Embed Size (px)
Citation preview
SOMATOFORM DISORDERS
Intended Learning Outcomes (ILOs)
1. Knowledge and understanding
1.1 List common characteristics of somatoform
disorders.
1.2 Identify various types of somatoform disorders.
3- Professional and practical Skills.
3.1 Apply nursing care plan for patient with
somatoform disorders.
4- General and transferable skills.
4.1 Develop the ability to perceive the clients’
symptoms as a real to him.
2- Intellectual Skills.
2.2 Analyze etiological factors contributing to
somatoform disorders.
2.3 Evaluate assessment data to formulate an
appropriate nursing diagnoses for patient with
somatoform disorders.
Somatoform disorders
• Somatoform disorders
_ A broad group of illnesses that have bodily signs
and symptoms as a major component. Pathological
concern of individuals with the appearance or
functioning of their bodies when there is no known
medical condition causing the physical complaints.
Common characteristics of somatoform disorders
• The symptoms are not intentionally produced
or feigned. In most disorders, the client is
worried about the symptom and excessively
seeks medical assistance. (Dr shopping )
Common characteristics of somatoform disorders
• The somatic symptoms & complaints cause
impairment in patient’s ability to function in
social & occupational roles.
• The purpose of the symptom is anxiety relief.

Classifications of somatoform disorders
1. Somatization disorder
2. Conversion disorder
3. Pain disorder
4. Hypochondriasis
5. Body Dysmorphic Disorder
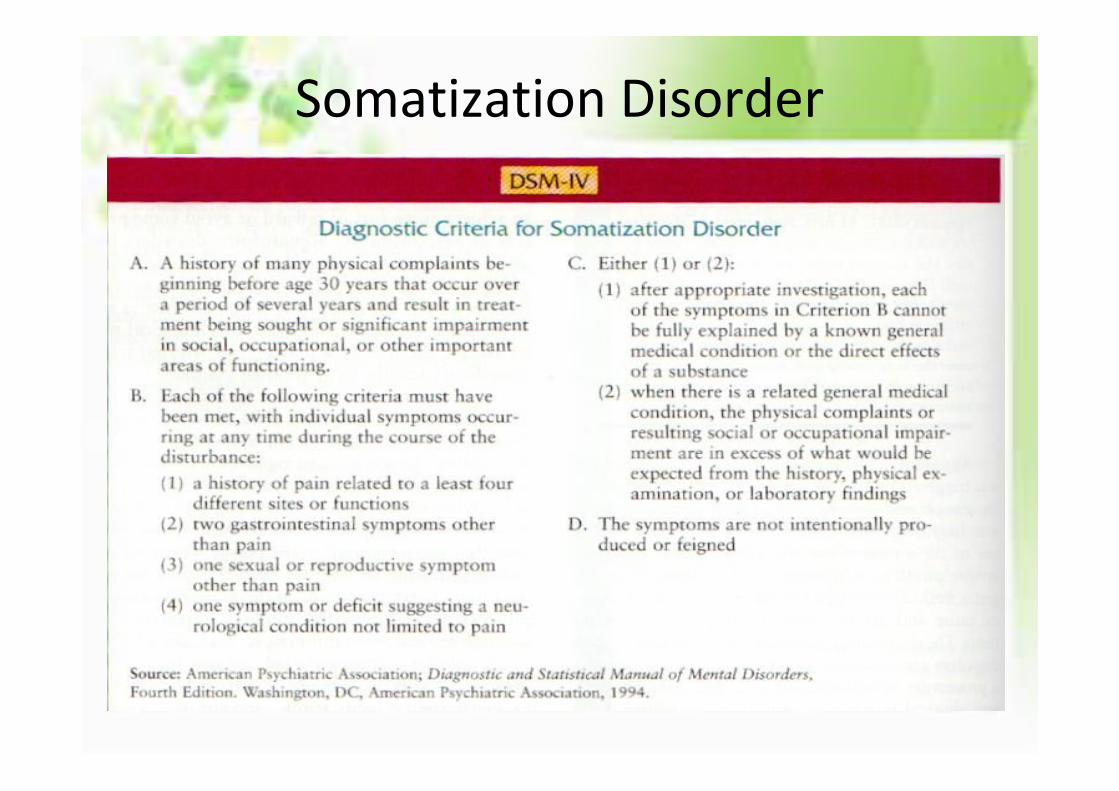
Somatization disorder
Known as Briquet’s syndrome (100 years ago) It’s
characterized by multiple physical symptoms for
which medical attention is sought but which
have no apparent physical cause.
