Embed Size (px)
Citation preview

1
MIDFACE TRAUMA
❖ well equipped to withstand forces directed superiorly or inferiorly
❖ poorly withstands lateral and frontal forces
❖ midface absorbs, conducts and effectively dissipates forces
❖ horizontal and vertical buttresses resist/transmit forces to base of skull
MIDFACE TRAUMAVertical Buttresses
❖zygomatico-maxillary
❖pterygomaxillary
❖nasomaxillary
MIDFACE TRAUMAHorizontal Buttresses
❖ Pyriform Aperture
❖ Maxillary Alveolus and Palate
❖ Orbital Rims
❖ Base of skull
MIDFACE TRAUMA
❖ Le Fort I, II & III
❖ NOE
❖ ZMC
❖ isolated maxillary, zygomatic, nasal

2
EMERGENCY TREATMENT
Airway/Breathing
❖ airway evaluation
❖ supraglottic obstruction due to secretions &/or debris
❖ intraoral wounds managed locally
❖ ET tube for severe bleeding
❖ C-spine fx must be ruled out or stabilized prior to ET tube placement
EMERGENCY TREATMENT
Tracheotomy vs ET tube
❖ upper airway obstruction w/ c-spine fx perform trach or cricothyroidotomy
❖ avoid c-spine manipulation and movement with ET tube
❖ laryngeal fx is indication for trach
❖ reconstructive procedure hampered by ET tube
EMERGENCY TREATMENT
Circulation
❖ blood volume: vitals, central subclavian catheter
❖ NS or LR through 2 large bore IV lines
❖ vascularity of region may result in severe hypovolemia
❖ typed/crossmatched blood
❖ ateriogram/esophagram

3
MIDFACE TRAUMA
Sensory Innervation
❖ 1st & 2nd divisions of trigeminal nerve
❖ V2 emerges from infraorbital foramen
❖ supplies lateral nasal, inferior palpebral, & superior labial regions
Classification of Le Fort Fractures
❖ Le Fort I- force delivered above level of teeth
❖ Le Fort II- force delivered at level of nasal bones
❖ Le Fort III- force delivered at orbital level resulting in craniofacial dysjunction
Classification of Le Fort Fractures
Classification of Le Fort Fractures
4
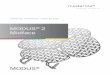
Le Fort I Fracture
❖ lateral border of pyriform sinus across lateral antral wall
❖ behind maxillary tuberosity
❖ across pterygoid jct
❖ concomitant nasal septum fx may be present
❖ unilateral fx may occur coursing through palatal suture line
5
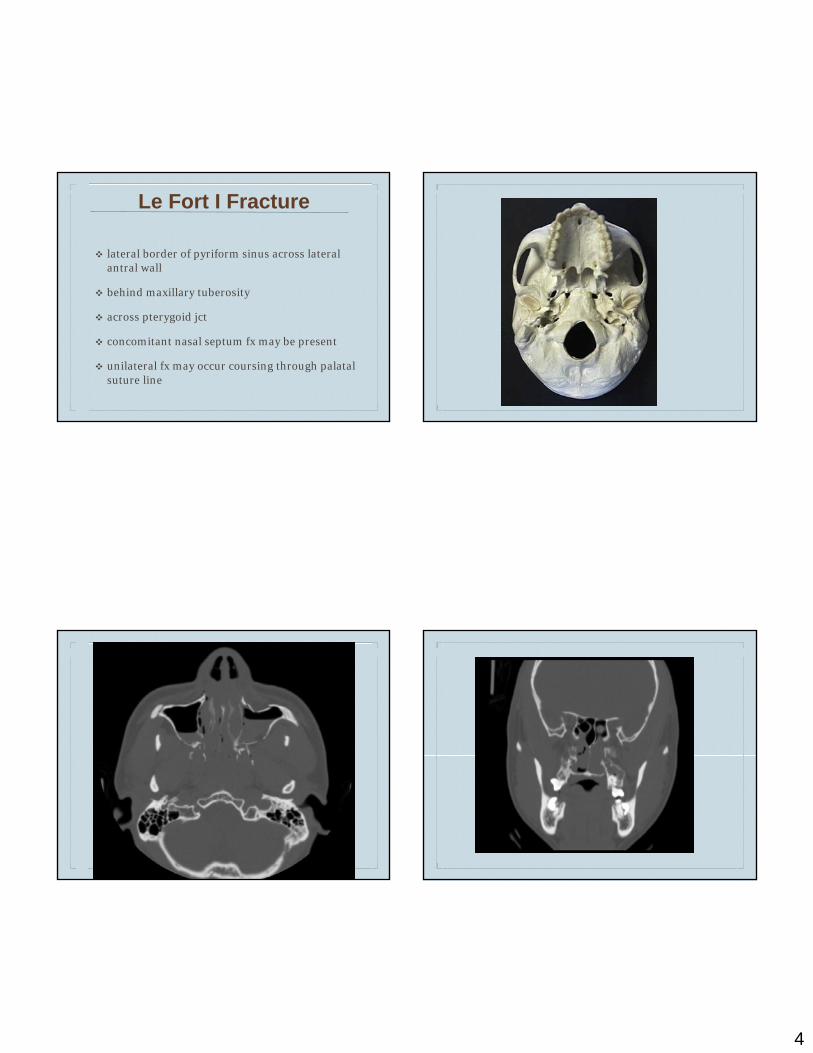
