Embed Size (px)
Citation preview
PRACTICAL GASTROENTEROLOGY • SEPTEMBER 2002 41
INTRODUCTION
Collagenous colitis (CC) (Figure 1) and lympho-cytic colitis (LC) (Figure 2) are uncommonchronic relapsing diarrheal illnesses. The major-
ity of patients are women in their fifth to sixth decadewho complain of profuse, watery diarrhea, and crampy
abdominal pain. Both conditions have normal mucosawhen viewed endoscopically, however biopsy speci-mens show chronic mucosal inflammation. In CCthere is a subepithelial collagen band of varying thick-ness in association with an inflammatory cell infiltratein the lamina propria (1). The collagen band is absentin LC (2,3). The term microscopic colitis (MC) wasoriginally used to describe patients with chronic diar-rhea and normal endoscopic and barium enema stud-ies, but who had evidence of mucosal inflammationwhen examined microscopically (4). This term issometimes used interchangeably with collagenous and
Microscopic Colitis: CollagenousColitis and Lymphocytic Colitis
A SPECIAL ARTICLE
Brennan A. Scott, MD, Clinical Fellow, Division of Gas-troenterology, University of California, Davis MedicalCenter. Thomas P. Prindiville, MD, FACG, Professor ofMedicine, Division of Gastroenterology, University ofCalifornia, Davis Medical Center, Sacramento, CA.
Collagenous colitis and lymphocytic colitis are chronic relapsing diarrheal illnesses,which are often referred to together as microscopic colitis. It most commonly occurs inwomen in their fifth to sixth decade. The symptoms usually include profuse waterydiarrhea and crampy abdominal pain. Laboratory and endoscopic studies are gener-ally normal but microscopic inflammation is seen when colonic biopsies are performed.In collagenous colitis there is a subepithelial collagen band in addition to chronicinflammation in the lamina propria. The etiology is not known but multiple theoriesexist including autoimmune, infectious, and medication-induced. Although the courseis generally benign, patients may have multiple relapses over many years. Treatmentregimens vary and have included anti-diarrheals, antibiotics, 5-aminosalicylates,steroids, and immunosuppressive agents.
Brennan A. Scott Thomas P. Prindiville
PRACTICAL GASTROENTEROLOGY • SEPTEMBER 200242
A SPECIAL ARTICLE
Microscopic Colitis
lymphocytic colitis, and sometimes used as anumbrella term for all forms of microscopic inflamma-tion in the colon. In this review the term MC will beused to describe either collagenous colitis and/or lym-phocytic colitis.
EPIDEMIOLOGYMicroscopic colitis can present in any age group butthe majority of patients are in their fifth to sixthdecade. While CC has a strong female predominance,with women accounting for 85%–90% of cases, LChas a roughly equal distribution between males andfemales (2,5). The incidence of CC has been reportedas 1.0/105 in France (6), 1.8/105, in Sweden (7), and1.1/105 in Spain (8). The prevalence of CC in Swedenis 15.7/105 (7). LC has been reported to have an inci-dence of 3.1/105 in Spain (8).
CLINICAL FEATURESThe most prominent feature of MC is diarrhea. In mostpatients it is described as profuse and watery, with upto ten bowel movements a day. Abdominal pain,cramping, fecal urgency, and nocturnal stools may alsobe associated. The onset is generally insidious but maybe abrupt in up to 40% of cases (9). Neither bloodystools nor steatorrhea is usually seen, and dehydrationis not a common complication. Weight loss has beenassociated with MC(9) but, if present, may suggest amore serious condition. The physical examination isunrevealing in the majority of patients as are routinelaboratory tests, stool studies, radiology, andendoscopy (Table 1). Autoantibodies and increasedserum IgM have been noted in some patients but thesignificance is not clear (10–12).