Con’t . Somatoform Disorders• Multiple recurrent physical complaints over many
years• (combination of pain, problems in gastrointestinal
,nervous system, and reproductive system ).– Begins before age 30.
– Chronic pattern.
– Higher prevalence for women than men. women (5-20 times more common)
• Somatization Disorder occurs more often with people of low income and little education
• WHAT ARE THE 3 MAIN DISTINCTIONS FOR SOMATIZATION DISORDER?
• 1) they are not faking their symptoms2) their complaints are vague and generalized3) there is no physical cause for their pain
• Example on CN symptoms or pseudo neurological : impaired
coordination or balance, paralysis or localized weakness,
difficulty swallowing, aphonia, urinary retention,
hallucinations, loss of touch or pain sensation, double vision,
amnesia, sensory losses, loss of consciousness.
Somatization Disorder
Conversion disorderConversion refers to unconscious
conflicts being converted into physical
symptoms .It involves unexplained
usually sudden, deficits in sensory
and/or motor function that suggest a
neurological disorder but are
associated with psychological factors.Freud
• Common symptoms: blindness, paralysis, mutism, or seizures.
• la belle indifference often accompanies Conversion disorder.It means Isolation of affect: where reality is accepted but without the expected human emotional response to that reality.
• How do you distinguish between Somatization Disorder and Conversion Disorder?
• Somatization Disorder: is often polysymptomatic, the age of onset is under 30, F>M, prognosis is poor to fair
Conversion Disorder: Acute and generally transient, monosymptomatic, onset 10-35 yrs, F>M, prognosis excellent
• Men with conversion disorder frequently served in the military
Pain disorder
The primary symptom of pain disorder is the
presence of pain in one or more sites that can
not be explained by medical or neurological
tests. e. g low back pain, headache, facial pain &
chronic pelvic pain.

Pain Symptoms
• Pain Symptoms: (4 or more experienced) pain in head, abdomen, back and joint
• Can also feel uncomfortable pain in the rectum.
• Abnormalities in menstruation, urination and sexual intercourse.
• Acute pain disorder <6 months
Chronic pain disorder >6 months
• the most type of pain seen in chronic pain
disorder?
• burning pain
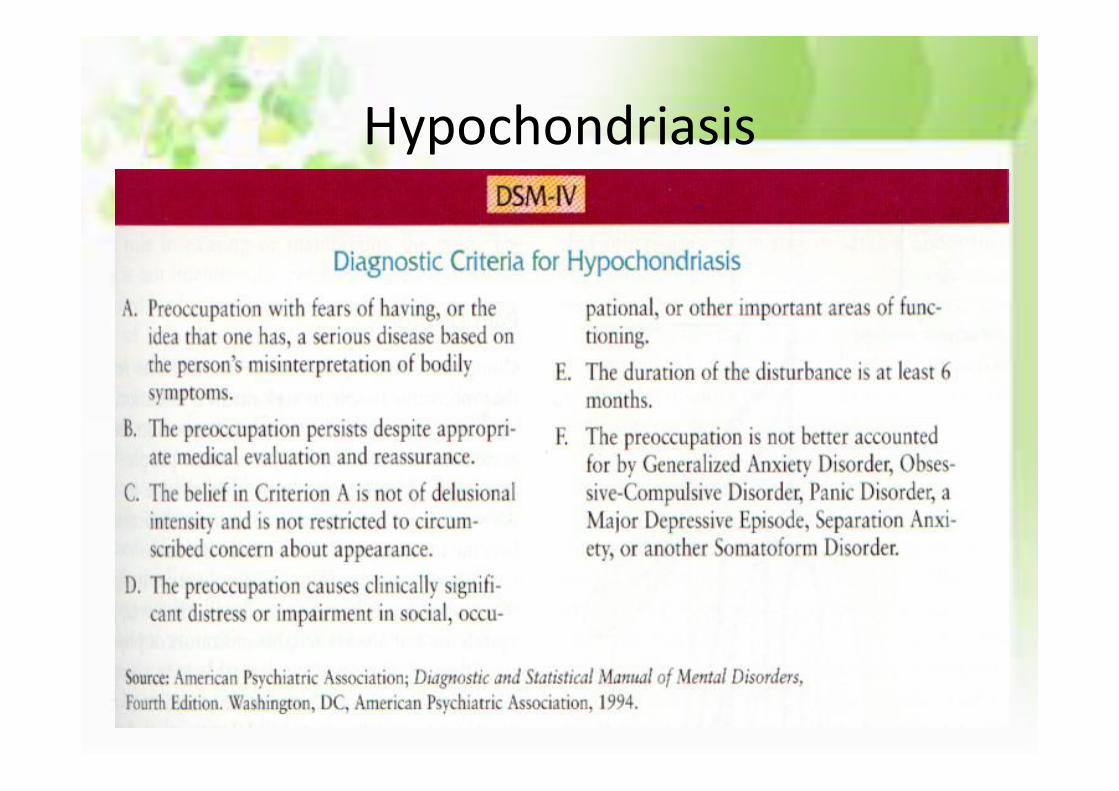
Hypochondriasis
Is the preoccupation with the fear that one has
or will get a serious disease based on the
person’s misinterpretation of bodily symptoms.