Le Fort I Fractures
Muscular Attachments
❖ medial pterygoid
❖ lateral pterygoid
❖ post/inf pull seen in fx of maxilla
❖ palatal ecchymosis from unilateral fracture
❖ posterior, inferior displacement creating a classic open bite
❖ segment can be impacted, immoveable, free floating
❖ displacement of fractured fragment
❖ CN V injury (infraorbital branch)
❖ movement of maxilla in AP direction with no movement of midface
Le Fort I FracturesPhysical Exam Findings
Le Fort I FracturesFracture Management
❖ minimally displaced fx
❖ early MMF
❖ 4-6 weeks of immobilization
❖ open reduction with plating
Le Fort I Fractures
Fracture Management
❖ significant displacement or impaction
❖ disimpaction forceps
❖ maxilla pulled forward and down
❖ rigid fixation with miniplates
❖ skeletal suspension with circumzygomatic wiring
❖ external fixation
6
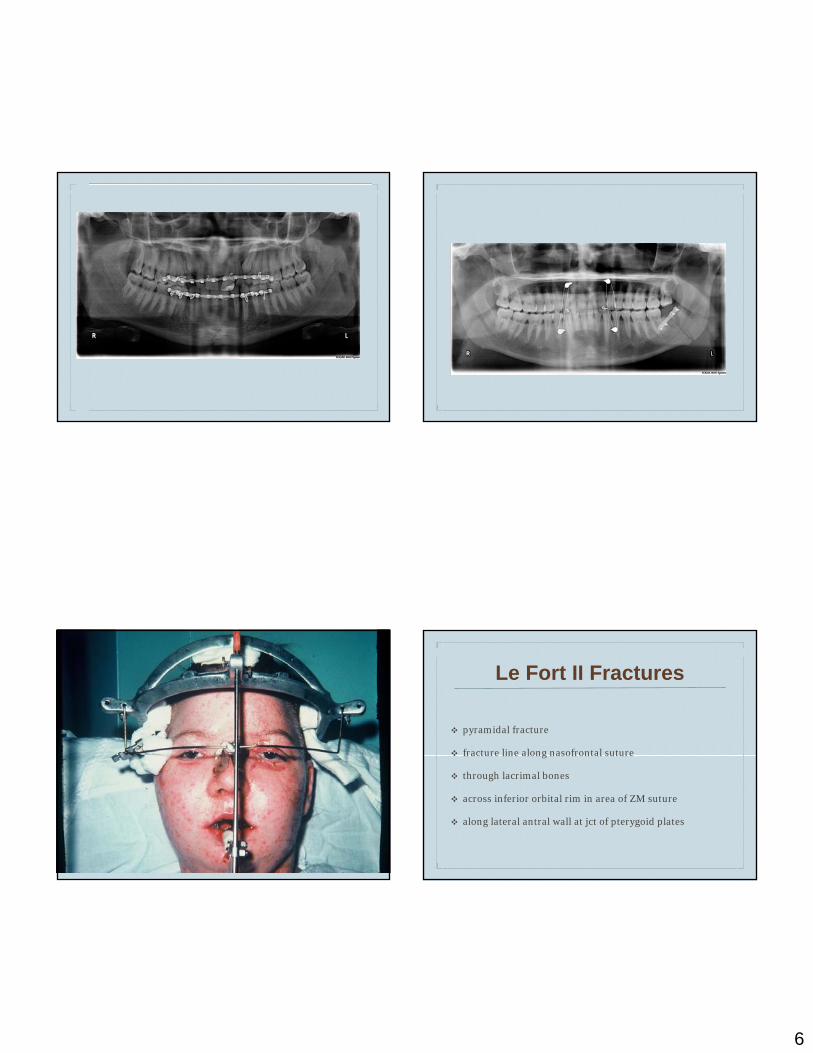
Le Fort II Fractures
❖ pyramidal fracture
❖ fracture line along nasofrontal suture
❖ through lacrimal bones
❖ across inferior orbital rim in area of ZM suture
❖ along lateral antral wall at jct of pterygoid plates
7
Le Fort II FracturesPhysical Exam Findings❖ bilateral periorbital edema and eccymosis; “raccoon sign”
❖ CN V injury (infraorbital nerve)
❖ malocclusion, open bite
❖ step deformity of infraorbital rim region or nasofrontal suture region
❖ mobility of fractured complex by grasping the mx anterior teeth and moving complex AP
❖ orbital blowout fx
❖ epistaxis
Le Fort II FracturesPhysical Exam Findings
❖ CSF rhinorrhea due to dural tear lateral to cribriform plate
❖ disruption of sphenoid, ethmoid, and frontal sinuses
❖ leakage generally noted immediately following trauma
❖ diagnosis of CSF is difficult if mixed with blood
❖ must be distinguished from nasal secretions & lacrimal secretions
❖ Glucose level of 45mg/dL
❖ will not stiffen handkerchief or guaze
❖ forms characteristic concentric rings
❖ pt may report “salty taste”
❖ high resolution CT cisternogram w/ intrathecal florescein
❖ beta-2-transferrin
Le Fort II FracturesPhysical Exam Findings
Le Fort II FracturesConsiderations within ER setting
❖ semirecumbent position
❖ no nose blowing, no straining, sneezing with mouth open
