Embed Size (px)
Citation preview
“Mini-MVR Is Better than Conventional MVR” - Con Ani Anyanwu, MD, FRCS
Associate Professor
Department of Cardiothoracic Surgery
The Mount Sinai Medical Center
New York, USA
I have no conflicts of interest or disclosures

Things are not always as they seem
There is more to mini-
MVR than a beautiful scar
There is more to mini-
MVR than beautiful data
“Mini-MVR Is Better than Conventional MVR” - Pro • It is less invasive • We are doing same operation through smaller
incision • Morbidity and mortality is less • Aesthetically superior • Less bleeding and blood transfusion • Less hospital stay • Better option for elderly and high-risk patient groups
TEN MYTHS OF MINIMALLY
INVASIVE CARDIAC SURGERY
Myth 1) MICS is Minimally Invasive
• MICS is invasive
• Invasion is not more different than with
sternotomy
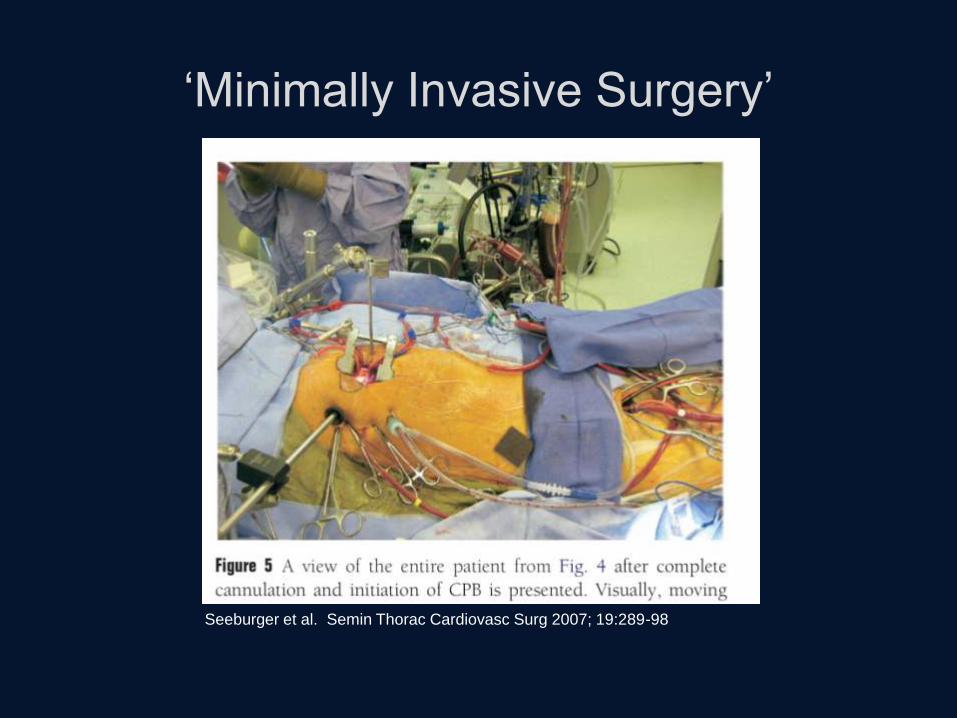
‘Minimally Invasive Surgery’
Seeburger et al. Semin Thorac Cardiovasc Surg 2007; 19:289-98
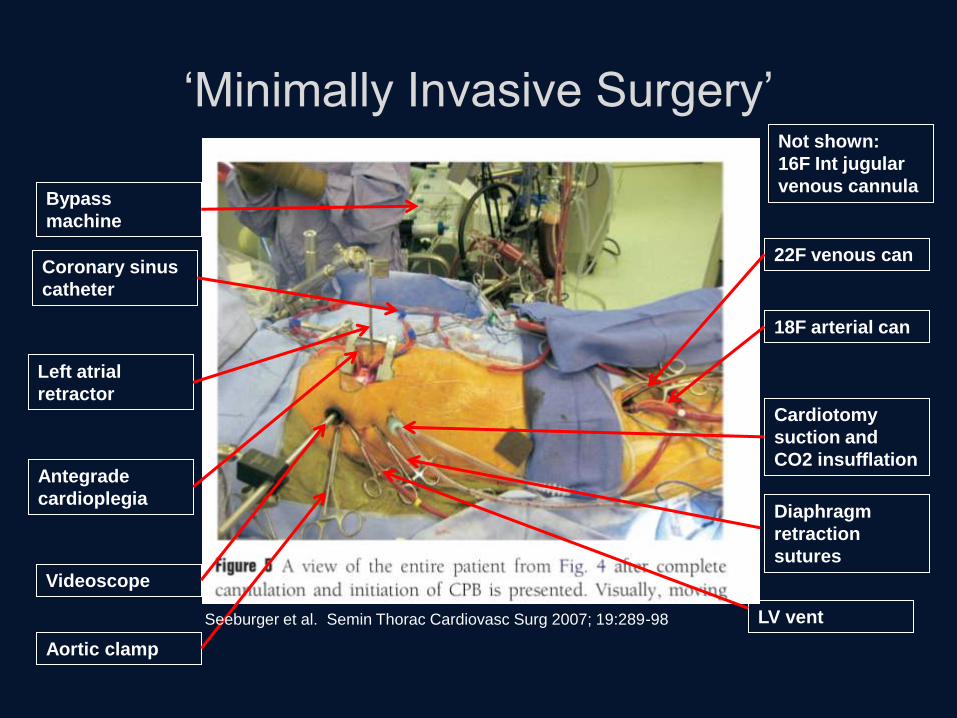
‘Minimally Invasive Surgery’
22F venous can
18F arterial can
Cardiotomy
suction and
CO2 insufflation
Diaphragm
retraction
sutures
LV vent
Antegrade
cardioplegia
Aortic clamp
Videoscope
Left atrial
retractor
Coronary sinus
catheter
Bypass
machine
Not shown:
16F Int jugular
venous cannula
Seeburger et al. Semin Thorac Cardiovasc Surg 2007; 19:289-98
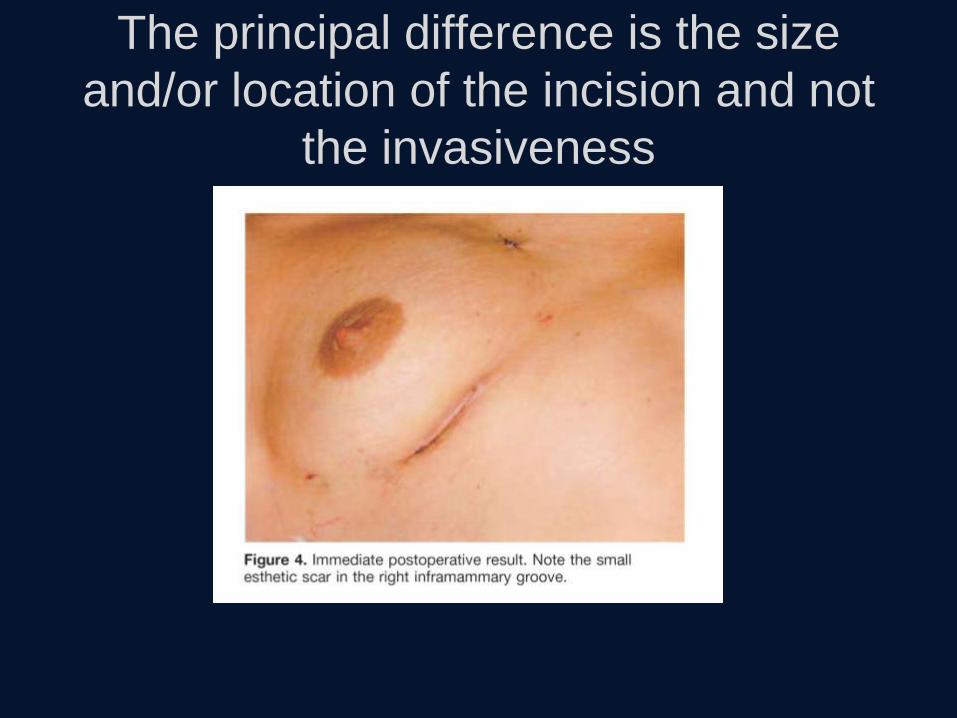
The principal difference is the size
and/or location of the incision and not
the invasiveness

General
Anesthesia
Tracheal
Intubation
MICS
Cardiopulmonary
bypass
Cardioplegic
arrest
Cardiotomy
Direct valve
repair
Closure
Elective
ventilation &
hospitalization
Limited Incision
General
Anesthesia
Tracheal
Intubation
STERNOTOMY
Cardiopulmonary
bypass
Cardioplegic
arrest
Cardiotomy
Direct valve
repair
Closure
Elective
ventilation &
hospitalization
Standard Incision
Casselman et al. Circuation 2003;108:II48-54
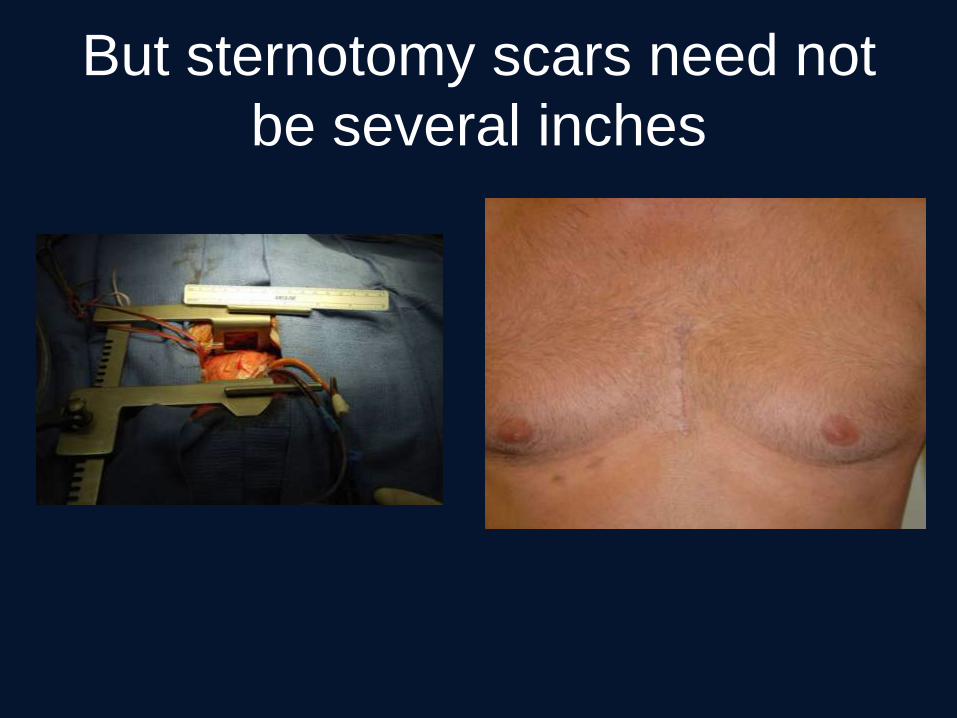
But sternotomy scars need not
be several inches
Myth 1) MICS is Minimally Invasive
• MICS is invasive
• ‘Invasion’ is not much different from
sternotomy
• Many MICS are merely cardiac surgery via
thoracotomy
• The term Minimally Invasive as applies to
cardiac surgery is an oxymoron
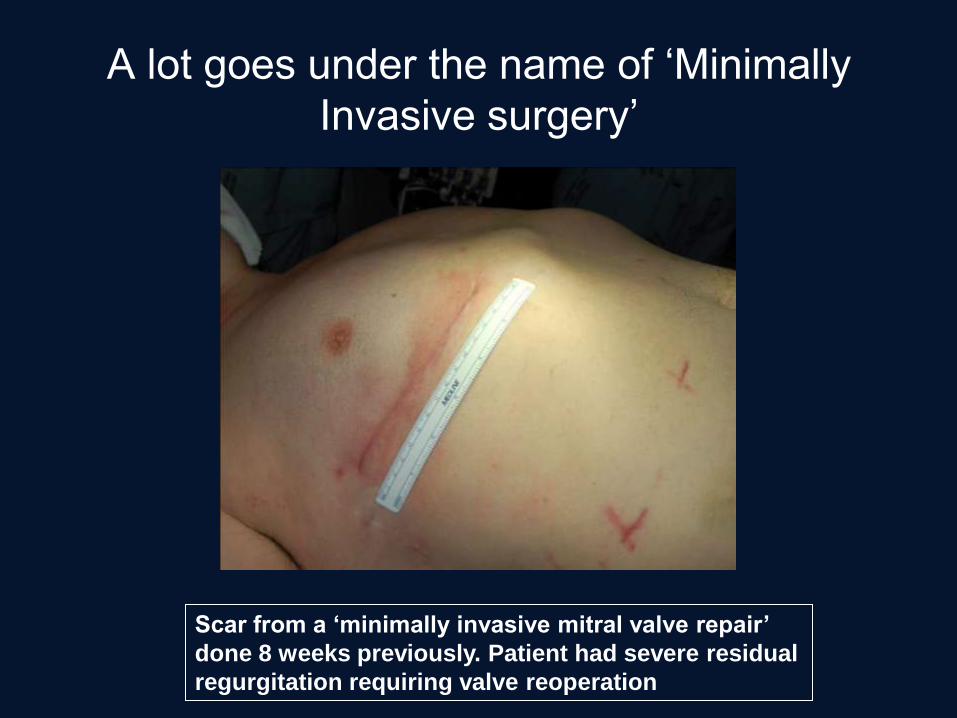
A lot goes under the name of ‘Minimally
Invasive surgery’
Scar from a ‘minimally invasive mitral valve repair’
done 8 weeks previously. Patient had severe residual
regurgitation requiring valve reoperation

