Embed Size (px)
Citation preview
Mindfulness in Clinical Psychology
Mark WilliamsUniversity of Oxford
Department of Psychiatry
Collaborators: Zindel Segal, John Teasdale, Jon Kabat-ZinnOxford Team: Melanie Fennell, Thorsten Barnhofer, Catherine Crane,
Danielle Duggan, Adhip Rawal, Emily Hargus, Wendy Swift
www.mbct.co.uk
Buddhism and Science
March 2010
Outline
• Clinical psychology and cognitive science– Depression recurrence– Outcome evidence
• What is going on?– Modes of self-focus
• Conceptual vs experiential• Exploring modes of self-focus
• in eating pathology• through neuroimaging
• Mindfulness and relapse signatures
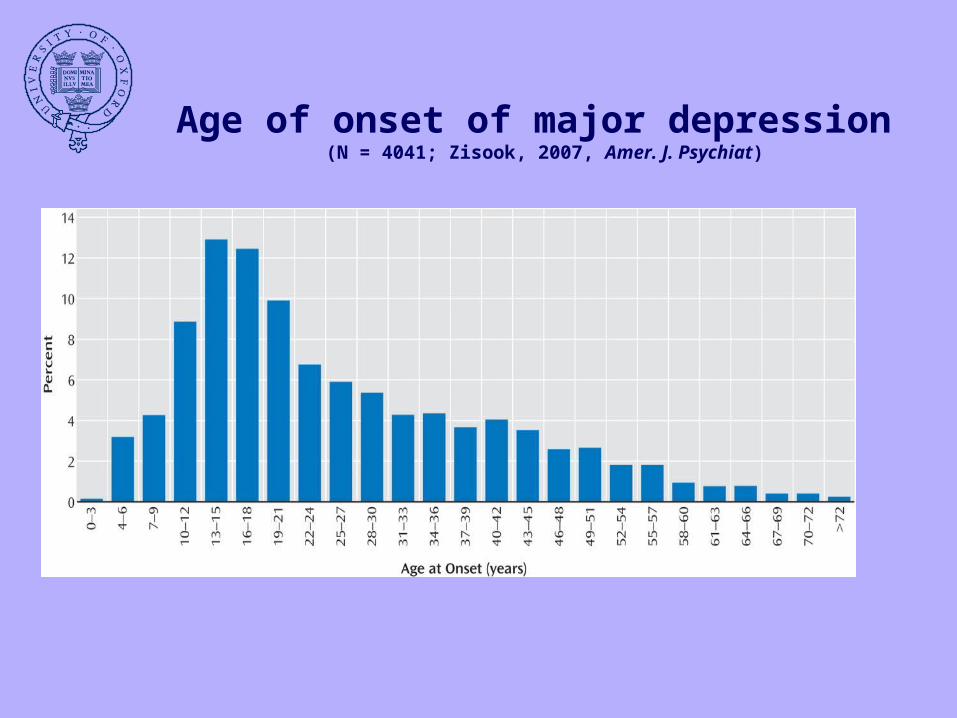
Age of onset of major depression (N = 4041; Zisook, 2007, Amer. J. Psychiat)
Depression recurrence
More than 50% who do recover will have at least one further episode