❖ abx therapy to counter development of meningitis

8
Le Fort II FractureTREATMENT
❖ IMF x 4-6 weeks
❖ disimpaction forceps
❖ orbital floor exploration and release of entraped muscle
❖ rigid fixation across nasofrontal sutures, zygomaticomaxillary sutures, or inferior orbital rims
❖ fx courses through ZT and ZF sutures
❖ along lateral orbital wall
❖ through inferior orbital fissure
❖ medially through nasofrontal suture
❖ ending at pterygomaxillary fissure
Le Fort III Fractures

9
Le Fort III Fracture
Physical Exam Findings
❖ mobility of zygomaticomaxillary complex
❖ CSF leakage
❖ periorbital edema and ecchymosis
❖ traumatic telecanthus
❖ epiphora
❖ epistaxis
Le Fort III Fracture
Treatment❖ establish outer framework
❖ immobilization of ZF, ZT and NF sutures
❖ if mand or mx involved 1st establish proper occlusion
❖ bicoronal, infraorbital, lateral brow &/or nasofrontal incision
❖ expose nasoethmoid complex, lateral rims and zygomatic arch

10
Zygomaticomaxillary Complex (ZMC)Fractures
❖ 2nd most common facial fx after nasal
❖ high incidence due to prominent position within facial skeleton
❖ male predilection 4:1
❖ 2nd and 3rd decades of life
❖ altercations & MVA
❖ greater incidence of left sided injury
❖ b/l fx most commonly result of MVA
❖ zygoma is major buttress of the facial skeleton
❖ important role in facial contour
❖ quadrilateral in shape (4 sided pyramid)
❖ articulates with 4 bones
❖ fx can result in ocular and mandibular functional impairment
❖ origin to masseter muscle & attachment to temporalis fascia, temporal and zygomatic muscles
Zygomaticomaxillary Complex (ZMC)Fractures
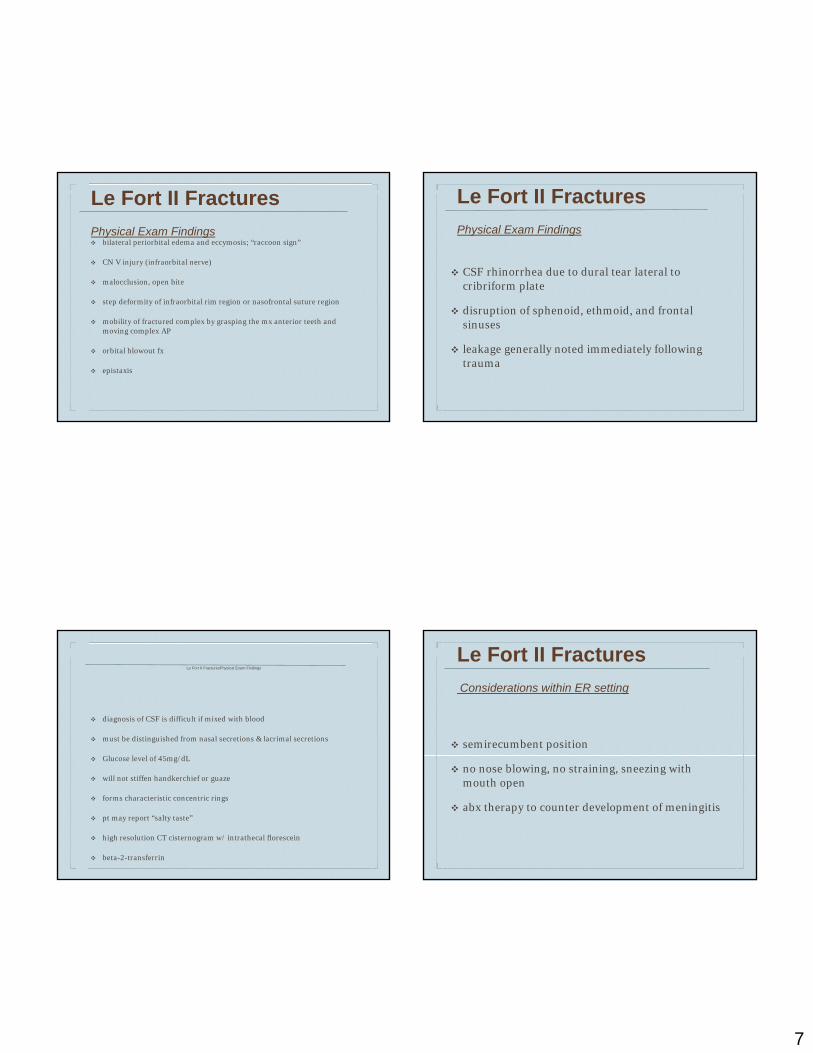
ZMC FracturesPhysical Exam Findings
❖ periorbital edema & ecchymosis
❖ flattening of malar prominence
❖ ecchymosis of maxillary buccal sulcus
❖ trismus-impinging coronoid
❖ infraorbital nerve deficit
❖ epistaxis
11
ZMC FracturesOcular Exam Findings
❖ subconjuctival ecchymosis
❖ crepitation from air emphysema
❖ displacement of palpebral fissure
❖ antimongoloid slant to eye
❖ unequal pupillary levels
❖ diplopia
❖ muscle entrapment & enophthalmus
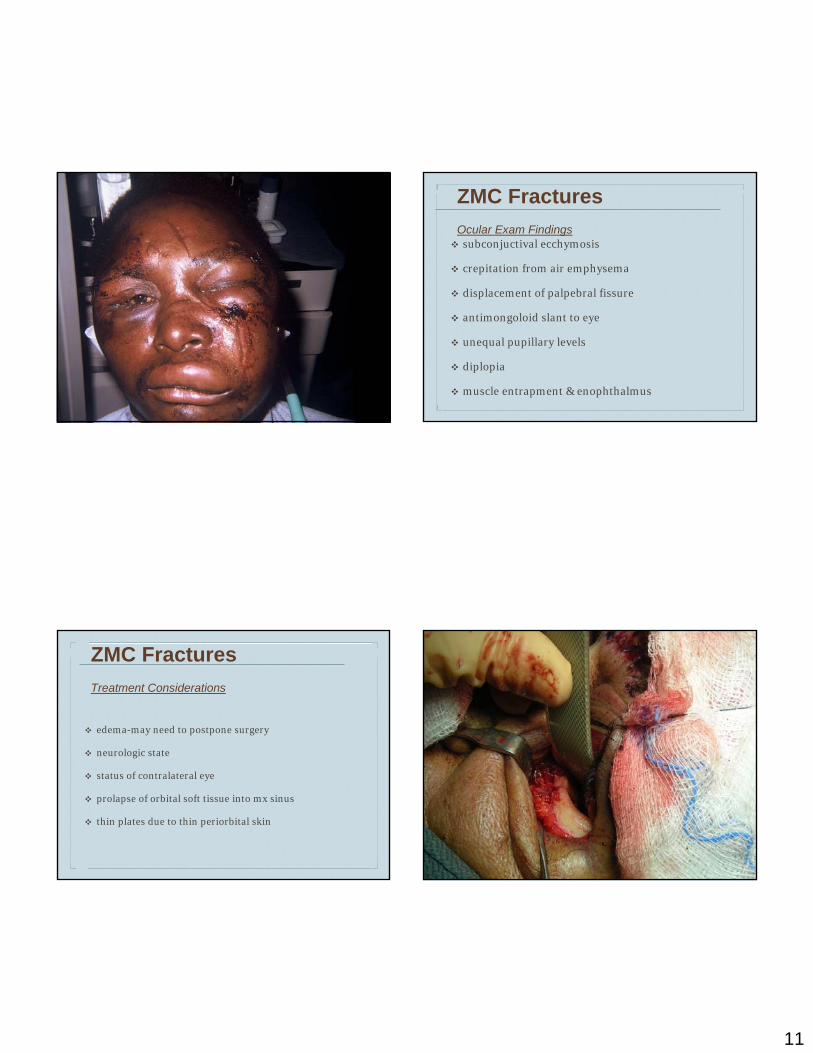
ZMC FracturesTreatment Considerations