A great con?
1st repair
via ‘MICS’
Valve
rerepair via
sternotomy
In reality many ‘MICS’
incisions are of similar
size to modern
sternotomy incisions
Real definition and meaning of MICS
• The most invasive aspects of cardiac surgery
relate to the anesthesia, pericardiotomy,
cardiotomy, cardiopulmonary bypass and
cardiac repair and not the incision
• In some ways MICS paradoxically introduces
invasiveness
– More exposure to cardiopulmonary bypass
– More gadgetry and invasive devices
Myth 2) MICS is the same operation
done through lesser access
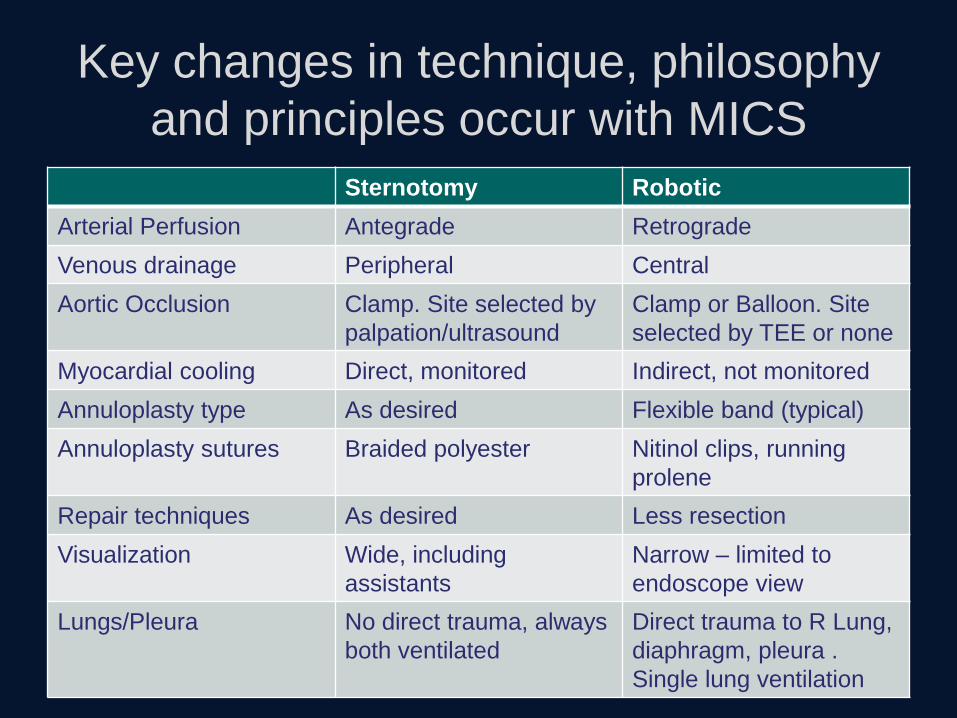
Key changes in technique, philosophy
and principles occur with MICS
Sternotomy Robotic
Arterial Perfusion Antegrade Retrograde
Venous drainage Peripheral Central
Aortic Occlusion Clamp. Site selected by
palpation/ultrasound
Clamp or Balloon. Site
selected by TEE or none
Myocardial cooling Direct, monitored Indirect, not monitored
Annuloplasty type As desired Flexible band (typical)
Annuloplasty sutures Braided polyester Nitinol clips, running
prolene
Repair techniques As desired Less resection
Visualization Wide, including
assistants
Narrow – limited to
endoscope view
Lungs/Pleura No direct trauma, always
both ventilated
Direct trauma to R Lung,
diaphragm, pleura .
Single lung ventilation
2) Is MICS is the same operation done
through lesser access?
• Reality is there is shifting of goal posts to
fulfill MICS objective
• Invariable compromise and/or change in
principles and technique which is more
exaggerated the smaller the incisions get
• Additionally there may be benefits seen with
MICS not seen with sternotomy
– E.g. better visualization
• But the two are not the same operation

Raanani et al. J Thorac Cardiovasc Surg 2010; 140:86-90
*Posterior Leaflet Pathology only
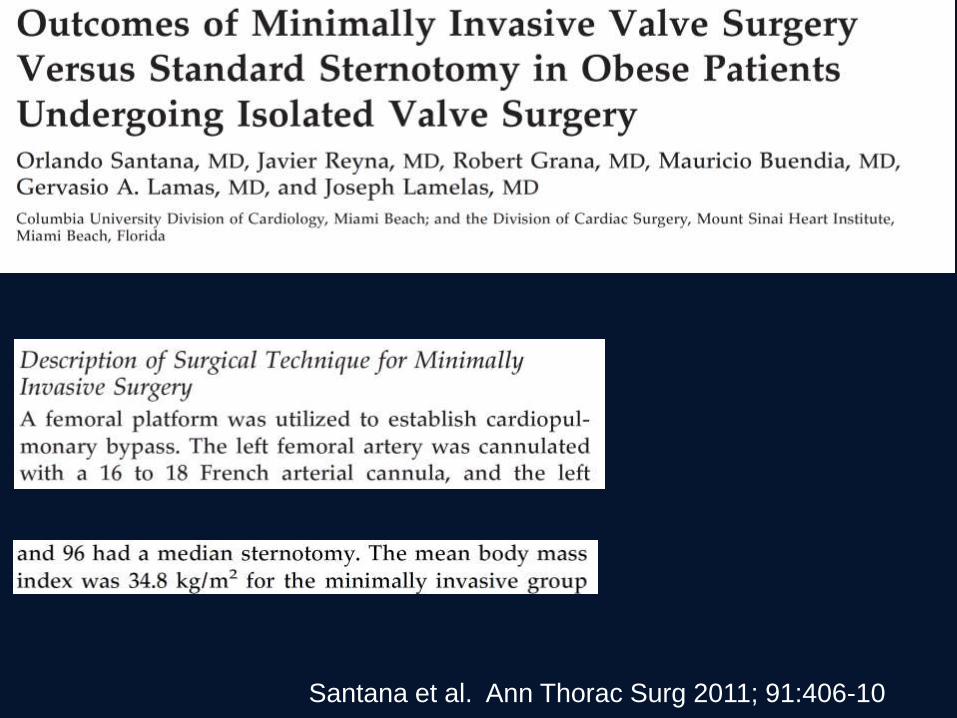
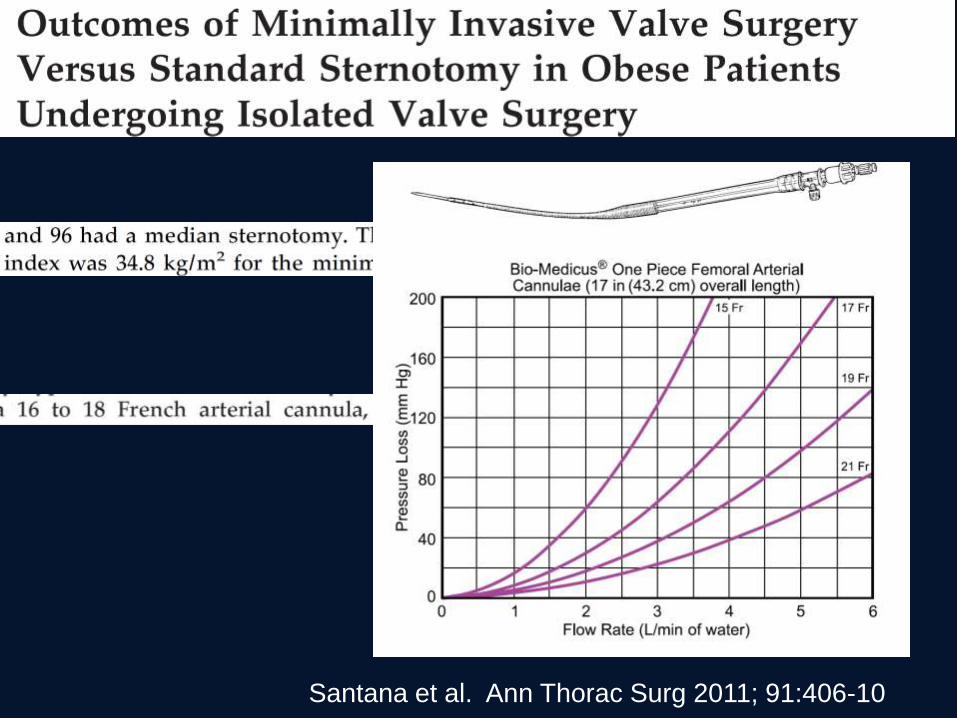
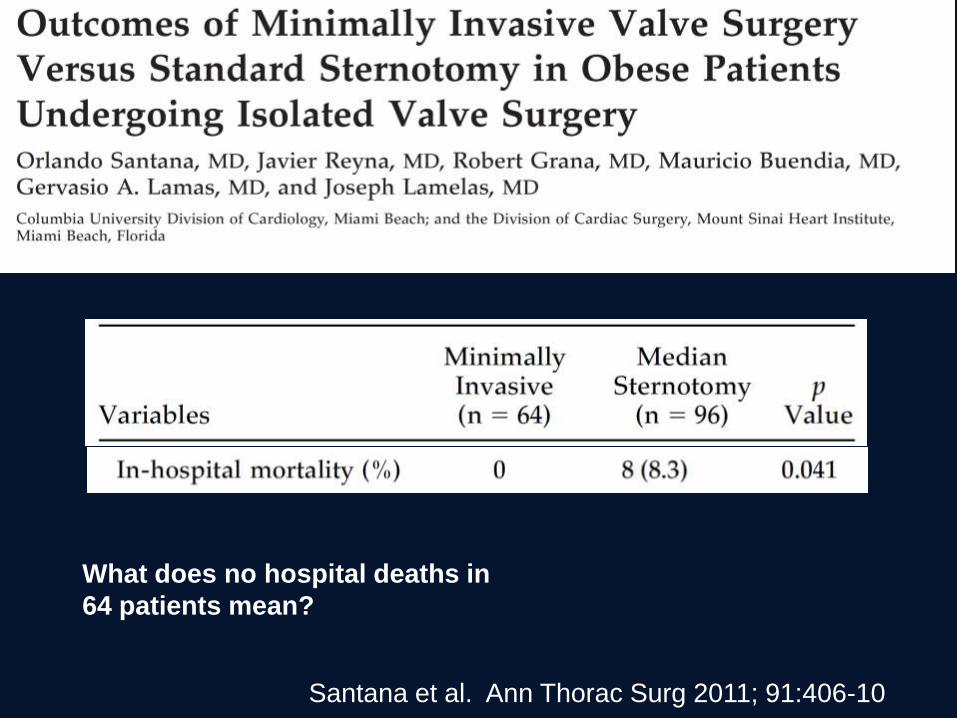
Santana et al. Ann Thorac Surg 2011; 91:406-10
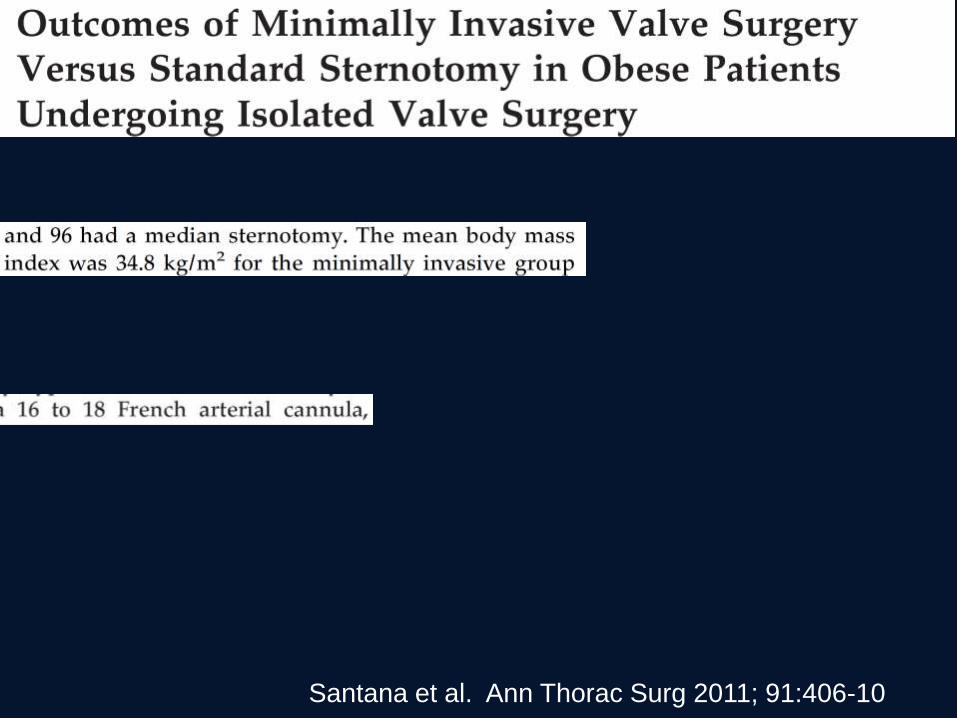
Santana et al. Ann Thorac Surg 2011; 91:406-10
Santana et al. Ann Thorac Surg 2011; 91:406-10
Myth 2) MICS is the same operation
done through lesser access
• There is invariable change in principles and
technique (whether positive or negative)
• The effect of these changes is often not
studied
• Some changes go against traditional surgical
belief and principles
• Tendency to make pathology conform to the
technique
– Everyone gets same technique

