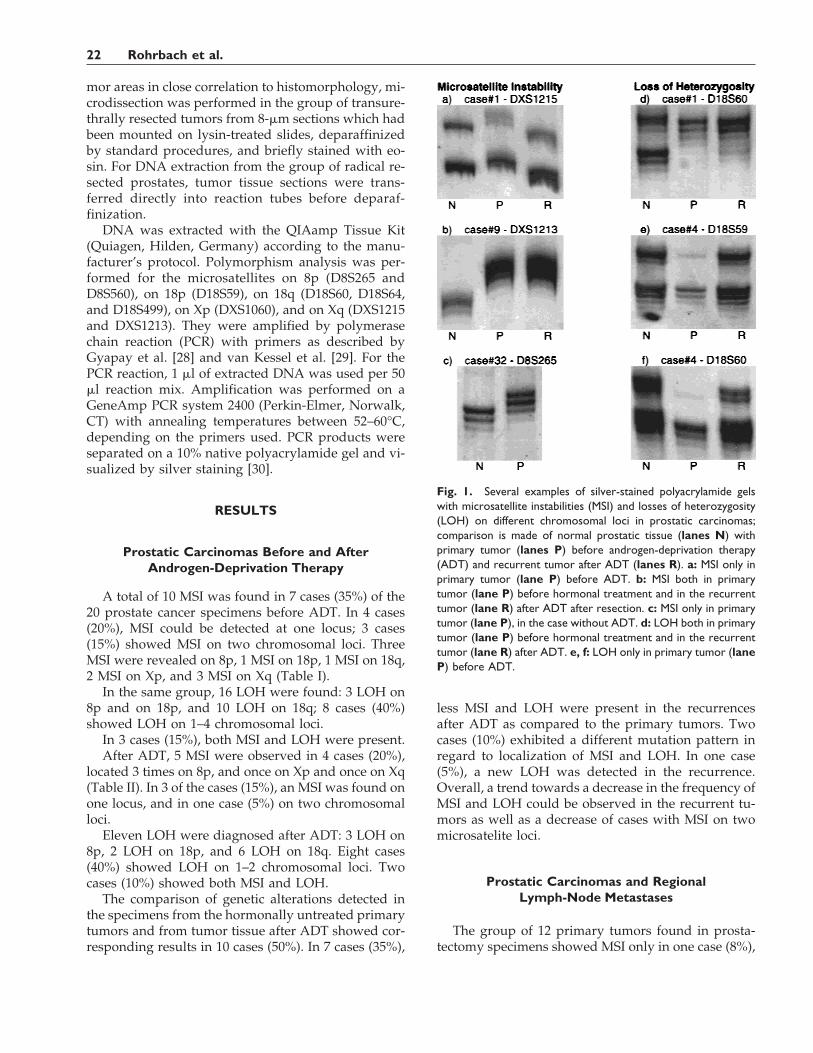
Fig. 1. Several examples of silver-stained polyacrylamide gelswith microsatellite instabilities (MSI) and losses of heterozygosity(LOH) on different chromosomal loci in prostatic carcinomas;comparison is made of normal prostatic tissue (lanes N) withprimary tumor (lanes P) before androgen-deprivation therapy(ADT) and recurrent tumor after ADT (lanes R). a: MSI only inprimary tumor (lane P) before ADT. b: MSI both in primarytumor (lane P) before hormonal treatment and in the recurrenttumor (lane R) after ADT after resection. c: MSI only in primarytumor (lane P), in the case without ADT. d: LOH both in primarytumor (lane P) before hormonal treatment and in the recurrenttumor (lane R) after ADT. e, f: LOH only in primary tumor (laneP) before ADT.
22 Rohrbach et al.
with two chromosomal loci being affected (8p and18q; Table III).
LOH of two different chromosomal loci on 8p wasfound in two cases (17%). No case with coexisting MSIand LOH could be registered.
In the corresponding lymph-node metastases, MSIwas found only in one case (11%) on two chromosom-al loci. Both MSI were located on Xq (Table IV).
In three cases (33%), a total of six LOH was found:3 LOH were located on 8p, 1 LOH on 18p, and 2 LOHon 18q; one case showed 4 LOH.
One metastasis showed both MSI and LOH.The genetic alterations found in the primary tumors
and those in lymph-node metastases corresponded in7 cases (78%). In one case, two MSI, and in another
case, four LOH present in the lymph-node metastaseshad no correlate in the primary tumors.