The preoccupation persist despite absence of
pathophysiological findings of medical and
neurological examination.
• it is equally as common in men and women.
• In hyperchondriasis there is no correlation to
social status/income.
• Prognosis is generally good, but symptoms
wax and wane over time.
How do you tell the difference between hypochondriasis and somatization disorder?
• In somatization disorder, patient is concerned about their symptoms but does not overreact to having those symptoms
In hypochondriasis, patient is super concerned about their symptoms and overreacts to having those symptoms
Also for hypochondriasis, there is no specific age of onset M=F
For somatization disorder, the age of onset is under 30. F>M
• Medical students frequently think they have
symptoms of disease/s they are studying. It
may be a type of hypochondriasis or it could
simply be nosophobia (fear of contracting a
disease)
Hypochondriasis
Body Dysmorphic Disorder
Is the preoccupation with some imagined defect
in their physical appearance. The preoccupation
is out of proportion to any actual abnormalities
• Body dysmorphic disorder is often associated with Eating disorders (e.g. anorexia nervosa)
• Sufferers of this disorder complain of several specific features or a single feature, or a vague feature or general appearance.
• 75% percent of patients with this disorder complain about their skin.
• suicidal rate in body dysmorphic disorder is higher
• What disorder is a form of body dysmorphicdisorder where males feel like they are 'puny' and thus work out excessively but they are never big enough?
• Bigorexia also known as muscle dysmorphia or the Adonis complex
Factitious Disorders
• Characterized by:– Physical or psychological symptoms that are
intentionally produced or feigned in order to assume the sick role.
– Conscious fabrication of symptoms to gain attention.
• The presence of factitious symptoms does not preclude the coexistence of true physical or psychological symptoms.
• Munchausen’s by proxy, occurs when a person inflicts illness or injury on someone else to gain the attention of emergency medical personnel or to be a “hero” for saving the victim. An example would be a nurse who gives excess intravenous potassium to a client and then “saves his life” by performing CPR.

Malingering
• Intentionally feigning or grossly exaggerating
illness or disability to derive benefit or
secondary gain (e.g., to escape work, gain
compensation, or obtain drugs)
Factitious Disorder vs. Malingering
• Factitious Disorder– May agree to
unnecessary surgery and interventions
– Motivated by psychological needs (attention, security, etc)
• Malingering– Will not agree to
unnecessary surgery/intervention
– Motivated by secondary gains (avoid work/stay on disability)
– More common in military populations and legal settings
Etiology of Somatization• Neurobiological
• Somatization results from defective or deficient neurobiological processing of sensory and emotional information.
• These disorders encompass mind and body interactions in which the brain, sends various signals that impinge on the patient's awareness, indicating a serious problem in the body.
• Additionally, minor or as yet undetectable
changes in neurochemistry, and
neurophysiology, may result from unknown
mental or brain mechanisms that cause illness
• Psychodynamic
– Somatized physiological sensations occur as
expressions of underlying emotional conflict.
– Somatization enables patients to meet latent
needs for nurturing and support.
Mechanisms of Somatization
• Behavioral
– Somatization is viewed as behavior that is
brought about and reinforced by others in the
patient’s environment
– “Illness-maintenance systems”
Mechanisms of Somatization
• Sociocultural– Social norms concerning emotions. – When a culture does not allow direct
communication of emotional content, one means available to express emotions is through physical symptoms
– Somatization serves to notify others of emotional or psychological distress in an acceptable or non-stigmatized manner.

Contributing Factors for Somatization
• Childhood abuse • Acute stress• Societal roles• Learned behavior • Secondary gain• Cultural factors • Histrionic, narcissistic, and borderline
personality traits
Assessment
It is helpful for nurses to assess for:
• Presence of secondary gains.
• Cognitive style.
• Ability to communicate emotional needs.
• Dependence on medication.