Myth 3) MICS does not compromise
valve repair rates
Myth 3) MICS does not compromise
valve repair rates
• It has to by definition
• Primary focus is on incision and not the repair
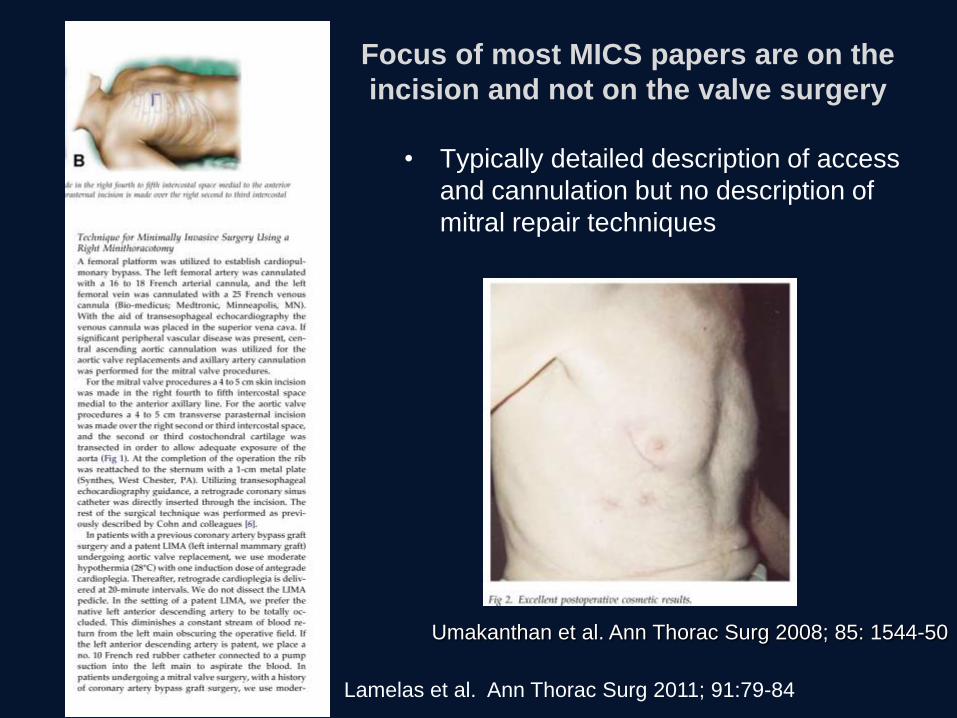
Focus of most MICS papers are on the
incision and not on the valve surgery
• Typically detailed description of access
and cannulation but no description of
mitral repair techniques
Lamelas et al. Ann Thorac Surg 2011; 91:79-84
Umakanthan et al. Ann Thorac Surg 2008; 85: 1544-50
Myth 3) MICS does not compromise
valve repair rates
• It has to by definition
• Primary focus is on incision and not the repair
• Certain repair techniques are more suited to
conventional instrumentation/exposure
• Also some valves are more difficult to repair.
Such valves will be even more difficult with
limited access
– Rheumatic valves
– Congenital
– Calcification

Can difficult repairs be replicated via MICS
or are these valves replaced?
Umakanthan et al. Ann Thorac Surg 2008; 85: 1544-50
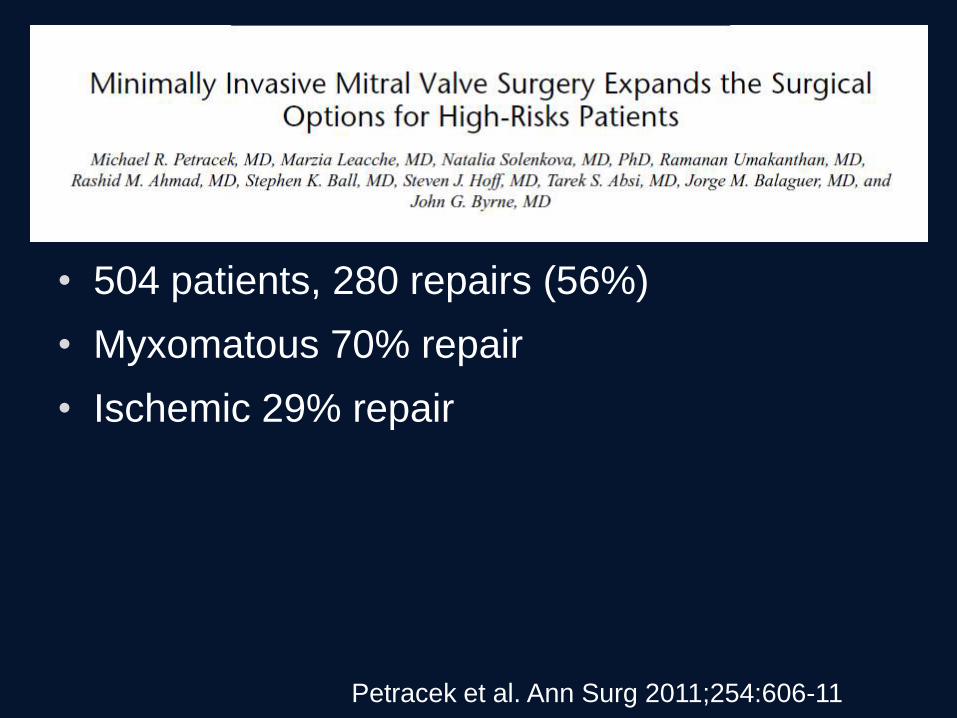
Petracek et al. Ann Surg 2011;254:606-11
• 504 patients, 280 repairs (56%)
• Myxomatous 70% repair
• Ischemic 29% repair
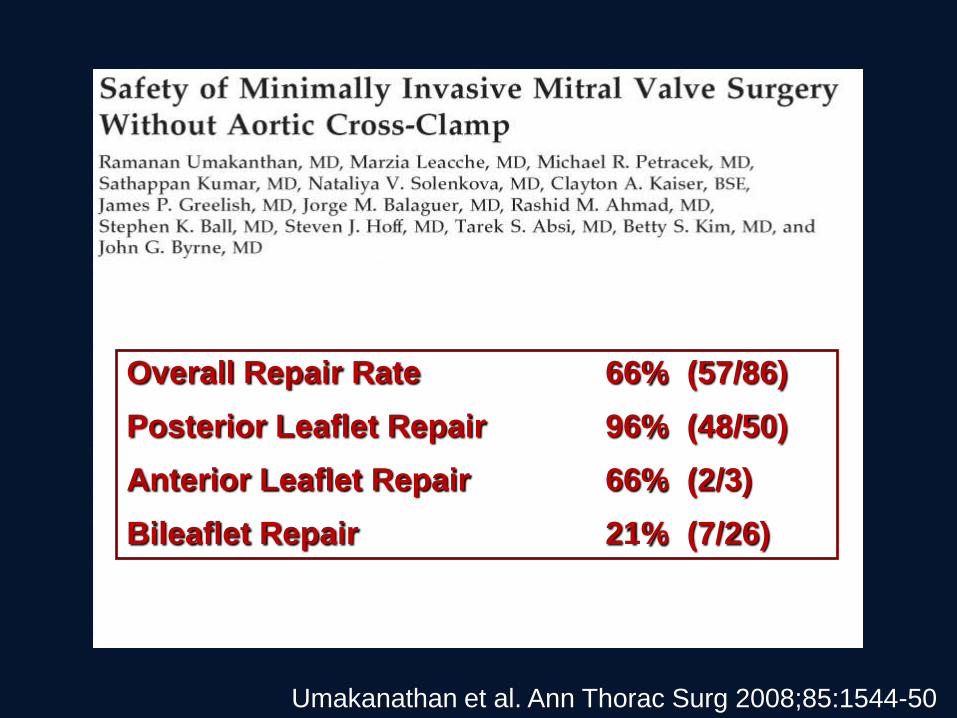
Umakanathan et al. Ann Thorac Surg 2008;85:1544-50
Overall Repair Rate 66% (57/86)
Posterior Leaflet Repair 96% (48/50)
Anterior Leaflet Repair 66% (2/3)
Bileaflet Repair 21% (7/26)
Seeburger et al. Eur J Cardiothorac Surg. 2009 Sep;36(3):532-8
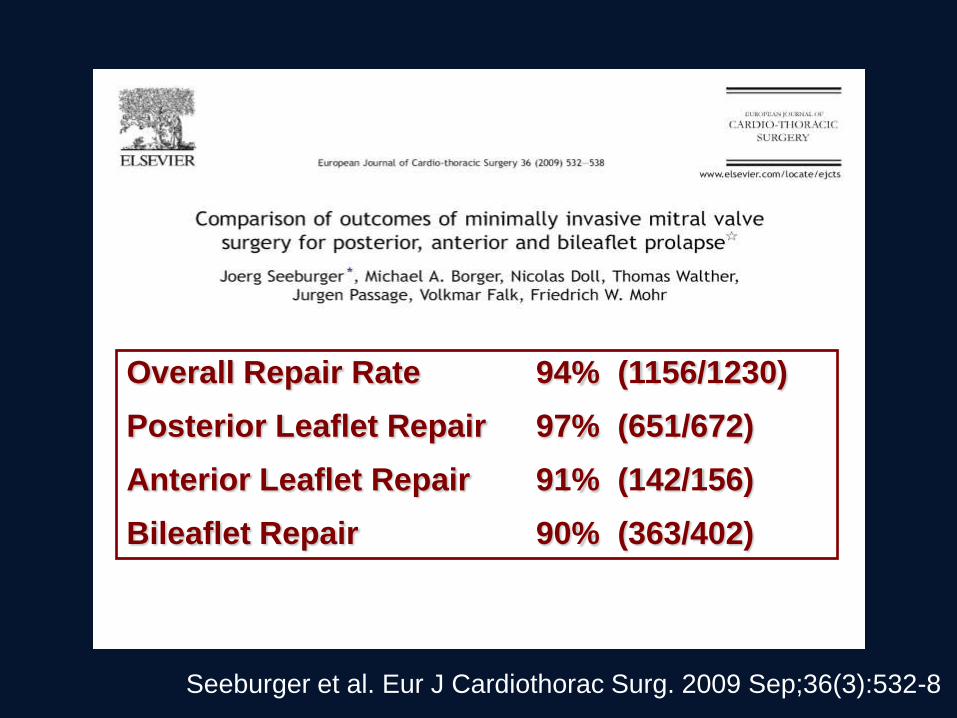
Overall Repair Rate 94% (1156/1230)
Posterior Leaflet Repair 97% (651/672)
Anterior Leaflet Repair 91% (142/156)
Bileaflet Repair 90% (363/402)
Does MICS compromise mitral valve
repair rates?
• Yes
– Maybe less so in the most experienced hands
– Maybe less so in those who have overcome
learning curve
– But otherwise there is direct and indirect evidence
that more valves are being replaced when MICS
is used
Myth 4) MICS is possible in ‘all’
patients
• Patient selection and referral bias gives a
false impression that MICS can be applied
consecutively to all comers without need for
conventional approach
• Even in reference centers, majority of valves
repaired via MICS are simple pathology
• Either via selection of referral patterns,
complex cases are not making there way into
MICS ORs
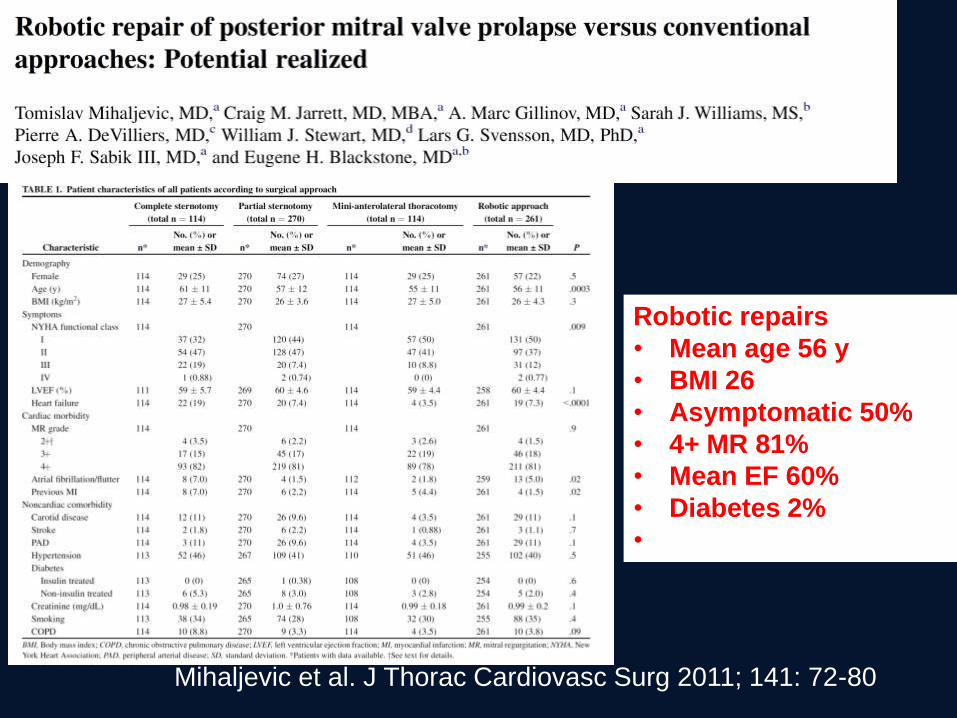
Mihaljevic et al. J Thorac Cardiovasc Surg 2011; 141: 72-80
Robotic repairs
• Mean age 56 y
• BMI 26
• Asymptomatic 50%
• 4+ MR 81%
• Mean EF 60%
• Diabetes 2%
•
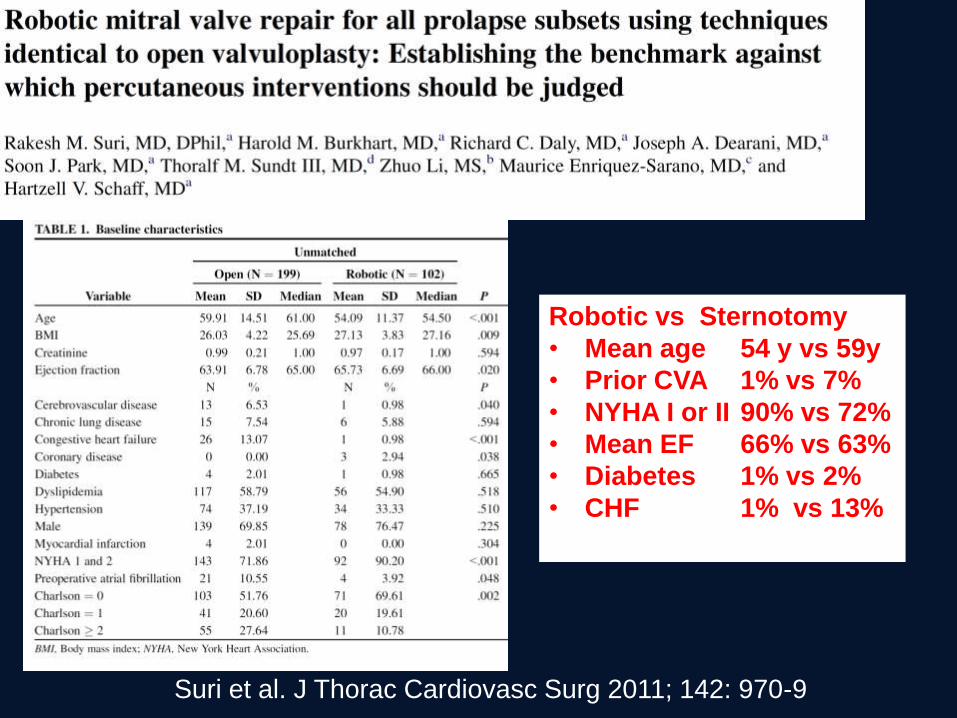
Suri et al. J Thorac Cardiovasc Surg 2011; 142: 970-9
Robotic vs Sternotomy
• Mean age 54 y vs 59y
• Prior CVA 1% vs 7%
• NYHA I or II 90% vs 72%
• Mean EF 66% vs 63%
• Diabetes 1% vs 2%
• CHF 1% vs 13%
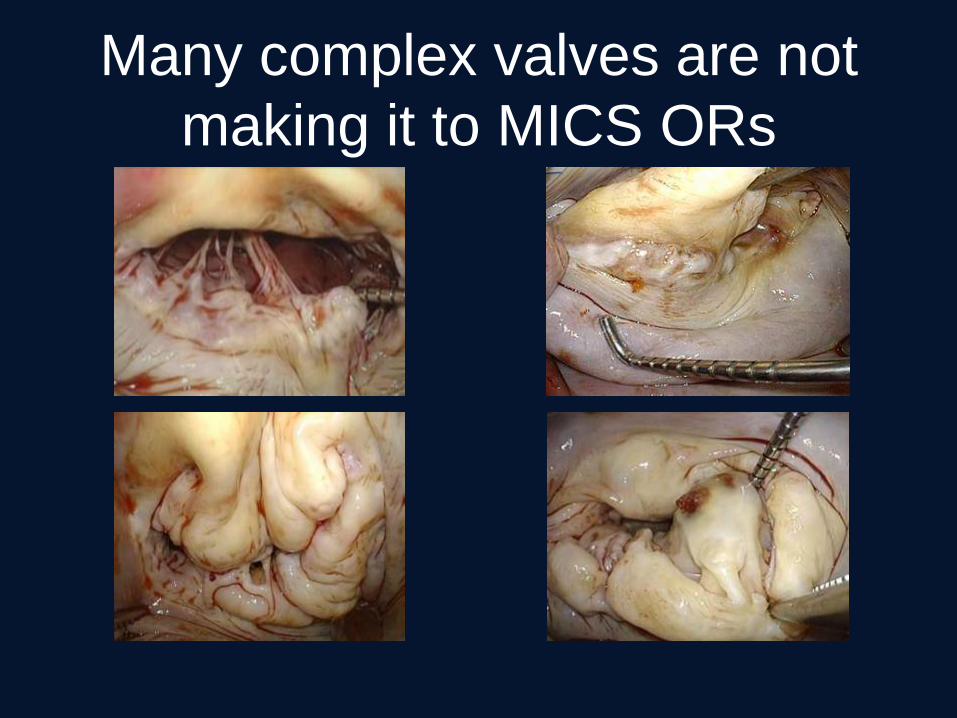
Many complex valves are not
making it to MICS ORs
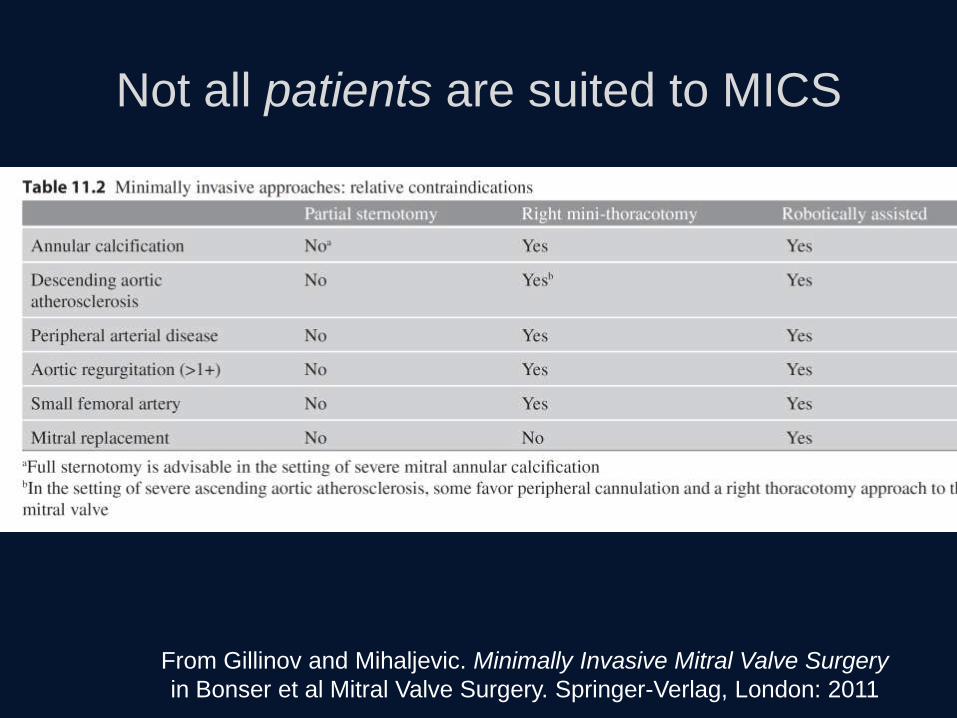
Not all patients are suited to MICS
From Gillinov and Mihaljevic. Minimally Invasive Mitral Valve Surgery
in Bonser et al Mitral Valve Surgery. Springer-Verlag, London: 2011
Myth 5) MICS repair is reproducible by
‘all’ surgeons
• MICS requires unique skill-sets and training
possessed currently limited to only a minority
of surgeons
Myth 5) MICS repair is reproducible by
‘all’ surgeons
• MICS requires unique skill-sets and training
possessed currently limited to only a minority
of surgeons
• Unpredictable learning curve
• Widespread penetration of MICS will likely
compromise patient outcomes
The learning curve
• Takes about 100 cases to become proficient,
efficient, and have stable results* with right
thoracotomy or robotic approach.
Casselman et . J Thorac Cardiovasc Surg 2003; 125: 273-82
Chitwood et al, J Thorac Cardiovasc Surg 2008;136:436
Gammie et al, Ann Surg 2009; 250: 409-15
Cheng et al. J Thorac Cardiovasc Surg 2010; 139: 628
*low complications, high repair rate and durable repair
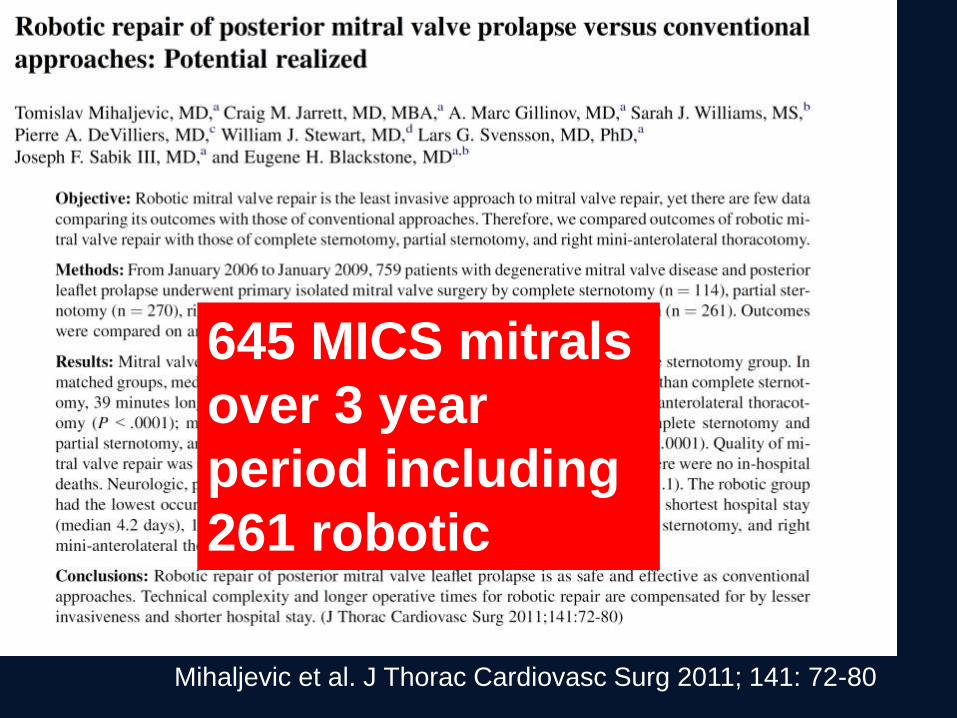
Mihaljevic et al. J Thorac Cardiovasc Surg 2011; 141: 72-80
645 MICS mitrals
over 3 year
period including
261 robotic

