Embed Size (px)
Citation preview

8/7/2019 Mineral Metabolism Final Printable
http://slidepdf.com/reader/full/mineral-metabolism-final-printable 1/11
PHYSIOLOGY: Hormone Regulation of Mineral Metabolism 1
SUBJECT: PHYSIOLOGY
TOPIC: Hormone Regulation of Mineral
Metabolism
LECTURER: DR. VIC MENDOZA
DATE: FEBRUARY 2011
Endocrine System:
• Maintains constant concentration of
ionized Calcium in the extracellular fluid
• Responsible for:
o Bone mineralization
o Neuromuscular excitability
o Membrane integrity
o Cellular biochemical reactions
o Stimulus‐secretion coupling
(especially in the GIT)o Blood coagulation
PHOSPHATE
• Critically important to all biological
systems
• Integral component of numerous
intermediates in the metabolism of
carbohydrates, lipids, and proteins
• Forms part of the structure of
– High‐energy transfer and storage
compounds such as ATP and
Creatine Phosphate
– Co‐factors such as NAD, NADP,
and thiamine pyrophosphate
– Second messengers such as
cAMP and inositol triphosphate
– DNA and RNA
• Functions as covalent modifier of many
enzymes
• Intracellularly, an important anion that
balances the cations K+ and Mg++
• Major constituent of the crystalline
structure of bone and teeth
– 85% in skeleton, 6% in muscle
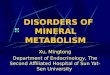
**The diagrams above show the Calcium
exchange between different tissue compartments
in a person ingesting 1000 mg of calcium per day.
Note: Most Calcium ingested is normally
eliminated in the feces, though kidneys also have
the capacity to excrete large amounts by reducing
tubular reabsorption of Calcium.

8/7/2019 Mineral Metabolism Final Printable
http://slidepdf.com/reader/full/mineral-metabolism-final-printable 2/11
PHYSIOLOGY: Hormone Regulation of Mineral Metabolism 2
CALCIUM BALANCE
• Balance means we talk about the amount
of Calcium that goes in the body (input)
and how much Calcium goes out (output).
• Therefore, if we say there's a "balance", it
means that the amount that goes in mustbe the amount that goes out. And if there
is more calcium going in than going out
(input > output), then there will be an
imbalance.
• In terms of Input:
o Basically from our diet, where
calcium intake may vary from
200 mg to 2000 mg per day. But
on average, we take in about
1000 mg. (American diet)
o But not all of this 1000 mg is
absorbed in our system. Only
about 300 mg is absorbed on
average.
NOTE: Calcium is actually absorbed in the ILEUM
• There are 2 processes that allow the
absorption of Calcium
1. Passive Diffusion (10%)
2. Active Transport (90%)
But although 300 mg is absorbed in the GIT, a lot
of calcium is also secreted by the GIT. (e.g. calcium
in the pancreatic secretion) Therefore, although you
absorb 300, as much as 125 mg is secreted by the
GIT. This means that in terms of absorption, there
is only a 175 mg net absorption of calcium, while
the rest is secreted out.
SO how much calcium goes in? 175 mg.
However, there is actually a really huge amount of calcium found in the body (about 1 kg) at any
point in time. 99% of this is found in the skeletal
system. The other 1% is found in soft tissue and
ECF.
About 1% of that in bone (about 10 g) is
exchangeable with that in the ECF.
How does this work?
The bone undergoes constant remodelling or a
continuous resorption of the bone. This means
that part of the bone is destroyed, but with newbone formation at the same time. (Because of this,
they estimated that the skeletal system is
regenerated every 10 years!)
Most of the calcium in the ECF is filtered
(ultrafilterable). But a good portion of the calcium
ECF is reabsorbed. In a day, about 10 g are
filtered. But out of this 10 g, more than 98% is
reabsorbed, while the rest is excreted out through
the urine.
Again, this balance works because of theregulators. (Major regulator is actually the
parathyroid hormone when it comes to calcium).
Recall:
There are 3 cell types in the bones:
1. Osteocytes ‐ the "imprisoned" osteoblasts
surrounded by new bone
2. Osteoblasts ‐ new bone formation
3. Osteoclasts ‐ bone resorption
3 Regulators of Calcium and PhosphateMetabolism:
• Parathyroid Hormone
• Vitamin D
• Calcitonin (concerned with Calcium ONLY)
1. PARATHYROID HORMONE
Target Organs:
• Bones
• Kidney (because the kidneys are involved in
calcium excretion)