Overall, a slight increase in the frequency of MSIand LOH in lymph-node metastases could be ob-served, as well as an increase in the number of caseswith MSI on two microsatellite loci. However, thelevel of statistical significance was not reached forboth observations.
DISCUSSION
Microsatellite Instability
Mutations in the human mismatch repair systemleading to MSI were primarily identified as a new car-
TABLE I. Microsatellite Instabilities and Losses of Heterozygosity of the InvestigatedChromosomal Loci in Transurethral Resected and Hormonally Untreated Primary Tumors Before
Androgen-Deprivation Therapy*
Chromosomallocus
Case number
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
D8 S265 O O O O L M − − M O O O L L − O − M O OD8 S560 O O O O O O O O O O O O O O O O O O O O
D18 S59 O O L L O O O O O O O O L O O M O O O OD18 S499 − O − L L O − − − O O O M O O O L O O OD18 S64 O O L L O − − L O O O O L L O O − O O OD18 S60 L O O L O O O O O O O O O O O O O O O O
DX S1060 O O O − O − O O O O O O M O O M O O O ODX S1213 − O − O M − O − M O O O O − O O − O O ODX S1215 M O O O − O O O O O O O O O O O − O O O
*O, informative without alteration; −, not informative; M, microsatellite instabilities; L, losses of heterozygosity.
TABLE II. Microsatellite Instabilities and Losses of Heterozygosity of the InvestigatedChromosomal Loci in Recurrent Tumors After Androgen-Deprivation Therapy*
Chromosomallocus
Case number
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
D8 S265 M O L O O O O − M O O O O L − O − M O OD8 S560 O O L O O O O O O O O O O O O O O O O O
D18 S59 O O O L O O O O O O O O L O O O O O O OD18 S499 − O O O L O − − − O O − − O O O L O L OD18 S64 O O O O O O − O O O O O L L O O O O O OD18 S60 L O O O O O O O O O O O O O O O O O O O
DX S1060 O O O O O − O O O O O O M O O O O O O ODX S1213 O O − O O − O O M O O O O − O O − O O ODX S1215 O O O O − O O O O O O O O − O O − O O O
*O, informative without alteration; −, not informative; M, microsatellite instabilities; L, losses of heterozygosity.
Microsatellite Instability in Prostate Cancer 23
cinogenic pathway in hereditary nonpolyposis colo-rectal cancer syndrome (HNPCC). In these familialcases of colorectal carcinoma, 75–100% of the tumorsexhibited this genetic instability or mutator phenotype[31]. In sporadic colorectal cancer and other malignantsolid tumors in man, MSI can be observed in lowerfrequencies.
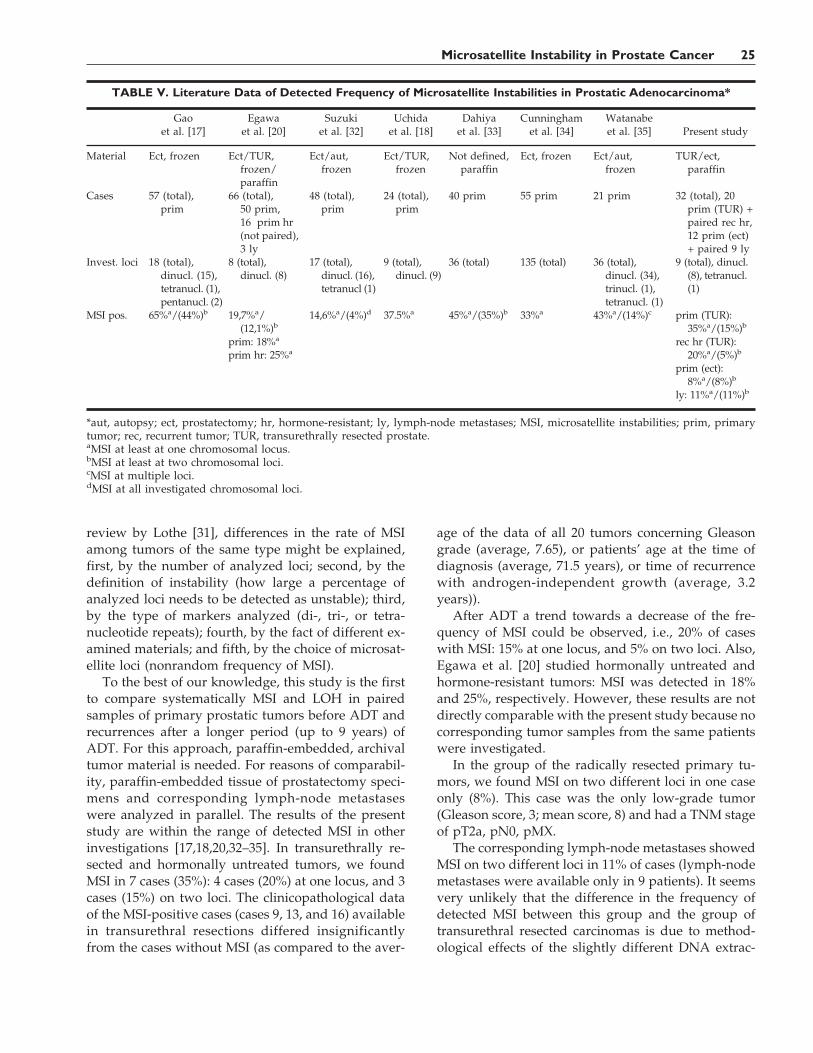
The studies on MSI in prostate cancer published inthe literature to date have shown different results con-cerning the rate of MSI. Investigating 57 prostatic ad-enocarcinomas at 18 different microsatellite loci, Gaoet al. [17] found MSI in 65% of the patients; 44% of
