Embed Size (px)
Citation preview



Mindfulness-Based Cognitive Therapy for distressed cancer patientsClinical relevance and therapeutic alliance

ISBN / EAN 978 94 6284 200 7Layout and cover design Bas Reijnen en Henriëtte JansenEditor Bas ReijnenTranslation The translation of the Dutch summary was assisted by Gerard Scanlan Printing Ipskamp Printing
This PhD research was funded by a grant from Pink Ribbon – a label by the Dutch cancer Society (KWF Kankerbestrijding), grant no. PR2012.WO.c153, The Netherlands.
Copyright @ 2019 by Else Maria Bisseling, Nijmegen, The Netherlands. All rights reserved. Any unauthorized reprint or use of this material is prohibited. No part of this thesis may be reproduced, stored of transmitted in any form or by any means, without written permission of the author or, when appropriate, of the publishers of the publications.

Mindfulness-Based Cognitive Therapy for distressed cancer patients
Clinical relevance and therapeutic alliance
Proefschrift ter verkrijging van de graad van doctoraan de Radboud Universiteit Nijmegen
op gezag van de rector magnificus prof. dr. J.H.J.M. van Krieken,volgens besluit van het college van decanen
in het openbaar te verdedigen op
donderdag 21 november 2019om 16.30 uur precies
door
Else Maria Bisseling
geboren op 27 juli 1973te Nijmegen

‘Although seldom explicitly recognized, connexional experience is basic to medical care. Awareness of this dimension of experience leads
clinicians to appreciate that establishing a therapeutic relationship is one of the principal goals of medical practice. It also reframes the doctor’s task to make clinical uncertainty more tolerable and
situations in which there is no appropriate biomedical response (such as care of the terminally ill) less frustrating and more fulfilling.’
(Suchman and Matthews 1988)
Promotor Prof. dr. A.E.M. Speckens Copromotoren dr. M.L. van der Lee (Helen Dowling Instituut) dr. M.P.J. Schellekens (Helen Dowling Instituut)
Manuscriptcommissie Prof. dr. J.H.W. de WiltProf. dr. N. HoogerbruggeProf. dr. I.M. Verdonck-de Leeuw (Amsterdam umc)
ParanimfenTanya BisselingMaike Bisseling

Opgedragen aan Sam Nanne & Merijn

In herinnering aanJan & Rianne
Voor Rianne
I was just guessing at numbers and figuresPulling your puzzles apart
Questions of science, science and progressDo not speak as loud as my heart
(Coldplay, The Scientist)

Contents
9 chapter 1 Introduction
27 chapter 2 Study protocol of a multicenter randomized controlled trial comparing the effectiveness of group and individual internet-based Mind-fulness-Based Cognitive Therapy with treatment as usual in reducing psy-chological distress in cancer patients: the BeMind study.
bmc Psychology (2015): 13;3:27
49 chapter 3 Face-to-face and individual internet-based Mindfulness-Based Cognitive Therapy compared to Treatment As Usual in reducing psychological distress in cancer patients: a multicentre randomized controlled trial
Journal of Clinical Oncology (2018): 10;36(23):2413-2421
73 chapter 4 Therapeutic alliance – not therapist competence or group cohesion – contributes to reduction of psychological distress in group-based Mindfulness-Based Cognitive Therapy for cancer patients.
Clinical Psychology & Psychotherapy (2019): 26(3):309-318
95 chapter 5 Development and Association of Therapeutic Alliance With Outcome of Internet-Based Mindfulness-Based Cognitive Therapy for Dis-tressed Cancer Patients: Secondary Analysis of a Multicenter Randomized Controlled Trial.
Journal of Medical Internet Research (2019): 21(9), e14065
117 chapter 6 Mindfulness-Based Stress Reduction for breast cancer patients: A mixed method study on what patients experience as a suitable stage to participate.
Supportive Care in Cancer (2017): 25(10):3067-3074
135 chapter 7 Summary and general discussion
addenda158 Nederlandse samenvatting178 Dankwoord183 Curriculum Vitae184 List of publications187 Data management statement188 Donders Graduate School for Cognitive Neuroscience


Chapter 1
Introduction

10
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Psychological distress in cancer Patients
From 2025 onwards, 20 million people worldwide will be diagnosed with cancer each year.1 The invasive treatment and physical burden have a major impact on patients’ wellbeing. The mental burden is commonly described as distress. The National Comprehensive Cancer Network (NccN) defines distress as: ‘A multifac-torial unpleasant emotional experience of a psychological (cognitive, behavioral, emotional), social and/or spiritual nature that may interfere with the ability to cope effectively with cancer, its physical symptoms and its treatment. Distress extends along a continuum ranging from common feelings of vulnerability, sadness and fears to problems that can become disabling such as depression, anxiety, panic, social isolation and existential and spiritual crisis’.2 About one third of all cancer patients suffer from psychological distress3 resulting in reduced quality of life, decreased compliance with medical care and prolonged duration of hospital stay.4 These psychological consequences of cancer or anticancer treatment seem to last up to months or even years after diagnosis and anticancer treatment.5
According to The Dutch Oncology Guidelines (www.oncoline.nl) all oncological patients should be screened for psychological distress or wish for psychological support. Special attention should be paid to people at risk for distress or high care need. Early recognition and subsequent referral of patients who develop psychological distress or problems as a result of the confrontation with cancer could improve the quality of these patients’ lives, and subsequently the satisfaction with (medical) care and communication with the primary health care providers.6 According to the guidelines there is a high probability of under-diagnosis of dis-tress and consequently under-treatment without systematic screening.
Psychiatric disorders in cancer Patients
In 30-40 % of cancer patients, the psychological distress is so severe that it meets the criteria of an anxiety or depressive disorder.4 Especially in the early treatment phase, affective disorders are often present.7 In a large population based sample (n=4020), cancer patients were more likely to have a depressive disorder than those in the general population.8 In a sample of breast cancer patients (n=24.537), over one third of the patients developed a depressive disorder within 5 years of diagnosis.9 However, in the long term anxiety rather than depression is the most likely problem for cancer survivors.5 Both anxiety and major depression have been related to over- and underutilization of oncology care10, 11 lower quality of life12, 13
and shortened survival time.14-16
Although 30-40% of cancer patients develop psychiatric disorders4, 17 and a further

11
15-25% present with other clinically relevant conditions like anxiety, demoraliza-tion or general psychological distress18, 19 less than 30% of them are recognized by oncology health professionals and referred to mental health or psycho-oncology services. So, a lot of distressed cancer patients remain untreated20, 21 while inter-ventions like counseling and psycho-education, and psychological treatments like group or individual cognitive behavioral, psychodynamic or existential therapy have been developed for this population and are available.21, 22
Psycho-oncological interventions
Psychological interventions have been demonstrated to be effective in reducing symptoms of psychological distress and affective disorders in cancer patients23-25 a lot of them based on Cognitive Behavioral Therapy (cBT) principles. cBT focus-es on interaction between thoughts, feelings and behaviors. It is a collaborative, problem-focused therapy with a pragmatic and structured approach to managing psychological problems. However, as traditional cBT techniques are generally based on the premise that anxious or depressive individuals have unrealistic appraisals of negative outcomes26, it is not always compatible with the realistic fears of disease progression, disability, and death in (advanced) cancer.27 cBT approaches adapted for cancer patients are based on the premises that psychological responses to cancer depend mainly on how a person views cancer and one’s coping ability.28
A maladaptive cycle of coping (appraised threat, a helpless coping response) is a risk for development of psychological distress and affective disorders.29 In recent meta analyses cBT approaches adapted to cancer patients have been demonstrated to be effective in reducing psychological distress.30-33 Individual cBT approaches outperformed group approaches.30 Depressed breast cancer patients after surgery32 and patients with early-stage breast cancer with anxiety symptoms33 treated with cBT techniques had significant less distress compared to control groups. For adults diagnosed with cancer who had comorbid elevated depressive symptoms or a depression diagnosis (n=1362), meta-analytic findings revealed reliable positive effects of psychotherapeutic and pharmacologic interventions, with some advantage for cBT compared to problem solving therapies.31 Challenging the veracity of fearful cognitions (e.g., cognitive restructuring), however, may not be successful for those patients whom a recurrence may indeed have elevated probability.34 cBT might not be suitable for a subgroup of patients who are continually re-exposed to external triggers as a result of their ongoing care.34, 35 Considering the rising prevalence of people living with (advanced) cancer,1 the absolute number of patients in need of psychological treatment is expected to increase. Addressing the increasing need for mental support, calls for innovative and effective psychological treatment options.
chapter 1

12
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Mindfulness-based interventionsMindfulness-Based Interventions (mBIs), such as Mindfulness-Based Stress Reduc-tion (mBSR)36 and Mindfulness-Based Cognitive Therapy (mBcT)37 are effective psychological treatment options and have increasingly been applied in somatic health care, including oncology. Mindfulness is defined as intentionally paying attention to present-moment experiences in an accepting and non-judgmental way.38 Traditionally, mBIs consist of 8-weekly f2f group-based 2.5-hour sessions, a 6-hour silent day between sessions 6 and 7, and daily 45-minute home practice. Each session consists of mindfulness practices, didactic teachings, and sharing experiences. mBSR was originally developed for patients with chronic somatic
Figure 1 Rationale for Mbct to reduce fear of cancer recurrence
Patients CharacteristicsDemographics (age, sex)
Medical factors (cancer stage, comorbidity)Psychosocial factors (neuroticism, support)
TriggersInternal somatic cues (pain, bumps)
External clues (medical visits, hearing about cancerLegitimate medical symptoms
Cognitive ReactivityCatastrophic thoughts
Worry, ruminationCognitive de-centeringCognitive reappraisal
Illness BeliefsRecurrence is likely
Recurrence = quick and painful death
Cognitive de-centering
Safety-Seeking BehavioursReassurance-seeking
Excessive body checkingAvoidance of medical visitis
Distress tolerance
Anxiety and UncertaintyAdditional physical symptoms
Urge to reduce anxiety, gather information
Anxiety reduction (e.g., relaxation)Tolerance of Uncertainty
Misperceive Bodily SymptomsAmbiguous but harmless symptoms
perceived as sign of recurrence
Non-judgementalbody awareness
Body VigilanceAttentional bias toward
physical symptoms
Attention regulation

13
conditions to help them cope more effectively with their condition, by increasing the capacity to focus on present-moment experiences, even in the presence of internal discomfort. mBcT combines mBSR with cBT elements and was originally developed to prevent relapse in patients with recurrent major depressive disorders.37 More recently, it has been applied in other conditions.39 A 2012 meta-analysis of nine randomized controlled trials (RcTs) (n=955) of mBIs in cancer patients found significant improvements in depressive and anxiety symptoms.40 Since then, a number of RcTs have replicated the reduction of distress following mBIs.41-45 Luberto et.al (2019) posted a theoretical rationale for mBcT to reduce symptoms of fear of cancer recurrence (figure 1), based on a model of Abramowitz et al. for anxiety,46 which can be seen as a blueprint for mBcT to reduce psychological dis-tress in cancer patients.
internet based Psycho-oncological interventions
For good reason, the integration of distress screening and psychological support in routine oncology practice is widely recommended.47 However, it has been found that uptake of face to face (f2f ) psychological interventions for cancer patients has been lower than, for instance, telephone-based interventions.48 Patients may have difficulties with interventions that demand attendance due to functional impairments, side-effects such as fatigue, and limited transportation options49
Internet-based interventions (IBIs) could be an alternative. Evidence of over 100 well-controlled trials suggests that internet-based treatments can be as effective as face-to-face psychological treatments for a wide range of psychiatric and somatic conditions. Effects were enhanced by the guidance of a therapist.50, 51
internet-based Mindfulness-based interventionsTraditional mBIs typically require in-person attendance at a series of classes over several weeks. In contrast, internet-based mindfulness based interventions (emBIs) are easily accessible, available and save travelling time.52 A recent review of 15 RcTs on emBIs demonstrated a small but significant beneficial impact on depression, anxiety, well-being and mindfulness. The largest effect was found for stress, with a moderate effect size. For stress and mindfulness, exploratory subgroup analyses indicated that guided emBIs had higher effect sizes than unguided emBI.52
Evidence for emBIs in cancer is scarce, one single controlled study investigated the quantitative feasibility of internet-based mBSR for cancer patients (Mindful-ness-Based Cancer Recovery (mBcR)) and found synchronous videoconferencing sessions led to significant improvements in mood, stress symptoms and mind-fulness skills.49 Individual emBcT was found to significantly reduce fatigue and psychological distress in severely fatigued cancer patients.53 In an RcT of severely
chapter 1

14
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
fatigued cancer survivors, participants (n=167) were randomized to an ambulant activity feedback program (AAF), therapist guided emBcT or unguided active control condition. Fatigue severity decreased significantly more in the AAF and emBcT groups compared to the psycho-educational group. Dropout was 38% in emBcT, mainly due to the perceived high intensity of the program.54
theraPeutic asPects in ( internet- based) Psychological interventions
The effectiveness of any psychological intervention depends on the skill or com-petence of the therapists,55 the strength of the established therapeutic relationship or therapeutic alliance47, 56 and the cohesiveness in group-based therapy.57
Therapist competence refers to the level of skills shown by the therapist in delivering the treatment and includes the consideration of and response to relevant contextual variables.55, 58 Therapist competence has been shown to be associated with positive symptom change in difference types of psychotherapy, including cBT, for patients with depressive and anxiety disorders.59-62 However, a recent large study (n=1247) including 43 cBT therapists in routine clinical practice could not confirm this association on outcome.63
Therapeutic alliance is described as the collaborative and affective bond between therapist and patient defined as how closely patient and therapist agree on goals of treatment, how to reach the treatment goals and the degree of mutual trust between patient and therapist.64, 65 According to recent meta-analyses, for 10-15% of the therapeutical change in psychological interventions can be attributed to the quality of the therapeutic alliance.66, 67 Therapeutic alliance has been found to predict outcome equally well in cBT, psycho-dynamic and experiential therapies68, 69 and may also reduce the risk of dropout.70
A systematic review on the development of the therapeutic alliance in IBIs indicated this to be equivalent in f2f therapy.71 In addition, Reynolds found that clients (n=30) and therapists (n=30) rated their session impact and alliances in online-text psychotherapy as strong as previously found in f2f psychotherapy.72 With regard to the association between therapeutic alliance and outcome in cancer patients, however, findings are mixed. In telephone assisted cBT for a sample of cancer survivors (n=46), a strong therapeutic alliance predicted depressive symptom reduction.73 In other studies of IBIs no significant association between treatment outcome and the therapeutic alliance has been found.74, 75
Group cohesion primarily refers to social-emotional cohesion: the intimacy, rec-iprocity and emotional disclosure that is felt among group members,57 contributing to the cooperation within the group to achieve a common therapeutic aim.76 It is presumed that when cohesion is high, the group is motivated to perform well and

15
is more able to carry out activities for successful performance.77 Research on the role of group cohesion in psychotherapy has shown that higher dimensions of group cohesion predict better treatment outcome.78-80 Research on the impact of group cohesion in interventions for cancer patients is scarce. In a group based rehabili-tation program for cancer survivors, dimensions of group cohesion seemed to be associated with intervention outcome.81 It was suggested that a subgroup of breast cancer patients, scoring high on bonding dimensions and being vulnerable for social comparison, should be protected from contact with fellow patients in a support group, as this was associated with reduced quality of life after the intervention.82
therapeutic aspects in ( internet-based) Mindfulness-based interventions
Therapist competence is highly valued in the clinical practice of teaching mBcT.83, 84 The therapists’ role is different in mBcT compared to cBT. In mBcT therapist embodiment is considered to very important. Dobkin et al. (2014) describe embod-iment as ‘the quality of instantiating into one’s being, actions and phenomeno-logical experience the skills that are cultivated through mindfulness practice’.85 Moreover, in mBcT the therapist is mainly focused on facilitating patients’ self- efficacy, without too much emphasis on exploring personal narratives. General skills that mindfulness therapists should share are formulated as four skills sets; 1) stewardship of the group; 2) the delivery of didactic materials; 3) guidance of formal and informal practices and 4) inquiry into participants direct experience.86 To evaluate therapist competence the Mindfulness-Based Interventions-Teachers Assessment Criteria (mBI:TAc)87 has been developed. The mBI:TAc is the first and most widely used tool to assess mindfulness-based teaching competence. The mBI:TAc consists of six domains: 1) organization; 2) relational skills; 3) embodi-ment of mindfulness; 4) guiding mindfulness practices; 5) didactical skills and 6) group environment. These domains consist of three to five key qualities which are scored at six competence levels: incompetent (1), beginner (2), advanced beginner (3), competent (4), proficient (5), and advanced (6). Only one multicenter study on mBcT for recurrent depression (n=241) focused on the role of therapist competence.87 In this study, no robust association between therapist competence and treatment outcome was found.88 In addition, a study on the impact of therapists’ training on participant outcome in mBSR (n=52) showed no significant relationship between therapists’ experience (not competence) and participants experienced mindfulness or wellbeing, yet did find a significant association between therapists’ experience and participants’ satisfaction with the course.89 Regarding the extent to what therapists experience barriers in embodying mindfulness via internet, qualitative findings revealed that therapists seemed more concerned about communicating mindfulness values in emBcT than patients.90
chapter 1

16
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Therapeutic alliance has been investigated intensively in psychotherapy, however, only one study in diabetic patients with depression examined the relationship between therapeutic alliance and treatment outcomes in mBcT. Comparing indi-vidual cBT with individual mBcT (n=76), findings showed that therapeutic alliance predicted outcomes of individual cBT but not of individual mBcT.91 To date, no studies have been conducted on the association of therapeutic alliance and out-come in group-based mBcT or emBcT for cancer patients. Qualitative findings revealed that participating in a group was experienced as motivating, resulting in a less dependent relationship with the therapist.92
To our knowledge there are no previous quantitative studies on the impact of group cohesion in mBIs, whether in cancer patients or in different settings. Only one study showed that social support partly mediated the effect of group Mindful-ness-Based Cancer Recovery (mBcR) on mood disturbance and stress symptoms.93 Qualitative studies showed that group-based settings in mBIs had added value to cancer patients in terms of feeling connected, accepted and experiencing trust, which in turn, facilitated learning processes, such as acknowledging emotions and gaining different perspectives.92, 94, 95 Moreover, it was found that participating in a group is experienced as a motivating factor for completing the therapy.92
timing
As anticancer treatment poses a burden on patients mental and physical wellbeing96, 97 it can interfere with participation in psychological treatments . When patients miss several sessions, the intervention might not be as effective. However, qualitative research findings suggested that prostate cancer patients on active anticancer treatment preferred individual support.98 Moreover, qualitative findings on timing of delivery of internet cBT (icBT) for anxiety and depression in cancer patients (n=15) showed that participants, considered icBT acceptable and potentially useful from the time of cancer diagnosis to post-treatment.99 More interestingly, a recent meta-analysis on uptake and adherence of psychological interventions for cancer patients demonstrated that patients were more likely to accept an intervention close to their diagnosis and before the start of anticancer treatment.100
tiMing of Mindfulness-based interventionsIn clinical practice and research settings, with a few exceptions,101 mBIs are offered after the active anticancer treatment phase,102-105 despite the knowledge that psycho-logical distress can be particularly high in the first year of diagnosis and during anticancer treatment.106, 107 So far, little is known about what patients themselves experience as the most suitable time to participate in mBIs.

17
Unraveling the underlying therapeutic factors will add to our knowledge about how to best deliver mBIs, in both f2f and online applications. This knowledge is of great importance for the implementation of scientific findings in clinical practice. Aspects as therapist competence, therapeutic alliance group cohesion, or other treatment delivery factors such as timing of the intervention can play an important role in patients’ adherence to therapy or outcomes of mBIs. As the focus of research activities in the mBI field has so far mainly been on the development of mBIs for specific populations , time has come to pay more attention to factors like competence, alliance and timing as possible working mechanisms of mBIs.108
aims of the thesis
The primary aim of this thesis is to investigate the effectiveness of emBcT and mBcT in reducing psychological distress in cancer patients. The secondary aim is to unravel underlying possible therapeutic factors, such as therapist competence, therapeutic alliance, group cohesion and timing. The following specific questions will be addressed:
1. We will conduct a multicenter Randomized Controlled Trial to investigate whether both group-based mBcT and emBcT are superior to Treatment As Usual (TAu) in reducing psychological distress in a sample of distressed heterogeneous cancer patients.
Are embcT and mbcT more effective compared to TAU in reducing psychological distress in cancer patients?
2. Subsequently, we will study the possibly predictive role of therapeutic factors (therapist competence, therapeutic alliance and group cohesion) on reduction of psychological distress after group-based mBcT. Additionally, we will examine whether therapist competence facilitates a strong therapeutic alliance and high group cohesion.
Are group cohesion, therapeutic alliance and therapist competence associated with outcome of mbcT for distressed cancer patients?
3. Furthermore, we will study the development of therapeutic alliance in emBcT compared to group-based mBcT.
Can therapeutic alliance become stronger in both embcT and mbcT and is early alliance associated with outcome of (e)mbcT?
chapter 1

18
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
4. Finally, we will examine the role of timing, to find out whether disease or treat-ment stage facilitates and/or hinders participation in mBSR for breast cancer patients.
How do breast cancer patients experience the timing of participating in a mbSR-training? What are specific benefits or barriers?
thesis outline
Chapter 2 describes the study protocol of our multicenter Randomized Con-trolled Trial comparing the effectiveness of face-to-face group and individual internet-based Mindfulness-Based Cognitive Therapy with TAu in reducing psy-chological distress in cancer patients; the BeMind study.
Chapter 3 reports the results of the BeMind study. We simultaneously compared the effectiveness of both mBcT and emBcT to treatment as usual (TAu). In total, 245 heterogeneous cancer patients (of any stage) with psychological distress (≥ 11 on the Hospital Anxiety and Depression Scale (HADS)) were included. Patients were randomly allocated to mBcT (n=77), emBcT (n=90) or TAu (n=78) and com-pleted baseline (T0) and post-intervention (T1) assessments. Continuous out-comes were analyzed using Linear Mixed Modeling on the intention-to-treat sample.
Chapter 4 focuses on therapist competence, therapeutic alliance, and group cohesion and their association with reduction of psychological distress (HADS) after group-based mBcT for distressed cancer patients. To examine the possible prediction of these factors on psychological distress reduction, participants who completed mBcT were included (n=84) and multilevel analyses were used, in which partici-pants were nested within therapists (n=9). Baseline scores of treatment outcome were included as covariates in analyses.
Chapter 5 examines the extent to which early therapeutic alliance is a predictor of the reduction of psychological distress (HADS) and the increase of positive mental health (mHc) at post-treatment in emBcT compared to mBcT. To examine pre-diction participants who completed (e)mBcT were included (n=163), with separate hierarchical linear regression models.
Chapter 6 investigates what patients experience as a suitable stage to participate. A mixed method design was used in a sample of breast cancer patients following mBSR. Sixty-four patients participated in mBSR. Five focus groups (n=37) and three

19
semi-structured individual interviews were conducted until data saturation was reached.
In chapter 7 we summarize our findings followed by a general discussion in the context of the current literature. The strengths, limitations, and implications for future research and practice are discussed.
chapter 1

20
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
References
1. Bray, F., Transitions in human development and the global cancer burden. In: Wild CP, Stewart B, eds. World Cancer Report. Lyon: International Agency for Research on Cancer, 2014. World Cancer Report, 2014: p. 54-68.
2. Network, N.C.C. and N.C.C. Network, NccN clinical practice guidelines in on-cology: distress management. Available at: (Accessed May 26, 2016) http://oral-cancerfoundation. org/treatment/pdf/distress. pdf View in Article, 2010.
3. Carlson, L., et al., High levels of untreat-ed distress and fatigue in cancer patients. British Journal of Cancer, 2004. 90(12): p. 2297-2304.
4. Mitchell, A.J., et al., Prevalence of depres-sion, anxiety, and adjustment disorder in oncological, haematological, and pallia-tive-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncology, 2011. 12(2): p. 160-74.
5. Mitchell, A.J., et al., Depression and anxi-ety in long-term cancer survivors compared with spouses and healthy controls: a sys-tematic review and meta-analysis. Lancet Oncology, 2013. 14(8): p. 721-32.
6. Velikova, G., et al., The clinical value of quality of life assessment in oncology practice—a qualitative study of patient and physician views. Psycho-Oncology: Journal of the Psychological, Social and Behavioral Dimensions of Cancer, 2008. 17(7): p. 690-698.
7. Wu, Y.S., et al., Anxiety and depression in patients with head and neck cancer: 6-month follow-up study. Neuropsychiatric Disease Treatment, 2016. 12: p. 1029-36.
8. Hartung, T.J., et al., The risk of being depressed is significantly higher in cancer patients than in the general population: Prevalence and severity of depressive symp-toms across major cancer types. European Journal Cancer, 2017. 72: p. 46-53.
9. Jacob, L., et al., Prevalence of depres-sion, anxiety and their risk factors in German women with breast cancer in
general and gynecological practices. Journal of Cancer Research and Clinical Oncology, 2016. 142(2): p. 447-452.
10. Thomas, S.F., et al., Anxiety in long-term cancer survivors influences the acceptability of planned discharge from follow-up. Psy-cho-Oncology, 1997. 6(3): p. 190-6.
11. Greer, J.A., et al., Behavioral and psycho-logical predictors of chemotherapy adherence in patients with advanced non-small cell lung cancer. Journal of Psychosomatic Research 2008. 65(6): p. 549-52.
12. Brown, L.F., et al., The association of depression and anxiety with health-related quality of life in cancer patients with depres-sion and/or pain. Psycho-Oncology, 2010. 19(7): p. 734-41.
13. Saevarsdottir, T., N. Fridriksdottir, and S. Gunnarsdottir, Quality of life and symptoms of anxiety and depression of patients receiving cancer chemotherapy: longitudinal study. Cancer Nurs, 2010. 33(1): p. E1-e10.
14. Weihs, K.L., et al., Negative affectivity, re-striction of emotions, and site of metastases predict mortality in recurrent breast cancer. Journal of Psychosomatic Research, 2000. 49(1): p. 59-68.
15. Pinquart, M. and P.R. Duberstein, De-pression and cancer mortality: a meta- analysis. Psychological Medicine, 2010. 40(11): p. 1797-810.
16. Jansen, F., et al., Depressive symptoms in relation to overall survival in people with head and neck cancer: A longitudinal cohort study. Psycho-Oncology, 2018. 27(9): p. 2245-2256.
17. Caruso, R., et al., Psychiatric Disorders Related to Cancer: Prevalence, Etiology, and Recognition. Neuropathological Diseases, 2012. 1(1).
18. Fava, G.A., L. Mangelli, and C. Ruini, Assessment of psychological distress in the setting of medical disease. Psychotherapy and Psychosomatics, 2001. 70(4): p. 171-5.
19. Grassi, L., et al., Psychological factors affecting oncology conditions. Advanced Psychosomatic Medicine, 2007. 28: p. 57-71.

21
20. Kissane, D.W., Unrecognized and untreated depression in cancer care. Lancet Psychia-try, 2014. 1(5): p. 320-1.
21. Grassi, L., D. Spiegel, and M. Riba, Ad-vancing psychosocial care in cancer patients. F1000Res, 2017. 6: p. 2083.
22. Tamagawa, R., et al., Who benefits from psychosocial interventions in oncology? A systematic review of psychological moderators of treatment outcome. Journal of Behavioral Medicine, 2012. 35(6): p. 658-673.
23. Meyer, T.J. and M.M. Mark, Effects of psychosocial interventions with adult cancer patients: a meta-analysis of randomized experiments. Health Psychol, 1995. 14(2): p. 101-8.
24. Osborn RL, Demoncada AC, and F. M, Psychosocial interventions for depression, anxiety, and quality of life in cancer survi-vors: meta-analyses. International Journal of Psychiatry in Medicine 2006.
25. Goedendorp, M.M., et al., Psychosocial interventions for reducing fatigue during cancer treatment in adults. Cochrane Data-base of Systematic Reviews, 2009.
26. Beck, A.T., G. Emery, and R.L. Green-berg, Anxiety disorders and phobias: A cognitive perspective. 2005: Basic Books.
27. Greer, J.A., et al., Tailoring Cogni-tive-Behavioral Therapy to Treat Anxiety Comorbid with Advanced Cancer. Journal of Cognitive Psychotherapy, 2010. 24(4): p. 294-313.
28. Folkman, S. and S. Greer, Promoting psy-chological well-being in the face of serious illness: when theory, research and practice inform each other. Psycho-Oncology, 2000. 9(1): p. 11-9.
29. Parle, M., B. Jones, and P. Maguire, Maladaptive coping and affective disorders among cancer patients. Psychol Med, 1996. 26(4): p. 735-44.
30. Tatrow, K. and G.H. Montgomery, Cognitive behavioral therapy techniques for distress and pain in breast cancer patients: a meta-analysis. Journal of Behavioral Medicine, 2006. 29(1): p. 17-27.
31. Hart, S.L., et al., Meta-analysis of efficacy
of interventions for elevated depressive symp-toms in adults diagnosed with cancer. J Natl Cancer Inst, 2012. 104(13): p. 990-1004.
32. Xiao, F., et al., Effectiveness of Psychological Interventions on Depression in Patients After Breast Cancer Surgery: A Meta-analysis of Randomized Controlled Trials. Clin Breast Cancer, 2017. 17(3): p. 171-179.
33. Sun, H., et al., The Efficacy of Cognitive Behavioral Therapy to Treat Depression and Anxiety and Improve Quality of Life Among Early-Stage Breast Cancer Patients. Integrated Cancer Therapies, 2019. 18: p. 1534735419829573.
34. Luberto, C.M., et al., Theoretical Rationale and Case Illustration of Mindfulness-Based Cognitive Therapy for Fear of Cancer Recur-rence. Journal of Clinical Psychology in Medical Settings, 2019.
35. Dinkel, A., et al., Comorbidity of fear of progression and anxiety disorders in cancer patients. General Hospital Psychiatry, 2014. 36(6): p. 613-9.
36. Kabat-Zinn, J., Full catastrophe living, revised edition: how to cope with stress, pain and illness using mindfulness meditation. 2013: Hachette uK.
37. Segal, Z.V., J.M.G. Williams, and J.D. Teasdale, Mindfulness-based cognitive therapy for depression: A new approach to relapse prevention. 2013, New York: Guilford Press.
38. Kabat-Zinn, J., Full catastrophe living: Using the wisdom of your body and mind in everyday life. New York: Delacorte, 1990.
39. Crane, R., Mindfulness-based cognitive therapy: Distinctive features. 2017: Routledge.
40. Piet, J., H. Wurtzen, and R. Zachariae, The Effect of Mindfulness-Based Therapy on Symptoms of Anxiety and Depression in Adult Cancer Patients and Survivors: A Sys-tematic Review and Meta-Analysis. Journal of Consulting and Clinical Psychology, 2012. 80(6): p. 1007-1020.
41. Carlson, L.E., et al., Randomized controlled trial of Mindfulness-based cancer recovery versus supportive expressive group therapy for distressed survivors of breast cancer.
chapter 1

22
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Journal of Clinical Oncology, 2013. 31(25): p. 3119-26.
42. Garland, S.N., et al., Mindfulness-Based Stress Reduction Compared With Cognitive Behavioral Therapy for the Treatment of Insomnia Comorbid With Cancer: A Ran-domized, Partially Blinded, Noninferiority Trial. Journal of Clinical Oncology, 2014. 32(5): p. 449-457.
43. Lengacher, C.A., et al., Examination of Broad Symptom Improvement Resulting From Mindfulness-Based Stress Reduction in Breast Cancer Survivors: A Randomized Controlled Trial. Journal of Clinical On-cology, 2016. 34(24): p. 2827-2834.
44. Johannsen, M., et al., Efficacy of Mind-fulness-Based Cognitive Therapy on Late Post-Treatment Pain in Women Treated for Primary Breast Cancer: A Randomized Con-trolled Trial. Journal of Clinical Oncolo-gy, 2016. 34(28): p. 3390-+.
45. Schellekens, M.P.J., et al., Mindful-ness-Based Stress Reduction added to care as usual for lung cancer patients and/or their partners: A multi-centre randomized controlled trial. Psycho-Oncology, 2017 (in press): p. 10.1002/pon.4430
46. Abramowitz, J.S., B.J. Deacon, and D.P. Valentiner, The short health anxiety inven-tory: Psychometric properties and construct validity in a non-clinical sample. Cognitive Therapy and Research, 2007. 31(6): p. 871-883.
47. Wise, T.N., M. Biondi, and A. Costantini, Psycho-oncology. 2013: American Psychi-atric Publications.
48. Brebach, R., et al., Psychological interven-tion targeting distress for cancer patients: a meta-analytic study investigating uptake and adherence. Psycho-Oncology, 2016. 25: p. 882-890.
49. Zernicke, K.A., et al., A randomized wait-list controlled trial of feasibility and efficacy of an online mindfulness–based cancer recovery program: the e-therapy for cancer applying mindfulness trial. Psychosomatic Medicine, 2014. 76(4): p. 257-67.
50. Saddichha, S., et al., Online interventions for depression and anxiety–a systematic
review. Health Psychology and Behav-ioral Medicine: an Open Access Journal, 2014. 2(1): p. 841-881.
51. Andersson, G., Internet-delivered psy-chological treatments. Annual review of clinical psychology, 2016. 12: p. 157-179.
52. Spijkerman, M.P., W.T. Pots, and E.T. Bohlmeijer, Effectiveness of online mind-fulness-based interventions in improving mental health: A review and meta-analysis of randomised controlled trials. Clin Psychol Rev, 2016. 45: p. 102-14.
53. Everts, F.Z.B., M.L. van der Lee, and E. de Jager Meezenbroek, Web-based individual Mindfulness-Based Cognitive Therapy for cancer-related fatigue – A pilot study. Internet Interventions, 2015. 2(2): p. 200-213.
54. Bruggeman-Everts, F.Z., et al., Effective-ness of Two Web-Based Interventions for Chronic Cancer-Related Fatigue Compared to an Active Control Condition: Results of the ‘Fitter na kanker’ Randomized Con-trolled Trial. Journal of Medical Internet Research, 2017. 19(10): p. e336.
55. Fairburn, C.G. and Z. Cooper, Therapist competence, therapy quality, and therapist training. Behavioral Research and Thera-py, 2011. 49(6-7): p. 373-8.
56. Kissane, D.W., et al., Cognitive-existential group psychotherapy for women with pri-mary breast cancer: a randomised controlled trial. Psycho-Oncology: Journal of the Psychological, Social and Behavioral Dimensions of Cancer, 2003. 12(6): p. 532-546.
57. Yalom, I.D., The theory and practice of group psychotherapy. 1995: Basic Books (AZ).
58. Waltz, J., et al., Testing the integrity of a psychotherapy protocol: assessment of adherence and competence. Journal of Consulting an Clinical Psychology, 1993. 61(4): p. 620-30.
59. Webb, C.A., R.J. Derubeis, and J.P. Bar-ber, Therapist adherence/competence and treatment outcome: A meta-analytic review. Journal of Consulting and Clinical Psychology, 2010. 78(2): p. 200-11.

23
60. Kuyken, W. and D. Tsivrikos, Therapist Competence, Comorbidity and Cognitive- Behavioral Therapy for Depression. Psycho-therapy and Psychosomatics, 2009. 78(1): p. 42-48.
61. Strunk, D.R., et al., Therapist Competence in Cognitive Therapy for Depression: Pre-dicting Subsequent Symptom Change. Jour-nal of Consulting & Clinical Psychology, 2010. 78(3): p. 429-437.
62. Ginzburg, D.M., et al., Treatment specific competence predicts outcome in cognitive therapy for social anxiety disorder. Behavior Research and Therapy, 2012. 50(12): p. 747-752.
63. Branson, A., R. Shafran, and P. Myles, Investigating the relationship between competence and patient outcome with cbT. Behavioral Research and Therapy, 2015. 68: p. 19-26.
64. Bordin, E.S., Theory and research on the therapeutic working alliance: New directions. The working alliance: Theory, research, and practice, 1994: p. 13-37.
65. Luborsky, L., Therapeutic alliances as predictors of psychotherapy outcomes: Fac-tors explaining the predictive success. The working alliance: Theory, research, and practice, 1994: p. 38-50.
66. Horvath, A.O. and B.D. Symonds, Rela-tion between working alliance and outcome in psychotherapy: A meta-analysis. Journal of Counseling Psychology, 1991. 38(2): p. 139.
67. Horvath, A.O., et al., Alliance in individual psychotherapy. Psychotherapy, 2011. 48(1): p. 9.
68. Salvio, M.-A., et al., The strength of the therapeutic alliance in three treatments for depression. Psychotherapy Research, 1992. 2(1): p. 31-36.
69. Spinhoven, P., et al., The therapeutic alliance in schema-focused therapy and transference-focused psychotherapy for borderline personality disorder. Journal of Consulting and Clinical Psychology, 2007. 75(1): p. 104-15.
70. Swift, J.K. and R.P. Greenberg, Premature discontinuation in adult psychotherapy: A
meta-analysis. Journal of consulting and clinical psychology, 2012. 80(4): p. 547.
71. Sucala, M., et al., The therapeutic relation-ship in e-therapy for mental health: a sys-tematic review. Journal Medical Internet Research, 2012. 14(4): p. e110.
72. Reynolds, D.J., Jr., et al., Impact of exchanges and client-therapist alliance in online-text psychotherapy. Cyberpsycho-logical Behavioral Social Network, 2013. 16(5): p. 370-7.
73. Applebaum, A.J., et al., Therapeutic alli-ance in telephone-administered cognitive-be-havioral therapy for hematopoietic stem cell transplant survivors. Journal of Consult-ing and Clinical Psychology, 2012. 80(5): p. 811-816.
74. Knaevelsrud, C. and A. Maercker, Does the quality of the working alliance predict treatment outcome in online psychotherapy for traumatized patients? Journal of Medi-cal Internet Research, 2006. 8(4): p. e31.
75. Preschl, B., A. Maercker, and B. Wagner, The working alliance in a randomized controlled trial comparing online with face-to-face cognitive-behavioral thera-py for depression. Bmc Psychiatry, 2011. 11: p. 189.
76. Budman, S.H., et al., Cohesion, alliance and outcome in group psychotherapy. Psy-chiatry, 1989. 52(3): p. 339-50.
77. Beal, D.J., et al., Cohesion and performance in groups: a meta-analytic clarification of construct relations. Journal Applied Psy-chology, 2003. 88(6): p. 989-1004.
78. van Andel, P., et al., Group cohesion and working alliance: prediction of treatment outcome in cardiac patients receiving cognitive behavioral group psychotherapy. Psychotherapy and Psychosomatics, 2003. 72(3): p. 141-149.
79. Taube-Schiff, M., et al., Group cohesion in cognitive-behavioral group therapy for social phobia. Behavioral Research Therapy, 2007. 45(4): p. 687-698.
80. Marziali, E., H. Munroe-Blum, and L. McCleary, The contribution of group cohesion and group alliance to the outcome of group psychotherapy. International
chapter 1

24
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Journal Group Psychotherapy, 1997. 47(4): p. 475-497.
81. May, A.M., et al., The effect of group cohesion on rehabilitation outcome in cancer survivors. Psycho-Oncology, 2008. 17(9): p. 917-925.
82. Brakel, T.M., A. Dijkstra, and A.P. Buunk, Targeting cancer patients’ quality of life through social comparison: A ran-domised trial. Psychology & health, 2014. 29(8): p. 950-966.
83. Crane R.S., K.W., Williams J.M.G., Hastings RP, Cooper L, Fennell M.J.V., Competence in teaching mindfulness-based courses: concepts, development and assess-ment. Mindfulness 2012. 3(1):p. 76-84.3.
84. Sharpless, B.A. and J.P. Barber, A concep-tual and empirical review of the meaning, measurement, development, and teaching of intervention competence in clinical psychol-ogy. Clinical Psychology Review, 2009. 29(1): p. 47-56.
85. Dobkin, P.L., S. Hickman, and K. Monshat, Holding the heart of mindful-ness-based stress reduction: balancing fidel-ity and imagination when adapting mbSR. Mindfulness, 2014. 5(6): p. 710-718.
86. McCown, D., D. Reibel, and M.S. Mi-cozzi, Teaching mindfulness. A practical guide for clinicians and educators. uS: Springer, 2010.
87. Crane, R.S., et al., Competence in Teaching Mindfulness-Based Courses: Concepts, De-velopment and Assessment. Mindfulness, 2012. 3(1):p. 76-84.3.
88. Huijbers, M.J., et al., Teacher Competence in Mindfulness-Based Cognitive Therapy for Depression and Its Relation to Treatment Outcome. Mindfulness (NY), 2017. 8(4): p. 960-972.
89. Ruijgrok-Lupton, P.E., R.S. Crane, and D. Dorjee, Impact of Mindfulness-Based Teacher Training on mbSR Participant Well-Being Outcomes and Course Satisfac-tion. Mindfulness, 2017: p. 1-12.
90. Compen, F.R., et al., Mindfulness-Based Cognitive Therapy for Cancer Patients De-livered via Internet: Qualitative Study of Pa-tient and Therapist Barriers and Facilitators.
Journal of Medical Internet Research, 2017. 19(12): p. e407.
91. Snippe, E., et al., The Therapeutic Alliance Predicts Outcomes of Cognitive Behavior Therapy but Not of Mindfulness-Based Cognitive Therapy for Depressive Symptoms. Psychotherapy and Psychosomatics, 2015. 84(5): p. 314-315.
92. van Aalderen, J.R., et al., The Role of the Teacher in Mindfulness-Based Approaches: A Qualitative Study. Mindfulness, 2014. 5(2): p. 170-178.
93. Schellekens, M.P.J., et al., Mindful-ness-Based Cancer Recovery (mbcR) versus Supportive Expressive Group Therapy (SET) for distressed breast cancer survivors: evalu-ating mindfulness and social support as me-diators. Journal of Behavioral Medicine, 2017. 40(3): p. 414-422.
94. Mackenzie, M.J., et al., A qualitative study of self-perceived effects of mindfulness-based stress reduction (mbSR) in a psychosocial oncology setting. Stress and Health, 2007. 23(1): p. 59-69.
95. Schellekens M.P.J., A qualitative study on mindfulness-based stress reduction for breast cancer patients: how women experience participating with fellow patients. Support Care Cancer, 2016. 24(4):p. 1813-1820
96. Henselmans, I., et al., Identification and prediction of distress trajectories in the first year after a breast cancer diagnosis. Health Psychology, 2010. 29(2): p. 160.
97. Mitchell A., F., D., Gill, J., Paul, J., Sy-monds, P., Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: a systematic review and meta-analysis. Lancet Oncology, 2013. 14(8): p. 721-732
98. Shapiro PJ, Coyne JC, and K. LK, Interest in services among prostate cancer patients receiving androgen deprivation therapy. Psy-cho-Oncology, 2004. 13(8): p. 512-525
99. Karageorge, A., et al., Acceptability of an in-ternet cognitive behavioural therapy program for people with early-stage cancer and cancer survivors with depression and/or anxiety: the-matic findings from focus groups. Supportive Care Cancer, 2017. 25(7): p. 2129-2136.

25
100. Brebach R., et al., Psychological interven-tion targeting distress for cancer patients: a meta-analytic study investigating uptake and adherence. Psycho-Oncology 2016. 25(8): p. 882-890
101. Henderson, V.P., et al., The effects of mindfulness-based stress reduction on psychosocial outcomes and quality of life in early-stage breast cancer patients: a ran-domized trial. Breast cancer research and treatment, 2012. 131(1): p. 99-109.
102. Lengacher, C.A., et al., Randomized controlled trial of mindfulness-based stress reduction (mbSR) for survivors of breast cancer. Psycho-Oncology, 2009. 18(12): p. 1261-72.
103. Hoffman, C.J., et al., Effectiveness of mindfulness-based stress reduction in mood, breast- and endocrine-related quality of life, and well-being in stage 0 to III breast can-cer: a randomized, controlled trial. Journal of Clinical Oncology, 2012. 30(12): p. 1335-42.
104. Carlson, L.E., et al., Randomized Con-trolled Trial of Mindfulness-Based Cancer Recovery Versus Supportive Expressive Group Therapy for Distressed Survivors of Breast Cancer (mINDSET). Journal of Clinical Oncology, 2013. 31(25): p. 3119-3126.
105. Cramer H, et al., Mindfulness based stress reduction for breast cancer – a systematic review and meta-analysis. Current Oncology 2012. 19(5): e343.
106. Carlson, L.E., et al., What goes up does not always come down: patterns of distress, physical and psychosocial morbidity in people with cancer over a one year period. Psycho-Oncology, 2013. 22(1): p. 168-76.
107. Costa-Requena, G., A. Rodriguez, and P. Fernandez-Ortega, Longitudinal assessment of distress and quality of life in the early stages of breast cancer treat-ment. Scandinavian Journal of Caring Science, 2013. 27(1): p. 77-83.
108. Dimidjian, S. and Z.V. Segal, Prospects for a clinical science of mindfulness-based intervention. American Psychology, 2015. 70(7): p. 593-620.
chapter 1


Chapter 2
Study protocol of a multicenter randomized controlled trial comparing the effectiveness of group and individual internet-based Mindfulness-Based Cognitive Therapy with treatment as usual in reducing psychological dis-tress in cancer patients: the BeMind study
This chapter has been published as:
F.R. Compen, E.M. Bisseling, M.L. Van der Lee, E.M.M. Adang, A.R.T. Donders, A.E.M. Speckensbmc Psychology (2015): 13;3:27
Acknowledgement of research support: This study is funded by breast cancer foundation Pink Ribbon (2012.WO14.C153)

28
Min
dfu
lness-based
cogn
itive therapy fo
r distressed
cancer patien
ts
abstract
background Mindfulness-based interventions have shown to reduce psycho-logical distress in cancer patients. The accessibility of mindfulness-based inter-ventions for cancer patients could be further improved by providing mindfulness using an individual internet-based format. The aim of this study is to test the effectiveness of a Mindfulness-Based Cognitive Therapy (mBcT) group interven-tion for cancer patients in comparison with individual internet-based mBcT and treatment as usual (TAu).
Methods A three-armed multicenter randomized controlled trial comparing group-based mBcT to individual internet-based mBcT and TAu in cancer patients who suffer from at least mild psychological distress (Hospital Anxiety and Depres-sion Scale (HADS) ≥ 11). Measurements will be conducted prior to randomization (baseline), post-treatment and at 3 months and 9 months post-treatment. Partic-ipants initially allocated to TAu are subsequently randomized to either group- or individual internet-based mBcT and will receive a second baseline measurement after 3 months. Thus, the three-armed comparison will have a time span of approx-imately 3 months. The two-armed intervention comparison includes a 9-month follow-up and will also consist of participants randomized to the intervention after TAu. Primary outcome will be post-treatment psychological distress (HADS). Second-ary outcomes are fear of cancer recurrence (Fear of Cancer Recurrence Inventory), rumination (Rumination and Reflection Questionnaire), positive mental health (Mental Health Continuum – Short Form), and cost-effectiveness (health-related quality of life (EuroQol –5D and Short Form-12) and health care usage (Trimbos and imTA questionnaire on Costs associated with Psychiatric illness). Potential predictors: DSm-IV-TR mood/anxiety disorders (ScID-I) and neuroticism (NEO-Five Factor Inventory) will be measured. Mediators of treatment effect: mindfulness skills, (Five-Facets of Mindfulness Questionnaire- Short Form), working alliance (Working Alliance Inventory) and group cohesion (Group Cohesion Questionnaire) will also be measured.
discussion This trial will provide valuable information on the clinical and cost-effectiveness of group versus internet-based mBcT versus TAu for distressed cancer patients.

