Embed Size (px)
Citation preview

Minimal and Moderate Minimal and Moderate SedationSedation
T. J. Gan, M.B., F.R.C.A., M.H.S., Li. Ac.T. J. Gan, M.B., F.R.C.A., M.H.S., Li. Ac.
Professor of AnesthesiologyProfessor of Anesthesiology
Vice Chair for Clinical ResearchVice Chair for Clinical Research
Duke University Medical CenterDuke University Medical Center

ContentContent
Why sedation?Why sedation?
Current sedation practiceCurrent sedation practice
Guidelines from professional society Guidelines from professional society governing sedation practicegoverning sedation practice
Pharmacologic properties of sedatives Pharmacologic properties of sedatives
Monitoring of patients undergoing sedationMonitoring of patients undergoing sedation
Clinical data on fospropofol for sedationClinical data on fospropofol for sedation

Procedural SedationProcedural SedationOver 40 million procedures performed each Over 40 million procedures performed each year with moderate sedationyear with moderate sedation
About 23 millions endoscopic procedures About 23 millions endoscopic procedures performed annuallyperformed annually
Depending of the intended level of sedation, Depending of the intended level of sedation, sedation is performed by trained nurses as well sedation is performed by trained nurses as well as anesthesia personnelas anesthesia personnel
Approximately two-thirds of the endoscopic Approximately two-thirds of the endoscopic procedural sedation performed by non procedural sedation performed by non anesthesia personnelanesthesia personnel

Importance of SedationImportance of Sedation
Relief of anxiety and fearRelief of anxiety and fear
Relief of discomfortRelief of discomfort
Increase patient compliance with Increase patient compliance with screening/surveillance guidelinesscreening/surveillance guidelines
Enhance quality of the examinationEnhance quality of the examination
Minimize risks and physical injury to the Minimize risks and physical injury to the patientspatients
Improve over experience and satisfactionImprove over experience and satisfaction

Common Sedation SitesCommon Sedation Sites
ColonoscopyColonoscopy
BronchoscopyBronchoscopy
GastroscopyGastroscopy
cardiac catheterizationcardiac catheterization
Office based outpatient surgeryOffice based outpatient surgery
Emergency department Emergency department

ColonoscopyColonoscopy
SafeSafe
Complications can occurComplications can occur
Majority are cardiopulmonary Majority are cardiopulmonary complications, e.g. over sedation, complications, e.g. over sedation, hypoventilation, aspiration, vasovagalhypoventilation, aspiration, vasovagal
CV complication rate: 2-4/1000CV complication rate: 2-4/1000
Patients at risk: elderly, morbidly obesePatients at risk: elderly, morbidly obese

Overview of agents used for Overview of agents used for minimal to moderate sedationminimal to moderate sedation

88
Characteristics of an Ideal SedativeCharacteristics of an Ideal Sedative
Rapid onset of action allows rapid recovery after discontinuationRapid onset of action allows rapid recovery after discontinuation11
Effective at providing adequate sedation with predictable dose Effective at providing adequate sedation with predictable dose responseresponse1,21,2
Easy to administerEasy to administer1,31,3
Lack of drug accumulationLack of drug accumulation11
Few adverse effectsFew adverse effects1-31-3
Minimal adverse interactions with other drugsMinimal adverse interactions with other drugs1-31-3
Predictable dose responsePredictable dose response22
Cost-effectiveCost-effective33
1Ostermann ME, et al. JAMA. 2000;283:1451-1459.2Jacobi et al. Crit Care Med. 2002;30:119-141.
3Dasta JF, et al. Pharmacother. 2006;26:798-805.4Nelson LE, et al. Anesthesiol. 2003;98:428-436.

Pharmacological Agents in MACPharmacological Agents in MAC
HypnoticsHypnotics– MidazolamMidazolam– PropofolPropofol– MethohexitalMethohexital– KetamineKetamine– Nitrous oxideNitrous oxide– DexmedetomidineDexmedetomidine
• AnalgesicsAnalgesics– OpioidsOpioids
– FentanylFentanyl– MeperidineMeperidine– HydromorphoneHydromorphone– MorphineMorphine
– Local anestheticsLocal anesthetics– NSAIDSNSAIDS

Current Sedation PracticeCurrent Sedation Practice
99% of colonoscopies are performed with 99% of colonoscopies are performed with sedationsedation– 75% with benzodiazepine and opioid75% with benzodiazepine and opioid– 25% with propofol and opioid25% with propofol and opioid
93% sedation with propofol performed with the 93% sedation with propofol performed with the presence of anesthesia professionalpresence of anesthesia professional
Cohen et al. Am J Gastroenterol 2006;101:967-74

