Embed Size (px)
Citation preview
yt
mtgtw
itmitd
dpstc(oefwtl
T
Editorial
e
rm
cb
mbdriclo
Mild Enteropathy Celiac Disease: AWolf in Sheep’s Clothing?
Although the remarkable variability of the clinical presen-tation of celiac disease has been apparent for many
ears,1,2 data are conflicting about whether degree of enteropa-hy correlates with severity of clinical symptoms.3,4 The intuitive
and logical assumption is that patients with greater degrees ofmucosal damage would manifest more severe symptoms,whereas patients with milder degrees of mucosal damage wouldhave a milder clinical course. However, this is not always thecase.3 In fact, the factors that influence disease severity are
ultifactorial in nature, and the psychosocial factors, in par-icular, play an important role in determining the severity ofastrointestinal symptoms and health-related quality of lifehat is independent of the histologic disease activity in patientsith celiac disease.5
Mild enteropathy celiac disease (CD) is characterized by aMarsh 1 or 2 lesion on small intestinal biopsy without villousatrophy in patients clinically suspected of having CD largely onthe basis of positive serologic tests including endomysial anti-bodies (EMAs), tissue transglutaminase antibodies (tTGs), ordeamidated gliadin peptide antibodies (DGPs).6 With increas-ng physician awareness of CD and use of modern serologicests, duodenal biopsy is increasingly performed, and as a result,
ild enteropathy has become a common finding. For example,n a large population-based study in Sweden, the authors foundhat about one-third of the patients had Marsh 1 and 2 mucosalamage.7 The mean prevalence of mild enteropathy CD from
other published articles is 24.6%, with a range of 10%–37%.6,8 –11
Interestingly, one study from Spain reported on a prevalence ofMarsh 1 and 2 lesions that was as high as 67.5%.12
Recognition of this cohort of patients with milder forms ofenteropathy raises a number of important questions. What isthe natural history of disease progression in this group? Shouldthese patients be universally placed on a gluten-free diet (GFD),and will this mitigate symptoms, improve quality of life, orreduce their risk of malignancy? Currently, there are no firmguidelines about starting a GFD in patients with positive celiacantibodies and mild enteropathy without villous atrophy inadults.13,14
In this issue of Clinical Gastroenterology and Hepatology, Zaniniand colleagues15 assess whether the severity of small intestinal
amage is associated with clinical and laboratory indexes inatients with CD. The authors conducted a retrospective cohorttudy of 1408 adult patients diagnosed clinically with CD onhe basis of symptoms and positive serology. Patients werelassified into 2 groups, one with duodenal villous atrophyMarsh 3) and the second with mild enteropathy. Mild enter-pathy CD constituted 11% of the study cohort overall. Inter-stingly, the proportion of patients in this group increasedrom 2% in 1991–1995 to 10% in 1996 –2000, 12% in 2001–2005hen the cutoff for intraepithelial lymphocytes was �40, and
o 15% thereafter with a lower cutoff of �25 intraepithelialymphocytes.
A number of interesting findings emerge from this study.
he authors clearly demonstrate that patients with mild enter-C
opathy CD do manifest nutritional deficiencies such as anemia,low ferritin levels, vitamin B12 and folate deficiencies, hypocal-cemia, and hyperparathyroidism. However, in general these de-ficiencies are milder compared with those with villous atrophy.These findings are in line with various other studies.6,9,12,16 Forxample, in a randomized controlled study by Kurppa et al,6 the
baseline hemoglobin, iron, vitamin B12, and folate levels werehigher in patients with mild enteropathy CD compared withthose with Marsh 3 mucosal damage. Another finding from thecurrent study is that patients with mild enteropathy tended tohave a higher body mass index and were more likely to beoverweight at initial diagnosis compared with patients withvillous atrophy. Similar findings have been seen in several otherstudies6,9,12 and are of particular concern because of recenteports of significant increases in body mass index with treat-