29
chapter 2
background
Cancer is a major health care challenge. Cancer causes more than a quarter of all deaths in OEcD countries with more than 5 million new cases diagnosed every year, averaging about 261 cases per 100 000 people.1 In the Netherlands it is expected that the incidence of cancer will increase with more than 40% between 2007 and 2020.2 These numbers indicate that we are looking at a steadily increasing number of patients who will have to cope with cancer in the near future. Living with cancer is a psychological burden. In a review of the prevalence of depression, anxiety and adjustment disorders in cancer patients in both palliative and non-palliative settings it was found that about one third of all patients suffer from a mood disorder in the first five years after diagnosis.3 A recent epidemiological survey based on more than 2000 structured clinical interviews across major tumor entities found the most prevalent mental disorders to be anxiety (11.5%) adjust-ment (11.1%) and depressive disorders (6.5%).4 Considering the rising prevalence of people living with cancer, the absolute number of cancer patients in need of psychological treatment is expected to increase. Addressing this increasing need calls for effective, widely available and accessible psychological treatment. In recent years, many studies have assessed the effect of mindfulness-based interventions for cancer patients. Mindfulness is defined as intentionally pay-ing attention to moment-by-moment experiences in a non-judgmental way.5 Mindfulness-Based Stress Reduction (mBSR)6 and Mindfulness-Based Cognitive Therapy (mBcT)7, the latter developed specifically to prevent relapse in depression, are protocols designed to teach the cultivation of mindfulness. In a review of 22 studies, mindfulness-based interventions were found to be moderately effective in reduction of symptoms of anxiety and depression in cancer patients.8 Recent-ly, another randomized controlled trial (RcT) showed that mindfulness-based treatment was superior to both supportive-expressive group therapy and a 1-day stress management condition in improving a range of psychological outcomes in a sample of 271 distressed breast cancer survivors.9 Although any follow-up results should still be considered preliminary, the recent review indicates that effect sizes (ES) at follow-up were significant with small to moderate ESs for nonrandomized studies and small ESs for RcTs. Psychological treatment for cancer patients implies treatment for people who have difficulty with travelling due to cancer -related impairments or fatigue. Also, treatment scheduling should be flexible, allowing for adaptation to individual cir-cumstances, for example ongoing radio- or chemotherapy. Taking this into account, internet-based treatment might hold promise to address these problems. A recent review concludes that guided internet-based Cognitive Behavioural Therapy (cBT) ‘appears to be a promising and effective treatment for chronic somatic conditions

30
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
to improve psychological and physical functioning and disease-related impact’.10 In addition to its clinical effectiveness, research also suggests evidence for the cost-effectiveness of internet-based cBT for somatic populations.11, 12
Literature on the effectiveness of internet-based mindfulness treatment is still scarce. There are a few studies in non-clinical populations which show that internet-based mindfulness treatment resulted in an improvement of mindfulness skills and reduction of perceived distress.13-15 Recently, encouraging evidence was presented for the feasibility and efficacy of internet-based mindfulness treatment in a study of 62 underserved and distressed cancer patients.16 Compared to treat-ment as usual (TAu) patients reported an increase of mindfulness and a reduction of depressive and stress symptoms. This provides preliminary evidence for the effectiveness of internet-based mindfulness treatment compared to TAu. Direct comparisons of internet-based mindfulness treatment to existing group treatments for distressed cancer patients are absent, let alone follow-up com-parisons. One of the biggest challenges in internet intervention research is low treatment adherence17 which affects treatment effectiveness.18 A recent study of internet-based mBcT for treatment of chronic cancer-related fatigue using a treatment format similar to ours indicated a non-adherence rate of 38%, which is higher than in comparable face-to-face interventions.19 The current trial will provide the first description of the relative long-term effectiveness of group- compared to internet-based mBcT by including a follow-up measurement up to 9 months post-treatment and keeping close track of treatment adherence in both intervention arms. Thus, it is unknown whether internet-based mBcT has similar effectiveness as group-based mBcT in alleviating distress in cancer. Therefore, we primarily compare post-treatment psychological distress between group-based and internet-based mBcT. Also, effectiveness in reducing psychological distress up to nine months post-treatment will be compared between group- and internet-based mBcT. More-over, we would like to determine whether the two interventions could reduce fear of cancer recurrence and rumination. Also, at the other end of the psychological spectrum, both group- and internet-based mBcT might be able to improve positive mental health in cancer patients compared to TAu. Furthermore, alongside the clinical trial, cost-effectiveness of both mBcT interventions compared to TAu will be determined. We expect both interventions to be cost-effective compared to TAu. We do not expect all individuals to benefit similarly from the two interventions. Therefore, studying predictors of each intervention’s effect potentially enables us to determine who benefits most from what treatment – group-based or inter-net-based mBcT. In this study we would like to explore two possible predictors: the presence/absence of a DSm-IV-TR mood/anxiety disorder and the personality trait neuroticism.

31
chapter 2
Research on mindfulness-based interventions for cancer patients has focused on the prevalence and treatment of distress rather than psychiatric disorders. Not much is known on the effectiveness of mBcT in oncology patients suffering from a mood and/or anxiety disorder as opposed to patients suffering from distress. We are interested to see if the presence of a psychiatric disorder is a better predictor of treatment outcome than psychological distress. Moreover, previous research has shown that a high score on neuroticism has a negative effect on (group) psychotherapy outcome.20 This study aims to explore the hypothesis that higher neuroticism at baseline has a negative predictive value for the primary outcome measure and to explore possible differences in treatment outcome between group- and internet-based mBcT. As it is known that mindfulness skills mediate the relationship between mindful-ness practice and improvements in psychological symptoms (e.g.21), we hypothesize that the improvement on the Hospital Anxiety and Depression Scale (HADS) in the mBcT intervention arms is mediated by mindfulness skills. Moreover, weekly measurements (mAAS and I-PANAS-SF) will be used to test the hypothesis that an increase in mindfulness skills antedates changes in affect during the intervention. One of the differences between face-to-face and online treatment is the rela-tionship with the therapist. Working alliance, or therapeutic alliance, is a long-rec-ognized concept in psychotherapy research. Although it is known that a working alliance is realizable in internet-based therapy,22 little is known about the possible difference in working alliance between group- and internet-based mBcT. We would be interested to see if working alliance mediates the relationship between intervention and outcome in both interventions. The relationship with both the therapist and other group members in group-based treatment, or group cohesion, is often considered to be one of the most important contributors to positive treatment effect in group therapy. The current study aims to assess whether group cohesion mediates the relationship between the group-based mBcT intervention and outcome. In conclusion, the primary aim of this study is to compare the effectiveness of group- and internet-based mBcT to TAu to reduce distress in cancer patients after treatment. Secondary outcome measures will be fear of cancer recurrence, rumination, and positive mental health. In addition, possible effect predictors (DSm-IV-TR mood/anxiety disorder and neuroticism) and mediators (mindfulness skills, working alliance, group cohesion) of treatment outcome will be explored. In order to determine the long-term stability of intervention effects, assessments will take place 3 and 9 months post-treatment. Alongside the clinical trial, the cost-effectiveness of both mBcT interventions compared to TAu will be determined. As far as we know, this is the first direct comparison between group-based mBcT, internet-based mBcT and TAu.

32
Min
dfu
lness-based
cogn
itive therapy fo
r distressed
cancer patien
ts
methods/design
study designThis study is a multicenter, parallel group randomized controlled trial. Participants are randomized to group-based mBcT, internet-based mBcT or TAu. Participants initially randomized to TAu are subsequently randomized to either group- or internet-based mBcT which participants receive after a waiting-list period of three months. During the waiting-list period, participants know which treatment they will receive after the waiting list and participants are allowed to receive care as usual, except for any mindfulness-based intervention. The study protocol has been approved by our ethical review board (cmO Arnhem-Nijmegen) and is registered under number 2013/542.
settingThe group mBcT is provided at the Radboud University Medical Centre in Nijme-gen, the Jeroen Bosch Hospital in ’s Hertogenbosch and at four mental health institutes specialized in psycho-oncology (Helen Dowling Institute (Bilthoven), Ingeborg Douwes Centrum (Amsterdam), De Vruchtenburg (Leiden), Het Behoud-en Huys (Haren)). The internet-based mBcT has been developed with, protected and hosted by IPPZ, a commercial e-health company in the Netherlands. Patients receive an invitational e-mail with the conditions of use. The internet-based mBcT is accessed using a personal double-step-verification- protected webpage on the participants’ own personal computer, mobile phone or tablet device.
study populationInclusion criteria of the study are a) a cancer diagnosis, any tumor or stage b) a score of 11 or higher on the Hospital Anxiety and Depression Scale (HADS), c) computer literacy and internet access d) a good command of the Dutch language and e) willingness to participate in either mBcT intervention. Exclusion criteria are a) severe psychiatric morbidity such as suicidal ideation and/or psychosis b) change in psychotropic medication dosage within a period of three months prior to baseline c) current or previous participation in a mindfulness-based intervention (> 4 sessions of mBcT or mBSR).
procedureParticipants are recruited in aforementioned participating centers and recruit-ed via social media, patient associations and advertorials in local newspapers. Patients who are interested in participation can enroll themselves at our website (www.bemind.info) at which point they complete the HADS. Patients with a score of 11 or higher are contacted by telephone by one of the researchers. During this call

33
chapter 2
more information about the study is provided and eligible patients are invited for a research interview. The subsequent research interview is conducted face-to-face or by telephone depending on participant preference. Written informed consent, demographic and clinical characteristics are obtained on paper via regular mail. Subsequently the Structured Clinical Interview for DSm-IV-TR Axis-I disorders (ScID-I) is administered to diagnose possible mood/anxiety disorders and the Trimbos and imTA questionnaire on Costs associated with Psychiatric illness (TiC-P) to assess medical and productivity loss costs. The participant completes the remainder of the (self-report) questionnaires online.
randoMizationRandomization is stratified for setting and minimized for a) gender, b) stage of disease (curative versus palliative) and c) type of cancer (breast cancer versus other). Randomization is computerized using a randomization website specifically designed for the current study. Randomization is conducted by one of the researchers (EB) who is not involved in the follow-up assessment.
follow-up assessMentFollow-up assessments take place directly post-treatment and at three and nine months follow-up. The follow-up assessments are similar to the baseline assessment: participants are contacted by telephone in order to re-administer the ScID-I and the TiC-P and participants receive an online survey with the self-report scales. In case of dropout, the researcher tries to contact the participant at least three times to complete the outcome measures and to identify the main reason for dropout.
interventionThe mBcT curriculum used in both group and internet-based mBcT interventions is primarily based on the mBcT program by Segal, Williams and Teasdale.23 The program was adapted to the oncology patient in terms of tailoring psycho-educative elements to themes relevant to the cancer patient (e.g. cancer-related fatigue) and adapted movement exercises (for patients suffering from edema). In both conditions, participants receive guided mindfulness meditation exercises for home practice and a reader with home practice instructions and background information. The group-based mBcT curriculum consists of 8 weekly 2,5 hour group sessions, a silent day between session six and seven and home practice assignments of about 45 minutes, 6 days per week (see table 2). During the weekly sessions the teacher guides different mindfulness exercises and introduces new exercises, and home practice assignments are discussed. The internet-based mBcT intervention is similar to group mBcT in curricu-lum content, but different in delivery. Participants in the internet-based mBcT

34
Min
dfu
lness-based
cogn
itive therapy fo
r distressed
cancer patien
ts
intervention log in on a secure personal webpage where all content relevant to that week’s session can be downloaded. Participants are asked to read the weekly information and do the mindfulness exercises and write down their experiences in their personal log. They are encouraged to correspond with their personal teacher about their practice experiences via a secure, integrated mailing system. The teacher replies to this log on a predetermined day of the week and guides the participant through the curriculum. Participants can continue with next weeks’ session only after registering their experiences in their log for the previous week. Participants are encouraged to follow the intervention within the nine-week structure. However, the teacher can decide to extend this period in case of illness or holidays. All teachers fulfill the advanced criteria of the Association of Mindfulness Based Teachers in the Netherlands and Flanders which are in concordance with the uK Mindfulness-Based Teacher Trainer Network Good Practice Guidelines for teaching mindfulness-based courses,24 including a minimum of 150 hours of education in mBSR/mBcT background and theory, training in teaching formal and informal meditation practices, psycho-education and inquiry, supervision and giving an mBSR or mBcT course including a reflection report, b) relevant professional training, c) minimum of three years of practicing meditation regu-larly and attending retreats, d) having attended mBSR/mBcT as a participant, e) continued training and f ) giving a minimum of two courses per two year. Three full-day plenary supervision meetings are held during the intervention phase of the trial, consisting of mindfulness practices, workshops, small group teachings and plenary discussions about difficulties or practical issues. All teachers are involved in both group and internet-based mBcT. Teachers without prior internet-based mBcT experience are provided with guidelines and supervised by more experienced internet-based mBcT teachers. In the group-based mBcT condition, sessions are videotaped to evaluate teacher competence and protocol adherence using the Mindfulness-Based Interventions - Teachers Assessment Criteria (mBI-TAc).25 The mBI-TAc was translated to Dutch using the guidelines of the International Test Commission.26 Group-based mBcT participants are requested to complete the same form for their teachers’ compe-tence. As the mBI-TAc is not applicable to internet-based treatment and there are currently no other ways to evaluate teacher competence in internet-based mind-fulness treatment, teacher competence will not be assessed in the internet-based condition using a standardized measurement.
priMary outcoMe MeasureFor a measurement scheme we refer to Table 1. The primary outcome measure is the post-treatment total score on the HADS, a 14-item self-report screening scale that was originally developed to indicate the possible presence of anxiety and

35
chapter 2
depressive states in the setting of a medical outpatient clinic.27, 28 As earlier research in a palliative setting suggested the total HADS score should be used, this score will be used rather than individual depression and anxiety subscales.29 The HADS shows good psychometric properties in the general medical population, includ-ing oncology patients in palliative phase.30 Internal consistency as measured with Cronbach’s α varied from .84 to .90.28, 31 Test-retest reliability was good as Pearson’s r > .80 were obtained.28, 32
secondary outcoMe MeasuresFear of cancer recurrence is assessed with the Fear of Cancer Recurrence Inven-tory (FcRI33). This 42-item 4-point Likert scale questionnaire has been found to have a robust factor structure with Cronbach’s α=0.75 to 0.91 across subscales and test-retest reliabilities over a two-week interval of 0.58 to 0.83 across subscales. The FcRI is positively associated with other measures of anxiety symptoms, intrusive thoughts and avoidance and negatively associated with quality of life in a large sample of cancer patients.33
Rumination is measured by the rumination subscale of the Rumination and Reflection Questionnaire (RRQ34). Subjects rate their level of agreement of dis-agreement on a five-point rating scale (e.g., ‘I always seem to be re-hashing in my mind recent things I’ve said or done’). The Dutch version has Cronbach’s alphas ranging between .88 and .93.35
Positive mental health is measured by the Mental Health Continuum-Short Form (mHc-SF36) which comprises 14 items, representing various feelings of well-being in the past month rated on a 6-point Likert scale (never, once or twice a month, about once a week, two or three times a week, almost every day, every day). The mHc-SF contains three subscales: emotional, psychological and social wellbeing. The short form of the mHc has shown excellent internal consistency (> .80). The test-retest reliability of the mHc-SF over three successive 3 month periods was .68 and the 9 month test-retest in a Dutch sample was .65.37
Data on medical and societal costs and data on health-related quality of life are collected to conduct the cost-effectiveness – analysis. Data on medical and societal costs are gathered using the TiC-P.38 The TiC-P generates quantitative data about direct health care utilization (the type of care, its duration and medication) and indirect societal costs (cancer-related absence from work and cancer-related impair-ment in non-paid work). Unit cost estimates are derived from the national manual for cost prices in the health care sector.39 Unit cost estimates are combined with resource utilization data to obtain a net cost per patient over the entire follow-up period. Unit cost estimates are derived from the national manual for cost prices in the health care sector. Costs of reduced ability to work are estimated using the friction costs method. Treatment costs are calculated using activity-based-costing

36
Min
dfu
lness-based
cogn
itive therapy fo
r distressed
cancer patien
ts
methods, thus measuring actual resources (time of therapist, time of patients, facilities) used. Unit cost estimates are combined with resource utilization data to obtain a net cost per patient over the entire follow-up period. To measure the health-related quality of life of cancer patients, a validated health-re-lated quality of life instrument is used, the EuroQol-5D (EQ-5D40). The EQ-5D is a generic instrument comprising five domains: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. The EQ-5D index is obtained by apply-ing predetermined weights to the five domains. This index gives a societal-based global quantification of the participant’s health status on a scale ranging from 0 (death) to 1 (perfect health). Participants are also asked to rate their overall quality of life on a visual analogue scale (EQ- 5D VAS) consisting of a vertical line ranging from 0 (worst imaginable health status) to 100 (best imaginable). The EQ-5D is available in a validated Dutch translation.41 Because there are indications that the Short Form-12 (SF-1242), another questionnaire on health-related quality of life, is more sensitive to change in populations with less severe morbidity than the EQ-5D,43 the SF-12 is administered as well. The SF-12 consists of 12 items yielding two summary scores for physical and mental health. Scoring is norm based with a mean of 50 (SD = 10); higher scores indicate better health.
effect predictorsPresence of DSm-IV Axis I mood/anxiety disorders is assessed by the ScID-I44 which is a structured clinical interview. The interviewer rates answers on standardized questions during the interview on a scoring form. Subsequently, the presence or absence of symptoms is assessed. The ScID-I is administered by trained inter-viewers. An experienced psychiatrist (EBI) supervises the administration of the ScID-I. In the current study, neuroticism is assessed with the NEO Five Factor Inventory.45 A shorter version of the Revised NEO Personality Inventory (NEO-PI-R), the NEO-FFI has 60 items (12 per domain) derived from the original 240 items. The five factor domains assessed by this measure are neuroticism, extraversion, openness to experience, agreeableness, and conscientiousness. The psychometric properties of the Dutch NEO-FFI are good.46
process MeasuresMindfulness skills are assessed with the 24-item Five Facet Mindfulness Questionnaire Short Form (FFmQ-SF). The FFmQ consists of five subscales: observing, describing, acting with awareness, non-judging of inner experience and non-reactivity to inner experience. The FFmQ is sensitive to change in mindfulness-based interventions (e.g.21). A Dutch 24-item short form of the FFmQ (FFmQ-SF) was developed and assessed in a sample of 376 adults with clinically relevant symptoms of depres-sion and anxiety and cross-validated in an independent sample of patients with

37
chapter 2
fibromyalgia47 The FFmQ-SF was positively related to well-being and openness to experience and inversely related to measures of psychological symptoms, experi-ential avoidance, and neuroticism. In addition, in both group and internet-based mBcT the following process measures are administered at the start of each weekly session in order to deter-mine processes of change during both interventions. In the group mBcT they are handed out in paper by the teacher, in the internet-based mBcT intervention they are provided online at the beginning of a new training week. The Mindful Atten-tion Awareness Scale (mAAS48) is administered weekly to assess mindful attention in daily life. The mAAS has been shown to have an similar factor structure in cancer patients as in the general population49 Chronbach’s alpha for the Dutch version ranged between .82 and .87.50 Positive and negative affect is assessed weekly using the International Positive and Negative Affect Scale – Short Form I-PANAS-SF). The crosscultural factorial invariance, internal reliability, temporal stability, and convergent and criterion-related validities of the I-PANAS-SF were found to be acceptable.51
Working alliance is measured with a translated and shortened form of the Working Alliance Inventory (WAI52), consisting of three subscales assessing: 1) how closely client and therapist agree on and are mutually engaged in the goals of treatment, 2) how closely client and therapist agree on how to reach the treatment goals, and 3) the degree of mutual trust, acceptance, and confidence between client and therapist. Patients score on a 5-point scale ranging from rarely to always.53, 54 The 12-item inventory was validated in a Dutch-speaking sample and a recent study showed that internal consistency of the short form was >.80 for all separate sub-scales and .87 for the total.55 The WAI is administered before session 2, 5 and 9. Self-reported group cohesion is assessed in the group mBcT condition with the Dutch Group Cohesion Questionnaire (GcQ) that has been used in cancer patients before.56 The GcQ consists of four subscales: the bond with the group as whole, the bond with other members, cooperation within the group and the instrumental value of the group bond. Each item is rated from 1 (totally disagree) to 6 (totally agree). Internal consistency of all scales was reported to range from adequate to good (0.66–0.88).57 The GcQ is administered before session 2, 5 and 9. Adherence is assessed during the entire treatment period with a calendar (both for group and internet-based mBcT) on which participants fill out whether they adhere to both formal (e.g. the sitting meditation) and informal (e.g. 3-min breathing space) mindfulness exercises. Adherence to protocol has been shown to mediate the effects of mBcT on depressive symptoms. Semi-structured interviews. In order to more fully understand how interventions bring about change, it is important to complement quantitative research with qualitative research.58 For this reason participants’ views on barriers and faci-

38
Min
dfu
lness-based
cogn
itive therapy fo
r distressed
cancer patien
ts
litators of the internet-based mBcT are explored in more detail by conducting semi-structured interviews in a purposive sample of participants in the trial.
statistical analysis Sample size
Based on post treatment HADS scores within the routine outcome data of cancer patients who received mindfulness at the Helen Dowling Institute, we expected post treatment HADS scores of 10.6 (SD 6.4) in the mBcT interventions and 14.8 (SD 8.1) in the TAu condition. In the power calculation we ignored the dependency caused by the therapy groups, which has been found in previous research to be small.59 As we compare both group and internet-based mBcT to TAu, we corrected the corresponding alpha level to 0.025. Assuming a power of 0.9, a sample size of 65 per condition is needed. Taking an estimated expected dropout rate of 15% in the group mBcT and TAu and 30% in the internet-based mBcT into account, we aim to recruit 76 participants in the group mBcT and TAu conditions and 93 in the internet-based mBcT, thus 245 patients in total.
Statistical analysisAll analyses are carried out using the intention to treat and per protocol samples. The primary analysis is aimed at showing superiority of group mBcT and inter-net-based mBcT compared to TAu in terms of psychological distress directly post treatment in the intention to treat sample. Secondary analyses of the stability of the treatment effect are conducted using the data from the assessments at 3 and 9 months post-treatment, using linear mixed models to control for possible dependency caused by the repeated measurements. We will use the bootstrapping procedure as it provides the most powerful and reasonable method of obtaining confidence limits for specific indirect effects under most conditions.60 In all mediation analyses, post-treatment HADS scores are controlled for baseline HADS scores. Residual change scores for all potential mediators are calculated.61 To explore whether the mediators (partly) affect the relation of condition on post-treatment symptom levels, the model including the potential mediators is compared with the model without mediators for both uni-variate and multivariate models. Subsequently, 95% bias corrected and accelerated confidence intervals (95% cI)62 are calculated to explore the contribution of each individual mediator and the group of mediators in total.
Cost-effectivenessThe economic evaluation is based on the general principles of a cost-utility analysis and is performed alongside the clinical trial which compares three alternatives: 1) group mBcT; 2) internet-based mBcT, and 3) TAu. Primary outcome measures

39
chapter 2
for the economic evaluation are: costs (here we follow the Dutch guidelines for costing research39) and quality adjusted life years (QALY) measured by the EQ-5D. Secondary analyses will explore the possible differences in outcome with HrQoL measured by SF-12. The societal perspective is operationalized by including pro-ductivity losses/gains applying the friction cost method on a per patient basis by means of the TiC-P.63
The incremental cost-effectiveness ratio (IcER) ‘cost per Quality-Adjusted Life Year (QALY) gained’ based on EQ-5D utilities according to the Dutch algorithm41 is computed and uncertainty surrounding these parameters is determined using the bootstrap method (dealing with potential skewness in the distributions). A cost-effectiveness acceptability curve will be derived that is able to evaluate efficiency by using a range of thresholds (Willingness To Pay for a QALY gained). The impact of uncertainty surrounding relevant deterministic parameters on the IcER is subsequently explored using one-way sensitivity analyses on the range of extremes. The cost analysis exists of two main parts. First, on patient level, volumes of care is measured using patient questionnaires. Per arm (intervention and control groups) full cost-prices are determined using activity based costing. The second part of the cost analysis consists of determining the cost prices for each volume of consumption in order to use these for multiplying the volumes registered for each participating patient. The Dutch guidelines for cost analyses are used with regard to prices.39 For units of care/resources where no guideline or standard prices are available real cost prices are determined.
discussion
A significant proportion of cancer patients suffers from psychological distress and is in need of appropriate psychological treatment.4 An increase in the num-ber of patients who will have to deal with the consequences of having cancer is to be expected,2, 3 which calls for more widely accessible and effective psychosocial treatment. Mindfulness-based treatment has proven to be effective in reducing psychological distress in cancer patients.8
Providing internet-based mindfulness could hold promise in terms of increasing accessibility: patients do not have to travel and treatment planning is more flexible in the light of individual circumstances. Therefore, the current trial investigates the effectiveness in reducing psychological distress of both group- and internet-based mBcT compared to TAu. Furthermore, although the need of cost-effectiveness evaluations of psycho-on-cological interventions has long been recognized,64 information on the cost-effec-tiveness of mindfulness interventions is largely absent. In addition to the clinical

40
Min
dfu
lness-based
cogn
itive therapy fo
r distressed
cancer patien
ts
effectiveness, the current trial also investigates cost-effectiveness of both group- and internet-based mBcT interventions compared to TAu. We hope that our trial provides further insight into the accessibility, effectiveness and cost-effectiveness of group and internet-based mBcT in the reduction of psychological distress in patients with cancer.
Competing interestsThe authors declare they have no competing interests.
Authors’ contributionsAS and mL are the principal investigators who designed the study. FRc and EBI contributed to the design. FRc and EBI are involved in recruiting participants and data collection while EBI takes care of the logistics of the study. FRc drafted this paper, which was modified and supplemented by AS, mL, EA, RD and EBI. RD con-tributed specifically to the statistical analyses and EA contributed to the design of the cost-effectiveness analyses. All authors read and approved the final manuscript.
Author details1 Radboud University Nijmegen Medical Centre, Department of Psychiatry, 6525
EX Nijmegen, The Netherlands2 Helen Dowling Institute, Centre for Psycho-Oncology, Scientific Research
Department, 3723 mB Bilthoven, The Netherlands3 Radboud University Nijmegen Medical Centre, Department for Health Evidence,
6525 EZ Nijmegen, The Netherlands
AcknowledgementsThis research is funded by a grant from Pink Ribbon (2012.WO14.C153) awarded to prof. dr. Anne E.M. Speckens and dr. Marije L. van der Lee.

41
chapter 2
List of abbreviationsTAu Treatment as UsualcBT Cognitive Behavioral TherapyES Effect SizemBcT Mindfulness-Based Cognitive TherapymBSR Mindfulness-Based Stress ReductionHADS Hospital Anxiety and Depression ScalemAAS Mindful Attention and Awareness ScaleI-PANAS-SF International Positive and Negative Affect Scale Short FormScID-I Structural Clinical Interview for DSm-IV Axis I Disorders TiC-P and iMTA questionnaire for Costs associated with Psychiatric illnessesmBI-TAc Mindfulness-Based Interventions – Teacher Assessment CriteriaFcRI Fear of Cancer Recurrence Inventory;mHc-SF Mental Health Continuum – Short FormEQ-5D EuroQol-5 DimensionsSF-12 Short-Form-12NEO-FFI NEO-Five Factor InventoryNEO-PI-R NEO-Personality Inventory-RevisedFFmQ-SF Five Factor Mindfulness Questionnaire – Short FormWAI Working Alliance InventoryGcQ Group Cohesion QuestionnaireIcER Incremental Cost Effectiveness RatioQALY Quality Adjusted Life Year

Tables and captions
Variable goal Measure Target Screening T0 During T0b (tau only) T1 T2 T3
Primary outcome hads Psychological distress
x x x x x x
Secondary outcomes
fcri Fear of cancer recurrence
x x x x x
rrQ Rumination Reflec-tion Questionnaire
x x x x x
mhc-sf Mental Health Continuum – Short Form
x x x x x
Effect predictors scid dsM-iv Axis i disorders
x x x x x
neo-ffi Personalitydimensions
x x
Process measures ffmQ-sf Mindfulness skills x x x x x
Wai Working alliance x
gcQ Group cohesion x
maas Mindfulness skills x
i-Panas-sf Mood x
Calendar Mindfulness adherence
x
Cost-effectiveness TiC-P Health care costs and productivity
x x x x x
EQ-5D Health-related quality of life (preference-based)
x x x x x
sf-12 Health-related quality of life (general health profile)
x x x x x
Table 1 Measurement scheme

Theme of session Meditation exercise Didactic teaching Homework
1. The automatic pilot • Body scan • Intention of participating• Raisin exercise
• Bodyscan• Mindful eating• Mindful routine activity
2. Dealing with barriers • Body scan • Observation exercise ‘walking through the streets’
• Mindfulness of the breath
• Bodyscan or mindfulness of the breath
• Positive experiences diary• Mindful routine acitivity
3. Mindfulness of the breath
• Movement exercises lying down
• Mindfulness of the breath and body
• 3-minutes breathing space
• Body scan or movement exercises
• Negative experiences diary
• 3-minute breathing space three times a day
4. Staying present • Sitting meditation• Walking meditation
• Psycho-education ‘react-ing/responding stress’
• Sitting meditation or walking meditation or movement exercises
• Stress diary• 3-minute breathing space • Walking meditation
5. Allowing • Sitting meditation• Walking meditation
• Psycho-education ‘anxiety, anger and depression, helping and non-helping thoughts’
• Sitting meditation• Mindful communication
exercise • 3-minute breathing space • Walking meditation
6. Mindful communica-tion
• Movement exercises standing up
• 3-minute breathing space in stressful situations
• Psycho-education ‘com-munication’
• Nonverbal (Aikido) and verbal (Deeply listening) communication exercises
• Sitting meditation, movement exercises or body scan
• 3-minute breathing space • Walking meditation
Silence day • Various exercises• Silent lunch and tea
breaks
7. Taking care of yourself • Sitting meditation, open awareness
• 3-minute breathing space
• Energy balance and relapse prevention
• Mindful exercise at will• Relapse prevention plan• 3-minute breathing space
8. From stress to inner strength
• Body scan • Training evaluation and glance at the future
Table 2 Mbct curriculum content

44
Min
dfu
lness-based
cogn
itive therapy fo
r distressed
cancer patien
ts
References
1. OEcD Health Policy Studies - Cancer Care: Assuring quality to improve survival. http://www.oecd.org/els/health-systems/Focus-on-Health_Cancer-Care-2013.pdf. Accessed May 7th 2015
2. Kanker in Nederland tot 2020: Trends en prognoses: KWF Kankerbestrijding 2011.
3. Mitchell AJ, Chan M, Bhatti H, Halton M, Grassi L, Johansen C et al. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies. The Lancet Oncology. 2011;12(2): p.160-174.
4. Mehnert A, Brähler E, Faller H, Härter M, Keller M, Schulz H et al. Four-Week Prevalence of Mental Disorders in Patients With Cancer Across Major Tumor Entities. Journal of Clinical Oncology. 2014;32(31): p. 3540-3546.
5. Segal ZV, Williams JMG, Teasdale JD. Mindfulness-based cognitive therapy for depression: A new approach to relapse pre-vention. New York: Guilford Press; 2002.
6. Kabat-Zinn J. An Outpatient Program in Behavioral Medicine for Chronic Pain Pa-tients Based on the Practice of Mindfulness Meditation - Theoretical Considerations and Preliminary-Results. General Hospital Psychiatry. 1982;4(1): p. 33-47.
7. Teasdale JD, Segal ZV, Williams JMG, Ridgeway VA, Soulsby JM, Lau MA. Prevention of relapse/recurrence in major depression by mindfulness-based cognitive therapy. Journal of Consulting and Clini-cal Psychology. 2000;68(4): p. 615-623.
8. Piet J, Wurtzen H, Zachariae R. The Effect of Mindfulness-Based Therapy on Symptoms of Anxiety and Depression in Adult Cancer Patients and Survivors: A Systematic Review and Meta-Analysis. Journal of Consulting and Clinical Psychology. 2012;80(6): p. 1007-1020.
9. Carlson LE, Doll R, Stephen J, Faris P, Tamagawa R, Drysdale E et al. Random-ized controlled trial of Mindfulness-based cancer recovery versus supportive expressive
group therapy for distressed survivors of breast cancer. Journal of Clinical Oncolo-gy. 2013;31(25): p. 3119-3126.
10. Van Beugen S, Ferwerda M, Hoeve D, Rovers MM, Spillekom-van Koulil S, van Middendorp H et al. Internet-Based Cog-nitive Behavioral Therapy for Patients With Chronic Somatic Conditions: A Meta-Ana-lytic Review. Journal of Medical Internet Research. 2014;16(3):e88.
11. Andersson E, Ljotsson B, Smit F, Paxling B, Hedman E, Lindefors N et al. Cost-ef-fectiveness of internet-based cognitive be-havior therapy for irritable bowel syndrome: results from a randomized controlled trial. Bmc Public Health. 2011;11(1): p. 215.
12. Ban Os-Medendorp H, Koffijberg H, Eland-de Kok PCM, van der Zalm A, de Bruin-Weller MS, Pasmans SGMA et al. E-health in caring for patients with atopic dermatitis: a randomized controlled cost-effectiveness study of internet-guided monitoring and online self-management training. British Journal of Dermatology. 2012;166(5): p. 1060-1068.
13. Cavanagh K, Strauss C, Cicconi F, Grif-fiths N, Wyper A, Jones F. A randomised controlled trial of a brief online mindful-ness-based intervention. Behaviour Re-search and Therapy. 2013;51(9): p. 573-578.
14. Morledge TJ, Emily Fox M, MSSA L. Feasibility of an Online Mindfulness Pro-gram for Stress Management – A Random-ized, Controlled Trial. Annals of Behavior-al Medicine. 2013: p. 1-12.
15. Krusche A, Cyhlarova E, King S, Wil-liams JMG. Mindfulness online: a prelim-inary evaluation of the feasibility of a web-based mindfulness course and the impact on stress. BmJ Open. 2012;2(3) e000803.
16. Zernicke KA, Campbell TS, Speca M, McCabe-Ruff K, Flowers S, Carlson LE. A Randomized Wait-List Controlled Trial of Feasibility and Efficacy of an Online Mind-fulness–Based Cancer Recovery Program: The eTherapy for Cancer Applying Mind-fulness Trial. Psychosomatic Medicine. 2014;76(4): p. 257-267.
17. Wangberg SC, Bergmo TS, Johnsen-AK.

45
chapter 2
Adherence in Internet-based interventions. Patient Preference and Adherence. 2008;2: p. 57-65.
18. Eysenbach G. Issues in evaluating health websites in an Internet-based randomized controlled trial. Journal of Medical Inter-net Research. 2002;4(3):E17
19. Everts FZB, van der Lee ML, de Jager Meezenbroek E. Web-based individual Mindfulness-Based Cognitive Therapy for cancer-related fatigue – A pilot study. Inter-net Interventions. 2015;2(2): p. 200-13.
20. Ogrodniczuk JS, Piper WE, Joyce AS, McCallum M, Rosie JS. NEO-five factor personality traits as predictors of response to two forms of group psychotherapy. Interna-tional Journal of Group Psychotherapy. 2003;53(4): p. 417-42.
21. Gu J, Strauss C, Bond R, Cavanagh K. How do mindfulness-based cognitive ther-apy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clinical Psychology Review. 2015;37: p. 1-12.
22. Cook JE, Doyle C. Working alliance in online therapy as compared to face-to-face therapy: Preliminary results. CyberPsychol-ogy & Behavior. 2002;5(2): p. 95-105.
23. Segal ZV, Williams JMG, Teasdale JD. Mindfulness-based cognitive therapy for depression. Guilford Press; 2012.
24. uK Network for Mindfulness-Based Teachers Good practice guidelines for teaching mindfulness-based courses. http://mindfulnessteachersuk.org.uk/pdf/teacher-guidelines.pdf. Accessed 31st of March 2015.
25. Crane RS, Kuyken W, Williams JMG, Hastings RP, Cooper L, Fennell MJV. Competence in Teaching Mindfulness-Based Courses: Concepts, Development and Assess-ment. Mindfulness. 2012;3: p. 76-84.
26. Hambleton RK. Guidelines for Adapting Educational and Psychological Tests: A progress report. European Journal of Psychological Assessment (Bulletin of the International Test Commission) 1994;10: p. 229-244.
27. Zigmond AS, Snaith RP. The hospital anx-iety and depression scale. Acta Psychiatrica Scandinavica. 1983;67(6): p. 361-70.
28. Spinhoven P, Ormel J, Sloekers PP, Kempen GI, Speckens AE, Van Hemert AM. A validation study of the Hospital Anx-iety and Depression Scale (HADS) in differ-ent groups of Dutch subjects. Psychological Medicine. 1997;27(2): p. 363-370.
29. Le Fevre P, Devereux J, Smith S, Lawrie SM, Cornbleet M. Screening for psychiatric illness in the palliative care inpatient setting: a comparison between the Hospital Anxiety and Depression Scale and the General Health Questionnaire-12. Palliative Medi-cine. 1999;13(5): p. 399-407.
30. Akechi T, Okuyama T, Sugawara Y, Shima Y, Furukawa TA, Uchitomi Y. Screening for depression in terminally ill cancer patients in Japan. Journal of Pain and Symptom Management. 2006;31(1): p. 5-12.
31. Bjelland I, Dahl AA, Haug TT, Neck-elmann D. The validity of the Hospital Anxiety and Depression Scale: an updated literature review. Journal of Psychosomat-ic Research. 2002;52(2):69-77.
32. Herrmann C. International experiences with the Hospital Anxiety and Depres-sion Scale-a review of validation data and clinical results. Journal of Psycho-somatic Research. 1997;42(1): p. 17-41.
33. Simard S, Savard J. Fear of Cancer Recur-rence Inventory: development and initial validation of a multidimensional measure of fear of cancer recurrence. Supportive Care in Cancer. 2009;17(3): p. 241-51.
34. Trapnell PD, Campbell JD. Private self-consciousness and the five-factor model of personality: distinguishing rumination from reflection. Journal of Personality and Social psychology. 1999;76(2): p. 284-304.
35. Luyckx K, Schwartz SJ, Berzonsky MD, Soenens B, Vansteenkiste M, Smits I et al. Capturing ruminative exploration: Extending the four-dimensional model of identity formation in late adolescence. Journal of Research in Personality. 2008;42(1): p. 58-82.

46
Min
dfu
lness-based
cogn
itive therapy fo
r distressed
cancer patien
ts
36. Keyes CL. Mental illness and/or mental health? Investigating axioms of the complete state model of health. Journal of Consulting and Clinical psychology. 2005;73(3): p. 539-548.
37. Lamers S, Westerhof GJ, Bohlmeijer ET, ten Klooster PM, Keyes CL. Evaluating the psychometric properties of the Mental Health Continuum-Short Form (mHc-Sf). Journal of Clinical Psychology. 2011;67(1): p. 99-110.
38. Tan SS, Bouwmans-Frijters CA, Hak-kaart-van Roijen L. Handleiding voor kostenonderzoek: methoden en referentie-prijzen voor economische evaluaties in de gezondheidszorg. Tijdschrift voor Gezondheidswetenschappen. 2012;90(6): p. 367-72.
39. Hakkaart-van Roijen L, Tan S, Bouw-mans C. Handleiding voor kostenonderzoek: Methoden en standaard kostprijzen voor economische evaluaties in de gezondheids-zorg. College voor zorgverzekeringen; 2010.
40. The EuroQol Group. EuroQol – a new facility for the measurement of health-re-lated quality of life. The EuroQol Group. Health Policy. 1990;16(3): p. 199-208.
41. Lamers L, Stalmeier P, McDonnell J, Krabbe P, Van Busschbach J. Kwaliteit van leven meten in economische evaluaties: het Nederlands EQ-5D-tarief. Neder-lands Tijdschrift voor Geneeskunde. 2005;149(28): p. 1574-1578.
42. Ware Jr JE, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Medical Care. 1996;34(3): p. 220-233.
43. Johnson JA, Coons SJ. Comparison of the EQ-5D and SF-12 in an adult US sample. Quality of Life Research. 1998;7(2): p. 155-166.
44. First MB, Spitzer RL, Gibbon M, Williams JB. Structured Clinical Interview for DSm-IV® Axis I Disorders (ScID-I), Clinician Version, Administration Booklet. American Psychiatric Pub; 2012.
45. Costa PT, McCrae RR. Normal personality
assessment in clinical practice: the NEO Personality Inventory. Psychological As-sessment. 1992;4(1): p. 5-13.
46. Hoekstra HA, Ormel J, de Fruyt F. Handleiding NEO Persoonlijkheids-vragen-lijsten NEO-PI-R en NEO-ffI. Lisse, The Netherlands: Swets Test Services; 1996.
47. Bohlmeijer E, Peter M, Fledderus M, Vee-hof M, Baer R. Psychometric properties of the Five Facet Mindfulness Questionnaire in depressed adults and development of a short form. Assessment. 2011;18(3): p. 308-320.
48. Brown KW, Ryan RM. The benefits of being present: Mindfulness and its role in psychological well-being. Journal of Per-sonality and Social Psychology. 2003;84: p. 822-48.
49. Carlson LE, Brown KW. Validation of the Mindful Attention Awareness Scale in a can-cer population. Journal of Psychosomatic Research. 2005;58(1): p. 29-33.
50. Schroevers M, Nykliček I, Topman R. Validatie van de nederlandstalige versie van de Mindful Attention Awareness Scale (mAAS). Gedragstherapie. 2008;1(3): p. 225-40.
51. Thompson ER. Development and valida-tion of an internationally reliable short-form of the positive and negative affect schedule (PANAS). Journal of Cross-Cultural Psy-chology. 2007;38(2): p. 227-242.
52. Horvath AO, Greenberg LS. Development and validation of the Working Alliance In-ventory. Journal of Counseling Psycholo-gy. 1989;36(2): p. 223-233.
53. Stinckens N, Ulburghs A, Claes L. De werkalliantie als sleutelelement in het therapiegebeuren: Meting met behulp van de WAV-12, de Nederlandstalige verkorte versie van de Working Alliance Inventory. Tijdschrift voor Klinische Psychologie. 2009;39: p. 44-60.
54. Hatcher RL, Gillaspy JA. Development and validation of a revised short version of the Working Alliance Inventory. Psycho-therapy Research. 2006;16(1): p. 12-25.
55. Janse P, Boezen-Hilberdink L, van Dijk MK, Verbraak MJPM, Hutschemaekers GJM. Measuring feedback from clients:

47
chapter 2
The psychometric properties of the Dutch Outcome Rating Scale and Session Rating Scale. European Journal of Psychological Assessment. 2014;30(2): p. 86-92.
56. May AM, Duivenvoorden HJ, Korstjens I, van Weert E, Hoekstra-Weebers JE, van den Borne B et al. The effect of group cohesion on rehabilitation outcome in cancer survivors. Psycho-Oncology. 2008;17(9): p. 917-925.
57. Trijsburg R, Bogaerds H, Letiche M, Bidzjel L, Duivenvoorden H. De ontwik-keling van de Group Cohesion Questionnaire (GcQ). Universiteit van Amsterdam/ Erasmus Universiteit Rotterdam: Am-sterdam/ Rotterdam; 2004.
58. Shennan C, Payne S, Fenlon D. What is the evidence for the use of mindfulness-based interventions in cancer care? A review. Psy-cho-Oncology. 2011;20(7): p. 681-97.
59. Van Aalderen J, Donders A, Giommi F, Spinhoven P, Barendregt H, Speckens A. The efficacy of mindfulness-based cognitive therapy in recurrent depressed patients with and without a current depressive episode: a randomized controlled trial. Psychological Medicine. 2012;42(5): p. 989-1001.
60. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and com-paring indirect effects in multiple mediator models. Behavior Research Methods. 2008;40(3): p. 879-91.
61. MacKinnon DP. Introduction to Statistical Mediation Analysis. Erlbaum Psych Press: London.; 2008.
62. Efron B. Better Bootstrap confidence inter-vals. Journal of the American statistical Association. 1987;82(397): p. 171-185.
63. Hakkaart-van Roijen L, Straten Av, Tie-mens B, Donker M. Handleiding Trimbos/iMTA questionnaire for Costs associated with Psychiatric illness (TiC-P). Institute of Medical Technology Assessment (iMTA)2002.
64. Carlson LE, Bultz BD. Efficacy and med-ical cost offset of psychosocial interventions in cancer care: making the case for economic analyses. Psycho-Oncology. 2004;13(12): p. 837-49.

48

Chapter 3
Face-to-face and individual internet-based Mindfulness-Based Cognitive Therapy compared to Treatment As Usual in reducing psychological distress in cancer patients: a multicentre randomized controlled trial
This chapter has been published as:
F.R. Compen*, E.M. Bisseling*, M.P.J. Schellekens, A.R.T. Donders, L.E. Carlson, M.L. Van der Lee**, A.E.M. Speckens** Journal of Clinical Oncology (2018) 36.23: 2413-2421
*Shared first authorship**Shared last authorship
Acknowledgement of research support: This study is funded by breast cancer foundation Pink Ribbon (2012.WO14.C153)

50
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
abstract
purpose Mindfulness-Based Cognitive Therapy (mBcT) has been shown to alleviate psychological distress in cancer patients. However, patients experience barriers in participating in face-to-face mBcT. Individual internet-based mBcT (emBcT) could be an alternative. The study aim was to compare mBcT and emBcT to treatment as usual (TAu) for psychological distress in cancer patients.
Methods We included obtained ethical and safety approval to include 245 cancer patients with psychological distress (≥ 11 on the Hospital Anxiety and Depression Scale (HADS)) in the study. They were randomly allocated to mBcT (n=77), emBcT (n=90) or TAu (n=78). Patients completed baseline (T0) and post-intervention (T1) assessments. The primary outcome was psychological distress on the HADS. Sec-ondary outcomes were psychiatric diagnosis, fear of cancer recurrence, rumina-tion, health-related quality of life, mindfulness skills and positive mental health. Continuous outcomes were analyzed using Linear Mixed Modeling on the inten-tion-to-treat sample. Since both interventions were compared to TAu, the type I error rate was set to p<.025.
results Compared to TAu, patients reported significantly less psychological distress after both mBcT (Cohen’s d =.43, p <.001) and emBcT(Cohen’s d=.63, p <.001) . In addition, Post-treatment prevalence of psychiatric diagnosis was lower in both mBcT (33% improvement; p=.030) and emBcT (29%, p=.076) in comparison with TAu (16%), but these changes were not statistically significant. Both interventions reduced fear of cancer recurrence, rumination and increased mental health-related quality of life, mindfulness skills and positive mental health compared to TAu (all p-values <.025). Physical health-related quality of life did not improve (p=.343).
conclusion Compared to TAu, mBcT and emBcT are similarly effective in reducing psychological distress in a sample of distressed heterogeneous cancer patients.