Those with history of 2 or more episodes have 70-80% chance of recurrence
Mindfulness-based Cognitive Therapy (MBCT)
Designed for patients in remission to prevent relapse/recurrence
Format Pre-class interview Eight weekly classes. Each 2 hours. Around 12 in each class Teaching meditation
sustained attention on breath and body thoughts as mental events
Home-based practice, up to one hour per day, 6 days a week - mostly CDs of mindfulness meditation practice
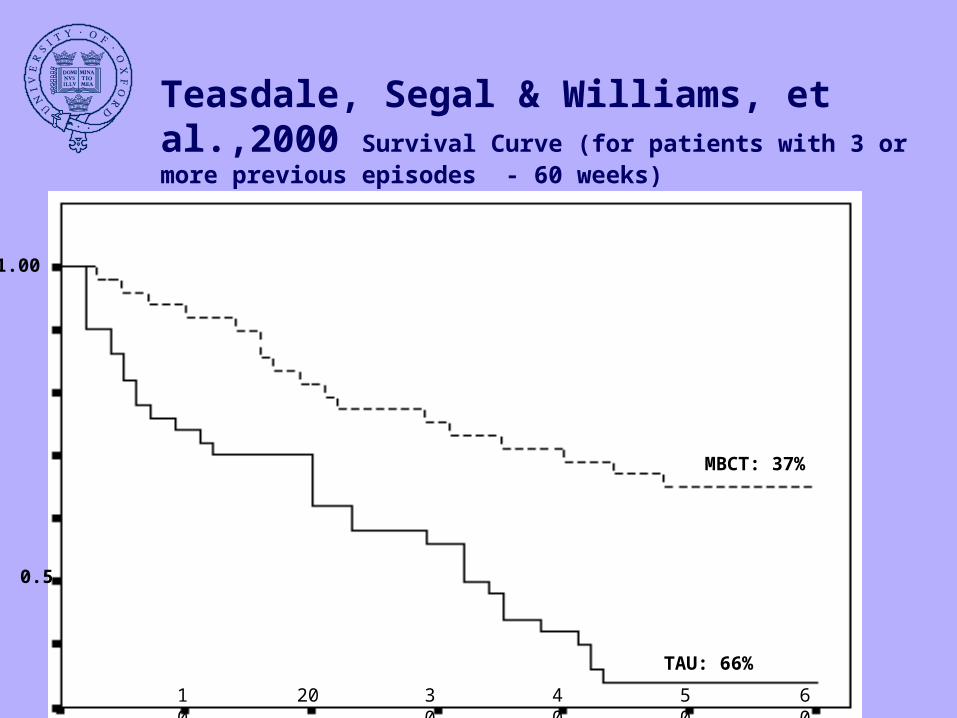
Teasdale, Segal & Williams, et al.,2000 Survival Curve (for patients with 3 or more previous episodes - 60 weeks)
MBCT: 37%
TAU: 66%
10 20 30 40 50 60
1.00
0.5
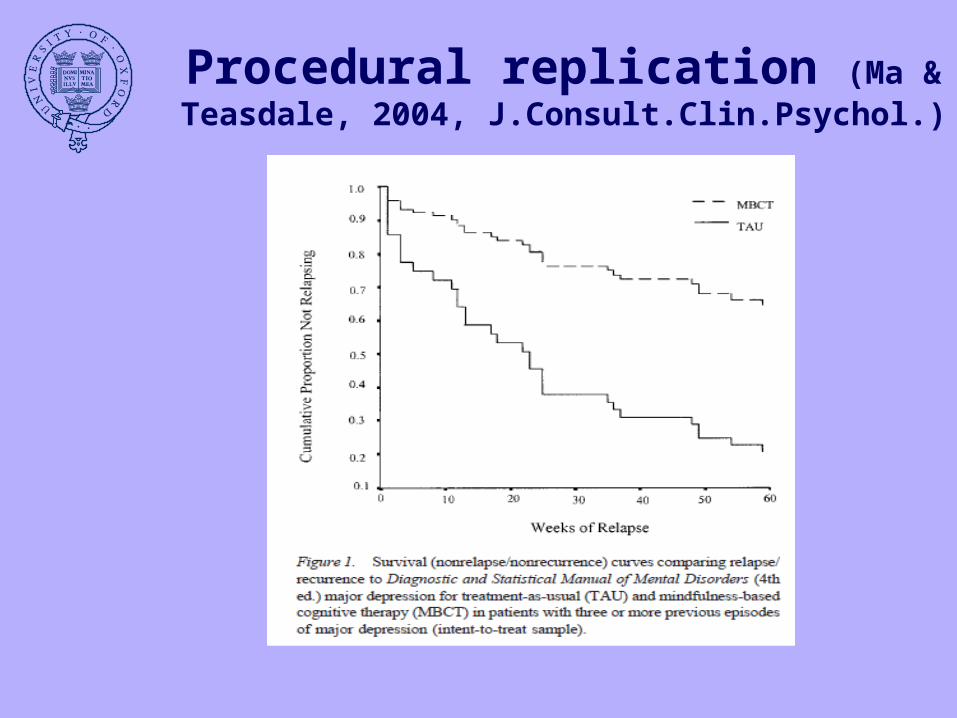
Procedural replication (Ma & Teasdale, 2004, J.Consult.Clin.Psychol.)
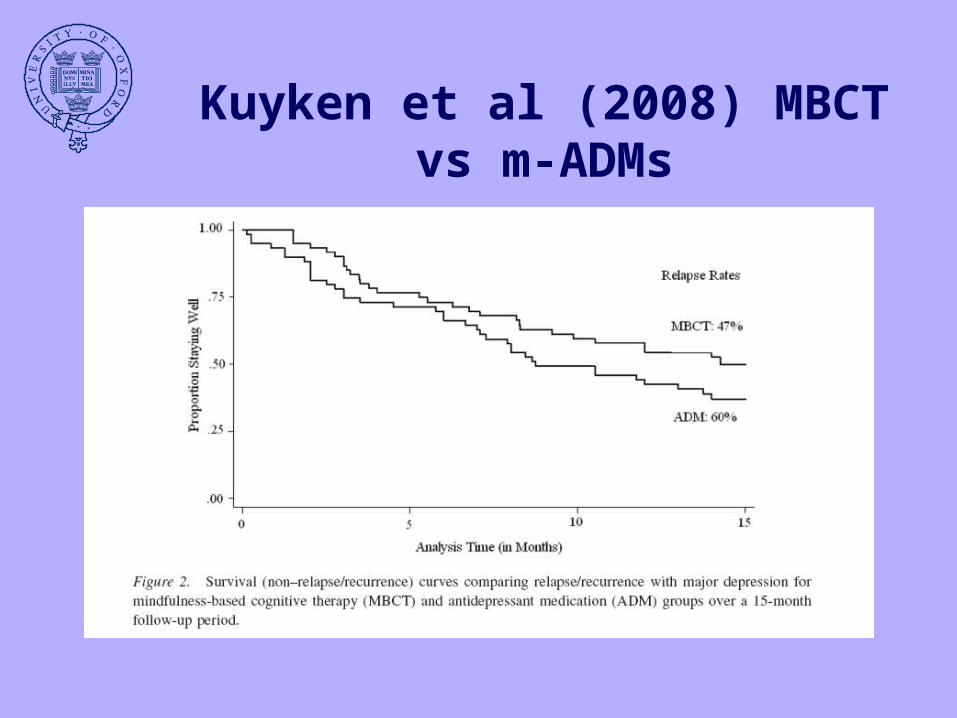
Kuyken et al (2008) MBCT vs m-ADMs
Outline
• Clinical psychology and cognitive science– Depression recurrence– outcome evidence
• What is going on?– Modes of self-focus
• Conceptual vs experiential• Exploring modes of self-focus
• in eating pathology• through neuroimaging
• Mindfulness and relapse signatures
Automatic vs strategic processes
• Darwin (1872)• What we seen in humans is a combination of
– evolutionary old, automatic reactions• Switch on AND OFF depending on
contingencies – evolutionary newer, strategic, representational
and symbolic reactions (working “off-line”)
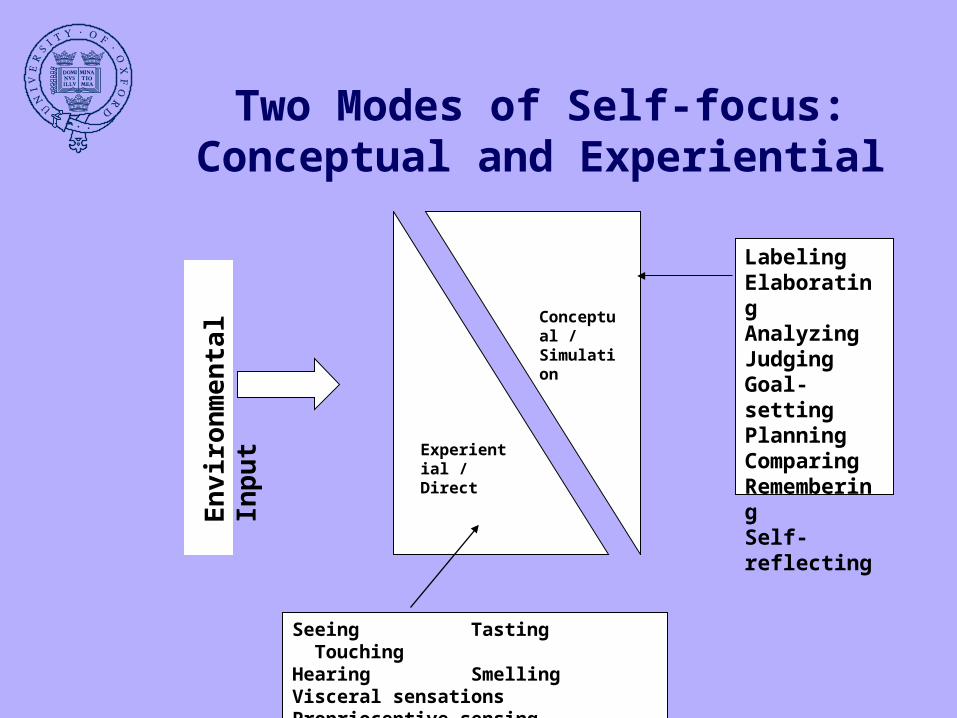
Two Modes of Self-focus: Conceptual and Experiential
Conceptual / Simulation
Experiential / Direct
LabelingElaboratingAnalyzingJudgingGoal-settingPlanningComparingRememberingSelf-reflecting
Seeing Tasting TouchingHearing SmellingVisceral sensationsProprioceptive sensing
En
viro
nm
enta
l In
pu
t
• Conceptual mode useful – To complete meanings– To complete tasks
• But when it becomes over-used– Preoccupied by meaning– Planning (even when not wanted)
•I find it difficult to stay focused on what’s happening in the present. •I tend to walk quickly to get where I’m going without paying attention to what I experience along the way.•It seems I am “running on automatic” without much awareness of what I’m doing.•I rush through activities without being really attentive to them.•I get so focused on the goal I want to achieve that I lose touch with what I am doing right now to get there.•I find myself preoccupied with the future or the past.
•Cf Cornell Campus experiment
Consequences of conceptual mode (from the Mindful Attention and Awareness Scale; Brown & Ryan, 2003)
…in depression
• Key maintaining factorPERSISTENT OVER-USE OF CONCEPTUAL MODE– “adhesive pre-occupation”(rumination) & Attempts to stop it(avoidance)
»lack of interest in anything else
For example
• Focus on• Feelings of tiredness
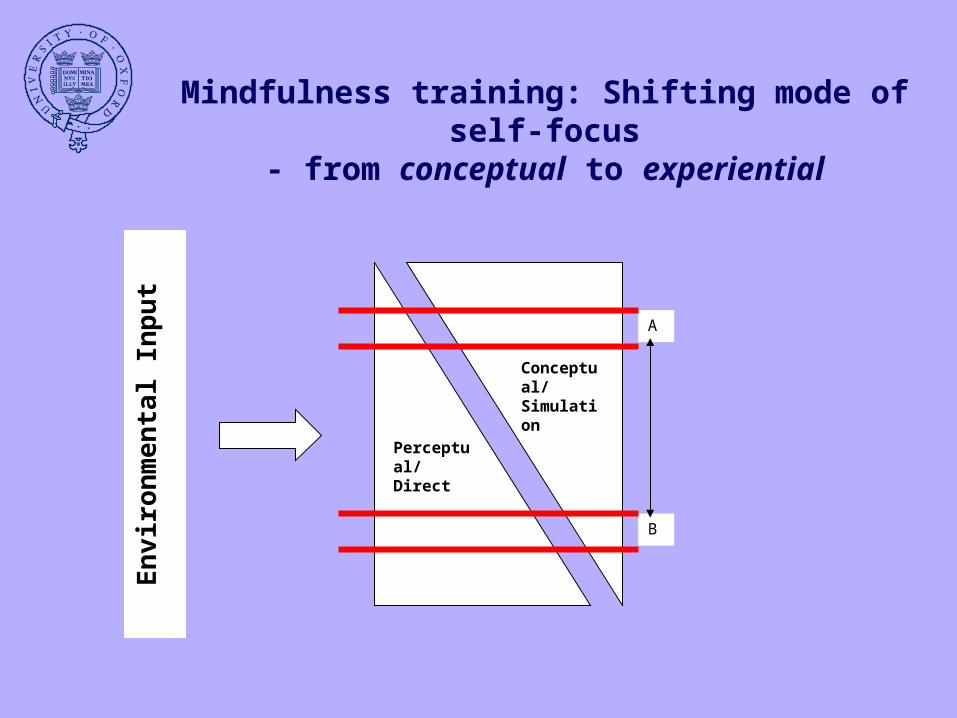
Mindfulness training: Shifting mode of self-focus
- from conceptual to experientialE
nvi
ron
men
tal I
np
ut
Conceptual/ Simulation
Perceptual/Direct
A
B
Outline
• Clinical psychology and cognitive science– Depression recurrence– outcome evidence
• What is going on?– Modes of self-focus
• Conceptual vs experiential• Exploring modes of self-focus
• in eating pathology• through neuroimaging
• Mindfulness and relapse signatures
(Adhip Rawal’s DPhil thesis)
• Choose a condition where self-focus most problematic– Students with high eating concerns– Anorexic in-patients
Induction of processing modes (Watkins & Teasdale, 2004)
• Sample item:
• the physical sensations in your body• the way you feel inside• how awake or tired you are
• Mode induction – Conceptual:
• Think about the causes, meanings and consequences of……
– Experiential:• Focus your attention on the experience of ……
• 8 minutes
Stress test for Eating Concerns
• Imaginary meal procedure (Shafran et al.,1999)
•Participants asked to imagine eating a fattening food for a period of 2 minutes.
Outcome measures
• Estimate of actual weight “How much do you think you weigh right now?”
• Moral wrongdoing: – How morally unacceptable/wrong do you feel (0-100%) it
was to think about eating the food• Urge to reduce/cancel effects:
– “How strong do you feel is your urge (0-100%) to reduce or cancel the effects of thinking about the food?”