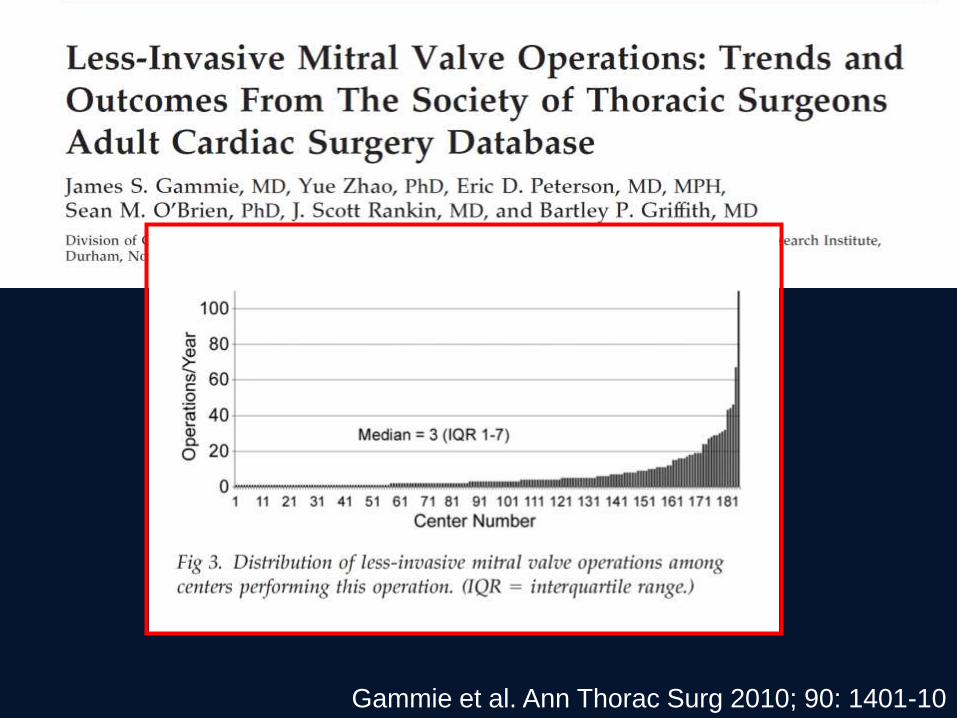
Gammie et al. Ann Thorac Surg 2010; 90: 1401-10

Gammie et al. Ann Thorac Surg 2010; 90: 1401-10
The average surgeon does 3 MICS mitrals per
year
The average surgeon does 3 MICS mitrals per
year
It takes about 100 procedures to gain
proficiency