Sedation StandardSedation StandardDrugs Used in SedationDrugs Used in Sedation
Opioid and Benzodiazepine combinationOpioid and Benzodiazepine combination
BenefitsBenefits– 1 + 1 = 41 + 1 = 4– Effective in 85% of patientsEffective in 85% of patients– Reversal drugs availableReversal drugs available
ChallengesChallenges– Significant pharmacodynamic variabilitySignificant pharmacodynamic variability– Drug interactionsDrug interactions– Potential for respiratory depressionPotential for respiratory depression
Cohen L. Gastroenterology 2007;133-675-701

Challenges ContinuedChallenges Continued
ChallengesChallenges– Delayed recovery, not “clear headed”Delayed recovery, not “clear headed”– Patients unable to recall postprocedural Patients unable to recall postprocedural
discussionsdiscussions– Potential for nausea and vomiting, drowsinessPotential for nausea and vomiting, drowsiness– Duration of effect may persist for more than Duration of effect may persist for more than
24 hours24 hours
Jonas DE. AM J Gastroenterol 2007;102;2401-10

MidazolamMidazolam
Highly lipophilic Highly lipophilic Onset of action in 1 to 2 minutes Onset of action in 1 to 2 minutes Offset: rapid redistributionOffset: rapid redistribution
TT1/21/2= 1.8-6.4 hrs = 1.8-6.4 hrs
Metabolism - hepatic and renal routesMetabolism - hepatic and renal routesProlonged action in elderly, hepatic and Prolonged action in elderly, hepatic and renally impaired renally impaired >65 – use half doses>65 – use half doses

MidazolamMidazolam
wide range of midazolam blood levels wide range of midazolam blood levels associated with adequate sedation associated with adequate sedation
Alcoholics: decreased sensitivity to drugAlcoholics: decreased sensitivity to drug
Elderly: greater depressant effects Elderly: greater depressant effects
Stimulatory effects in some patientsStimulatory effects in some patients
cytochrome P450 (CYP) 3A4 oxidases cytochrome P450 (CYP) 3A4 oxidases

DiazepamDiazepam
longer half-lifelonger half-life
a greater chance of phlebitisa greater chance of phlebitis
has less amnestic propertieshas less amnestic properties
initial bolus of 2.5 to 5.0 mg.initial bolus of 2.5 to 5.0 mg.
Incremental doses of 2.5 mg can be given Incremental doses of 2.5 mg can be given in 3 to 4 minute intervals.in 3 to 4 minute intervals.

OpioidsOpioids
FentanylFentanyl– Synthetic opioidSynthetic opioid– Fast onsetFast onset– 25-50 mcg, total doses <200 mcg25-50 mcg, total doses <200 mcg– Titrate to comfort Titrate to comfort
MeperidineMeperidine– 50-100 mg50-100 mg
HydromorphoneHydromorphone

Pharmacological AntagonistsPharmacological AntagonistsFlumazenilFlumazenil– For reversing benzodiazepinesFor reversing benzodiazepines– Does not reverse respiratory depressionDoes not reverse respiratory depression– 0.2 mg boluses up to 3 mg0.2 mg boluses up to 3 mg– Risk of resedationRisk of resedation
NaloxoneNaloxone– Central opioid antagonistCentral opioid antagonist– Short acting, renarcotization riskShort acting, renarcotization risk– 40-100 mcg40-100 mcg– Risk of pulmonary edemaRisk of pulmonary edema

http://www.asahq.org/publicationsAndServices/standards/20.pdf, 2004
Continuum of Depth of SedationContinuum of Depth of Sedation

Standards for procedural Standards for procedural monitoring for minimal to monitoring for minimal to
moderate sedationmoderate sedation

Evaluation of Patients Evaluation of Patients Undergoing SedationUndergoing Sedation
History and physical examHistory and physical exam
Review of current medications and Review of current medications and allergiesallergies
Assessment of cardiopulmonary statusAssessment of cardiopulmonary status
Patient instruction – e.g. NPO Patient instruction – e.g. NPO

Sedation-related risk factors Sedation-related risk factors
Sedation-related risk factors include:Sedation-related risk factors include:– significant medical conditions suchsignificant medical conditions suchas as
extremes of age, severe pulmonary, cardiac, extremes of age, severe pulmonary, cardiac, renal or hepatic disease, pregnancy, renal or hepatic disease, pregnancy,
– the abuse of drugs or alcoholthe abuse of drugs or alcohol– uncooperative patientsuncooperative patients– a potentially difficult airway for intubation.a potentially difficult airway for intubation.