• Neutralization– imagining exercising– imagining eating celery– checking shape in a mirror
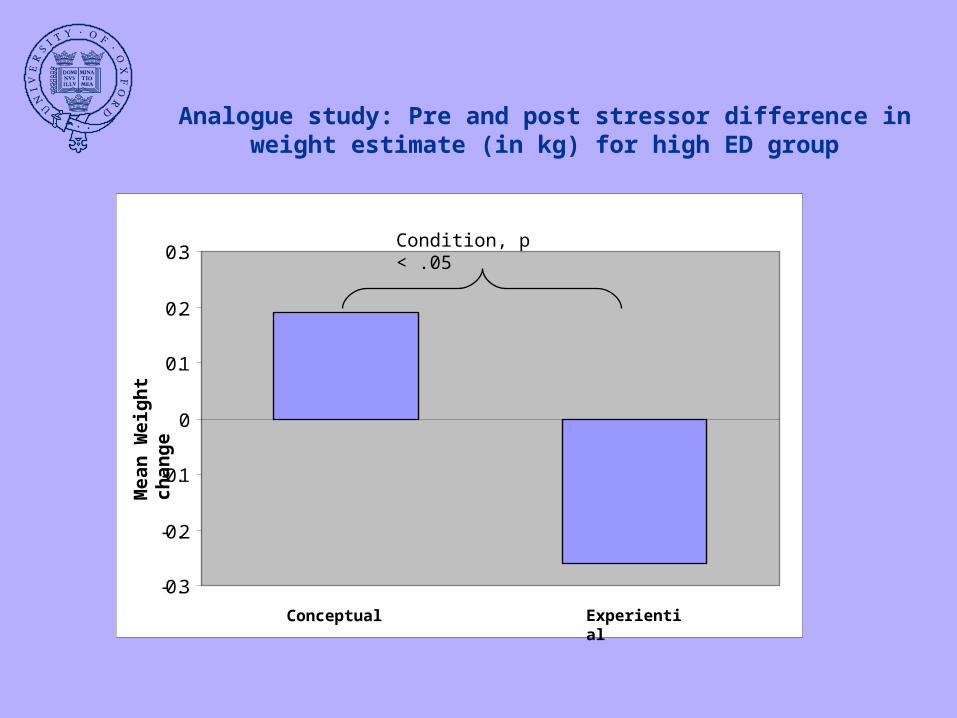
Analogue study: Pre and post stressor difference in weight estimate (in kg) for high ED group
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
Conceptual Experiential
Mea
n W
eig
ht
chan
ge
Condition, p < .05
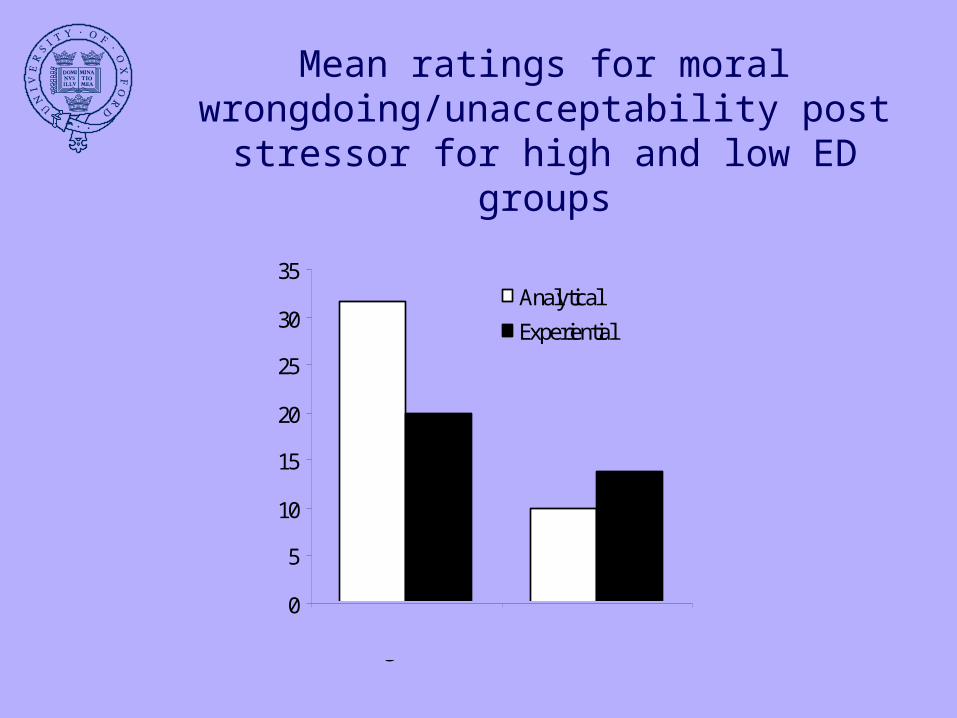
Mean ratings for moral wrongdoing/unacceptability post
stressor for high and low ED groups
0
5
10
15
20
25
30
35Analytical
Experiential
Mor
al W
rong