The average surgeon does 3 MICS mitrals per
year
It takes about 100 procedures to gain
proficiency
• Most surgeons, by definition will never gain
proficiency in their lifetime
• Majority of MICS mitrals, at least in the USA,
are being performed by surgeons who lack
proficiency to do so
The result
Plethora of
• Complications
• Deaths
• Unnecessary valve replacements
• Early failures of repair
• Incomplete procedures
Directly attributable to use of MICS
Myth (6) MICS has been demonstrated
to be non-inferior in outcomes
(6) Has MICS has been demonstrated
to be non-inferior in outcomes?
• Non-inferior results seen in selected reports
from pioneering centers have not been
duplicated in large databases and other
single center series
• Be wary of outcome data from small series
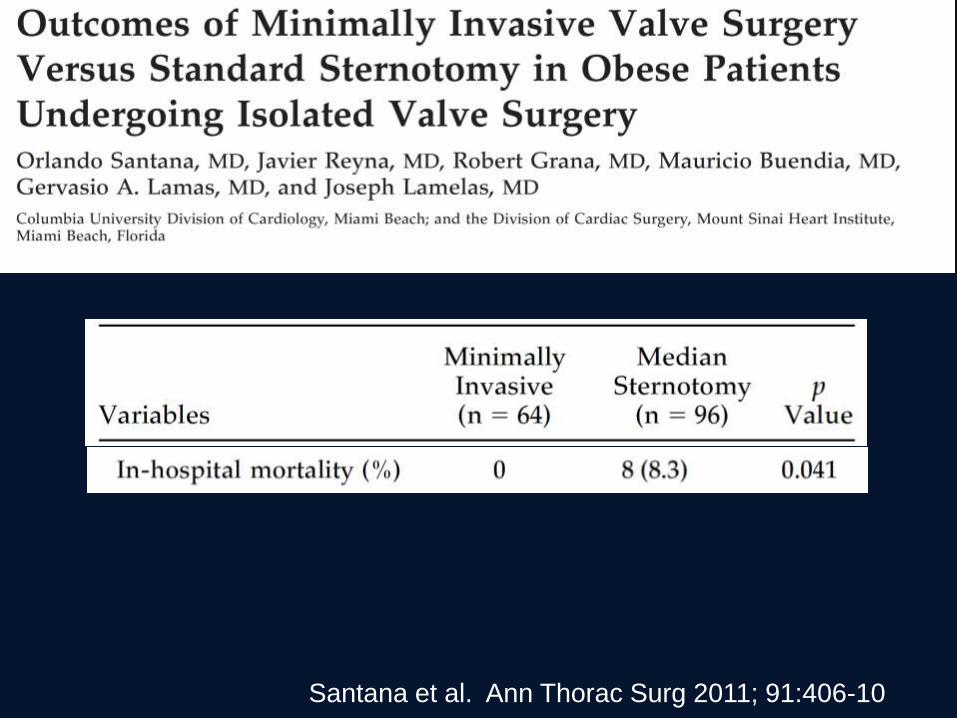
Santana et al. Ann Thorac Surg 2011; 91:406-10
Santana et al. Ann Thorac Surg 2011; 91:406-10
What does no hospital deaths in
64 patients mean?
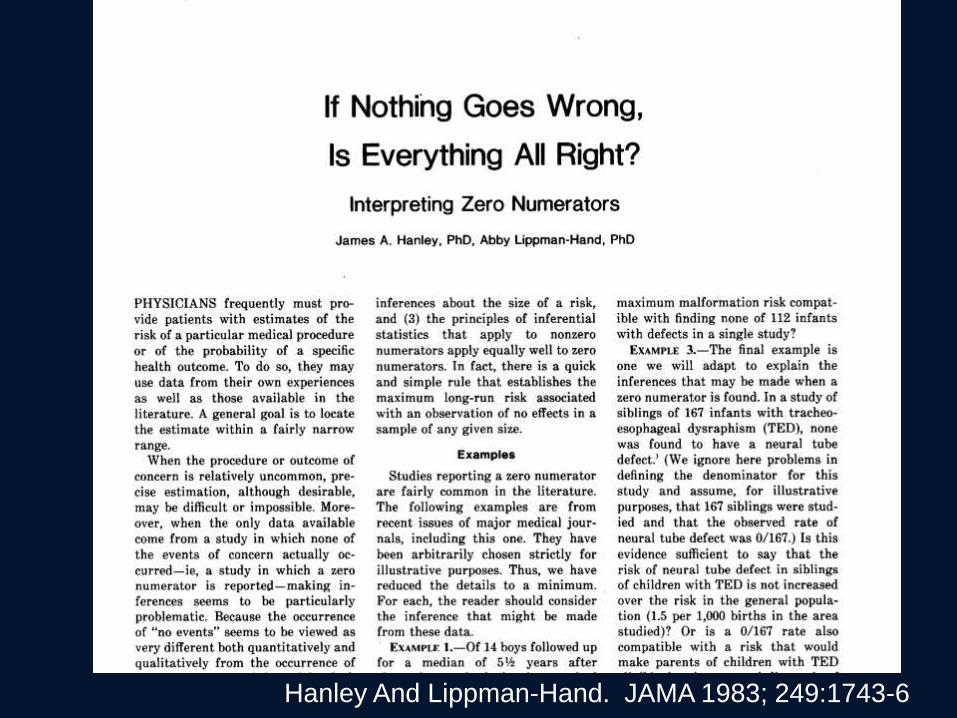
Hanley And Lippman-Hand. JAMA 1983; 249:1743-6
Hanley And Lippman-Hand. JAMA 1983; 249:1743-6
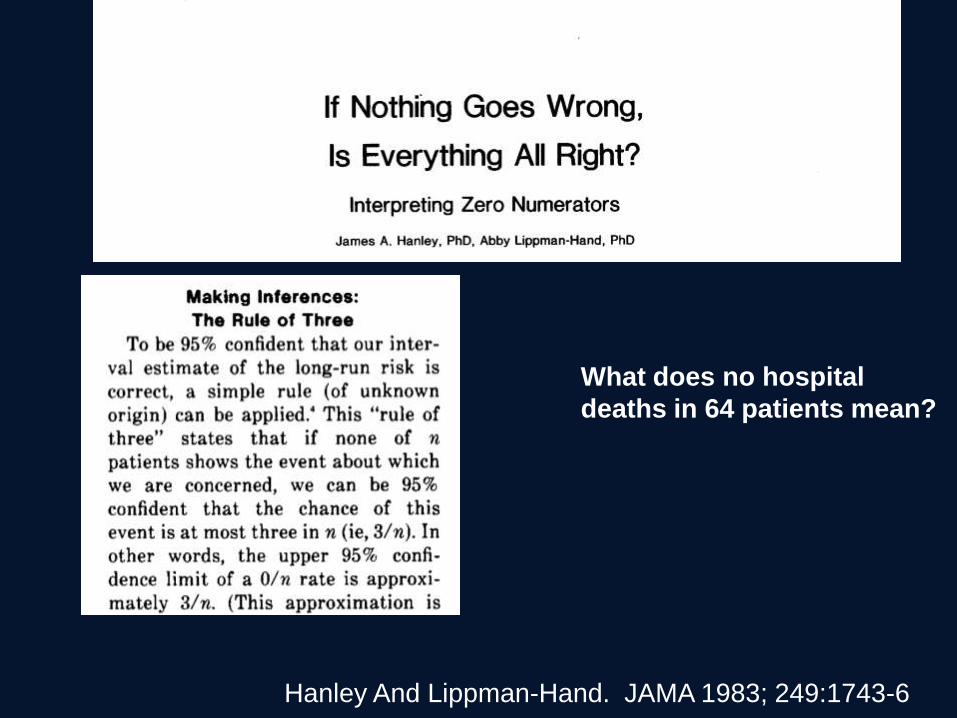
What does no hospital
deaths in 64 patients mean?
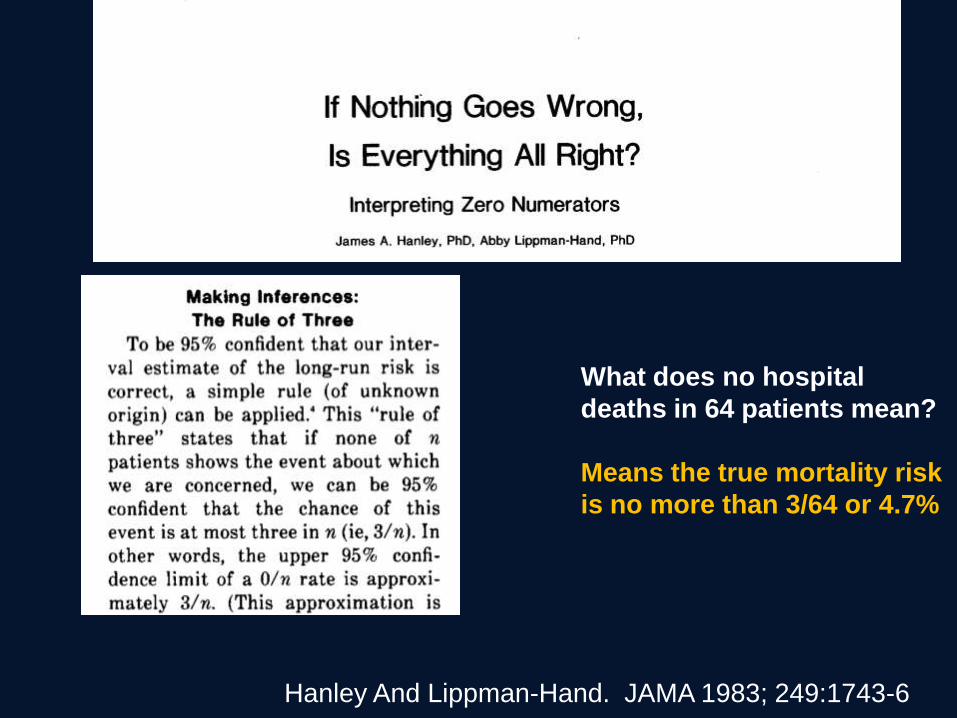
Hanley And Lippman-Hand. JAMA 1983; 249:1743-6
What does no hospital
deaths in 64 patients mean?
Means the true mortality risk
is no more than 3/64 or 4.7%

Hanley And Lippman-Hand. JAMA 1983; 249:1743-6
What does no hospital
deaths in 64 patients mean?
Means the true mortality risk
is no more than 4.7%
One has to do 1000 cases to
be reasonably sure the
mortality risk is <1%
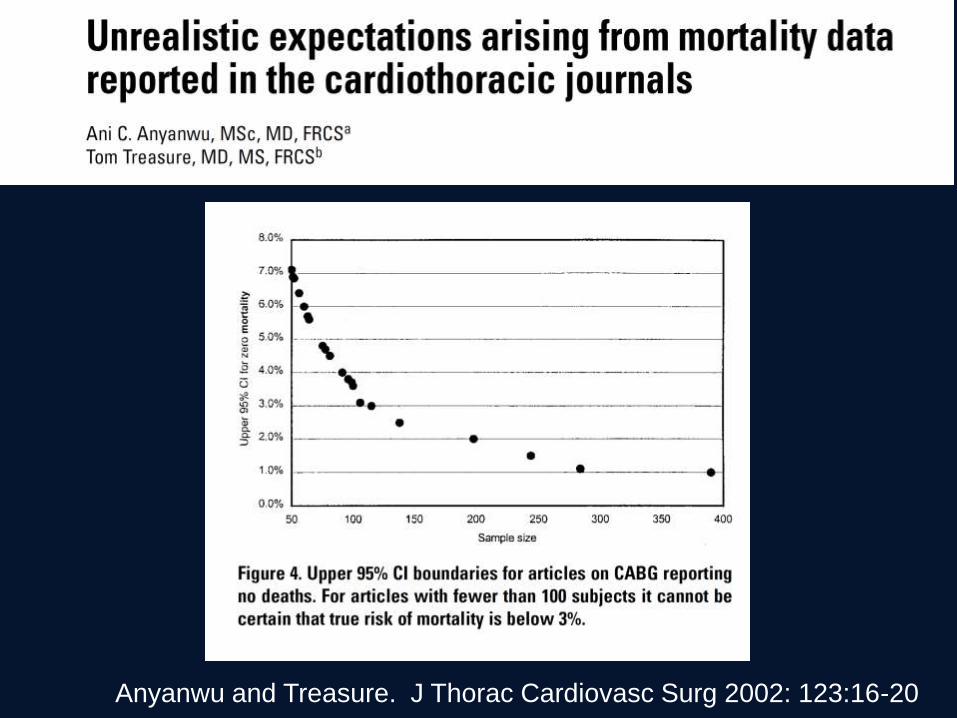
Anyanwu and Treasure. J Thorac Cardiovasc Surg 2002: 123:16-20
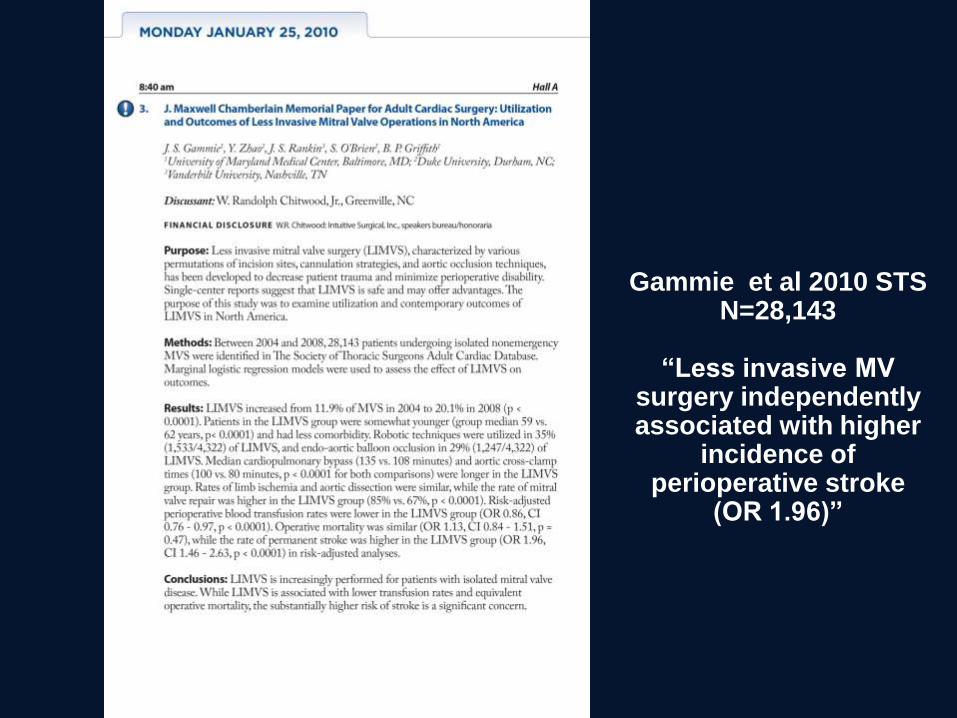
Gammie et al 2010 STS N=28,143
“Less invasive MV
surgery independently associated with higher
incidence of perioperative stroke
(OR 1.96)”
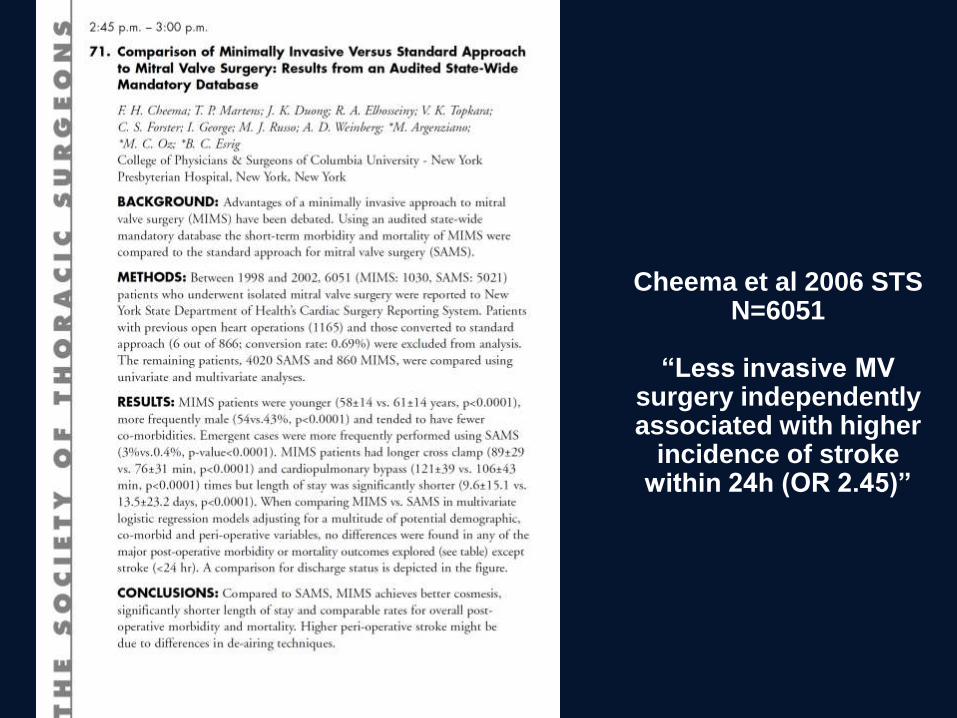
Cheema et al 2006 STS N=6051
“Less invasive MV
surgery independently associated with higher
incidence of stroke within 24h (OR 2.45)”
Petracek et al. Ann Surg 2011;254:606-11
• 504 patients
• Fibrillatory no clamp approach
• Femoral perfusion in 89.5% (rest axillary)
• Mortality 11 (2.2%)
• Stroke or TIA 18 (3.6%)
• 4 fatal strokes (stroke responsible for a third
of deaths)

Raanani et al. J Thorac Cardiovasc Surg 2010; 140:86-90
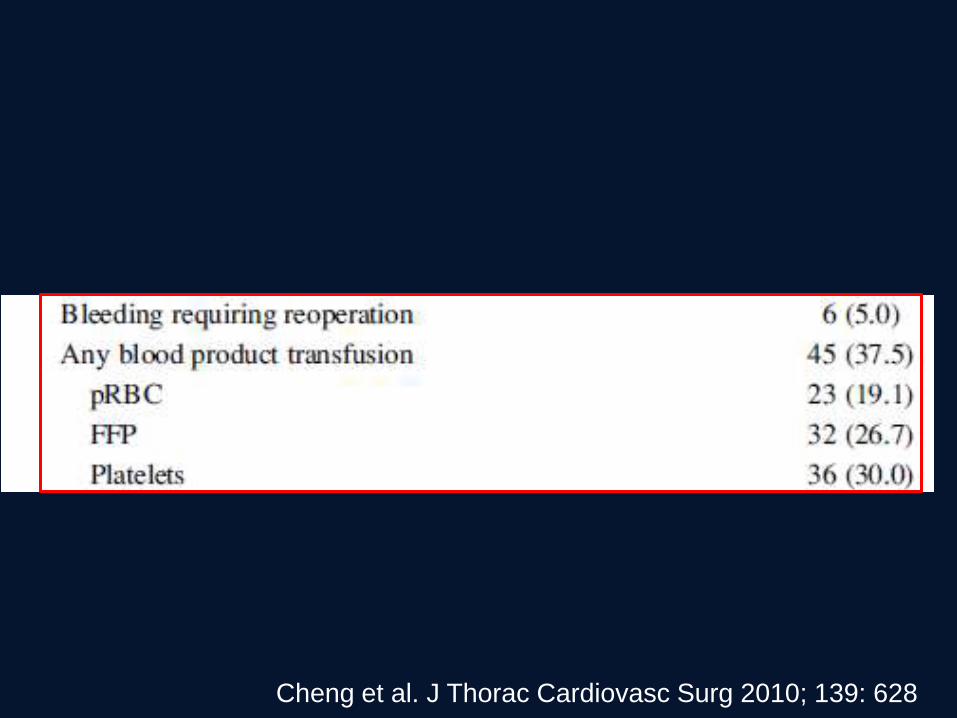
Cheng et al. J Thorac Cardiovasc Surg 2010; 139: 628
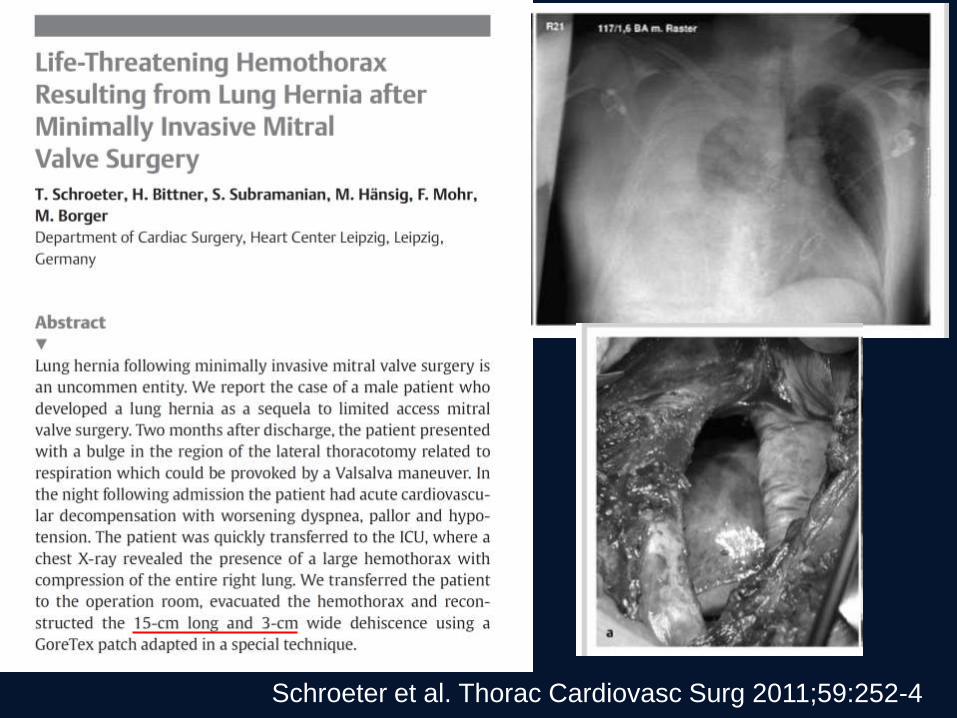
Schroeter et al. Thorac Cardiovasc Surg 2011;59:252-4
There are though some patients too
where Sternotomy is harmful…
• In these patients, MICS is potentially
advantageous
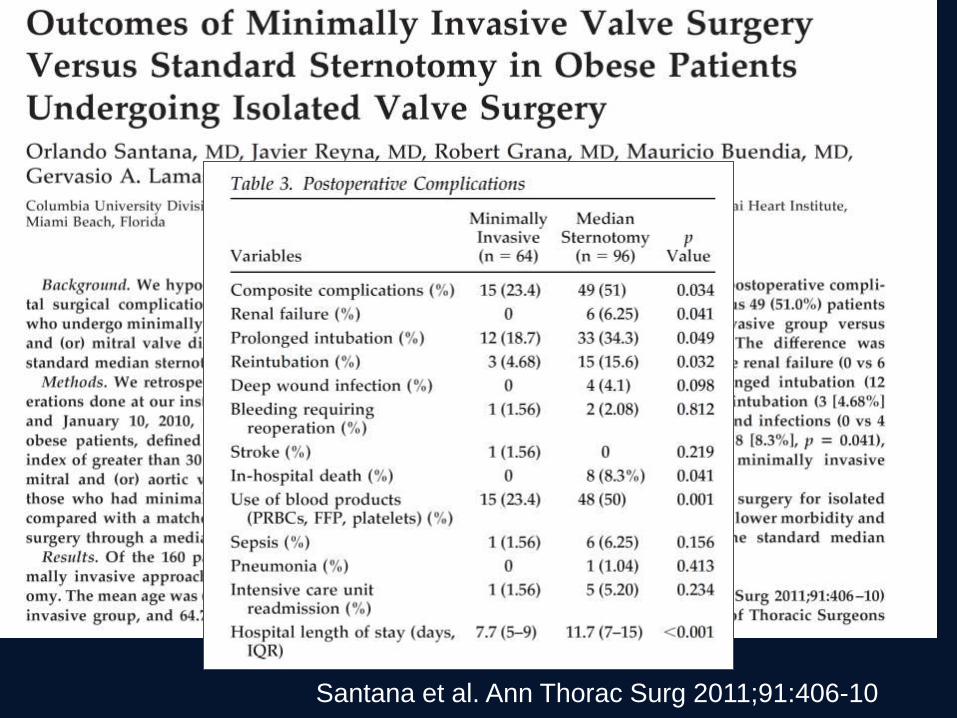
Santana et al. Ann Thorac Surg 2011;91:406-10
Myth 7) Patients recover quicker with
MICS
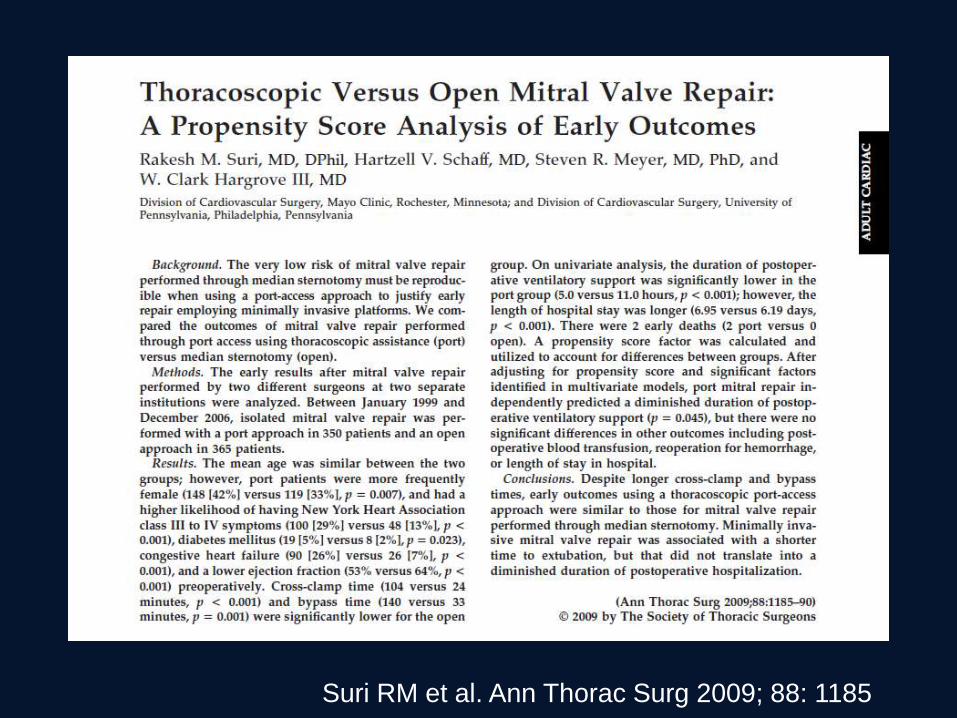
Suri RM et al. Ann Thorac Surg 2009; 88: 1185
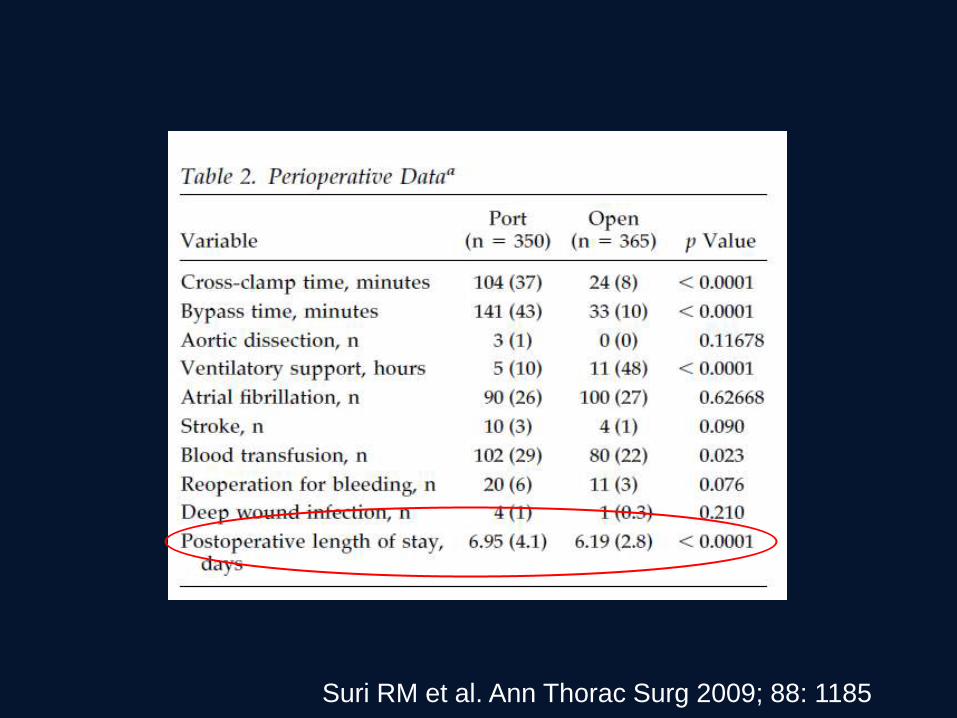
Suri RM et al. Ann Thorac Surg 2009; 88: 1185
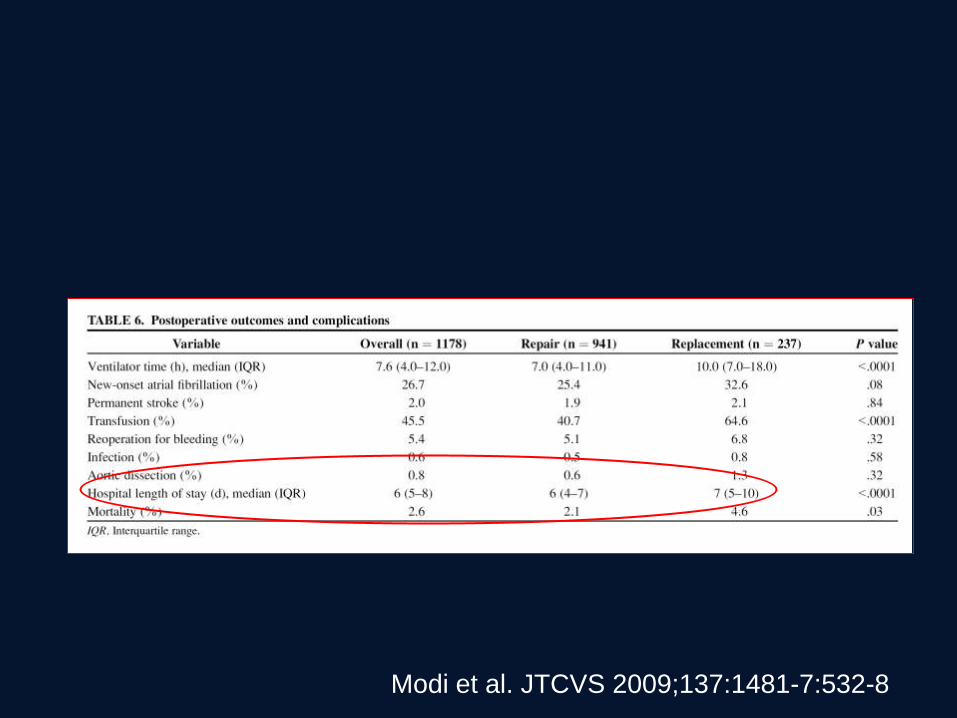
Modi et al. JTCVS 2009;137:1481-7:532-8
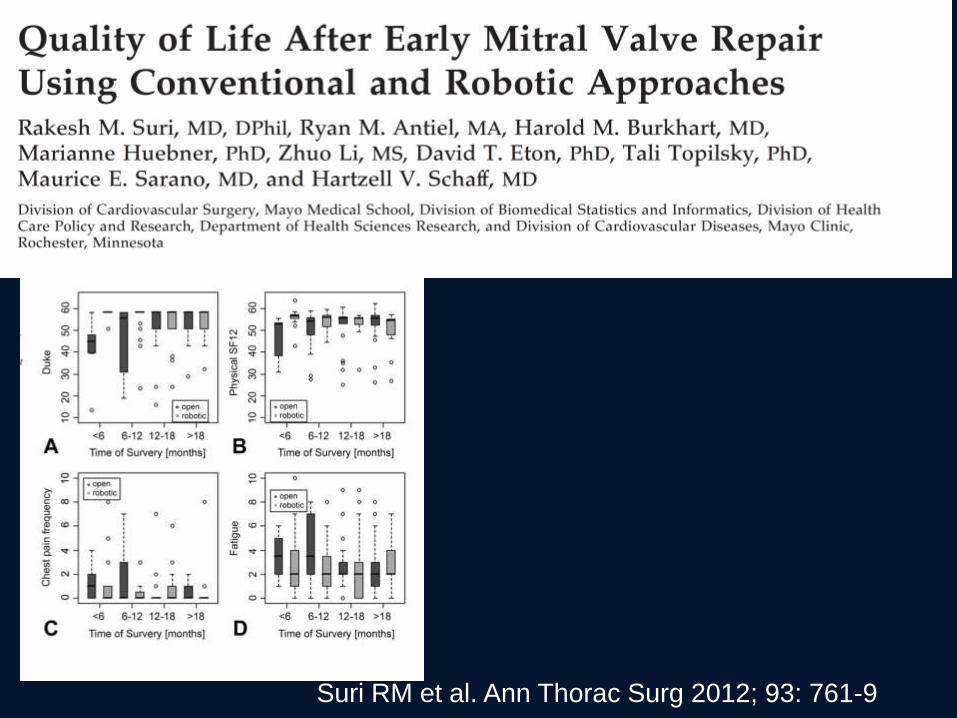
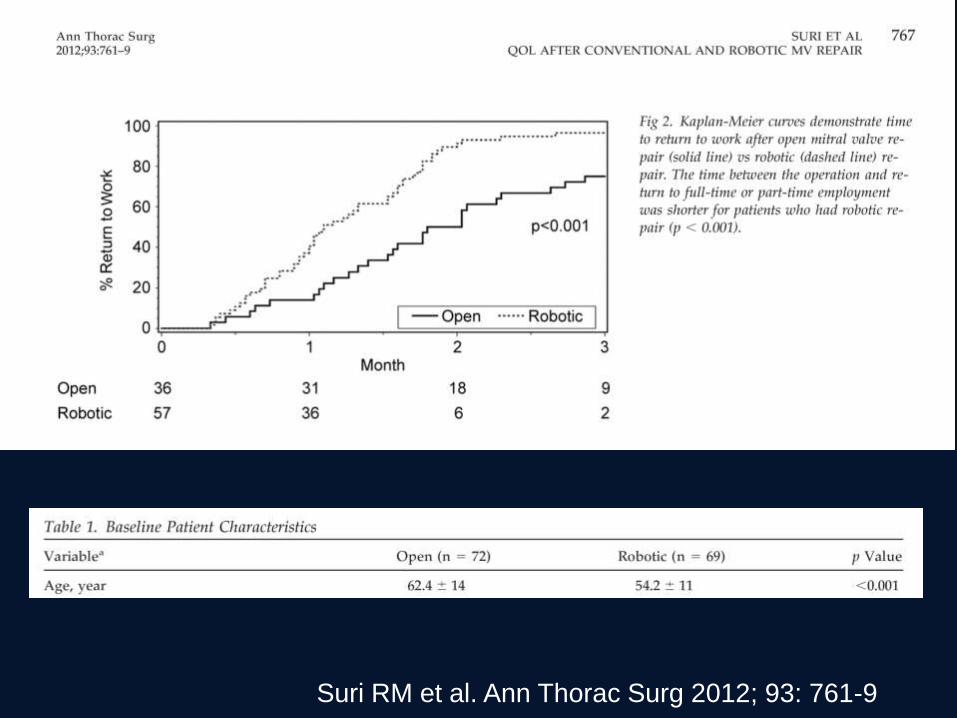
Suri RM et al. Ann Thorac Surg 2012; 93: 761-9
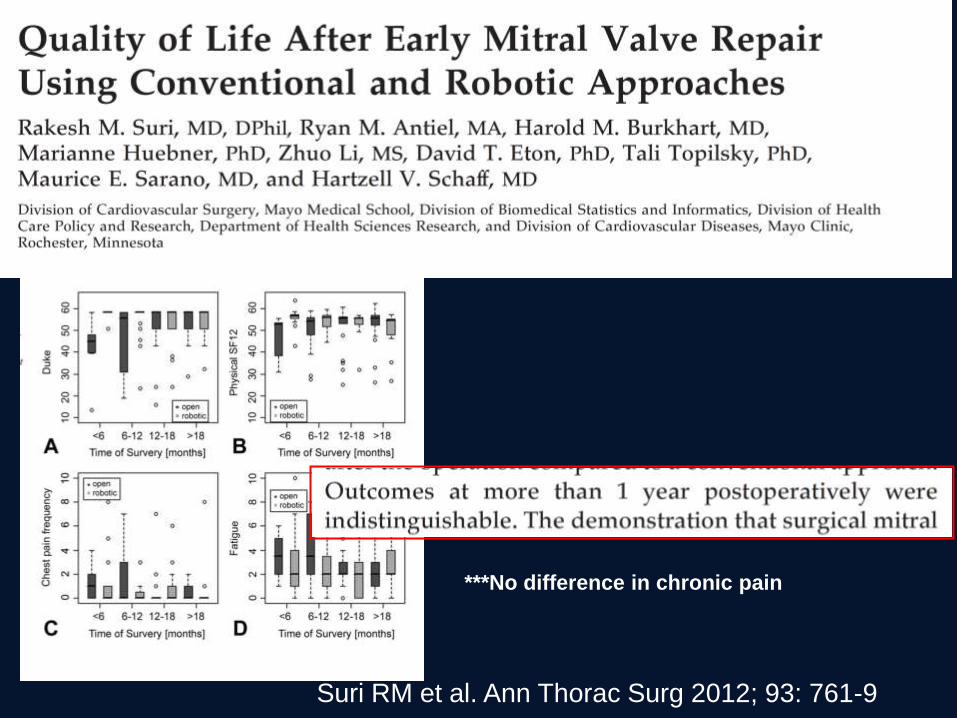
Suri RM et al. Ann Thorac Surg 2012; 93: 761-9
***No difference in chronic pain
Suri RM et al. Ann Thorac Surg 2012; 93: 761-9