51
introduction
From 2025 onwards, 20 million people worldwide will be diagnosed with cancer each year.1 About one third of cancer patients suffer from significant psychological distress2, resulting in reduced quality of life, decreased compliance with medical care and prolonged duration of hospital stay.3,4 The prevalence of psychiatric dis-orders in oncological settings is 30 to 40%.3 Effective and accessible interventions are needed to reduce psychological distress and psychiatric disorders in cancer patients. Mindfulness-based interventions (mBIs)5,6 such as Mindfulness-Based Cognitive Therapy (mBcT) teach participants to be more mindful in daily life through medi-tation exercises, yoga, group discussions and didactic teaching.5 A 2012 meta-anal-ysis of randomized controlled trials (RcTs) of mBIs in 955 cancer patients found significant improvements in depressive and anxiety symptoms.7 Since then, a number of RcTs have confirmed this.8-13
However, as mBIs typically require in-person attendance at classes over sever-al weeks, many cancer patients experience barriers to participation. These may include impairments due to illness and anticancer treatments, side-effects which results in advice to avoid groups of people, or limited transportation options.14 Consequently, uptake of face-to-face interventions for cancer patients has been lower than, for instance, telephone-based interventions.15
In contrast, internet-based interventions are easily accessible and save travel-ling time.16 Therapist-guided internet interventions have been shown effective for psychiatric and somatic conditions.17 Although evidence for internet-based mBIs (emBIs) in cancer is scarce, one controlled study of 62 patients found synchronous videoconferencing sessions led to significant improvements in mood, stress symp-toms and mindfulness skills18, In addition, an uncontrolled cohort of 257 fatigued patients showed significant improvements in fatigue and psychological distress after individual emBcT.19
To date, no study has simultaneously compared the effectiveness of both mBcT and emBcT to treatment as usual (TAu). The primary aim of this RcT was to investi-gate whether mBcT and emBcT were each superior to TAu in reducing psychological distress in a sample of distressed cancer patients. Moreover, we hypothesized a reduction of psychiatric diagnosis, fear of cancer recurrence and rumination and an improvement in health-related quality of life, mindfulness skills and positive mental health in both interventions compared to TAu. We explored modera-tors of intervention dropout and outcome in the interventions: sex, age, cancer diagnosis, anticancer treatment intent, psychiatric diagnosis, neuroticism, and therapist.
chapter 3

52
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Patients and methods
trial designA three-armed multicentre, parallel group RcT was conducted to compare the effectiveness of mBcT and emBcT to TAu in reducing psychological distress in cancer patients. Anticipated dropout rates were 15% in mBcT and TAu, and 30% in emBcT.19 Given the anticipated dropout rates, the allocation ratio was 1:1.2:1. Patients randomized to TAu were secondarily randomized to mBcT or emBcT, to be received after the TAu period of three months. The study was approved by the ethical review board of the Radboud University Medical Center (cmO Arn-hem-Nijmegen 2013/542).All centers provided local ethics approval. The study was registered on Clinicaltrials.gov (NCT02138513) shortly after the start of recruitment, reported following cONSORT guidelines20 and a protocol paper was published in advance.21
participantsInclusion criteria were: a) a cancer diagnosis, any tumor type or stage, at any time, on or off treatment; b) a score of ≥ 11 on the HADS; c) computer literacy and internet access; d) ability to participating in both mBcT and emBcT; and e) good command of the Dutch language. Exclusion criteria were: a) severe psychiatric morbidity such as suicidal ideation and/or current psychosis; b) change in psychotropic medica-tion within a period of three months prior to baseline; c) previous participation in ≥ 4 sessions of an mBI.
procedurePatients were recruited from April 2014 to December 2015 via healthcare profes-sionals in six centres (n=64, 26%), via online media (n=49, 20%), offline media (n=44, 18%), patient associations (n=43, 18%) and peers (n=27, 11%). Eighteen patients (7%) could not remember how they heard about the study. Interested patients filled out the HADS on the research website. Patients with HADS ≥11 received a phone call from one of the researchers during which the remaining inclusion and exclusion criteria were assessed. Once patients provided oral and written consent and had completed the baseline assessment, they were randomized to mBcT, emBcT or TAu and informed about their allocation by EB.
interventionFace-to-face MBCT
The mBcT protocol6 was tailored to cancer patients by including cancer-related psycho-education and adapted movement exercises. The mBcT consisted of eight weekly 2.5h group sessions, a six-hour silent day and daily home practice assign-

53
ments guided by audiofiles. Each participant in both interventions received a folder with information on each session.
eMBCTThe emBcT was delivered individually and included weekly asynchronous written interaction with a therapist over email. Patients were granted access to a secure website containing material for eight weeks + a silent day and an inbox. Each session included an introduction and daily meditation exercises with meditation audio files. Patients were asked to practice and fill out practice dia-ries on a daily basis. They were provided with (fictional) patients’ descriptions to emphasize common experiences and clarify the use of the diaries. Patients were given written instructions after week 5 to prepare for their silent day at home. In the week of the silent day, patients were provided with a programme similar to the mBcT silent day. At the end of the silent day, emBcT patients wrote about their experiences in an essay. The therapist provided written feedback on the completed forms and the essay via the secured inbox on a pre-arranged day of the week. Having completed four or more sessions of mBcT was defined as a minimum adequate dose in both interventions.22
TAUTAu consisted of all healthcare patients usually receive. Except for not partici-pating in mBIs during the study period, there were no restrictions on healthcare utilization. Data on healthcare utilization were gathered using the Trimbos/iMTA questionnaire for Costs associated with Psychiatricillnesses (TiC-P).23
therapistsFourteen therapists participated: n=7 provided both interventions, n=2 only pro-vided mBcT and n=5 only emBcT. All therapists fulfilled the criteria of the uK Mindfulness-Based Teacher Therapist Network Good Practice Guidelines for teaching mBIs.24 Three full-day supervision meetings were held during the inter-vention phase of the trial. All face-to-face mBcT sessions were videotaped to eval-uate therapist competency using the Mindfulness-Based Interventions-Teachers Assessment Criteria (mBI:TAc).25 Therapist competency levels were determined by two independent therapists who evaluated two random sessions from each of the nine therapists providing face-to-face mBcT (who treated 80.8% of all patients receiving either intervention). Interrater-reliability was .72. Of the nine therapists rated, four were considered proficient (n=64 patients), three competent (n=64 patients) and two beginner (n=7 patients).
chapter 3

54
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
MeasuresPrimary Outcome
Psychological distress was measured with the HADS, a 14-item self-report scale designed to assess anxiety and depression in medical outpatients.26,27 It has good psychometric properties in the general medical population, including cancer patients in palliative care.28 The internal consistency in this sample was high (α =.87).
Secondary OutcomesPsychiatric diagnosis was assessed by the ScID-I.29 The ScID-I was administered by trained interviewers following or having completed a Master in Behavioral Science (Fc), supervised by either an experienced psychiatrist (EB and AS) or psychologist (mL). All interviews were audio taped. Fear of cancer recurrence was assessed with the severity subscale of the Fear of Cancer Recurrence Inventory (FcRI).30, 31 Rumination was measured by the rumination subscale of the Rumination and Reflection Ques-tionnaire (RRQ),32 health-related quality of life by the mental and physical scales of the Short-Form 12 (SF-12)33 using Dutch norm scores from a clinical sample,34 mindfulness skills by the Five Facet Mindfulness Questionnaire Short Form (FFmQ-SF)35 and positive mental health by the Mental Health Continuum-Short Form (mHc-SF).36 As a potential moderator, neuroticism was measured by the Neuroticism Extraversion Openness-Five Factor Inventory (NEO-FFI).37 Further details of the measures used are included in the study protocol.21
saMple s izeThe sample size calculation was based on previous post-intervention HADS scores of cancer patients who received mBcT at the Helen Dowling Institute (M=10.6, SD=6.4) compared to those who had not (M=14.8, SD=8.1). With 90% power, n=65 patients per condition were needed. Due to anticipated differential dropout rates between treatment arms, the recruitment target was n=245: n=76 in each of mBcT and TAu, and n=93 in emBcT.
randoMization and blindingOnce patients provided oral and written consent and completed the baseline assessment, they were randomized to mBcT, emBcT or TAu by a computer-gener-ated allocation sequence designed by an independent biostatistician. This custom software was accessed by researcher EB via a study-specific website. Randomization was carried out with a fixed block size of sixteen stratified for region and minimized for sex, cancer diagnosis (breast vs. other) and anticancer treatment intent (cura-tive vs. palliative). After randomization, EB informed patients of their allocation by email. EB planned and invited participants for the follow-up assessments, the standardised psychiatric interviews were conducted by Fc and research assistants

55
who were blind to treatment allocation. Both EB and Fc instructed patients not to mention their treatment condition at the beginning of each psychiatric interview.
statistical analysisStatistical analyses were carried out using SPSS22 (IBm). Differences between con-ditions in demographic and clinical variables were tested by chi-square analysis and t-tests. Continuous outcomes were analyzed with linear mixed modeling in a model with uncorrelated residual errors and random intercepts, including group allocation and its interaction with time and stratification (region) and minimization (sex, cancer diagnosis, anticancer treatment intent) variables as fixed factors. Since both mBcT and emBcT were compared to TAu, the two-sided type I error rate was corrected to .025 for the two direct (e)mBcT comparisons with TAu. All reported analyses used the Intent-To-Treat (ITT) sample. Missing continuous outcomes were imputed with Automatic Multiple Imputation (mI) on basis of linear regression (20 iterations). The multiple imputation-dataset was considered the primary dataset. Cohen’s d effect size (ES) were calculated using post-intervention means and baseline pooled SD’s. These statistics are commonly used in psychological contexts to com-pare effect sizes across studies38 and in accordance with Cohens’ guidelines, Cohens’s d effect sizes were interpreted as small (0.2 to 0.5), medium (0.5 to 0.8) or large (>0.8).39
In addition, the Reliable Change Index (RcI) was calculated by dividing the observed difference score by the standard error of measurement. Each participant was categorized as improved (RcI <-1.96), no change (-1.96 to 1.96) or deteriorated (RcI >1.96).40 Improvements in terms of psychiatric diagnosis and RcI were assessed using chi-square analyses. Exploratory moderation analyses of dropout were done using logistic regression including an interaction term between completer (yes/no) and possible modera-tors: sex, age, cancer diagnosis, anticancer treatment intent, psychiatric diagno-sis, neuroticism, and therapist. Exploratory moderation analyses of the primary outcome were done by including a three-way interaction term between condition, time and possible moderators: sex, age, cancer diagnosis, anticancer treatment intent, psychiatric diagnosis, neuroticism, and therapist. First, moderators were assessed in two separate analyses of either intervention compared to TAu. Second, moderators were assessed in analyses of the two intervention conditions only.
results
study saMpleIn total, 532 patients were screened with the HADS (see Figure 1), of which 98 (18.4%) were excluded for scoring below 11. Of 434 patients who were contacted by tele-phone, 24 (5.5%) were excluded because of previous experience with mindfulness, 22
chapter 3

56
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
(5.1%) could not be contacted and 95 (21.9%) declined participation due to possible travelling distance (55, 12.7%), strong randomization preference (12 (2.8%), of which 4 had a preference for emBcT and 8 for in-person group mBcT, and scheduling difficulties (11, 2.5%). Of the remaining 293 patients, another 10 (3.4%) could not be contacted and 38 (13.0%) declined participation after the baseline assessment. There were no significant differences in mean HADS scores between the 133 decliners (M=20.4, SD=5.6) and those who were randomized (M=20.6, SD=6.2). In total, 245 cancer patients were randomly assigned to mBcT (n=77), emBcT (n=90) or TAu (n=78). The three conditions did not differ in terms of baseline demographic or clinical characteristics (see Table 1). The number of months between baseline and post-intervention assessments did not differ between mBcT (M=5.4, SD=2.3) and emBcT (M=5.9, SD =1.8) (p =.13), but was higher in both intervention conditions than in TAu (M=3.5, SD=0.9) (p <.001). Seventy out of 77 (90.9%) patients started mBcT and 71 (%) completed four or more sessions (M=7.9, SD=1.3) (see Figure 1). Eighty-two out of 90 (91.1%) patients started emBcT and 71 completed four or more session (M=8.6, SD=12). The amount of estimated daily minutes of mindfulness practice did not differ significantly between mBcT (n=56, M=30.6, SD=26.0) and emBcT (n=70, M=28.7, SD=29.3) (p = .69). Dropouts from the interventions were significantly higher in the emBcT than in the mBcT group: (χ2(1, n = 167) = 3.92, p = .047). Non-response on the post-treatment assessment was substantial (16.9% in mBcT, 16.7% in emBcT and 10.3% in TAu) but did not differ significantly between conditions (p = .41). Non-responders were more often female (p=.033) and had less education (p=.037) than responders.
healthcare util izationThere were no significant differences in healthcare utilization between the inter-vention conditions and TAu (see Table 4) except for the proportion of patients receiving day-ward treatment (e.g. chemotherapy), which was higher in TAu.
safetyA total of (n=21) (S)AEs unrelated to the intervention were reported in mBcT (n=6), in emBcT (n=9) and TAu (n=6), see Table S1 (Online only). One SAE occurred during the study period: a patient died after randomization due to illness.
intervention outcoMesIn between-groups comparisons of both interventions compared to TAu, patients in the mBcT and emBcT conditions reported significantly less psychological distress post-intervention than those receiving TAu, with small to medium effect sizes (Cohen’s d =.43 and .63, respectively) (see Table 2). The proportion of patients demonstrating reliable improvement was significantly greater in mBcT than TAu

57
(36% vs. 14%, χ2(1, n = 134) = 8.44, p = .004)) and in emBcT than TAu (37% vs. 14%, χ2(1, n = 145) = 9.95, p = .002)). Improvement in rates of psychiatric diagnosis favoured both interventions compared to TAu but were not statistically significant (mBcT: 32% vs. 16%, χ2(1, n = 126) = 4.73, p = .030) and emBcT: 29% vs. 16%, χ2(, n = 138) = 3.15, p = .076)). Compared to TAu, both mBcT and emBcT significantly reduced fear of can-cer recurrence (d=.29 and .53) rumination (d=.42 and .52) and improved mental health-related quality of life (d=.56 and .70) but not physical health-related quality of life (d=.33 and .24). They also resulted in better mindfulness skills (d=.46 and .84) and increased positive mental health compared to TAu (d=.11 and .44, respectively).
ModerationExploratory analyses yielded no significant moderation of intervention dropout or primary outcome in the analyses comparing both interventions to TAu separately (all p-values >.05), except for neuroticism. In the analyses comparing either mBcT interventions to TAu, there was a significant interaction between neuroticism and intervention condition (mBcT vs. TAu p = .014, emBcT vs. TAu p = .004). Patient scoring higher on neuroticism on baseline improved more on psychological dis-tress in both intervention conditions than in TAu.
discussion
This is the first study to simultaneously compare mBcT and emBcT with TAu in a large sample of distressed heterogeneous cancer patients. Both mBcT and emBcT resulted in a statistically significant and clinically reliable reduction of psychological distress compared to TAu. Both interventions demonstrated similar reductions of fear of cancer recurrence, rumination, and improvements in mental (but not physical) health-related quality of life, mindfulness skills and positive mental health compared to TAu. Our study confirms previous findings regarding the effectiveness of emBIs for cancer patients.19,41 Although the group-based setting is considered important for mBIs,42 the current study suggests that individual guided emBcT with limited teacher feedback is also effective, thus improving the accessibility of this inter-vention for cancer patients. However, emBcT did result in higher dropout rates than mBcT. Exploratory analyses did not yield any moderators of intervention dropout. Further, possibly qualitative, research examining reasons for dropout is critical to improve efficacy of web-based interventions.43
A strength of the current study is the patient-centred nature of the recruitment across multiple regions as in previous research we encountered difficulties with consecutive sampling of patients in hospital outpatient settings.44 Other strengths
chapter 3

58
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
are that the interventions followed strict protocols, was delivered by qualified therapists, and therapist competency was rated by two independent, experienced therapists. We systematically collected data on healthcare utilization during the study. The study used a broad array of outcome measures, including both observer- rated interviews and self-report questionnaires. In addition to these strengths, the study has some limitations. The study was not powered to directly compare or determine non-inferiority of emBcT to mBcT, as this would have required a larger sample size. As with other psycho-oncology research, the majority of the patients were middle-aged breast cancer patients. Although this is in line with the characteristics of cancer patients seeking psy-chosocial support,45 this might limit generalizability to patients with other types of cancer. As one inclusion criterion was the ability and willingness to attend both mBcT and emBcT, the sampling frame for the current study was probably not representative of patients who would prefer emBcT in clinical practice. As treatment preference is often positively correlated with treatment outcome,46 we would expect that this RcT under- rather than over-estimated the effects of emBcT. In terms of research implications, long-term results should be gathered to examine the stability of effects. In addition, data on cost-utility of mBIs in can-cer patients should be collected47. Internet interventions do not involve costs of transportation, travelling time, space, equipment, cleaning, and other overhead costs and thus could be more cost effective. Possible mediators of the effect, such as mindfulness skills or rumination, should be further investigated.48,49 Moreover, mediation analyses could also examine possible differences in adherence in both mBcT and emBcT. In terms of clinical implications, implementation of emBcT could make mBIs more accessible for cancer patients without having to compromise intervention efficacy. However, intervention dropout could possibly be improved by the delivery mode of emBIs.50 Qualitative work demonstrates that aspects such as the individ-ual nature and the asynchronous interaction of the current emBcT is helpful for somepatients.51
Future studies should assess how different emBcT designs (e.g. blended designs combining the advantages of face-to-face and internet-based elements)52 could further improve intervention accessibility, adherence and effectiveness.51

59
AcknowledgmentsWe are grateful to the patients for their participation in this trial and to physicians and therapists from Radboud University Medical Centre, Nijmegen; Helen Dowl-ing Institute, Bilthoven; De Vruchtenburg, Leiden/Rotterdam; Ingeborg Douwes Centrum, Amsterdam; Het Behouden Huys, Haren; Jeroen Bosch Ziekenhuis, Den Bosch for referring patients to the trial. We would like to thank Ms. Heidi Willemse, Eva Witteveen, Merel Brands and Mr. David Huijts for their help in data collection; Ellen Jansen, Rinie van den Boogaart, Coen Völker, Joyce Vermeer, Bert Vedder, Ineke Vogel, Mira Reus, Lot Heijke, Maria van Balen, Annetje Brunner, Maya Schroevers, Stephanie Verhoeven and Janine Mutsaers for providing the online and group mBcT. We would like to thank Caroline Hoffman for her contribution to the supervision of the therapists. Linda E. Carlson holds the Enbridge Research Chair in Psychosocial Oncology, co-funded by the Canadian Cancer Society Albert/NWT Division and the Alberta Cancer Foundation.
Conflicts of interestNone declared
Author contributionsConception and design: Anne Speckens, Marije van der Lee Data acquisition: Else Bisseling, Félix CompenData analysis and interpretation: All authors. Drafting of manuscript: Félix Compen, Else BisselingCritical revision: All authors.
chapter 3

60
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
List of abbreviationsRcT Randomized Controlled TrialmBI Mindfulness-based interventionmBcT Mindfulness-Based Cognitive TherapyemBI Internet-Based Mindfulness-Based InterventionTAu Treatment As UsualHADS Hospital Anxiety and Depression ScaleemBcT Internet-based Mindfulness-based Cognitive TherapymBI:TAc Mindfulness-Based Interventions: Teachers Assessment CriteriaFcRI Fear of Cancer Recurrence Inventory RRQ Rumination Reflection Questionnaire SF-12 Short Form-12FFmQ-SF Five Facet Mindfulness Questionnaire - Short Form mHc-SF Mental health Continuum - Short FormNEO-FFI Neuroticism-Extraversion-Openness Five-Factor InventoryScID-I Structured Clinical Interview for DSm-IV-TR Axis I disorders ITT Intention to treatmI Multiple Imputation RcI Reliable Change Index ES Effect Size

61
Figure 1 consort diagram (n=245) ch
apter 3
Declined after baseline (n=38)Strong randomization preference (n=12)
Scheduling difficulties (n=11)Not interested after baseline (n=15)
Unreachable (n=10)
Declined after screening (n=95)Travel distance (n=55)
Unknown / no reason provided (n=18)Other services needed (n=12)
Physical limitations (n=10)
Unreachable (n=22)Excluded (n=24)
Experience with mindfulness (n=21)Severe psychiatric morbidity (n=3)
Screened(n=532)
Eligible(n=434)
Baseline assessment
(n=293)
Randomized(n=245)
Internet-basedMbct
(n=90, 36.7%)
Group-basedMbct
(n=77, 31.4%)
Treatment as usual
(n=78, 31.8%)
CompletedInternet-based
Mbct(n=63, 70.0%)
CompletedGroup-based
Mbct(n=64, 83.1%)
CompletedTreatment as
usual(n=77, 98.7%)
Completed T1assessment
(n=75, 83.3%)
Completed T1assessment
(n=64, 83.1%)
Completed T1assessment
(n=70, 89.7%)
Not started (n=7, 9.1%)
Scheduling (n=2)Group unavailable (n=2)
Medical reason (n=1)Other intervention (n=1)
Deceased (n=1)
Not started(n=8, 8.9%)
Other intervention (n=4)No reason provided (n=2)
Medical reason (n=1)Computer difficulties (n=1)
Not started(n=0)
Discontinued(< 4 sessions)(n=6, 7.8%)
No motivation (n=2)Medical reason (n=2)
Too burdensome (n=1)Mbct experience (n=1)
Discontinued (< 4 sessions)(n=9, 21.1%)
No motivation (n=6)No reason provided (n=2)
Medical reason (n=2)Scheduling (n=3)
Too burdesome (n=3)Computer difficulties (n=3)
Discontinued(n=1, 1.3%)
Mbct during tau (n=1)
Lost to follow up(n=13, 16.9%)
No reason provided (n=5)Withdrawal (n=4)
Medical reason (n=1)Authors’ mistake (n=1)
Deceased (n=1)
Lost to follow up(n=15, 16.7%)
No reason provided (n=8)Withdrawal (n=6)
Medical reason (n=1)
Lost to follow up(n=8, 10.3%)
No reason provided (n=4)Withdrawal (n=3)
Medical reason (n=1)
Ineligible (n=98)hads too low (n=98)

Characteristic All Mbct eMbct tau p
n=245 n=77 n=90 n=78
n (%) n (%) n (%) n (%)
Sex .912
Female 210 (85.7) 67 (87.0) 77 (85.6) 66 (84.6)
Male 35 (14.3) 10 (13.0) 13 (14.4) 12 (15.4)
Age, years .464
Mean 51.7 52.1 52.4 50.4
SD 10.7 11.4 10.7 9.9
Married / in a relationship .491
Yes 202 (82.4) 65 (84.4) 76 (84.4) 61 (78.2)
No 43 (17.6) 12 (15.6) 14 (15.6) 17 (21.8)
Children .314
Yes 169 (69.0) 48 (62.3) 65 (72.2) 56 (71.8)
No 76 (31.0) 29 (37.7) 25 (27.8) 22 (28.2)
Education .451
High 166 (67.8) 54 (70.1) 56 (62.2) 56 (71.8)
Middle 77 (31.4) 22 (28.6) 34 (37.8) 21(26.9)
Low 2 (0.8) 1 (1.3) 0 1(1.3)
Diagnosis .724
Breast cancer 151 (61.6) 53 (68.8) 53(58.9) 45 (57.7)
Gynecological cancer 18 (7.3) 2 (2.6) 9 (10.0) 7 (9.0)
Prostate cancer 16 (6.5) 6 (7.8) 7 (7.8) 3 (3.8)
Colon cancer 12 (4.9) 4 (5.2) 4 (4.4) 4 (5.1)
Non-hodgkin’s lymphoma 11 (4.5) 1 (1.3) 3 (3.3) 7 (9.0)
Skin cancer 5 (2.0) 1 (1.3) 3 (3.3) 1 (1.3)
Thyroid cancer 4 (1.6) 1 (1.3) 1 (1.1) 2 (2.6)
Bladder cancer 4 (1.6) 1 (1.3) 2 (2.2) 1(1.3)
Neuroendocrine tumor 4 (1.6) 1 (1.3) 2 (2.2) 1 (1.3)
Other 20 (8.2) 7 (9.1) 6 (6.7) 7 (9.0)
Years since diagnosis .616
Mean 3.5 3.9 3.3 3.2
SD 4.7 5.7 4.0 4.3
Anticancer treatment intent .472
Curative 206 (84.1) 68 (88.3) 74 (82.2) 64 (82.1)
Palliative 39 (15.9) 9 (11.7) 16 (17.8) 14 (17.9)
Current treatment .694
None 133 (53.1) 43 (55.8) 49 (54.4) 41 (52.6)
Table 1 Baseline Sociodemographic and Clinical Characteristics (n=245).

Characteristic All Mbct eMbct tau p
n=245 n=77 n=90 n=78
n (%) n (%) n (%) n (%)
Hormone therapy 79 (32.2) 22 (28.6) 28 (31.1) 29 (37.2)
Combination of treatments 12 (4.9) 4 (5.2) 4 (4.4) 4 (5.1)
Immunotherapy 9 (3.7) 1 (1.3) 5 (5.6) 3 (3.8)
Radiotherapy 8 (3.3) 5 (6.5) 3 (3.3) 0
Chemotherapy 4 (1.6) 2 (2.6) 1 (1.1) 1 (1.3)

Table 2 Mean scores at baseline and post-intervention (both listwise deletion and pooled multiple imputation scores are depicted) and between group differences for primary and secondary outcome measures
aSince both Mbct and eMbct were compared to tau, the two-sided type i error rate was corrected to .025bse for imputed means
Groups Linear Mixed Modeling: Between-group differences
Mbct eMbct tau pa tau-Mbct tau-eMbct
Outcome measure n M SDb n M SDb n M SDb overall Est. SE p ES Est. SE p ES
Primary
hads
T0 77 18.81 6.70 90 17.24 7.07 78 17.04 5.79
T1 original 64 13.25 6.33 75 11.87 6.16 70 16.37 6.50 <.001 4.65 1.00 <.001 .50 4.63 .96 <.001 .70
T1 imputed 77 13.69 .78 90 11.88 .69 78 16.48 .78 <.001 4.55 1.02 <.001 .43 4.81 .95 <.001 .63
Secondary
fcri severity
T0 77 21.49 6.55 90 21.20 5.80 77 21.13 7.28
T1 original 64 18.05 6.49 75 17.28 7.33 68 20.66 7.10 <.001 2.27 .86 .009 .38 3.34 .82 <.001 .51
T1 imputed 77 18.65 .79 90 17.06 .81 78 20.53 .84 <.001 2.234 .89 .013 .29 3.52 .84 <.001 .53
rrQ rumination
T0 77 44.04 7.96 90 43.09 8.17 77 42.69 8.56
T1 original 64 37.61 8.16 75 36.81 8.90 68 41.65 8.85 <.001 4.87 1.14 <.001 .49 4.85 1.10 <.001 .58
T1 imputed 77 38.12 1.04 90 37.26 .97 78 41.56 1.05 <.001 4.77 1.20 <.001 .42 4.68 1.14 <.001 .52
sf-12 Mental
T0 77 32.48 10.19 90 34.50 12.15 78 34.74 11.10
T1 original 64 43.41 9.67 72 44.17 9.95 63 36.78 11.31 <.001 -8.89 2.01 <.001 .62 -7.87 1.95 <.001 .64
T1 imputed 77 42.71 1.23 90 44.25 1.21 78 36.42 .95 <.001 -8.55 1.98 <.001 .56 -8.07 1.92 <.001 .70
sf-12 Physical
T0 77 46.06 8.88 90 45.62 10.25 78 45.40 8.24
T1 original 64 48.24 8.45 72 48.19 10.51 63 45.24 9.77 .343 -2.14 1.61 .19 .35 -1.91 1.57 .22 .32
T1 imputed 77 48.43 1.11 90 47.60 1.20 78 45.40 1.21 >.05 -2.37 1.61 .14 .33 -1.99 1.57 .21 .24
ffMQ-sf total
T0 77 72.43 9.69 90 76.39 10.87 77 75.75 11.18
T1 original 64 82.02 10.42 75 85.52 11.94 70 77.26 11.80 <.001 -8.03 1.76 <.001 .45 -8.06 1.69 <.001 .75
T1 imputed 77 81.61 1.29 90 85.75 1.33 78 76.73 1.41 <.001 -8.17 1.82 <.001 .46 -8.35 1.70 <.001 .84
Mhc-sf total
T0 77 34.05 12.39 90 37.16 13.77 77 37.56 12.46
T1 original 64 40.02 12.39 75 43.53 13.14 70 37.86 13.34 .001 -5.19 1.71 .003 .17 -6.10 1.64 <.001 .43
T1 imputed 77 38.85 1.51 90 43.13 1.46 78 37.36 1.59 <.005 -4.97 1.71 .004 .11 -6.15 1.66 <.001 .44

Groups Linear Mixed Modeling: Between-group differences
Mbct eMbct tau pa tau-Mbct tau-eMbct
Outcome measure n M SDb n M SDb n M SDb overall Est. SE p ES Est. SE p ES
Primary
hads
T0 77 18.81 6.70 90 17.24 7.07 78 17.04 5.79
T1 original 64 13.25 6.33 75 11.87 6.16 70 16.37 6.50 <.001 4.65 1.00 <.001 .50 4.63 .96 <.001 .70
T1 imputed 77 13.69 .78 90 11.88 .69 78 16.48 .78 <.001 4.55 1.02 <.001 .43 4.81 .95 <.001 .63
Secondary
fcri severity
T0 77 21.49 6.55 90 21.20 5.80 77 21.13 7.28
T1 original 64 18.05 6.49 75 17.28 7.33 68 20.66 7.10 <.001 2.27 .86 .009 .38 3.34 .82 <.001 .51
T1 imputed 77 18.65 .79 90 17.06 .81 78 20.53 .84 <.001 2.234 .89 .013 .29 3.52 .84 <.001 .53
rrQ rumination
T0 77 44.04 7.96 90 43.09 8.17 77 42.69 8.56
T1 original 64 37.61 8.16 75 36.81 8.90 68 41.65 8.85 <.001 4.87 1.14 <.001 .49 4.85 1.10 <.001 .58
T1 imputed 77 38.12 1.04 90 37.26 .97 78 41.56 1.05 <.001 4.77 1.20 <.001 .42 4.68 1.14 <.001 .52
sf-12 Mental
T0 77 32.48 10.19 90 34.50 12.15 78 34.74 11.10
T1 original 64 43.41 9.67 72 44.17 9.95 63 36.78 11.31 <.001 -8.89 2.01 <.001 .62 -7.87 1.95 <.001 .64
T1 imputed 77 42.71 1.23 90 44.25 1.21 78 36.42 .95 <.001 -8.55 1.98 <.001 .56 -8.07 1.92 <.001 .70
sf-12 Physical
T0 77 46.06 8.88 90 45.62 10.25 78 45.40 8.24
T1 original 64 48.24 8.45 72 48.19 10.51 63 45.24 9.77 .343 -2.14 1.61 .19 .35 -1.91 1.57 .22 .32
T1 imputed 77 48.43 1.11 90 47.60 1.20 78 45.40 1.21 >.05 -2.37 1.61 .14 .33 -1.99 1.57 .21 .24
ffMQ-sf total
T0 77 72.43 9.69 90 76.39 10.87 77 75.75 11.18
T1 original 64 82.02 10.42 75 85.52 11.94 70 77.26 11.80 <.001 -8.03 1.76 <.001 .45 -8.06 1.69 <.001 .75
T1 imputed 77 81.61 1.29 90 85.75 1.33 78 76.73 1.41 <.001 -8.17 1.82 <.001 .46 -8.35 1.70 <.001 .84
Mhc-sf total
T0 77 34.05 12.39 90 37.16 13.77 77 37.56 12.46
T1 original 64 40.02 12.39 75 43.53 13.14 70 37.86 13.34 .001 -5.19 1.71 .003 .17 -6.10 1.64 <.001 .43
T1 imputed 77 38.85 1.51 90 43.13 1.46 78 37.36 1.59 <.005 -4.97 1.71 .004 .11 -6.15 1.66 <.001 .44

Table 3 Clinically significant improvement measured by Jacobson–Truax Reliable Change Index on hads and psychiatric diagnosis between baseline and post-intervention for Mbct, eMbct and tau groups.
Reliable change index (n=209) Psychiatric diagnosis (n=202)
Mbct eMbct tau Mbct eMbct tau
n=64 n=75 n=70 n=64 n=76 n=62
n % p* n % p* n % n % p* n % p* n %
Improved 23 36 .004 28 37 .002 10 14 21 33 .030 22 29 .076 10 16
No change 39 61 47 63 54 77 34 67 50 66 49 79
Deteriorated 2 3 .184 0 0 .010 6 9 0 0 .075 4 5 .910 3 5
Figure 2 Change in hads scores between baseline and post-intervention for Mbct, eMbct and tau groups. The diagonal line represents ‘no change in hads between baseline and post-intervention’ and the dashed upper and lower lines represent the upper (above indicates deteriorated) and lower (below indicates improved) bounds of the 95% ci of the Jacobson–Truax Reliable Change Index.
0 10 20
20
30
30
40
40
10
hads baseline
had
s en
d of
trea
tmen
t
mbct
0 10 20
20
30
30
40
40
10
hads baseline
had
s en
d of
trea
tmen
t
embct
0 10 20
20
30
30
40
40
10
hads baseline
had
s en
d of
trea
tmen
t
Treatment as usual rci
No changeImprovedDeteriorated
*Between group chi-square tests for the respective condition compared to tau

Reliable change index (n=209) Psychiatric diagnosis (n=202)
Mbct eMbct tau Mbct eMbct tau
n=64 n=75 n=70 n=64 n=76 n=62
n % p* n % p* n % n % p* n % p* n %
Improved 23 36 .004 28 37 .002 10 14 21 33 .030 22 29 .076 10 16
No change 39 61 47 63 54 77 34 67 50 66 49 79
Deteriorated 2 3 .184 0 0 .010 6 9 0 0 .075 4 5 .910 3 5
All Mbct eM-bct
tau pa
n=198 n=63 n=72 n=63
n % n % n % n %
Hospital outpatient 153 77 45 71 61 85 47 75 .153
Hospital overnight 13 7 4 9 4 6 5 8 .853
Hospital day ward 36 18 6 10 12 17 18 29 .020
Hospital emergency depart-ment
7 4 1 1 3 3 3 4 .588
Mental healthcareb 62 31 18 29 24 33 20 32 .834
General practitioner 116 59 35 56 39 54 42 67 .285
Physical therapist 92 47 29 46 40 56 23 37 .086
Complementary care 56 28 21 33 20 28 15 34 .491
Table 4 Healthcare utilization during the intervention period for Mbct, eMbct and tau groups.
aPearson Chi-Square Testb Social worker, psychologist

68
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
References
1. Bray F., Transitions in human development and the global cancer burden. In: Wild CP, Stewart B, eds. World Cancer Report. Lyon: International Agency for Research on Cancer, 2014. World Cancer Report: p. 54-68
2. Carlson L, Angen M, Cullum J, et al., High levels of untreated distress and fatigue in cancer patients. British Journal of Can-cer, 2004. 90: p. 2297-2304
3. Mitchell AJ, Chan M, Bhatti H, et al., Prevalence of depression, anxiety, and adjustment disorder in oncological, hae-matological, and palliative-care settings: a meta-analysis of 94 interview-based studies. The Lancet Oncology, 2011. 12: p. 160–174
4. Mitchell A. F, D., Gill, J., Paul, J., Sy-monds, P., Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: a systematic review and meta-analysis. Lancet Oncology, 2013. 14: p. 671-786
5. Kabat-Zinn J., Full catastrophe living, revised edition: how to cope with stress, pain and illness using mindfulness meditation, Hachette uK, 2013
6. Segal ZV, Williams JMG, Teasdale JD., Mindfulness-based cognitive therapy for depression: A new approach to relapse pre-vention, New York: Guilford Press, 2013
7. Piet J, Wurtzen H, Zachariae R., The Effect of Mindfulness-Based Therapy on Symptoms of Anxiety and Depression in Adult Cancer Patients and Survivors: A Sys-tematic Review and Meta-Analysis. Journal of Consulting and Clinical Psychology, 2012. 80: p. 1007-1020
8. Carlson LE, Doll R, Stephen J, et al., Randomized controlled trial of Mindful-ness-based cancer recovery versus supportive expressive group therapy for distressed sur-vivors of breast cancer. Journal of Clinical Oncology, 2013.31: p. 3119-26
9. Garland SN, Carlson LE, Stephens AJ, et al., Mindfulness-Based Stress Reduc-tion Compared With Cognitive Behavioral
Therapy for the Treatment of Insomnia Comorbid With Cancer: A Randomized, Par-tially Blinded, Noninferiority Trial. Journal of Clinical Oncology, 2014. 32: p. 449-457
10. Lengacher CA, Reich RR, Paterson CL, et al., Examination of Broad Symptom Improvement Resulting From Mindful-ness-Based Stress Reduction in Breast Cancer Survivors: A Randomized Controlled Trial. Journal of Clinical Oncology, 2016. 34: p. 2827-2834
11. Johannsen M, O’Connor M, O’Toole MS, et al., Efficacy of Mindfulness-Based Cognitive Therapy on Late Post-Treatment Pain in Women Treated for Primary Breast Cancer: A Randomized Controlled Trial. Journal of Clinical Oncology, 2016. 34: p. 3390-3399
12. Schellekens MPJ, van den Hurk DGM, Prins JB, et al., Mindfulness-Based Stress Reduction added to care as usual for lung cancer patients and/or their partners: A multi-centre randomized controlled trial. Psycho-Oncology:10.1002/pon.4430 2017
13. Carlson LE, Tamagawa R, Stephen J, et al., Randomized-controlled trial of mindful-ness-based cancer recovery versus supportive expressive group therapy among distressed breast cancer survivors (mINDSET): long-term follow-up results. Psycho-Oncology, 2016. 25: p. 750-759
14. Zernicke KA, Campbell TS, Speca M, et al., A randomized wait-list controlled trial of feasibility and efficacy of an online mindfulness–based cancer recovery program: the etherapy for cancer applying mindfulness trial. Psychosomatic Medicine, 2014. 76: p. 257-67
15. Brebach R, Sharpe L, Costa DSJ, et al., Psychological intervention targeting dis-tress for cancer patients: a meta-analytic study investigating uptake and adherence. Psycho-Oncology, 2016. 25: p. 882-890
16. Spijkerman MPJ, Pots WTM, Bohlmei-jer ET., Effectiveness of online mindful-ness-based interventions in improving mental health: A review and meta-analysis of randomised controlled trials. Clinical Psychology Review, 2016.45: p. 102-114

69
17. Andersson G., Internet-Delivered Psychological Treatments. Annual Review of Clinical Psychology, 2016.12: p. 157-179
18. Zernicke KA, Campbell TS, Speca M, et al., The eCALM Trial: eTherapy for Cancer Applying Mindfulness. Exploratory Analyses of the Associations Between Online Mind-fulness-Based Cancer Recovery Participation and Changes in Mood, Stress Symptoms, Mindfulness, Posttraumatic Growth, and Spirituality. Mindfulness, 20167: p. 1071-1081
19. Everts FZB, van der Lee ML, de Jager Meezenbroek E, Web-based individual Mindfulness-Based Cognitive Therapy for cancer-related fatigue – A pilot study. Inter-net Interventions, 2015 2: p. 200-213
20. Schulz KF, Altman DG, Moher D, cON-SORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMC medicine, 2010. 8: p. 18
21. Compen FR, Bisseling EM, Van der Lee ML, et al., Study protocol of a multicenter randomized controlled trial comparing the effectiveness of group and individual internet-based Mindfulness-Based Cognitive Therapy with treatment as usual in reducing psychological distress in cancer patients: the BeMind study. Bmc Psychology, 2015 3: 27
22. Crane C, Williams JMG, Factors Associ-ated with Attrition from Mindfulness-Based Cognitive Therapy in Patients with a History of Suicidal Depression. Mindfulness, 2010. 1: p. 10-20
23. Hakkaart-van Roijen L, Straten A, Donk-er M, et al., Trimbos/iMTA questionnaire for Costs associated with Psychiatric Illness (TiC-P). Rotterdam, Institute for Medi-cal Technology Assessment, 2002.
24. uK Network for Mindfulness-Based Teachers Good practice guidelines for teaching mindfulness-based courses, 2015
25. Crane RS, Kuyken W, Williams JM, et al., Competence in Teaching Mindfulness-Based Courses: Concepts, Development and Assess-ment. Mindfulness (NY), 2012. 3: p. 76-84
26. Zigmond AS, Snaith RP, The hospital anx-iety and depression scale. Acta psychiatrica scandinavica, 1983. 67: p. 361-370
27. Spinhoven P, Ormel J, Sloekers PP, et al., A validation study of the Hospital Anxiety and Depression Scale (HADS) in different groups of Dutch subjects. Psychological Medicine, 1997 27: p. 363-370
28. Akechi T, Okuyama T, Sugawara Y, et al., Screening for depression in terminally ill can-cer patients in Japan. Journal of Pain and Symptom Management, 2006. 31: p. 5-12
29. First MB, Spitzer RL, Gibbon M, et al., Structured Clinical Interview for DSm-IV® Axis I Disorders (ScID-I), Clinician Version. Administration Booklet, American Psychiatric Pub, 2012
30. Simard S, Savard J, Fear of Cancer Recur-rence Inventory: development and initial validation of a multidimensional measure of fear of cancer recurrence. Supportive Care in Cancer, 2009 17: p. 241-51.
31. van Helmondt SJ, van der Lee ML, de Vries J, Translation and validation of the Dutch version of the Fear of Cancer Recurrence Inventory (fcRI-NL). Journal of Psychosomatic Research , 2017. 102: p. 21-28
32. Trapnell PD, Campbell JD, Private self-consciousness and the five-factor model of personality: distinguishing rumination from reflection. Journal of Personality and Social psychology, 1999. 76: p. 284-304
33. Ware Jr JE, Kosinski M, Keller SD, A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Medical care , 1996. 34: p. 220-233
34. Mols F, Pelle AJ, Kupper N, Normative data of the SF-12 health survey with valida-tion using postmyocardial infarction patients in the Dutch population. Quality of Life Research, 2009. 18: p. 403-414
35. Bohlmeijer E, ten Klooster PM, Fled-derus M, et al., Psychometric properties of the five facet mindfulness questionnaire in depressed adults and development of a short form. Assessment, 2011. 18: p. 308-320
36. Keyes CL, Mental illness and/or mental health? Investigating axioms of the complete state model of health. Journal of Consulting and Clinical Psychology 73:539-48, 2005
chapter 3

70
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
37. Costa PT, McCrae RR, Revised NEO Per-sonality Inventory (NEO-PI-R) and the Five Factor Inventory (NEO-ffI): Professional Manual. Odessa, Florida, Psychological Assessment Resources Inc., 1992
38. McGough JJ, Faraone SV, Estimating the Size of Treatment Effects: Moving Beyond P Values. Psychiatry (Edgmont), 2009.6: p. 21-29
39. Cohen J, Statistical power analysis for the behavioral sciences (revised ed.), New York: Academic Press, 1977
40. Jacobson NS, Truax P, Clinical signif-icance: a statistical approach to defining meaningful change in psychotherapy research. J Consult Clinical Psycholy, 1991. 59:12-19
41. Zernicke KA, Campbell TS, Speca M, et al., A Randomized Wait-List Controlled Trial of Feasibility and Efficacy of an Online Mindfulness-Based Cancer Recovery Program: The eTherapy for Cancer Applying Mindfulness Trial. Psychosomatic Medi-cine,2014. 76: p. 257-267
42. Schellekens MP, Jansen ET, Willemse HH, et al., A qualitative study on mindful-ness-based stress reduction for breast cancer patients: how women experience partici-pating with fellow patients. Support Care Cancer , 2016.24: p. 1813-1820
43. Melville KM, Casey LM, Kavanagh DJ., Dropout from Internet-based treatment for psychological disorders. British Journal of Clinical Psychology, 2010. 49: p. 455-471
44. van Scheppingen C, Schroevers MJ, Pool G, et al., Is implementing screening for distress an efficient means to recruit patients to a psychological intervention trial? Psy-cho-Oncology , 2014. 23: p. 516-523
45. Garssen B, Van der Lee M, Van der Poll A, et al., Characteristics of patients in routine psycho-oncological care, and changes in outcome variables during and after their treatment. Psychology & health, 2016. 31: p. 1237-1254
46. Swift JK, Callahan JL, The impact of cli-ent treatment preferences on outcome: a meta-analysis. J Clin Psychol 65:368-81, 2009
47. Carlson LE, Bultz BD, Efficacy and med-ical cost offset of psychosocial interventions in cancer care: making the case for economic analyses. Psycho-Oncology, 2004. 13: p. 837-849
48. Kazdin AE, Mediators and mechanisms of change in psychotherapy research. Annual Review of Clinical Psychology, 2007 3: p. 1-27
49. Gu J, Strauss C, Bond R, et al., How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clinical Psychology, 2015. Review 37: p. 1-12
50. Toivonen KI ZK, Carlson LE, Web-Based Mindfulness Interventions for People With Physical Health Conditions: Systematic Review. Journal of Medical Internet Research, 2017. 19:e303
51. Compen FR, Bisseling EM, Schellekens MP, et al., Mindfulness-Based Cognitive Therapy for Cancer Patients Delivered via Internet: Qualitative Study of Patient and Therapist Barriers and Facilitators. Journal of medical Internet research, 2017. 19(12):e407
52. Wentzel J, van der Vaart R, Bohlmeijer ET, et al., Mixing Online and Face-to-Face Therapy: How to Benefit From Blended Care in Mental Health Care. JmIR Mental Health, 2016. 3:e9



Chapter 4
Therapeutic alliance -not therapist competence or group cohesion- contributes to reduction of psychological distress in group-based Mindfulness-Based Cognitive Therapy for cancer patients
This chapter has been published as:
Else M. Bisseling, Melanie P.J. Schellekens, Philip Spinhoven, Félix R. Compen, Anne E.M. Speck-ens, Marije L. van der Lee Clinical Psychology & Psychotherapy (2019): 26(3):309-318
Acknowledgement of research support: This study is funded by breast cancer foundation Pink Ribbon (2012.WO14.C153)

74
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
abstract
Mindfulness-Based Cognitive Therapy (mBcT) is an innovative evidence-based intervention in mental and somatic health care. Gaining knowledge of therapeutic factors associated with treatment outcome can improve mBcT. This study focused on predictors of treatment outcome of mBcT for cancer patients and examined whether group cohesion, therapeutic alliance and therapist competence predicted reduction of psychological distress after mBcT for cancer patients. Moreover, it was examined whether therapist competence facilitated therapeutic alliance or group cohesion. Multilevel analyses were conducted on a subsample of patients collected in a larger randomized controlled trial on individual internet-based versus group-based mBcT versus treatment as usual in distressed cancer patients. The current analyses included the 84 patients who completed group-based mBcT out of 120 patients who were randomized to group-based mBcT. Group cohesion and therapist competence did not predict reduction in psychological distress, whereas therapeutic alliance did. In addition, therapist competence did not pre-dict therapeutic alliance, but was associated with reduced group cohesion. Our findings revealed that therapeutic alliance significantly contributed to reduction of psychological distress in mBcT for cancer patients. Elaborating the clinical implications of the predictive significance of therapeutic alliance might be of added value to enhance the potential effect of mBcT.

75
chapter 4
key Practitioner message
1. Mindfulness-Based Cognitive Therapy (mBcT) is an innovative evidence-based intervention in mental and somatic health care and has been increasingly applied in oncology to reduce psychological distress.
2. Therapeutic alliance predicts reduction in psychological distress after mBcT for cancer patients, whereas group cohesion and therapist competence did not.
3. Therapist competence did not appear to be a precondition for a good ther-apeutic alliance and high group cohesion.
4. Contrary to expectation we found competence to be negatively related to group cohesion.
5. Elaborating the clinical implications of the predictive significance of ther-apeutic alliance might be of added value to enhance the potential effect of mBcT for cancer patients.
6. The current findings should be taken into account in the training of mBcT therapists.
key Words
Therapist competence; therapeutic alliance; group cohesion; psychological dis-tress; cancer; mBcT.

76
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
background
Mindfulness-Based Interventions (mBIs) are innovative, evidence-based interven-tions in mental and somatic health care.1, 2 mBIs have increasingly been applied in oncology. A 2012 meta-analysis of nine randomized controlled trials (RcTs) (n=955) in cancer patients demonstrated that mBIs result in significant improvements in depressive and anxiety symptoms.3 Since then several RcTs have confirmed these effects.4-7 Mindfulness is defined as: ‘paying attention; on purpose, in the present moment and non-judgmentally’.8 mBIs teach patients to become more aware of their experiences in daily life through meditation exercises, yoga, group discussion and didactic teaching. mBI protocols designed to teach the cultivation of mind-fulness are Mindfulness-Based Stress Reduction (mBSR) and Mindfulness-Based Cognitive Therapy (mBcT), the latter incorperating elements of Cognitive Behav-ioral Therapy (cBT). Research on predictors of treatment outcome focuses on both intrapsychological characteristics of participants as well as interpsychological therapeutic aspects, such as group cohesion, therapeutic alliance and therapeutic competence. Inde-pendent of treatment orientation, studies on therapeutic aspects accentuate the importance of these general factors.9, 10 Other studies indicate specific therapeutic factors to predict outcome of particular psychotherapies, such as embodiment as a key element of therapist competence in mBIs.11 Identifying therapeutic factors related to outcome may deepen our understanding of the processes that account for therapeutic change. Such knowledge can help to develop and test more precise treatment strategies that trigger critical change processes.12
Group cohesion primarily refers to social-emotional cohesion: the intimacy, reciprocity and emotional disclosure that is felt among group members,13 contrib-uting to the cooperation within the group to achieve a common therapeutic aim.14 It is presumed that when cohesion is high, the group is motivated to perform well and is more able to carry out activities for successful performance.15 Research on the role of group cohesion in psychotherapy has shown that a higher level of group cohesion predicts better treatment outcome.16-18
To measure group cohesion, the Dutch Group Cohesion Questionnaire (GcQ-22)19 was developed, which is based on the Group Attitude Scale20 and the Three Factor Group Questionnaire.21 The GcQ- 22 compromises 22 items across four scales: 1) the bond with the group as total; 2) the bond with other members of the group; 3) the cooperation within the grup; and 4) the instrumental value of the group. To our knowledge there are no previous studies on the impact of group cohesion in mBIs, whether in cancer patients or in different settings. However, qualitative studies showed that group-based settings in mBIs are of added value to cancer patients,11, 22 and that peer support facilitated the learning process in mBSR.23

77
Therapeutic alliance is defined as the collaborative and affective bond between therapist and patient.24, 25 Several meta-analyses demonstrated the significant impact of therapeutic alliance on psychotherapy outcomes.26, 27 Therapeutic alliance is often measured with the Working Alliance Inventory (WAI28), including three subscales: 1) how closely client and therapist agree on goals of treatment; 2) how closely client and therapist agree on how to reach the treatment goals: and 3) the degree of mutual trust between client and therapist. Only one small RcT exam-ined the role of therapeutic alliance in mBcT.29 Comparing individual cBT with individual mBcT, findings showed that therapeutic alliance predicted outcomes of cBT but not of mBcT in depressed patients with diabetes.29
Therapist competence refers to the level of therapist skills in delivering the treatment. It includes the therapists’ consideration of and response to relevant contextual variables.30, 31 Therapist competence has been shown to be associated with positive symptom change in cBT for patients with depressive and anxiety disorders.32-35 However, recently a large study (n=1247) in routine clinical practice could not confirm this association.36 The therapists’ role is slightly different in mBcT compared to traditional cBT. In mBcT, for instance, therapist embodiment is considered to largely determine the quality of the therapy. Moreover, in mBcT the therapist is mainly focused on facilitating patients’ self-efficacy, without too much emphasis on exploring personal narratives. To evaluate therapist competence the Mindfulness-Based Interventions - Teachers Assessment Criteria (mBI:TAc37) is commonly used. The mBI:TAc consists of six domains. These domains consist of three to five key qualities which are scored by independent raters. Although these domains are considered important37 only one multicentre study (n=241) conducted on mBcT for recurrent depression elaborated upon teacher competence. In this study, no robust effects of teacher competence were found.38
In conclusion, group cohesion and therapeutic alliance are closely related constructs, contributing independently to treatment outcome.16 Therapeutic alliance and therapist competence are closely related as well. In some studies it was found that therapeutic alliance mediates the relationship between competence and outcome in psychotherapy39-41 and was suggested that therapeutic competence can be seen as a precondition for developing a good therapeutic alliance. Put differently, only when the therapist is able to deliver the treatment competently, a good therapeutic alliance can be formed. However, conclusive evidence whether group cohesion, therapeutic alliance and therapist competence predict treatment outcome is lacking. The aim of our explorative study was to examine the role of group cohesion, therapeutic alliance and therapist competence on outcome of mBcT for distressed cancer patients. It was hypothesized that a) group cohesion, therapeutic alliance
chapter 4

78
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
and therapist competence independently predict reduction of psychological dis-tress and b) therapist competence is a precondition for developing both group cohesion and therapeutic alliance which, in turn, independently predict reduction of psychological distress.
methods
designThe present study was part of a larger multicentre RcT on the effectiveness of mBcT for distressed cancer patients (Clinicaltrials.gov no. NCT02138513).42 Partic-ipants were randomized to either 1) face-to-face group mBcT; 2) online individual mBcT (emBcT); or 3) treatment as usual (TAu). After three months, patients in TAu were randomly allocated to 1) face-to-face group-based mBcT or 2) emBcT. For the present study we used the data of 120 patients who were allocated to the face-to-face group-based mBcT after the initial randomization (n=77) or after the completing the TAu condition (n=43). The analyses only included patients who completed the group-based mBcT, i.e. attended four or more sessions (n=84). The local ethics committee approved this study (cmO Arnhem Nijmegen 2013/542). All patients and therapists provided written informed consent.
study populationPatients
Patients were recruited in participating specialized mental health care institutes for psycho-oncology, via social media, patient associations and advertorials in local newspapers in the Netherlands. Patients who were interested in participation could enroll themselves at the study website (www.bemind.info) at which point they completed the screening assessment, the Hospital Anxiety and Depression Scale (HADS). Patients with a score of ≥11 on the HADS were contacted by telephone by one of the researchers to assess eligibility. Inclusion criteria were having any cancer diagnosis, experiencing at least mild psychological distress, sufficient computer literacy and access to internet, good command of Dutch language and willingness to participate in either online or face-to-face group based mBcT. Exclusion criteria were severe psychiatric morbidity like suicidal ideation and/or psychosis, change in psychotropic medication within three months of baseline, and current or pre-vious participation in mBcT or mBSR. Prior to randomization, patients completed the baseline assessment and (self-report) questionnaires, including the following demographic and clinical characteristics: gender, age, marital status, children, education, cancer diagnosis, and years since diagnosis, anticancer treatment intent, current anticancer treatment and psychiatric diagnosis.