ent of CD.17
Metabolic bone disease such as osteopenia or osteoporosis isanother common presentation of both mild enteropathy andCD. In the current study, the authors report that only 5% ofpatients with mild enteropathy CD had abnormal bone mineraldensity (BMD) results compared with 22% of patients withvillous atrophy (P � .0005). However, BMD data were availablefor only a relatively small proportion of patients in bothgroups. Nonetheless, these findings are supported by a recentlypublished article that found a direct association between degreeof enteropathy and BMD.12 The prevalence of osteopenia orosteoporosis in mild enteropathy overall has been reported tobe between 18.8%–58%, which is significant but consistentlylower than is found in cohorts with CD and villous atro-phy.6,12,18 Because the overall fracture risk for CD is only in-reased by roughly 30%,19 it is not surprising that the degree ofone loss and risk of fracture are low in mild enteropathy CD.12
From all these data, it is tempting to conclude that mildenteropathy CD differs minimally from classic CD with villousatrophy. However, it is worth remembering that all patients inthe current study were diagnosed with CD on the basis ofclinical suspicion and serology results. Mild enteropathy, in theabsence of positive celiac serologies, has broad differential,20
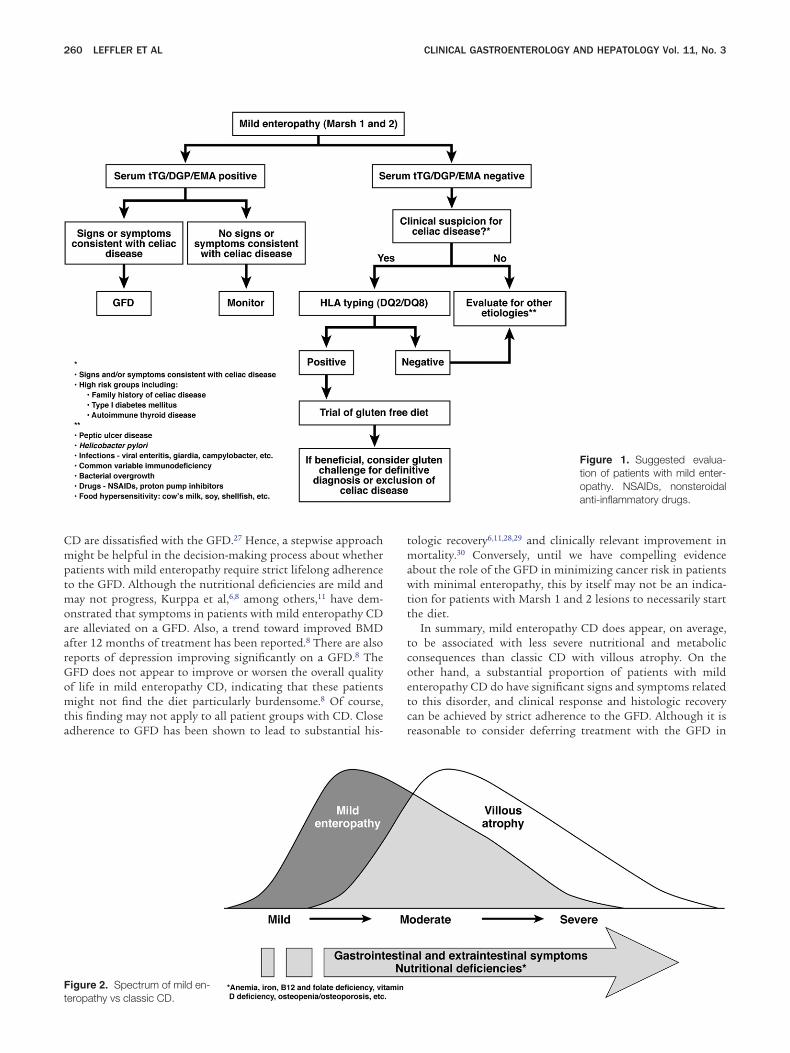
and identifying the correct diagnosis and treating the underly-ing cause are the necessary initial actions (Figure 1). Althoughthe sensitivity of serologic testing is questionable in patientswith Marsh 1 and 2 lesions,10,21 Biagi et al22 showed that
inimal intestinal lesions in the absence of endomysial anti-odies are most often unrelated to CD. If CD is still consideredespite negative serologic testing, HLA testing is generally war-anted. It is also notable that the spectrum of histologic lesionsn CD is a continuum (Figure 2). Continuous gluten exposurean lead to histologic progression from Marsh 1 to Marsh 3esions,6,18 and persistent mucosal damage is associated with anverall increased mortality even in the absence of symptoms.7
We also know that histologic severity in CD can be patchy,23,24
and mild enteropathy in one area does not preclude the exis-tence of villous atrophy in another. Finally, the long-term ab-solute risk of malignancy in patients with Marsh 1 and 2 lesionsis small compared with villous atrophy, but it is a real risk,nonetheless.25,26
Therefore, should all patients with mild enteropathy CD be
placed on a GFD? In fact, a large proportion of patients withLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2013;11:259–261
mptmoaa
Gomta
t
260 LEFFLER ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 11, No. 3
CD are dissatisfied with the GFD.27 Hence, a stepwise approachight be helpful in the decision-making process about whether
atients with mild enteropathy require strict lifelong adherenceo the GFD. Although the nutritional deficiencies are mild and
ay not progress, Kurppa et al,6,8 among others,11 have dem-nstrated that symptoms in patients with mild enteropathy CDre alleviated on a GFD. Also, a trend toward improved BMDfter 12 months of treatment has been reported.8 There are also
reports of depression improving significantly on a GFD.8 TheFD does not appear to improve or worsen the overall qualityf life in mild enteropathy CD, indicating that these patientsight not find the diet particularly burdensome.8 Of course,
his finding may not apply to all patient groups with CD. Closedherence to GFD has been shown to lead to substantial his-
Figure 2. Spectrum of mild en-
eropathy vs classic CD.tologic recovery6,11,28,29 and clinically relevant improvement inmortality.30 Conversely, until we have compelling evidenceabout the role of the GFD in minimizing cancer risk in patientswith minimal enteropathy, this by itself may not be an indica-tion for patients with Marsh 1 and 2 lesions to necessarily startthe diet.
