-
TECHNICAL NOTE
Miethke DualSwitch Valve in lumboperitoneal shunts
Suhas Udayakumaran & Jonathan Roth & Anat Kesler
&Shlomi Constantini
Received: 4 May 2010 /Accepted: 17 June 2010 /Published online:
4 July 2010# Springer-Verlag 2010
AbstractIntroduction Despite the existence of wide variety of
shuntsystems, physiological regulation of intracranial pressure
inshunted patients remains a utopian dream. Lumboperitonealshunts
(LPS) have long been used for treating idiopathicintracranial
hypertension and other types of communicat-ing hydrocephalus.
Although they can provide rapid andeffective symptom resolution,
cerebrospinal fluid (CSF)over-drainage remains a common
complication of LPS. Weintroduce the use of the Miethke DualSwitch
Valve (M-DSV) for LPS and describe our preliminary experiencewith
these valves in managing and avoiding CSF over-drainage. This is
the first description of the use of M-DSVfor LPS.Materials and
methods Over 6 months, we treated fivepatients with LPS using
M-DSV. Prior to the use of the M-DSV, four patients experienced
significant over-drainagesymptoms secondary to LPS. Data was
collected prospec-tively, including preoperative details and
clinical outcome.Results Five patients (age range, 22 to 71 years)
wereoperated upon. Three patients had pseudotumor cerebri,
onepatient had an LPS for treatment of a posterior fossa
pseudomeningocele, and one had an LPS for treatment ofcauda
equina syndrome secondary to lumbar dural ectasia.Four patients had
a history of clinical over-drainagesecondary to pre-existing LPS
systems. The fifth patienthad an LPS revision after the previous
LPS migrated.Follow-up ranged from 5 to11 months (mean, 7.83
months). All patients had a good outcome with immediateresolution
of over-drainage symptoms and are currentlyasymptomatic.Conclusions
The use of M-DSV in LPS is an effectivealternative for avoiding
posture-related over-drainage andmanaging patients with LPS-related
over-drainage symp-toms. Further experience is required to address
the long-termoutcome, balancing sufficient drainage while
preventingover-drainage.
Keywords Lumboperitoneal shunt . Over-drainage .
Miethke DualSwitch Valve . Gravity-assisted valve .
Pseudotumor cerebri . Intracranial pressure
Introduction
Physiological regulation of intracranial pressure (ICP) hasbeen
an unachievable goal since the introduction of shuntsfor
cerebrospinal fluid (CSF) diversion despite the develop-ment of
over 200 different types of shunts with more thanthousand pressure
permutations within the last 50 years [1].
Lumboperitoneal shunts (LPS) have long been used forthe
treatment of idiopathic intracranial hypertension (pseu-dotumor
cerebri (PTC)), postoperative pseudomeningocele,CSF leaks, and
"communicating hydrocephalus". Althoughthey can provide a rapid and
effective resolution ofsymptoms, there are major disadvantages
associated withLPS use, such as posture-related CSF over-drainage
and its
S. Udayakumaran (*) : J. Roth : S. Constantini (*)Department of
Pediatric Neurosurgery, Dana Childrens Hospital,Tel Aviv
University,Tel Aviv Sourasky Medical Center, 6 Weizman Street,Tel
Aviv 64239, Israele-mail: [email protected]:
[email protected]
A. KeslerNeuro-ophthalmology Unit, Department of
Ophthalmology,Tel Aviv University,Tel Aviv Sourasky Medical Center,
6 Weizman Street,Tel Aviv 64239, Israel
Acta Neurochir (2010) 152:17931800DOI
10.1007/s00701-010-0724-4
-
myriad manifestations, occasionally associated with ac-quired
Chiari malformation [2].
Various methods have been used to avoid or manage
CSFover-drainage with LPS, including upgrading the shunt
tohigher-pressure settings, using programmable valves, andusing
flow-restricting or hydrostatic devices [35].
Hydrostatic valves take into account the patientsposture,
restricting CSF drainage during upright positions.The Miethke
DualSwitch Valve (M-DSV) system is a typeof horizontalvertical (HV)
switcher type of hydrostaticvalve with its resistance depending on
the patient position.Since its introduction in 1994 by Miethke and
co-workers,the DualSwitch Valve has been used effectively to
avoidand manage over-drainage in different types of
adulthydrocephalus [1, 69].
Flow-restricting devices, as a rule, require the deviceplacement
parallel to the body axis, making it cumbersometo use together with
LPS. The M-DSV designed for LPScan conveniently be interposed in
line with the shunttubing. This, along with many other advantages
describedin this paper, makes it an attractive device for LPS.
We introduce the use of the M-DSV to avoid and
manageover-drainage in LPS and describe our preliminary
experiencewith these valves for LPS. This is the first case series
focusingon the use of M-DSVas a restrictive component in LPS.
Materials and methods
During the period of June to December 2009, we treatedfive
patients with LPS using an M-DSV. All patients hadLPS revisions
with the M-DSV, four for clinically signif-icant over-drainage
(presenting with new-onset positionalheadaches) and one for distal
shunt migration.
Prospectively collected data included patient demo-graphics,
clinical status (including details of prior surgeriesand
preoperative neurological and neuro-ophthalmologicalstatus),
operative findings, and clinical and neuro-ophthalmological
follow-up.
The M-DSV technology
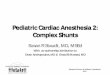
The M-DSV valve consists of two integrated chambers,each with a
different opening pressure (www.miethke.com).The low-pressure
chamber is activated when the patient isrecumbent. The
high-pressure chamber is activated whenthe patient is in an upright
position. Toggling betweenchambers is by a heavy tantalum sphere
which occludes thedrainage through the low-pressure chamber as soon
as thepatient is in upright position (Fig. 1). Switching
betweenpressure settings is not gradual but occurs at an angle
ofabout 60-70 (C. Miethke, personal communication, 2009).For
example, the actual opening pressure in a 10/40 M-
DSV is 10 cm H2O when at an angle between 0 (supine) to60-70,
and 40 cm H2O when at an angle between 60-70to 90 (upright). Thus,
the ICP is kept in a physiologicalrange whether the patient is
supine or upright (C. Miethke,personal communication, 2009). The
M-DSV has beenevaluated in adult hydrocephalus and has been found
tomaintain ICP within physiological limits independent ofpatient
posture [1, 6, 8, 9].
The M-DSV is available with opening pressures of 5, 10,13, and
16 cm H2O for the supine position and 30, 40, and50 cm H2O for the
upright position. When supine, the M-DSV operates like a
conventional differential pressurevalve. The recommended standard
pressure setting for thelower-pressure valve, according to the
manufacturer (C.Miethke GmbH & Co. KG) is 10 cm H2O (5 cm H2O
forpatients with normal-pressure hydrocephalus (NPH)).
Thehigh-pressure side of the valve is calculated as a function
ofthe sitting height and is chosen in such a way that with
thepatient upright, a ventricular pressure of at least 5 cm H2Owill
be maintained under all circumstances (C. MiethkeGmbH & Co.
KG).
Suitable pressure is calculated as follows:
1 Measure the distance between the third ventricle (at thelevel
of the foramen of Monro, as roughly measured fromthe external
auditory meatus) and the patients diaphragm(as roughly measured at
the level of the costal arch).
2 Subtract 5 cm from the measured distance.3 Choose a valve
whose high-pressure setting exceeds the
final measured value by the smallest amount. Ventricularpressure
in the patient will then be kept between 5 cmH2O and +5 cm H2O at
all times.
Surgical aspects of the M-DSV
The M-DSV valve is interposed and placed in theabdominal wall
(or at the flank) (manufacturer's recom-
Fig. 1 Schematic representation of the valve technology.
1Inletconnecting to the intrathecal catheter. 2 Outlet towards the
peritonealcatheter. 3 Low-pressure chamber. 4 High-pressure
chamber. 5 Ballresponsible ("switch") for toggling between pressure
chambersdepending on the position
1794 Acta Neurochir (2010) 152:17931800
-
mendation: arcus costalis). The valve function requires it
beplaced in an axis parallel to the body (direction as indicatedby
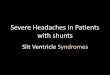
an arrow on the valve). The specific design of the M-DSV meant for
the LPS has a perpendicular connectorallowing it to be interposed
in line with the LPS [Fig. 2].An antechamber that can be used for
pressure measurementand fluid aspiration is located proximal to the
valve. Theantechamber has a narrow connecter for connection withthe
intrathecal catheter. The valve is connected distally toan
abdominal catheter for intra-peritoneal insertion; alter-natively,
it can be connected to a pre-existing distalabdominal catheter
using a straight connector. The valvemay be anchored to the tissue
layers using sutures tomaintain its orientation with respect to the
axis of the body.
We used a valve with opening pressures of 10/40 for allfive
patients in accordance with their sitting height. Thepatients were
regularly followed, and the outcomes wereevaluated based on the
preoperative and postoperativesymptomatology.
Results
From June to December 2009, we treated five patients,
fourfemales and one male, ages ranging from 22 to 71 years.Patient
demographic data, clinical history, indications for
LPS and for using the M-DSV, and follow-up aresummarized in
Table 1.
Initial indications for LPS
Three patients had PTC, one patient had an LPS fortreatment of a
posterior fossa pseudomeningocele (follow-ing an excision of a
tentorial meningioma), and one elderlypatient had an LPS for
treatment of cauda equina syndromesecondary to a lumbar dural
ectasia associated withankylosing spondylitis.
Indications for LPS revision
Four patients (all females) had a history of posturalheadaches
consistent with over-drainage, secondary topre-existing LPS
systems. One of the patients had a historyof upgrading her valve
(medium pressure to Delta 2); twopatients had a prior LPS, one with
a medium-pressure valve(PS medical, Medtronic) and another with a
Delta 1.5valve. The fourth patient, with a valveless LPS for
PTC,presented with visual deterioration associated with
posturalheadaches that were attributed to over-drainage secondaryto
LPS and not raised ICP. The fifth patient, an elderlymale, had an
LPS revision with an M-DSV after theprevious LPS (placed for
treatment of a symptomaticlumbar dural ectasia) migrated.
Operative and perioperative course
Four valves were placed along the right side and onealong the
left. There were no technical difficulties in anyof the patients,
including in the three PTC patients whowere severely obese.
Patients were discharged within 2-3 days following surgery. There
were no exacerbations ofpreoperative symptoms following surgery.
One patientrequired a distal revision 2 weeks later for
proximalmigration of the peritoneal catheter to the new
valvepocket.
Long-term follow-up
Average follow-up was 7.83 months, ranging from 5 to11 months.
All four patients presenting with over-drainage symptoms had
immediate significant improve-ment and are currently asymptomatic.
There were noexacerbations in any of the PTC patients. The patient
whopresented with visual deterioration experienced improve-ment.
The patient with the cauda equina syndromesecondary to a lumbar
dural ectasia has had completerelief of his symptoms with no
symptoms of over-drainage. None of the patients had any
ophthalmologicalsequelae.
Fig. 2 Photograph of the valve constituents. The arrows show
theinlet (1) to the valve and outlet (2) from the valve. The inlet
has anarrow connecter for the intrathecal catheter and leads to
anantechamber. The outlet has a connector for the abdominal
catheterfor intra-peritoneal insertion. An arrow on the valve
indicates thedirection of the valve, to be placed parallel to the
body axis. Noticethat the M-DSV meant for LPS has been specifically
designed withperpendicular connectors to allow it to be easily
interposed in linewith the LPS. The valve may be anchored to the
tissue layers usingsutures to maintain its orientation with respect
to the axis of the body
Acta Neurochir (2010) 152:17931800 1795
-
Illustrative case
A 22-year-old obese female presented with severe andconstant
headaches. Her neurological examination wasnormal apart from
bilateral papilledema. Imaging wasunremarkable, and she was
diagnosed with PTC. She faileda trial of conservative measures
including weight loss andmedical therapy with Diamox
(acetazolamide) as shedeveloped side effects. Subsequently, an LPS
with amedium-pressure valve (PS Medical, Medtronic) wasinserted.
Although she initially experienced marked im-provement in her
headaches, she later began complaining ofpositional headaches which
improved on recumbent posi-tion. She had no significant relief of
symptoms withconservative measures over a period of 1 year. One of
theepisodes was severe enough to bring her to the
emergencydepartment. An urgent head CT and shunt
radiographscompleted during this episode were normal. Puncture of
theshunt chamber revealed free flow but a very low pressure of2 cm
H2O.
Two months later, with a provisional diagnosis of low-pressure
headaches, she underwent a valve upgrade to aDelta 2 (PS Medical,
Medtronic). The headaches initiallyimproved but the effect wore
off, and she continued tosuffer substantial headaches, especially
when in the uprightposition. The headaches worsened with physical
activityand led to severe impairment of quality of life.
Eightmonths later, she underwent a valve revision with an M-DSV
10/40. The patient improved immediately aftersurgery and no longer
complained of postural headaches.At 11-month follow-up, she
continues to remain symptomfree with a normal fundus.
Discussion
Several authors have reported a clear reduction in theincidence
of over-drainage among patients with adulthydrocephalus treated by
ventriculoperitoneal shunts(VPS) with M-DSV [1, 610]. In view of
these previouslypublished results showing the advantage of M-DSV in
VPSfor various hydrocephalic pathologies in adults, we opted
toutilize the M-DSV in our patients with LPS. Our series is
thefirst series focusing on the usage of M-DSV for LPS in anattempt
to avoid and manage posture-related over-drainage.
Since the introduction of LPS in the 1950s and silasticcatheters
in 1975 by Selman et al. [11], LPS have evolvedas an important
option for CSF diversion, serving as analternative to VPS for
several indications [11, 12]. LPShave been used to treat a host of
conditions including CSFrhinorrhea, normal pressure hydrocephalus,
lumbar pseu-domeningocele, slit ventricle syndrome, and in
particularPTC [13, 14].Ta
ble1
Patient
details
Serialno:Patient
characteristics
Indicatio
nforLPS
Valve
used
priorto
M-D
SV
Clin
ical
Features
Indicatio
nforLPS
revision
OutcomeafterLPSwith
M-D
SV
122/F
PTC
Medium
pressure
(PSmedical),
over-drainageY
(Delta
2.0)
Posturalheadaches
Clin
ical
over-drainage
Improved
inclinical
symptom
swith
norm
alvision,andfundus
262/F
Postoperativ
epseudomeningocele
aftersurgeryfortentorial
meningiom
a
Cystoperitoneal
shuntY
VPS
(Medium-pressurevalve),
malfunctio
nY
LPSwith
medium-pressurevalve
Posturalheadaches
Clin
ical
over-drainage
Improved
symptom
s,no
pseudomeningocele
371/M
Ankylosingspondylitiswith
symptom
atic
duralectasia
LPSthat
migrated.
Nonfunctio
nalUrinary
incontinence
and
pseudomeningocele
ofthe
lumbararea
LPSmalfunctio
nIm
proved
symptom
s
428/F
PTCwith
optic
nervefenestratio
nDelta
1.5
Posturalheadaches
Clin
ical
over-drainage
Improved
symptom
s
530/F
PTC
Valveless
Posturalheadaches,Visual
deterioration,
ICPshow
ednegativ
evalue;
Fundus-optic
atrophy
Clin
ical
over-drainage
Improved
symptom
s
Y:representschange
to,follo
wingsymptom
sof
overdrainage.
1796 Acta Neurochir (2010) 152:17931800
-
LPS offer numerous advantages over VPS includingavoidance of the
need to access ventricular cavities withinthe brain parenchyma,
thereby avoiding potential compli-cations such as cortical venous
injury or hemorrhage, aswell as lower seizure and infection rates
[15, 16] and a verylow mortality rate compared to VPS [5, 17]. In
the contextof communicating hydrocephalus, LPS are probably
morephysiological, maintaining patency of all ventricular cavi-ties
compared to a VPS [18], as they access CSF from boththe ventricles
and cortical subarachnoid spaces through thespinal subarachnoid
space.
Although LPS provide rapid and effective resolution ofthe
primary symptoms, several disadvantages are associatedwith their
use. Complication rates associated with thecurrent LPS systems are
considered high [17]. Orthostaticover-drainage and its myriad
manifestations are especially aconcern when using LPS [14]. The
incidence of symptom-atic over-drainage secondary to LPS is
reported to be ashigh as 15-20% [1921].
Although over-drainage is a general concern whenplacing an LPS,
patients who receive LPS with valves hada lower frequency of
over-drainage symptoms compared topatients whose shunts had no
valve [22].
Historically, lumboperitoneal shunting was performed
byimplanting a single tube with the proximal end in thelumbar CSF
space and the distal end intraperitoneally.Tonsillar herniation was
a common sequel following theseshunts [2]. Spetzler et al. and
others introduced LPS with avalve system [11, 23]. Valve types used
for LPS can besubdivided into three types:
1 conventional differential pressure valves with a fixedopening
pressure,
2 adjustable devices, enabling noninvasive percutaneouschange of
the opening pressure, and
3 hydrostatic valves that take into account the patientposture
and include flow-restricting devices that changetheir flow
regulation in a gradual way (analog type ofvalves e.g., Miethke's
ShuntAssistant) or have an abruptchange of regulation status (e.g.,
as with the M-DSV).
Many of these valves are not subject to reliable qualitycontrol
[24]. In their detailed evaluation of shunt valves,Czosnyka et al.
concluded that the actual in vivo behaviorof the majority of valves
currently available may notexactly match the manufacturers product
information.Significant problems encountered by Czosnyka and
col-leagues included over-drainage, sensitivity of CSF flow tobody
posture, blockage caused by subcutaneous pressure,and changes in
settings related to external magnetic fields[2527]. Czosnyka et al.
reported that the over-drainagerate might be reduced in Medtronic
PS Medical LPSbecause of the very high hydrodynamic resistance of
thethin tube (internal diameter of 0.8 mm, compared with
1.2 mm for most distal drains). On the other hand, suchhigh
resistance may potentially cause the shunt to under-drain in
horizontal body positions [27].
Various additional methods have been used to avoid andmanage CSF
over-drainage, including upgrading the valveto a higher-pressure
valve, adding an anti-siphon device,and using a programmable valve,
all with inconsistentresults [35, 28, 29]. Upgrading the valve
pressure settingto overcome over-drainage may lead to increased
resis-tance, especially in the supine position, and may lead
tosymptoms of under-drainage.
Wang et al. reported that among the74 patients with LPS,11 had
symptoms of over-drainage. Seven of these patientshad a valveless
system, and four had a HV valve. In nine ofthese 11 patients,
symptoms resolved after a valve wasinserted or after their valves
were set to a higher pressure[5]. The Integra HV valve (Integra
LifeSciences, Plains-boro, NJ) utilized in that series was
introduced in the 1990sfor LPS. The Integra HV incorporated two
different valvesto allow for control of CSF flow when a patient is
in eitherupright or supine position. In addition, an antechamber
isavailable for access to the LPS.
Chang et al. in their series of LPS with Codman
Hakimprogrammable valves for NPH observed over-drainagesymptoms in
five of 32 patients, but they recovered afterincreasing the valve
pressure. According to Chang et al.,the major advantage in the use
of programmable valve isthe ability to modify the pressure and thus
manage over-drainage or under-drainage noninvasively. Thus,
inclusionof the Codman Hakim programmable valve in the LPS mayavoid
the need for a second operation in which a differentpressure valve
is implanted [3].
Nadkarni et al. placed a ventricular access device (VAD)and an
LPS using a Codman Hakim programmable shuntwith a SIPHONGUARD
(Codman Corp.). The VAD wasmeant for ICP measurement, and the shunt
also had a flow-limiting device, the (flow-restricting device
[30]). Thisadd-on device increases resistance linearly with high
CSFflow and may therefore prevent over-drainage [4]. Asignificant
disadvantage of programmable valves is findingthe correct pressure
as the rate of CSF production and thepressureflow curve are not
precisely known in individualpatients. Also, the programming may be
inaccurate espe-cially if the patient is obese, as is often the
case for patientswith PTC. Additionally, since the main problem
forpressure valves is maintaining sufficient CSF drainagewhile the
patient is in supine, sitting, and standingpositions, they may
reduce but cannot exclude over-drainage [31]. In addition, valve
pressure setting may bealtered even by low magnetic fields [32].
The additionalplacement of a VAD requires an additional
procedure(usually stereotaxy-based) and entails the potential
morbid-ity of an invasive cortical procedure and infection.
Zemack
Acta Neurochir (2010) 152:17931800 1797
-
and Romner conducted a cost analysis of programmablevalves and
concluded that the increased cost cannot beadequately justified
with the current evidence of complica-tions associated with these
valves [32].
In principle, siphoning per se should not significantlyaffect an
LPS due to the comparable heights of theproximal and distal tips of
the shunt system. However,the pressure at the proximal end of the
valve reflects thehydrostatic pressure of a fluid-filled column
(between theintracranial compartment and the spinal
subarachnoidspace upstream from the tip of the intrathecal
catheter).As the valve is a pressure-regulated system, the
elevatedpressure differential across the valve during
uprightpositions increases the flow and CSF drainage rates
ascompared to that during a supine position, hence the highrate of
over-drainage in LPS.
The efficacy of an anti-siphon device to counter over-drainage
in LPS is questionable [30]. The reason is, asdiscussed above, that
true siphoning may not have a role inthe CSF dynamics of an LPS.
Also, susceptibility tosubcutaneous pressures in general and during
routineactivity in particular raises questions over their
efficacy.Hence, valves with anti-siphon devices (such as the
Deltavalves) probably have a limited role to play in preventingLPS
over-drainage.
The concept of gravitational shunts has existed since1970s and
has been found to have encouraging results inavoiding
posture-related over-drainage in adult and child-hood hydrocephalus
[3335]. In 1975, Hakim presented theHakim Lumbar HV valvethe first
technically maturegravitational shunt. The first concept of the
switcher typeof gravitational valve was introduced with
MarionsSophysa AS valve in 1983. This valve too was not
wellaccepted. The first valve regulation for HV change
wasintroduced by Hakim-Cordis in the 1980s. These valves didnot
stand the test of time and are mostly no longer available[31].
The M-DSV system is also a type of kind of a HVswitcher type of
valve. As described above in thesubsection The M-DSV Technology
under section Materialsand Methods, the valve resistance changes
depending onthe patient position, toggling between a
low-resistanceopening pressure while in supine position and a
high-resistance opening pressure while in upright position.
Several authors found clear reduction in over-drainageamong
patients with adult hydrocephalus who were treatedby VPS with M-DSV
[1, 610]. Mier et al. in their series ofM-DSV for 128 patients with
NPH treated by VPS with M-DSV found an over-drainage rate of 2%
[6]. Another studyby the same author compared different valves,
reporting anover-drainage rate of about 6% with Cordis standard
valves,16% with Cordis-Orbis-Sigma valves, and 2% with M-DSV[36].
Tsunoda et al. in their series of VPS with M-DSV for
101 patients with adult hydrocephalus reported only
threepatients with over-drainage. Six patients, in this
series,experienced under-drainage (importantly all
bedriddenpatients) [9].
In our series, four patients with prior LPS (variousvalves
including two with Delta valves) presented withsymptoms of
over-drainage. In view of the prior publishedresults showing the
advantage of M-DSV in VPS forvarious hydrocephalic pathologies in
adults, we opted toplace the M-DSV in these LPS patients with
apparentsuccess. In the fifth patient, by using an M-DSV, we seemto
have averted the possible complication of over-drainagewhich
elderly patients are prone to [37].
Although in our small series we seem to have overcomethe issue
of over-drainage in all patients using the samelower-pressure
setting (10 cm H2O), over-drainage may stilloccur in some patients.
In such cases, an M-DSV with ahigher low-pressure setting could be
used. Unlike mostprogrammable valves, opening pressures of the
M-DSVvalves are not affected by magnetic field, and the
titaniumcasing makes it resistant to changes in
subcutaneouspressure [38, 39]. The M-DSV also has an
antechamberthat can be used for pressure measurement, fluid
aspirationfor analysis, and ruling out proximal malfunction.
Also,unlike other flow-restricting devices (where the
requirementfor the device to be placed parallel to the body axis
foreffective action may be inconvenient in cases of LPS), theM-DSV
designed for LPS can conveniently be interposedin line with the
shunt tubing.
Unlike the Cordis HV valve and the Chabbra valve, theforce
exerted by CSF flow in the M-DSV is downward onthe
gravity-propelled ball whenever the patient is in theupright
position, supporting the closing mechanism of thetantalum ball, as
opposed to the other two valves wherethe CSF flows against the
gravity-activated closingmechanism of the balls. Therefore, in the
M-DSV, theforces acting upon the tantalum ball closing the
low-pressure chamber become stronger with rising ICP
and/orhydrostatic pressure. Thus, the danger that the
closingmechanism will be influenced by normal activities ofdaily
life such as walking, running, or other valsalvamaneuvers is much
lower with the M-DSV than with theother valves. Simulation of such
normal daily activities invivo proved the superiority of the
closing mechanism of thetantalum ball in the M-DSV over those in
the Cordis HVvalve and the Chabbra valve [39]. Conventional
radiographsallow checking of the graduation and position of the
M-DSV and can also test the tantalum ball movements [39].
While hydrostatic valves theoretically have a higher riskof
clogging [40, 41], the M-DSV seems to have a lower riskof clogging
due to a larger diaphragm surface area, andhence may maintain CSF
flow irrespective of its composi-tion [35, 39].
1798 Acta Neurochir (2010) 152:17931800
-
One possible disadvantage of the M-DSV valves is thefixed
pressure settings. Any change of settings requires anoperative
intervention. Although our patients had goodoutcomes, shunt
revisions to implement necessary pressurechanges are a definite
possibility. Tsunado et al. in theirstudy on treatment of adult
hydrocephalus with M-DSVhad a rate of 7.5% shunt revisions due to
under-drainage[9].
The M-DSV has been proven to establish a physiologicalCSF
diversion irrespective of patient posture and CSFcomposition in
adult hydrocephalus [79, 39]. Our attemptto exhibit the same for
LPS seems to hold promise. Therestill remains the need for larger
studies as well as longerfollow-up.
Conclusions
Using the M-DSV in LPS may balance the need foreffective CSF
drainage on one hand while preventingover-drainage on the other.
However, controlled studiesare indispensable, and further
evaluation of this valve,both as a primary choice for LPS and in
revisions forover-drainage, should be sought. Our early
experiencehighlights the advantages of this valve for patients
withLPS.
Disclosure The authors report no conflict of interest concerning
thematerials or methods used in this study or the findings
specified in thispaper. None of the authors have received any
financial support for thearticle from any organization.
References
1. Hertel F, Zuchner M, Decker C, Schill S, Bosniak I, Bettag
M(2008) The Miethke dual switch valve: experience in 169
adultpatients with different kinds of hydrocephalus: an open
fieldstudy. Minim Invasive Neurosurg 51:147153
2. Chumas PD, Armstrong DC, Drake JM, Kulkarni AV, HoffmanHJ,
Humphreys RP, Rutka JT, Hendrick EB (1993) Tonsillarherniation: the
rule rather than the exception after lumboperitonealshunting in the
pediatric population. J Neurosurg 78:568573
3. Chang CC, Kuwana N, Ito S (1999) Management of patients
withnormal-pressure hydrocephalus by using lumboperitoneal
shuntsystem with the Codman Hakim programmable valve.
NeurosurgFocus 7:e8
4. Nadkarni TD, Rekate HL, Wallace D (2008) Concurrent use of
alumboperitoneal shunt with programmable valve and
ventricularaccess device in the treatment of pseudotumor cerebri:
review of40 cases. J Neurosurg Pediatr 2:1924
5. Wang VY, Barbaro NM, Lawton MT, Pitts L, Kunwar S, ParsaAT,
Gupta N, McDermott MW (2007) Complications of lumbo-peritoneal
shunts. Neurosurgery 60:10451048, discussion 1049
6. Meier U, Kiefer M, Sprung C (2004) Evaluation of the
Miethkedual- switch valve in patients with normal pressure
hydrocepha-lus. Surg Neurol 61:119127, discussion 127-118
7. Sprung C, Miethke C, Shakeri K, Lanksch WR (1998) Pitfalls
inshunting of hydrocephalusclinical reality and improvement bythe
hydrostatic dual-switch valve. Eur J Pediatr Surg
8(Suppl1):2630
8. Trost HA, Sprung C, Lanksch W, Stolke D, Miethke C
(1998)Dual-switch valve: clinical performance of a new
hydrocephalusvalve. Acta Neurochir Suppl 71:360363
9. Tsunoda A, Maruki C (2007) Clinical experience with a
dualswitch valve (Miethke) for the management of adult
hydroceph-alus. Neurol Med Chir (Tokyo) 47:403408, discussion
408
10. Meier U, Zeilinger FS, Reyer T, Kintzel D (2000)
Clinicalexperience with various shunt systems in normal
pressurehydrocephalus. Zentralbl Neurochir 61:143149
11. Spetzler RF, Wilson CB, Grollmus JM (1975)
Percutaneouslumboperitoneal shunt Technical note. J Neurosurg
43:770773
12. Selman WR, Spetzler RF, Wilson CB, Grollmus JW
(1980)Percutaneous lumboperitoneal shunt: review of 130
cases.Neurosurgery 6:255257
13. Burgett RA, Purvin VA, Kawasaki A (1997)
Lumboperitonealshunting for pseudotumor cerebri. Neurology
49:734739
14. Chumas PD, Kulkarni AV, Drake JM, Hoffman HJ, HumphreysRP,
Rutka JT (1993) Lumboperitoneal shunting: a retrospectivestudy in
the pediatric population. Neurosurgery 32:376383,discussion 383
15. Aoki N (1990) Lumboperitoneal shunt: clinical
applications,complications, and comparison with
ventriculoperitoneal shunt.Neurosurgery 26:9981003, discussion
10031004
16. Choux M, Genitori L, Lang D, Lena G (1992) Shunt
implantation:Reducing the incidence Of shunt infection. J Neurosurg
77:875880
17. Karabatsou K, Quigley G, Buxton N, Foy P, Mallucci C
(2004)Lumboperitoneal shunts: are the complications acceptable?
ActaNeurochir (Wien) 146:11931197
18. Khorasani L, Sikorski CW, Frim DM (2004) Lumbar CSFshunting
preferentially drains the cerebral subarachnoid over theventricular
spaces: implications for the treatment of slit ventriclesyndrome.
Pediatr Neurosurg 40:270276
19. Eggenberger ER, Miller NR, Vitale S (1996)
Lumboperitonealshunt for the treatment of pseudotumor cerebri.
Neurology46:15241530
20. McGirt MJ, Woodworth G, Thomas G, Miller N, Williams
M,Rigamonti D (2004) Cerebrospinal fluid shunt placement
forpseudotumor cerebri-associated intractable headache: predictors
oftreatment response and an analysis of long-term outcomes.
JNeurosurg 101:627632
21. Rosenberg ML, Corbett JJ, Smith C, Goodwin J, Sergott
R,Savino P, Schatz N (1993) Cerebrospinal fluid diversion
proce-dures in pseudotumor cerebri. Neurology 43:10711072
22. Virella AA, Galarza M, Masterman-Smith M, Lemus R,
LazareffJA (2002) Distal slit valve and clinically relevant CSF
overdrainagein children with hydrocephalus. Childs Nerv Syst
18:1518
23. Rekate HL, Wallace D (2003) Lumboperitoneal shunts in
children.Pediatr Neurosurg 38:4146
24. Aschoff A (1994) In-vitro-Testung von
Hydrocephalus-Ventilen.University of Heidelberg, Habilitation
25. Czosnyka M, Czosnyka Z, Momjian S, Pickard JD
(2004)Cerebrospinal fluid dynamics. Physiol Meas 25:R51R76
26. Czosnyka Z, Czosnyka M, Richards H, Pickard JD
(1998)Hydrodynamic properties of hydrocephalus shunts. Acta
Neuro-chir Suppl 71:334339
27. Czosnyka Z, Czosnyka M, Richards HK, Pickard JD
(1998)Posture-related overdrainage: comparison of the performance
of10 hydrocephalus shunts in vitro. Neurosurgery
42:327333,discussion 333-324
28. Lam FC, Wheatley MB, Mehta V (2007) Treatment of
secondarytonsillar herniation by lumboperitoneal shunt revision.
Can JNeurol Sci 34:237242
Acta Neurochir (2010) 152:17931800 1799
-
29. Lundkvist B, Eklund A, Kristensen B, Fagerlund M,
KoskinenLO, Malm J (2001) Cerebrospinal fluid hydrodynamics
afterplacement of a shunt with an antisiphon device: a long-term
study.J Neurosurg 94:750756
30. Nissels R, inventor; Johnson & johnson Professional,
Inc.,assignee (1997) Fluid flow limiting device. US patent
6,126,628
31. Aschoff A, Kremer P, Benesch C, Fruh K, Klank A, Kunze
S(1995) Overdrainage and shunt technology. A critical comparisonof
programmable, hydrostatic and variable-resistance valves
andflow-reducing devices. Childs Nerv Syst 11:193202
32. Zemack G, Romner B (2001) Do adjustable shunt valves
pressureour budget? A retrospective analysis of 541 implanted
CodmanHakim programmable valves. Br J Neurosurg 15:221227
33. Haberl EJ, Messing-Juenger M, Schuhmann M, Eymann R,Cedzich
C, Fritsch MJ, Kiefer M, Van Lindert EJ, Geyer C,Lehner M, Rohde V,
Stroux A, von Berenberg P (2009)Experiences with a gravity-assisted
valve in hydrocephalicchildren. J Neurosurg Pediatr 4:289294
34. Kiefer M, Eymann R, Strowitzki M, Steudel WI
(2005)Gravitational shunts in longstanding overt ventriculomegaly
inadults. Neurosurgery 57:109119
35. Rohde V, Haberl EJ, Ludwig H, Thomale UW (2009)
Firstexperiences with an adjustable gravitational valve in
childhoodhydrocephalus. J Neurosurg Pediatr 3:9093
36. Meier U, Kintzel D (2002) Clinical experiences with
differentvalve systems in patients with normal-pressure
hydrocephalus:evaluation of the Miethke dual-switch valve. Childs
Nerv Syst18:288294
37. Aschoff A, Kremer P (1998) Determining the best
cerebrospinalfluid shunt valve design: the pediatric valve design
trial.Neurosurgery 42:949951
38. Miethke C, Affeld K (1994) A new valve for the treatment
ofhydrocephalus. Biomed Tech (Berl, Z) 39:181187
39. Sprung C, Miethke C, Trost HA, Lanksch WR, Stolke D
(1996)The dual-switch valve. A new hydrostatic valve for the
treatmentof hydrocephalus. Childs Nerv Syst 12:573581
40. Aschoff A, Benesch C, Kremer R, Haken MS, Klank A,
OsterlohM, Fruh K (1993) The solved and unsolved problems
ofhydrocephalus valves: a critical comment. Adv
Neurosurg21:103114
41. Sainte-Rose C (1993) Shunt obstruction.A preventable
complica-tion? Pediatr Neurosurg 19:156164
1800 Acta Neurochir (2010) 152:17931800
-
Reproduced with permission of the copyright owner. Further
reproduction prohibited without permission.
c.701_2010_Article_724.pdfMiethke DualSwitch Valve in
lumboperitoneal
shuntsAbstractAbstractAbstractAbstractAbstractIntroductionMaterials
and methodsThe M-DSV technologySurgical aspects of the M-DSV
ResultsInitial indications for LPSIndications for LPS
revisionOperative and perioperative courseLong-term follow-up
Illustrative caseDiscussionConclusionsReferences