doin
g
High ED Low ED
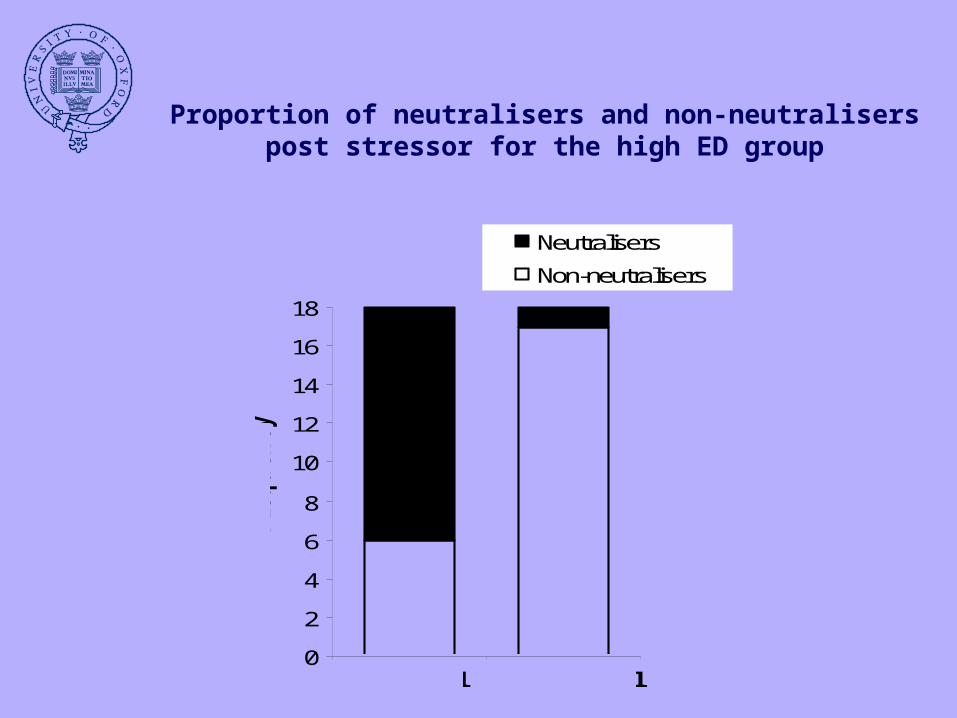
Proportion of neutralisers and non-neutralisers post stressor for the high ED group
0
2
4
6
8
10
12
14
16
18
Neutralisers
Non-neutralisersFre
quency
Analytical Experiential
Anorexic patients?
• N = 13 in-patients• BMI=17.2• Matched controls
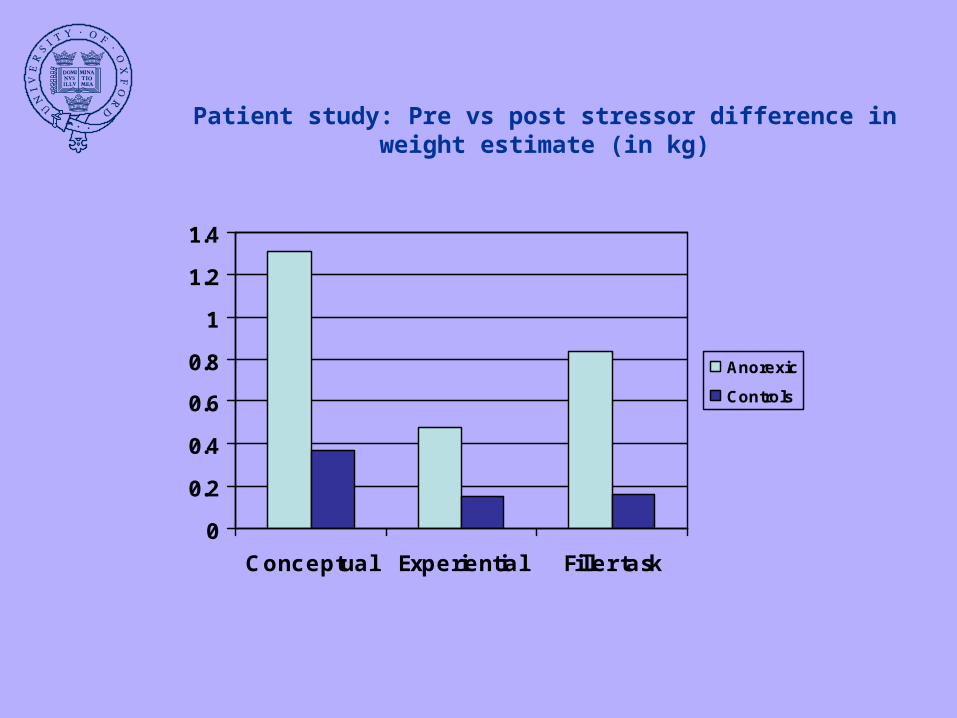
Patient study: Pre vs post stressor difference in weight estimate (in kg)
0
0.2
0.4
0.6
0.8
1
1.2
1.4
Conceptual Experiential Filler task
Anorexic
Controls
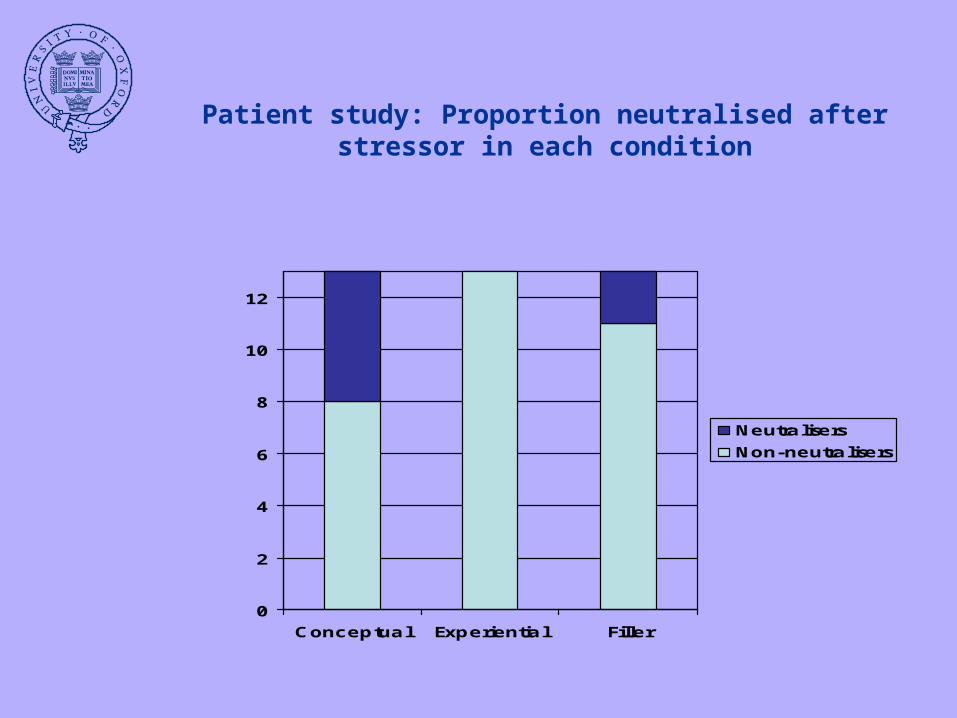