In summary, mild enteropathy CD does appear, on average,to be associated with less severe nutritional and metabolicconsequences than classic CD with villous atrophy. On theother hand, a substantial proportion of patients with mildenteropathy CD do have significant signs and symptoms relatedto this disorder, and clinical response and histologic recoverycan be achieved by strict adherence to the GFD. Although it isreasonable to consider deferring treatment with the GFD in
Figure 1. Suggested evalua-tion of patients with mild enter-opathy. NSAIDs, nonsteroidalanti-inflammatory drugs.

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
March 2013 MILD ENTEROPATHY CELIAC DISEASE 261
patients not yet manifesting signs and symptoms consistentwith CD, in general, data at this time support treatment ofpatients with CD regardless of the degree of enteropathy. Fu-ture research should be geared toward prospective population-based studies in determining the role of the GFD in mildenteropathy CD in relation to morbidity and mortality includ-ing cancer risk. Such data would add significantly to our clin-ical decision-making abilities about whether to routinely rec-ommend the GFD in this population. Until then, it would be areasonable option to recommend a GFD in mild enteropathyCD when the benefits to the patient overweigh the burden ofadherence to the diet.
DANIEL LEFFLER, MD, MSROHINI VANGA, MBBS, MD
RUPA MUKHERJEE, MDThe Celiac Center
Division of GastroenterologyBeth Israel Deaconess Medical Center
Boston, Massachusetts
References
1. Fasano A. Celiac disease: how to handle a clinical chameleon.N Engl J Med 2003;348:2568–2570.
2. Reilly NR, Green PH. Epidemiology and clinical presentations ofceliac disease. Semin Immunopathol 2012;34:473–478.
3. Brar P, Kwon GY, Egbuna II, et al. Lack of correlation of degree ofvillous atrophy with severity of clinical presentation of coeliacdisease. Dig Liver Dis 2007;39:26–32.
4. Tursi A, Brandimarte G, Giorgetti GM, et al. Endoscopic featuresof celiac disease in adults and their correlation with age, histo-logical damage, and clinical form of the disease. Endoscopy2002;34:787–792.
5. Dorn SD, Hernandez L, Minaya MT, et al. Psychosocial factors aremore important than disease activity in determining gastrointes-tinal symptoms and health status in adults at a celiac diseasereferral center. Dig Dis Sci 2010;55:3154–3163.
6. Kurppa K, Collin P, Viljamaa M, et al. Diagnosing mild enteropathyceliac disease: a randomized, controlled clinical study. Gastroen-terology 2009;136:816–823.
7. Ludvigsson JF, Montgomery SM, Ekbom A, et al. Small-intestinalhistopathology and mortality risk in celiac disease. JAMA 2009;302:1171–1178.
8. Kurppa K, Collin P, Sievänen H, et al. Gastrointestinal symptoms,quality of life and bone mineral density in mild enteropathiccoeliac disease: a prospective clinical trial. Scand J Gastroen-terol 2010;45:305–314.
9. Dickey W, Hughes DF, McMillan SA. Patients with serum IgAendomysial antibodies and intact duodenal villi; clinical charac-teristic and management options. Scand J Gastroenterol 2005;40:1240–1243.
0. Licata A, Cappello M, Arini A, et al. Serology in adults with celiacdisease: limited accuracy in patients with mild histological le-sions. Intern Emerg Med 2012;7:337–342.