MonitoringMonitoring
Patients undergoing endoscopic Patients undergoing endoscopic procedures with moderate or deep procedures with moderate or deep sedation must have continuous monitoring sedation must have continuous monitoring before, during, and after the administration before, during, and after the administration of sedatives.of sedatives.
Standard monitoring Standard monitoring – heart rate (ECG), blood pressure, respiratory heart rate (ECG), blood pressure, respiratory
rate, and oxygen saturation rate, and oxygen saturation

Monitoring for SedationMonitoring for Sedation
Nurse-Patient interactionNurse-Patient interaction
Sedation Scores – Ramsay, OAAS/SSedation Scores – Ramsay, OAAS/S
MonitorsMonitors– Pulse oximetryPulse oximetry– ET CO2ET CO2– Depth of sedation monitor: EEG basedDepth of sedation monitor: EEG based
BIS, Sedline, AEP, EntropyBIS, Sedline, AEP, Entropy

Observer’s Assessment of Observer’s Assessment of Alertness/Sedation Scale (OAAS)Alertness/Sedation Scale (OAAS)
Scores Descriptions
5 Responds readily to name spoken in normal tone
4 Lethargic response to name spoken in normal tone
3 Responds only after name is called loudly and/or repeatedly
2 Responds only after mild prodding or shaking
1 Responds only after painful trapezius squeeze
0 No response after painful trapezius squeeze

Post procedural ManagementPost procedural Management
Post-procedural monitoring including Post-procedural monitoring including observation and vital sign monitoringobservation and vital sign monitoring
Post-procedure written instructions for Post-procedure written instructions for patientspatients

Guideline statements by Guideline statements by ASA, AGA, ASGE, AAAASF, ASA, AGA, ASGE, AAAASF,
and others professional and others professional societies on conscious societies on conscious
sedationsedation

Professional Societies Professional Societies GuidelinesGuidelines
ASA, AGA, ASGE, AAAASF, AANA all ASA, AGA, ASGE, AAAASF, AANA all have specific guidelines on sedation for have specific guidelines on sedation for endoscopic proceduresendoscopic procedures
Purpose is to ensure patient safetyPurpose is to ensure patient safety

What are the national What are the national organizations’ positions?organizations’ positions?
The American Association for the The American Association for the Accreditation of Ambulatory Surgical Accreditation of Ambulatory Surgical Facilities (AAAASF) has explicitly taken Facilities (AAAASF) has explicitly taken the position that the position that propofol, unlike other propofol, unlike other intravenous sedation, may not be intravenous sedation, may not be administered by a registered nurse.administered by a registered nurse.

ASA and AANAASA and AANA
The joint ASA/ AANA statement on The joint ASA/ AANA statement on propofol use indicates that, “personnel propofol use indicates that, “personnel who administer propofol should be who administer propofol should be qualified to rescue patients whose level of qualified to rescue patients whose level of sedation becomes deeper than initially sedation becomes deeper than initially intended and who enter, if briefly, a state intended and who enter, if briefly, a state of general anesthesia.”of general anesthesia.”

JCAHOJCAHO
The Joint Commission on The Joint Commission on Accreditation of Healthcare Accreditation of Healthcare Organizations (JCAHO) requires that Organizations (JCAHO) requires that clinicians intending to administer deep clinicians intending to administer deep sedation sedation be qualified to rescue be qualified to rescue patients from general anesthesia and patients from general anesthesia and be competent to manage an unstable be competent to manage an unstable cardiovascular system as well as a cardiovascular system as well as a compromised airway and inadequate compromised airway and inadequate oxygenation and ventilation.oxygenation and ventilation.

AGA, ACG and ASGEAGA, ACG and ASGE
The American Gastroenterological The American Gastroenterological Association (AGA), the American College Association (AGA), the American College of Gastroenterology (ACG), and the of Gastroenterology (ACG), and the American Society for Gastrointestinal American Society for Gastrointestinal Endoscopy (ASGE) issued a joint Endoscopy (ASGE) issued a joint statement supporting nurse-administered statement supporting nurse-administered propofol by nonanesthesiologists for propofol by nonanesthesiologists for endoscopy. endoscopy.