❖ edema-may need to postpone surgery
❖ neurologic state
❖ status of contralateral eye
❖ prolapse of orbital soft tissue into mx sinus
❖ thin plates due to thin periorbital skin

12
Naso-Orbital-Ethmoid Fracture
Physical Exam Findings❖ fractured nose
❖ widened nasal bridge
❖ epistaxis
❖ periorbital edema and ecchymosis
❖ disruption of lateral canthal ligament
❖ traumatic telecanthus
❖ damage to lacrimal apparatus (20% of pt’s)
❖ epiphora
Naso-Orbital-Ethmoid Fracture
Physical Exam Findings
❖ average intercanthal distance: 33-34mm (males), 32-34mm (females)
❖ intercanthal distance > 35mm are suggestive of NOE fx
❖ distances >40mm are generally diagnostic
❖ intercanthal distance roughly 1/2 the interpupillary distance
❖ crepitus/movement of medial orbital rim indicates instability
Naso-Orbital-Ethmoid Fracture
Markowitz & Manson Classification System
❖ Class I: canthal ligament attached to large fragement/no comminution
❖ Class II: canthal ligament attached to substantial fragment of bone despite some comminution
❖ Class III: detachment of canthal ligament, severe comminution, ligament attached to very small fragment of bone
13
Naso-Orbital-Ethmoid Fracture
Treatment
❖ adequate exposure
❖ coronal flap with lower eyelid incisions
❖ existing lacerations
❖ medial canthal tendon injury may require canthopexy with transnasal wiring
❖ ORIF of nasal bones to frontal bone & inferior & medial orbtial rims
❖ nasal dorsum bone grafting
Naso-Orbital-Ethmoid Fracture
Nasolacrimal Injury
❖ loss of protection provided by medial canthal ligament
❖ ORIF of fx segments to reestablish lacrimal drainage
❖ stent (Crawford tube) to bridge two severed ends & closure of pericannular tissue
❖ dacrocystography
❖ uncorrected epiphora may require dacrocystorhinostomy
Naso-Orbital-Ethmoid Fracture
Dacrocystorhynostomy
❖ incision midway between corner of eye and bridge of nose
❖ lacrimal sac located and connected to nasal mucosa
❖ new tear drainage pathway
❖ stent placed to prevent scarring
Complications of Midface Trauma
❖ CSF otorrhea & rhinorrhea
❖ Damage to Lacrimal System
❖ Ocular
❖ Neurologic

14
Ocular Complications of Midface Trauma
❖ Diplopia
❖ Enophthalmos