Median sternotomy…four weeks later
Median sternotomy…five weeks later
Myth 8) Quality of repair is similar with
MICS
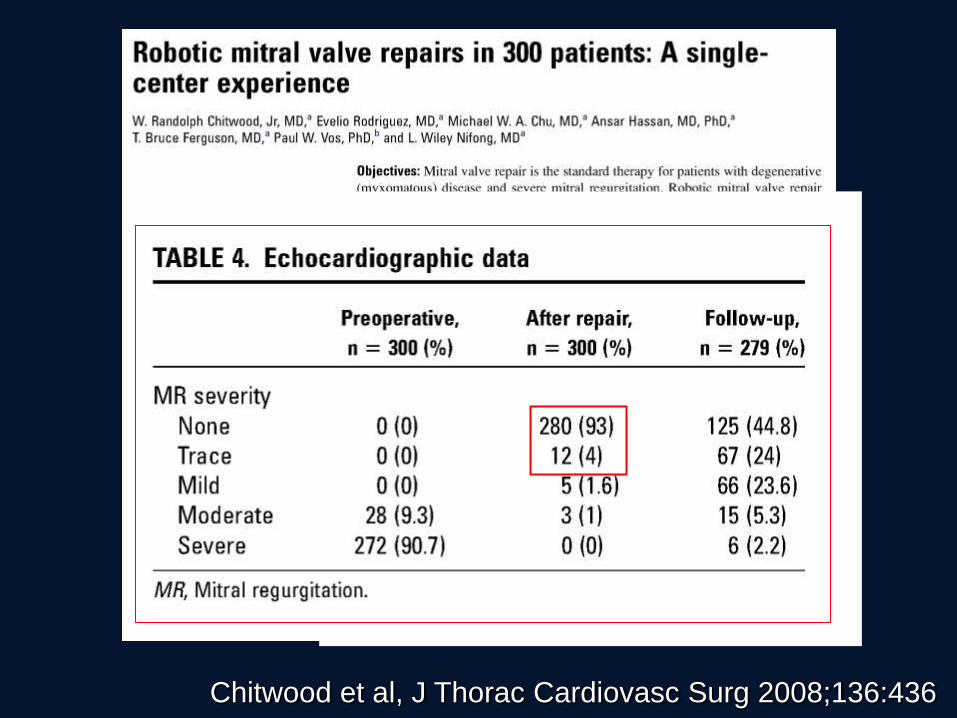
Chitwood et al, J Thorac Cardiovasc Surg 2008;136:436
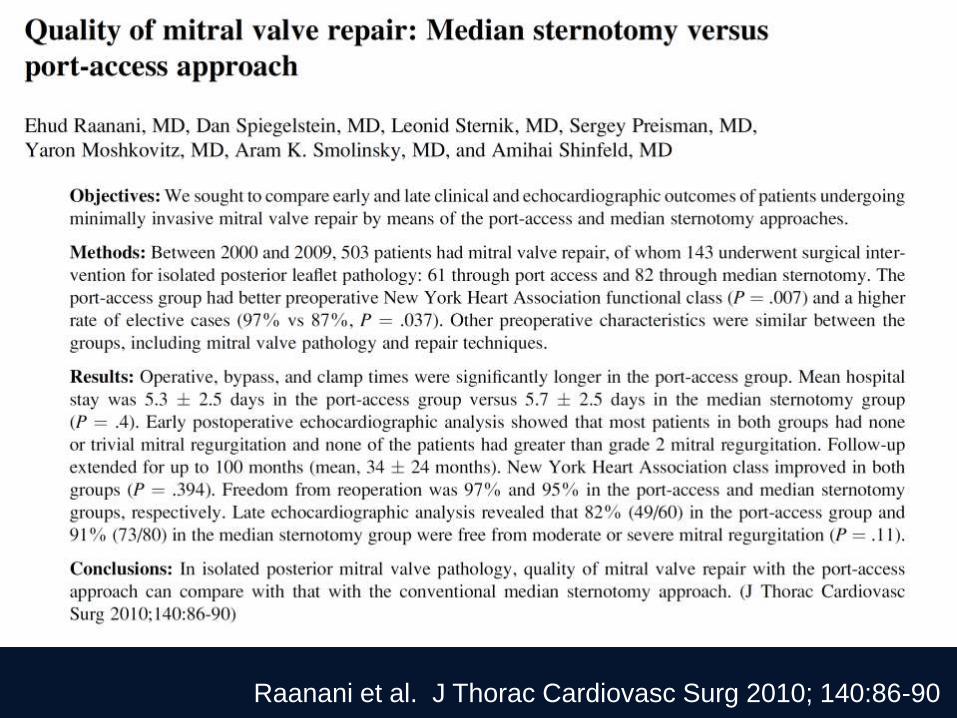
Raanani et al. J Thorac Cardiovasc Surg 2010; 140:86-90