these cases showed MSI at two or more loci, and 11%at five or more loci. Moreover, a correlation betweenMSI and high histological tumor grade could be es-tablished. Egawa et al. [20] studied 8 different micro-satellite loci in 66 prostate cancer patients and de-tected MSI in 19.7% of the carcinomas in at least one ormore loci. Eight of their cases (12.1%) showed MSI inat least two loci. Eighteen percent of the hormonallyuntreated carcinomas and 25% of hormone-refractorytumors exhibited MSI. In a study by Suzuki et al. [32],MSI was revealed in 14.6% of poorly differentiatedadenocarcinomas from 48 prostate cancer patients.Seventeen different microsatellite loci were analyzed,of which 2 cases showed MSI in all loci; in that study,MSI were found more frequently in cancer-relateddeaths. Uchida et al. [18] investigated 9 different mi-crosatellite loci in 24 prostatic carcinomas and de-tected MSI in 37.5% of cases at one or more loci. Morealterations occurred in high-grade tumors and in ad-vanced prostate cancer. A study by Dahiya et al. [33]showed MSI in 45% at one or more loci and no corre-lation to stage or grade in 40 investigated prostatecancer cases using 36 different microsatellite loci. Cun-ningham et al. [34] investigated a widespread patternof 135 different microsatellite loci in 55 prostatic car-cinomas and found 33% cases with MSI at one or twoloci. A study by Watanabe et al. [35] investigated 36microsatellite loci in 21 prostatic carcinomas and de-tected 29% with MSI at one locus, and in 14% with MSIat three loci. A correlation to tumor stage or grade wasnot found.
Comparing these seven studies [17,18,20,32–35]with our investigations, the differences in the fre-quency of MSI are striking (Table V). According to a
TABLE III. Microsatellite Instabilities and Losses of Heterozygosity ofthe Investigated Chromosomal Loci in Radically Resected and
Hormonally Untreated Primary Prostatic Carcinomas*
Chromosomallocus
Case number
21 22 23 24 25 26 27 28 29 30 31 32
D8 S265 − L O O O O O O O O O MD8 S560 O O L − O O O O O O O O
D18 S59 O O O O O O O O O O O OD18 S499 O O − − O O O O O O O −D18 S64 O O O O O O O O O O O MD18 S60 O O O O O O O O O O O O
DX S1060 O O O O O O O O O O O ODX S1213 − O O O O O O O O O O −DX S1215 O O O O O O O O O O O O
*O, informative without alteration; −, not informative; M, microsatellite insta-bilities; L, losses of heterozygosity.
TABLE IV. Microsatellite Instabilities and Losses ofHeterozygosity of the Investigated Chromosomal Lociin Lymph-Node Metastases of Hormonally Untreated,
Radically Resected Prostatic Carcinomas*
Chromosomallocus
Case number
21 22 23 24 25 26 27 28 29
D8 S265 − L O − O L O O OD8 S560 O O L − O O O O O
D18 S59 O O O O O L O O OD18 S499 O O − − O L O O OD18 S64 O O O O O L O O OD18 S60 O O O O O O O O O
DX S1060 O O O O O O O O ODX S1213 − M O O O − O O ODX S1215 O M O O O − O O O
*O, informative without alteration; −, not informative; M, mi-crosatellite instabilities; L, losses of heterozygosity.