8/7/2019 Mineral Metabolism Final Printable
http://slidepdf.com/reader/full/mineral-metabolism-final-printable 3/11
PHYSIOLOGY: Hormone Regulation of Mineral Metabolism 3
How PTH works:
When you have very high levels of PTH, bone
resorption occurs. A high activity of bone
resorption means there will be a release of
calcium and phosphate from the skeletal system.
These go to the ECF.
Therefore, calcium serum level rises, and,
theoretically, phosphate levels should rise too.
However, it was found that when you have high
PTH, there is indeed a rise in calcium levels BUT
phosphate levels seem to decrease. This is due to
the effect of the PTH on the kidneys.
Effect of PTH on Kidneys
1. Promotes calcium reabsorption
Therefore, calcium serum levels ELEVATE more.
Note: Calcium reabsorption occurs in the distal
nephron
2. Promotes phosphate excretion
So you lose a lot of phosphate through the
urine.
This action of the PTH on the kidneys is
greater/more dominant than the effect of PTH on
the bone. Therefore, even if phosphate is released
in the bones too, the net effect is that it causes
your phosphate levels to decrease in the serum.
Reducing phosphate levels is actually very
important because if both calcium and phosphate
are very high in your serum, there is a tendency
for mineralization of bone rather than increasing
serum calcium levels.
What regulates the PTH secretion?
Amount of ionized calcium in the body.
This is a negative feedback effect, wherein if calcium in the serum is high, amount of PTH is
low. But, if serum calcium is low, PTH secretion is
high.
Again:
Low ionized serum calcium = High PTH secretion
High ionized serum calcium = Low PTH secretion
There are also other factors that can change the
amounts of total serum calcium such as change in
acid‐base balance
If in a state of acidosis, the acidosis will displace
calcium from its binding with protein.
On the other hand, alkalosis can enhance the
binding of ionized calcium to protein, thereby
reducing the ionized portion!
Hyperventilation Syndrome:
A case wherein an individual hyperventilates, thus
CO2 is blown off. This induces respiratory alkalosis.
The alkalosis will cause the calcium to bind more,
and therefore the ionized serum calcium level goes
down. As a result, these people present with a form
of muscular tetany .
(Since calcium is involved in muscular excitability)
How is the amount of ionized serum calciumdetermined if we can only measure total serum
calcium?
They found out that about 50% of the total serum
calcium is ionized.
The other 50% is not ionized because 40% is bound to
protein, whereas the other 10% is complexed with
diffusable anions.
So, when there is a change in serum protein levels
(especially albumin, since calcium is really bound to
albumin), there is bound to be a change in the total
serum calcium concentration as well.
They postulated that if there is a decrease in serum
albumin levels by about 1mg/deciliter, then the total
serum calcium concentration will also be reduced by
about 0.8 mg/dL.

8/7/2019 Mineral Metabolism Final Printable
http://slidepdf.com/reader/full/mineral-metabolism-final-printable 4/11
PHYSIOLOGY: Hormone Regulation of Mineral Metabolism 4
Action of PTH in Promoting Calcium
• Of the 3 cell types found in the bones, it is
the osteoclasts that are directly affected
by PTH.
• PTH indirectly affects osteoblasts.
If there is new bone formation, the
osteoblasts draw calcium from the ECF to
incorporate in the new bone. As a result, it will
cause a DECREASE in the amount of calcium in
the ECF.
Remember that there is a relationship between
your osteoblasts and osteoclasts.
Osteoblasts come from the stromal cells (CT
within bone marrow), whereas the osteoclasts
come from macrophages. The osteoblasts secrete
a chemical signal that has an effect on the
differentiation of osteoclasts.
These chemical signals are:
1. RANK Ligand
2. Osteoprotegerin
The RANK Ligand acts on the receptor found on
macrophages. So once this attaches to the
receptor, these macrophages are stimulated to
differentiate into osteoclasts!
At the same time, the RANK‐receptor complex
causes the formed osteoclasts to live longer by
suppressing apoptosis.
The Osteoprotegerin suppresses or inhibits the
development and activity of osteoclasts.
So PTH is supposed to inhibit the bone forming
activity of osteoblasts and stimulate recruitment
of osteoclasts.
Again, in a nutshell:
PARATHYROID HORMONE
• PTH acts directly on bone and kidney to
INCREASE Calcium influx into Plasma.
• By stimulating 1,25 (OH)2‐D synthesis,
PTH also increases calcium absorption
from the gut thus increasing plasmacalcium levels.
(will be further discussed in succeeding
text)
• In contrast, PTH INHIBITS renal tubular
resorption of phosphate, thereby
increasing urinary phosphate excretion.
o This offsets entry from bone and
gut therefore decreasing plasma
phosphate levels.
Among Females
Upon reaching the menopausal stage, females tend to
develop more brittle bones. Osteoporosis becomes a
significant problem. This is because estrogen actually
promotes the secretion of Osteoprotegerin, which
suppresses osteoclast development and activity.
Therefore, in menopause there is more of RANK.