Patient study: Proportion neutralised after stressor in each condition
0
2
4
6
8
10
12
Conceptual Experiential Filler
Neutralisers
Non-neutralisers
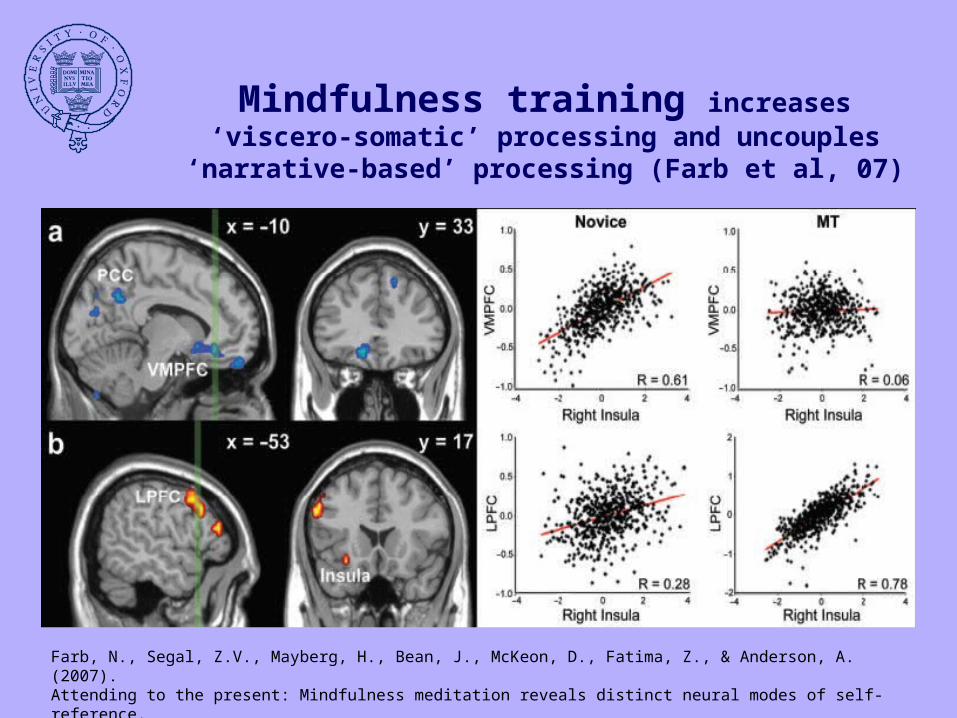
Mindfulness training increases ‘viscero-somatic’ processing and uncouples ‘narrative-
based’ processing (Farb et al, 07)
Farb, N., Segal, Z.V., Mayberg, H., Bean, J., McKeon, D., Fatima, Z., & Anderson, A. (2007).Attending to the present: Mindfulness meditation reveals distinct neural modes of self-reference.Soc Cog Aff Neurosci., 2, 313-322.