24 Rohrbach et al.
review by Lothe [31], differences in the rate of MSIamong tumors of the same type might be explained,first, by the number of analyzed loci; second, by thedefinition of instability (how large a percentage ofanalyzed loci needs to be detected as unstable); third,by the type of markers analyzed (di-, tri-, or tetra-nucleotide repeats); fourth, by the fact of different ex-amined materials; and fifth, by the choice of microsat-ellite loci (nonrandom frequency of MSI).
To the best of our knowledge, this study is the firstto compare systematically MSI and LOH in pairedsamples of primary prostatic tumors before ADT andrecurrences after a longer period (up to 9 years) ofADT. For this approach, paraffin-embedded, archivaltumor material is needed. For reasons of comparabil-ity, paraffin-embedded tissue of prostatectomy speci-mens and corresponding lymph-node metastaseswere analyzed in parallel. The results of the presentstudy are within the range of detected MSI in otherinvestigations [17,18,20,32–35]. In transurethrally re-sected and hormonally untreated tumors, we foundMSI in 7 cases (35%): 4 cases (20%) at one locus, and 3cases (15%) on two loci. The clinicopathological dataof the MSI-positive cases (cases 9, 13, and 16) availablein transurethral resections differed insignificantlyfrom the cases without MSI (as compared to the aver-
age of the data of all 20 tumors concerning Gleasongrade (average, 7.65), or patients’ age at the time ofdiagnosis (average, 71.5 years), or time of recurrencewith androgen-independent growth (average, 3.2years)).
After ADT a trend towards a decrease of the fre-quency of MSI could be observed, i.e., 20% of caseswith MSI: 15% at one locus, and 5% on two loci. Also,Egawa et al. [20] studied hormonally untreated andhormone-resistant tumors: MSI was detected in 18%and 25%, respectively. However, these results are notdirectly comparable with the present study because nocorresponding tumor samples from the same patientswere investigated.
In the group of the radically resected primary tu-mors, we found MSI on two different loci in one caseonly (8%). This case was the only low-grade tumor(Gleason score, 3; mean score, 8) and had a TNM stageof pT2a, pN0, pMX.
The corresponding lymph-node metastases showedMSI on two different loci in 11% of cases (lymph-nodemetastases were available only in 9 patients). It seemsvery unlikely that the difference in the frequency ofdetected MSI between this group and the group oftransurethral resected carcinomas is due to method-ological effects of the slightly different DNA extrac-
TABLE V. Literature Data of Detected Frequency of Microsatellite Instabilities in Prostatic Adenocarcinoma*
Gaoet al. [17]
Egawaet al. [20]
Suzukiet al. [32]
Uchidaet al. [18]
Dahiyaet al. [33]
Cunninghamet al. [34]
Watanabeet al. [35] Present study
Material Ect, frozen Ect/TUR,frozen/paraffin
Ect/aut,frozen
Ect/TUR,frozen
Not defined,paraffin
Ect, frozen Ect/aut,frozen
TUR/ect,paraffin
Cases 57 (total),prim
66 (total),50 prim,16 prim hr(not paired),3 ly
48 (total),prim
24 (total),prim
40 prim 55 prim 21 prim 32 (total), 20prim (TUR) +paired rec hr,12 prim (ect)+ paired 9 ly
Invest. loci 18 (total),dinucl. (15),tetranucl. (1),pentanucl. (2)
8 (total),dinucl. (8)
17 (total),dinucl. (16),tetranucl (1)
9 (total),dinucl. (9)
36 (total) 135 (total) 36 (total),dinucl. (34),trinucl. (1),tetranucl. (1)
9 (total), dinucl.(8), tetranucl.(1)
MSI pos. 65%a/(44%)b 19,7%a/(12,1%)b
prim: 18%a
prim hr: 25%a
14,6%a/(4%)d 37.5%a 45%a/(35%)b 33%a 43%a/(14%)c prim (TUR):35%a/(15%)b
rec hr (TUR):20%a/(5%)b
prim (ect):8%a/(8%)b
ly: 11%a/(11%)b
*aut, autopsy; ect, prostatectomy; hr, hormone-resistant; ly, lymph-node metastases; MSI, microsatellite instabilities; prim, primarytumor; rec, recurrent tumor; TUR, transurethrally resected prostate.aMSI at least at one chromosomal locus.bMSI at least at two chromosomal loci.cMSI at multiple loci.dMSI at all investigated chromosomal loci.