8/7/2019 Mineral Metabolism Final Printable
http://slidepdf.com/reader/full/mineral-metabolism-final-printable 5/11
PHYSIOLOGY: Hormone Regulation of Mineral Metabolism 5
NOTE: There is an inverse relationship between
PTH secretion and plasma ionized concentration
in humans.
The diagram below further reinforces the indirect
relationship between PTH secretion and Serum
Calcium levels.
VITAMIN D
• Derived from cholesterol, therefore can
be classified as a steroid hormone
• Basically, from cholesterol converted
to pregnenolone eventually forming 7‐
Dehydrocholesterol.
7‐Dehydrocholesterol is actually abundant inthe skin. The exposure of skin to sunlight
(which has UV rays) promotes the conversion
of 7‐dehydrocholesterol to Vit. D3, or
cholecalciferol .
This cholecalciferol is bound to protein (globulin),
and upon binding enables it to circulate in thebloodstream. Once it finds its way into the liver,
the cholecalciferol is hydroxylated in the carbon
25 (C25) position. Thus, it becomes the 25‐
hydroxycholecalciferol. (aka 25‐hydroxy vitamin
D3, or the major circulating form of Vit. D).
As it circulates, it will find its way to the kidney
where it will again undergo hydroxylation. This
hydroxy group can attach to 2 positions: C24 and
C1.
If it attaches to C1, it will form 1,25(OH)2‐D3.If it attaches to C24, it will form 24,25(OH)2‐D3.
1,25(OH)2‐D3 is the biologically active form of
vitamin D3!
If there is a high rate of hydroxylation at the C1
position, then the hydroxylation at the C24 will be
very low. (Inversely proportional!)
They also postulated that hydroxylations in C24 is
a form of inactivation when it comes to vitamin D.
What will promote the development of the
active form (1,25(OH)2‐D3)?
Hydroxylation in the C1 position is facilitated by
an enzyme called 1‐alpha‐hydroxylase .

8/7/2019 Mineral Metabolism Final Printable
http://slidepdf.com/reader/full/mineral-metabolism-final-printable 6/11
PHYSIOLOGY: Hormone Regulation of Mineral Metabolism 6
If the activity of this enzyme is very high, then
more of 1,25(OH)2‐D3 (the more biologically active
one) will be formed. But if there is low activity of
1‐alpha‐hydroxylase, then there will be greater
formation of 24,25(OH)2‐D3.
What stimulates the activity of the enzyme 1‐
alpha‐hydroxylase?
1. High levels of PTH
High levels stimulate 1‐alpha‐hydroxylase
so that more of the active form (1,24) will
be formed.
2. Low levels of serum phosphate
3. High levels of 24,25(OH)2‐D3
But, in what situations will you have high levels of
PTH and low levels of serum phosphate?
When you have low serum calcium levels.
If your ionized serum calcium level is low, that will
cause your PTH levels to go up and thus cause
your phosphate levels in the serum to go down.
** Vit. D deficiency, calcium deficiency,
phosphate deficiency will also cause very high
levels of PTH.
What will promote the formation of the
INACTIVE form (24,25(OH)2‐D3)?
1. High levels of active vitamin D
2. Excess calcium
3. Excess phosphate
Action of Vitamin D
• Main target organ: GIT (directly affected)
• Although it also has (indirect) effects on:
‐ Bone
‐ Kidneys
‐ Immune system(Vitamin D actually stimulates
lymphocytes, macrophages)
‐ Skeletal muscle strength
Vitamin D on the Kidneys
Promotes the reabsorption of calcium as well.
PTH, however, has an indirect effect on the GIT by
promoting the synthesis of the active form of
vitamin D. Since a high level of PTH and low level
of serum phosphate stimulate the synthesis of 1,25(OH)2‐D3.
Does vitamin D qualify to be called a hormone?
Yes. The endocrine gland would be the skin. And
as it is produced in the skin, it goes through the
circulation without passing through any ducts.
It's just that it was only discovered first as a
vitamin D and so the name "stuck" as "vitamin D".
Vitamin D deficiency:
‐ Rickets for kids
‐ Osteomalacia for adults
If we are exposed to enough sunlight, there is no
need to take supplemental vitamin D.
The only problem is that nowadays, we are rarely
exposed to enough sunlight since some no longer
want to stay outdoors. This mentality causes us to
need to take in vitamin D supplements, especially
for dark‐skinned individuals (they need more
exposure to the sun to produce the same level of
vitamin D). This is a problem, due to the growing
trend of migration wherein a lot of black people
migrate to areas where there is very little sunlight
(e.g. Scandinavian countries).