Raanani et al. J Thorac Cardiovasc Surg 2010; 140:86-90
*Posterior Leaflet Pathology only
Cheng et al. J Thorac Cardiovasc Surg 2010; 139: 628
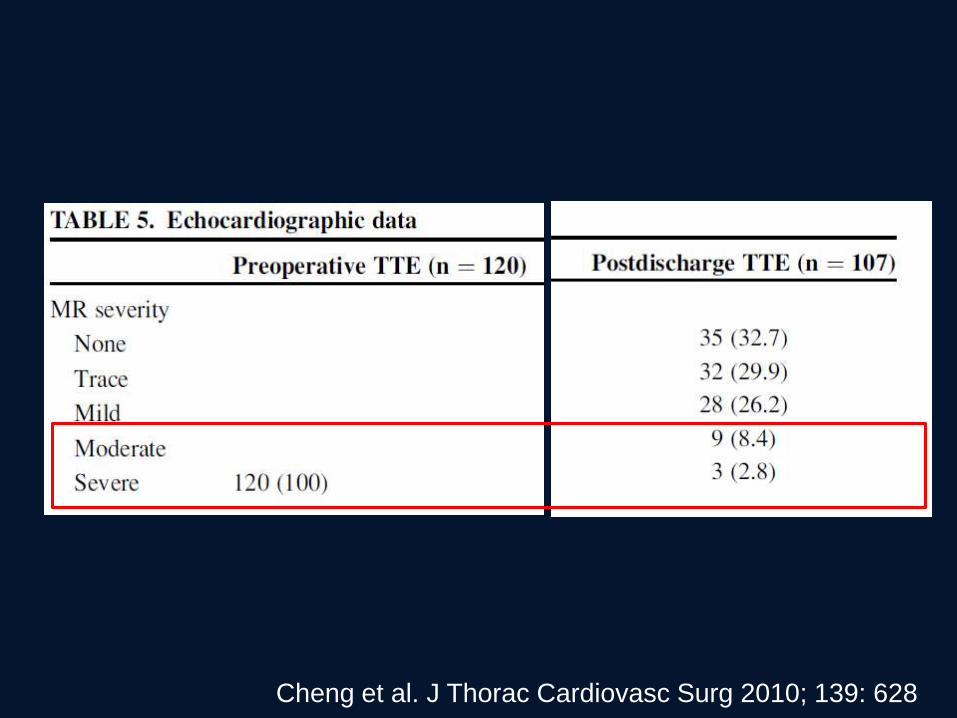
Cheng et al. J Thorac Cardiovasc Surg 2010; 139: 628
Myth 9) MICS is the new standard
9) Is MICS is new standard?
• Reality is little penetration of MICS in recent
years
• Most growth comes from established MICS
centers
Gammie et al. Ann Thorac Surg 2010; 90: 1401-10

Falk et al. Innovations 2011; 6:66-76
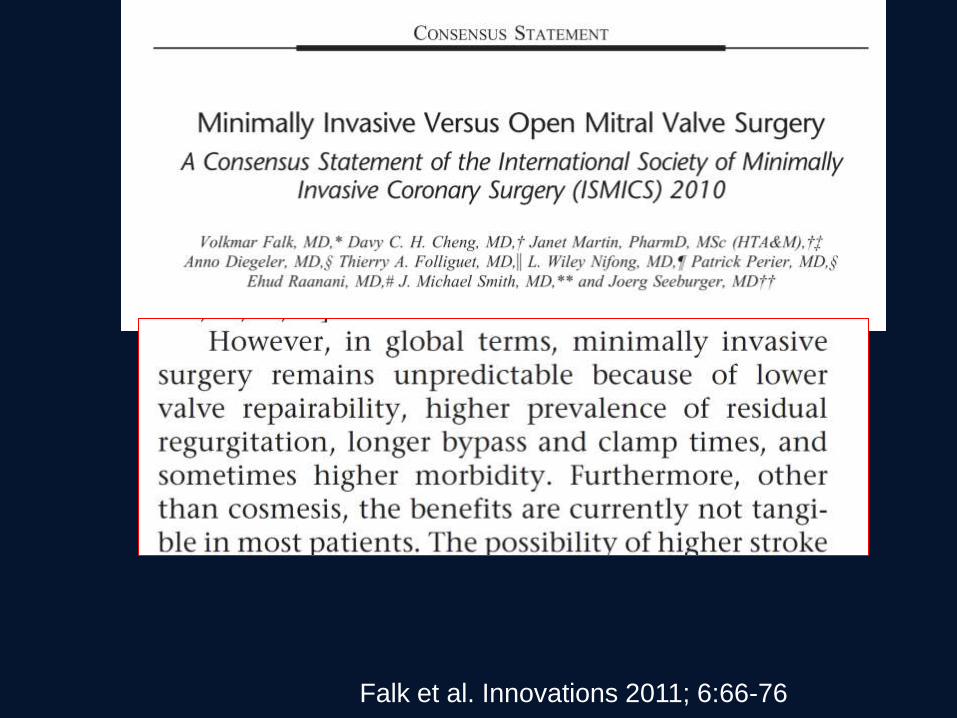
Falk et al. Innovations 2011; 6:66-76
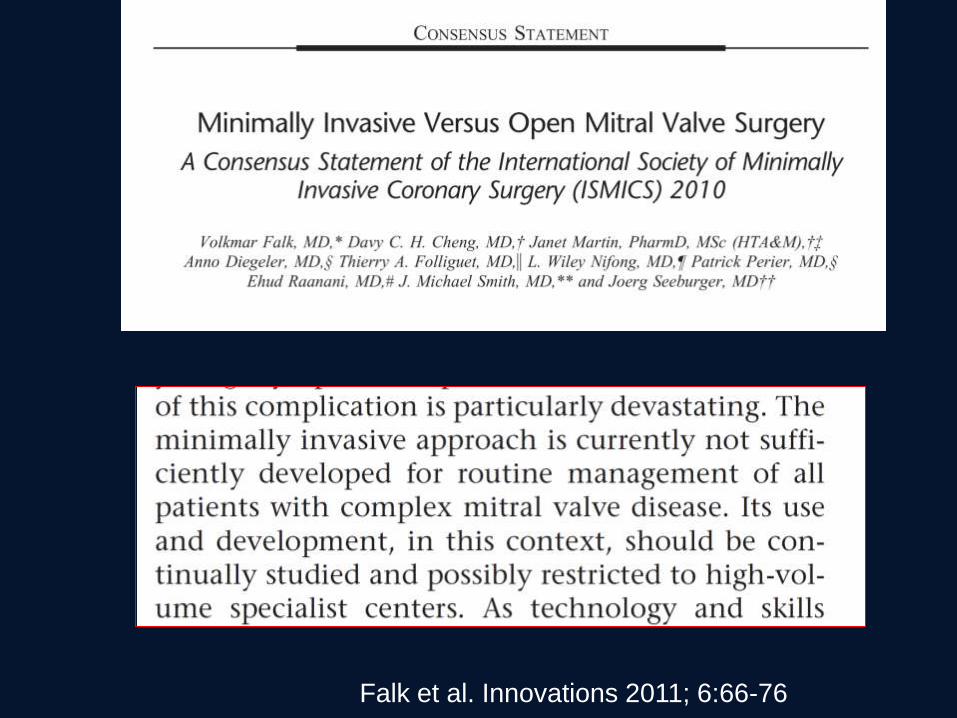
Falk et al. Innovations 2011; 6:66-76
Myth 10) MICS is better for the patient
• Only clear benefit to the patient is cosmesis
• MICS is more a marketing tool for surgical
egos and surgical programs
• MICS does not improve chances of a good
short or long-term outcome for the patient
Lets be honest….
• Only clear patient benefit of MICS is cosmesis
• MICS is largely an expression of the surgical
self
• We like challenges and technical evolution
We like to be at the cutting edge
We like to demonstrate our craft and ability
We like the sexy stuff
What really is best for the patient….
• Adherence to ‘Carpentier principles’ is most
important factor in achieving durable repair
– Competent valve
– Good surface of coaptation
– Preserve mobility and orifice
How the surgeon gets to the valve is of much less
importance
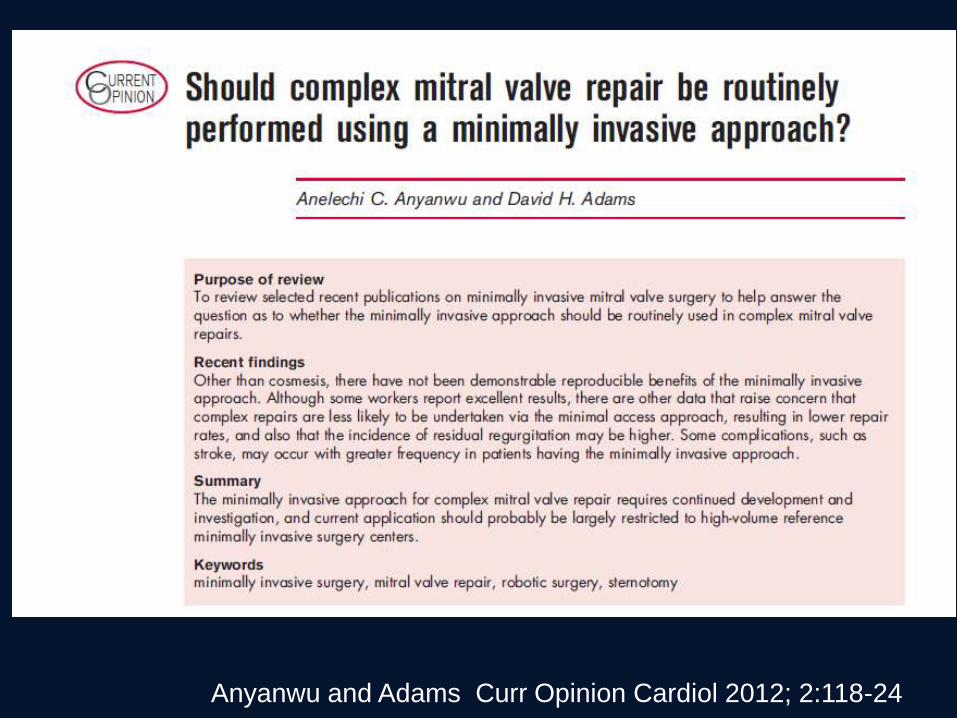
Anyanwu and Adams Curr Opinion Cardiol 2012; 2:118-24
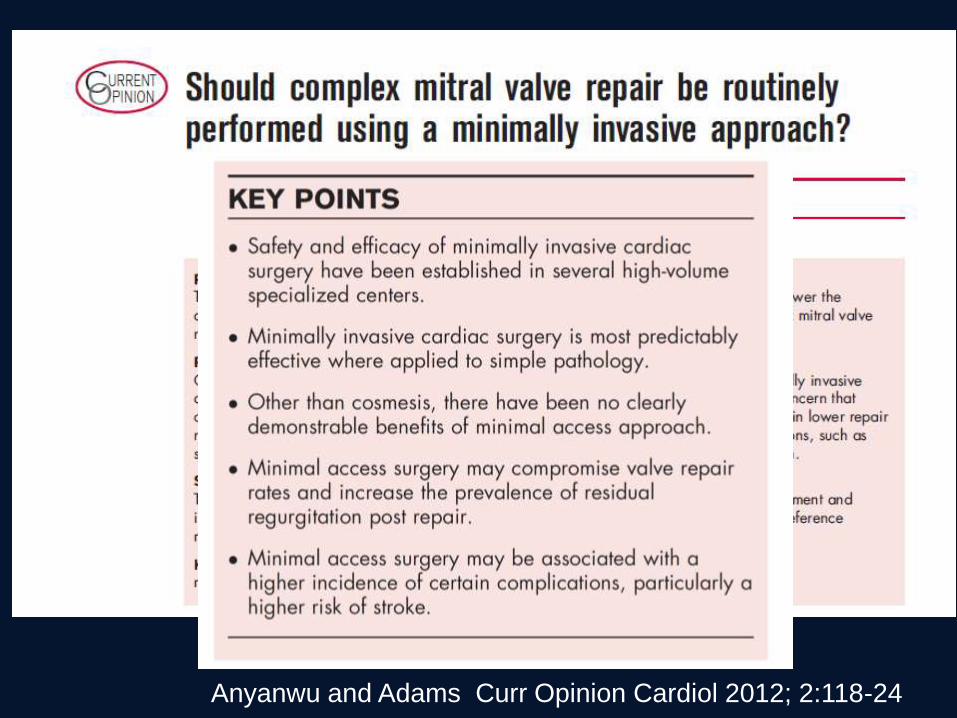
Anyanwu and Adams Curr Opinion Cardiol 2012; 2:118-24

“Mini-MVR Is Better than Conventional MVR” - Con
• There is more morbidity • There is no tangible benefit • Less valves are repaired • Quality of repair is inferior
Thank You





