79
TherapistsTherapists (n=9) were affiliated to the participating centers, including specialized outpatients clinics for psycho-oncology (n=4), a general and an academic hospital (n=3), private practices (n=2). All therapists fulfilled the advanced criteria of the Association of Mindfulness Based Teachers in the Netherlands and Flanders which are in concordance with the UK Mindfulness-Based Teacher Trainer Net-work Good Practice Guidelines for teaching mindfulness-based courses.43 These include a minimum of 150 hours education in mBSR/mBcT, at least three years of personal practice of meditation, having attended at least one 5-10 days retreat, and teaching a minimum of 2 mBcT trainings a year. The supervision offered within the multicenter trial was on a national level. All therapists received a two-day workshop and additional training in the mBcT study protocol by experienced senior psychologists and psychiatrists who were also mindfulness teachers. Two additional supervision meetings were organized during the intervention phase which lasted one year and six months. In addition, all therapists received regular supervision at their individual working places. When facing difficulties, therapists were encouraged to contact one of the researchers, who were experienced psychi-atrists and mindfulness trainers.
interventionMindfulness Based Cognitive Therapy
Patients randomized to group-based mBcT received the intervention according to the mBcT protocol of Segal et al.44 The group-based mBcT consisted of eight weekly 2.5h group sessions, one six-hour silent day and daily home practice assignments guided by audio files. The sessions consisted of mindfulness practices, sharing experiences and didactic teachings, which were adapted to cancer patients.45 Each participant received a folder with information on each session and a cD containing the audio files. The group-based mBcT was provided at the Radboud University Medical Centre in Nijmegen, the Jeroen Bosch Hospital in ‘s Hertogenbosch and at four mental health institutes specialized in psycho-oncology (Helen Dowling Institute (Bilthoven), Ingeborg Douwes Centrum (Amsterdam), De Vruchtenburg (Leiden), Het Behouden Huys (Haren)). In the group-based mBcT condition, all sessions of all therapists were videotaped to evaluate teacher competence and protocol adherence. In total 14 face-to-face mBcT groups were delivered. The intervention is described in more depth in our protocol paper.42
MeasuresTreatment outcome
The primary outcome measure was psychological distress according to the 14-item Hospital Anxiety and Depression Scale (HADS45, 46). It has been validated in somatic
chapter 4

80
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
patient populations, including cancer patients.47 Internal consistency of the total scale in the present sample was high (Cronbach’s alpha= 0.82).
Therapeutic factorsGroup cohesion was assessed with the Dutch Group Cohesion Questionnaire -22 (GcQ48) which has been used in cancer patients before.49 The Dutch GcQ consists of four subscales: 1) the bond with the group as whole; 2) the bond with other members; 3) cooperation within the group; and 4) the instrumental value of the group bond. Each item of this 22-item inventory is rated from 1 (totally disagree) to 6 (totally agree). Internal consistency of total scale of the version used in this study was 0.95. In this study, the GcQ was administered at the start of session 5, in accordance with a previous study in cancer patients, suggesting group cohesion to develop early in the intervention and to stay relatively stable over time.49 Due to the layout of the GcQ Teleform, the percentage of missing values on the last 3 items was 24%. These missing values were replaced with mean values of the available items.
Therapeutic alliance was measured with a translated and shortened form of the Working Alliance Inventory (WAI28), which was administered at the start of session 5. The WAI consists of three subscales assessing: 1) how closely client and therapist agree on and are mutually engaged in the goals of treatment; 2) how closely cli-ent and therapist agree on how to reach the treatment goals; and 3) the degree of mutual trust, acceptance, and confidence between client and therapist. Items were scored on a 5-point scale ranging from rarely to always.50, 51 The 12-item inventory was validated in a Dutch-speaking sample, showing an internal consistency of >.80 for all separate subscales and .87 for the total scale.52 Internal consistency of the total scale of the version used in this study was 0.87.
Therapist Competence was assessed with the Mindfulness-Based Interventions - Teachers Assessment Criteria (mBI:TAc37) which consists of six domains: 1) organiza-tion; 2) relational skills; 3) embodiment of mindfulness; 4) guiding mindfulness practices; 5) didactical skills and 6) group environment. These domains consist of three to five key qualities which are scored at six competence levels: incom-petent (1), beginner (2), advanced beginner (3), competent (4), proficient (5), and advanced (6). Therapist competency levels were determined for all 9 therapists providing face-to-face mBcT. From each therapist, two videotaped sessions were randomly selected (www.random.org). The sessions were rated by two indepen-dent raters who were both experienced mindfulness teachers. Both assessors had not participated in the RcT as a therapist and had experience with assess-ing competence using the mBI:TAc. To assess the interrater reliability of the

81
mBI:TAc, intra-class correlations were calculated using a two-way mixed con-sistency model with single measures, based on the independent ratings of two assessors per videotape (n=5). The IRR was substantial with an Icc score of the total scale of 0.70. The Icc’s of the six domains were: fair for guiding practices (0.27), moderate for organization (0.59), substantial for relational skills (0.78), embodi-ment (0.71) and group environment (0.79), and almost perfect for didactical skills (0.84). Correlations between the domains were high, ranging from .72 to .96 (all p values < 0.05).
statistical analysesAll analyses were conducted in SPSS Version 25.0. (IBm Corp., 2017) using an intervention completer sample. To examine possible predictors (group cohesion, therapeutic alliance, and therapist competence) of the effect of mBcT on psycho-logical distress, multilevel analyses were used, in which participants were nested within therapist. We ran separate models for each predictor. The post-treatment HADS score was the dependent variable and baseline HADS score was added as a covariate and the predictor of choice as a fixed factor. In addition, intercepts were allowed to vary across therapists. An unstructured covariance structure was used with no constraints or patterns specified in the covariance matrix. As the sample size was relatively small, Restricted Maximum Likelihood (REmL) was used to handle missing data.53 In addition, we explored whether therapist competence was a predictor for developing both group cohesion and therapeutic alliance. We used similar multilevel models adding competence as the predictor and group cohesion or therapeutic alliance as dependent variable. When the therapeutic factor was a significant predictor of outcome, we performed exploratory analysis to examine the effects of the subscales of that particular factor on outcome. Similar multilevel models were used, adding all subscale scores of the significant factor in one model.Patients filled out the HADS prior to randomization (baseline, T0), directly after the intervention (T1) or directly after TAu (T0b). After TAu, the scores on the HADS in the TAu condition had not significantly changed.54 For patients partic-ipating in the group-based mBcT after TAu, baseline scores on the HADS were replaced with end-of-waiting list scores as those were closer in time to the start of the treatment, in accordance with a previous study on the long-term effect of (e)mBcT in cancer patient.55 These scores did not significantly differ from base-line scores of the original intervention group. Only 3 out of n=25 (12%) of the completers, who started the intervention after TAu, scored <11 on the HADS at the start of the intervention. Analyses were also performed with only individu-als scoring above the cutoff of ≥ 11 on the HADS. These analyses showed similar results.
chapter 4

82
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
result
participantsPatients
Of the cancer patients participating in the RcT (n=245), 120 were randomized to the face-to-face group mBcT: n=77 starting immediately and n=43 after the TAu condition. Of those, n=25 (21%) decided not to take part after all and n=95 (79%) actually started with mBcT. See Figure 1 for the study flow diagram. Of all individ-uals randomized to group-based mBcT, n=84 (70%) completed more than 4 sessions of mBcT. As shown in Table 1, patients were mostly female, middle aged, highly educated, suffered from breast cancer and were treated with a curative intent. There were no significant differences between the patients who completed the mBcT and those who did not start or dropped out the intervention. Multilevel analyses revealed that psychological distress (F (1,74) =72,11, p<.001) was significantly less at post-treatment compared to baseline.
TherapistsAll therapists were middle-aged females, with a mean duration of teaching mBcT of 6.1 years (SD=2.9; Mdn=7) and an average number of 26 courses taught (SD=28.6; Mdn= 12). Of the nine rated therapists, two therapists were rated as beginner (22%), three as competent (33%) and four as proficient (44%) based on the mean scores of the subscales. No therapist was rated as incompetent. Table 2 shows further details of therapist competence.
prediction of treatMent outcoMeMean level of psychological distress was reduced from 18.3 (SD= 6.5) to 13.5 (SD=6.8) at post-treatment. Mean level of group cohesion at the start of session 5 was 95.3 (SD=11.3) and mean level of therapeutic alliance 39.1 (SD= 8.8). As Table 3 demon-strates, group cohesion did not significantly predict reduction of psychological distress (b= -0.10, p=.058) whereas therapeutic alliance did (b = -0.18, p= .016). As the therapeutic alliance significantly predicted reduction of psychological dis-tress, we further explored potential effects of the three subscales. Exploratory analyses suggested significant predictive values of the Goal subscale (b= -.53, p=.010) but not of the Task subscale (b= -0.08, p=.552) or the Bond subscale (b= -0.19, p=.382). Therapist competence did not predict reduction of psychological distress (b = -.10, p= .883). Therapist competence and therapeutic alliance were not sig-nificantly correlated (r= -.206, p =.103). In addition, therapist competence was not associated with level of therapeutic alliance (b =-2.16, p =.120). However, therapist competence was inversely correlated (r=-2.83, p=.018) with group cohesion. Ther-apist competence appeared to be negatively associated with lower group cohesion

83
(b =-3.90, p= .018), as shown in Table 4. Moreover, analyses revealed that group cohesion and therapeutic alliance were moderately correlated with one another (r= .515, p <.001). Exploratory analyses of the six domains of therapist competence suggested that the negative association with group cohesion was mainly due to the significant negative association with the domain Relational skills (b=-3.58, p=.012). The other domains were not significantly associated with group cohesion.
discussion
The present study investigated the association of group cohesion, therapeutic alliance and therapist competence with reduction of psychological distress after mBcT for cancer patients. It was hypothesized that group cohesion, therapeutic alliance and therapist competence would predict treatment outcome, and that therapist competence was a prerequisite for developing both group cohesion and therapeutic alliance. Our findings revealed that therapeutic alliance and not group cohesion significantly contributed to reduction of psychological distress in mBcT for cancer patients. Therapist competence did not predict post-treatment psychological distress and did not appear to be a precondition for a good thera-peutic alliance and high group cohesion. In accordance with comprehensive and consistent findings in meta-analyses in psychotherapy26, 27 therapeutic alliance was positively associated with treatment outcome in our study as well, particularly in terms of goal aspects. This is in line with previous research but contrary to findings of one recent study investigating the relationship between therapeutic alliance and treatment outcomes in individ-ual mBcT. In this study no significant association with dimensions of the alliance were found.29 Snippe et al. suggested that in general the low predictive value of task and goals aspects in mBcT could be explained by the experiential nature of mBcT. In contrast with this study, our results suggest that although mBcT focuses on experiential learning, still mutual agreement on the goals of the treatment is associated with a positive outcome. This has previously been established in cBT.56, 57
Moreover, we did not find a significant association of group cohesion with symptom reduction. This is in line with a previous study showing that only the cooperation subscale, yet not the total scale, of the GcQ was positively correlated with outcome in a rehabilitation program for cancer patients.49 In a well-structured setting, group cohesion might be of less importance to acquire certain skills.
Therapist competence did not have a significant effect on reduction of psycholog-ical distress. This is in line with previous findings that did not show a relationship between therapist competence and treatment outcome in mBcT for recurrent depression.38 In addition, previous research in cBT also found little support for an
chapter 4

84
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
association between competence and patient outcome.36 An explanation could be that all therapists operated at least at a basic skill level as they all fulfilled the advanced criteria of the Association of Mindfulness Based Teachers in the Netherlands and Flanders. Although there was a range in competence level, none of the therapists were observed as incompetent or advanced on the mBI:TAc. Therefore, differences in competence might have been too small to find an association with outcome. Therapist competence did not predict therapeutic alliance either. This could be explained by the finding that valued aspects of observed competence, such as a non-reacting stance are not necessarily seen as positive by patients.11 Personal style differences of therapists could have had a negative or positive impact on perceived therapeutic alliance from patients’ perspective, irrespective of their competence. A second explanation could be that the highly structured program, the pre-recorded audio files, and the emphasized self-efficacy may be predominant. These aspects should be further explored. From a more methodological view, therapist compe-tence was assessed by observers and both therapeutic alliance, group cohesion and psychological distress was self-reported by patients. In other words, the association between therapeutic alliance and group cohesion and outcome were based on data of a common source (e.g. therapeutic alliance from patients predicts psychological distress from patients) while the association between therapist competence and outcome was based on data of different sources (e.g. competence from therapists predicts psychological distress from patients). Due to shared method variance,58 chances of finding an effect based on data of a common source (patients effects) are higher than finding an effect based on different sources (therapist effect), and this might have influenced our results.
Contrary to our expectations, therapist competence appeared to be associated with lower group cohesion, mainly due to the significant negative association with the domain ‘Relational skills’. In the observer-rated mBI:TAc relational skills refer to skills in managing a group learning environment, such as managing issues as ground rules, boundaries and confidentiality, and to leadership style. In contrast, the self-rated GcQ mainly focuses on social-emotional aspects that are felt among group members within the group as a whole. It seems that the more skilled the mBcT therapist is in managing a group learning environment, the less patients need to rely on their fellow participants for support. Another explanation could be that competent therapists might focus more on guiding the exercises and conduct-ing the inquiry, whereas less competent therapists might leave more room for the casual exchange of individual experiences enhancing group cohesion. An alternative explanation could be that independent raters observing video fragments have a different perspective on relational skills of the mBcT teacher than the mBcT par-ticipants themselves. More research is needed to examine these relational aspects.

85
This is the first study that examined the concurrent effect of group cohesion, thera-peutic alliance and therapist competence on outcome of mBcT. The strength of this study was that we rigorously observed therapist competence by two independent experienced raters with a measure developed to assess competence of mindful-ness therapists. A few limitations need to be mentioned as well. First, following from the aim of the study, its design was uncontrolled. We could not perform a formal mediation analysis since we could not measure therapist competence or therapeutic alliance in a control group, nor could we measure group cohesion in the individual internet-based mBcT. As there is no competence measure for inter-net-based mBcT, we could not measure therapist competence in this intervention either. Furthermore, our sample size was small and the diversity in competence of the therapists was limited. Different results might be found in a larger group of therapists with a broader range of competence, although this might be diffi-cult to achieve in clinical trials. Moreover, patients could enroll themselves in the study. This patient-centred nature of recruitment resulting in a convenience sample might benefit generalization of research findings to clinical practice but inherently leads to selection bias.
Further research examining the effect of competence on outcome in mBcT should consider the use of data from different perspectives, such as therapist competence as perceived by patients. In addition, it should elaborate clinical implications of the predictive significance of therapeutic alliance in mBcT. Consequently, as therapeutic alliance may also serve to reduce risk of dropout,59 better therapeutic alliance might contribute to better adherence. This is of clinical importance, par-ticularly in internet-based mBcT, where dropout was shown to be higher than in face-to-face group mBcT.54
clinical iMplicationsCompleting mBcT is valuable for cancer patients as it results in long-term reduc-tions of psychological distress, and long-term increases in positive mental health and quality of life.55 The findings that agreement on therapeutic goals is associated with better outcomes should be taken into account in the training of mBcT ther-apists in order to enhance the potential effect of mBcT. More attention could be paid, for example, on explaining the rationale of mBcT and engaging patients in the process or at least be willing to explore this.
chapter 4

Figure 1 Study-flow describing the composition of the subsample of n=120 patients who received group-based Mbct
CompletedGroup-based
Mbct(n=84)
Treatmentas usual(n=78)
Internet-basedMbct(n=90)
Internet-basedMbct(n=125)
Randomized(n=245)
Group-basedMbct
(n=120)
StartedGroup-based
Mbct(n=120)Dropout intervention
(n=11)Medical reason (n=5)
Other expectations (n=3)Familiar with Mnf (n=1)
Not specified (n=1)Too stressfull (n=1)
Declined after randomization(n=25)
Schedule (n=10)Medical reason/died (n=4)Other expectations (n=3)
Distance (n=3)Not specified (n=4)
Psych treatment (n=1)
Group-basedMbct(n=43)
Internet-basedMbct(n=35)
Group-basedMbct(n=77)

Table 1 Demographical and clinical characteristics of Mbct patients (n=120)
Completer(n=84)
Decliner / Dropout
(n=36)
Test- statistic
(t or chi2)
p
Sociodemographic Age M(SD) Years 52.6 (10.7) 49.2 (11.9) 1.5 .127
Gender n(%) Female 70 (83.3) 31 (86.1) 1.5 .702
Educational level n(%) Secondary 25 (29.8) 10 (27.3) 0.48 .827
Vocational/University
59 (70.2) 26 (72.7)
Clinical Cancer diagnosis n (%) Breast 54 (64.3) 21 (58.3) 0.38 .537
Prostate 7(8.3) 1(2.8)
Colon 5(6.0) 3(8.3)
Gyn. 4(4.8) 1(2.8)
Non-Hod-gkin
2(2.4) 3(8.3)
Other 12 (14.3) 7(19.4)
Time since diagnosis M(SD)
Years 3.7 (5.3) 3.0 (4.1) 0.67 .506
Cancer treatment intent n(%)
Curative 74 (88.1) 30 (83.3) 0.5 .482
Current anticancer treat-ment n(%)
Yes 41 (48.8) 15 (41.7) 0.52 .472
Treatment outcome Psychological distress M(SD)
hads 18.3 (6.5) 18.0 (7.0) 0.22 .826
Process factor Therapeutic alliance M(SD) wai 39.1 (8.8)
Group Cohesion M(SD) gcQ 95.3 (11.3)

M SD range N %
Age Years 52.9 5.3 42-60
Gender Female 9 100%
Experience teaching Mbct Years 6.1 2.9 2-10
Experience teaching Mbct Lifetime number of groups 25.9 28.6 8-91
Level of Competence Mbi:tac total 4.1 0.8 1.8-5
Mbi:tac organization 3.5 1.0 1-5
Mbi:tac relational skills 4.8 1.0 2-6
Mbi:tac embodiment 4.1 1.1 2-6
Mbi:tac guiding practices 3.9 0.9 2-5
Mbi:tac didactical skills 4.1 1.1 1-5
Mbi:tac group environment 4.3 0.9 2-5
Table 2 Demographical characteristics and competence levels of Mbct therapist (n= 9)

Table 3 Group cohesion (A), therapeutic alliance (B) and competence (C) as predictor of treatment outcome
A. Group cohesion as predictor of treatment outcome of Mbct
B SE 95% CI t p
Intercept 10.68 5.19 0.27 to 21.1 2.06 .045
Baseline level of outcome 0.73 0.09 0.55 to 0.91 7.93 <0.01
Group cohesion -0.10 0.53 -0.21 to 0.01 -1.94 .058
• Group subscale -0.36 0.15 -0.66 to -.06 -2.38 .020**
• Member subscale -0.02 0.18 -0.39 to 0.35 -0.10 .918
• Cooperation subscale -0.41 0.25 -0.92 to 0.10 -1.60 .113
• Instrumental subscale -0.33 0.12 -0.57 to -0.09 -2.75 .008**
B. Therapeutic alliance as predictor of treatment outcome of Mbct
B SE 95% CI t p
Intercept 9.90 3.87 2.08 to 17.7 2.55 .014
Baseline level of outcome 0.63 0.09 0.44 to 0.82 6.63 <.001
Therapeutic alliance -0.18 0.71 -0.32 to - 0.03 -2.50 .016**
• Goal subscale -0.53 0.20 -0.92 to -0.13 -2.68 .010**
• Task subscale -0.08 0.12 -0.33 to0.18 -0.60 .552
• Bond subscale -0.19 0.22 -0.62 to 0.24 -0.88 .382
C. Therapist competence as predictor of treatment outcome of Mbct
B SE 95% CI t p
Intercept 0.70 3.29 -6.31 to 7.72 0.21 .833
Baseline level of outcome 0.74 0.09 0.57 to 0.92 8.45 <.001
Therapist Competence -0.10 0.68 -1.68 to 1.48 -0.15 .833
• coverage 0.21 0.64 -1.41 to 1.84 0.33 .752
• relational skills -0.16 0.61 -1.59 to 1.27 -0.26 .802
• embodiment -0.16 0.55 -1.57 to 1.25 -0.29 .783
• guiding mindfulness -0.01 0.70 -1.67 to 1.65 -0.15 .988
• didactic teaching -0.01 0.55 -1.29 to 1.28 -0.02 .987
• group environment -0.37 0.63 -1.86 to 1.11 -0.58 .576
** p= <0.05 Total scale and subscale analyses were performed in separate multilevel analyses.

Table 4 Therapist competence as predictor of therapeutic alliance (A) and group cohesion (B).
A. Therapist competence as predictor of therapeutic alliance
B SE 95% CI t p
Intercept 48.2 5.61 36.4 to 60.0 8.59 <.001
Therapist Competence -2.16 1.32 -4.95 to 0.63 -1.64 .120
• coverage -2.33 1.36 -5.34 to 0.67 -1.72 .115
• relational skills -2.1 1.12 -4.35 to 0.15 -1.87 .066
• embodiment -1.39 1.07 -3.87 to 1.07 -1.31 .229
• guiding mindfulness -1.63 1.35 -4.66 to 1.39 -1.21 .256
• didactic teaching -1.55 1.13 -3.95 to 0.84 -1.38 .188
• group environment -1.63 1.31 -4.44 to 1.19 -1.24 .235
B. Therapist competence as predictor of group cohesion
B SE 95% CI t p
Intercept 111 6.87 97.9 to 125 16.25 <.001
Therapist Competence -3.90 1.61 -7.11 to 0.68 -2.42 .018**
• coverage -3.44 1.59 -7.01 to 0.12 -2.163 .056
• relational skills -3.58 1.39 -6.34 to -.81 -2.58 .012**
• embodiment -2.67 1.37 -5.81 to 0.48 -1.94 .086
• guiding mindfulness -3.18 1.71 -7.05 to 0.70 -1.85 .097
• didactic teaching -2.87 1.37 -5.84 to 0.10 -2.10 .057
• group environment -2.72 1.62 -6.24 to 0.80 -1.68 .118
** p= <0.05 Total scale and subscale analyses were performed in separate multilevel analyses.

91
References
1. Gotink, R.A., et al., Standardised mind-fulness-based interventions in healthcare: an overview of systematic reviews and meta-analyses of RcTs. PloS one, 2015. 10(4): p. e0124344.
2. Kuyken, W., et al., Efficacy of mindful-ness-based cognitive therapy in prevention of depressive relapse: an individual patient data meta-analysis from randomized trials. JAmA psychiatry, 2016. 73(6): p. 565-574.
3. Piet, J., H. Wurtzen, and R. Zachariae, The effect of mindfulness-based therapy on symptoms of anxiety and depression in adult cancer patients and survivors: a systemat-ic review and meta-analysis. Journal of Consulting and Clinical Psychology, 2012. 80.
4. Carlson, L.E., et al., Randomized Con-trolled Trial of Mindfulness-Based Cancer Recovery Versus Supportive Expressive Group Therapy for Distressed Survivors of Breast Cancer (mINDSET). Journal of Clinical Oncology 2013. 31: p. 3119-26
5. Garland, S.N., et al., Mindfulness-Based Stress Reduction Compared With Cognitive Behavioral Therapy for the Treatment of Insomnia Comorbid With Cancer: A Ran-domized, Partially Blinded, Noninferiority Trial. Journal of Clinical Oncology, 2014. 32(5): p. 449-457.
6. Johannsen, M., et al., Efficacy of Mind-fulness-Based Cognitive Therapy on Late Post-Treatment Pain in Women Treated for Primary Breast Cancer: A Randomized Controlled Trial. Journal of Clinical Oncology, 2016. 34(28): p. 3390-3399.
7. Lengacher, C.A., et al., Examination of Broad Symptom Improvement Resulting From Mindfulness-Based Stress Reduction in Breast Cancer Survivors: A Randomized Controlled Trial. Journal of Clinical Oncology, 2016. 34(24): p. 2827-2834.
8. Kabat-Zinn, J., Full catastrophe living, revised edition: how to cope with stress, pain and illness using mindfulness meditation. 2013: Hachette uK.
9. Ahn, H.-n. and B.E. Wampold, Where
Oh Where Are the Specific Ingredients? A Meta-Analysis of Component Studies in Counseling and Psychotherapy. Journal of Counseling Psychology, 2001. 48(3): p. 251-257.
10. Messer, S.B. and B.E. Wampold, Let’s Face Facts: Common Factors Are More Potent Than Specific Therapy Ingredients. Clinical Psychology: Science and Prac-tice, 2002. 9(1): p. 21-25.
11. van Aalderen, J.R., et al., The Role of the Teacher in Mindfulness-Based Approaches: A Qualitative Study. Mindfulness, 2014. 5(2): p. 170-178.
12. Kazdin, A.E., Evidence-based treatment and practice: new opportunities to bridge clinical research and practice, enhance the knowledge base, and improve patient care. American psychologist, 2008. 63(3): p. 146.
13. Yalom, I.D., The theory and practice of group psychotherapy. 1995: Basic Books (AZ).
14. Budman, S.H., et al., Cohesion, alliance and outcome in group psychotherapy. Psychiatry, 1989. 52(3): p. 339-50.
15. Beal, D.J., et al., Cohesion and performance in groups: a meta-analytic clarification of construct relations. J Appl Psychol, 2003. 88(6): p. 989-1004.
16. van Andel, P., et al., Group cohesion and working alliance: prediction of treatment outcome in cardiac patients receiving cognitive behavioral group psychotherapy. Psychother Psychosom, 2003. 72(3): p. 141-9.
17. Taube-Schiff, M., et al., Group cohesion in cognitive-behavioral group therapy for social phobia. Behav Res Ther, 2007. 45(4): p. 687-98.
18. Marziali, E., H. Munroe-Blum, and L. McCleary, The contribution of group cohesion and group alliance to the outcome of group psychotherapy. Int J Group Psy-chother, 1997. 47(4): p. 475-97.
19. Trijsburg, R., et al., De ontwikkeling van de Group Cohesion Questionnaire (GcQ). 2004.
20. Evans, N.J. and P.A. Jarvis, The group attitude scale: A measure of attraction to
chapter 4

92
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
group. Small Group Behavior, 1986. 17(2): p. 203-216.
21. Stokes, J.P., Components of group cohesion: Intermember attraction, instrumental value, and risk taking. Small Group Behavior, 1983. 14(2): p. 163-173.
22. Mackenzie, M.J., et al., A qualitative study of self-perceived effects of mindfulness-based stress reduction (mbSR) in a psychosocial oncology setting. Stress and Health, 2007. 23(1): p. 59-69.
23. Schellekens, M.P.J., et al., A qualitative study on mindfulness-based stress reduction for breast cancer patients: how women experience participating with fellow patients. Support Care Cancer, 2016.
24. Bordin, E.S., Theory and research on the therapeutic working alliance: New directions. The working alliance: Theory, research, and practice, 1994: p. 13-37.
25. Luborsky, L., Therapeutic alliances as predictors of psychotherapy outcomes: Fac-tors explaining the predictive success. The working alliance: Theory, research, and practice, 1994: p. 38-50.
26. Martin, D.J., J.P. Garske, and M.K. Davis, Relation of the therapeutic alliance with outcome and other variables: a meta-analyt-ic review. 2000, American Psychological Association.
27. Horvath, A.O., et al., Alliance in indi-vidual psychotherapy. 2011, Educational Publishing Foundation.
28. Horvath, A.O. and L.S. Greenberg, Development and validation of the Working Alliance Inventory. Journal of counseling psychology, 1989. 36(2): p. 223.
29. Snippe, E., et al., The Therapeutic Alliance Predicts Outcomes of Cognitive Behavior Therapy but Not of Mindfulness-Based Cognitive Therapy for Depressive Symptoms. Psychother Psychosom, 2015. 84(5): p. 314-5.
30. Waltz, J., et al., Testing the integrity of a psychotherapy protocol: assessment of adherence and competence. J Consult Clin Psychol, 1993. 61(4): p. 620-30.
31. Fairburn, C.G. and Z. Cooper, Thera-pist competence, therapy quality, and
therapist training. Behav Res Ther, 2011. 49(6-7): p. 373-8.
32. Webb, C.A., R.J. Derubeis, and J.P. Barber, Therapist adherence/competence and treatment outcome: A meta-analytic review. J Consult Clin Psychol, 2010. 78(2): p. 200-11.
33. Kuyken, W. and D. Tsivrikos, Therapist Competence, Comorbidity and Cognitive-Be-havioral Therapy for Depression. Psycho-therapy and Psychosomatics, 2009. 78(1): p. 42-48.
34. Strunk, D.R., et al., Therapist Competence in Cognitive Therapy for Depression: Pre-dicting Subsequent Symptom Change. Jour-nal of Consulting & Clinical Psychology, 2010. 78(3): p. 429-437.
35. Ginzburg, D.M., et al., Treatment specific competence predicts outcome in cogni-tive therapy for social anxiety disorder. Behaviour Research and Therapy, 2012. 50(12): p. 747-752.
36. Branson, A., R. Shafran, and P. Myles, Investigating the relationship between competence and patient outcome with cBT. Behav Res Ther, 2015. 68: p. 19-26.
37. Crane, R.S., et al., Competence in Teaching Mindfulness-Based Courses: Concepts, Development and Assess-ment. Mindfulness, 2012. 3.
38. Huijbers, M.J., et al., Teacher Competence in Mindfulness-Based Cognitive Therapy for Depression and Its Relation to Treatment Outcome. Mindfulness (NY), 2017. 8(4): p. 960-972.
39. Despland, J.N., et al., The role of alliance in the relationship between therapist compe-tence and outcome in brief psychodynamic psychotherapy. J Nerv Ment Dis, 2009. 197(5): p. 362-7.
40. Sharpless, B.A. and J.P. Barber, A concep-tual and empirical review of the meaning, measurement, development, and teaching of intervention competence in clinical psychol-ogy. Clinical Psychology Review, 2009. 29(1): p. 47-56.
41. Weck, F., et al., Therapist competence and therapeutic alliance are import-ant in the treatment of health anxiety

93
(hypochondriasis). Psychiatry Res, 2015. 228(1): p. 53-8.
42. Compen, F.R., et al., Study protocol of a multicenter randomized controlled trial comparing the effectiveness of group and in-dividual internet-based Mindfulness-Based Cognitive Therapy with treatment as usual in reducing psychological distress in cancer patients: the BeMind study. Bmc Psycholo-gy, 2015. 3(1): p. 27.
43. Crane RS, K.W., Williams JMG, Hastings RP, Cooper L, Fennell MJV Competence in teaching mindfulness-based courses: concepts, development and assessment. Mindfulness 2012.
44. Segal, Z.V., et al., The mindfulness-based cognitive therapy adherence scale: Inter-rater reliability, adherence to protocol and treat-ment distinctiveness. Clinical Psychology & Psychotherapy, 2002. 9(2): p. 131-138.
45. Compen F. R , B.E.M., . Van der Lee M. L, Adang E. M. M.,. Donders A. R. T, Speckens A. E. M. , Study protocol of a multicenter randomized controlled trial comparing the effectiveness of group and in-dividual internet-based Mindfulness-Based Cognitive Therapy withtreatment as usual in reducing psychological distress in cancer patients: the BeMind study. Bmc Psycholo-gy 2015. 3(1): p. 27.
46. Zigmond, A.S. and R.P. Snaith, The hospital anxiety and depression scale. Acta Psychiatr Scand, 1983. 67(6): p. 361-70.
47. Spinhoven, P., et al., A validation study of the Hospital Anziety and Depression Scale (HADS) in different groups of Dutch subject. Psychological Medicine, 1997.
48. Bjelland, I., et al., The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res, 2002. 52(2): p. 69-77.
49. Trijsburg, R., et al., De ontwikkeling van de Group Cohesion Questionnaire (GcQ ). 2004, Amsterdam/ Rotterdam: Universi-teit van Amsterdam/ Erasmus Universi-teit Rotterdam.
50. May, A.M., et al., The effect of group cohesion on rehabilitation outcome in cancer survivors. Psycho-Oncology, 2008. 17(9): p. 917-25.
51. Stinckens, N., A. Ulburghs, and L. Claes, De werkalliantie als sleutelelement in het therapiegebeuren. Meting met behulp van de WAV-12, de nederlandstalige verkorte versie van de working alliance inventory. Tijdschr Klin Psychol, 2009. 1: p. 44-60.
52. Hatcher, R.L. and J.A. Gillaspy, Devel-opment and validation of a revised short version of the Working Alliance Inventory. Psychotherapy Research, 2006. 16(1): p. 12-25.
53. Janse, P., et al., Measuring feedback from clients. European Journal of Psy-chological Assessment, 2014.
54. Newman, D.A., Missing data: Five prac-tical guidelines. Organizational Research Methods, 2014. 17(4): p. 372-411.
55. Cillessen, L., et al., Consolidation and pre-diction of long-term treatment effect of group and online mindfulness-based cognitive therapy for distressed cancer patients. Acta Oncol, 2018: p. 1-10.
56. Salvio, M.-A., et al., The strength of the therapeutic alliance in three treatments for depression. Psychotherapy Research, 1992. 2(1): p. 31-36.
57. Spinhoven, P., et al., The therapeutic alliance in schema-focused therapy and transference-focused psychotherapy for bor-derline personality disorder. J Consult Clin Psychol, 2007. 75(1): p. 104-15.
58. Orth, U., How large are actor and partner effects of personality on relationship satis-faction? The importance of controlling for shared method variance. Personality and Social Psychology Bulletin, 2013. 39(10): p. 1359-1372.
59. Swift, J.K. and R.P. Greenberg, Premature discontinuation in adult psychotherapy: A meta-analysis. Journal of consulting and clinical psychology, 2012. 80(4): p. 547.
chapter 4

Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts

Chapter 5
Development and Association of Therapeutic Alliance With Outcome of Internet-Based Mindfulness-Based Cognitive Therapy for Distressed Cancer Patients: Secondary Analysis of a Multicenter Randomized Controlled Trial
This chapter has been published as: Else M. Bisseling, Linda Cillessen, Philip Spinhoven, Melanie P.J. Schellekens, Félix R. Compen, Marije L. van der Lee, Anne E.M. Speckens Journal of Medical Internet Research (2019): 21(9), e14065
Acknowledgement of research support: This research was funded by the Dutch national cancer foundation (KWF Kankerbestrijding) (Grant no. 2012.WO14.C153).

96
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
abstract
background Mindfulness-based cognitive therapy (mBcT) is an evidence-based group-based psychological treatment in oncology, resulting in reduction of depres-sive and anxiety symptoms. Internet-based mBcT (emBcT) has been found to be an effective alternative for mBcT. The therapeutic alliance, that is, the bond between therapist and patient, is known to have a significant impact on psychological treatment outcomes, including mBcT. A primary concern in the practice of emBcT is whether a good therapeutic alliance can develop. Although evidence for the beneficial effect of therapist assistance on treatment outcome in internet-based interventions (IBIs) is accumulating, it is still unclear whether the therapeutic alliance is related to outcome in IBIs.
objective This study aimed to (1) explore whether early therapeutic alliance predicts treatment dropout in (e)mBcT, (2) compare the development of the thera-peutic alliance during emBcT and mBcT, and (3) examine whether early therapeutic alliance is a predictor of the reduction of psychological distress and the increase of mental well-being at posttreatment in both conditions.
Methods This study was part of a multicenter randomized controlled trial (n=245) on the effectiveness of (e)mBcT for distressed cancer patients. The thera-peutic alliance was measured at the start of week 2 (ie, early therapeutic alliance), week 5, and week 9. Outcome measures were psychological distress, measured with the Hospital Anxiety and Depression Scale, and mental well-being, measured with the Mental Health Continuum-Short Form
results The strength of early therapeutic alliance did not predict treatment dropout in (e)mBcT (B=−.39; P=.21). Therapeutic alliance increased over time in both conditions (F(2,90)=16.46; Wilks λ=0.732; P<.001). This increase did not differ between emBcT and mBcT (F(1,91)=0.114; P=.74). Therapeutic alliance at week 2 predicted a decrease in psychological distress (B=−.12; t114=−2.656; P=.01) and an increase in mental well-being (B=.23; t113=2.651; P=.01) at posttreatment. The relationship with reduction of psychological distress differed between treatments: a weaker early therapeutic alliance predicted higher psychological distress at posttreatment in mBcT but not in emBcT (B=.22; t113=2.261; P=.03).
conclusions A therapeutic alliance can develop in both emBcT and mBcT. Findings revealed that the strength of early alliance did not predict treatment drop-out. Furthermore, the level of therapeutic alliance predicted reduced psychological distress and increased mental well-being at posttreatment in both conditions.

97
chapter 5
Interestingly, the strength of therapeutic alliance appeared to be more related to treatment outcome in group-based mBcT than in emBcT.
keyWords
therapeutic alliance; telemedicine; mindfulness, cancer; patient dropouts

98
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
introduction
backgroundFrom 2025 onward, 20 million people worldwide will be diagnosed with cancer each year.1 Approximately one-third of all cancer patients suffer from psychological distress,2 resulting in long-lasting reduced quality of life, decreased compliance with medical care, and prolonged duration of hospital stay.3, 4 Mindfulness-based interventions (mBIs) such as mindfulness-based cognitive therapy (mBcT) 5 are viable psychological treatment options for cancer patients. Mindfulness is defined as ‘Paying attention; on purpose, in the present moment and non-judgmentally’.6 mBIs are effective in reducing psychological distress in cancer patients.7, 8 However, as mBIs typically require in-person attendance at a series of classes over several weeks, many cancer patients experience barriers to participate due to illness, side effects of anticancer treatment, fatigue, limited mobility or transport options.9
Internet-based mBcT (emBcT), overcoming many of these barriers, was found to be as effective as face-to-face (f2f ) group-based mBcT in reducing psychological distress and in improving positive mental health and quality of life in a multicenter randomized controlled trial (RcT) in cancer patients.10 Although treatment dropout was higher in emBcT than in mBcT, this did not influence treatment efficacy. In the long term, the reduction of psychological distress was significantly higher in emBcT than in mBcT.11
The effectiveness of a psychological intervention depends on therapist skills and the strength of the established therapeutic relationship or the therapeutic alliance.12, 13 Therapeutic alliance is defined as the collaborative and affective bond between the therapist and the patient.14, 15 A good alliance means that the patient and therapist are working well toward the goals of the therapy.16 The quality of the therapeutic alliance can attribute to the change in outcome of psychological interventions.17, 18 Alliance measures can assess this working relationship.16 The therapeutic alliance is often assessed with the Working Alliance Inventory (WAI),19 measuring the degree of mutual trust between the client and therapist, their agreement on treatment goals, and their agreement on how to reach these goals. Alliance is commonly measured early, middle, and late in therapy. Early alliance strength does seem to be associated with outcome.16 The significant impact of therapeutic alliance on f2f psychotherapy outcomes has been demonstrated in several meta-analyses.18, 20 It was recently found that therapeutic alliance also predicts the outcome of mBcT in cancer patients.21
A systematic review of the therapeutic alliance in internet-based interventions (IBIs) indicated the development of therapeutic alliance to be equivalent to its

99
chapter 5
development in f2f therapy.22 In addition, Reynolds found that clients (n=30) and therapists (n=30) rated their session impact and alliances in web-based text psychotherapy as strong as previously found in f2f psychotherapy.23 With regard to the association between therapeutic alliance and outcome, findings are mixed. Earlier research found an association between therapeutic alliance and outcome in internet-based cognitive behavioral therapy (cBT) for depression and symptoms of posttraumatic stress24, 25 and in blended cBT for depression.26 In a sample of cancer survivors (n=46), it was found that a strong therapeutic alliance predicted depres-sive symptom reduction in telephone-assisted cBT.27 However, in other studies, no significant relationship between treatment outcome and the therapeutic alliance was found.28, 29 As far as we know, no studies have been conducted on the associa-tion of therapeutic alliance and outcome in emBcT, although online mindfulness interventions are increasingly used.30 To date, findings in internet-based formats are uncertain, and the relationship between therapeutic alliance and outcome of internet-based psychological interventions remains understudied.31 The main aim of this study was to contribute to the ongoing debate in psychotherapy research on the relative importance of the therapeutic relationship on treatment outcome in (internet-based) psychological interventions. Gaining knowledge about whether therapeutic aspects, such as therapeutic alliance, influence outcome in emBcT might improve therapeutic strategies and adequate implementation strategies.
objectivesThe objectives of this study were to (1) explore whether early therapeutic alliance predicts treatment dropout in (e)mBcT, (2) compare the development of the thera-peutic alliance during emBcT and mBcT, and (3) examine whether early therapeutic alliance is a predictor of the reduction of psychological distress and the increase of mental well-being at posttreatment in both conditions.
methods
designThis study was part of a large multicenter RcT (n=245) on the effectiveness of mBcT and emBcT versus treatment as usual (TAu) for distressed cancer patients. The study was registered on Clinicaltrials.gov (NCT02138513) shortly after the start of recruitment, reported following cONSORT guidelines,32 and a protocol paper was published in advance.10, 33. Participants were randomized to mBcT, emBcT, or TAu. After 3 months, patients in TAu were randomly allocated to either mBcT or emBcT.This study involved data from all patients randomized to (e)mBcT, including those patients who were randomized to (e)mBcT after they had completed the 3-month TAu period. The local ethics committee approved this study (cmO Arnhem

100
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Nijmegen 2013/542). All participants provided written informed consent before study enrolment.
study population and procedurePatients were recruited in specialized mental health care institutes for psycho-on-cology via social media, patient associations, and advertorials in local newspapers in the Netherlands. Patients who were interested in participation could enroll themselves at the study website for a screening assessment with the Hospital Anxiety and Depression Scale (HADS). Patients with a score of 11 or greater on the HADS were contacted by telephone by one of the researchers to assess eligibility. Inclusion criteria were as follows: (1) having any cancer diagnosis, (2) experiencing at least mild psychological distress, (3) computer literacy and access to the inter-net, (4) good command of the Dutch language, and (5) willingness to participate in either online or f2f group–based mBcT. Exclusion criteria were as follows: (1) severe psychiatric morbidity such as suicidal ideation or psychosis, (2) change in psychotropic medication within 3 months of baseline, and (3) current or previous participation in mBcT or mindfulness-based stress reduction. Before randomiza-tion, patients completed the baseline assessment.
intervention and therapistsmBIs, such as mBcT,5 are innovative and effective psychological treatment options and have increasingly been applied in somatic health care, including oncology. Mindfulness is defined as intentionally paying attention to present-moment expe-riences in an accepting and nonjudgmental way.34 They were originally developed for patients with chronic somatic conditions to help them cope more effectively with their condition, by increasing the capacity to focus on present-moment expe-riences, even in the presence of internal discomfort, and furthermore to prevent relapse in patients with recurrent major depressive disorders.5 More recently, it has been applied in other conditions.35 A 2012 meta-analysis of 9 RcTs (n=955) of mBIs in cancer patients found significant improvements in depressive and anxiety symptoms.7 Since then, a number of RcTs have replicated the reduction of distress following mBIs.36-40
group-based Mindfulness-based cognitive therapy Patients randomized to group-based mBcT received the intervention according to the mBcT protocol of Segal et al.5 The mBcT protocol was tailored to cancer patients by including cancer-related psychoeducation and adapted movement exercises. The group-based mBcT consisted of 8 weekly 2.5-hour group sessions, one 6-hour silent day, and daily home practice assignments guided by audio files. The sessions consisted of mindfulness practices, sharing experiences, and didactic

101
teachings. Each participant received a folder with information on each session and a cD containing the audio files. The group-based mBcT was provided at the Radboud University Medical Center in Nijmegen, the Jeroen Bosch Hospital in ’s-Hertogenbosch, and 4 mental health institutes specialized in psycho-oncology (Helen Dowling Institute in Bilthoven, Ingeborg Douwes Centrum in Amsterdam, de Vruchtenburg in Rotterdam/Leiden, and Het Behouden Huys in Haren).
internet-based Mindfulness-based cognitive therapyThe emBcT followed exactly the same protocol as the group-based mBcT. The emBcT was mainly text based and included asynchronous written interaction with a therapist over email, similar to the study by Bruggeman-Everts et al.41 Patients were given access to a website divided into a workspace containing 9 sessions (8 weeks+1 full-day silent retreat) and a secured inbox. The silent day consists of a 6-hour program of practicing mindfulness in silence, with various exercises, and a lunch and tea breaks in silence. The therapist initiated the emBcT by sending a welcome message to the patient, personalized with a photo or brief description of oneself as introduction. When patients logged in, they were presented with the overview of all information and assignments due for that week. Each session contained an introductory text; daily formal (eg, sitting meditation) and informal exercises (eg, awareness of everyday activities); and other home practice, with guided audio files and accompanying diaries. They were shown (fictional) patients’ descriptions to emphasize common experiences and clarify the use of the logfiles. The therapist provided written feedback on the completed logfiles via the secured inbox on a prearranged day of the week. Patients were given written instructions after week 5 to prepare for their silent day at home. In the week of the silent day, patients were pro-vided with a program similar to the mBcT silent day. Having completed 4 or more sessions of mBcT was defined as a minimum adequate dose in both interventions.42
therapistsA total of 14 therapists participated: 7 taught both interventions, 2 taught only mBcT, and 5 taught only emBcT. All therapists fulfilled the advanced criteria of the Association of Mindfulness-Based Teachers in the Netherlands and Flanders, which are in concordance with the uK Mindfulness-Based Teacher Trainer Network Good Practice Guidelines.43 All therapists had previous experience in working with oncology patients and received a 2-day training workshop in the mBcT study protocol at the start of the study. Moreover, 2 additional day-long supervision meetings were organized during the intervention phase of 1 year and 6 months. Therapists without previous emBcT experience were provided with guidelines and were supervised by more experienced emBcT therapists.
chapter 5

102
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
measures
therapeutic allianceTherapeutic alliance was measured with a translated and shortened form of the WAI,19 which was administered at the start of week 2, week 5, and week 9. The WAI consists of 3 subscales assessing (1) how closely client and therapist agree on and are mutually engaged in the goals of treatment; (2) how closely client and thera-pist agree on how to reach the treatment goals; and (3) the degree of mutual trust, acceptance, and confidence between the client and therapist. Items were scored on a 5-point scale ranging from rarely (0) to always (5).44, 45 The 12-item inventory was validated in a Dutch-speaking sample, showing an internal consistency of greater than 0.80 for all separate subscales and 0.87 for the total scale.46 The scale was used before in oncology patients following emBcT.47 Internal consistency of the total scale of the version used in this study was high (Cronbach alpha=.93).
psychological distressPsychological distress was measured with the 14-item HADS developed to measure depression and anxiety in general medical populations.32 Items were scored on a 4-point scale ranging from rarely (0) to almost always (4). It has been validated in medical populations, including cancer patients,48 and has adequate psycho-metric properties to detect distress and to screen for psychiatric disorders in cancer patients.49, 50 Internal consistency of the total scale in the present sample was high (Cronbach alpha=.87). Patients completed the HADS before and after the intervention.
Mental well-beingMental well-being was measured by the Mental Health Continuum-Short Form (mHc-SF) 51, which comprises 14 items, representing various feelings of well-being in the past month rated on a 6-point Likert scale from never (0), once or twice a week (1), about once a week (2), 2 or 3 times a week (3), almost every day (4), and every day (5). The mHc-SF contains 3 subscales: emotional, psychological, and social well-being. The short form of the mHc-SF has shown excellent internal consis-tency (>0.80). The test-retest reliability of the mHc-SF over 3 successive 3-month periods was 0.68, and the 9-month test-retest in a Dutch sample was 0.65.52 Internal consistency of the total scale in the sample used in this study was high (Cronbach alpha=.97). Patients completed the mHc-SF before and after the intervention.
statistical analysesAll analyses were conducted in SPSS version 25.0 (IBm Corp, 2017). Differences between conditions and between completers and noncompleters (<4 sessions

103
attended) in demographic and clinical variables were tested with chi-square tests and t tests. To test whether strength of alliance predicted dropout of emBcT and mBcT, binary logistic regression analyses were used. For further analyses, we only included patients who completed (e)mBcT (n=163). To test the development of the therapeutic alliance during emBcT and mBcT, repeated-measures analyses of variance were used. To examine whether therapeutic alliance predicted outcome and whether this was different in the 2 conditions, separate hierarchical linear regression models were conducted. The dependent variable was posttreatment psychological distress (HADS) or mental well-being (mHc-SF). In the first step, independent variables were the baseline level of psy-chological distress or mental well-being and condition (mBcT/emBcT). In the second step, therapeutic alliance at week 2 was included as predictor. In the third step, the interaction between condition and therapeutic alliance was added to test moderation.
results
participantsOf the cancer patients participating in the RcT (n=245), 125 were randomized to emBcT and 120 were randomized to mBcT. Of all patients (n=125) randomized to emBcT, 22 (19.2%) declined participation after randomization. Of all patients (n=120) randomized to mBcT, 25 (20.8%) declined participation after randomization (see Figure 1). Participants were mostly female, middle aged, and highly educated. Most patients were diagnosed with breast cancer and were treated with a curative intent (see Table 1).
chapter 5

Figure 1 Flowchart
Dropoutintervention
(n=11)Medical reason (n=4)
Other expectations (n=3)Familiar with Mnf (n=1)
Not specified (n=1)Too burdensome (n=1)No motivation (n=1)
Randomized(n=245)
Group-basedMbct(n=43)
eMbct(n=35)
Treatmentas usual(n=78)
eMbct(n=90)
Group-basedMbct(n=77)
CompletedGroup-based
Mbct(n=84)
Group-basedMbct
(n=120)
StartedGroup-based
Mbct(n=95)
CompletedeMbct(n=78)
eMbct(n=125)
StartedeMbct(n=102)
Declined afterrandomization
(n=25)Schedule (n=10)
Medical reason/died (n=4)Other expectations (n=3)
Distance (n=3)Not specified (n=4)
Psych treatment (n=1)
Declined afterrandomization
(n=23)Schedule (n=3)
Medical reason/died (n=1)Other expectations (n=3)
Not specified (n=8)Wanted Mbct (n=7)Other Psychological
treatment (n=1)
Dropoutintervention
(n=24)Schedule (n=4)
Medical reason (n=2)Other expectations (n=6)
Not specified (n=5)Too burdensome (n=3)
No motivation (n=1)Computer difficulties (n=1)

Characteristics Mbct
(n=120)eMbct
(n=125)Test statistic (chi-square)
Test statistic (t )
P value
Sociodemographics
Gender, n (%)
Female 101 (84.2) 109 (87.2) 0.46 .50
Relation, n (%)
Yes 102 (85) 100 (80) 1.58 .40
Children, n (%)
Yes 79 (65.8) 90 (72) 1.09 .30
Education level, n (%)
Low/middle 35 (29.2) 44 (35.4) 1.02 .31
High 85 (70.8) 81 (64.8) 1.02 .31
Age (years), mean (SD)
51.5 (11.1) 51.8 (10.2) −0.18 .86
Clinical
Cancer diagnosis, n (%)
Breast 75 (62.5) 76 (60.8) 0.08 .78
Other 45 (37.5) 49 (39.2) 0.08 .78
Treatment intent, n (%)
Curative 104 (86.7) 102 (81.6) 1.17 .28
Palliative 16 (13.3) 23 (18.4) 1.17 .28
Current anticancer treatment, n (%)
Yes 56 (46.7) 60 (48) 0.44 .83
Psychiatric diagnosis, n (%)
Yes 44 (36.0) 45 (36.7) 0.012 .91
Time since diagnosis, mean (SD)
3.5 (5.0) 3.4 (4.4) 0.21 .84
Psychological distress, Hospital Anxi-ety and Depression Scale, mean (SD)
18.2 (6.7) 16.9 (6.9) 1.49 .14
Mental well-being, Mental Health Continuum-Short Form, mean (SD)
35.0 (12.8) 37.4 (13.6) −1.46 .15
Table 1 Sample characteristics per intervention (mindfulness-based cognitive therapy/internet-based mindfulness-based cognitive therapy).
aBoth categories include the patients that were initially randomized to the tau group.