Outline
• Clinical psychology and cognitive science– Depression recurrence– outcome evidence
• What is going on?– Modes of self-focus
• Conceptual vs experiential• Exploring modes of self-focus
• in eating pathology• through neuroimaging
• Mindfulness and relapse signatures
Relapse signatures (Emily Hargus’s data)
• Individual patterns of prodromal features that warn of onset of episode
• Very important for self-management (schizophrenia, bipolar disorder, suicidal behaviour)
• Not just whether noticed, but how we relate to them –– enmeshed
• “I’m not ever going to be able to sleep again”– with meta-awareness (“decentered”)
• “I felt life was getting difficult, but it was my own inability to cope at that time”
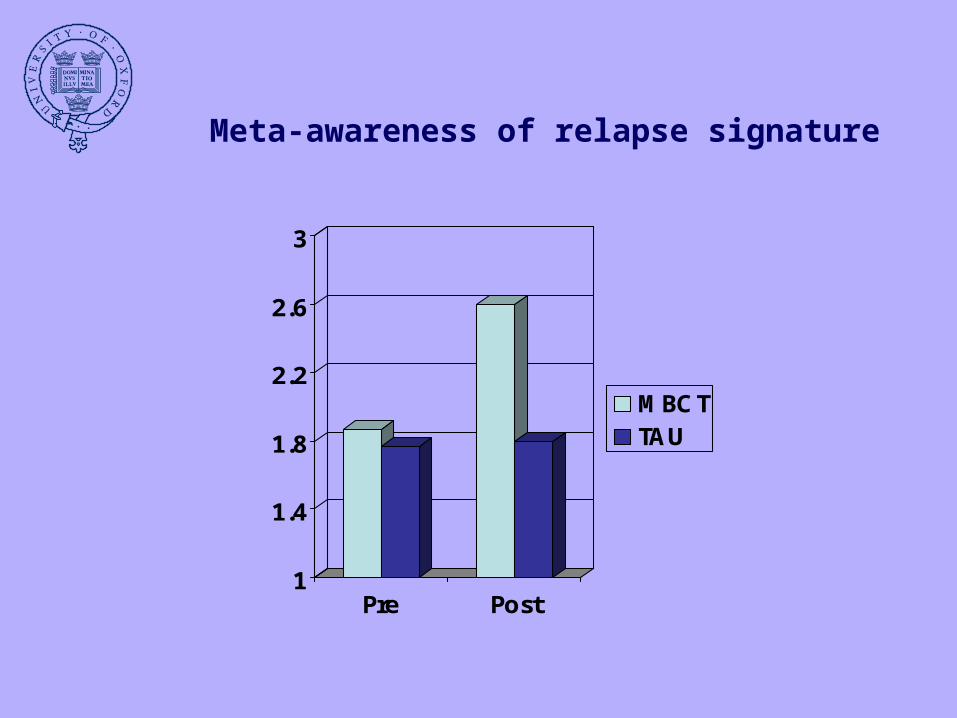
Meta-awareness of relapse signature
1
1.4
1.8
2.2
2.6
3
Pre Post
MBCTTAU
Summary
• Mindfulness training can reduce depression recurrence
• Training in experiential mode of self-focus- can prevent over-use of conceptual mode
• Impact of mode of self-focus – also seen in eating pathology– can be explored through neuroimaging
• Encouraging evidence for MBCT in decentring from suicidal thinking

Thank you
• www.mbct.co.uk