(continued on page 44)
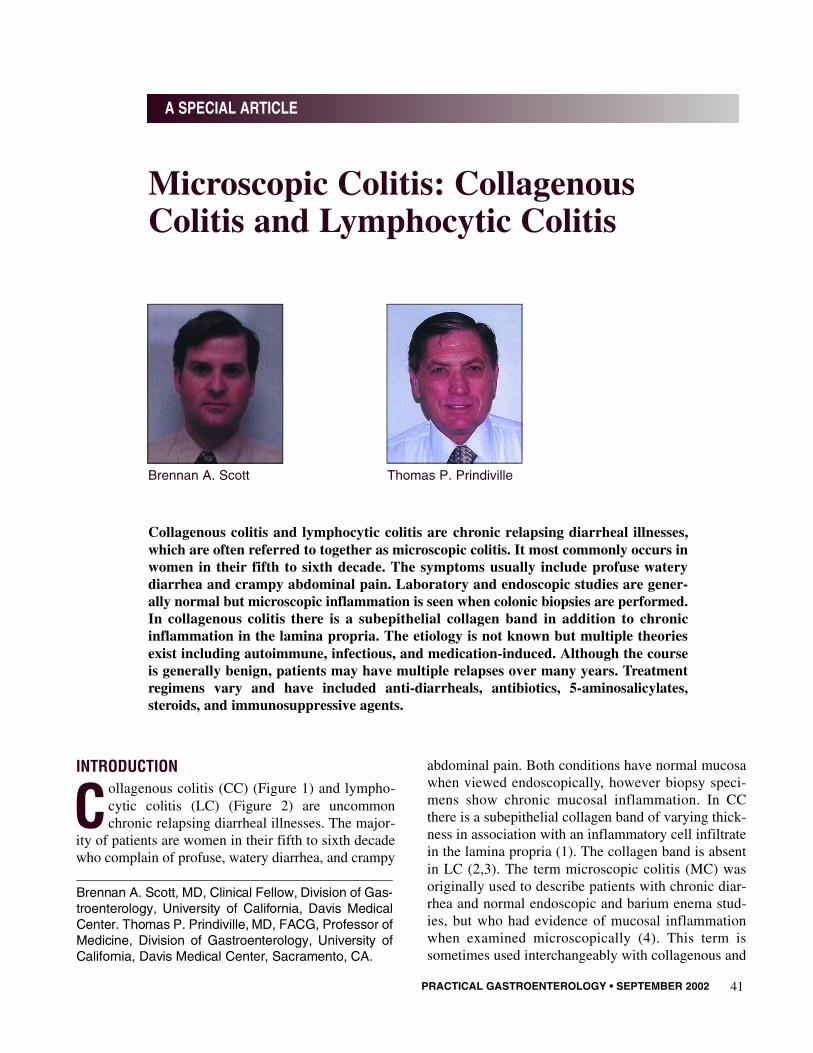
Figure 1. Collagenous Colitis: There is a mild increase in cel-lularity with a thickened subepithelial collagen band. (H&Estaining 400×)
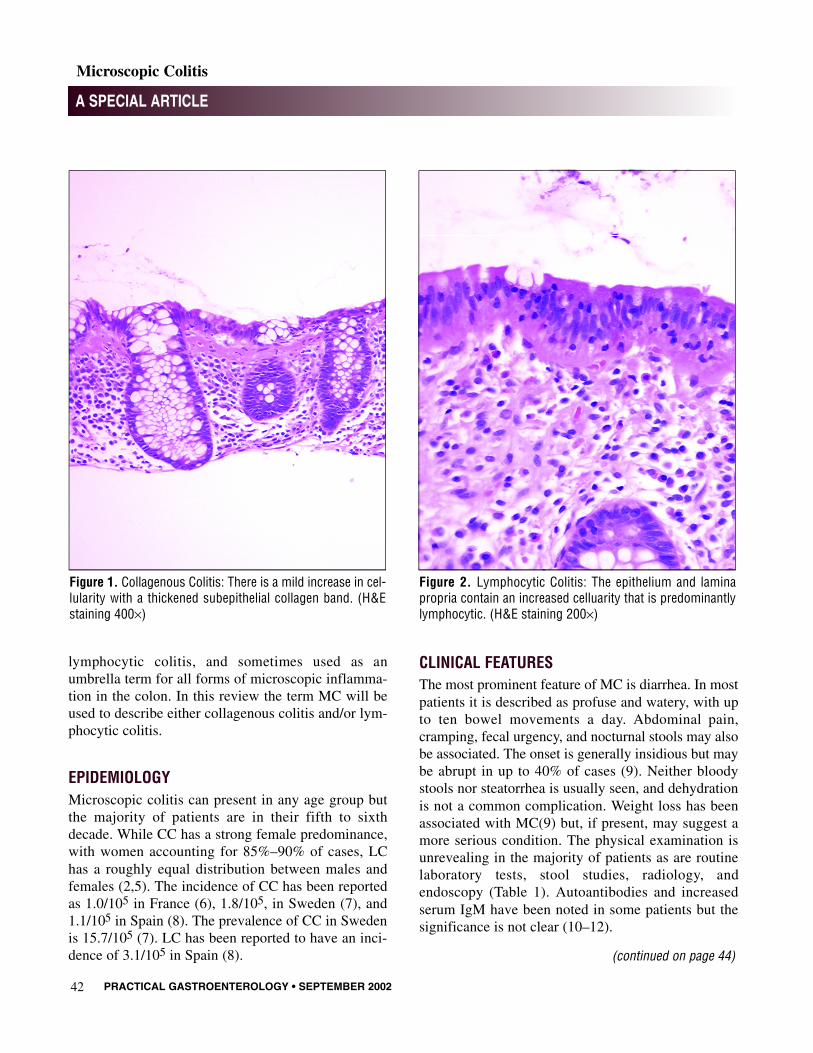
Figure 2. Lymphocytic Colitis: The epithelium and laminapropria contain an increased celluarity that is predominantlylymphocytic. (H&E staining 200×)

PRACTICAL GASTROENTEROLOGY • SEPTEMBER 200244
A SPECIAL ARTICLE
Microscopic Colitis
ASSOCIATED CONDITIONSMicroscopic colitis has been associated with otherenteropathies and autoimmune diseases. Celiac diseasehas been associated with both CC and LC, with reportsof LC patients having a 15%–27% incidence of celiacdisease (13–15). There have been reports of CC asso-ciated with Crohn’s disease (16) as well as CC pro-gressing to ulcerative colitis (17,18). There has alsobeen a case reported of synchronous CC andpseudomembranous colitis (19). Although there is noclear autoimmune etiology of MC, it has been found inassociation with many autoimmune and rheumatologicdiseases such as rheumatoid arthritis (20), systemicand discoid lupus erythematosis (21,22), spondy-loarthritis (23), CRST syndrome (24), diabetes melli-tus, pernicious anemia, Sjogren’s syndrome, autoim-mune thyroid disease, linear IgA dermatosis (25), andprimary biliary cirrhosis (26). Collagenous gastritishas been described in association with CC, suggestinga diffuse intestinal tract disorder (27). The relative riskof colorectal malignancy does not appear to beincreased in these patients (28).
DIAGNOSISIn a patient with the appropriate clinical history andunremarkable physical exam and laboratory studies, a
flexible sigmoidoscopy or colonoscopy with biopsy isnecessary to make the diagnosis. The endoscopicexamination is in most cases grossly normal, but ran-dom mucosal biopsies will show evidence of micro-scopic chronic inflammation.