1. Tursi A, Brandimarte G. The symptomatic and histologic re-sponse to a gluten-free diet in patients with borderline enterop-athy. J Clin Gastroenterol 2003;36:13–17.
2. García-Manzanares A, Tenias JM, Lucendo AJ. Bone mineral densitydirectly correlates with duodenal Marsh stage in newly diagnosed adultceliac patients. Scand J Gastroenterol 2012;8-9:927–936.
3. Hill ID, Dirks MH, Liptak GS, et al. Guideline for the diagnosis and
treatment of celiac disease in children: recommendations of the NorthAmerican Society for Pediatric Gastroenterology, Hepatology andNutrition. J Pediatr Gastroenterol Nutr 2005;40:1–19.
4. Ludvigsson JF, Green PH. Clinical management of coeliac dis-ease. J Intern Med 2011;269:560–571.
5. Zanini B, Caselani F, Magni A, et al. Celiac disease with mildenteropathy is not mild disease. Clin Gastroenterol Hepatol2013;11:253–258.
6. Taavela J, Kurppa K, Collin P, et al. Degree of damage to the smallbowel and serum antibody titers correlate with clinical presentation ofpatients with celiac disease. Clin Gastroenterol Hepatol 2013;11:166–171.
7. Kabbani TA, Goldberg A, Kelly CP, et al. Body mass index and therisk of obesity in coeliac disease treated with the gluten-free diet.Aliment Pharmacol Ther 2012;35:723–729.
8. Wahab PJ, Crusius JB, Meijer JW, et al. Gluten challenge inborderline gluten-sensitive enteropathy. Am J Gastroenterol2001;96:1464–1469.
9. West J, Logan RF, Card TR, et al. Fracture risk in people withceliac disease: a population-based cohort study. Gastroenterol-ogy 2003;125:429–436.
0. Bao F, Green PH, Bhagat G. An update on celiac disease histo-pathology and the road ahead. Arch Pathol Lab Med 2012;136:735–745.
1. Tursi A, Brandimarte G, Giorgetti GM. Prevalence of antitissue transglu-taminase antibodies in different degrees of intestinal damage in celiacdisease. J Clin Gastroenterol 2003;36:219–221.
2. Biagi F, Bianchi PI, Campanella J, et al. The prevalence and thecauses of minimal intestinal lesions in patients complaining ofsymptoms suggestive of enteropathy: a follow-up study. J ClinPathol 2008;61:1116–1118.
3. Weir DC, Glickman JN, Roiff T, et al. Variability of histopatholog-ical changes in childhood celiac disease. Am J Gastroenterol2010;105:207–212.
4. Murray JA, Rubio-Tapia A, Van Dyke CT, et al. Mucosal atrophy inceliac disease: extent of involvement, correlation with clinicalpresentation, and response to treatment. Clin GastroenterolHepatol 2008;6:186–193.
5. Elfström P, Granath F, Ekström Smedby K, et al. Risk of lym-phoproliferative malignancy in relation to small intestinal histo-pathology among patients with celiac disease. J Natl Cancer Inst2011;103:436–444.
6. Elfström P, Granath F, Ye W, et al. Low risk of gastrointestinalcancer among patients with celiac disease, inflammation, orlatent celiac disease. Clin Gastroenterol Hepatol 2012;10:30–36.
7. Aziz I, Evans KE, Papageorgiou V, et al. Are patients with coeliacdisease seeking alternative therapies to a gluten-free diet? JGastrointest Liver Dis 2011;20:27–31.
8. Kaukinen K, Mäki M, Partanen J, et al. Celiac disease withoutvillous atrophy: revision of criteria called for. Dig Dis Sci 2001;46:879–887.
9. Tursi A, Brandimarte G, Giorgetti GM, et al. Endoscopic andhistological findings in the duodenum of adults with celiac dis-ease before and after changing to a gluten-free diet: a 2-yearprospective study. Endoscopy 2006;38:702–707.
0. Rubio-Tapia A, Rahim MW, See JA, et al. Mucosal recovery andmortality in adults with celiac disease after treatment with agluten-free diet. Am J Gastroenterol 2010;105:1412–1420.
Conflicts of interestThis author discloses the following: Dr Daniel Leffler has research
support from and consulted for the following companies: PrometheusLaboratories, Shire Pharmaceuticals, Alvine Pharmaceuticals, andAlba Therapeutics. The remaining authors disclose no conflicts.
http://dx.doi.org/10.1016/j.cgh.2012.11.005