❖ Retrobulbar Hematoma
❖ Superior Orbital Fissure Syndrome
❖ Orbital Apex Syndrome
❖ Blindness
Traumatic Diplopia❖ most frequent complication
❖ usually temporary but may become permanent if not treated
❖ must distinguish between neurologic damage and muscle entrapment & edema
❖ forced duction test
❖ limitation of motion may indicate entrapment
❖ absence of resistance may indicate neurologic deficit
Traumatic DiplopiaCauses
❖ interference with function of EOM
❖ displaced globe
❖ muscle or fat entrapment
❖ bony displacement (orbital floor)
❖ displacement of Lockwood’s inferior suspensory ligament
❖ impingement of CN III, IV, VI
Traumatic DiplopiaTreatment
❖ large defects
❖ displaced zygoma
❖ orbital floor defect with damage to Lockwood’s ligament
❖ inferior repositioning of globe
❖ trap door injury with physical restriction of movement
15
Traumatic DiplopiaTreatment
❖ edema
❖ steroids for 5-7 days
❖ determine if diplopia secondary to edema or entrapment
❖ CT scan with 3mm cuts
❖ result of forced duction test
Traumatic DiplopiaTreatment Objectives
❖ prevent loss of orbital contents
❖ provide support for orbital contents
❖ reconstruct floor to mirror opposite side
❖ retrieve herniated fat in trap door injury
Traumatic DiplopiaMonocular Diplopia
❖ detached lens
❖ hyphema
❖ traumatic globe injury
Enophlalmos❖ loss/atrophy of orbital fat
❖ enlargement of bony orbit
❖ cicatricial contraction of retrobulbar tissue
❖ unrepaired fracture of orbital wall
❖ displacement of orbital tissue
❖ increased orbital volume, decrease orbital contents, disruption of ligamentous structures

16
EnophlalmosTreatment
❖ ORIF orbital fx
❖ repair orbital floor and restoration of orbital contents
❖ freeing of soft tissue from herniated positions
❖ repair of zygoma fx
Retrobulbar Hematoma
❖ compromise optic nerve function
❖ central retinal artery obstruction
❖ infraorbital arterial rupture
❖ anterior/posterior ethmoid arterial rupture
Retrobulbar Hematoma
Subjective/Objective Findings
❖ severe aching pain
❖ progressive loss of vision
❖ proptosis
❖ increased IOP (normal:12-20mm Hg)
❖ subconjunctival hemorrhage
❖ gross eyelid swelling
❖ fixed, dilated pupil