106
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
dropoutOf the patients who started the (e)mBcT (n=198), 35 (17.7%) dropped out of the intervention. Dropout rate in emBcT (n=24, 12.1%) was significantly higher than that in mBcT (n=11, 5.6%; P=.03). There were no differences in sociodemographics between participants who completed the (e)mBcT and those who did not.
Patients who dropped out after the first sessions did not fill out the WAI question-naire and, consequently, were not included in the analyses testing whether early therapeutic alliance predicted dropout of emBcT and mBcT. However, reasons for dropout after session 1 were collected. Main reason was that the intervention was not as expected (n=6, 25.7%). Other reasons for dropout are summarized in Multimedia Appendix 1.
Analyses testing whether early therapeutic alliance predicted dropout of emBcT and mBcT revealed that there was no significant difference in early therapeutic alliance between participants who dropped out of the intervention (mean 33.3, SD 7.9) and those who completed the (e)mBcT (mean 36.6, SD 9.5; P=.23). Moreover, this effect was not moderated by treatment condition, as there was no significant interaction between condition and the therapeutic alliance at the start of week 2 in association with dropout (B=−0.13; P=.08).
developMent of therapeutic allianceAs shown in Figure 2, level of therapeutic alliance increased significantly over time (F2,90=16.46; Wilks ʎ=0.732; P<.001) and did not differ significantly between conditions (P=.74). There was no significant interaction between condition and time (F2,90=1.636; Wilks ʎ=0.965; P=.20), implying that the development of therapeutic alliance did not differ between emBcT and mBcT either.
association of therapeutic alliance with treatMent outcoMe As you can see in Table 2 en Table 3, early therapeutic alliance predicted both reduc-tion of psychological distress (B=−.12; t114=−2.656; P=.01) and increase of mental well-being (B=.23; t113=2.651; P=.01) at posttreatment. Adding the interaction term between early therapeutic alliance and condition resulted in a significant increase in explained variance (∆R2=0.031; F1,114=6.622; P=.01). The relationship between early therapeutic alliance and psychological distress at posttreatment was moderated by condition (B=.22; t113=2.245; P=.03).

107
Figure 2 Mean level of therapeutic alliance throughout Mbct and eMbct.
50
40
30
35
45
0 2 4 6 8 10Week
wai
-tot
aal
mbct
embct
Therapeutic alliance
Table 2 Relationship between therapeutic alliance and Psychological distress: regression analyses.
Variables Regression analyses Psychological distress Predictor
F value (df ) P value Adjusted R2 B t113 P value
Psychological distress baseline 42.72 (2, 115) <.001 0.416 .58 8.69 <.001
Condition 42.72 (2, 115) <.001 0.416 −2.3 −2.36 .011
Therapeutic alliance week 2a 32.08 (3, 114) <.001 0.443 −.12 −2.573 .01
Therapeutic alliance week 2 × conditiona
26.17 (4, 113) <.001 0.463 .22 2.245 .03
a Corrected for baseline psychological distress and the condition, and the predictor × intervention inter-action and psychological distress at posttreatment with separate hierarchical linear regressions (n=163).
Table 3 Relationship between working alliance and Mental well-being: regression analyses.
Variables Regression analyses Mental well-being Predictor
F value (df ) P value Adjusted R2 B t113 P value
Mental well-being baseline 65.26 (2, 115) <.001 .523 .76 10.84 <.001
Condition 65.26 (2, 115) <.001 .523 1.9 1.16 .24
Therapeutic alliance week 2b 48.15 (3, 114) <.001 .547 .24 2.66 .01
Therapeutic alliance week 2 × conditionb
36.07 (4, 113) <.001 .545 −.12 −.697 .49
b Corrected for baseline mental well-being and the condition, and the predictor×intervention interac-tion and mental well-being at posttreatment with separate hierarchical linear regressions (n=163).
chapter 5

108
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Examination of the interaction plot showed that participants of the group-based mBcT with a weaker early therapeutic alliance showed a significant higher level of psychological distress at posttreatment than those of emBcT (P=.004; see also Multimedia Appendix 2).
discussion
principal f indingsThe aims of this study were to (1) explore whether the strength of early therapeutic alliance predicts treatment dropout in (e)mBcT, (2) compare the development of the therapeutic alliance during emBcT and mBcT, and (3) examine whether early therapeutic alliance is a predictor of the reduction of psychological distress and the increase of mental well-being at posttreatment in both conditions. Results showed that early alliance did not predict dropout and that the development of the therapeutic alliance did not differ between emBcT and mBcT. In addition, early therapeutic alliance predicted the reduction of psychological distress and improvement of mental well-being at posttreatment. Moreover, we found that the association between a weaker therapeutic alliance and smaller reduction of psychological distress was stronger in group-based mBcT than in emBcT. In our sample, dropout rates in emBcT were somewhat higher than those in mBcT. This is in line with previous research findings that dropout rates in emBcT are relatively high.10, 53 We could not confirm previous findings that a strong early alliance prevents patients from dropping out of psychological treatment.54 In this respect, we would like to stress that our findings should be interpreted with caution. We were unable to include data from patients who dropped out after the first session because early therapeutic alliance was measured at the start of the second session. The main reason for dropping out after the first session was ‘other expectations’. This finding stresses the importance of clearly explaining the treat-ment rationale and developing a shared understanding with patients at the start of (e)mBcT. In our study, the therapist initiated the contact in emBcT by sending a welcome message to the patient. As it was previously found in a qualitative study that in emBcT asynchronicity of therapist contact/feedback is experienced by some patients as uncomfortable,9 adding an (f2f ) appointment with the therapist at the start of emBcT and synchronous therapist assistance in the early treatment phase might be useful to prevent dropout. Moreover, it was previously found that therapists seem concerned with the level of continuity of the training. Missing out on nonverbal information of patients made them unable to spot withdrawal at an early stage.9 Alliance building may enhance engagement to treatment. So far, quantitative studies concerning the association of therapeutic alliance and adherence to IBIs are missing. Knowledge about alliance and adherence can be

109
important to define the optimal level of therapist support in IBIs.31
Regarding the association of therapeutic alliance and outcome, our findings are in line with previous (meta-analytic) research findings, showing that the therapeutic alliance is associated with outcome in f2f psychotherapy,18, 20 including mBcT21 and IBIs.24, 25 An explanation for the finding that the strength of the early alliance affects the outcome more in mBcT than in emBcT could be that in a group-based setting, patients with a weak therapeutic alliance might conceal themselves in the group and might put in less effort to share experiences or practice. This might explain why psychological distress levels of those patients remained high compared with patients who experienced a strong therapeutic alliance. As a consequence, partic-ularly in group-based settings, mindfulness therapists should be aware of their way of bonding with patients. Although we did not investigate this in our study, it has been previously found that for patients who have difficulties in building a relationship with others, which might be reflected in a weak therapeutic alliance, therapists who model effective ways of forming a strong alliance can process the formation of a strong (repaired) alliance,55, 56 which in turn may lead to better out-come. Another explanation for this finding could be that in individual emBcT, one’s self-efficacy and intrinsic motivation are also important for treatment outcome than the experienced therapeutic alliance.11 This is in line with previous qualitative findings in emBcT for cancer patients, which revealed that participants stressed the importance of self-discipline, and the individual nature as facilitators for emBcT9 suggesting that experienced motivation and discipline is also related to outcome.
strengths and liMitationsA major strength of this study was that we directly compared the development of therapeutic alliance between patients participating in emBcT and mBcT. Except for the delivery format, both interventions were similar in content. Moreover, we investigated the relationship between therapeutic alliance and treatment outcome both in terms of symptom reduction and mental well-being. Some limitations, however, need to be mentioned. At first, this study was conducted in a self-selected group of distressed cancer patients. Although this is in line with patients seeking help in clinical practice, this might limit the extent to which the findings of the present study generalize to the broader population of cancer patients.57, 58 Second, an inclusion criterium was that participants would agree with randomization to an f2f or online intervention. Our inclusion criterium might have prevented patients that were not interested in online interventions from participating. This might limit the extent to which the present findings generalize to the broader population of cancer patients.
chapter 5

110
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
research iMplicationsFurther research should investigate the relation between therapeutic alliance and dropout more thoroughly, for instance, by measuring therapeutic alliance after each session. It would also be interesting to focus on examining what therapeutic techniques might be suitable to improve the development of a strong therapeutic alliance, both in emBcT and mBcT. Further research in emBcT could examine how therapeutic alliance can develop in different (e)mBcT formats and how this influences treatment outcome. Treatment formats could vary from blended care to intensive synchronous individual therapist-assisted emBcT to stand-alone emBcT with computerized feedback.
clinical iMplicationsAs dropout rates were somewhat higher in emBcT, efforts should be taken to prevent dropout. It is of interest to shed more light on how to encourage patients to adhere to the treatment. Building a good therapeutic alliance is of clinical importance in (e)mBcT. By measuring therapeutic alliance as a routine outcome after every session, therapists can be encouraged to really tune in to patient’s needs and adjust their therapy or their therapeutic attitude at an early treatment stage, which may benefit treatment outcome in both mBcT and emBcT.
AcknowledgementsAcknowledgments: This research was funded by the Dutch national cancer founda-tion (KWF Kankerbestrijding) (Grant no. 2012.WO14.C153).We would like to thank all patients and therapists who participated in this study, and Heidi Willemse, Eva Witteveen and David Huijts for their help in gathering data.
Conflicts of InterestNone declared
AbbreviationscBT cognitive behavioral therapyemBcT internet-based mindfulness-based cognitive therapyHADS Hospital Anxiety and Depression ScaleIBI internet-based interventionicBT internet-based cognitive behavioral therapymBI mindfulness-based intervention mBcT mindfulness-based cognitive therapy RcT randomized controlled trialTAu treatment as usualWAI Working Alliance Inventory

Multimedia Appendix 1 Dropout rates and reasons for dropout per condition
Dropout Reason After week 1 After week 2 After week 3 Total
Mbct Other expectations 2 1 0 3
Too burdensome 0 1 0 1
No reason provided 0 0 1 1
Schedule 0 0 0 0
Familiar with mindfulness 1 0 0 1
No motivation 1 0 0 1
Medical reason 1 1 2 4
Computer difficulties 0 0 0 0
5 3 3 11
eMbct Other expectations 4 1 1 6
Too burdensome 1 1 1 3
No reason provided 3 1 1 5
Schedule 2 1 1 4
Familiar with mindfulness 0 0 0 0
No motivation 0 0 0 1
Medical reason 0 1 1 2
Computer difficulties 2 1 0 3
13 6 5 24
Multimedia Appendix 2 The association of early therapeutic alliance and outcome per condition.
20
10
5
15
low highTherapeutic alliance week 2
had
s p
ost t
reat
men
t
mbct
embct
Therapeutic alliance

112
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
References
1. Bray F., Transitions in human development and the global cancer burden. In: Wild CP, Stewart B, eds. World Cancer Report. Lyon: International Agency for Research on Cancer, 2014. World Cancer Report, 2014: p. 54-68.
2. Carlson L, Angen M, Cullum J, Goodey E, Koopmans J, et al., High levels of untreated distress and fatigue in cancer patients. British Journal of Cancer, 2004. 90(12): p. 2297-2304.
3. Mitchell AJ, Chan M, Batti H, Halton M, Grassi L, et al., Prevalence of depression, anxiety, and adjustment disorder in oncolog-ical, haematological, and palliative-care set-tings: a meta-analysis of 94 interview-based studies. Lancet Oncology, 2011. 12(2): p. 160-74.
4. Mitchell AJ, Ferguson DW, Gill J, Paul J, Symonds P, et al., Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: a systematic review and meta-analysis. Lancet Oncolo-gy, 2013. 14(8): p. 721-32.
5. Segal ZV, Williams JMG, Teasdale JD., Mindfulness-based cognitive therapy for depression: A new approach to relapse pre-vention. 2013, New York: Guilford Press.
6. Kabat-Zinn J, Full catastrophe living, revised edition: how to cope with stress, pain and illness using mindfulness meditation. 2013: Hachette uK.
7. Piet J, Wurtzen H, Zachariae R., The Effect of Mindfulness-Based Therapy on Symptoms of Anxiety and Depression in Adult Cancer Patients and Survivors: A Sys-tematic Review and Meta-Analysis. Journal of Consulting and Clinical Psychology, 2012. 80(6): p. 1007-1020.
8. Zainal NZ, Booth S, Huppert FA., The ef-ficacy of mindfulness-based stress reduction on mental health of breast cancer patients: a meta-analysis. Psycho-Oncology, 2013. 22(7): p. 1457-1465.
9. Compen FR, Bisseling EM, Schellekesn MPJ, Jansen E, van der Lee ML, et al. Mindfulness-Based Cognitive Therapy for
Cancer Patients Delivered via Internet: Qualitative Study of Patient and Thera-pist Barriers and Facilitators. Journal of Medical Internet Research, 2017. 19(12): p. e407.
10. Compen F, Bisseling EM, Schellek-ens MPJ, Donders R, Carlson L, et al., Face-to-Face and Internet-Based Mindful-ness-Based Cognitive Therapy Compared With Treatment as Usual in Reducing Psy-chological Distress in Patients With Cancer: A Multicenter Randomized Controlled Trial. Journal of Clinical Oncology, 2018: p. 10;36(23):2413-2421
11. Cillessen L, Schellekens MPJ, van der Ven MOM, Donders ART,Compen FR, et al., Consolidation and prediction of long-term treatment effect of group and online mindfulness-based cognitive therapy for distressed cancer patients. Acta Oncologica, 2018: p. 1-10.
12. Kissane DW, et al., Cognitive-existential group psychotherapy for women with pri-mary breast cancer: a randomised controlled trial. Psycho-Oncology: Journal of the Psychological, Social and Behavioral Dimensions of Cancer, 2003. 12(6): p. 532-546.
13. Wise TN, Biondi M, Costantini A, Psy-cho-oncology. 2013: American Psychiatric Pub.
14. Bordin ES, Theory and research on the therapeutic working alliance: New directions. The working alliance: Theory, research, and practice, 1994: p. 13-37.
15. Luborsky L, Therapeutic alliances as predictors of psychotherapy outcomes: Fac-tors explaining the predictive success. The working alliance: Theory, research, and practice, 1994: p. 38-50.
16. Muran JC, Barber JP, The therapeutic al-liance: An evidence-based guide to practice. 2011: Guilford Press.
17. Horvath AO, Symonds BD, Relation between working alliance and outcome in psychotherapy: A meta-analysis. Journal of counseling psychology, 1991. 38(2): p. 139-149.
18. Horvath AO, Del Re AC, Flückiger

113
C, Symonds D. Alliance in individual psychotherapy. Psychotherapy, 2011. 48(1): p. 9-16.
19. Horvath AO, Greenberg LS, Development and validation of the Working Alliance Inventory. Journal of counseling psychol-ogy, 1989. 36(2): p. 223-233.
20. Martin DJ, Garske JP, and Davis MD, Relation of the therapeutic alliance with out-come and other variables: a meta-analytic review, 2000, Journal of Consulting and Clinical Psychology, 68(3), 438-450.
21. Bisseling EM, Schellekens MPJ, Spin-hoven P, Compen FR, Speckens AEM, et al. Therapeutic alliance -not therapist competence or group cohesion- contributes to reduction of psychological distress in group-based Mindfulness-Based Cognitive Therapy for cancer patients. Clinical Psychology and Psychotherapy, 2019.
22. Sucala M, Schnur JB, Constantino MJ, Miller SJ, Brackman EH, et al. The ther-apeutic relationship in e-therapy for mental health: a systematic review. Journal of Medi-cal Internet Research, 2012. 14(4): p. e110.
23. Reynolds DJ jr, Stiles WB, Bailer AJ, Hughes MR. Impact of exchanges and cli-ent-therapist alliance in online-text psycho-therapy. Cyberpsychological Behavioral Social Network, 2013. 16(5): p. 370-7.
24. Bergman Nordgren L, Carlbring P, Linna E, Andersson G. Role of the Work-ing Alliance on Treatment Outcome in Tai-lored Internet-Based Cognitive Behavioural Therapy for Anxiety Disorders: Randomized Controlled Pilot Trial. JmIR Res Protoc, 2013. 2(1): p. e4.
25. Wagner B, Brand J, Schulz W, Knaev-elsrud C.Online working alliance predicts treatment outcome for posttraumatic stress symptoms in arab war-traumatized patients. Depression and Anxiety, 2012. 29(7): p. 646-651.
26. Ly KH, Topooco N, Cederlund H, Wallin A, Bergstrom J,et al. Smartphone-Support-ed versus Full Behavioural Activation for Depression: A Randomised Controlled Trial. PLoS One, 2015. DOI: 10.1371/journal.pone.0126559
27. Applebaum AJ, DuHamel KN, Winkel G, Rini C, Greene PB, et al. Therapeutic alli-ance in telephone-administered cognitive-be-havioral therapy for hematopoietic stem cell transplant survivors. J Consulting Clinical Psychology, 2012. 80(5): p. 811-6.
28. Knaevelsrud C, Maercker A. Does the quality of the working alliance predict treat-ment outcome in online psychotherapy for traumatized patients? J Medical Internet Research, 2006. 8(4): p. e31.
29. Preschl B., Maercker A, Wagner B. The working alliance in a randomized controlled trial comparing online with face-to-face cognitive-behavioral therapy for depression. Bmc Psychiatry, 2011. 11: p. 189.
30. Plaza I, Demarzo M, Herrera-Mercaldel P, Garcia-Camparo J. Mindfulness-based mobile applications: literature review and analysis of current features. JmIR mHealth and uHealth, 2013. 1(2): p. e24.
31. Pihlaja, S., et al., Therapeutic alliance in guided internet therapy programs for depres-sion and anxiety disorders - A systematic review. Internet Interventions, 2018. 11: p. 1-10.
32. Schulz KF, Altman DG, Moher D, cON-SORT 2010 statement: updated guidelines for reporting parallel group randomised trials. Bmc medicine, 2010. 8(1): p. 18.
33. Compen, F.R., Bisseling EM, van der Lee ML, Adang EMM, Donders ART, et al. Study protocol of a multicenter randomized controlled trial comparing the effectiveness of group and individ-ual internet-based Mindfulness-Based Cognitive Therapy with treatment as usual in reducing psychological distress in cancer patients: the BeMind study. Bmc Psychology, 2015. 3(1): p. 27.
34. Kabat-Zinn J, Full catastrophe living: Using the wisdom of your body and mind in every-day life. New York: Delacorte, 1990.
35. Crane R, Mindfulness-based cognitive ther-apy: Distinctive features. 2017: Routledge.
36. Carlson LE, Doll R, Stephen J, Faris P, Tamagawa R, et al. Randomized controlled trial of Mindfulness-based cancer recovery versus supportive expressive group therapy
chapter 5

114
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
for distressed survivors of breast cancer. Journal of Clinical Oncology, 2013. 31(25): p. 3119-3126.
37. Garland SN, Carlson L, Stephens A, Antle M, Samuals C, et al. Mindful-ness-Based Stress Reduction Compared With Cognitive Behavioral Therapy for the Treatment of Insomnia Comorbid With Cancer: A Randomized, Partially Blinded, Noninferiority Trial. Journal of Clinical Oncology, 2014. 32(5): p. 449-457.
38. Lengacher CA, Reich C, Paterson C, Ramesar S, Park j, et al. Examination of Broad Symptom Improvement Resulting From Mindfulness-Based Stress Reduction in Breast Cancer Survivors: A Randomized Controlled Trial. Journal of Clinical On-cology, 2016. 34(24): p. 2827-2834.
39. Johannsen M, O’Connor M, O’TooleM, Jensen A, Hojris A, et al., Efficacy of Mindfulness-Based Cognitive Therapy on Late Post-Treatment Pain in Women Treated for Primary Breast Cancer: A Randomized Controlled Trial. Journal of Clinical On-cology, 2016. 34(28): p. 3390-3399.
40. Schellekens MPJ, van den Hurk DGM, Prins JB, Donders ART, Molema J, et al. Mindfulness-Based Stress Reduction added to care as usual for lung cancer patients and/or their partners: A multi-centre randomized controlled trial. Psycho-Oncology, 2017: p. 2118-2126.
41. Everts FZB, van der Lee ML,, de Jager Meezenbroek E. Web-based individual Mindfulness-Based Cognitive Therapy for cancer-related fatigue—A pilot study. Inter-net Interventions, 2015. 2(2): p. 200-213.
42. Crane C, Williams JMG. Factors associ-ated with attrition from mindfulness-based cognitive therapy in patients with a history of suicidal depression. Mindfulness, 2010. 1(1): p. 10-20.
43. Crane RS, Williams JMG, Hastings RP, Cooper L, Fennell MJV. Competence in teaching mindfulness-based courses: concepts, development and assessment. Mindfulness 2012.
44. Stinckens N, Ulburghs A, Claes L., De werkalliantie als sleutelelement in het
therapiegebeuren. Meting met behulp van de WAV-12, de nederlandstalige verkorte versie van de working alliance inventory. Tijdschr Klinische Psychologie, 2009. 1: p. 44-60.
45. Hatcher RL, Gillaspy JA. Development and validation of a revised short version of the Working Alliance Inventory. Psycho-therapy Research, 2006. 16(1): p. 12-25.
46. Janse P, et al. Measuring feedback from clients. European Journal of Psychologi-cal Assessment, 2014.
47. Wolvers MD, Bruggemans-Everts FZ, van der Lee ML, vande Schoot R, Vollenbroek-Hutten MMR. Effectiveness, mediators, and effect predictors of internet interventions for chronic cancer-related fatigue: the design and an analysis plan of a 3-armed randomized controlled trial. JmIR research protocols, 2015. 4(2).
48. Bjelland I, Dahl A,Haug T, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. Journal of Psychosomatic Research, 2002. 52(2): p. 69-77.
49. Mitchell AJ, Meader N, Symonds P, Diagnostic validity of the Hospital Anxiety and Depression Scale (HADS) in cancer and palliative settings: a meta-analysis. Journal of affective disorders, 2010. 126(3): p. 335-348.
50. Vodermaier A, Linden W, Siu C., Screen-ing for emotional distress in cancer patients: a systematic review of assessment instru-ments. Journal of the National Cancer Institute, 2009. 101(21): p. 1464-1488.
51. Keyes CL., Mental illness and/or mental health? Investigating axioms of the complete state model of health. Journal of consult-ing and clinical psychology, 2005. 73(3): p. 539.
52. Lamers SM, Westerhof G, Bohlmei-er ET, ten klooster PM, Keyes CLM, Evaluating the psychometric properties of the mental health continuum-short form (mHc-Sf). Journal of clinical psychology, 2011. 67(1): p. 99-110.
53. Bruggeman-Everts FZ, Wolvers MDJ, van de Schoot R, Volenbroek-Hutten MMR, van der Lee ML, Effectiveness of

115
Two Web-Based Interventions for Chronic Cancer-Related Fatigue Compared to an Ac-tive Control Condition: Results of the ‘Fitter na kanker’ Randomized Controlled Trial. Journal of Medical Internet Research, 2017. 19(10): p. e336.
54. Swift JK, Greenberg RP, Premature discontinuation in adult psychotherapy: a meta-analysis. Journal Consultating Clinical Psychology, 2012. 80(4): p. 547-59.
55. Tsai M, Kohlenberg RJ, Kanter JW, A functional analytic psychotherapy (fAP) approach to the therapeutic alliance. The therapeutic alliance: An evidence-based guide to practice, 2010: p. 172-190.
56. Zilcha-Mano S, Errazuriz P, Early development of mechanisms of change as a predictor of subsequent change and treat-ment outcome: The case of working alliance. Journal Consulting Clinical Psychology, 2017. 85(5): p. 508-520.
57. Berger T, The therapeutic alliance in internet interventions: A narrative review and suggestions for future research. Psycho-therapy Research, 2017. 27(5): p. 511-524.
58. Berger T, Boettcher J, Caspar F, Inter-net-based guided self-help for several anxiety disorders: a randomized controlled trial comparing a tailored with a standardized disorder-specific approach. Psychotherapy (Chic), 2014. 51(2): p. 207-19.
chapter 5

Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Are you okay with vulnerability or are you someone who says: no, I don’t want this. That’s what it depends on very much, I think’.
Early empowerment. Participants mentioned the value of being able to make their own decision about whether and when to take part. They preferred to be informed about mBSR as soon as possible in order to do so. It seemed to strengthen the sense of autonomy in patients.
‘You’re in the hospital regularly anyway, they could address it sooner.. Then you can decide for yourself, well it’s too early for me or oh, I would like that.’
Participation too early. A possible barrier of being informed about the mBSR train-ing at an early stage is that patients may participate too early to fully benefit from the program. Some patients mentioned they were not emotionally prepared to participate, they felt too vulnerable to become aware of their thoughts and feelings.
‘I wanted something quickly, but in hindsight I think it might have been better to start a little bit later. Seeing what the chemo did to me, particularly mentally.’
discussion
This mixed method study explored what patients experience as a suitable stage to participate in mBSR. Our quantitative findings confirmed previous studies in showing that in the whole group of breast cancer patients mBSR resulted in a reduc-tion of psychological distress.8, 9 The quantitative data showed that participating during or after anticancer treatment interacts with changes in mindfulness. Those participating after anticancer treatment seem to improve more, however, this could possibly be explained by lower baseline scores. The qualitative data revealed that although participating in mBSR during anticancer treatment helped patients to cope with the treatment, their physical symptoms could also hinder participation. After anticancer treatment their gain in energy facilitated participation in mBSR, but some patients mentioned they participated too late to fully benefit. Finally, in addition to the cancer treatment phase, right timing also seemed to depend on the stage of emotional processing. Women emphasized the importance of being informed about the possibility to take part in mBSR at an early stage as it enabled them to decide for themselves whether and when to enroll. These qualitative findings are in line with former studies showing that patients would like to be offered psychological interventions soon after diagnosis.26-28 A

Chapter 6
Mindfulness-Based Stress Reduction for breast cancer patients: A mixed method study onwhat patients experience as a suitable stage to participate
This chapter has been published as:
Else M. Bisseling, Melanie P.J. Schellekens, Ellen T.M. Jansen, Hanneke W.M. van Laarhoven, Judith B. Prins, Anne E.M. Speckens Supportive Care in Cancer (2017):25(10):3067-3074
Acknowledgments: This research was funded by the funding agency for breast cancer Pink Ribbon.

118
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
abstract
purpose Breast cancer is associated with high levels of psychological distress. Mindfulness Based Stress Reduction (mBSR) has proven to be effective in reducing distress in cancer patients. In several studies patients who are currently undergoing somatic anticancer treatment are excluded from participating in mBSR. Little is known about what would be the most suitable stage of disease to offer mBSR. We examined whether stage of disease facilitated and/or hindered participation in mBSR for breast cancer patients.
Method A mixed method design was used. Self-report questionnaires on psy-chological distress (HADS) and quality of life (EORTc QLQ-c30) were administered before and after mBSR. Five focus groups and three semi-structured individual interviews were conducted. Qualitative data were analyzed with the constant com-parative method in order to develop a grounded theory.
results 64 females participated in mBSR. In 52 patients who completed the questionnaires, psychological distress improved significantly. Qualitative data showed that participating in mBSR both during and after anticancer treatment has specific advantages and disadvantages. Interestingly, being emotionally ready to take part in mBSR seems equally important as physical ability. Informing patients at an early stage seemed to strengthen autonomy and self-management skills.
conclusions In contrast to the common practice to tailoring the timing of mBSR to physical impairments or demands of the anticancer treatment, our find-ings revealed that emotional readiness is equally important to take into account. These findings might support professionals in their choices whether and when to inform and refer patients to mBSR.
key Words
breast cancer, mindfulness, mBSR, timing, disease stage, qualitative

119
chapter 6
introduction
Breast cancer is the most common cancer among women with an estimated 1.67 million new cancer cases each year.1 The invasive treatment and physical symptoms have a major impact on patients’ wellbeing. Henselmans2 showed that during active anticancer treatment 33% of breast cancer patients suffer from psychological distress, 15% of patients experience distress directly after treatment in the reentry phase, and another 15% remain distressed for several years. So, psychological con-sequences of the cancer and/or its treatment seem to be long-lasting.3 Psychological interventions have been shown to be effective in reducing these symptoms.4-6 An innovative intervention in cancer patients is Mindfulness-Based Stress Reduction (mBSR). Mindfulness is defined as intentionally paying attention to present-moment experiences in an accepting and non-judgmental way.7 Recent meta-analyses con-cluded that mBSR and other mindfulness-based interventions (mBIs) are effective in decreasing psychological distress in cancer patients,8, 9 including reductions of anxiety and depressive symptoms and improvement of quality of life. With a few exceptions,10 in clinical practice and research settings mBSR is mostly offered after the active anticancer treatment phase.11-13 As anticancer treatment poses a burden on patients mental and physical wellbeing2, 3 it can interfere with participation in psychosocial group interventions. When patients miss several sessions, the intervention might not be as effective. Consequently, although one third of women experience psychological distress during active anticancer treatment, they often need to wait before they can partici-pate in mBSR. Interestingly, a recent meta-analysis on uptake and adherence of psy-chological interventions for cancer patients demonstrated that patients were more likely to accept an intervention close to their diagnosis.14 Patients who were offered a psychological intervention during active anticancer treatment were not, however, more likely to drop out than those who received a support offer before treatment. Little is known about what patients themselves experience as the most suitable time to participate in psychosocial interventions such as mBSR. The aim of this study is to explore how patients experience the possible benefits and impediments of participation in mBSR during different stages of their anticancer treatment. This could be of help to practitioners and researchers in their choices about what is a suitable time to enroll patients in mBSR.
materials and methods
setting and study populationPatients with breast cancer were recruited at the departments of oncology of the Radboud University Medical Centre in Nijmegen, hospital Rijnstate in Arnhem

120
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
and through the website of a funding agency for breast cancer patients (www.pinkribbon.nl) from September 2012 to March 2014. Patients were included when they had been diagnosed with breast cancer, were at least 18 years old, and able to understand and use the Dutch language. No further eligibility criteria or sampling techniques were used. All participants provided written informed consent. The local ethics committee indicated that as this was an uncontrolled cohort study of an intervention already used in clinical care no formal approval was required (registration number cmO 2012/493).
procedureAfter referral, patients were invited for a research interview at the Radboudumc Centre for Mindfulness. They filled out self-report questionnaires on psychoso-cial functioning before and after mBSR. Some patients participated in mBSR for breast cancer patients only and they were invited for a focus group interview with their fellow participants one week after completion of the training. Some patients participated with their partner in mBSR for patients with various types of cancer. They were invited for an individual interview after completing the course.
interventionmBSR consists of 8-weekly group-based 2.5-hour sessions, a 6-hour silent day between sessions 6 and 7, and daily 45-minute home practice. The curriculum was based on the treatment format developed by Kabat-Zinn.7 The sessions consisted of mindfulness practices, didactic teaching on stress, and sharing experiences with one another. Participants received a CD with guided meditations and a workbook with written information. To tailor the intervention to cancer patients, psycho-ed-ucation about grief was added.15 Furthermore, patients could invite their partner or close other to attend a session on mindful communication, discussing the impact of cancer on their relationship. The training was conducted by a qualified health professional and mindfulness teacher who fulfilled the mindfulness-based intervention teacher assessment criteria.16
Quantitative assessMent Psychological distress. We used the total scale of the 14-item Hospital Anxiety and Depression Scale (HADS), which was developed to measure psychological distress in somatic patient populations. It consists of an anxiety and depression subscale.17
Rumination. The Ruminative Response Scale (RRS) was used to measure rumina-tion and distinguishes a more adaptive thinking style (reflection) from a more maladaptive one (brooding).18 We used the 5-item brooding subscale.
Quality of life. The European Organization for Research and Treatment of Cancer

121
(EORTc) Core Quality of Life Questionnaire (QLQ-C30) was used to assess quality of life.19 It contains several functioning and symptom subscales. We used the Global Quality of Life, emotional and physical functioning subscales.
Well-being. The 14-item Warwick-Edinburgh Mental Well-being Scale (WEmWBS) measures wellbeing.20 It contains the majority of the range of concepts associat-ed with positive mental health: hedonic and eudemonic aspects, positive affect, satisfying interpersonal relationships and positive functioning.
Mindfulness. The 24-item Short Form of the Five Facet Mindfulness Questionnaire (FFmQ-SF)21 is a valid and reliable alternative to the original FFmQ.22 The FFmQ-SF can be divided into five facets: observing, describing, acting with awareness, non-judging of inner experiences, non-reactivity to inner experiences. We used the total score.
Self-compassion. The 12-item Short Form of the Self-compassion Scale (ScS-SF)23 is a reliable and valid alternative to the original ScS.24 The ScS-SF can be divided into six subscales: self-kindness versus self-judgment, common humanity versus isolation and mindfulness versus over-identification. We used the total score.
Qualitative assessMents: focus groups and interviewsTo explore how patients experience participating in mBSR at different stages of their disease, focus groups and semi-structured individual interviews were used. The mBSR groups existed of a mixed group of breast cancer patients who partic-ipated both during and after anticancer treatment. Patients participated in mBSR for breast cancer patients only and they were invited for a focus group interview with their fellow participants one week after completion of the training. Participants were asked the following question: ‘You participated in the mBSR training while you are in a certain treatment stage for breast cancer. How was it to par-ticipate is this stage you are in?’ Focus groups took place at the Radboud Centre for Mindfulness one week after completion of mBSR, and lasted 100-120 minutes. Four focus groups were led by a psychiatrist and qualified mindfulness teacher (AS), and one focus group was conducted by a psychologist and qualified mindful-ness teacher (EJ). Both interviewers had not been involved in teaching the mBSR training. The individual interviews were also conducted by EJ, by telephone or face-to-face, and lasted 30-60 minutes. Focus groups and individual interviews started by explaining confidentiality and the explorative nature of the interview. Questions were asked in an open non-directive manner, allowing participants to speak freely about their experiences. For previous analyses on this qualitative data regarding the experience of peer support, see Schellekens et al.25
chapter 6

122
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Quantitative data analysis Repeated Measures ANOVAs were used to examine differences between baseline and post-treatment scores. To examine whether the timing of the intervention (during or after anti-cancer treatment) is a moderator of the intervention, we added Timing as a between subjects factor and examined the corresponding interaction. In addition, we controlled the analysis for covariates (i.e. age, marital status, education, employment).
Qualitative data analysisThe focus group and individual interviews were audio-taped and transcribed verbatim. A summary was returned to the participants for a member-check. Data analysis started after the first focus group had been transcribed, and continued with each additional focus group. Two researchers (EJ and mS, behavioral scientist and mindfulness teacher in training) coded the transcripts independently. After three focus groups the codes were compared by three researchers (mS, EJ and AS) until consensus was reached. This led to the identification of several themes. After five focus groups and three semi-structured individual interviews saturation was reached. Four researchers mS, EJ, AS and EB (psychiatrist and qualified mindfulness teacher) eventually grouped the subthemes into themes, in order to derive hypoth-eses from the data. After data analysis, relevant quotes were translated into English.
results
study saMpleIn total, 90 patients were recruited of whom 1 was excluded because she suffered from ovarian cancer. Of the 89 eligible patients, 64 (71%) participated (see Figure 1 for study flow). As can be seen, the main reasons for declining participation were distance to the centre, scheduling conflicts and participation in other psycholog-ical interventions. The demographic and clinical characteristics of the 64 patients who started with mBSR are shown in Table 1. Of those who started, 10 (16%) dropped out during the intervention. Patients who dropped out did not differ from those who completed the mBSR program. Main reasons for dropout were fear of fellow patients and physical impairments (see Figure 1).
effects of MbsrAfter mBSR, participants reported significantly less psychological distress (p=.0.03, d=0.44). In addition, significant improvements were found in mindfulness skills (p=0.01, d=0.48) self-compassion (p= 0.00, d=0.6), wellbeing (p= 0.03, d=0.31) and physical (p= 0.06, d=0.40) and emotional quality of life ( p=0.01, d=0.38). See Table 2.

123
No significant improvement was found in rumination or global quality of life (all p-values >.05). Timing of treatment did not moderate the outcomes, except for mindfulness. Those patients participating after anti-cancer treatment reported a larger increase in mindfulness skills than those participating during anti-cancer treatment, possibly because those participating after anti-cancer treatment reported a lower baseline score of mindfulness skills. When adding Timing of intervention to the analysis, the effects on emotional functioning (p=0.11) and wellbeing (p=0.18) were no longer significant. Controlling for baseline variables: age, marital status, education and employment did not change the results.
Qualitative resultsThirty-seven patients who participated in mBSR solely for breast cancer patients participated in the focus groups. Each focus group varied from 7-13 participants. Overall, 12 women participated during treatment and 25 participated after treat-ment. They were randomly divided over the focus groups. One palliative patient was interviewed individually, because she was not able to join the group. Two patients who participated with their partner in the group for mixed cancer patients were also interviewed individually. Both participated in mBSR during their anti-cancer treatment. The analysis of the 5 focus groups and 3 individual interviews resulted in three main themes: mBSR during cancer treatment, mBSR after cancer treatment, and Participation in relation to emotional processing. These themes could be subdivided into 7 subthemes (see Table 3). Patients experienced several advantages and disad-vantages when participating in mBSR during and after medical treatment. Besides the treatment stage, emotional processing also seemed an important indicator of the most suitable time to enroll.
theMe 1 . participation during anticancer treatMentMBSR supports coping with anticancer treatment. Many patients benefited from mBSR during treatment, which mainly consisted of chemotherapy but also long-term hormone treatment. They noted that what they learned during mBSR was imme-diately applicable to coping with their anticancer treatment. For instance, the training program in itself helped participants deal with their aversion to aspects of the somatic treatment.
‘You can apply it immediately, when you want to actively use it and if you need to learn to live in the moment especially, then it’s immediately useful. Then maybe your ideas about that therapy change.’
Physical challenges. Several patients, however, were physically challenged to par-ticipate during their somatic treatment due to their illness and side-effects of the
chapter 6

124
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
treatment. Participants mentioned that somatic symptoms or fatigue hindered attendance of the mBSR sessions and home practice. Others described how their somatic treatment schedule limited their time to participate.
‘Every three weeks I had chemo, so I was there on and off, I also missed two ses-sions because I really felt ill.’
At the same time, a few patients mentioned that they had plenty of time during somatic treatment and that they were able to handle it physically.
theMe 2. participation after anticancer treatMentPhysically stronger. The physical challenges experienced during treatment were not mentioned by participants who participated after treatment. In this phase participants experienced their physical recovery as being facilitating. Patients had gained energy, felt physically stronger and generally had a better physical condi-tion. In turn, patients felt they also gained energy from participating in the mBSR.
‘So some time needs to pass, and then you have a little bit of energy and then with the training, you get the rest of the energy’
Too late to benefit. Participants noted that several months after treatment they already experienced and coped with the fear and insecurities of diagnosis and treatment. They felt it was too late to fully benefit from the training and would have wanted to participate earlier. As one participant noted, she would have been able to move out of her survival mode much sooner. Others described they might have achieved more ‘clarity and peace’ if there had been an opportunity to follow the training earlier, especially regarding work reintegration issues.
‘I think in that stage I.. in that stage when I tried to get back to work and get on with daily life, it would have clarified things for myself and it would have brought me some rest’
theMe 3 . participation in relation to eMotional processing Coping with emotions. The participants noted that the timing of participation also depended on the willingness to emotionally engage with the mBSR, regardless of the treatment phase they were in. The need for psychological help depended on the degree of vulnerability patients allowed themselves to feel.
Are you okay with vulnerability or are you someone who says: no, I don’t want this. That’s what it depends on very much, I think’.

125
Early empowerment. Participants mentioned the value of being able to make their own decision about whether and when to take part. They preferred to be informed about mBSR as soon as possible in order to do so. It seemed to strengthen the sense of autonomy in patients.
‘You’re in the hospital regularly anyway, they could address it sooner.. Then you can decide for yourself, well it’s too early for me or oh, I would like that.’
Participation too early. A possible barrier of being informed about the mBSR train-ing at an early stage is that patients may participate too early to fully benefit from the program. Some patients mentioned they were not emotionally prepared to participate, they felt too vulnerable to become aware of their thoughts and feelings.
‘I wanted something quickly, but in hindsight I think it might have been better to start a little bit later. Seeing what the chemo did to me, particularly mentally.’
discussion
This mixed method study explored what patients experience as a suitable stage to participate in mBSR. Our quantitative findings confirmed previous studies in showing that in the whole group of breast cancer patients mBSR resulted in a reduction of psychological distress.8, 9 The quantitative data showed that par-ticipating during or after anticancer treatment interacts with changes in mind-fulness. Those participating after anticancer treatment seem to improve more, however, this could possibly be explained by lower baseline scores. The qualitative data revealed that although participating in mBSR during anticancer treatment helped patients to cope with the treatment, their physical symptoms could also hinder participation. After anticancer treatment their gain in energy facilitated participation in mBSR, but some patients mentioned they participated too late to fully benefit. Finally, in addition to the cancer treatment phase, right timing also seemed to depend on the stage of emotional processing. Women emphasized the importance of being informed about the possibility to take part in mBSR at an early stage as it enabled them to decide for themselves whether and when to enroll. These qualitative findings are in line with former studies showing that patients would like to be offered psychological interventions soon after diagnosis.26-28 A recent meta-analysis showed that the sooner after diagnosis psychological help was offered the higher the uptake.14
Nevertheless, a large part of cancer patients decline help, despite being distressed. Patients seem to belief that one’s level of distress is not severe enough to warrant psychosocial interventions and prefer to manage on their own, even in the subgroup
chapter 6

126
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
with high levels of distress.29 When psychosocial care becomes more integrated into regular cancer care, psychosocial interventions such as mBSR might become more acceptable and accessible for patients. However, as health care professionals focus on physical symptoms and treatment, emotional and psychological symp-toms are often overlooked. Health care professionals also report lack of time and lack of confidence as barriers to address psychological symptoms.30 Patients may be embarrassed or reluctant to mention their psychological problems to their physician.31 Offering psychosocial help soon after diagnosis and providing clear information about the different options, such as mBSR, to all patients might be a first step. It might contribute to the patients’ autonomy and self-management skills at a moment when they are deprived of these in many ways.
strengths and liMitationsBreast cancer patients with different disease and treatment stages were all wel-come to participate, enabling us to explore how women experienced the timing of participating in mBSR. Quantitative findings were presented with qualitative findings to provide an overview of the effects and experiences of mBSR participa-tion. As a relatively large sample of breast cancer patients participated in the focus groups we reached data saturation and reported on a broad view of experiences. We also performed member-checks, ensuring the interpretation of the data was valid. The study also has a number of limitations. The focus groups were mixed, in line with the mixed group of patients (both during and after anticancer treat-ment) participating in the intervention. For the aim of this study, we might have gained more specific information about timing of the intervention, by interviewing them separately. The quantitative results were uncontrolled, we did not carefully register all psychosocial treatments participants might have been using. Most of our patients were in a curative stage. In addition, the women who dropped out the intervention were not invited to the focus groups or individual interviews. Although these women provided reasons for dropping out (i.e. fear of fellow patients and physical impairments), unfortunately they did not provide information on how they experienced the time of enrollment and whether the stage of anticancer treatment might play a role in dropping out the intervention.
clinical iMplications and further researchSeveral factors should be taken into account when helping breast cancer patients interested in mBSR to time their participation. To stimulate patients’ self-manage-ment, information on mBSR should be provided in an early stage. This can help patients to decide for themselves when they are emotionally ready to participate. Health care professionals should be alert on those women who ‘rush into it’ as they might still be too vulnerable to become mindfully aware of their thoughts,

127
emotions and bodily sensations. Capability building strategies for health care professionals might support them addressing these issues with patients.32 Patients should also be informed about how physical symptoms can hinder participation, especially during anticancer treatment. Depending on women’s’ physical symptoms, participation in mBSR can be experienced as beneficial both during and after anti-cancer treatment. Future research could examine whether participation during and after anticancer treat-ment is equally feasible and effective for women with breast cancer. Additionally, it would be interesting to study whether these results extend to cancer patients with a higher symptom burden (e.g. lung cancer). Alternatively, future studies could further explore whether tailored version of the mBSR program, such as online or blended versions, might make mBSR more accessible for patients currently undergoing anticancer treatment.33
chapter 6

128
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Figure 1 Study flow of patients.
Assessed for eligibility (n = 90)
Excluded (n = 1) Ovarium cancer (n = 1)
Eligible (n = 89)
Completed Mbsr (n = 54)Dropout intervention (n = 10) Fear of fellow patients (n = 5) Physical impairment (n = 3) Other expectations (n = 1) Scheduling conflict (n = 1)
Participation (n = 64)
Baseline assesment (n = 64)
Post assessment (n = 52)Failed to complete (n = 2)
Declined participation (n = 25) Travel distance (n = 5) Scheduling conflict (n = 6) Other psychol intervention (n = 6) Not interested (n = 3) Fear of fellow patients (n = 1) Other (n = 3)

Treatment phase Total(n=64)
During(n=19)
After(n=45)
n (%) n (%) n (%)
Age, M (sd) 52.3 (8.0) 53.8 (7.5) 51.7 (8.3)
Marital Status
Married, living together
50 (78.1) 15 (78.9) 35 (79.5)
Divorced 13 (20.3) 4 (21.1) 9 (20.5)
Educational level A
Low 1 (1.6) 0 (0) 1 (2.2)
Intermediate 25 (39.1) 7 (36.8) 18 (40.0)
High 38 (59.4) 12 (63.2) 26 (57.8)
Employment
Paid job 35 (54.7) 11 (57.9) 24 (53.3)
Unpaid job 7 (10.9) 2 (10.5) 5 (11.1)
Disabled 20 (31.3) 5 (26.3) 15 (33.3)
Retired 2 (3.1) 1 (5.3) 1 (2.2)
Stage of disease
Curative 58 (90.6) 16 (84.2) 42 (93.3)
Palliative 6 (9.4) 3 (15.8) 3 (6.7)
Time since diagnosis
< 6 months 13 (20.3) 12 (63.2) 1 (2.3)
6 - 12 months 18 (28.1) 5 (26.3) 13 (29.5)
> 1 year 32 (50.0) 2 (10.5) 30 (68.2)
Table 1 Demographic and clinical characteristics of 64 patients who participated.
A Low educational level = primary and lower secondary education; intermediate = upper secondary education; high = higher vocational training and university.