Microsatellite Instability in Prostate Cancer 25

tion. However, it is a given fact that an exact patho-histological determination of tumor stage is not pos-sible in transurethrally resected prostatic tumor tissue.Thus a direct comparison between the transurethrallyresected and prostatectomy group is hampered re-garding stages. As transurethral resection and ADTare palliative therapy approaches, it might be as-sumed that the clinical stage was higher in the trans-urethrally resected group.
In the literature, the criteria classifying a case asmutator phenotype-positive or -negative are not ap-plied always in the same way. According to Ruschoffet al. [36], cases with instability involving only onedinucleotide repeat may fall into a potential back-ground rate and therefore should not be classified asmutator phenotype-positive. Thus, the diagnosis ofmutator phenotype-positive should be based upon atleast two affected loci, and at least five loci should betested. A muliticenter study for reliability and qualitycontrol of microsatellite instability analysis performedby Bocker et al. [37] showed a high concordance indetecting MSI, using different techniques such as sil-ver and ethidium bromide staining of polyacrylamidegels or radioactive labeling or automated fluorescencedetection.
Konishi et al. [38], investigating 20 cases of HNPCCon 5 different microsatellite loci, found in all cases MSIon 3–5 loci. Nine of the 20 cases showed mutations inthe mismatch repair genes hMSH2 or hMLH1. Apply-ing the above-mentioned criteria to our study, wewere unable to find any case that fulfilled the defini-tion of a mutator phenotype, i.e., mutations in the mis-match repair genes do not seem to play an importantrole in the progression of prostate cancer to acquiredandrogen-independence or metastatic behavior.
Loss of Heterozygosity
Allelotyping studies of prostate cancer revealed fre-quent allelic loss on different chromosomes [9]. Theinvestigation of 25 different microsatellite loci on theshort arm of chromosome 8 by Vocke et al. [13]showed LOH in a frequency from 1.2–74%. In the pre-sent study, we observed LOH on 8p in two differentloci, in a frequency up to 22% of the cases. The longarm of chromosome 18 carrying the tumor-suppressorgene DCC also showed different frequencies of de-tected LOH. Whereas Egawa et al. [20] detected noLOH, Gao et al. [22] found LOH in 45% of cases at theDCC locus. In the present study, we noticed LOH inup to 15% of the cases on one locus on 18p and onthree different loci on 18q in a frequency up to 25% ofthe cases. LOH for a microsatellite on chromosome Xcould not be proven, of course, but may be hidden inthe noninformative cases.
The frequency of detected LOH on different chro-mosomal loci in the present study showed no signifi-cant accumulation in the investigated loci.
CONCLUSIONS
Microsatellite instability (mutator phenotype) obvi-ously does not seem to play a major role in progres-sion, i.e., androgen-independent growth or lymphog-enous spread of prostate cancer. The frequency of de-tected LOH on different chromosomal loci in thepresent study showed no significant accumulation onthe investigated loci.
ACKNOWLEDGMENTS
G.B.B. and U.L. were supported by grant BA 1458/2-1 from the Deutsche Forschungsgemeinschaft.
REFERENCES
1. Dhom G. Epidemiologic aspects of latent and clinically manifestcarcinoma of the prostate. J Cancer Res Clin Oncol 1983;106:210–218.
2. Huggins C, Hodges CV. Studies on prostatic cancer. I. The effectof castration, of estrogen and of androgen injection on serumphosphatases in metastatic carcinoma of the prostate. CancerRes 1941;1:293–297.
3. Gittes RF. Carcinoma of the prostate. N Engl J Med 1991;324:236–245.
4. Taplin ME, Bubley GJ, Shuster TD, Frantz ME, Spooner AE,Ogata GK, Keer HN, Balk SP. Mutation of the androgen-receptor gene in metastatic androgen-independent prostate can-cer. N Engl J Med 1995;332:1393–1398.