8/7/2019 Mineral Metabolism Final Printable
http://slidepdf.com/reader/full/mineral-metabolism-final-printable 7/11
PHYSIOLOGY: Hormone Regulation of Mineral Metabolism 7
In a nutshell:
VITAMIN D
Target Organs:
• GIT:
Promote intestinal calcium absorption
and intestinal phosphate absorption• Bone:
Promotes mineralization of bone
• Kidney:
Facilitates Calcium reabsorption in the
distal nephron
• Immune System:
• Promotes differentiation of monocyte
precursors to monocytes & macrophages
• Skeletal Muscle
**Vitamin D affects both T and B cells, inhibiting
interleukin‐2 production and other effector
functions.
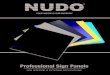
Below is a diagram [taken from Harper’s Illustrated
Biochemistry since the one in the powerpoint is not
that clear] that shows the formation and hydroxylation
of Vitamin D.
• Vitamin D undergoes 25‐hydroxylation in
the liver.
• It is then further hydroxylated in the
kidney in the position 1 [when more
biological reaction is needed] or position
24 [when less biological activity is
required].
CALCITONIN
• Produced by the T cells of thyroid gland
• Reduces bone resorption by inhibiting
osteoclast function
o Effect: Decreased concentrations
of Calcium and Phosphate in the
serum
• Receptors for Calcitonin are found in
bones and kidneys.
• Calcitonin lowers circulating Calcium and
Phosphate levels.
• It exerts its Calcium‐lowering effect by
inhibiting bone resorption.
• It also increases Calcium secretion in
urine.
Regulator of calcitonin levels:
Amount of calcium in the serum
If very, very HIGH serum calcium level
(hypercalcemia) Calcitonin secretion INCREASE
Osteoblast activity DECREASE reduced bone
resorption reduction in serum phosphate.

8/7/2019 Mineral Metabolism Final Printable
http://slidepdf.com/reader/full/mineral-metabolism-final-printable 8/11
PHYSIOLOGY: Hormone Regulation of Mineral Metabolism 8
But calcitonin is not so important as a regulator if
calcium is concerned. It is only important when
there are very, very high levels of serum calcium,
which rarely occurs. In fact, one can do away with
calcitonin.
On the other hand, PTH is said to be essential forlife. So if you take out the parathyroid gland (in
the process of taking out the thyroid, for
example), supplementation of calcium is needed.
In such cases, it will also help to be rich in vitamin
D so as to enhance the absorption of calcium in
the system.
TO SUMMARIZE:
• PTH increases serum calcium levels by
mobilizing calcium from the bone
•
This will increase the Calciumreabsorption in the kidney but may be
offset due to Calcium that is filtered
• Increased PTH will also lead to increased
formation of 1,25‐
dihydroxycholecalciferol.
• 1,25‐dihydroxycholecalciferol will
increase Calcium absorption from the
intestine and increases Calcium
reabsorption in the kidneys.
• Calcitonin will then inhibit bone
resorption and it will increase the amount
of Calcium in the urine.
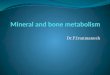
Image above:
Schema of how calcium is maintained at a
constant level:
Low serum calcium level will induce
increased PTH secretion.
PTH will then act on the bone, causing
resorption
As a result of resorption: Calcium levels
INCREASE, Phosphate levels DECREASE
(since PTH enhances the excretion of
phosphate)
If renal phosphate is low, and PTH is high
= cause the secretion of more active form of
vitamin D Vitamin D will then cause the gut to absorb
more calcium, specifically the active
transport of calcium in the GIT
Therefore the serum calcium level eventually
goes UP
Only if there is an excessive amount of
calcium will the calcitonin act! (very rare
occurrence)
—END OF TRANSCRIPTION—
Please read Guyton or Ganong for a more detailed
discussion.
Good luck BATCH 2014!

8/7/2019 Mineral Metabolism Final Printable
http://slidepdf.com/reader/full/mineral-metabolism-final-printable 9/11
PHYSIOLOGY: Hormone Regulation of Mineral Metabolism 9

8/7/2019 Mineral Metabolism Final Printable
http://slidepdf.com/reader/full/mineral-metabolism-final-printable 10/11
PHYSIOLOGY: Hormone Regulation of Mineral Metabolism 10
Vitamin D:
Bone:

8/7/2019 Mineral Metabolism Final Printable
http://slidepdf.com/reader/full/mineral-metabolism-final-printable 11/11
PHYSIOLOGY: Hormone Regulation of Mineral Metabolism 11
Indirect relationship between PTH secretion and
Serum Calcium: