Embed Size (px)
Citation preview

Migration and depression
Introduction
Migration is of different types and different groupsand communities migrate for a number of reasons.These reasons include study, economic betterment,political exile or social momentum. In order tounderstand the process of migration, the clinicianmust take into account personal, familial, socialand cultural factors. A predisposition to migrate isa function of deprivation of social contacts, finan-cial, economic or educational deprivation as well asdeprivation of housing and climatic factors. Peoplemay weigh up rationally the advantages of utilitiesin two settings, e.g. across the rural–urban divideor transnational, before making a decision tomigrate.Shaw (1) concludes that in addition to who the
migrants are and why they are migrating theresearcher must also look into culture systemscomponents, including ideological commitments,personality systems, including the individuals aspir-ations identity, integrity and role performance aswell as levels of stress in the system. The typologies
of migration are related to motives for migration,whether it is forced or voluntary, and length of stayafter migration. People moving within the sameculture, for instance from rural to urban areas, alsofeel the stress of migration, change of environmentand altered social support. All these factors tend tointeract and to increase stress which, according tothe stress diathesis model, is likely to increase thelikelihood of mental illness – more so in schizo-phrenia, although the data for affective disordersin general and depression in particular are notclearcut.Rack (2) cautions that the clinician must be
aware of cultural pitfalls in the recognition ofdepression and anxiety. Somatization as a meta-phor and as a pathway into medical health-caresystems is an important aspect and the individualperception and interpretation of these factors arecrucial in the signposting of pathways to care. Thesymptomalology of psychotic depression may wellbe similar across cultures but factors such as guiltas a key symptom of depression do not fall easilyinto diagnostic categories. In some cultures thenotion of shame may well be more predominantwhen compared with guilt. Thus any epidemio-logical observations have to be placed into thatparticular context. Bhugra et al. (3) identified thatamong middle-aged Punjabi women depression (as
Bhugra D. Migration and depression.Acta Psychiatr Scand 2003: 108 (Suppl. 418): 67–72.ª Blackwell Munksgaard 2003.
Objective: Migrants migrate for a number of reasons and varyingduration. The objective in this paper is to review the findings toascertain whether rates of depression among migrants are highercompared with the non-migrant populations.Method: We used the published data to review the theoreticalbackground for migration and to study the existing literature on ratesof depression in various migrant and ethnic groups.Results: The rates of depressive neurosis vary according to migrantstatus. Migrants in some groups are less likely to report symptoms ofdepression. Using fluency in language as a proxy measure ofacculturation it appears that acculturated individuals are more likely tobe depressed.Conclusion: The impact of migration on depression is not as clear andstraightforward as for other psychiatric conditions. More work needsto be carried out in understanding the impact of migration ondepression.
D. BhugraSection of Cultural Psychiatry, Institute of Psychiatry,London, UK
Key words: culture; culture shock; depression;migration
D. Bhugra, Professor of Mental Health & CulturalDiversity, Section of Cultural Psychiatry, PO 25, HSRD,David Goldberg Centre, Institute of Psychiatry,De Crespigny Park, London SE5 8AF, UK
A preliminary version of this paper was read at the 2ndInternational Zurich Conference on Clinical and Social Psy-chiatry, Zurich, 6–8 September 2001. The symposium and thispublication were sponsored by Eli Lilly Suisse.
Acta Psychiatr Scand 2003: 108 (Suppl. 418): 67–72Printed in UK. All rights reserved
Copyright ª Blackwell Munksgaard 2003
ACTA PSYCHIATRICASCANDINAVICAISSN 0065-1591
67

identified by clinicians at reactive level) is not seenas an illness for which prayers, visits to the templeor mosque are seen as sufficient. The ongoingdebate about the typology of depression suggeststhat medical and lay models of depression are notonly different but also place different emphases onsymptoms.The following studies, therefore, have to be seen
in that particular context. In most of the epidemi-ological studies the data have been collected usingEuro-centric instruments that may not always pickup features of depression, which may be culturallyspecific.
Prevalence of depression among migrants
Several studies show that rates of common mentaldisorders are higher among migrating groups andgroups with out-migration (4, 5), whereas othershave shown that the rates remain broadly similarto the host population.In the USA, among various ethnic groups
affective and anxiety disorders show a fairlyconstant crude rate but somewhat age-specificand sex-specific rates (6). Many studies havedemonstrated a relationship between mentalhealth and academic performances of foreignstudents (7–9). Still (9) reported that 14% of theBritish students had psychological problems com-pared with 28% Iranian and Nigerian students,22% Egyptian and Turkish and 18% of Indiansubcontinent students. Ward (10) described theforeign student syndrome, which he characterizedby vague non-specific physical complaints, passivewithdrawn interaction style and dishevelledunkempt appearance, and went on to suggest thatthese students sought medical help more often forphysical complaints. This was confirmed byBabiker et al. (11) when they found that culturedistance in foreign students was associated withmedical consultations, symptoms and examinationsuccess. These authors found that culturally distantstudents perceived the health services as anapproachable safe haven and suffered more phys-ical illness. The findings of common mental dis-order among foreign students are variable.Cochrane (12) studied the admission rates to
mental hospitals and found that the rate ofadmission for British-born individuals was265 ⁄100 000, whereas for immigrants these rateswere higher at 495 ⁄100 000. However, after ageand sex standardization, the rates for the Irish(1110 ⁄100 000) and West Indians (539 ⁄100 000)were much higher compared with Indians(403 ⁄100 000) and Pakistanis (336 ⁄100 000), bothof whom showed lower admission rates. For
affective disorders, too, the rates among Indian,West Indian and Pakistani immigrants were lowerthan the British-born but those of Irish immigrantswere higher. All immigrants except West Indiansshowed higher rates of suicide. Cochrane (13)suggests that some of the discrepancy can beexplained by selective migration, ambivalent rela-tionships and adjustment to culture.Nazroo (14) reported in a community survey
that weekly prevalence of depressive neurosis was2.7% for white males and 4.8% for white females,but for the Irish the rates were 5.8% and 6.8%,respectively. Of Caribbean males, 5.6% reporteddepressive neurosis as did 6.4% females, but only2.5% Indian males and 3.2% Indian females.Among Pakistanis, 3.8% males and 2.9% femalesand among Bangladeshis, 1.6% males and 2.2%females reported symptoms, which reached diag-nosis of depressive neurosis on Clinical InterviewSchedule (Revised) (CIS-R) interview. He foundthat, overall, migrants had much lower rates thannon-migrants. Yet among Pakistanis, non-migrants had the same rates as the equivalentwhite group. Those who were fluent in Englishreported the same rates as their British counter-parts. This, if taken as a proxy measure foracculturation, suggests that acculturated individu-als have the same levels of morbidity as a result ofdepression.
Possible causation of depression in migrants
Furnham and Bochner (15) identified eight theor-etical considerations for adjustment – these includ-ed movements such as loss, fatalism, selectivemigration, expectations, negative life events,social support, social skills deficit and clash ofvalues (see Table 1).The intergroup contact can lead to genocide,
assimilation, segregation and integration. It istherefore possible that levels of depression willvary across all these groups and processes. On anindividual level response can also vary and lead toa sense of alienation and isolation.
Table 1. Theoretical considerations of adjustment and their measurement (afterFurnham and Bochner (15))
Factors Measurements
Movement as loss and bereavementFatalism (locus of control) Locus of control scalesSelective migration Personality scalesExpectations Achievement–expectationsNegative life events LEI, LEDSSocial support Social support network
Social skills deficitClash of values Acculturation scales
Bhugra
68

Acculturation is the phenomenon by which theminority culture assimilates the values of majorityculture. This occurs when a group or a wholesociety adapts voluntarily or perforce the customs,value lifestyle and language of the majority culture.Pressures to assimilate can arouse strong feelings.The process of acculturation can occur at bothindividual and group levels and requires thecontact of at least two autonomous culturalgroups – there must be change in one or both ofthe groups. Four varieties of acculturation havebeen identified and these include assimilation,integration, rejection and deculturation. Assimil-ation is the process by which cultural differencesdisappear and a few generations later it is difficultto ascertain the differences between the twocultural groups. The areas of psychological func-tioning, which are related to acculturation, arelanguage, cognitive style, personality identity, atti-tudes and acculturate stress. Thus some individualsmay well be wary of giving up their culturalidentity voluntarily. Deculturation is the processby which the dominant culture denigrates theminority and is characterized by a sense of alien-ation, loss of identity and acculturative stress andmay lead to genocide if imposed by the largergroup. The individuals may reject the process andindividuals or groups may withdraw from thelarger society. When rejection is imposed by thedominant group it becomes a kind of segregation,leading to mutual distrust. Under these circum-stances it is likely that a sense of loss may lead todepression. It is possible that vulnerability todepression will also be influenced by individualpersonality factors. The individuals may feelsocially isolated and rejected, leading to lowself-esteem and thereby producing features ofdepression.
Culture shock
The concept of culture shock illustrates an experi-ence of the new culture as a sudden unpleasantfeeling that may violate expectations of the newculture and cause one to evaluate one’s own culturenegatively. Oberg (16) identified six aspects ofculture shock as strain; sense of loss and feelings ofdeprivation; rejection by and of members of newculture, confusion in role; role expectations, values,feelings and self-identity; surprise, anxiety disgustand indignation; and feelings of impotence.Furnham (17) argues that others have attemptedto improve upon Oberg’s (16) multifaceted defini-tion but have simply placed the emphasis on slightlydifferent problems – language, physical irritability,role ambiguity, etc. Furnham (17) points out that no
one has attempted to specify the relationshipsamong various facets of culture shock to prioritizetheir importance and to identify which groups aremore vulnerable than others. Bock (18) uses the term‘culture shock’ to describe an emotional reaction,which is consequent upon being able to understand,control andpredict behaviour,which appears to be abasic need.The lackof familiaritymaywell extend toclothes, etiquette, food and entertainment as well asaspects of social environment such as buildings andfunctions of buildings. Culture shock is thereforeseen as stress reaction, which involves uncertainsalient psychological and physical rewards. Themigrants thus remain anxious, confused and some-times apathetic or angry until some level of adjust-ment can be reached.Although culture shock is associated most often
with negative consequences, in some cases it mayactivate a manic defence leading to greater levels ofachievement. It may be seen as important for self-development and personal growth. It may be atransitional experience, which in the presence offactors such as high self-esteem, adequate socialsupport, appropriate achievement according toexpectation may produce a sense of achievementby overcoming a depressogenic situation.Within the field of study of cultural identity and
culture shock not enough attention has been paidto explaining individual responses in ascertainingwho will find the shock more intense and whethereducational and economic factors can be protect-ive. If the individual or group is aware of themajority culture in terms of language, etc. devel-opment of culture shock may be less likely.Similarly, actors, businessmen or diplomats maybe less likely to face culture shock compared withpoor political exiles who have been forced tomigrate.
Culture conflict
The concept of culture conflict is not new. Itrefers to the conflict which people coming fromthe same culture may face, especially if onemember is acculturated and the other is not. Itis often seen among adolescents who, while atschool, are able to follow the customs and moresof their peers but not at home with their parents.Such conflict has been associated with increasedrates of deliberate self-harm. The children mayhold more modern views compared with theirparents, who hold traditional views (19). Theconflict may contribute to a sense of isolation andabandonment, although there are few empiricaldata to suggest that culture conflict is associatedwith depression.
Migration and depression
69

Explanations of depression
Depression among migrants can be attributed to anumber of possible explanations. We shall discusssome of these explanations further below. Suffice itto say that a multi-axial aetiology, includingpsychobiosocial and additional anthropologicaland religio-spiritual aspects, must be taken intoaccount.
Psychoanalytical explanations
Mourning and melancholia are well described inthe psychoanalytical literature. A sense of loss,especially if the individual has not had an adequateopportunity to mourn that loss, is likely to lead todepression. Grief is ubiquitous and is a reaction tothe real or imagined loss of a significant object orrole, which may or may not be resolved, when anew object or personal relationship is established.Migration is linked with being deprived of specificobjects as well as specific relationships. Theseinclude family, friends, occupational status andother factors. The loss may be followed by griefand mourning. As bereavement behaviour variesacross different cultures, it would become difficultfrom the clinician’s perspective to identify thesefactors. Unresolved grief and prolonged mourningare likely to lead to depression. If the grief is notallowed to be expressed (which the new culturemay well look down upon), the internalization ofsuch a grief may lead to depression.Grief can be normal, exaggerated, abbreviated,
inhibited, anticipatory or delayed. It is not certainwhat specific factors determine the various patternsof grief. Clearly, the degree of attachment andresponse to loss will influence whether the individu-al becomes anxious or depressed. Bereavementexperienced by political exiles may be seen as aresult of loss of roots, changed geography, loss ofemotional support, loss of the cognitive world aswell as social and economic status prior to exile.Migration may well be an escape for someindividuals.
Cognitive theories
Cognitive models of depression include the depres-sive triad of ‘I am a failure’, ‘the world is bleak’and ‘the future is bleak’. However, as mentionedpreviously guilt may not be present in all cultures’models of depression, thereby making the universalapplicability of this triad difficult. The notions ofself-hood and illness differ across sociocentric andegocentric societies, therefore it is likely that theindividual cognitive schemata are and will be
different. The sense of loss in the context ofexternal locus of control and lack of social supportmay produce features of depression, which maynot be identified easily by clinicians.The cognitive schema among refugees may have
realistic components of persecution. Such paranoidor persecutory thoughts allow the individual todevelop a sense of isolation and alienation. Themost common psychiatric condition among refu-gees is depression. The time elapsed since migra-tion is another factor of which the researchers andclinicians must be aware. In Gilbert and Allen’s(20) model, among cognitive factors for depressionwork, defeat and a sense of entrapment were someof the key factors. A sense of entrapment wasdefined as being trapped in the area, which islinked with learned helplessness. In depressionentrapment may be a more appropriate hypothesis,especially if the pathway to flight is blocked by anumber of reasons. Arrested flight thus involvessuppression of exploration behaviour, submissivepostures, feeling cut off and severe demobilization,all of which can be seen among immigrants.Locus of control is defined as the belief which
the individual holds to perceive any event as beingcontingent upon his own behaviour or his ownrelatively permanent characteristics as internalcontrol or perceived as being the result of chance,fate or fortune or in the stars, so that the individualdoes not hold or feel any responsibility for theevent. Fatalism is thus the situation where indi-vidualism places the locus of control to be externalto the individual for whom, by and large, theindividual holds no responsibility, and such anattitude is related to the non-changeability ofresponsibility. The opposite of fatalism is instru-mentalism. Furnham and Bochner (15) suggestthat external locus of control or fatalism beliefs arerelated to poor mental health and lack of adapta-tion.It is possible that when the individuals accept
their fate they may become more accepting of theirstresses, thereby linking it with cognitions whichare less threatening. The fatalism of control explan-ations may explain the lower rates of reportedmental distress among Indian subcontinent immi-grants by virtue of their fatalistic beliefs. Negativelife events are associated with onset of depression –an association of fatalistic beliefs and negative lifeevents related to the process of migration itself canlead to depression, especially if social support ismissing or is inadequate.Selective migration and expectations are two
additional factors. Of these expectations, selectivemigration appears to be a superficially attractiveoption, suggesting that people who become
Bhugra
70

depressed after migration were prone to bedepressed due to biological or social factors inany case. It is superficially attractive because itexplains differential rates of depression acrossdifferent groups and can explain why selectedindividuals did or did not appear to be depressed.However, the idea of selection is not entirely clear.It is logical that those who are fittest to withstandthe process of migration and are aware of languageand new cultural norms are more likely to survivecompared with those who are likely to be depressedin any case. Psychologically and physically healthymigrants are less likely to become depressed inresponse to loss.Expectations of the new cultural setting are more
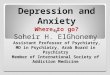
likely to play a role in the genesis of depressionif the individual does not reach the expected level ofachievement. A person’s behaviour is relateddirectly to the expectations that they hold and thesubjective value of the consequences that mightoccur following the action. High expectations thatcannot or do not become fulfilled may be related topoor adjustment and increased mental illness.A sense of alienation which may lead to depressionresults from a failure both to meet these expecta-tions and to reach the assimilation goals set by theindividual. People who migrate for economic rea-sons may well have higher expectations. Thus, lowexpectations may well be better for mental healthbut in turn will lead to poor social mobility, whichmay ignite other problems. A hypothetical modelbased on the above factors is illustrated in Fig. 1.The individual may well be vulnerable to
depression prior to migration and the stress ofmigration, if associated with sense of loss andnegative life events, may trigger depression. Suchan episode may also be associated with various
aspects of culture shock. Culture conflict andculture distance or alienation may add further tostress and vulnerability to depression. The cogni-tive triad of depression among migrant and refugeegroups may well be different, thereby allowingdepression to present in forms other than stan-dardized western perspectives.Protective factors in the genesis are not only
social support but positive helpful support, whichthe individual uses. This contributes to a sense ofacceptance and improved self-esteem and if asso-ciated with locus of control, in generating depres-sion avoidance factors. Individual, group andsocietal factors will all play a part in the genesisand perpetuation of depressive thought and symp-toms of depression.
Conclusions
Not all migrants will develop depression and notall depressives have history of migration. It is likelythat a certain degree of biological or psychologicalvulnerability, combined with social vulnerabilityafter migration, may lead to a sense of depression.Cultural identity changes may lead to cultureshock and cultural distance may contribute to assense of alienation and isolation, thereby leading todepression. It is possible that cognitive schema ofmigrants may differ depending upon their socialand cultural backgrounds. Culture shock and senseof real or perceived loss of family, family history,geography, social environment, etc. may contributeto the genesis of depression.
References
1. Shaw RP. Migration theory and fact: a review and bib-liography of current literature. Philadelphia, PA: RegionalSciences Research Institute, 1975.
2. Rack P. Race culture and mental disorder. London:Tavistock, 1982.
3. Bhugra D, Desai M, Baldwin D. Focus groups: implica-tions for primary and cross-cultural psychiatry. PrimaryCare Psychiatry 1997;3:45–50.
4. Kimura SD, Mikolashek P, Kirk S. Madness in paradise:psychiatric crises among newcomers in Honolulu. HawaiiMed J 1975;34:275–278.
5. Krupinski J. Sociological aspects of mental illness inmigrants. Soc Sci Med 1967;1:267–281.
6. Regier DA, Myers JK, Kramer M et al. NIMH Epidemio-logical Catchment Area Program. Arch Gen Psychiatry1984;41:934–941.
7. Schild E. The foreign students, as a stranger, learning thenorms of host-culture. J Soc Issues 1962;18:41–54.
8. Hopkins J, Malleson N, Sarroff I. Some non-intellectualcorrelates of success and failure among university students.Br J Sociol 1975;9:25–36.
9. Still R. Mental health in overseas students. Cited in:Furnham A. Adjustment of sojourners. In: Kim YY,
PsychologicalPre migration
GroupBiological migration voluntaryVulnerablility –Social skills deficitLocus of control
Negative life events MigrationBereavement
+
+
Culture Shock Post migration Culture identitySocial support Ethnic densitySelective migration –Achievement expectation
DEPRESSION
Fig. 1. Inter-relationship of factors.
Migration and depression
71

Gudykunst WB, eds. Crosscultural Adaptation. NewburyPark, CA: Sage, 1988.
10. Ward E. Some observations of the underlying dynamics ofconflict in a foreign student. J Am Coll Health Ass1967;10:430–440.
11. Babiker I, Cox J, Mitter P. The measurement of culturedistance and its relationship to medical consultations,symptomatology and examination performance of over-seas students at Edinburgh University. Soc Psychiatry1980;15:109–116.
12. Cochrane R. Mental illness in immigrants to England andWales: an analysis of hospital admissions 1971. SocPsychiatry 1977;12:25–35.
13. Cochrane R. The social causation of mental illness.London: Longman, 1983.
14. Nazroo J. Ethnicity and mental health. London: PSI, 1997.15. Furnham A, Bochner S. Culture shock. London: Routledge
1986.16. Oberg K. Culture shock: adjustment to new culture
environments practical. Pract Anthropol 1960;7:197–182.
17. Furnham A. Adjustment of sojourners. In: Kim YY,Gudykunst WB, eds. Cross-cultural adaptation. NewburyPark, CA: Sage, 1988.
18. Bock P, ed. Culture shock. New York: Knopf, 1970.19. Bhugra D, Bhui KS, Desai M et al. Asian cultural identity
schedule. Int J Meth Psych Res 1999;8:212–218.20. Gilbert P, Allan S. The role of defeat and entrapment
(arrested flight) in depression. Psychol Med 1998;28:585–595.
Bhugra
72