Assessing secondary gains• Getting out usual responsibilities .
• Getting extra attention .
• Manipulating others in the environment.
• Fulfillment of dependency needs.
• Financial gain from insurance, worker’s
compensation, or sick benefits.
Nursing diagnosis
Ineffective individual coping may be related to
• Repressed anxiety.
• Unmet dependency needs.
• Psychological conflicts/stressors.
• Ineffective use of adaptive coping strategies.
Evidence by•Verbalization of physical complaints in the absence
of any pathophysiological evidence.
•Total focus on the self and physical symptoms.
•Verbalizes continued need to seek medical
assistance for perceived physical symptoms inspite
of physician’s reassurance of no demonstrable
organic pathology “doctor shopping”.
Evidence by
•Denies correlation between physical symptoms
and psychological conflicts/stressors.
•Demonstrate excessive dramatic or exaggerated
behavior when describing perceived physical signs
and symptoms.
Goal
•Patient will demonstrate adaptive coping
mechanism with anxiety without resorting to
physical symptoms.
Other possible nursing diagnosis
1. Impaired social interaction
2. Ineffective family coping
3. Self-esteem disturbance
Nurses’ reactions and feelings•At the first Nurses and other health care workers
often find working with clients with somatoform
disorders difficult and unsatisfying.
•It is helpful to remember that the symptom the
client is experiencing is very real to him or her, even
though the objective data do not prove physiologic
basis.
NURSING MANAGEMENT
SOMATIZATION DISORDER• Nursing diagnosis• Ineffective coping related to repressed anxiety and unmet
dependency needs• Nursing interventions• Recognize and accept that the physical complaint is real to
the client, even though no organic aetiology can be identified• Identify the gains that the physical symptoms are providing
for the patient.• Initially fulfill the client’s urgent dependency needs but
gradually withdraw attention to physical symptoms.
• Minimize time given in response to physical complaints.
• Encourage client to verbalize fears and anxieties.
• Discuss possible alternative coping strategies client may use in response to stress.
• Help client identify ways to achieve recognition from others without restoring to physical complaints
Chronic pain
• Recognize and accept that the pain is real to the individual, even though no organic cause can be identified. Denying the client’s feelings is non therapeutic and hinders the development of a trusting relationship.
• Observe and record the duration and intensity of the pain. Note factors that precipitate the onset of pain. Identification of the precipitating stressor is important for assessment purposes. This information will be used to develop a plan for assisting the client to cope more adaptively.
• Provide pain medication as prescribed by physician. Client comfort and safety are nursing priorities.
• Assist with comfort measures, such as back rub, warm bath, and heating pad. Be careful, however, not to respond in a way that reinforces the behavior. Secondary gains from physical symptoms may prolong maladaptive behaviors.
• Offer attention at times when client is not focusing on pain. Positive reinforcement encourages repetition of adaptive behaviors.
• Identify activities that serve to distract client from focus on self and pain. These distractors serve in a therapeutic manner as a transition from focus on self or physical manifestations tofocus on unresolved psychological issues.
• Encourage verbalization of feelings. Explore meaning that pain holds for client. Help client connect symptoms of pain to times of increased anxiety and to identify specific situations that cause anxiety to rise. Verbalization of feelings in a nonthreatening environment facilitates expression and resolution of disturbing emotional issues.
disturbed body image
Nursing diagnosis• Confusion in mental picture of one’s physical self.
related to low self-esteem unmet dependency needs.
• Interventions• If there is actual change in structure or function,
encourage client to progress through stages of grieving. Assess level of knowledge and provide information regarding normal grieving process and associated feelings. Knowledge of acceptable feelings facilitates progression through the grieving process.
• Identify misperceptions or distortions client has regarding body image. Correct inaccurate perceptions in a matter-of-fact, nonthreatening manner. Withdraw attention when preoccupation with distorted image persists. Lack of attention may encourage elimination of undesirable behaviors.
• Help client recognize personal body boundaries. Use of touch may help him or her recognize acceptance of the individual by others and reduce fear of rejection because of changes in bodily structure or function.
• Encourage independent self-care activities, providing assistance as required. Self-care activities accomplished independently enhance self-esteem and also create the necessity for client to confront reality of his or her bodily condition.
• Provide positive reinforcement for client’s expressions of realistic bodily perceptions. Positive reinforcement enhances self-esteem and encourages repetition of desired behaviors.

Thanks for helping in our course . I appreciated yourcommitment . I hope for all satisfaction & success.
My door open to you at any time..
It’s the end but not the last I am willing to listen for you at any time