Table 2 Baseline and post- assessment scores of 52 patients who completed participation.
Total Main effect of Treatment
Duringtreatment
Aftertreatment
Main effect of Treatment
Interaction effect of Treatment X Timing
Baseline M (sd)
PostM (sd) p-value A
Baseline M (sd)
Post M (sd)
Baseline M (sd)
Post M(sd) p-value B
Psychological distress (hads) 12.6 (6.2) 10.2 (6.2) .003 12.9 (6.2) 11.3 (6.4) 12.4(6.2) 9.7(6.1) .013 . 512
Rumination (rrs-br) 9.0 (2.6) 8.4(2.4) .071 8.3(2.3) 8.1(1.4) 9.3(2.6) 8.5(2.7) .219 .382
Quality of life (QlQ-c30)
Global quality of life 66.7 (12.8) 70.5 (17.8) .085 62.3(12.9) 60.6(22.7) 68.5(12.5) 74.5(13.8) .362 .104
Physical functioning 84.5(12.1) 88.0 (11.0) .031 86.2(7.7) 88.1(9.0) 83.8(13.6) 87.9(11.8) .031 .406
Emotional functioning 69.6(17.3) 75.9 (15.7) .014 71.1(16.0) 71.1(16.6) 68.9(18.0) 77.9(15.1) .105 .105
Mindfulness skills (ffMQ) 80.9(11.1) 85.5 (10.5) .010 86.7(9.9) 86.9(9.8) 78.6(10.8) 84.9(10.8) .025 .032
Self-compassion (scs-sf) 3.2 (0.7) 3.6 (0.7) .000 3.5(0.57) 3.8(0.48) 3.1(0.71) 3.5(0.73) <.001 .673
Wellbeing (webwbs) 51.9 (7.0) 54.0 (7.2) .028 54.3(7.1) 54.0(8.6) 50.9(6.8) 54.0(6.6) .176 .095
A Repeated measures anova using Treatment (pre- and post-intervention measurements) as within- subjects factor; significance p< .05.B Repeated measures anova using Treatment as within subjects factor and Timing (during or after cancer treatment) as between-subjects factor; significance p< .05.
Themes Subthemes
Participation during anticancer treatment Mbsr supports coping with anticancer treatment
Physical challenges
Participation after anticancer treatment Physically stronger
Too late to benefit
Participation in relation to emotional processing Coping with emotions.
Early empowerment
Participation too early
Table 3 Themes and subthemes of what patients experience as a suitable stage to participate.

Total Main effect of Treatment
Duringtreatment
Aftertreatment
Main effect of Treatment
Interaction effect of Treatment X Timing
Baseline M (sd)
PostM (sd) p-value A
Baseline M (sd)
Post M (sd)
Baseline M (sd)
Post M(sd) p-value B
Psychological distress (hads) 12.6 (6.2) 10.2 (6.2) .003 12.9 (6.2) 11.3 (6.4) 12.4(6.2) 9.7(6.1) .013 . 512
Rumination (rrs-br) 9.0 (2.6) 8.4(2.4) .071 8.3(2.3) 8.1(1.4) 9.3(2.6) 8.5(2.7) .219 .382
Quality of life (QlQ-c30)
Global quality of life 66.7 (12.8) 70.5 (17.8) .085 62.3(12.9) 60.6(22.7) 68.5(12.5) 74.5(13.8) .362 .104
Physical functioning 84.5(12.1) 88.0 (11.0) .031 86.2(7.7) 88.1(9.0) 83.8(13.6) 87.9(11.8) .031 .406
Emotional functioning 69.6(17.3) 75.9 (15.7) .014 71.1(16.0) 71.1(16.6) 68.9(18.0) 77.9(15.1) .105 .105
Mindfulness skills (ffMQ) 80.9(11.1) 85.5 (10.5) .010 86.7(9.9) 86.9(9.8) 78.6(10.8) 84.9(10.8) .025 .032
Self-compassion (scs-sf) 3.2 (0.7) 3.6 (0.7) .000 3.5(0.57) 3.8(0.48) 3.1(0.71) 3.5(0.73) <.001 .673
Wellbeing (webwbs) 51.9 (7.0) 54.0 (7.2) .028 54.3(7.1) 54.0(8.6) 50.9(6.8) 54.0(6.6) .176 .095

132
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
References
1. Ferlay, J., et al., Cancer incidence and mortality worldwide: sources, methods and major patterns in GLObOcAN 2012. Inter-national Journal Cancer, 2015. 136(5): p. E359-86.
2. Henselmans, I., et al., Identification and prediction of distress trajectories in the first year after a breast cancer diagnosis. Health Psychology, 2010. 29(2): p. 160.
3. Mitchell A., Ferguson., D., Gill, J., Paul, J., Symonds, P. , Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: a systematic review and meta-analysis. Lancet Oncolo-gy, 2013. 14(8):721-32.
4. Meyer, T.J. and M.M. Mark, Effects of psychosocial interventions with adult cancer patients: a meta-analysis of randomized experiments. Health Psychol, 1995. 14(2): p. 101-8.
5. Osborn RL, Demoncada AC, and F. M, Psychosocial interventions for depres-sion, anxiety, and quality of life in cancer survivors: meta-analyses. International Journal of Psychiatry in Medicine 2006. 36(1):13-34.
6. Goedendorp, M.M., et al., Psychosocial interventions for reducing fatigue during cancer treatment in adults. Cochrane Database of Systematic Reviews, 2009 21(1):CD006953.
7. Kabat-Zinn, J., Full catastrophe living: Using the wisdom of your body and mind in everyday life. New York: Delacorte, 1990.
8. Cramer H., et al., Mindfulness based stress reduction for breast cancer – a systematic review and meta-analysis. Current Oncology 2012. 19(5):e343-52
9. Piet J, Wurtzen H, and Zacharea. R, The effect of mindfulness based therapy on symptoms of anxiety and depression in adult cancer patients and survivors: a systematic review and meta-analysis. J Consulting Clinical Psychology 2012. 80(6):1007-1020.
10. Henderson, V.P., et al., The effects of mindfulness-based stress reduction on
psychosocial outcomes and quality of life in early-stage breast cancer patients: a ran-domized trial. Breast cancer research and treatment, 2012. 131(1): p. 99-109.
11. Lengacher, C.A., et al., Randomized controlled trial of mindfulness-based stress reduction (mbSR) for survivors of breast cancer. Psycho-oncology, 2009. 18(12): p. 1261-1272.
12. Hoffman, C.J., et al., Effectiveness of mindfulness-based stress reduction in mood, breast- and endocrine-related quality of life, and well-being in stage 0 to III breast can-cer: a randomized, controlled trial. J Clini-cal Oncology, 2012. 30(12): p. 1335-1342.
13. Carlson, L.E., et al., Randomized Con-trolled Trial of Mindfulness-Based Cancer Recovery Versus Supportive Expressive Group Therapy for Distressed Survivors of Breast Cancer (mINDSET). Journal of Clinical Oncology, 2013. 31(25):3119-26.
14. Brebach R., et al., Psychological interven-tion targeting distress for cancer patients: a meta-analytic study investigating uptake and adherence. Psycho-Oncology 2016. 25(8):882-90.
15. Schellekens M.P., et al., Study protocol of a randomized controlled trial comparing Mindfulness-Based Stress Reduction with treatment as usual in reducing psycholog-ical distress in patients with lung cancer and their partners: the mILON study. Bmc Cancer, 2014.14:3.
16. Crane R.S., et al., Competence in teach-ing mindfulness-based courses: concepts, development and assessment. Mindfulness 2012 3(1):76-84.
17. Spinhoven, P., et al., A validation study of the Hospital Anziety and Depression Scale (HADS) in different groups of Dutch subject. Psychological Medicine, 1997 27(2):363-70.
18. Raes F., et.al., Reflection en brooding als subtypes van het rumineren: een herziening van de Ruminative Response Scale. Ge-dragstherapie, 2009. 42:205-214.
19. Bjordal K., et al., A 12 country field study of the EORTc QLQ-C30 (version 3.0) and the head and neck cancer specific module

133
(EORTc QLQ-H&N35) in head and neck patients. EORTc Quality of Life Group. European Journal Cancer 2000 36 (14):1796-1807.
20. Stewart-Brown S., et.al., Internal construct validity of the Warwick-Edinburgh Mental Well-being Scale (WEmWbS): a Rasch analysis using data from the Scottish health Education Population Survey. Health and Quality of Life Outcomes 2009 7:15.
21. Baer R.A., Smith.G.T., Lykins E. , Con-struct Validity of the Five Facet Mindfulness Questionnaire in Meditating and Non-meditating Samples. Assessment, 2008. 15(3):329-42
22. Bohlmeijer E.T., ten Klooster P., Fled-derus M, Veehof M.M, Baer R., Psycho-metric properties of the Five Facet Mindful-ness Questionnaire in depressed adults and development of a short form. Assessment 2011. 18(3):308-20.
23. Raes, F., et al., Construction and factorial validation of a short form of the Self-Com-passion Scale. Clinical Psychology & Psychotherapy, 2011 18(3):250-5.
24. Neff C., The Development and Validation of a Scale to Measure Self-Compassion. Self and Identity 2003 2(3); 223-50.
25. Schellekens MP, et al., A qualitative study on mindfulness-based stress reduction for breast cancer patients: how women experi-ence participating with fellow patients. Sup-portive Care Cancer, 2016 24(4):1813-20.
26. Shapiro PJ, Coyne JC, and Kruus. LK, Interest in services among prostate cancer pa-tients receiving androgen deprivation therapy. Psycho-Oncology, 2004. 13 (8): 512-525.
27. Allen SM, Shah AC, and Nezu AM, A problemsolving approach to stress reduction among younger women with breast carcino-ma: a randomized controlled trial. Cancer, 2002 94(12):3089-100.
28. Arving C, Sjoden PO, and Bergh J, Satisfaction, utilisation and perceived benefit of individual psychosocial support for breast cancer patients-A randomised study of nurse versus psychologist interventions. Patient Education and Counseling, 2006 62(2):235-43.
29. Clover K.A., et al., Why do oncology outpa-tients who report emotional distress decline help? Psycho-Oncology 2014 24(7):812-8.
30. Maguire P., Improving communication with cancer patients. European Journal of Cancer, 1999 35(10): 1415-22.
31. Valente, S.M., Saunders J.M., Cohen M.Z, Evaluating depression among patients with cancer. Cancer Practices, 1994. 2(1): p. 65-71.
32. Dilworth S., Higgins I., Parker V., Kelly B., Turner J. , Patient and health profes-sional’s perceived barriers to the delivery of psychosocial care to adults with cancer: a systematic review. Psycho-Oncology 2014. 23(6):601-12.
33. Compen F. R , Bisseling E.M., Van der Lee M. L., Adang E. M. M., Donders A. R. T, Speckens A. E. M. , Study protocol of a multicenter randomized controlled trial comparing the effectiveness of group and in-dividual internet-based Mindfulness-Based Cognitive Therapy with treatment as usual in reducing psychological distress in cancer patients: the BeMind study. Bmc Psychol-ogy 2015. 3:27.
chapter 6


Chapter 7
Summary and General Discussion

136
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
summary and general discussion
The present thesis focused on examining the effectiveness of an internet-based mBcT (emBcT) and a group-based Mindfulness-Based Cognitive therapy (mBcT) in reducing psychological distress in cancer patients. In this chapter the results from the previous chapters are summarized and discussed in relation to existing literature. Methodological considerations are discussed, as well as implications and suggestions for further research and clinical practice.

137
chapter 7
summary
The worldwide prevalence of people living with cancer is rising. As anticancer treat-ment options improve rapidly, the amount of patients surviving cancer increases. Experiencing psychological distress is part of cancer survivorship. Specific worry about cancer recurrence is one of the most common concerns and unmet needs of cancer patients and survivors. In addition, anxiety and depressive disorders are more prevalent in cancer patients than in the general population. This calls for effective, widely available and accessible psychological treatment options. Mindfulness-based interventions (mBIs) are innovative and effective evidence-based interventions in somatic and mental health care. mBIs, both Mindfulness-Based Stress Reduction (mBSR)1 and Mindfulness-based Cognitive Therapy (mBcT)2 have proven to be effective in reducing psychological distress in cancer patients. However, as they typically require in-person attendance at classes over several weeks, many cancer patients experience barriers to participation. Internet-based Mindfulness-based Cognitive Therapy (emBcT) seems to be an effective alternative treatment option. To increase their effectiveness, it is of great importance to gain knowledge about factors influencing outcome of mBIs, in both face to face (f2f ) and online applica-tions. By investigating the relationship between treatment outcome and therapist competence, therapeutic alliance and (group) cohesion in both emBcT and mBcT, and other factors such as timing of the intervention, we can further improve avail-able formats of mBIs for cancer patients. Gaining insight into what factors affect treatment outcome can facilitate the implementation of mBIs in clinical practice.
Are mbcT and embcT more effective compared to TAU in reducing psychological distress in cancer patients?
In our multicenter RcT (Chapter 3), the BeMind study, we investigated the effective-ness of both internet and group- based mBcT in reducing psychological distress in cancer patients. We included 245 cancer patients with psychological distress (≥ 11 on the Hospital Anxiety and Depression Scale (HADS)). They were randomly allocated to mBcT (n=77), emBcT (n=90) or TAu (n=78). Patients completed baseline (T0) and post-intervention (T1) assessments. The primary outcome was psycho-logical distress on the HADS. Secondary outcomes were psychiatric diagnosis, fear of cancer recurrence, rumination, health-related quality of life, mindfulness skills and positive mental health. Continuous outcomes were analyzed using Linear Mixed Modeling on the intention-to-treat sample. Results showed that patients in both mBcT and emBcT conditions reported a clinically relevant reduction of psychological distress than those in the TAu condition. In addition, post-treatment prevalence of psychiatric diagnosis appeared lower in both mBcT and emBcT than

138
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
in TAu, but these changes were not statistically significant. Both interventions significantly reduced fear of cancer recurrence and rumination and improved mental health-related quality of life, mindfulness skills and positive mental health compared to TAu. Physical health-related quality of life did not improve.
Are group cohesion, therapeutic alliance and therapist competence associated with outcome of mbcT for distressed cancer patients?
As (e)mBcT seemed to be effective interventions for distressed cancer patients, we investigated whether therapist competence, therapeutic alliance and group cohe-sion are associated with treatment outcome in terms of reduction of psychological distress (Chapter 4). It was hypothesized that therapist competence, therapeutic alliance and group cohesion would predict treatment outcome, and that therapist competence was a prerequisite for developing both therapeutic alliance and group cohesion. Data of 120 patients who were allocated to the f2f group format of mBcT after the initial randomization (n=77) or after the completing the TAu condition (n=43) were used. The analyses only included completers of the course, i.e. patients who attended four or more sessions (n=84). The findings revealed that therapeutic alliance significantly contributed to reduction of psychological distress in mBcT for cancer patients, but group cohesion did not. Therapist competence did not predict post-treatment psychological distress and did not appear to be a precondition for a strong therapeutic alliance and group cohesion. Contrary to our expectations, therapist competence did appear to be associated with lower group cohesion.
Can therapeutic alliance develop in embcT as well as in mbcT and is early alli-ance associated with outcome of (e)mbcT?
Chapter 5 showed the results of an explorative study examining the level of ther-apeutic alliance in emBcT compared to mBcT. The objectives of the study were to explore whether early therapeutic alliance predicts treatment dropout in (e)mBcT; to compare the development of the therapeutic alliance during emBcT and mBcT; and to examine whether early therapeutic alliance is a predictor of the reduction of psychological distress and the increase of mental well-being at post-treatment in both conditions. The study was part of our multicenter randomized controlled trial (RcT; n=245) on the effectiveness of (e)mBcT for distressed cancer patients. The therapeutic alliance was measured at the start of week 2 (i.e. early therapeu-tic alliance), week 5 and week 9. Outcome measures were psychological distress, and mental-wellbeing. The strength of early therapeutic alliance did not predict treatment dropout in (e)mBcT. For further analyses we only included patients who completed the intervention, i.e. attended four or more sessions (n=163). Therapeu-

139
tic alliance increased over time in both conditions. This increase did not differ between emBcT and mBcT. Early therapeutic alliance predicted a significant reduction of psychological distress and a significant increase of in mental well-be-ing at post-treatment. The relationship with reduction of psychological distress differed between treatments: a weaker early therapeutic alliance predicted higher psychological distress at post-treatment in mBcT but not in emBcT.
How do breast cancer patients experience the timing of participating in an mbSR-training? What are specific benefits or barriers?
In clinical practice and research settings mBIs are mostly offered after the active anticancer treatment stage. We were interested in what patients themselves expe-rience as the most suitable time to participate in mBSR. For the mixed method study (Chapter 6), patients with breast cancer were recruited at the departments of oncology of the Radboud University Medical Centre in Nijmegen, hospital Rijnstate in Arnhem and through the website of a funding agency for breast cancer patients (www.pinkribbon.nl). To explore how patients experience participating in mBSR at different stages of their disease, focus groups and semi-structured individual interviews were used. Of the 89 eligible patients, 64 (71%) participated in the study and started mBSR. Thirty-seven patients participated in the focus groups. Focus group varied from 7-13 participants. Overall, 12 women participated during treatment and 25 participated after treatment. Three patients were interviewed individually. The qualitative data revealed that although participating in mBSR during anticancer treatment helped patients cope with the treatment, their physical symptoms could also hinder participation. After anticancer treatment their gain in energy facilitated participation in mBSR, but some patients mentioned they participated too late to fully benefit. In addition to the cancer treatment phase, right timing also seemed to depend on the stage of emotional processing. Women emphasized the importance of being informed about the possibility to take part in mBSR at an early stage as it would enable them to decide for themselves whether and when to enroll.
general discussion
The main study of the BeMind research project presented in this thesis (Chapter 2 and 3) was the first study comparing the effectiveness of both emBcT and mBcT to TAu in distressed cancer patients. The additional quantitative studies includ-ed in this thesis focused mainly on aspects of the therapeutic relationship of both applications (Chapter 4 and 5 ). The qualitative study included in this thesis (Chapter 6) gathered personal experiences to explore the feasibility and optimal
chapter 7

140
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
timing of intervention delivery. These studies contribute to the ongoing debate in psychotherapy research on the relative importance of aspects of the therapeu-tic relationship such as therapist competence, therapeutic alliance and group cohesion, and treatment delivery, such as timing, and their respective impact on treatment outcome.
methodological considerations
designA major strength of the thesis was the design of the main trial (Chapter 2 and 3), a three-armed multicenter, parallel group RcT to compare the effectiveness of emBcT and mBcT versus TAu in reducing psychological distress in cancer patients. It was the first study which simultaneously compared emBcT and mBcT with TAu in a large sample of heterogeneous cancer patients with psychological distress. Both interventions were protocolized and were delivered by qualified therapists in different areas in the Netherlands, which was important in terms of its generalizability. Although the group-based setting is considered important for mBIs3 the studies in this thesis suggest that individual guided emBcT with weekly online therapist feedback is also effective. However, our study was not powered to directly compare or determine non-inferiority of emBcT to mBcT, as this would have required a larger sample size. Interestingly, our follow-up study (not in this thesis) showed that the effects of both emBcT and mBcT appeared to further improve over the follow-up period, during which emBcT seemed to outperform mBcT.4 The results of the RcT inspired further research on treatment delivery factors and integrity, in both online applications and f2f formats, as these might increase the effectiveness of (e)mBcT for cancer patients.
study population As a previous study in cancer patients indicated important difficulties associated with consecutive sampling of distressed patients in hospital outpatient settings,5 our study recruited patients through self-referral. Patients were broadly recruit-ed, via healthcare professionals in affiliated centers, via online and offline media, patient associations and peers. We are aware that in RcTs consecutive sampling is generally considered first choice as it reduces sampling bias.6 However, in cancer patients, the presence of psychological distress does not necessarily mean that they also are interested in help.7-9 So, the implicit assumption within consecutive sampling that all patients can benefit from an intervention might not be valid for psycho-oncology interventions.10 A large part of cancer patients decline help despite being distressed. Patients feel embarrassed and prefer to manage on their own, even amongst patients with high levels of distress.8 This is also reflected by the

141
fact that only 14% of distressed patients are willing to talk with their professional about their distress post-treatment11 and less than 30% of distressed patients are recognized by oncology health professionals.12, 13 So, on the one hand not all patients who are invited for a psycho-oncological intervention by consecutive sampling might be interested. On the other hand, not all patients who are interested will be found by consecutive sampling at an oncology clinic.
The advantage of such a patient-centered recruitment procedure is that it resulted in a sample of patients who are both distressed and interested in psychological help. However, the majority of the patients in our sample were middle-aged breast cancer patients. Although this is in line with the characteristics of other cancer patients seeking psychosocial support14 this might be a limitation in terms of the generalizability of our results.
assessMent of treatMent outcoMe Another strength of the trial is that we used a broad array of outcome measures, including both observer-rated interviews and self-report questionnaires. Our pri-mary outcome, psychological distress, was measured with a self-report question-naire, the Hospital Anxiety and Depression scale (HADS). Even though the HADS was originally developed as a screening instrument in hospital settings, previous research has shown that its total score is sensitive enough to identify overall symptom change.15, 16 However, a statistically significant change is not identical to a clinically reliable change. To measure whether the statistical change we found is of clinical relevance, we calculated the Reliable Change Index (RcI).17 We found that the proportion of patients demonstrating clinically reliable improvement was significantly greater in (e)mBcT (36% in mBcT and 37% in emBcT) than TAu (14%). In addition, we assessed psychiatric diagnosis by the Structured-Clinical-Interview for DSm-IV-TR Axis-I disorders (ScID-I18). Improvement in rates of psychiatric diagnosis favoured both interventions compared to TAu (32% in mBcT and 29% in emBcT vs 16% in TAu). These effect sizes are in line with other available psy-chological interventions in cancer patients.19 Our conclusion that (e)mBcT is an effective and viable psychological treatment option in oncology is also supported by the results of two recent meta-analyses on efficacy of mBIs for psychological and physical health outcomes in cancer patients.20, 21
substantive considerations
therapist coMpetenceWhile therapist competence is considered to be important in the clinical practice of teaching cognitive behavioral approaches,22, 23 recent research in both cBT and
chapter 7

142
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
mBcT found little support for an association between competence and patient outcome.24, 25 Our study was the first study examining therapist competence as a predictor of outcome in mBcT in the population of cancer patients. Our findings revealed that therapist competence was not related to outcome in mBcT for cancer patients, which was in line with a previous study conducted on competence as predictor of outcome in mBcT in patients with recurrent depression.25 An expla-nation could be that all therapists operated at least at a basic skill level as they all fulfilled the advanced criteria of the Association of Mindfulness Based Teachers in the Netherlands and Flanders. Although there was a range of competence levels, none of the therapists were rated as incompetent or advanced on the Mindful-ness-based Interventions Teaching Assessment Criteria (mBI:TAc). A second explanation for the lack of association between competence and treat-ment outcome concerns the instrument that we used in our study, the mBI:TAc. Although it was originally developed for teaching purposes, the mBI:TAc has regularly been used to measure therapist competence in treatment studies.26 The mBI:TAc is the most widely used tool developed to assess mindfulness-based teaching integrity and competence. Treatment integrity refers to the degree to which an intervention is implemented as intended and can be subdivided in two dimensions: adherence and differentiation.27, 28 The dimensions adherence and differentiation tell us something about delivering the treatment with integrity. Adherence refers to the extent to which the therapist both applies the appropriate content while also refraining from introducing elements that are not recognized as part of the approach. Differentiation refers to the degree to which the approach can be distin-guished from other approaches. The dimension competence refers to the teachers’ skills in delivering the intervention.22 An intervention delivered with integrity does not necessarily mean that the intervention has been delivered competently.26
One of the problems of examining therapist competence as a predictor of outcome in mBcT, is that it is not easy to measure competence adequately. First of all, the overall inter-rater reliability (IRR), was lower in our study (0.7) than it was in the validation study of the mBI:TAc.22 However, the validation study had a relative small sample size of both assessors and teachers, was conducted within routine practice, with assessors and teachers knowing each other and involved in the development of the scale and therefore sensitive to bias.29 Secondly, the mBI:TAc was developed in the UK context, and thus sensitive for the cultural expressions of teaching mindfulness practices within the uK and not necessarily those of other countries. During teaching workshops on applying the mBI-TAc we had the impression, for example, that Dutch assessors had a tendency to be stricter and more critical than their uK counterparts. So, the mBI:TAc might need adaptations to increase its sensitivity to other cultural expressions of teaching practice.30 In

143
addition, there are some practical matters to consider. The mBI:TAc should be used by intensively trained assessors, who are also experienced in teaching mindfulness. This makes the application of the scale in research setting quite complex, time consuming and costly. And even for experienced observer assessors, a selected subset of recorded sessions do not always provide an entire picture of the therapist competence and skills. The developer of the scale, R. Crane22, 31 speaks in this light about the ‘hidden curriculum’ for each therapist: the personal development, the internalising and integration of the learning in the therapist’s live and teachings, which might be less visible or less reflected in the assessed observations of the therapist. To get a broader picture of therapist competence, it might be helpful to combine different perspectives, such as the therapist’s own reflections and patients’ perspectives with assessor observations.30 Further research should also focus on adapting competence assessment measures to other delivery formats, such as online applications. In this eHealth era more attention should be paid to how to measure therapist competence in online mBIs. For this purpose, it might be very helpful to use linguistic analysis of written feedback and online chats between therapist and patients.
Finally, it might be that, although therapist competence is considered to be import-ant in clinical practice and an assumed prerequisite for treatment efficacy, the perceived therapeutic alliance by patients is more relevant for treatment outcome than the observed therapist competence.
therapeutic alliance Therapeutic alliance is defined as the collaborative and affective bond between therapist and patient.32, 33 In therapy both therapist and patients bring their expec-tations. While therapist expectations are mainly based on the treatment method they apply patients expectations are mainly based on their own personal goals.34 A good alliance means that patient and therapist are working well towards the goals of the therapy.34 The therapeutic alliance is often measured with the Working Alliance Inventory (WAI35), including three subscales: 1) how closely client and therapist agree on goals of treatment; 2) how closely client and therapist agree on how to reach the treatment goals: and 3) the degree of mutual trust between client and therapist. The therapeutic alliance has shown to be a predictor of outcome in f2f psycho-therapy in multiple studies over many years, regardless treatment orientation.36, 37 Although the WAI was originally developed for f2f interventions, it also seems to perform well in measuring therapeutic alliance in internet-based interventions.38
In cBT approaches the collaborative relationship between therapist and patient is used extensively, mainly to adhere to specific cBT techniques and to reach treatment
chapter 7

144
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
goals. The alliance is mostly seen as facilitating the techniques not as treatment factor, while in other psychotherapeutic orientations, alliance is often seen as a mechanism of change in itself. In mBcT the role of the therapist is slightly dif-ferent compared to traditional cBT. In mBcT the therapist is mainly focused on facilitating patients’ self-efficacy, and less on actively exploring personal narratives. The therapist is the steward of the group, delivering didactic teachings, guiding practices and inquiring participants direct experiences.39
In our study, we found that therapeutic alliance as assessed with the WAI is relat-ed to outcome in both mBcT and emBcT. In our study on group-based mBcT, we found outcome to be mainly associated with clear goal setting.40 Furthermore, in our study comparing mBcT and emBcT, we found that a weaker early therapeutic alliance predicted worse outcome at post-treatment in group mBcT, but not in emBcT.41 In contrast to our expectations, therapeutic alliance did not appear to be not related to dropout.41, 42 However, a good number of patients who dropped out after the first session mentioned that they had ‘other expectations’ of the treatment.
Regarding expectation management, therapists should clearly explain the treat-ment rationale at an early stage in therapy and develop a shared understanding with patients in (e)mBcT. Therapists should be particularly aware of this shared understanding in group-based settings as a weaker alliance is associated with worse outcome. Muran and Barber (2011) emphasize the significance of ‘hitting the ground running’ in short-term group therapy, meaning establishing a strong alliance very early in therapy.34 Similar to our findings, previous studies have found a significant relation between early alliance and outcome in group therapy.43, 44
A subgroup of patients may have difficulties in building a therapeutic relation-ship, for instance due to certain personality traits. In those cases, therapists can facilitate the formation of a strong (repaired) alliance by modeling. This has been shown to lead to better outcome.45, 46 As such, mindfulness therapists should be aware of their capacity and responsibility to model and teach mindfulness effec-tively.47 In this light, they should also be aware of their own (counter) transference phenomena. In their recommendation for mindfulness therapists, Shonin et al (2014) caution against negative transference phenomena in teaching mBIs.48 Inap-propriate personal styles of therapists48 or too much of a non-reacting stance are not necessarily experienced as positive by patients49 and may impact on perceived therapeutic alliance from patients’ perspective.
Regarding emBcT, research on the therapeutic alliance in online interventions is still scarce, even though online applications are increasingly used to improve the access to mental healthcare.50 The building of the therapeutic alliance might develop differently, particularly in formats delivering a large part of the treatment

145
content through online self-help materials. Research on treatment design and working mechanism of emBIs is still in its early stages. No previous studies have been published on the association of therapeutic alliance and outcome in emBIs for cancer patients. Our finding that the therapeutic alliance is related to outcome of emBcT, is in accordance with earlier research on the relationship between therapeutic alliance and outcome of internet-based cBT (iCBT) for depression and symptoms of post-traumatic stress in mental health care51, 52 and with findings of blended cBT (bCBT) for depression.53 Blended forms of cBT mix f2f (group) therapy and online therapy. In contrast, Preschl et al. (2011) could not confirm this relation.54 Although patient-rated alliance measures are mostly used, alliance can also be measured with therapist-rated alliance measures such as the therapist version of the WAI.36 Therapist-rated alliance might gain additional insight in the building of therapeutic alliance in online or blended interventions with limited therapist feedback. Preschl et al. (2011) found only therapist-rated alliance to be associated with outcome in iCBT.54 Vernmark et al. (2018) explored recently the relation of the patient-rated and therapist-rated therapeutic alliance in bCBT for depression. They found that only therapist-rated alliance and not patient-rated alliance predicted outcome of bCBT.55 To date, the limited findings in internet-based formats are mixed and the relationship between therapeutic alliance and outcome of inter-net-based psychological interventions is still understudied.56
Although in our study dropout was higher in emBcT than mBcT, this did not seem to be associated with the strength of early therapeutic alliance. Questions remain about how to prevent dropout in emBcT. Qualitative research on facilita-tors and barriers of emBcT revealed that therapists are concerned with the lack of continuity of the training as they were missing out on nonverbal information of patients indicating they might withdraw at an early stage.57 So far, no studies have explored the association between therapeutic alliance and treatment adherence in internet-based interventions. According to review findings guidance, in general, seems a beneficial feature of internet-based interventions.58 Therefore, alliance building may enhance engagement to treatment in internet-based interventions.59
Knowledge about alliance and adherence can be important to define the optimal level of therapist support in internet-based interventions.56 It is of interest to shed more light on how to encourage patients to adhere to the treatment in online interventions. Both patient- and therapist-rated measures should be considered in upcoming studies, including measuring the interaction of patients with the online content of interventions, the ‘digital alliance’, irrespective of the therapist. Research on (digital) alliance and adherence in emBcT should include both treat-ment outcome and possible dropout.
chapter 7

146
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Knowledge about the nature of therapeutic alliance and the specific role of the alliance in (e)mBcT can increase the effectiveness of (e)mBcT. Conducting routine outcome measures of therapeutic alliance after every session within (e)mBcT courses might be informative. This can encourage therapists to adjust their therapy, their therapeutic attitude and communication with patients at an early treatment stage and thus improve treatment outcome of (e)mBcT for cancer patients. Gathering weekly measures of both therapeutic alliance and symptom change in a research setting would also make it possible to examine therapeutic alliance as a possible mediator of change in more detail.
group cohesionIn group-based settings, besides the therapist and patient, two additional parties are present: the other patients and the group as a whole.34 Cohesion of a group is often conceptualize as the ‘we-ness’ that is felt among group members: the inti-macy, reciprocity and emotional disclosure that is felt among group members,60 contributing to the cooperation within the group to achieve a common therapeutic aim.61 Cohesion is a complex structure involving member-to-member, member-to-group, member-to-leader, leader-to-leader, and leader-to-co-leader alliances embedded in different dimensions considering the structure and quality of the relationships.62, 63 A problem in the scientific research on group cohesion is that there is lack of clarity and consistency in both measurement and conceptualization of cohesion.64 There is ‘little cohesion in the cohesion literature’.65
Three studies, using different measures for group cohesion, have shown that a higher levels of group cohesion predict better treatment outcome in psychother-apy.66-68 For our study, we used the Dutch Group Cohesion Questionnaire (GcQ) which was designed by van Andel e.a. (2003) on the basis of the Group Attitude Scale (GAS)69 and the Three-Factor Group Questionnaire.70 It consists of two bonding subscales (bonding with other members and bonding with the group as a whole), a cooperation subscale and instrumental subscale. Using only the bonding subscales of the GcQ, Van Andel e.a. (2003) found that these were associated with outcome after cBT for cardiac patients.66 A second study, including all subscales of the GcQ showed that only the cooperation subscale, not the total GcQ score, was associated with outcome in a rehabilitation program for cancer patients.71 Our findings also revealed that a higher total level of group cohesion did not predict better treat-ment outcome in mBcT for cancer patients. However, bonding with the group as a whole and the instrumental subscale did predict mBcT outcome.40 Moreover we found therapist competence appeared to be associated with lower group cohesion. An explanation for this finding could be that the self-rated GcQ mainly focuses on social-emotional aspects that are felt among group members within the group

147
as a whole, whereas the observer-rated mBI:TAc relational skills refer to skills in managing a group learning environment, such as managing issues as ground rules, boundaries and confidentiality, and to leadership style. It might be that the more skilled the mBcT therapist is in managing a group learning environment, the less patients need to rely on their fellow participants for support. Another explanation could be that less competent therapists might leave more room for the casual exchange of individual experiences enhancing group cohesion. To our knowledge, there are no previous quantitative studies on the impact of group cohesion in mBIs, whether in cancer patients or in different settings. Qualitative studies, however, showed that group-based settings in mBIs seem to be of added value to cancer patients in terms of feeling connected, accepted and experiencing trust.49, 72 In addition, it was found that peer support facilitates the learning process, such as acknowledging emotions and gaining different perspectives in mBSR.73
Before conducting new studies on the possible role of group cohesion on outcome in psychotherapy studies, among which (e)mBcT, it might be necessary to reach a broader consensus of both the definition and assessment of group cohesion. In terms of clinical implications of above findings, it has been suggested that prior training in group-work skills are valuable for teaching mindfulness in terms of being able to hold a group and deal with reactivity.39
tiMingFinally, we found participating in mBSR both during and after anticancer treatment helped cancer patients to cope with (anticancer treatment related) mental burden. Irrespective of cancer treatment stage, right timing of participating also seemed to depend on the stage of emotional processing. It was emphasized by patients that being informed at an early stage about the possibility to take part in mBSR is important as it would enable patients to decide for themselves whether and when to enroll. Unfortunately, we do not know whether the timing of the intervention might have played a role in dropping out of the intervention, as we did not gather sufficient information of patients who dropped out the intervention.
The qualitative findings on timing of mBIs have additional value and clinical relevance as they stress the importance of patients autonomy during and after anticancer treatment. These findings are in line with the increasingly recognized notion of personalized medicine with shared decision making as key feature. Shared decision making means that a clinician and patient discuss treatment options, to determine the treatment option that best fits. In this model a clinician needs to invite the patient to work together as a team to make a decision between options and to provide information on the options. A clinician should also elaborate with
chapter 7

148
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
the patient to elicit the preference and finally make a treatment decision togeth-er.74, 75 Although it is acknowledged that shared decision making contributes to patients’ knowledge about treatment and satisfaction with the decision made,76 the essential part of the process, eliciting preferences of the individual patient and a shared understanding, is often hurried through so that clinicians can start offering their own views about choices and treatment options on offer.74 In line with these quantitative findings, a recent qualitative study in a sample of breast cancer patients needing surgery also showed that clinicians guiding patients in their choice between a mastectomy or breast saving operation and radiotherapy, primarily focus on the choices and options, while neglecting the preferences and decision talk.77
Regarding mBIs, the common assumption in medical and psycho-oncological care about when to offer psychological interventions to patients, namely after the anticancer treatment phase, is in contrast with the results of our study. Patients accentuate that they should be informed at an early stage, to strengthen their sense of autonomy. In addition, shared decision making allows them after being well informed and after elaborating preferences, to choose for themselves whether, and if so at which moment in time, to participate in mBIs.
iMpleMentation in clinical practice From clinical perspective, in line with the Dutch oncological guidelines, greater accessibility of evidence-based interventions and treatment programs should be a priority. There are several evidence-based f2f psychological interventions,78-81 blended and online therapy approaches82 for patients with psychological distress available. There are also specific interventions for distressed patients in palliative care.83 We showed that (e)mBcT is a valuable addition to the therapeutic options for distressed cancer patients. Moreover, our follow-up study showed that the reduction of psychological distress and improvement of positive mental health and quality of life are maintained at long-term follow-up (not in this thesis).4 In addition, we found that both interventions also seemed to be cost-effective com-pared to TAu (not in this thesis).84
There are many barriers to overcome to implement effective interventions such as (e)mBcT, from both healthcare professionals’ and patients’ perspectives. However, there are indications that clearly stated goals, cyclic evaluation and improvement processes, encourage the introduction of psychosocial care needs programs for cancer patients in clinical practice.85-87 Capability building strategies for health care professionals might support professionals addressing psychological issues with patients,85 which in turn may help patients to feel less embarrassed or reluc-

149
tant to mention their psychological problems to their physician.88 Interestingly, mBIs for health care professionals themselves might facilitate this process even further. It has been shown in quantitative studies that mBIs and interventions with mindfulness elements, such as acceptance and commitment therapy, might support volunteer aid givers89 and health professionals90, 91 in their daily work, which in turn may result in an increasing confidence to discuss the mental burden of cancer with patients. Qualitative research showed that medical and surgical residents indicated an increased awareness, also regarding their communication skills, and enhanced self-reflection and compassion after following mBSR.92 Being aware of the important task of guiding patients to the best of our ability through their suffering, might be the true base of cancer care.
The findings of the present thesis may also have relevance for the way in which evidence-based psycho-oncological interventions are funded. In the Nether-lands evidence-based psycho-oncological interventions are only reimbursed by healthcare insurers for cancer patients with a diagnosed psychiatric disorder. It is questionable whether having a psychiatric disorder or not is a sensible basis for reimbursing interventions in cancer patients. In 2018, the Dutch National Cancer Society (KWF Kankerbestrijding), presented a Social Business Case to the Dutch Ministry of Health,93 based on Meaning Centered Therapy81 and (e)mBcT as a result of, amongst others, studies conducted within the BeMind research project. A Social Business Case is a common method for mapping the economic and social benefits of an intervention. We agree with the Dutch National Cancer Society that all people suffering from and surviving cancer who are in need of support should be given access to appropriate quality of life care. It is now the responsibility of the Ministry of Health to solve the remaining obstacles to achieve this and facilitate healthcare professionals to make psychosocial interventions for cancer patients widely accessible. We hope the BeMind research project will contribute to this important ambition.
chapter 7

150
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
References
1. Kabat-Zinn, J., Full catastrophe living, revised edition: how to cope with stress, pain and illness using mindfulness meditation. 2013: Hachette uK.
2. Segal, Z.V., J.M.G. Williams, and J.D. Teasdale, Mindfulness-based cognitive therapy for depression: A new approach to relapse prevention. 2013, New York: Guil-ford Press.
3. Schellekens, M.P., et al., A qualitative study on mindfulness-based stress reduction for breast cancer patients: how women experience participating with fellow patients. Supportive Care Cancer, 2016. 24(4): p. 1813-20.
4. Cillessen, L., et al., Consolidation and pre-diction of long-term treatment effect of group and online mindfulness-based cognitive therapy for distressed cancer patients. Acta Oncol, 2018: p. 1-10.
5. van Scheppingen, C., et al., Is imple-menting screening for distress an efficient means to recruit patients to a psychological intervention trial? Psycho-Oncology, 2014. 23(5): p. 516-523.
6. Polit, D.F. and C.T. Beck, Essentials of nursing research: Appraising evidence for nursing practice. 2010: Lippincott Wil-liams & Wilkins.
7. Thorsen, L., et al., Cancer patients’ needs for rehabilitation services. Acta Oncologica, 2011. 50(2): p. 212-22.
8. Clover K.A., et al., Why do oncology outpa-tients who report emotional distress decline help? Psycho-Oncology 2014.
9. Garssen, B. and M. Van der Lee, Re: Screening for emotional distress in cancer patients: a systematic review of assessment instruments. J National Cancer Institute, 2010. 102(7): p. 506-8; author reply 508.
10. Thewes, B., et al., One way or another: The opportunities and pitfalls of self-referral and consecutive sampling as recruitment strategies for psycho-oncology intervention trials. Psycho-Oncology, 2018. 27(8): p. 2056-2059.
11. Tuinman, M.A., S.M.
Gazendam-Donofrio, and J.E. Hoek-stra-Weebers, Screening and referral for psychosocial distress in oncologic practice: use of the Distress Thermometer. Cancer, 2008. 113(4): p. 870-8.
12. Kissane, D.W., Unrecognised and untreated depression in cancer care. Lancet Psychia-try, 2014. 1(5): p. 320-1.
13. Grassi, L., et al., Psychological factors affecting oncology conditions. Advanced Psychosomatic Medicine, 2007. 28: p. 57-71.
14. Garssen, B., et al., Characteristics of patients in routine psycho-oncological care, and changes in outcome variables during and after their treatment. Psychology & health, 2016. 31(10): p. 1237-1254.
15. Mitchell, A.J., N. Meader, and P. Sy-monds, Diagnostic validity of the Hospital Anxiety and Depression Scale (HADS) in cancer and palliative settings: A meta-anal-ysis. Journal of Affective Disorders, 2010. 126(3): p. 335-348.
16. Roberts, M.H., R.B. Fletcher, and P.L. Merrick, The validity and clinical utility of the Hospital Anxiety and Depression Scale (HADS) with older adult New Zealanders. International Psychogeriatrics, 2014. 26(2): p. 325-333.
17. Jacobson, N.S. and P. Truax, Clinical significance: a statistical approach to de-fining meaningful change in psychotherapy research. J Consulting Clinical Psycholo-gy, 1991. 59(1): p. 12-9.
18. First, M.B., et al., Structured Clinical Interview for DSm-IV® Axis I Disorders (ScID-I), Clinician Version, Administration Booklet. 2012: American Psychiatric Pub.
19. Faller, H., et al., Effects of psycho-oncologic interventions on emotional distress and quality of life in adult patients with cancer: systematic review and meta-analysis. Jour-nal of Clinical Oncology, 2013: p. JCO. 2011.40. 8922.
20. Zhang, Q., H. Zhao, and Y. Zheng, Effectiveness of mindfulness-based stress reduction (mbSR) on symptom variables and health-related quality of life in breast cancer patients—a systematic review and

151
meta-analysis. Supportive Care in Can-cer, 2019. 27(3): p. 771-781.
21. L. Cillessen et al., Mindfulness-based interventions for psychological and physical health outcomes in cancer patients and -survivors: a meta-analysis of randomized controlled trials. Under review.
22. Crane RS, K.W., Williams JMG, Hastings RP, Cooper L, Fennell MJV Competence in teaching mindfulness-based courses: concepts, development and assessment. Mindfulness 2012.
23. Sharpless, B.A. and J.P. Barber, A concep-tual and empirical review of the meaning, measurement, development, and teaching of intervention competence in clinical psychol-ogy. Clinical Psychology Review, 2009. 29(1): p. 47-56.
24. Branson, A., R. Shafran, and P. Myles, Investigating the relationship between competence and patient outcome with cBT. Behavioral Research Therapy, 2015. 68: p. 19-26.
25. Huijbers, M.J., et al., Teacher Competence in Mindfulness-Based Cognitive Therapy for Depression and Its Relation to Treatment Outcome. Mindfulness, 2017. 8(4): p. 960-972.
26. Crane, R.S. and F.M. Hecht, Intervention Integrity in Mindfulness-Based Research. Mindfulness (N Y), 2018. 9(5): p. 1370-1380.
27. Borrelli, B., The Assessment, Monitoring, and Enhancement of Treatment Fidelity In Public Health Clinical Trials. J Public Health Dent, 2011. 71(s1): p. S52-s63.
28. Weck, F., et al., Reliability of adherence and competence assessment in psychoeducational treatment: influence of clinical experience. J Nervous Mental Diseases, 2011. 199(12): p. 983-986.
29. Crane, R.S., et al., Development and validation of the mindfulness-based interventions - teaching assessment criteria (mbI:TAc). Assessment, 2013. 20(6): p. 681-8.
30. Crane, R.S. and W. Kuyken, The Mind-fulness-Based Interventions: Teaching As-sessment Criteria (mBI:TAC): reflections on
implementation and development. Current Opinion Psychology, 2018. 28: p. 6-10.
31. Crane, R.S. and B. Reid, Training Mind-fulness Teachers: Principles, Practices and Challenges, in Resources for Teaching Mind-fulness: An International Handbook, D. McCown, D. Reibel, and M.S. Micozzi, Editors. 2016, Springer International Publishing: Cham. p. 121-140.
32. Bordin, E.S., Theory and research on the therapeutic working alliance: New directions. The working alliance: Theory, research, and practice, 1994: p. 13-37.
33. Luborsky, L., Therapeutic alliances as predictors of psychotherapy outcomes: Fac-tors explaining the predictive success. The working alliance: Theory, research, and practice, 1994: p. 38-50.
34. Muran, J.C. and J.P. Barber, The thera-peutic alliance: An evidence-based guide to practice. 2011: Guilford Press.
35. Horvath, A.O. and L.S. Greenberg, Development and validation of the Working Alliance Inventory. Journal of counseling psychology, 1989. 36(2): p. 223.
36. Horvath, A.O., et al., Alliance in individual psychotherapy. Psychotherapy, 2011. 48(1): p. 9.
37. Ardito, R.B. and D. Rabellino, Therapeu-tic alliance and outcome of psychotherapy: historical excursus, measurements, and prospects for research. Front Psychology, 2011. 2: p. 270.
38. Berger, T., The therapeutic alliance in in-ternet interventions: A narrative review and suggestions for future research. Psychother-apy Research, 2017. 27(5): p. 511-524.
39. McCown, D., D. Reibel, and M.S. Mi-cozzi, Teaching mindfulness. A practical guide for clinicians and educators. uS: Springer, 2010.
40. Bisseling, E.M., et al., Therapeutic alliance -not therapist competence or group cohesion- contributes to reduction of psychological distress in group-based Mindfulness-Based Cognitive Therapy for cancer patients. Clini-cal Psychology and Psychotherapy, 2019.
41. Bisseling E.M. et al.,. The development and association of therapeutic alliance
chapter 7