5. Schoenberg MP, Hakimi JM, Wang S, Bova GS, Epstein JI, Fis-chbeck KH, Issaacs WB, Walsh PC, Barrack ER. Microsatellitemutation (CAG 24-18) in the androgen receptor gene in humanprostate cancer. Biochem Biophys Res Commun 1994;198:74–80.
6. Culig Z, Klocker H, Eberle J, Kaspar F, Hobisch A, CronauerMV, Bartsch G. DNA sequence of the androgen receptor in pros-tatic tumor cell lines and tissue specimens assessed by means ofthe polymerase chain reaction. Prostate 1993;22:11–22.
7. Irvine RA, Yu MC, Koss RK, Coetzee GA. The CAG and GGCmicrosatellites of the androgen receptor gene are in linkage dis-equilibrium in men with prostate cancer. Cancer Res 1995;55:1937–1940.
8. Visakorpi T, Hyytinen E, Koivisto P, Tanner M, Keinanen R,Palmberg C, Palotie A, Tammela T, Isola J, Kallioniemi OP. Invivo amplification of the androgen receptor gene and progres-sion of human prostate cancer. Nat Genet 1995;9:401–406.
9. Kallioniemi OP, Visakorpi T. Genetic basis and clonal evolutionof human prostate cancer. Cancer Res 1996;68:225–255.
10. Sandberg A. Chromosomal abnormalities and related events inprostate cancer. Hum Pathol 1992;23:368–380.
11. Cher ML, Bova GS, Moore DH, Small EJ, Carroll PR, Pin SS,Epstein JI, Isaacs WB, Jensen RH. Genetic alterations in un-treated metastases and androgen-independent prostate cancerdetected by comparative genomic hybridization and allelotyp-ing. Cancer Res 1996;56:3091–3102.
12. Kagan J, Stein J, Babaian RJ, Joe YS, Pisters LL, Glassman AB,von Eschenbach AC, Troncoso P. Homozygous deletions at
26 Rohrbach et al.
8p22 and 8p21 in prostate cancer implicate these regions as thesites for candidate tumor suppressor genes. Oncogene 1995;11:2121–2126.
13. Vocke CD, Pozzatti RO, Bostwick DG, Florence CD, JenningsSB, Strup SE, Duray PH, Liotta LA, Emmert-Buck MR, LinehanWM. Analysis of 99 microdissected prostate carcinomas revealsa high frequency of allelic loss on chromosome 8p12–21. CancerRes 1996;56:2411–2416.
14. Bova GS, Carter BS, Bussemakers MJG, Emi M, Fujiwara Y,Kyprianou N, Jacobs SC, Robinson JC, Epstein JI, Walsh PC,Isaacs WB. Homozygous deletion and frequent allelic loss ofchromosome 8p22 loci in human prostate cancer. Cancer Res1993;53:3869–3873.
15. Macoska JA, Trybus TM, Benson PD, Sakr WA, Grignon DJ,Wojno KD, Pietruk T, Powell IJ. Evidence for three tumor sup-pressor gene loci on chromosome 8p in human prostate cancer.Cancer Res 1995;55:5390–5395.
16. Trapman J, Sleddens HFBM, van der Weiden MM, DinjensWNM, Konig JJ, Schroder FH, Faber PW, Bosman FT. Loss ofheterozygosity of chromosome 8 microsatellite loci implicates acandidate tumor suppressor gene between the loci D8S87 andD8S133 in human prostate cancer. Cancer Res 1994;54:6061–6064.
17. Gao X, Wu N, Grignon D, Zacharek A, Liu H, Salkowski A, LiG, Sakr W, Sarkar F, Porter AT, Chen YQ, Honn KV. Highfrequency of mutator phenotype in human prostatic adenocar-cinoma. Oncogene 1994;9:2999–3003.
18. Uchida T, Wada C, Wang C, Ishida H, Egawa S, Yokoyama E,Ohtani H, Koshiba K. Microsatellite instability in prostate can-cer. Oncogene 1995;10:1019–1022.
19. Sakr WA, Macoska JA, Benson P, Grignon DJ, Wolman SR, Pon-tes JE, Crissman JD. Allelic loss in locally metastatic multi-sampled prostate cancer. Cancer Res 1994;54:3273–3277.
20. Egawa S, Uchida T, Suyama K, Wang C, Ohori M, Irie S,Iwamura M, Koshiba K. Genomic instability of microsatelliterepeats in prostate cancer: relationship to clinicopathologicalvariables. Cancer Res 1995;55:2418–2421.