HISTOLOGYBoth LC and CC have evidence of chronic inflamma-tory cell deposition in the lamina propria (generally 20lymphocytes per 100 surface epithelial cells is used for diagnosis (3)). Neutrophils, plasma cells, andeosinophils are seen less commonly (1). In CC there isan eosinophilic staining subepithelial band of collagen,which measures between 7 and 100 microns in thick-ness. The band thickness varies from each area of thecolon and is an average of 9 microns (29). The super-ficial collagen layer has been shown to stain stronglyfor collagen types I, III, and VI, as well as the glyco-protein tenascin, which is involved in matrix remodel-ing (30). A labile imbalance between fibrogenesis andfibrolysis has been proposed as the mechanism thatinduces collagen band formation (31). Biopsies shouldbe done from both the proximal and distal colon inorder to most accurately classify the disorder becausethe collagen layer is generally less thick in the distalcolon (5). Immunostaining of mucosal biopsies fortenascin and type VI collagen has recently been pro-posed as a sensitive and specific method for determin-ing the presence of CC, especially in indefinite cases(32). The sensitivity of this method may allow for thediagnosis to be made from biopsies of the rectum andsigmoid colon, avoiding colonoscopy in some patients.
PATHOGENESISMultiple theories for the etiology of microscopic colitisexist: environmental, infectious, and autoimmune. Nonutritional component or medication has been directlylinked to the disorder, but NSAID use has been sug-gested to play an etiological role, with some patients’symptoms improving after the withdrawal of the med-ication (33). There have been reports of CC associatedwith lansoprazole (34), and cimetidine (35), and reportsof LC associated with ticlodipine (36–38), ranitidine
(continued from page 42)
(continued on page 46)
Table 1 Diagnosis
Symtoms• Watery diarrhea• Crampy abdominal pain
Laboratory• Normal
Endoscopy• Normal
Muscosal biopsy• Chronic inflammatory infiltrate• Thickened subepithelial collagen layer (collagenous
colitis)

PRACTICAL GASTROENTEROLOGY • SEPTEMBER 200246
A SPECIAL ARTICLE
Microscopic Colitis
(39), and acarbose (40). Fecal stream diversion surg e r yhas been shown to induce histological remission withclinical and histologic recurrence after ostomy closure(41), suggesting that noxious luminal material mayplay a role. Bile salt malabsorption has also been pos-tulated to play a role in pathogenesis (42). Others haveraised the question of bacterial endotoxins as a cause ofMC, with the toxin-binding resin cholestyramineshown to improve symptoms (43). A toxigenic strain ofB a c t e roides fragilis has been associated with MC(44),and there have been reports of CC associated withClostridium difficile (19,45) infection. A small seriesreported collagenous colitis diagnosed after Ye r s i n i ae n t e ro c o l i t i c a infection (46), and a case of lymphocyticcolitis was attributed to Campylobacter jejuni i n f e c t i o nin one patient (47), raising the question of a post-infec-tious response causing MC. Additionally, treatment ofHelicobacter pylori has been associated with improve-ment in CC (48) (Table 2).
Some authors have suggested an immune-mediatedmechanism due to the high incidence of autoantibodiesin these patients (2). Although there are associations withmany autoimmune diseases as noted above, no clearautoimmune etiology has been postulated or proven.
The mechanism of diarrhea in patients with MC isnot entirely clear. One hypothesis has been that thecollagen band in collagenous colitis is responsible forthe symptoms, but some believe that the collagen is amere consequence of mucosal inflammation (49) andnot the causative abnormality. In addition, the symp-toms are similar between LC and CC, and there is nocollagen band to alter mucosal permeability in LC.Eosinophil activation has been noted to be increased inthe mucosa of patients with collagenous colitis (50),and has been suggested to be related to altered mucosalpermeability (51). Increased numbers of mucosal mastcells and clinical response to an H1 antagonist wasnoted in one patient suggesting a role for this mecha-nism in the production of diarrhea (52). It is possiblethat bacterial toxins induce an altered host inflamma-tory cell response in some patients leading to diarrhea.