152
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
with outcome of internet-based Mindful-ness-Based Cognitive Therapy compared to group-based mbcT for distressed cancer patients: a secondary analysis of a multi-center randomized controlled trial. Journal of Medical Internet Research (2019): doi: 10.2196/14065
42. Compen, F., et al., Face-to-Face and In-ternet-Based Mindfulness-Based Cognitive Therapy Compared With Treatment as Usual in Reducing Psychological Distress in Patients With Cancer: A Multicenter Ran-domized Controlled Trial. Journal Clinical Oncology, 2018: p.
43. Piper, W.E., et al., Level of alliance, pattern of alliance, and outcome in short–term group therapy. International Journal of Group Psychotherapy, 2005. 55(4): p. 527-550.
44. Taft, C.T., et al., Personality, interpersonal, and motivational predictors of the working alliance in group cognitive-behavioral therapy for partner violent men. Journal of consulting and clinical psychology, 2004. 72(2): p. 349.
45. Tsai, M., R.J. Kohlenberg, and J.W. Kanter, A functional analytic psycho-therapy (FAP) approach to the therapeutic alliance. The therapeutic alliance: An evidence-based guide to practice, 2010: p. 172-190.
46. Zilcha-Mano, S. and P. Errazuriz, Early development of mechanisms of change as a predictor of subsequent change and treat-ment outcome: The case of working alliance. J Consult Clin Psychol, 2017. 85(5): p. 508-520.
47. Piet, J., L. Fjorback, and S. Santorelli, What Is Required to Teach Mindful-ness Effectively in mBSR and mBcT?, in Mindfulness and Buddhist-Derived Approaches in Mental Health and Addiction, E. Shonin, W.V. Gordon, and M.D. Griffiths, Editors. 2016, Springer International Publishing: Cham. p. 61-83.
48. Shonin, E. and W. Van Gordon, Practical recommendations for teaching mind-fulness effectively. Mindfulness, 2015. 6(4): p. 952-955.
49. van Aalderen, J.R., et al., The Role of the Teacher in Mindfulness-Based Approaches: A Qualitative Study. Mindfulness, 2014. 5(2): p. 170-178.
50. Plaza, I., et al., Mindfulness-based mobile applications: literature review and anal-ysis of current features. JmIR Mhealth Uhealth, 2013. 1(2): p. e24.
51. Bergman Nordgren, L., et al., Role of the Working Alliance on Treatment Outcome in Tailored Internet-Based Cognitive Behavioural Therapy for Anxiety Disorders: Randomized Controlled Pilot Trial. JmIR Res Protoc, 2013. 2(1): p. e4.
52. Wagner, B., et al., Online working alliance predics treatment outcome for posttraumatic stress symptoms in Arab War-traumatized patients. Depression and Anxiety, 2012. 29(7): p. 646-651.
53. Ly, K.H., et al., Smartphone-Supported versus Full Behavioural Activation for Depression: A Randomised Controlled Trial. PLoS One, 2015. 10(5): p. e0126559.
54. Preschl, B., A. Maercker, and B. Wagner, The working alliance in a randomized controlled trial comparing online with face-to-face cognitive-behavioral thera-py for depression. Bmc Psychiatry, 2011. 11: p. 189.
55. Vernmark, K., et al., Working alliance as a predictor of change in depression during blended cognitive behaviour therapy. Cogn Behav Ther, 2018: p. 1-15.
56. Pihlaja, S., et al., Therapeutic alliance in guided internet therapy programs for depres-sion and anxiety disorders - A systematic review. Internet Interventions, 2018. 11: p. 1-10.
57. Compen, F.R., et al., Mindfulness-Based Cognitive Therapy for Cancer Patients Delivered via Internet: Qualitative Study of Patient and Therapist Barriers and Facilita-tors. Journal Medical Internet Res, 2017. 19(12): p. e407.
58. Baumeister, H., et al., The impact of guidance on Internet-based mental health interventions — A systematic review. Inter-net Interventions, 2014. 1(4): p. 205-215.
59. Hilvert-Bruce, Z., et al., Adherence as a

153
determinant of effectiveness of internet cognitive behavioural therapy for anxi-ety and depressive disorders. Behaviour research and therapy, 2012. 50(7-8): p. 463-468.
60. Yalom, I.D., The theory and practice of group psychotherapy. 1995 (press 2005): Basic Books (AZ).
61. Budman, S.H., et al., Cohesion, alliance and outcome in group psychotherapy. Psychiatry, 1989. 52(3): p. 339-50.
62. Burlingame, G.M., D.T. McClendon, and J. Alonso, Cohesion in group therapy. Psychotherapy, 2011. 48(1): p. 34.
63. Schnur, J.B. and G.H. Montgomery, A systematic review of therapeutic alliance, group cohesion, empathy, and goal con-sensus/collaboration in psychotherapeutic interventions in cancer: Uncommon factors? Clinical Psychology Review, 2010. 30(2): p. 238-247.
64. Hornsey, M.J., L. Dwyer, and T.P. Oei, Beyond cohesiveness: Reconceptualizing the link between group processes and outcomes in group psychotherapy. Small Group Research, 2007. 38(5): p. 567-592.
65. Joyce, A.S., W.E. Piper, and J.S. Ogrod-niczuk, Therapeutic alliance and cohesion variables as predictors of outcome in short–term group psychotherapy. International Journal of Group Psychotherapy, 2007. 57(3): p. 269-296.
66. van Andel, P., et al., Group cohesion and working alliance: prediction of treatment outcome in cardiac patients receiving cognitive behavioral group psychotherapy. Psychotherapy and Psychosomatics, 2003. 72(3): p. 141-9.
67. Taube-Schiff, M., et al., Group cohesion in cognitive-behavioral group therapy for social phobia. Behavioral Research and Therapy, 2007. 45(4): p. 687-98.
68. Marziali, E., H. Munroe-Blum, and L. McCleary, The contribution of group cohesion and group alliance to the outcome of group psychotherapy. International Journal Group Psychotherapy, 1997. 47(4): p. 475-97.
69. Evans, N.J. and P.A. Jarvis, The group
attitude scale: A measure of attraction to group. Small Group Behavior, 1986. 17(2): p. 203-216.
70. Stokes, J.P., Components of group cohesion: Intermember attraction, instrumental value, and risk taking. Small Group Behavior, 1983. 14(2): p. 163-173.
71. May, A.M., et al., The effect of group cohesion on rehabilitation outcome in cancer survivors. Psycho-Oncology, 2008. 17(9): p. 917-25.
72. Mackenzie, M.J., et al., A qualitative study of self-perceived effects of mindfulness-based stress reduction (mBSR) in a psychosocial oncology setting. Stress and Health, 2007. 23(1): p. 59-69.
73. Schellekens MPJ et al. , A qualitative study on mindfulness-based stress reduction for breast cancer patients: how women experience participating with fellow patients. Support Care Cancer, 2016. 24: p. 1813-1820
74. Elwyn, G., et al., A three-talk model for shared decision making: multistage consul-tation process. British Medical Journal, 2017. 359: p. j4891.
75. Elwyn, G., et al., Using a ‘talk’model of shared decision making to propose an obser-vation-based measure: Observer OPTION5 Item. Patient education and counseling, 2013. 93(2): p. 265-271.
76. Barry, M.J. and S. Edgman-Levitan, Shared decision making—the pinnacle of pa-tient-centered care. New England Journal of Medicine, 2012. 366(9): p. 780-781.
77. Savelberg, W., et al., Does lack of deeper understanding of shared decision making explains the suboptimal performance on crucial parts of it? An example from breast cancer care. European Journal of Oncolo-gy Nursing, 2019. 38: p. 92-97.
78. Smith, A., et al., Pilot of a theoretically grounded psychologist-delivered intervention for fear of cancer recurrence (Conquer Fear). Psycho-Oncology, 2015. 24(8): p. 967-70.
79. Herschbach, P., et al., Evaluation of two group therapies to reduce fear of progression in cancer patients. Support Care Cancer, 2010. 18(4): p. 471-9.
chapter 7

154
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
80. Butow, P.N., et al., Randomized Trial of ConquerFear: A Novel, Theoretically Based Psychosocial Intervention for Fear of Cancer Recurrence. J Clin Oncol, 2017: p. Jco2017731257.
81. van der Spek, N., et al., Efficacy of mean-ing-centered group psychotherapy for cancer survivors: a randomized controlled trial. Psychological Medicine, 2017. 47(11): p. 1990-2001.
82. van de Wal, M., et al., Efficacy of Blended Cognitive Behavior Therapy for High Fear of Recurrence in Breast, Prostate, and Colorectal Cancer Survivors: The SWORD Study, a Randomized Controlled Trial. Journal Clinical Oncology, 2017. 35(19): p. 2173-2183.
83. Rodin, G., et al., Managing Cancer and Living Meaningfully (cALm): A Random-ized Controlled Trial of a Psychological Intervention for Patients With Advanced Cancer. Journal Clinical Oncology, 2018. 36(23): p. 2422-2432.
84. Compen F.R. et al., Cost-utility of individual internet-based and face-to-face Mindfulness-Based Cognitive Therapy compared to Treatment As Usual in reducing psychological distress in cancer patients. Under review.
85. Dudgeon, D., et al., Cancer Care Ontario’s experience with implementation of routine physical and psychological symptom distress screening. Psycho-Oncology, 2012. 21(4): p. 357-64.
86. Riblet, N., et al., Addressing distress in pa-tients with head and neck cancers: a mental health quality improvement project. J Na-tional Comprehensive Cancer Network, 2014. 12(7): p. 1005-1013.
87. van der Hout, A., et al., Efficacy, cost-utili-ty and reach of an eHealth self-management application ‘Oncokompas’ that helps cancer survivors to obtain optimal supportive care: study protocol for a randomised controlled trial. Trials, 2017. 18(1): p. 228.
88. Valente, S.M., J.M. Saunders, and M.Z. Cohen, Evaluating depression among patients with cancer. Cancer Pract, 1994. 2(1): p. 65-71.
89. Buter, M., Mindfulness voor mantelzorgers; een tijdelijk succes of winst op lange termijn? Psychology, 2014. 6(5): p. 413-423.
90. Rudaz, M., et al., Mindfulness and acceptance-based trainings for fostering self-care and reducing stress in mental health professionals: A systematic review. Journal of Contextual Behavioral Science, 2017. 6(4): p. 380-390.
91. Verweij, H., et al., Mindfulness-based stress reduction for residents: A randomized con-trolled trial. Journal of general internal medicine, 2018: p. 1-8.
92. Verweij, H., et al., Does mindfulness train-ing enhance the professional development of residents? A qualitative study. Academic Medicine, 2018. 93(9): p. 1335-1340.
93. Maatschappelijk Business Case. Inter-venties gericht op vermindering van angstige en depressieve gevoelens bij mensen met kanker, 2018. Sinzer en KWF Kankerbestrijding.



Addenda
Nederlandse samenvattingDankwoordCurriculum VitaePublicatielijstData management statementDonders Graduate School for Cognitive Neuroscience

158
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Nederlandse samenvatting (van dit proefschrift)
introductie
psychische distress en kankerVanaf 2025 zullen wereldwijd ieder jaar 20.000.000 mensen worden gediagnosticeerd met kanker.1 De invasieve behandelingen en fysieke symptomen kunnen van grote invloed zijn op het welzijn. De mentale last die patiënten kunnen ervaren, wordt vaak omschreven als psychische distress. Het National Comprehensive Cancer Network (NccN) definieert psychische distress als ‘een multifactoriële onaangename emotionele ervaring van psychologische (dat wil zeggen cognitief, gedragsmatig, emotionele), sociale of spirituele aard die het vermogen om effectief om te gaan met de ziekte kanker en de fysieke symptomen ervan en de behandeling ervan beperken. Psychische distress strekt zich uit over een continuüm, variërend van normale gevoelens van kwetsbaarheid, verdriet en angsten tot problemen die een invaliderend karakter krijgen zoals depressie, angst, paniek, sociaal isolement en een existentiële of spirituele crisis.’2 Ongeveer een derde van alle kankerpatiënten lijdt aan een dusdanige mate van distress dat ondersteuning gewenst lijkt.3 Distress gaat veelal gepaard met een verminderde kwaliteit van leven, verminderde therapietrouw en langere ziekenhuis opnames.4 Deze psychologische gevolgen van kanker kunnen maanden of zelfs jaren aanhouden.5
Volgens de Nederlandse oncologische richtlijnen (www.oncoline.nl) zouden alle oncologische patiënten moeten worden gescreend op psychische distress om vroegtijdig te kunnen signaleren of er een behoefte aan zorg is, en of een eventuele verwijzing naar psychologische ondersteuning noodzakelijk is. Vroegtijdige (h)erkenning en verwijzing van patiënten die psychische problemen ontwikkelen als gevolg van de confrontatie met kanker kan de kwaliteit van het leven van deze patiënten verbeteren, en bijdragen aan tevredenheid over (medische) zorg en communicatie met zorgverleners.6 Volgens de richtlijnen is er een grote kans op onderdiagnostiek van distress, en in het verlengde daarvan ook op onderbehan-deling ervan, zonder systematische screening.
psychiatrische stoornissen bi j kankerpatiëntenBij 30-40% van de kankerpatiënten, zijn de psychische klachten zo ernstig dat deze eveneens voldoen aan de criteria van een angst- of depressieve stoornis.4 Vooral in de vroege behandelingsfase zijn deze stoornissen vaak aanwezig.7 Op de lange termijn lijkt angst in plaats van depressie het voornaamste probleem voor veel kankerpatiënten.5 Angst- en depressieve stoornissen zijn gerelateerd aan zowel over- als onderconsumptie van oncologische zorg,8, 9 lagere kwaliteit van leven 10,11 en verkorte overlevingstijd.12-14

159
ned
erland
se saMen
vatting
Ondanks dat 30-40% van de kankerpatiënten een psychiatrische stoornis ontwik-kelt,4, 15 en de 15-25% andere klinisch relevante aandoeningen rapporteren, zoals angst voor terugkeer van kanker, demoralisatie of algemene psychische distress,16,
17 wordt minder dan 30% van hen herkend door oncologisch werkende professio-nals,18 laat staan adequaat verwezen naar geestelijke gezondheidszorginstellingen of psycho-oncologische centra. Veel noodlijdende patiënten blijven onbehan-deld,18, 19 terwijl interventies zoals counseling en psycho-educatie, en psychologische behandelingen (zoals groep of individuele cognitieve gedrags-, psychodynamische of existentiële therapie) ontwikkeld en beschikbaar zijn voor deze populatie.19, 20
psycho-oncologische interventiesPsychologische interventies zijn effectief in het verminderen van de symptomen van psychische distress en affectieve stoornissen bij kankerpatiënten.21-23 Veel van deze interventies zijn gebaseerd op cognitieve gedragstherapeutische (cGT) principes. cGT richt zich op interactie tussen gedachten, gevoelens en gedragingen. Het is een collaboratieve, probleemgerichte therapie met een pragmatische en gestruc-tureerde aanpak voor het beheersen van psychologische problemen. Aangezien traditionele cGT-technieken in het algemeen gebaseerd zijn op de veronderstel-ling dat angstige of depressieve individuen irrealistische negatieve automatische gedachten hebben,24 is het niet altijd verenigbaar met de realistische vrees voor ziekteprogressie, invaliditeit en overlijden in (gevorderde) kanker.25 cGT is mogelijk minder geschikt voor een subgroep van patiënten bij wie een recidief inderdaad een verhoogde kans heeft en die voortdurend opnieuw worden blootgesteld aan externe triggers als gevolg van hun voortdurende zorg.26, 27 Gezien de stijgende prevalentie van mensen die leven met (gevorderde) kanker,1 zal het absolute aantal patiënten dat psychologische behandeling nodig heeft, toenemen. Het aanpakken van de toenemende behoefte aan mentale ondersteuning, vraagt om innovatieve en effectieve psychologische behandelingsopties.
op Mindfulness gebaseerde interventiesOp mindfulness gebaseerde interventies (‘Mindfulness-Based Interventions’, afgekort als (mBI’s), zoals Mindfulness-Based Stress Reduction (mBSR)28 en Mind-fulness-Based Cognitive Therapy (mBcT)29 zijn effectieve psychologische behan-delingsopties. Mindfulness wordt gedefinieerd als het bewust aandacht schenken aan actuele ervaringen op een accepterende en niet-veroordelende manier.28 Tradi-tioneel bestaan mBSR en mBcT uit 8-wekelijkse 2,5 uur durende groepssessies, een 6-uur durende stille dag tussen sessies 6 en 7, en dagelijks 45 minuten beoefening thuis. Elke sessie bestaat uit mindfulness-oefeningen, didactische onderricht en het delen van ervaringen. mBSR werd oorspronkelijk ontwikkeld voor patiënten met chronische somatische aandoeningen om hen te helpen effectiever te omgaan

160
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
met hun aandoening door het vergroten van het vermogen om zich te concen-treren op de huidige ervaringen, zelfs in de aanwezigheid van intern ongemak. mBcT combineert mBSR met cGT-elementen en werd oorspronkelijk ontwikkeld om terugval te voorkomen bij patiënten met terugkerende ernstige depressieve stoornissen.29 Steeds vaker wordt mBcT ook toegepast bij andere doelgroepen, zoals kankerpatiënten.30
op Mindfulness gebaseerde online interventiesHoewel mBI’s nuttig zijn, vereisen ze in traditionele vorm fysieke aanwezigheid gedurende een aantal weken. Op mindfulness gebaseerde online interventies (‘internet-mBI’s’, afgekort als emBI’s) daarentegen zijn gemakkelijk toegankelijk, beschikbaar en besparen reistijd.31 Een recente review van 15 RcTs naar emBI’s toonde een klein maar belangrijk gunstig effect op depressie, angst, welzijn en mindful-ness. Bewijs voor emBI’s in kanker is schaars. Individuele online mBcT (‘internet mBcT’, afgekort als emBcT) bleek aanzienlijk vermindering van vermoeidheid en psychische distress bij ernstig vermoeide kankerpatiënten.32 Dropout was met 38% relatief hoog in emBcT, voornamelijk als gevolg van de ervaren intensiteit van het programma.33
therapeutische aspecten De effectiviteit van iedere psychologische behandeling hangt mede samen van de vaardigheid of competentie van de therapeut,34 de sterkte van de gevestigde therapeutische relatie (ook wel therapeutische alliantie genoemd),35, 36 en als het een groep betreft groepsfactoren zoals de groepscohesie.37
De competentie van de therapeut verwijst naar het niveau van vaardigheden die de therapeut heeft getoond bij het leveren van de behandeling.34, 38 Slechts één multicenter studie naar mBcT voor recidiverende depressie (n = 241) richtte zich op de rol van de therapeut competentie.39 In deze studie werd geen robuuste associatie gevonden tussen de competentie van de therapeut en de behandelingsuitkomst. 39
De therapeutische alliantie wordt beschreven als de collaboratieve en affectieve band tussen therapeut en patiënt, en gedefinieerd als de mate waarin therapeut en patiënt het eens zijn over de doelstellingen van de behandeling; over hoe deze behandeldoelen te bereiken; en de mate van wederzijds vertrouwen tussen patiënt en therapeut.40, 41 De therapeutische alliantie is een veel onderzocht maar over onderzoek naar de therapeutische alliantie in mBI’s voor kankerpatiënten werd tot op heden niet gepubliceerd. Groepscohesie verwijst voornamelijk naar sociaal-emotionele samenhang: de intimiteit, wederkerigheid en emotionele openheid die wordt gevoeld onder groepsleden.37 Onderzoek naar de impact van groepscohesie bij interventies voor kankerpatiënten is zeer schaars. In een revalidatie programma voor kanker patiënten

161
leek een aantal dimensies van groepscohesie in verband te worden gebracht met interventie resultaten.42 Zover wij weten is er nog niet eerder kwantitatieve onder-zoek verricht naar de impact van groepscohesie in mBI’s voor kankerpatiënten.
tiMing In de klinische praktijk en bij wetenschappelijk onderzoek worden mBI’s veelal aangeboden na de actieve antikankerbehandelingen, ondanks de wetenschap dat psychische distress bijzonder hoog kan zijn in het eerste jaar van de diagnose en tijdens kankerbehandelingen.43, 44 Tot op heden is er weinig bekend over wat pati-enten zelf ervaren als de meest geschikte moment om deel te nemen aan mBI’s. Het ontrafelen van onderliggende therapeutische factoren zal onze kennis over mBI’s verrijken. De focus van onderzoeksactiviteiten op het mBI-gebied heeft tot op heden voornamelijk betrekking op de (door)ontwikkeling van mBI’s voor spe-cifieke doelgroepen. Door het bestuderen van de relatie tussen behandeluitkomst en therapeutcompetentie, de therapeutische alliantie en groepscohesie, en andere factoren zoals de timing van de interventie, kunnen we de beschikbare vormen van mBI’s voor kankerpatiënten verder verbeteren. Inzicht in welke factoren de uitkomst van de behandeling beïnvloeden kan de implementatie van mBI’s in de klinische praktijk vergemakkelijken.45
doel van het proefschriftDit proefschrift richt zich op het onderzoeken van de effectiviteit van online mBcT (emBcT) en mindfulness-based cognitieve therapie (mBcT) in groepsverband bij het verminderen van psychische problemen bij kankerpatiënten. Daarnaast bestudeerden we de relatie tussen behandeluitkomst en therapeutcompetentie, de therapeutische alliantie en groepscohesie, en andere factoren zoals de timing van de interventie. Het vervolg van dit hoofdstuk biedt een samenvatting van de resultaten uit hoofdstukken twee tot en met zes en bespreekt deze in relatie tot bestaande literatuur. Er worden methodologische overwegingen besproken, evenals implicaties en suggesties voor verder onderzoek en voor de klinische praktijk.
saMenvattingIn ons multicenter Randomized Controlled Trial (RcT) (hoofdstuk 3), de BeMind- studie, onderzochten we de effectiviteit van zowel emBcT als mBcT in groeps-verband bij het verminderen van psychische klachten bij kankerpatiënten. We onderzochten 245 kankerpatiënten met psychologische distress (≥ 11 op de Hospital Anxiety and Depression Scale (HADS)). Zij werden willekeurig toegewezen aan mBcT (n=77), emBcT (n=90) of gebruikelijke zorg (‘Treatment As Usual’, afgekort als TAu) (n=78). Patiënten vulden een evaluatie in voor de baseline (T0) en na interventie (T1). Resultaten toonden aan dat patiënten na zowel mBcT als emBcT
ned
erland
se saMen
vatting

162
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
een klinisch relevante vermindering van psychologische distress meldden dan patiënten na de TAu. Bovendien bleken psychiatrische diagnoses na behandeling lager bij zowel mBcT als emBcT dan bij TAu, maar deze veranderingen waren niet statistisch significant. Beide interventies verminderden de angst voor terugkeer van de kanker en rumineren aanzienlijk, en verbeterden de kwaliteit van leven wat betreft geestelijke gezondheid, mindfulnessvaardigheden en positieve geestelijke gezondheid, in vergelijking met TAu. Kwaliteit van leven wat betreft lichamelijke gezondheid verbeterde niet. We onderzochten vervolgens of therapeutcompetentie, de therapeutische alliantie en groepscohesie een rol zouden kunnen spelen bij de behandelingsresultaten (hoofdstuk 4). De hypothese was dat de therapeutcompetentie, de therapeutische alliantie en de groepscohesie het resultaat van de behandeling zouden voorspellen, en dat de therapeutcompetentie een voorwaarde was voor het ontwikkelen van zowel therapeutische alliantie als groepscohesie. Er werden gegevens gebruikt van 120 patiënten die werden toegewezen aan de f2f-groepsvorm van mBcT na de initiële randomisatie (n=77) of na het voltooien van TAu (n=43). De analyses omvatten alleen patiënten die de mBcT hadden voltooid: patiënten die vier of meer sessies hadden bijgewoond (n=84). De bevindingen toonden aan dat de the-rapeutische alliantie significant bijdroeg aan vermindering van distress bij mBcT, maar de groepscohesie niet. De competentie van de therapeut voorspelde de mate van distress na de behandeling niet en leek ook geen voorwaarde te zijn voor een sterke therapeutische alliantie en hogere mate van groepscohesie. In tegenstelling tot onze verwachtingen leek therapeutcompetentie wel een rol te spelen bij een lagere groepscohesie. Hoofdstuk 5 toonde de resultaten van een verkennend onderzoek naar het niveau van therapeutische alliantie in emBcT vergeleken met mBcT. Ook deze studie was onderdeel van onze multicenter RcT (n=245) naar de effectiviteit van (e)mBcT voor kankerpatiënten met distress. Onderzoeksvragen waren of vroege therapeutische alliantie uitval van de behandeling in (e)mBcT voorspelt, hoe de therapeutisch alliantie zich opbouwt in zowel emBcT als mBcT en of de vroege alliantie een voorspeller is van de vermindering van distress en de toename van geestelijk welzijn na de behandeling in beide condities. De alliantie werd geme-ten aan het begin van week 2 (vroege alliantie), week 5 en week 9. Uitkomstmaten waren psychische distress en geestelijk welzijn. De vroege alliantie voorspelde geen voortijdige uitval van de behandeling bij (e)mBcT. De therapeutische alliantie nam in de loop van de tijd in beide condities toe. Deze stijging verschilde niet tussen emBcT en mBcT. De kracht van de vroege therapeutische alliantie voorspelde wel een significante daling van distress en een significante stijging van geestelijk welzijn na de behandeling in beide behandelingen. De relatie met vermindering van distress verschilde tussen behandelingen: een zwakkere vroege therapeutische

163
alliantie voorspelde grotere mate van distress na behandeling bij mBcT maar niet bij emBcT. In zowel de klinische praktijk als in onderzoekssituaties worden mBI’s vaak aangeboden na de actieve behandeling tegen kanker. Wij waren geïnteresseerd in wat patiënten zelf ervaren als de meest geschikte tijd om deel te nemen aan mBSR. Voor deze studie (hoofdstuk 6) werden patiënten met borstkanker gewor-ven bij de oncologieafdelingen van het Radboud Universitair Medisch Centrum in Nijmegen, het Rijnstate-ziekenhuis in Arnhem en via de website van Pink Ribbon (www.pinkribbon.nl). Er werden focusgroepen en semi-gestructureerde individuele interviews gebruikt om te onderzoeken hoe patiënten het ervaren om deel te nemen aan mBSR in verschillende stadia van hun ziekte. Uit de kwalitatieve gegevens bleek dat hoewel deelname aan mBSR tijdens de behandeling patiënten hielp om met de behandeling om te gaan, lichamelijk klachten deelname ook kon-den belemmeren. Na de actieve behandeling tegen kanker vonden patiënten het makkelijker deelnemen omdat men meer energie had. Echter sommige patiënten gaven aan dat ze te laat hadden deelgenomen om er volledig van te profiteren. Naast de fase van de behandeling leek de juiste timing ook afhankelijk te zijn van het stadium van emotionele verwerking. Deelnemers benadrukten het belang om in een vroeg stadium te worden geïnformeerd over de mogelijkheid om deel te nemen aan mBSR, omdat zij hierdoor zelf zouden kunnen beslissen of en wanneer ze zich zouden inschrijven.
discussieDe hoofdstudie van het BeMind-onderzoeksproject in dit proefschrift (hoofdstuk 2 en 3) was de eerste studie waarin de effectiviteit van zowel emBcT als mBcT werd vergeleken met TAu bij kankerpatiënten met distress. De aanvullende kwantita-tieve studies in dit proefschrift waren vooral gericht op aspecten van therapeuti-sche factoren in relatie tot beide interventies (hoofdstuk 4 en 5). Het kwalitatieve onderzoek in dit proefschrift (hoofdstuk 6) verzamelde persoonlijke ervaringen om de haalbaarheid en optimale timing van de interventie te onderzoeken. Deze studies dragen bij aan het voort durende debat in psychotherapieonderzoek over het relatieve belang van therapeutische aspecten, zoals therapeutcompetentie, therapeutische alliantie en groepscohesie, en de uitvoering van de behandeling, waaronder timing op de behandeluitkomst.
Methodologische overwegingenOntwerp
Een belangrijke kracht van het proefschrift was het ontwerp van de hoofdonder-zoek (hoofdstuk 2 en 3), een drie-armige multicenter-RcT met parallelle groepen om de effectiviteit van emBcT en mBcT versus TAu te vergelijken bij het vermin-
ned
erland
se saMen
vatting

164
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
deren van psychologische distress bij kankerpatiënten. Het was de eerste studie waarin emBcT en mBcT gelijktijdig werden vergeleken met TAu in een grote steekproef van heterogene kankerpatiënten met psychologische distress. Beide interventies waren geprotocolleerd en werden geleverd door gekwalificeerde therapeuten op verschillende locaties in Nederland, wat belangrijk is met het oog op generaliseerbaarheid. Hoewel de groep belangrijk wordt geacht voor mBI’s,46 hebben de studies in dit proefschrift laten zien dat individueel begeleide emBcT met wekelijkse feedback van online therapeuten ook effectief is. Ons onderzoek was echter niet geschikt om emBcT rechtstreeks met mBcT te vergelijken, omdat hiervoor een grotere steekproefomvang zou zijn vereist. Interessant is dat onze follow-upstudie (niet in dit proefschrift) aantoonde dat de effecten van zowel emBcT als mBcT verder leken te verbeteren tijdens de follow-upperiode, waarin emBcT beter leek te presteren dan mBcT.47 De resultaten van de RcT stimuleren verder onderzoek naar behande-lingsfactoren en integriteit, zowel in online toepassingen als in f2f-vormen, omdat deze de effectiviteit van (e)mBcT voor kankerpatiënten zouden kunnen vergroten.
Studiepopulatie Aangezien een eerdere studie bij kankerpatiënten aantoonde hoe moeilijk het was om patiënten met distress in poliklinische situaties te vinden,48 zochten we voor onze studie patiënten via zelfverwijzing. Patiënten werden breed geworven, via zorgverleners in aangesloten ziekenhuizen, via online en offline media, patiënten-verenigingen en collega-patiënten. We zijn ons ervan bewust dat opeenvolgende steekproeven (verder genoemd: consecutive sampling) bij RcT’s in het algemeen als eerste keuze wordt beschouwd omdat het steekproefvertekening (bias) ver-mindert.49 Bij kankerpatiënten betekent de aanwezigheid van distress echter niet noodzakelijkerwijs dat men ook geïnteresseerd zijn in hulp.50-52 De impliciete veronderstelling binnen consecutive sampling dat alle patiënten baat kunnen hebben bij een interventie, is dus mogelijk niet geldig voor psycho-oncologische interventies.53 Veel kankerpatiënten weigeren hulp ondanks het feit dat ze last van psychische problemen hebben. Patiënten voelen zich beschaamd of geven er de voorkeur aan om het alleen te doen, zelfs patiënten met veel psychische proble-men.54 Dit wordt ook weerspiegeld in het feit dat slechts 14% van de patiënten met distress bereid is met hun behandelaar te praten over hun psychische problemen53 en dat professionals, werkzaam binnen de oncologie, problemen bij minder dan 30% van de patiënten met distress herkennen.18, 55 Enerzijds zijn dus misschien niet alle patiënten die worden uitgenodigd voor een psycho-oncologische interventie door consecutive sampling interessant. Anderzijds zullen niet alle geïnteresseerde patiënten worden gevonden door consecutive sampling in een polikliniek oncologie. Het voordeel van een patiëntgerichte wervingsprocedure is dat deze resulteerde in

165
een steekproef van patiënten die zowel psychische problemen rapporteerden als geïnteresseerd waren in psychologische hulp. De meerderheid van de patiënten in onze steekproef waren echter borstkankerpatiënten van middelbare leeftijd. Hoewel dit in overeenstemming is met de kenmerken van andere kankerpatiënten die psychosociale ondersteuning zoeken,56 kan dit een beperking zijn in termen van de generaliseerbaarheid van onze resultaten.
Beoordeling van het behandelresultaat Een andere kracht van de trial is dat we een breed scala aan uitkomstmaten gebruikt hebben, waaronder interviews en vragenlijsten voor zelfrapportage. Onze primaire uitkomst, psychologische distress, werd gemeten met een vragenlijst, de Hospital Anxiety and Depression Scale (HADS57). Hoewel de HADS oorspronkelijk werd ontwikkeld als een screeninginstrument in ziekenhuizen, heeft eerder onderzoek aangetoond dat de totale score gevoelig genoeg is om de algemene symptoom-verandering te identificeren.58, 59 Een statistisch significante verandering is echter niet identiek aan een klinisch betrouwbare verandering. Om te meten of de sta-tistische verandering die we hebben gevonden van klinische relevantie is, hebben we de Reliable Change Index (RcI) berekend.60 We stelden vast dat het percentage patiënten dat klinisch betrouwbare verbetering vertoonde significant groter was in (e)mBcT (36% in mBcT en 37% in emBcT ) dan TAu (14%). Daarnaast hebben we psychiatrische diagnoses beoordeeld met behulp van het Structured-Clini-cal-Interview for DSm-IV-TR Axis-I Disorders (ScID-I61). Verbetering van het aantal psychiatrische diagnoses was gelijk bij beide interventies in vergelijking met TAu (32% in mBcT en 29% in emBcT versus 16% in TAu). Deze effectgroottes zijn in lijn met andere beschikbare psychologische interventies bij kankerpatiënten.62 Onze conclusie dat (e)mBcT een effectieve en levensvatbare optie voor psychologische behandeling in de oncologie is, wordt ook ondersteund door de resultaten van twee zeer recente meta-analyses over de effectiviteit van mBI’s voor psychologische en fysieke problemen bij kankerpatiënten.63, 64
inhoudeli jke overwegingenTherapeutcompetentie
Onze studie was de eerste studie waarin de competentie van de therapeut werd onderzocht als voorspeller van de uitkomst bij mBcT in de populatie van kanker-patiënten. Onze bevindingen toonden aan dat de competentie van de therapeut niet gerelateerd was aan de uitkomst in mBcT voor kankerpatiënten, wat in lijn was met een eerdere studie naar competentie als voorspeller van de uitkomst in mBcT bij patiënten met recidiverende depressie.37 Een verklaring zou kunnen zijn dat alle therapeuten op zijn minst op basisniveau werkten, omdat ze allemaal voldeden aan de geavanceerde criteria van de VmBN (Vereniging voor Mindfulness-Based
ned
erland
se saMen
vatting

166
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Trainers in Nederland en Vlaanderen). Hoewel er een scala aan competentieniveaus was, werd geen van de therapeuten beoordeeld als incompetent of gevorderd op de Mindfulness-Based Interventions Teaching Assessment Criteria (mBI:TAc65). Een tweede verklaring voor het gebrek aan verband tussen competentie en behandeluit-komst betreft het instrument dat we in onze studie hebben gebruikt, de mBI:TAc. De mBI:TAc is de meest gebruikte tool die is ontwikkeld om mindfulness-based competentie te beoordelen. Een van de problemen bij het onderzoeken van de competentie van de therapeut als voorspeller van de uitkomst bij mBcT, is dat het niet eenvoudig is om competentie adequaat te meten. Allereerst in bij onze studie de algehele inter-rater reliability (IRR) lager (0,7) dan in de validatiestudie van de mBI:TAc.65 Ten tweede is de mBI:TAc ontwikkeld in een Britse context en mogelijk gevoelig voor de culturele uitingen van het onderwijzen van mindfulness in het Verenigd Koninkrijk en niet noodzakelijkerwijs die van andere landen. Tijdens workshops over het toepassen van de mBI:TAc kregen Nederlandse onderzoekers bijvoorbeeld de indruk dat Nederlandse beoordelaars de neiging hadden strenger en kritischer te zijn dan hun Britse collega’s. Het is dus mogelijk dat de mBI:TAc aanpassingen nodig heeft om de gevoeligheid ervan voor andere culturele uitingen van het onderricht in mindfulness te vergroten.66, 67 Daarnaast zijn er enkele prak-tische zaken ter overweging. De mBI:TAc wordt gebruikt door intensief getrainde beoordelaars, die ook ervaring hebben met het onderwijzen van mindfulness. Dit maakt de toepassing van de schaal in een onderzoeks-setting vrij complex, tijdro-vend en duur. En zelfs voor ervaren beoordelaars geeft een geselecteerde deel van opgenomen sessies niet altijd een volledig beeld van de competentie en vaardig-heden van de therapeut. Om een breder beeld te krijgen van de competentie van de therapeut kan het nuttig zijn om verschillende perspectieven, zoals de eigen reflecties van de therapeut en het perspectief van de patiënt, te combineren met observaties van de beoordelaar.66 Verder onderzoek zal zich ook kunnen gaan richten op het aanpassen van de competentiebeoordeling aan andere uitvoeringsvormen. In dit eHealth-tijdperk zal bijvoorbeeld meer aandacht moeten worden besteed aan het meten van de competentie van de therapeut in online mBI’s. Voor dit doel kan het zeer nuttig zijn om een taalkundige analyse te gebruiken van schriftelijke feedback en online chats tussen therapeut en patiënten.
Therapeutische alliantieIn een therapie brengen zowel therapeut als patiënten hun verwachtingen mee. Hoewel de verwachtingen van de therapeut voornamelijk zijn gebaseerd op de behandelmethode die ze gebruiken, zijn de verwachtingen van de patiënt voor-namelijk gebaseerd op eigen persoonlijke doelen.68 Een goede alliantie betekent dat patiënt en therapeut goed werken aan de gemeenschappelijke doelen van de therapie. In onze studies hebben we vastgesteld dat therapeutische alliantie zoals

167
beoordeeld met de WAI gerelateerd is aan de uitkomst in zowel mBcT als emBcT.69 In onze studie naar mBcT in groepsverband vonden we dat de uitkomst voorna-melijk verband hield met het stellen van duidelijke doelen.70 Bovendien hebben we in onze studie waarin mBcT en emBcT werden vergeleken, vastgesteld dat een zwakkere vroege therapeutische alliantie een slechtere uitkomst voorspelde na de behandeling in groeps-mBcT, maar niet in emBcT.69 In tegenstelling tot onze verwachtingen leek therapeutische alliantie geen verband te houden met uitval.69, 71 Veel patiënten die al afhaakten na de eerste sessie verklaarden echter wel dat ze ‘andere verwachtingen’ hadden van de behandeling. Wat verwachtingsmanagement betreft, is het belangrijk dat therapeuten de motivering achter de behandeling in een vroeg stadium van de therapie duidelijk uitleggen en zorgen dat patiënten in (e)mBcT dit ook begrijpen. Therapeuten moeten zich vooral bewust zijn van dit gedeelde begrip in groepssituaties, omdat een zwakkere alliantie geassocieerd wordt met een slechtere uitkomst. Muran en Barber (2011) benadrukken het belang van ‘een vliegende start maken’ in kortdu-rende groepstherapie, dat wil zeggen al in het begin van de therapie een sterke alliantie tot stand brengen.68
Een subgroep patiënten kan moeite hebben met het opbouwen van een thera-peutische relatie, bijvoorbeeld vanwege bepaalde karaktertrekken. In die gevallen kunnen therapeuten de vorming van een sterke (herstelde) alliantie vergemakke-lijken door modellering.72 Er is aangetoond dat dit tot een beter resultaat leidt.72,
73 Daarom moeten mindfulness-therapeuten zich bewust zijn van hun vermogen en verantwoordelijkheid om mindfulness effectief te modelleren en te doceren.74 In dit licht moeten ze zich ook bewust zijn van hun eigen (tegen)overdrachtsver-schijnselen. In hun aanbeveling voor mindfulness-therapeuten waarschuwen Shonin et al (2014) voor negatieve overdrachtsverschijnselen bij het onderwijzen van mBI’s.75 Niet passende persoonlijke stijlen van therapeuten75 of een te niet-re-actieve houding76 wordt niet noodzakelijkerwijs door patiënten als positief ervaren en kan van invloed zijn op de waargenomen therapeutische alliantie vanuit het perspectief van de patiënt. Met betrekking tot emBcT: het onderzoek naar de therapeutische alliantie bij online interventies is nog steeds schaars. Er zijn geen eerdere studies gepubli-ceerd over het verband tussen therapeutische alliantie en uitkomst bij emBI’s voor kankerpatiënten. Het opbouwen van de therapeutische alliantie kan zich anders ontwikkelen, met name in die behandelvormen die een groot deel van hun behandelingsinhoud leveren via online zelfhulpmaterialen. Hoewel meestal door de patiënt beoordeelde alliantiematen worden gebruikt, kan de therapeutische alliantie ook worden gemeten met door de therapeut beoordeelde alliantie-maten, zoals de therapeutversie van de WAI . Door de therapeut beoordeelde alliantie kan aanvullend inzicht geven in het opbouwen van een therapeutische alliantie
ned
erland
se saMen
vatting

168
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
in online of blended interventies met beperkte feedback van de therapeut.77, 78 Tot op heden is de relatie tussen therapeutische alliantie en de uitkomst van online psychologische interventies nog erg weinig onderzocht en zijn de zeer beperkte bevindingen niet eenduidig.79
Kennis over de therapeutische alliantie en therapietrouw kan eveneens belang-rijk zijn voor de definiëring van het optimale niveau van therapeutondersteuning bij online interventies.79 Zowel door de patiënt als door de therapeut beoordeelde vragenlijsten zullen in toekomstige studies kunnen worden meegewogen, inclusief het meten van de interactie van patiënten met de online inhoud van interventies, de ‘digitale alliantie’, ongeacht de therapeut. Onderzoek naar (digitale) alliantie en therapietrouw in emBcT moet zowel het behandelresultaat als mogelijke uitval omvatten. Kennis over de aard van de therapeutische alliantie en de specifieke rol van de alliantie in (e)mBcT kan de effectiviteit van (e)mBcT vergroten. Het uitvoeren van routinematige metingen van therapeutische alliantie na elke sessie binnen (e)mBcT kan informatief zijn. Dit kan therapeuten aanmoedigen om hun therapie, hun therapeutische houding en de communicatie met patiënten in een vroeg stadium van de behandeling aan te passen en zo de behandelingsresultaten van (e)mBcT voor kankerpatiënten te verbeteren. Het verzamelen van wekelijkse indicatoren van zowel therapeutische alliantie als symptoomverandering in een onderzoeks-setting zou het ook mogelijk maken therapeutische alliantie als een mogelijk werkzame factor in zichzelf verder te onderzoeken.
groepscohesieIn groepssituaties zijn er naast de therapeut en de patiënt twee extra partijen aanwezig: de andere patiënten en de groep als geheel.68 Cohesie van een groep wordt vaak geconceptualiseerd als de ‘wij-heid’ die wordt gevoeld onder groeps-leden: de intimiteit, wederkerigheid en emotionele openheid die wordt ervaren onder groepsleden37 en die bijdraagt aan de samenwerking binnen de groep om een gemeenschappelijk therapeutisch doel te bereiken.80 Cohesie is een complexe structuur waarbij allianties van lid tot lid, lid tot groep, lid tot leider, leider tot leider en leider tot mede-leider zijn ingebed in verschillende dimensies, rekening houdend met de structuur en de kwaliteit van de relaties.81, 82 Een probleem in het wetenschappelijk onderzoek naar groepscohesie is dat er een gebrek is aan duidelijkheid en consistentie bij zowel meting als conceptualisatie van cohesie.83 Er is ‘weinig cohesie in de cohesieliteratuur’.84
Onze bevindingen lieten in lijn meer eerdere bevindingen zien dat een hoger totaalniveau van groepscohesie geen betere behandelingsresultaten voorspelde bij mBcT voor kankerpatiënten.85 Bovendien zagen we dat therapeutcompetentie verband leek te houden met lager totaalniveau van groepscohesie. Een verklaring

169
voor deze laatste bevinding kan zijn dat de zelf-beoordeelde GcQ zich vooral richt op sociaal-emotionele aspecten die onder groepsleden worden gevoeld binnen de groep als geheel, terwijl de door de waarnemer beoordeelde mBI:TAc relationele vaardigheden verwijzen naar vaardigheden in het beheren van een leeromgeving in groepsverband, zoals het omgaan met kwesties als basisregels, grenzen en vertrouwelijkheid, en leiderschapsstijl. Het is mogelijk dat hoe meer ervaring de mBcT-therapeut heeft in het omgaan met een leeromgeving in groepsverband, hoe minder patiënten afhankelijk zijn van hun mede-deelnemers voor ondersteu-ning. Een andere verklaring zou kunnen zijn dat minder competente therapeuten meer ruimte laten voor de toevallige uitwisseling van individuele ervaringen die de cohesie van de groep verbeteren. Voor zover wij weten, zijn er geen eerdere kwantitatieve studies over de impact van groepscohesie bij mBI’s, noch bij kan-kerpatiënten noch in andere situaties. Eerdere kwalitatieve studies toonden echter aan dat groepsgebaseerde situaties in mBI’s van toegevoegde waarde lijken te zijn voor kankerpatiënten wat betreft thema’s als zich verbonden en geaccepteerd voelen en vertrouwen ervaren.76, 86 Bovendien ervaart men dat ondersteuning door lotgenoten het leerproces vergemakkelijkt, zoals het erkennen van emoties en het verkrijgen van verschillende perspectieven in mBSR.87
Alvorens nieuwe studies uit te voeren naar de mogelijke rol van groepscohesie in de resultaten van psychotherapiestudies, waaronder (e)mBcT, kan het nodig zijn een bredere consensus te bereiken over zowel de definitie als de beoordeling van groepscohesie. Wat de klinische implicaties van bovenstaande bevindingen betreft, is gesuggereerd dat voorafgaande training in groepswerkvaardigheden en het leren omgaan met reactiviteit in een groep waardevol is voor het onderwijzen van mindfulness.88
tiMingTen slotte vonden we dat deelname aan mBSR zowel tijdens als na de behandeling tegen kanker kankerpatiënten hielp bij het omgaan met (aan kanker gerelateerde) mentale last. Ongeacht het stadium van de behandeling van kanker, leek de juiste timing van deelname ook afhankelijk te zijn van het stadium van emotionele ver-werking. Patiënten benadrukten dat het belangrijk is om in een vroeg stadium te worden geïnformeerd over de mogelijkheid om deel te nemen aan mBSR, omdat dit patiënten in staat stelt zelf te beslissen of en wanneer zij zich willen inschrij-ven. Helaas weten we niet of de timing van de interventie mogelijk een rol heeft gespeeld bij het vroegtijdig stoppen met de interventie, omdat we onvoldoende informatie hebben verzameld over patiënten die de interventie hebben stopgezet. De kwalitatieve bevindingen over de timing van mBSR hebben extra waarde en klinische relevantie omdat ze het belang van de autonomie van patiënten tij-dens en na de behandeling tegen kanker benadrukken. Deze bevindingen zijn
ned
erland
se saMen
vatting

170
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
in overeenstemming met het steeds meer erkende begrip van gepersonaliseerde geneeskunde met gedeelde besluitvorming als sleutelfunctie. Gedeelde besluit-vorming betekent dat een arts en een patiënt behandelingsopties bespreken om de behandelingsoptie te bepalen die het beste past. In dit model moet een arts de patiënt uitnodigen om als team samen te werken en een keuze tussen opties te maken en moet de arts de juiste informatie over de opties verstrekken.89 Een arts moet ook met de patiënt overleggen om diens voorkeur duidelijk te krijgen en uiteindelijk samen een behandelingsbeslissing te nemen.90, 91 Hoewel wordt erkend dat gedeelde besluitvorming bijdraagt aan de kennis van patiënten over de behan-deling en de tevredenheid met de genomen beslissing,92 wordt het essentiële deel van het proces, het duidelijk krijgen van voorkeuren van de individuele patiënt en een gedeeld begrip vaak gehaast doorlopen. Artsen beginnen relatief snel met het aanbieden van hun eigen mening over aangeboden keuzes en behandelingsopties.91 Een recent kwalitatief onderzoek in een steekproef van borstkankerpatiënten die geopereerd moesten gaan worden heeft eveneens aangetoond dat artsen die patiënten begeleiden bij hun keuze tussen een borstamputatie of borstsparende operatie en radiotherapie zich vooral richten op de keuzes en opties, terwijl ze de voorkeuren en gezamenlijke behandelingsbeslissing verwaarlozen.92
Met betrekking tot mBI’s is de algemene veronderstelling binnen de medische en psycho-oncologische hulpverlening dat psychologische interventies moeten worden aangeboden na de behandelingsfase tegen kanker, niet in lijn met de resultaten van onze studie. Patiënten benadrukken dat ze in een vroeg stadium willen worden geïnformeerd. Het werkt autonomie bevorderend. Bovendien stelt gedeelde besluit-vorming hen in staat, na goed geïnformeerd te zijn en na het bespreken van voor-keuren, zelf te kiezen of, en zo ja op welk moment, ze willen deelnemen aan mBI’s.
klinische iMplicatiesVanuit klinisch perspectief en in overeenstemming met de Nederlandse oncologi-sche richtlijnen moet een grotere toegankelijkheid van evidence-based interventies en behandelingsprogramma’s prioriteit krijgen. Er zijn verschillende evidence-ba-sed f2f psychologische interventies,93-97 blended en online therapiebenaderingen voor patiënten met psychologische distress beschikbaar. Er zijn ook specifieke interventies voor patiënten met distress in palliatieve zorg.98 We hebben aange-toond dat (e)mBcT een waardevolle aanvulling is op de therapeutische opties voor kankerpatiënten met distress. Bovendien heeft onze follow-upstudie aangetoond (niet in dit proefschrift) dat de vermindering van psychologische distress en ver-betering van positieve geestelijke gezondheid en kwaliteit van leven bij langdurige follow-up gehandhaafd blijft.47 Tevens hebben we vastgesteld dat beide interventies ook kosteneffectief lijken in vergelijking met TAu (niet in dit proefschrift).99
Er zijn echter nog veel obstakels te overwinnen bij de implementatie van effectieve

171
interventies, zoals (e)mBcT, zowel vanuit het perspectief van zorgverleners als van patiënten. Duidelijk aangegeven doelen, cyclische evaluatie en verbeteringsproces-sen kunnen de introductie van programma’s voor psychosociale zorgbehoeften voor kankerpatiënten in de klinische praktijk aanmoedigen.110, 101 Strategieën voor het opbouwen van vaardigheden voor oncologische zorgverleners kunnen de betref-fende professionals ondersteunen om psychologische problemen van patiënten te bespreken.102 Dit kan ertoe bijdragen dat patiënten zich minder beschaamd of terughoudend voelen om hun psychische problemen aan hun arts te melden.103 Interessant is dat mBI’s voor zorgverleners bij kunnen dragen aan dit proces In kwantitatieve studies is aangetoond dat mBI’s en Acceptatie en Commitment-Thera-pie mantelzorgers104 en zorgverleners105, 106 kunnen ondersteunen bij hun dagelijkse werkzaamheden, wat kan leiden tot een toenemend vertrouwen om de psychische belasting van kanker met patiënten te bespreken. Kwalitatief onderzoek heeft laten zien dat arts-assistenten (chirurgie) een toegenomen bewustzijn rapporteerden, ook met betrekking tot hun communicatievaardigheden, en een verbeterde zelfreflectie en mededogen na het volgen van mBSR.107 De basis van kankerzorg is misschien wel het ons bewust zijn van de belangrijke taak om patiënten zo goed mogelijk bij hun lijden te begeleiden. De bevindingen van dit proefschrift zijn relevant voor de manier waarop evi-dence-based psycho-oncologische interventies worden gefinancierd. In Nederland worden evidence-based psycho-oncologische interventies alleen vergoed door zorgverzekeraars voor kankerpatiënten met een gediagnosticeerde psychiatrische stoornis. Het is de vraag of een psychiatrische stoornis al dan niet een zinvolle basis is voor het vergoeden van interventies bij kankerpatiënten. In 2018 presenteerde KWF Kankerbestrijding een Maatschappelijke Business Case aan het Ministerie van Volksgezondheid108 op basis van Meaning Centered Therapy96 en (e)mBcT als resultaat van onder meer studies uitgevoerd binnen het BeMind-onderzoeks-project. Een Maatschappelijke Business Case is een veelgebruikte methode voor het in kaart brengen van de economische en maatschappelijke voordelen van een interventie. Wij zijn het eens met het KWF dat alle mensen die aan kanker lijden of kanker overleven en die behoefte hebben aan ondersteuning toegang moeten krijgen tot de juiste zorg voor bevorderen van kwaliteit van leven. Het is nu de verantwoordelijkheid van het Ministerie van Volksgezondheid de resterende obsta-kels op te lossen om dit te bereiken, en zorgverleners te faciliteren psychosociale interventies voor kankerpatiënten breed toegankelijk te maken. We hopen dat het BeMind-onderzoeksproject zal bijdragen aan deze belangrijke ambitie.
ned
erland
se saMen
vatting

172
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Referenties
1. Bray, F., Transitions in human development and the global cancer burden. In: Wild CP, Stewart B, eds. World Cancer Report. Lyon: International Agency for Research on Cancer, 2014. World Cancer Report, 2014: p. 54-68.
2. Network, N.C.C. and N.C.C. Network, NCCN clinical practice guidelines in oncology: distress management. Avail-able at: (Accessed May 26, 2016) http://oralcancerfoundation. org/treatment/pdf/distress. pdf View in Article, 2010.
3. Carlson, L., et al., High levels of untreat-ed distress and fatigue in cancer patients. British Journal of Cancer, 2004. 90(12): p. 2297-2304.
4. Mitchell, A.J., et al., Prevalence of depres-sion, anxiety, and adjustment disorder in oncological, haematological, and pallia-tive-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncology, 2011. 12(2): p. 160-74.
5. Mitchell, A.J., et al., Depression and anxi-ety in long-term cancer survivors compared with spouses and healthy controls: a sys-tematic review and meta-analysis. Lancet Oncology, 2013. 14(8): p. 721-32.
6. Velikova, G., et al., The clinical value of quality of life assessment in oncology practice—a qualitative study of patient and physician views. Psycho-Oncology: Journal of the Psychological, Social and Behavioral Dimensions of Cancer, 2008. 17(7): p. 690-698.
7. Wu, Y.S., et al., Anxiety and depression in patients with head and neck cancer: 6-month follow-up study. Neuropsychiatric Disease Treatment, 2016. 12: p. 1029-36.
8. Thomas, S.F., et al., Anxiety in long-term cancer survivors influences the acceptability of planned discharge from follow-up. Psy-cho-Oncology, 1997. 6(3): p. 190-6.
9. Greer, J.A., et al., Behavioral and psycho-logical predictors of chemotherapy adherence in patients with advanced non-small cell lung cancer. Journal of Psychosomatic Research 2008. 65(6): p. 549-52.
10. Brown, L.F., et al., The association of depression and anxiety with health-related quality of life in cancer patients with depres-sion and/or pain. Psycho-Oncology, 2010. 19(7): p. 734-41.
11. Saevarsdottir, T., N. Fridriksdottir, and S. Gunnarsdottir, Quality of life and symptoms of anxiety and depression of patients receiving cancer chemotherapy: longitudinal study. Cancer Nurs, 2010. 33(1): p. E1-e10.
12. Weihs, K.L., et al., Negative affectivity, re-striction of emotions, and site of metastases predict mortality in recurrent breast cancer. Journal of Psychosomatic Research, 2000. 49(1): p. 59-68.
13. Pinquart, M. and P.R. Duberstein, De-pression and cancer mortality: a meta-anal-ysis. Psychological Medicine, 2010. 40(11): p. 1797-810.
14. Jansen, F., et al., Depressive symptoms in relation to overall survival in people with head and neck cancer: A longitudinal cohort study. Psycho-Oncology, 2018. 27(9): p. 2245-2256.
15. Caruso, R., et al., Psychiatric Disorders Related to Cancer: Prevalence, Etiology, and Recognition. Neuropathological Diseases, 2012. 1(1).
16. Fava, G.A., L. Mangelli, and C. Ruini, Assessment of psychological distress in the setting of medical disease. Psychotherapy and Psychosomatics, 2001. 70(4): p. 171-5.
17. Grassi, L., et al., Psychological factors affecting oncology conditions. Advanced Psychosomatic Medicine, 2007. 28: p. 57-71.
18. Kissane, D.W., Unrecognized and untreated depression in cancer care. Lancet Psychia-try, 2014. 1(5): p. 320-1.
19. Grassi, L., D. Spiegel, and M. Riba, Ad-vancing psychosocial care in cancer patients. F1000Res, 2017. 6: p. 2083.
20. Tamagawa, R., et al., Who benefits from psychosocial interventions in oncology? A systematic review of psychological moderators of treatment outcome. Journal of Behavioral Medicine, 2012. 35(6): p. 658-673.