Retrobulbar HematomaTreatment
❖ post-surgical wound opening
❖ IV injection of acetazolamide to decrease IOP (up to 500mg)
❖ lateral canthotomy
17
Superior Orbital Fissure Syndrome
❖ direct compression or hematoma on contents of superior orbital fissure
❖ pupillary dilation due to altered CN III function
❖ unopposed sympathetic control
❖ paresis of CN III, IV, VI resulting in ophthalmoplegia
❖ ptosis from paresis of levator palpebrae superiorus
❖ neurosensory disturbance CN V (frontal branch causing loss of sensation over forehead)
❖ deficit of supraorbital/supratrochlear nerves
❖ loss of corneal reflex (nasociliary branch of CN V)
❖ proptosis from engorgement of ophthalmic vein and lymphatics
Orbital Apex Syndrome
❖ superior orbital fissure syndrome
❖ optic nerve involvement
❖ change in visual acuity
Blindness
❖ 0.03-2.1%
❖ retrobulbar hemorrhage
❖ occlusion of ciliary arteries
❖ ischemia leads to optic neuropathy
❖ prompt diagnosis and treatment
❖ rapid evacuation of hematoma
BlindnessImmediate Reduction in IOP
❖20% mannitol (2g/kg IV, max 12.5g in 3-4min)
❖Acetazolamide sodium (Diamox) 500mg IV
❖Methylprednisolone sodium succinate (Solu-Medrol) 1g IV
18
Bibliography❖ Fonseca R et al, Oral & Maxillofacial Trauma. Vol I &II,
2005
❖ Bagheri S, Jo C, Clinical Review of Oral & Maxillofacial Surgery. 2008
❖ Zacharides et al, The Superior Orbital Fissure Syndrome. J Maxillofacial Surg: 125-8, 1985
❖ Zacharides et al, Orbital Apex Syndrome. Int J Oral & Maxillofacial Surg: 352-4, 1987
❖ Markowitz BL, Manson PN, Sargent L, et al: Management of the Medial Canthal Tendon in NOE Fractures; the Importance of the Central Fragement in Classification & Treatment. Plast Reconstr Surg: 843, 1991
Bibliography❖ Manson P et al, Structural Pillars of the Facial Skeleton,
An approach to the Management of Le Fort Fractures. Plastic & Reconstructive Surgery: 57, 1980
❖ Manolidis S, Management of Frontal Sinus Trauma. Seminars in Plastic Surgery: 261-271, 2002
❖ Assael LA, Atlas of Facial Fractures. OMS Clinics of N.America:Vol 11, 320-1, 1999
❖ Osguthorpe JD, Hoang G, Nasolacrimal Injuries,Evaluation & Management. Otolaryngologic Clinics of N. America: 59-78, 1991
The End