TREATMENTA variety of therapeutic agents have been used inpatients with microscopic colitis. Most regimens aresupported by case-reports or small, uncontrolled seriesonly. A recent double-blind placebo-controlled trial of9 mg of oral budesonide versus placebo in 24 patientswith CC showed both clinical and histological short-term response (53) with budesonide. This study, how-ever, used a different formulation of budesonide thanthat currently available in the United States. An openlabel trial of bismuth subsalicylate in 13 patients withmicroscopic colitis showed it to be safe and efficacious(54). Case series or case reports have noted the suc-cessful use of many other agents. Antidiarrheals andverapamil have been used to control symptoms insome cases (55,56), and bismuth subsalicylate hasbeen shown to have a prolonged response in some(54,57). The 5-aminosalicylates, sulphasalazine, andcholestyramine have been shown to be useful in somepatients with more severe symptoms (9,58,59). Somepatients may respond to variable courses of steroids(9,58), and the immunomodulatory drugs methotrexateand 6-mercaptopurine have been used with some suc-cess in patients who have refractory symptoms or whoare steroid dependent (60–63) (Table 3).
(continued from page 44)
(continued on page 48)
Table 1 Proposed Etiologies
• Environmental (medications, dietary)• Bacterial toxins• Autoimmune
Table 3 Treatment Options
• Antidarrheals• Bismuth Subsalicylate• Cholestyramine• 5-Aminosalicylates• Sulphasalazine• Antibiotics• Budesonide• Prednisone• Methotrexate• 6-Mercaptopurine

PRACTICAL GASTROENTEROLOGY • SEPTEMBER 200248
A SPECIAL ARTICLE
Microscopic Colitis
SUMMARYMicroscopic colitis is a term that is often used toencompass the two similar disorders, lymphocytic col-itis and collagenous colitis. Both disorders are charac-terized by chronic, relapsing watery diarrhea. The diag-nosis is made in patients with the appropriate clinicalpresentation, who have normal radiographic, labora-t o r y, and endoscopic findings, but have evidence ofmicroscopic inflammation on colonic biopsy. Althoughmany theories as to its cause exist, no etiology is cur-rently known. Many treatments ranging from antidiar-reals to immunosuppressants have shown eff i c a c y, butcontrolled trials are lacking. The course of microscopiccolitis is benign in the vast majority of cases. ■
AcknowledgmentThe authors wish to thank Mark Wu, MD, and KristenVa n d e w a l k e r, MD for providing the photomicrographs.
References1. Jessurun J, Yardley JH, Giardiello FM, Hamilton SR, Bayless
TM. Chronic colitis with thickening of the subepithelial collagenlayer (collagenous colitis): histopathologic findings in 15patients. Hum Pathol, 1987;18(8):839-848.
2. Giardiello FM, Lazenby AJ, Bayless TM, et al. Lymphocytic(microscopic) colitis. Clinicopathologic study of 18 patients andcomparison to collagenous colitis. Dig Dis Sci, 1989;34(11):1730-1738.
3. Lazenby AJ, Yardley JH, Giardiello FM, Jessurun J, Bayless TM.Lymphocytic (“microscopic”) colitis: a comparative histopatho-logic study with particular reference to collagenous colitis. HumPathol, 1989;20(1):18-28.
4. Read NW, Krejs GJ, Read MG, Santa Ana CA, Morawski SG,Fordtran JS. Chronic diarrhea of unknown origin. Gastroenterol -ogy, 1980;78(2):264-271.
5. Zeroogian JM, Chopra S. Collagenous colitis and lymphocyticcolitis. Annu Rev Med, 1994;45:105-118.
6. Raclot G, Queneau PE, Ottignon Y, et al. Incidence of collage-nous colitis. A restrospective study in the east of France. Gas -troenterology, 1994;106:A23.
7. Bohr J, Tysk C, Eriksson S, Jarnerot G. Collagenous colitis inOrebro, Sweden, an epidemiological study 1984-1993. Gut,1995;37(3):394-397.
8. Fernandez-Banares F, Salas A, Forne M, Esteve M, Espinos J,Viver JM. Incidence of collagenous and lymphocytic colitis: a 5-year population- based study. Am J Gastroenterol, 1999;94(2):418-423.
9. Bohr J, Tysk C, Eriksson S, Abrahamsson H, Jarnerot G. Col-lagenous colitis: a retrospective study of clinical presentation andtreatment in 163 patients. Gut, 1996;39(96):846-851.
10. Bohr J, Tysk C, Yang P, Danielsson D, Jarnerot G. Autoantibod-ies and immunoglobulins in collagenous colitis. Gut, 1996;39(1):73-76.
11. Giardiello FM, Bayless TM, Jessurun J, Hamilton SR, YardleyJH. Collagenous colitis: physiologic and histopathologic studiesin seven patients. Ann Intern Med, 1987;106(1):46-49.
12. Roubenoff R, Ratain J, Giardiello F, et al. Collagenous colitis,enteropathic arthritis, and autoimmune diseases: results of apatient survey. J Rheumatol, 1989;16(9):1229-1232.
13. McCashland TM, Donovan JP, Strobach RS, Linder J, QuigleyEM. Collagenous enterocolitis: a manifestation of gluten-sensi-tive enteropathy. J Clin Gastroenterol, 1992;15(1):45-51.
14. Gillett HR, Freeman HJ. Prevalence of celiac disease in collage-nous and lymphocytic colitis. Can J Gastroenterol, 2000;14(11):919-921.
15. Matteoni CA, Goldblum JR, Wang N, Brzezinski A, Achkar E,Soffer EE. Celiac disease is highly prevalent in lymphocytic col-itis. J Clin Gastroenterol, 2001;32(3):225-227.
16. Chandratre S, Bramble MG, Cooke WM, Jones RA. Simultane-ous occurrence of collagenous colitis and Crohn’s disease. Diges -tion, 1987;36(1):55-60.
17. Giardiello FM, Jackson FW, Lazenby AJ. Metachronous occur-rence of collagenous colitis and ulcerative colitis. Gut, 1991;32(4):447-449.
18. Pokorny CS, Kneale KL, Henderson CJ. Progression of collage-nous colitis to ulcerative colitis. J Clin Gastroenterol, 2001;32(5):435-438.
19. Vesoulis Z, Lozanski G, Loiudice T. Synchronous occurrence ofcollagenous colitis and pseudomembranous colitis. Can J Gas -troenterol, 2000;14(4):353-358.
20. Wengrower D, Pollak A, Okon E, Stalnikowicz R. Collagenouscolitis and rheumatoid arthritis with response to sulfasalazine. Acase report and review of the literature. J Clin Gastroenterol,1987;9(4):456-460.
21. Heckerling P, Urtubey A, Te J. Collagenous colitis and systemiclupus erythematosus. Ann Intern Med, 1995;122(1):71-72.
22. Castanet J, Lacour JP, Ortonne JP. Arthritis, collagenous colitis,and discoid lupus. Ann Intern Med, 1994;120(1):89-90.
23. Kingsmore SF, Kingsmore DB, Hall BD, Wilson JA, GottfriedMR, Allen NB. Cooccurrence of collagenous colitis withseronegative spondyloarthropathy: report of a case and literaturereview. J Rheumatol, 1993;20(12):2153-2157.
24. Kenesi-Laurent M, Chapelon-Abric C, Fattah ZA, Naudin G,Godeau P. The first case of CRST syndrome associated with col-lagenous colitis. J Rheumatol, 1991;18(11):1765-1767.
25. Stuber E, Swensson O, Nitsche R, et al. Association of lympho-cytic colitis with linear IgA dermatosis. Z Gastroenterol,1999;37(6):519-523.
26. Zins BJ, Sandborn WJ, Tremaine WJ. Collagenous and lympho-cytic colitis: subject review and therapeutic alternatives. Am JGastroenterol, 1995;90(9):1394-1400.
27. Lagorce-Pages C, Fabiani B, Bouvier R, Scoazec JY, Durand L,Flejou JF. Collagenous gastritis: a report of six cases. Am J SurgPathol, 2001;25(9):1174-1179.
28. Chan JL, Tersmette AC, Offerhaus GJ, Gruber SB, Bayless TM,Giardiello FM. Cancer risk in collagenous colitis. Inflamm BowelDis, 1999;5(1):40-43.
29. Lee E, Schiller LR, Vendrell D, Santa Ana CA, Fordtran JS.Subepithelial collagen table thickness in colon specimens frompatients with microscopic colitis and collagenous colitis. Gas -troenterology, 1992;103(6):1790-1796.
30. Ulrich S, Wagner U, Wegmann W. [Tenascin: a simple tool in thediagnosis of collagenous colitis]. Schweiz Med Wochenschr,1999;129(38):1363-1367.
31. Gunther U, Schuppan D, Bauer M, et al. Fibrogenesis and fibrol-ysis in collagenous colitis. Patterns of procollagen types I and IV,matrix-metalloproteinase-1 and -13, and TIMP-1 gene expres-sion. Am J Pathol, 1999;155(2):493-503.
32. Muller S, Neureiter D, Stolte M, et al. Tenascin: a sensitive andspecific diagnostic marker of minimal collagenous colitis. Vir -chows Arch, 2001; 438(5): 435-441.
(continued from page 46)
(continued on page 51)

PRACTICAL GASTROENTEROLOGY • SEPTEMBER 2002 51
A SPECIAL ARTICLE
Microscopic Colitis
33. Riddell RH, Tanaka M, Mazzoleni G. Non-steroidal anti-inflam-matory drugs as a possible cause of collagenous colitis: a case-control study. Gut, 1992;33(5):683-686.
34. Wilcox GM, Mattia A. Collagenous colitis associated with lanso-prazole. J Clin Gastroenterol, 2002;34(2):164-166.
35. Duncan HD, Talbot IC, Silk DB. Collagenous colitis and cimeti-dine. Eur J Gastroenterol Hepatol, 1997;9(8):819-820.
36. Rosa I, Nahon S, Cohen C, et al. Ticlopidine-induced lympho-cytic colitis. Ann Med Interne (Paris), 1999;150(5):437-439.
37. Feurle GE, Bartz KO, Schmitt-Graff A. Lymphocytic colitis,induced by ticlopidine. Z Gastroenterol, 1999;37(11):1105-1108.
38. Berrebi D, Sautet A, Flejou JF, Dauge MC, Peuchmaur M, PotetF. Ticlopidine induced colitis: a histopathological study includingapoptosis. J Clin Pathol, 1998; 51(4):280-283.
39. Beaugerie L, Patey N, Brousse N. Ranitidine, diarrhoea, and lym-phocytic colitis. Gut, 1995;37(5):708-711.
40. Piche T, Raimondi V, Schneider S, Hebuterne X, Rampal P.Acarbose and lymphocytic colitis. Lancet, 2000;356(9237):1246.
41. Jarnerot G, Bohr J, Tysk C, Eriksson S. Faecal stream diversionin patients with collagenous colitis. Gut, 1996;38(1):154-155.
42. Rampton DS, Baithun SI. Is microscopic colitis due to bile-saltmalabsorption? Dis Colon Rectum, 1987;30(12):950-952.
43. Andersen T, Andersen JR, Tvede M, Franzmann MB. Collage-nous colitis: are bacterial cytotoxins responsible? Am J Gas -troenterol, 1993;88(3):375-377.
44. Scott BA, Prindiville TP, Sheikh RA, Tang-Feldman YJ, Silva JJ, Cohen SH. Bacteroides fragilis Enterotoxin Gene Sequences inPatients with Microscopic Colitis. Submitted for Publication.
45. Khan MA, Brunt EM, Longo WE, Presti ME. Persistent Clostrid-ium difficile colitis: a possible etiology for the development ofcollagenous colitis. Dig Dis Sci, 2000; 45(5):998-1001.
46. Makinen M, Niemela S, Lehtola J, Karttunen TJ. Collagenouscolitis and Yersinia enterocolitica infection. Dig Dis Sci,1998;43(6):1341-1346.