21. Baretton GB, Valina C, Vogt T, Schneiderbanger K, Diebold J,Lohrs U. Interphase cytogenetic analysis of prostatic carcinomasby use of nonisotopic in situ hybridization. Cancer Res 1994;54:4472–4480.
22. Gao X, Honn KV, Grignon D, Sakr W, Chen YQ. Frequent allelicloss of expression and loss of heterozygosity of the putativetumor suppressor gene DCC in prostatic carcinomas. CancerRes 1993;53:2723–2727.
23. Loeb LA. Microsatellite instability: marker of a mutator pheno-type in cancer. Cancer Res 1994;54:5059–5063.
24. Thibodeau SN, Bren G, Schaid D. Microsatellite instability incancer of the proximal colon. Science 1993;260:816–819.
25. Aaltonen LA, Peltomaki P, Mecklin JP. Replication errors in
benign and malignant tumors from hereditary nonpolyposis co-lorectal cancer patients. Cancer Res 1994;54:1645–1648.
26. Gleason DF, Mellinger GI. Veterans Administration Coopera-tive Urological Research Group. Prediction of prognosis forprostatic adenocarcinoma by combined histological grading andclinical staging. J Urol 1974;111:58–64.
27. Sobin LH, Wittekind C. TNM classification of malignant tu-mours. New York: Wiley-Liss; 1997. p 170–173.
28. Gyapay G, Morisette J, Vignal A, Dib C, Fizames C, MillasseauP, Marc S, Bernardi G, Lathrop M, Weissenbach J. The 1993–94Genethon human genetic linkage map. Nat Genet 1994;7:246–339.
29. van Kessel HG, Straub RE, Silverman GA, Gerken S, Over-hauser J. Report of the second international workshop on hu-man chromosome 18 mapping. Cytogenet Cell Genet 1994;65:142–165.
30. Sanguinetti CJ, Dias Neto E, Simpson AJ. Rapid silver stainingand recovery of PCR products separated on polyacrylamidegels. Biotechniques 1994;17:914–921.
31. Lothe RA. Microsatellite instability in human solid tumors. MolMed Today 1997;3:61–68.
32. Suzuki H, Komiya A, Aida S, Akimoto S, Shiraishi T, Yatani R,Igarashi T, Shimazaki J. Microsatellite instability and other mo-lecular abnormalities in human prostate cancer. Jpn J CancerRes 1995;86:956–961.
33. Dahiya R, Lee C, McCarville J, Hu W, Kaur G, Deng G. Highfrequency of genetic instability of microsatellites in human pros-tatic adenocarcinoma. Int J Cancer 1997;72:762–767.
34. Cunningham J, Shan A, Wick M, McDonnell S, Schaid D, TesterD, Qian J, Takahashi S, Jenkins R, Bostwick D, Thibodeau S.Allelic imbalance and microsatellite instability in prostatic ad-enocarcinoma. Cancer Res 1996;56:4475–4482.
35. Watanabe M, Imai H, Shiraishi T, Shimazaki J, Kotake T, YataniR. Microsatellite instability in human prostate cancer. Br J Can-cer 1995;72:562–564.
36. Ruschoff J, Bocker T, Schlegel J, Stumm G, Hofstaedter F. Mic-rosatellite instability: new aspects in the carcinogenesis of colo-rectal carcinoma. Virchows Arch 1995;426:215–222.
37. Bocker T, Diermann J, Friedl W, Gebert J, Holinski-Feder E,Karner-Hanusch J, von Knebel-Doeberitz M, Koelble K,Moeslein G, Schackert H, Wirtz H, Fishel R, Ruschoff J. Micro-satellite instability analysis: a multicenter study for reliabilityand quality control. Cancer Res 1997;57:4739–4743.
38. Konishi M, Kikuchi-Yanoshita R, Tanaka K, Muraoka M, OndaA, Okumura Y, Kishi N, Iwama T, Mori T, Koike M, Ushio K,Chiba M, Nomizu S, Konishi F, Utsunomiya J, Miyaki M. Mo-lecular nature of colon tumors in hereditary nonpolyposis coloncancer, familial polyposis and sporadic colon cancer. Gastroen-terology 1996;111:307–317.
Microsatellite Instability in Prostate Cancer 27





