173
21. Meyer, T.J. and M.M. Mark, Effects of psychosocial interventions with adult cancer patients: a meta-analysis of randomized experiments. Health Psychol, 1995. 14(2): p. 101-8.
22. Osborn RL, Demoncada AC, and F. M, Psychosocial interventions for depression, anxiety, and quality of life in cancer survi-vors: meta-analyses. International Journal of Psychiatry in Medicine 2006.
23. Goedendorp, M.M., et al., Psychosocial interventions for reducing fatigue during cancer treatment in adults. Cochrane Data-base of Systematic Reviews, 2009.
24. Beck, A.T., G. Emery, and R.L. Green-berg, Anxiety disorders and phobias: A cognitive perspective. 2005: Basic Books.
25. Greer, J.A., et al., Tailoring Cogni-tive-Behavioral Therapy to Treat Anxiety Comorbid with Advanced Cancer. Journal of Cognitive Psychotherapy, 2010. 24(4): p. 294-313.
26. Sun, H., et al., The Efficacy of Cognitive Behavioral Therapy to Treat Depression and Anxiety and Improve Quality of Life Among Early-Stage Breast Cancer Patients. Integrated Cancer Therapies, 2019. 18: p. 1534735419829573.
27. Luberto, C.M., et al., Theoretical Rationale and Case Illustration of Mindfulness-Based Cognitive Therapy for Fear of Cancer Recur-rence. Journal of Clinical Psychology in Medical Settings, 2019.
28. Kabat-Zinn, J., Full catastrophe living, revised edition: how to cope with stress, pain and illness using mindfulness meditation. 2013: Hachette uK.
29. Segal, Z.V., J.M.G. Williams, and J.D. Teasdale, Mindfulness-based cognitive therapy for depression: A new approach to relapse prevention. 2013, New York: Guil-ford Press.
30. Crane, R., Mindfulness-based cognitive therapy: Distinctive features. 2017: Rout-ledge.
31. Spijkerman, M.P., W.T. Pots, and E.T. Bohlmeijer, Effectiveness of online mind-fulness-based interventions in improving mental health: A review and meta-analysis
of randomised controlled trials. Clin Psy-chol Rev, 2016. 45: p. 102-14.
32. Everts, F.Z.B., M.L. van der Lee, and E. de Jager Meezenbroek, Web-based individual Mindfulness-Based Cognitive Therapy for cancer-related fatigue—A pilot study. Internet Interventions, 2015. 2(2): p. 200-213.
33. Bruggeman-Everts, F.Z., et al., Effective-ness of Two Web-Based Interventions for Chronic Cancer-Related Fatigue Compared to an Active Control Condition: Results of the ‘Fitter na kanker’ Randomized Con-trolled Trial. Journal of Medical Internet Research, 2017. 19(10): p. e336.
34. Fairburn, C.G. and Z. Cooper, Therapist competence, therapy quality, and therapist training. Behavioral Research and Thera-py, 2011. 49(6-7): p. 373-8.
35. Wise, T.N., M. Biondi, and A. Costantini, Psycho-oncology. 2013: American Psychi-atric Publications.
36. Kissane, D.W., et al., Cognitive-existential group psychotherapy for women with pri-mary breast cancer: a randomised controlled trial. Psycho-Oncology: Journal of the Psychological, Social and Behavioral Dimensions of Cancer, 2003. 12(6): p. 532-546.
37. Yalom, I.D., The theory and practice of group psychotherapy. 1995: Basic Books (AZ).
38. Waltz, J., et al., Testing the integrity of a psychotherapy protocol: assessment of adherence and competence. Journal of Consulting an Clinical Psychology, 1993. 61(4): p. 620-30.
39. Huijbers, M.J., et al., Teacher Competence in Mindfulness-Based Cognitive Therapy for Depression and Its Relation to Treatment Outcome. Mindfulness (NY), 2017. 8(4): p. 960-972.
40. Luborsky, L., Therapeutic alliances as predictors of psychotherapy outcomes: Fac-tors explaining the predictive success. The working alliance: Theory, research, and practice, 1994: p. 38-50.
41. Horvath, A.O. and B.D. Symonds, Rela-tion between working alliance and outcome
ned
erland
se saMen
vatting

174
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
in psychotherapy: A meta-analysis. Journal of Counseling Psychology, 1991. 38(2): p. 139.
42. May, A.M., et al., The effect of group cohesion on rehabilitation outcome in cancer survivors. Psycho-Oncology, 2008. 17(9): p. 917-925.
43. Cramer H, et al., Mindfulness based stress reduction for breast cancer—a systematic review and meta-analysis. Current Oncology 2012. 19(5): e343.
44. Carlson, L.E., et al., What goes up does not always come down: patterns of distress, physical and psychosocial morbidity in people with cancer over a one year period. Psycho-Oncology, 2013. 22(1): p. 168-76.
45. Dimidjian, S. and Z.V. Segal, Prospects for a clinical science of mindfulness-based intervention. American Psychology, 2015. 70(7): p. 593-620.
46. Schellekens, M.P., et al., A qualitative study on mindfulness-based stress reduction for breast cancer patients: how women experience participating with fellow patients. Support Care Cancer, 2016. 24(4): p. 1813-20.
47. Cillessen, L., et al., Consolidation and pre-diction of long-term treatment effect of group and online mindfulness-based cognitive therapy for distressed cancer patients. Acta Oncol, 2018: p. 1-10.
48. van Scheppingen, C., et al., Is imple-menting screening for distress an efficient means to recruit patients to a psychological intervention trial? Psycho-Oncology, 2014. 23(5): p. 516-523.
49. Polit, D.F. and C.T. Beck, Essentials of nursing research: Appraising evidence for nursing practice. 2010: Lippincott Wil-liams & Wilkins.
50. Thorsen, L., et al., Cancer patients’ needs for rehabilitation services. Acta Oncol, 2011. 50(2): p. 212-22.
51. Clover K.A., et al., Why do oncology outpa-tients who report emotional distress decline help? Psycho-Oncology 2014.
52. Garssen, B. and M. Van der Lee, Re: Screening for emotional distress in cancer patients: a systematic review of assessment
instruments. J Natl Cancer Inst, 2010. 102(7): p. 506-8; author reply 508.
53. Thewes, B., et al., One way or another: The opportunities and pitfalls of self-referral and consecutive sampling as recruitment strategies for psycho-oncology intervention trials. Psycho-Oncology, 2018. 27(8): p. 2056-2059.
54. Tuinman, M.A., S.M. Gazendam-Donof-rio, and J.E. Hoekstra-Weebers, Screening and referral for psychosocial distress in onco-logic practice: use of the Distress Thermome-ter. Cancer, 2008. 113(4): p. 870-8.
55. Grassi, L., et al., Psychological factors affecting oncology conditions. Adv Psycho-som Med, 2007. 28: p. 57-71.
56. Garssen, B., et al., Characteristics of patients in routine psycho-oncological care, and changes in outcome variables during and after their treatment. Psychology & health, 2016. 31(10): p. 1237-1254.
57. Zigmond, A.S. and R.P. Snaith, The hospital anxiety and depression scale. Acta Psychiatr Scand, 1983. 67(6): p. 361-70.
58. Mitchell, A.J., N. Meader, and P. Sy-monds, Diagnostic validity of the Hospital Anxiety and Depression Scale (HADS) in cancer and palliative settings: A meta-anal-ysis. Journal of Affective Disorders, 2010. 126(3): p. 335-348.
59. Roberts, M.H., R.B. Fletcher, and P.L. Merrick, The validity and clinical utility of the Hospital Anxiety and Depression Scale (HADS) with older adult New Zealanders. International Psychogeriatrics, 2014. 26(2): p. 325-333.
60. Jacobson, N.S. and P. Truax, Clinical significance: a statistical approach to de-fining meaningful change in psychotherapy research. Journal Consulting and Clinical Psychology, 1991. 59(1): p. 12-19.
61. First, M.B., et al., Structured Clinical Interview for DSm-IV® Axis I Disorders (ScID-I), Clinician Version, Administra-tion Booklet. 2012: American Psychiatric Pub.
62. Faller, H., et al., Effects of psycho-oncologic interventions on emotional distress and quality of life in adult patients with cancer:

175
systematic review and meta-analysis. Jour-nal of Clinical Oncology, 2013: p. JCO. 2011.40. 8922.
63. Zhang, Q., H. Zhao, and Y. Zheng, Effectiveness of mindfulness-based stress reduction (mbSR) on symptom variables and health-related quality of life in breast cancer patients – a systematic review and me-ta-analysis. Supportive Care in Cancer, 2019. 27(3): p. 771-781.
64. L. Cillessen et al., Mindfulness-based interventions for psychological and physical health outcomes in cancer patients and -survivors: a meta-analysis of randomized controlled trials. Under review.
65. Crane RS, K.W., Williams JMG, Hastings RP, Cooper L, Fennell MJV, Competence in teaching mindfulness-based courses: concepts, development and assessment. Mindfulness 2012.
66. Crane, R.S. and W. Kuyken, The Mind-fulness-Based Interventions: Teaching As-sessment Criteria (mbI:TAc): reflections on implementation and development. Current Opinion Psychology, 2018. 28: p. 6-10.
67. Crane, R., Mindfulness-based cognitive therapy: Distinctive features. 2017: Rout-ledge.
68. Muran, J.C. and J.P. Barber, The thera-peutic alliance: An evidence-based guide to practice. 2011: Guilford Press.
69. Bisseling et al., The development and association of therapeutic alliance with out-come of internet-based Mindfulness-Based Cognitive Therapy compared to group-based mbcT for distressed cancer patients: a sec-ondary analysis of a multicenter randomized controlled trial. Journal of Medical Inter-net Research (2019): doi: 10.2196/14065
70. Bisseling, E.M., et al., Therapeutic alliance -not therapist competence or group cohesion- contributes to reduction of psychological distress in group-based Mindfulness-Based Cognitive Therapy for cancer patients. Clin Psychol Psychotherapy, 2019.
71. Compen, F., et al., Face-to-Face and In-ternet-Based Mindfulness-Based Cognitive Therapy Compared With Treatment as Usual in Reducing Psychological Distress
in Patients With Cancer: A Multicenter Randomized Controlled Trial. Journal of Clinical Oncology, 2018: p. 31(25): p. 3119-3126.
72. Tsai, M., R.J. Kohlenberg, and J.W. Kanter, A functional analytic psycho-therapy (fAP) approach to the therapeutic alliance. The therapeutic alliance: An evidence-based guide to practice, 2010: p. 172-190.
73. Zilcha-Mano, S. and P. Errazuriz, Early development of mechanisms of change as a predictor of subsequent change and treat-ment outcome: The case of working alliance. J Consult Clinical Psychology, 2017. 85(5): p. 508-520.
74. Piet, J., L. Fjorback, and S. Santorelli, What Is Required to Teach Mindfulness Ef-fectively in mbSR and mbcT?, in Mindful-ness and Buddhist-Derived Approaches in Mental Health and Addiction, E. Sho-nin, W.V. Gordon, and M.D. Griffiths, Editors. 2016, Springer International Publishing: Cham. p. 61-83.
75. Shonin, E. and W. Van Gordon, Practical recommendations for teaching mindfulness effectively. Mindfulness, 2015. 6(4): p. 952-955.
76. van Aalderen, J.R., et al., The Role of the Teacher in Mindfulness-Based Approaches: A Qualitative Study. Mindfulness, 2014. 5(2): p. 170-178.
77. Preschl, B., A. Maercker, and B. Wagner, The working alliance in a randomized controlled trial comparing online with face-to-face cognitive-behavioral therapy for depression. Bmc Psychiatry, 2011. 11: p. 189.
78. Vernmark, K., et al., Working alliance as a predictor of change in depression during blended cognitive behaviour therapy. Cogni-tive Behavavioral Therapy, 2018: p. 1-15.
79. Pihlaja, S., et al., Therapeutic alliance in guid-ed internet therapy programs for depression and anxiety disorders - A systematic review. Internet Interventions, 2018. 11: p. 1-10.
80. Budman, S.H., et al., Cohesion, alliance and outcome in group psychotherapy. Psy-chiatry, 1989. 52(3): p. 339-50.
ned
erland
se saMen
vatting

176
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
81. Burlingame, G.M., D.T. McClendon, and J. Alonso, Cohesion in group therapy. Psychotherapy, 2011. 48(1): p. 34.
82. Schnur, J.B. and G.H. Montgomery, A systematic review of therapeutic alliance, group cohesion, empathy, and goal con-sensus/collaboration in psychotherapeutic interventions in cancer: Uncommon factors? Clinical Psychology Review, 2010. 30(2): p. 238-247.
83. Hornsey, M.J., L. Dwyer, and T.P. Oei, Beyond cohesiveness: Reconceptualizing the link between group processes and outcomes in group psychotherapy. Small Group Research, 2007. 38(5): p. 567-592.
84. Joyce, A.S., W.E. Piper, and J.S. Ogrod-niczuk, Therapeutic alliance and cohesion variables as predictors of outcome in short–term group psychotherapy. International Journal of Group Psychotherapy, 2007. 57(3): p. 269-296.
85. May, A.M., et al., The effect of group cohesion on rehabilitation outcome in cancer survivors. Psycho-Oncology, 2008. 17(9): p. 917-25.
86. Mackenzie, M.J., et al., A qualitative study of self-perceived effects of mindfulness-based stress reduction (mbSR) in a psychosocial oncology setting. Stress and Health, 2007. 23(1): p. 59-69.
87. Schellekens, M.P.J. et al., A qualitative study on mindfulness-based stress reduction for breast cancer patients: how women experience participating with fellow patients. Support Care Cancer, 2016. 24: p. 1813-1820
88. McCown, D., D. Reibel, and M.S. Mi-cozzi, Teaching mindfulness. A practical guide for clinicians and educators. uS: Springer, 2010.
89. Elwyn, G., et al., A three-talk model for shared decision making: multistage consul-tation process. British Medical Journal, 2017. 359: p. j4891.
90. Elwyn, G., et al., Using a ‘talk’model of shared decision making to propose an obser-vation-based measure: Observer OPTION5 Item. Patient education and counseling, 2013. 93(2): p. 265-271.
91. Barry, M.J. and S. Edgman-Levitan, Shared decision making—the pinnacle of patient-centered care. New England Jour-nal of Medicine, 2012. 366(9): p. 780-781.
92. Savelberg, W., et al., Does lack of deeper understanding of shared decision making explains the suboptimal performance on crucial parts of it? An example from breast cancer care. European Journal of Oncolo-gy Nursing, 2019. 38: p. 92-97.
93. Smith, A., et al., Pilot of a theoretically grounded psychologist-delivered intervention for fear of cancer recurrence (Conquer Fear). Psycho-Oncology, 2015. 24(8): p. 967-70.
94. Herschbach, P., et al., Evaluation of two group therapies to reduce fear of progression in cancer patients. Supportive Care in Cancer, 2010. 18(4): p. 471-9.
95. Butow, P.N., et al., Randomized Trial of ConquerFear: A Novel, Theoretically Based Psychosocial Intervention for Fear of Cancer Recurrence. Journal of Clinical Oncology, 2017: p. Jco2017731257.
96. van der Spek, N., et al., Efficacy of mean-ing-centered group psychotherapy for cancer survivors: a randomized controlled trial. Psychological Medicine, 2017. 47(11): p. 1990-2001.
97. van de Wal, M., et al., Efficacy of Blended Cognitive Behavior Therapy for High Fear of Recurrence in Breast, Prostate, and Col-orectal Cancer Survivors: The SWORD Study, a Randomized Controlled Trial. Journal of Clinical Oncology, 2017. 35(19): p. 2173-2183.
98. Rodin, G., et al., Managing Cancer and Living Meaningfully (cALm): A Random-ized Controlled Trial of a Psychological Intervention for Patients With Advanced Cancer. Journal of Clinical Oncology, 2018. 36(23): p. 2422-2432.
99. Compen F.R. et al., Cost-utility of individual internet-based and face-to-face Mindfulness-Based Cognitive Therapy compared to Treatment As Usual in reducing psychological distress in cancer patients. Under review.
100. Dudgeon, D., et al., Cancer Care Ontario’s experience with implementation of routine

177
physical and psychological symptom distress screening. Psycho-Oncology, 2012. 21(4): p. 357-64.
101. Riblet, N., et al., Addressing distress in pa-tients with head and neck cancers: a mental health quality improvement project. J Na-tional Comprehensive Cancer Network, 2014. 12(7): p. 1005-1013.
102. van der Hout, A., et al., Efficacy, cost-utili-ty and reach of an eHealth self-management application ‘Oncokompas’ that helps cancer survivors to obtain optimal supportive care: study protocol for a randomised controlled trial. Trials, 2017. 18(1): p. 228.
103. Valente, S.M., J.M. Saunders, and M.Z. Cohen, Evaluating depression among pa-tients with cancer. Cancer Practises, 1994. 2(1): p. 65-71.
104. Buter, M., Mindfulness voor mantelzorgers; een tijdelijk succes of winst op lange termijn? Psychology, 2014. 6(5): p. 413-423.
105. Rudaz, M., et al., Mindfulness and acceptance-based trainings for fostering self-care and reducing stress in mental health professionals: A systematic review. Journal of Contextual Behavioral Science, 2017. 6(4): p. 380-390.
106. Verweij, H., et al., Mindfulness-based stress reduction for residents: A randomized con-trolled trial. Journal of General Internal Medicine, 2018: p. 1-8.
107. Verweij, H., et al., Does mindfulness train-ing enhance the professional development of residents? A qualitative study. Academic Medicine, 2018. 93(9): p. 1335-1340.
108. Maatschappelijk Business Case. Inter-venties gericht op vermindering van angstige en depressieve gevoelens bij mensen met kanker, 2018. Sinzer en KWF Kankerbe-strijding.
ned
erland
se saMen
vatting

178
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Dankwoord
Toen ik in 2013 vlak na mijn 40e verjaardag aan vrienden, collega’s en familie ver-telde dat ik mijn inmiddels stevig verworven positie als psychiater zou inruilen voor een promotie traject, nota bene af te ronden in 4 jaar met een aanstelling van 0.3fte, vroeg men zich af of ik niet in een midlifecrisis beland was. Met de kennis van nu kan ik ze geen ongelijk geven. Het werden er 6, waarbij ik mijn werkzaamheden voor dit proefschrift in de laatste 2 jaar voornamelijk tussen eten, afwas en ochtendgloren verrichtte. Wat een traject! Het college voor zorgverzekeraars gaf vlak na onze start een negatief advies over vergoeding van mindfulness voor psychische problemen. Wij hadden daar als onderzoeksgroep behoorlijk mentale last van, maar vonden echter snel een groep behandelaren bereid, mindfulness trainers van het eerste uur, om onze interventies onbezoldigd te begeleiden. Hier ben ik hen (en ik spreek ook namens Félix) tot op de dag van vandaag zeer dankbaar voor. Zonder deze trainers was dit onderzoek in de aanvangsfase al een stille dood gestorven. Rinie (!), Ellen, Stephanie, Janine, Maya, Annetje, Coen, Joyce, Bert, Lot, Maria, Mira, Ineke en Marije ontzettend bedankt voor jullie inzet en begeleiding van de patiënten die deelnamen aan ons onderzoek. Onze participerende patiënten wil ik in eenzelfde adem bedanken voor hun bereidheid tot deelname. Jullie bleven, ondanks alles wat ziekte aan zorg met zich meebrengt, bereid om ons tot een jaar na het volgen van een training te woord te staan en vragenlijsten in te vullen. Zonder Pink Ribbon was het gehele BeMind project überhaupt niet mogelijk geweest. Dank voor de financiële steun en het grote vertrouwen in dit project. Dank ook aan Karify, Roparun en de Hetty Odink Stichting voor jullie bijdragen en inzet ten behoeve van dit project.
Ik wil, hoewel wat ongebruikelijk, heel graag Félix vervolgens als eerste ‘persoonlijk’ bedanken, mijn maatje en makker in dit project. Ik ben je bijzonder dankbaar voor onze samenwerking. Wat hebben we samen sterk gestaan binnen het stormachtige BeMind en wat zijn we toch lekker complementair aan elkaar. Ik lig vaak dubbel om jouw grote mate van no-nonsense serieus-zijn, wat een heerlijke combinatie! En zonder jouw wat obsessieve precisie was dit onderzoek op de grote lijnen blij-ven steken. Ook ben ik je zeer dankbaar voor de zomer van 2016 waarin jij voor twee gewerkt hebt in een periode waarin ik uitgeschakeld was. Jij bent een van de weinigen aan wie ik destijds schaamteloos foto’s durfde toe te sturen en dat zegt iets over jouw oprechtheid en je eerlijkheid, en onze wederzijdse betrokkenheid. Ik ben zo trots op je keuze (zonder twijfel geënthousiasmeerd door de vele BeMind ScIDS) om óók als clinicus te gaan werken. Het maakt je als onderzoeker nog krachtiger (en je bent al meer dan goed) en het geeft net wat meer sjeu, is het niet?

179
dan
kwo
ord
En het moet niet gekker worden maar je werkt inmiddels ook als mindfulness trainer! Had jij dat in 2013 kunnen voorspellen?
En dan natuurlijk mijn begeleiders. Anne, promotor van dit project, en in bredere zin ook van de ontwikkeling van mij als professional, sinds 2010, het jaar waarin ik startte met mijn opleiding tot mindfulness trainer. Ik ben je zeer dankbaar voor de mogelijkheden die je mij geboden hebt. En denk soms met angst en beven terug hoe jouw kritische geest feilloos aanhaakt(e) in die van mij. Of dit een remmende of stimulerende factor geweest is kan ik nog steeds niet zeggen. Maar feit is wel dat er binnen 6 jaar, met alles wat er ook was, een proefschrift ligt, naar beider tevredenheid. Een proef-schrift waarvan ik om twee voor twaalf toch nog besloot dat het een heel andere invulling zou moeten krijgen dan ik 5 jaar lang voor ogen had gehad. Wat jij – en dát weet ik zeker – in een veel eerder stadium al had gezien. Marije, copromotor, jij bracht rust in de drukte, als een baken in een zee. Ik waardeer je erg, als collega binnen het HDI, als onderzoeker en als mens. Met een aangename mate van gelijkmoedigheid, vriendelijkheid en ruimte voor overleg, liet jij me vallen en opstaan en mijn weg vinden in de jungle van onderzoek. Jouw optimisme en vertrouwen zijn eigenschappen waar ik van kan leren. Ik wil je bedanken voor je begeleiding deze jaren. Melanie, jij werd als tweede copromotor toegevoegd, om de kloof tussen Nij-megen en Bilthoven wat te overbruggen en mij vanuit Nijmegen te ondersteunen. Onze samenwerking was kort maar krachtig zal ik maar zeggen. Jij bleek vlak na deze aanstelling bij Marije in het HDI te gaan werken. Ik ben je dankbaar voor je ondersteuning, je kritisch meedenken over de opzet van een aantal studies en het meelezen van de manuscripten. Je oog voor detail is een groot goed. Philip Spinhoven, veel dank voor je begeleiding bij twee studies. Als ware nestor bewoog je mee, stelde je gerust en stimuleerde mijn ontwikkeling. Dank ook aan overige co-auteurs binnen het BeMind project: Belinda Thewes, Eddy Adang, Linda Carlson, Linda Cillessen en Rogier Donders. En daarbuiten: Ellen Jansen, Hanneken Laarhoven en Judith Prins. En Rogier: Wat is een mensenwereld toch zonder statistiek? Leden van de manuscript commissie, te weten Hans de Wilt en Nicoline Hooger-brugge en Irma Verdonck-de Leeuw, wat fijn dat jullie mijn manuscript hebben willen beschouwen. Ik ben jullie zeer erkentelijk. Mijn opleiders van weleer, Johan Havenaar en Ralph Kupka, en ook Arjan Braam, wil ik bedanken voor de goede opleiding die ik genoten heb in het Willem Arntz Huis. Jullie zijn erg belangrijk geweest voor mijn vorming als psychiater.

180
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Alle IPSO instellingen en andere deelnemende centra wil ik bedanken: Het Behou-den Huys, het Ingeborg Douwes Centrum, de Vruchtenburg en het Jeroen Bosch Ziekenhuis (bedankt Tineke!).
Alle collega’s van het Helen Dowling Instituut en in het bijzonder Anette, Marijke en Stieneke (geen warmer welkom dan een anekdote over Rianne toen ik kwam solliciteren als PhD), Mélanie G. en Sia. En Coen, Joyce en Bert nogmaals. En natuurlijk onze onderzoekersgroep: Fieke, Marije W, Sanne en Bert G. en Eltica. Eltica wil ik eigenlijk driedubbel bedanken voor de veelheid aan ondersteuning.
Collega’s van het Radboud Centrum voor Mindfulness, Ramona, Irma, Kelly, Hanne, Mira, Lotte, Carolien, Marloes, Linda, Imke, Marleen, Ellen, Rinie, Dirk, Ineke, Wendy, Rhoda, Nicole, heel veel dank voor de fijne samenwerking. En Linda, wat mooi om met jou te sparren. Ons eerste artikel samen ging als een speer, ik kijk uit naar wat komt. Geert, dank voor het ontwerpen en verwerken van dozijnen aan Teleforms. Dank ook Merel en Melanie, voor het beoordelen en raten van de videobeelden. Dank aan David, Heidi, Eva en andere Merel voor jullie ondersteu-ning bij de data verzameling.
Collega’s van het Canisius-Wilhelmina Ziekenhuis, vakgroepmaten Erwin, Twan, Harm-Jan en Sophie. De dynamiek binnen onze vakgroep verveelt gelukkig nooit. Dank ook voor de ruimte die ik kreeg in de laatste fase, waardoor ik het proefschrift heb kunnen afronden. Team op onze PAAZ / mPu (secretariaat, arts assistenten, verpleegkundigen, voedingsmedewerkers, maatschappelijk werkenden, vak- en psychotherapeuten): Jullie zijn kanjers! En mijn oncologie psychiater club: Dit proefschrift laat weer eens zien, het wordt echt tijd om ons formeel te verenigen binnen de NVvP.
Geen boek zonder kaft. Dank lieve Jet voor je fantastische ontwerp en Bas Reijnen voor de uitwerking ervan én het vormgeven van mijn gehele proefschrift. Geen boek zonder muziek. Zonder de albums van Michiel Borstlap, die mij bij herhaling in een schrijfstaat brachten, was dit proefschrift beduidend trager tot stand gekomen. Geen boek zonder talenknobbel. Dank Gerard Scanlan voor de ondersteuning bij de Nederlandse samenvatting.
Fokko Nagengast moet ik speciaal bedanken, omdat goede dokters hun statistieken kennen, maar betere dokters weten wanneer ze deze naast zich neer moeten leg-gen. Zonder jou, Fokko, hadden Tanya en ik hier vermoedelijk niet meer gestaan.
En natuurlijk wil ik ook vrienden en bekenden bedanken, gewoon omdat jullie er

181
zijn en belangrijk voor mij zijn. Met een aantal van jullie deel ik een behoorlijke geschiedenis en voel ik me verbonden in het heden. Dat over de jaren heen contacten wisselend verlopen zijn, doet daar niets aan af. En komt niet alleen door het leven zelf, maar ook…. door simpelere zaken zoals het schrijven van een proefschrift. Arleen (ik hou gewoon ontzettend veel van jou), Géraud (in een volgend leven gaan we onze midlifecrisis anders bezweren dan met het schrijven van een proefschrift), Marike (wat is het toch fijn stil in Berlijn -behalve die laatste keer- maar ook dat had met het proefschrift te maken), Roos & Sjaan (ik ben erg blij met jullie, en heb veel dierbare herinneringen aan het delen van onze fantastische studiejaren in de Dorpsstraat 82), Charlot (engel uit Utrecht), Annelies (fijne vriendin in het Nijmeegse), en de vurige 4 moeders (samengebracht door onze zonen hoop ik dat we de post-proefwerkweek etentjes erin houden).
Dan kom ik bij mijn dierbaren. Allereerst die ontvallen zijn. Mijn vader Jan. Aan jouw hand liep ik als kind door de gangen van het Radboud. Jij vertelde mij er spannende verhalen onder het genot van ziekenhuislucht. Ik snoof beiden hartstochtelijk in mij op en vond het heerlijk. Dáár is de kiem gelegd. Dat wilde ik later ook. Dank voor al je wijze lessen! Mijn zusje Rianne. Ziel in mijn hart. Wat was jij toch waanzinnig eigenzinnig, intelligent, en attent. Jij betekende alles voor me en jouw dood was te groot voor mij. Gelukkig kijk ik inmiddels ook met een glimlach terug naar wat was. En prijs ik me erg gelukkig met wat is. De laatste woorden – geleend van Heather Nova – zijn voor jou.
Mijn moeder Ria, lieve mama, jij leerde ons dat sociale rechtvaardigheid, behulp-zaamheid en creativiteit minstens zo belangrijk zijn als al het cognitieve, wat bij ons thuis zo hoog in het vaandel stond. Daar ben ik je ontzettend dankbaar voor. Jij bent zo’n krachtige vrouw! Mijn zus Tanya, lieve Tan, we delen dezelfde professionele passie en dragen dezelfde last. Leven een groot deel van ons leven in het ziekenhuis. Fijn dat je achter en naast me staat. Ik dank Erik en jou voor alles wat jullie voor mij gedaan hebben. Daden van zusterliefde! Mijn zusje Maike, lieve Mai, ik bewonder jouw enorme levenslust, je vermogen om te genieten samen met Bas. In ons hart lijken wij best op elkaar. En ondanks dat je wars bent van de academie, sta je toch mooi naast me, veel dank daarvoor! Peggy, lieve Puk, jij hoeft dit proefschrift niet te lezen om te begrijpen wat er staat. We ondervonden alles aan den lijve. Jij en ik hebben het toch goed gedaan, dat zie en voel ik zo duidelijk, ook als ik kijk naar onze kinderen Sam Nanne en Merijn. Lieve Sam, je groeide in deze jaren uit van kind tot jong volwassen vrouw. Ik
dan
kwo
ord

182
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
hou van je gedrevenheid en eigenzinnigheid, je humor en je dynamische en aan-stekelijke energie. Je bent een prachtmeid! Lieve Merijn, je bent me in deze jaren boven het hoofd gegroeid, en niet alleen qua lengte. Ik hou van jouw warme ogen, je innemende lach, je sociale en relati-verende karakter, en je stoerheid daarin. Jij bent een prachtvent! Henriëtte, liefste Jet, jij bracht muziek terug in mijn leven. De laatste stelling is voor jou. En toch: Het is de stilte waarin we elkaar vinden. Jij creëert rust en warmte, en maakt het leven lichter. Jij leert mij bij de dag te blijven (ondanks dit proefschrift). En ik geef jou wat van mijn dynamiek. Wat een prachtig evenwicht! Op de lemniscaat van ons leven…. Ik hou van jou!

183
curricu
luM
vitae
Curriculum Vitae
Else Bisseling (1973) werd geboren in Nijmegen, als tweede van vier dochters. Na het behalen van het Gymnasium diploma aan Het Stedelijk Gymnasium te Nijmegen (1991), studeerde zij geneeskunde aan de Rijksuniversiteit Utrecht alwaar zij, na wat extra-curriculaire activiteiten, haar docto-raal (1998) en artsexamen (2000) behaalde. In 2000 startte zij als arts-onderzoeker en ANIOS in respectievelijk het umc Utrecht en het Willem Arntz Huis, waar zij van 2003-2006 tevens haar opleiding tot psychiater doorliep. Van 2007-2011 werkte zij als psychiater, manager patiëntenzorg en als hoofd van de medische dienst (locaties Nijmegen en Zeeland) binnen de Pom-pestichting (nu Pro Persona). In deze periode werkte zij eveneens als forensisch rapporteur voor Justitie. In 2010 startte zij met de opleiding tot mindfulness trainer aan het Radboud Universitair Centrum voor Mindfulness. Zij werkte nog enige tijd voor Scelta (2011-2012), centrum voor persoonlijkheidsproblematiek (onderdeel van GGNet), en creëerde als chef bij Molemann Mental Health een succesvolle doorstart van een vestiging in Zutphen (2012-2013). Echter, de hulpverlening aan mensen met gecombineerd psychisch en somatisch lijden trok aan haar. Zij solliciteerde op de mogelijkheid om als PhD kandidaat onderzoek te gaan doen bij het Radboudumc in nauwe samenwerking met het Helen Dowling Instituut, centrum voor psycho-oncologie. In 2013 maakte zij definitief de overstap naar dit onderzoek, in een duo constructie met collega Compen, en combineerde deze positie met haar werk als psychiater bij Mentaal Beter (2013-2014), het Radbou-dumc (2014-2015) en het Helen Dowling Instituut (2015-2018). In 2016 volgde zij naast haar werk de postmaster opleiding psychosociale oncologie. In 2017 startte zij als waarnemend psychiater op de polikliniek van de afdeling psychiatrie van het Canisius-Wilhelmina Ziekenhuis te Nijmegen. In 2018 trad zij toe tot de vak-groep. Binnen het Canisius-Wilhelmina ziekenhuis werkt zij momenteel als Chef de Clinique, als psychiater op de polikliniek en bij de consultatieve dienst met als aandachtsgebied psycho-oncologie. Daarnaast fungeert zij als Opleider Psychiatrie. Tot slot werkt zij sinds 2019 als coach binnen de leerlijn professionaliteit van de faculteit geneeskunde en biomedische wetenschappen van de Radboud Universiteit.
Else heeft 2 kinderen die zij in co-ouderschap opvoedt en woont samen met haar partner Henriëtte.

184
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
List of publications
in this thesisPeer reviewed
E.M. Bisseling, L. Cillessen, P. Spinhoven, M.P.J. Schellekens, F.R. Compen, M.L. van der Lee, A.E.M. Speckens (2019). Development and Association of Therapeutic Alliance With Outcome of Internet-Based Mindfulness-Based Cogni-tive Therapy for Distressed Cancer Patients: Secondary Analysis of a Multicenter Randomized Controlled Trial. Journal of Medical Internet Research: 21(9), e14065
E.M. Bisseling, M.P.J. Schellekens, P. Spinhoven, F.R. Compen, A.E.M. Speck-ens, M.L. van der Lee (2018). Therapeutic alliance -not therapist competence or group cohesion- contributes to reduction of psychological distress in group-based Mindfulness-Based Cognitive Therapy for cancer patients. Clinical Psychology & Psychotherapy: 26(3):309-318
E.M. Bisseling, M.P.J. Schellekens, E. Jansen, J. Prins, A.E.M. Speckens (2017). Mindfulness-Based Stress Reduction for breast cancer patients: A mixed method study on what patients experience as a suitable stage to participate. Supportive Care in Cancer, 25: 3067–3074
F.R. Compen*, E.M. Bisseling*, M.P.J. Schellekens, A.R.T. Donders, M.L. Van der Lee, A.E.M. Speckens (2018). Face-to-face and individual internet-based Mind-fulness-Based Cognitive Therapy are superior to Treatment As Usual in reducing psychological distress in cancer patients: a multicenter randomized controlled trial. Journal of Clinical Oncology: 10;36(23):2413-2421 *shared first authorship
F.R. Compen, E.M. Bisseling, M.L Van der Lee, E.M.M. Adang, A.R.T. Donders, A.E.M. Speckens (2015). Study protocol of a multicenter randomized controlled trial comparing the effectiveness of group and individual internet-based Mindful-ness-Based Cognitive Therapy with treatment as usual in reducing psychological distress in cancer patients: the BeMind study. Bmc Psychology, 3:27
not in this thesis Peer reviewed
F.R. Compen*, E.M. Bisseling*, M.P.J. Schellekens, A.R.T. Donders, L. Carlson, M.L. Van der Lee, A.E.M. Speckens (2019). RcT naar mindfulness-based cogni-

185
list of pu
blication
s
tieve therapie voor psychische klachten bij oncologische patiënten. Tijdschrift voor psychiatrie: 61(9): p. 2-12 *gedeeld eerste auteur
Melanie Schellekens, Marije Wolvers, Félix Compen, Else Bisseling, Fieke Brug-geman-Everts, Miriam Vollenbroek-Hutten, Anne Speckens, Marije van der Lee (2019). Online mindfulness-based cognitieve therapie bij kanker: Resulta-ten van twee gerandomiseerde gecontroleerde trials. Tijdschrift voor gedragsthe-rapie en cognitieve therapie, 52(2): p. 166-190
L. Cillessen M.P.J. Schellekens M.O.M. Van de Ven, A.R.T. Donders, F.R. Compen, E.M. Bisseling, M. L. Van der Lee, A.E.M. Speckens (2018). Consolidation and prediction of long-term treatment effect of group and online mindfulness-based cog-nitive therapy for distressed cancer patients. Acta Oncologica,57(10): p. 1293-1302.
F.R. Compen, EMM Adang, E.M. Bisseling, ML Van der Lee, AEM Speckens (2018). Exploring associations between psychiatric disorder, psychological distress, and health care utilization in cancer patients. Psycho-Oncology, 27(3):p. 871–878.
FR Compen, E.M. Bisseling, MPJ Schellekens MP, ET Jansen, ML van der Lee, AEM Speckens (2017). Mindfulness-Based Cognitive Therapy for Cancer Patients Delivered via Internet: Qualitative Study of Patient and Therapist Barriers and Facilitators. Journal of Medical Internet Research;19(12):e407
Submitted
E.M. Bisseling, F.R. Compen, M.P.J. Schellekens, B. Thewes, A.E.M. Speckens, M.L. van der Lee. Exploring Fear of Cancer Recurrence in a sample of heteroge-neous distressed cancer patients with and without a psychiatric disorder
L S. van Helmond, M.L. Van der Lee, E.M. Bisseling, P. Lodder, J. de Vries. Factor analysis of the Dutch version of the Fear of Cancer Recurrence Inventory (fcRI-NL)
F.R. Compen, E.M.M. Adang, E.M. Bisseling, M.L. Van der Lee ML, A.E.M. Speckens. Cost-effectiveness of individual internet-based and face-to-face Mind-fulness-Based Cognitive Therapy compared to Treatment As Usual in reducing psychological distress in cancer patients
Cillessen, M.O.M. Van de Ven, W. J. Burk, E.M. Bisseling, F.R. Compen, M. L. Van der Lee & A.E.M. Speckens. Temporal changes in mindfulness skills and

186
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
positive and negative affect and their interrelationships during Mindfulness-Based Cognitive Therapy for cancer patients

187
data M
anageM
ent stateM
ent
Data management statement
This thesis is based on the results of human studies, which were conducted in accordance with the principles of the Declaration of Helsinki. The medical and ethical review board Committee on Research Involving Human Subjects Region Arnhem Nijmegen, Nijmegen, The Netherlands has given approval to conduct these studies (cmO Arnhem – Nijmegen 2013/542). This project is stored on the Radboudumc, department server: (H:)PSYdata$ in the folder: H:\Research\BeMind. The patient data for the analyses of the studies as presented in chapter 3, 4, 5, and 6 is stored on this departments’ H-drive in a secured folder specifically for this project to which access is only granted to autho-rized personnel, as to be determined by the management of the department of Psychiatry. All paper informed consent forms are stored in a locked cabinet at the Centre for Mindfulness. Data management and monitoring were performed using a Microsoft Excel file which is also stored in the secured folder on the department server. An audit trail was incorporated to provide evidence of the activities that has altered the original data. The privacy of the participants in this study is warranted by use of encrypted and unique individual subject codes. This code correspondents with the code used in the patient report forms. The code was stored separately from the study data in a separate folder on the department server. Patient report forms were converged from Surveymonkey to SPSS (SPSS Inc., Chicago, Illinois, uSA). The original Surveymonkey files are also available. The data will be saved for 15 years after termination of the study (December 21, 2015). Using these patient data in future research is only possible after a renewed permission by the patient as recorded in the informed consent. The datasets analyzed during these studies are available from the corresponding author on reasonable request.

188
Min
dfu
lness-Based
Cogn
itive therapy fo
r distressed
CanCer patien
ts
Donders Graduate School for Cognitive Neuroscience
For a successful research Institute, it is vital to train the next generation of young scientists. To achieve this goal, the Donders Institute for Brain, Cognition and Behaviour established the Donders Graduate School for Cognitive Neuroscience (DGcN), which was officially recognised as a national graduate school in 2009. The Graduate School covers training at both Master’s and PhD level and provides an excellent educational context fully aligned with the research programme of the Donders Institute. The school successfully attracts highly talented national and international students in biology, physics, psycholinguistics, psychology, behavioral science, medicine and related disciplines. Selective admission and assessment centers guarantee the enrolment of the best and most motivated students. The DGcN tracks the career of PhD graduates carefully. More than 50% of PhD alumni show a continuation in academia with postdoc positions at top institutes worldwide, e.g. Stanford University, University of Oxford, University of Cambridge, ucL London, mPI Leipzig, Hanyang University in South Korea, NTNu Norway, University of Illinois, North Western University, Northeastern University in Boston, ETH Zürich, University of Vienna etc. Positions outside academia spread among the following sectors: specialists in a medical environment, mainly in genetics, geriatrics, psychiatry and neurology. Specialists in a psychological environment, e.g. as specialist in neuropsychology, psychological diagnostics or therapy. Posi-tions in higher education as coordinators or lecturers. A smaller percentage enters business as research consultants, analysts or head of research and development. Fewer graduates stay in a research environment as lab coordinators, technical sup-port or policy advisors. Upcoming possibilities are positions in the IT sector and management position in pharmaceutical industry. In general, the PhDs graduates almost invariably continue with high-quality positions that play an important role in our knowledge economy. For more information on the DGcN as well as past and upcoming defenses please visit: http://www.ru.nl/donders/graduate-school/phd/

I carry you with me,A ghost inside
And in these shattered arms,You’re still alive.
The bones we buried,Will feed the trees
But every word you ever spoke,Is still in me.
I will feel for you in the music,I will send that river home.
I will cry for you sometimes,When the night is down.
Then I raise my head up to the mountains,
Talk to the birds and I fly,‘Cause the spirit lives on,
When the body dies.
(Heather Nova – Walking higher)












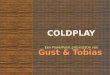




![[Book] Coldplay - Parachutes](https://img.pdfslide.net/doc/110x75/55cf925e550346f57b95ea12/book-coldplay-parachutes.jpg)