47. Perk G, Ackerman Z, Cohen P, Eliakim R. Lymphocytic colitis:a clue to an infectious trigger. Scand J Gastroenterol, 1999;34(1):110-112.
48. Narayani RI, Burton MP, Young GS. Resolution of collagenouscolitis after treatment for Helicobacter pylori. Am J Gastroen -terol, 2002;97(2):498-499.
49. Tremaine WJ. Collagenous colitis and lymphocytic colitis. J ClinGastroenterol, 2000;30(3):245-249.
50. Levy AM, Yamazaki K, Van Keulen VP, et al. Increasedeosinophil infiltration and degranulation in colonic tissue frompatients with collagenous colitis. Am J Gastroenterol,2001;96(5):1522-1528.
51. Taha Y, Carlson M, Thorn M, Loof L, Raab Y. Evidence of localeosinophil activation and altered mucosal permeability in col-lagenous colitis. Dig Dis Sci, 2001;46(4):888-897.
52. Baum CA, Bhatia P, Miner PB, Jr. Increased colonic mucosalmast cells associated with severe watery diarrhea and micro-scopic colitis. Dig Dis Sci, 1989;34(9):1462-1465.
53. Baert F, Schmit A, D’Haens G, et al. Budesonide in collagenouscolitis: a double-blind placebo-controlled trial with histologic fol-low-up. Gastroenterology, 2002;122(1):20-25.
54. Fine KD, Lee EL. Efficacy of open-label bismuth subsalicylatefor the treatment of microscopic colitis. G a s t r o e n t e r o l o g y,1998;114(1):29-36.
55. Goff JS, Barnett JL, Pelke T, Appelman HD. Collagenous colitis:histopathology and clinical course. Am J Gastroenterol,1997;92(1):57-60.
56. Scheidler MD, Meiselman M. Use of verapamil for the sympto-matic treatment of microscopic colitis. J Clin Gastroenterol,2001;32(4):351-352.
57. Amaro R, Poniecka A, Rogers AI. Collagenous colitis treatedsuccessfully with bismuth subsalicylate. Dig Dis Sci,2000;45(7):1447-1450.
58. Fiedler LM, George J, Sachar DB, Kornbluth AA, Janowitz HD,Harpaz N. Treatment responses in collagenous colitis. Am J Gas -troenterol, 2001;96(3):818-821.
59. Fasoli R, Jewell DP. Response to treatment of microscopic coli-tis. Ital J Gastroenterol, 1994;26(5):229-232.
60. Bhullar DS, Tymms KE, Hillman L, Jain S. Treatment of col-lagenous colitis with methotrexate. Aust N Z J Med, 1996;26(1):114.
61. Vennamaneni SR, Bonner GF. Use of azathioprine or 6-mercap-topurine for treatment of steroid- dependent lymphocytic and col-lagenous colitis. Am J Gastroenterol, 2001;96(9):2798-2799.
62. Ben Soussan E, Savoye G, Lemoine F, Ducastelle P, Colin R.Azathioprine as a treatment of refractory lymphocytic colitis. EurJ Gastroenterol Hepatol, 2001;13(4):457-458.
63. Pardi DS, Loftus EV, Jr., Tremaine WJ, Sandborn WJ. Treatmentof refractory microscopic colitis with azathioprine and 6-mercap-topurine. Gastroenterology, 2001;120(6):1483-1484.
(continued from page 48)
Practical Gastroenterology invites its readers to share theirPEARLS OF GASTROENTEROLOGY
Submissions should be brief (about 200 words maximum). Those accepted for publication maybe edited for space and style. An honorarium of $25 will be paid upon publication.
Mail your “Pearls of Gastroenterology” to Practical Gastroenterology9 9 B Main Street, Westhampton Beach, NY 11978
or fax them to us at (631) 288-4435.
Please include your name, address, affiliations, and telephone and fax numbers.





