Mild to moderate sedationMild to moderate sedation– Non anesthesiology personnelNon anesthesiology personnel
Deep sedation and general anesthesiaDeep sedation and general anesthesia– Anesthesia personnelAnesthesia personnel

Approved Drugs for Approved Drugs for Monitored Anesthesia CareMonitored Anesthesia Care

PropofolPropofol
highly lipophilic highly lipophilic
Large VdLarge Vd
Triphasic distributionTriphasic distribution– Rapid redistribution – 2-3 minRapid redistribution – 2-3 min– MetabolismMetabolism– Slow elimination from adipose tissuesSlow elimination from adipose tissues

Advanatges of PropofolAdvanatges of Propofol
Rapid onsetRapid onset
Rapid offsetRapid offset
Optimal sedation levelOptimal sedation level
AntiemeticAntiemetic

Propofol MetabolismPropofol Metabolism
Eliminated as sulfate and/or glucuronide Eliminated as sulfate and/or glucuronide conjugates in the urineconjugates in the urineLess than 0.3% excreted as the parent Less than 0.3% excreted as the parent compound compound Extra hepatic metabolismExtra hepatic metabolismHepatic and renal dysfunction do not Hepatic and renal dysfunction do not significantly alter the pharmacokinetics of significantly alter the pharmacokinetics of propofol propofol Elderly – lower Vd and lower clearance, lower Elderly – lower Vd and lower clearance, lower doses neededdoses needed

Caution on sedationCaution on sedation
Sedation is a continuumSedation is a continuum
rapid, profound changes in sedative depth
non-anesthesia personnel who administer propofol should be qualified to rescue patients from deeper level of sedation from deeper level of sedation
education and training to manage the potential medical complications of sedation/anesthesia

Adverse Effects of PropofolAdverse Effects of Propofol
IV injection site painIV injection site pain
Hypotension especially in hypovolemiaHypotension especially in hypovolemia
HypoxiaHypoxia
Microbial contaminationMicrobial contamination
lipidemia > 3 days of infusionlipidemia > 3 days of infusion
Green discoloration of the urine Green discoloration of the urine

Pharmacodynamics and Pharmacodynamics and pharmacokinetics of fospropofolpharmacokinetics of fospropofol

FospropofolFospropofol
new sedative/hypnotic agent new sedative/hypnotic agent Fospropofol – water soluble prodrug of Fospropofol – water soluble prodrug of propofol propofol Developed in an attempt to reduce the Developed in an attempt to reduce the disadvantages of the lipid emulsion of disadvantages of the lipid emulsion of propofolpropofolenzymatic action of alkaline phosphatases in enzymatic action of alkaline phosphatases in the vascular endothelium the vascular endothelium

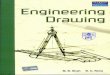
Fospropofol Disodium Metabolism(Enzymatic Liberation of Propofol)
Fechner J, et al. Anesthesiology. 2003;99:303-1313.
• Water-soluble prodrug of propofol with differentiated PK/PD• Alkaline phosphatase is widely distributed in body• Fospropofol disodium is rapidly and completely metabolized
fospropofol disodium
SulphationGlucuronidation
UrinaryExcretion
alkaline
phosphatase
Propofol Formaldehyde Phosphate
OH O
HH O
P
O
OOO
O
O O
OP

Fospropofol - PK and PDFospropofol - PK and PD
Non-linear, 6 compartments with an effect Non-linear, 6 compartments with an effect site compartmentsite compartmentlonger half-life, larger Vd, and a delayed longer half-life, larger Vd, and a delayed onset of action compared with propofolonset of action compared with propofollower peak concentrations and more lower peak concentrations and more prolonged plasma concentrations prolonged plasma concentrations No pain on injection in the armNo pain on injection in the armParasthesia and itching in the perineal Parasthesia and itching in the perineal regionregion

Fospropofol PD – Single bolus and BIS Levels

Fospropofol Doses and BIS Levels

Clinical profiles of fospropofolClinical profiles of fospropofol

Dose titrationDose titration
The solution for a steep concentration-The solution for a steep concentration-response relationshipresponse relationship– Administer small fractions of initial doseAdminister small fractions of initial dose
Phase II/III studies for Aquavan do Phase II/III studies for Aquavan do nicely follow this guidelinenicely follow this guideline– Fospropofol 6.5 mg/kg as initial dose Fospropofol 6.5 mg/kg as initial dose
followed by ¼ of this dose (1.6 mg/min) followed by ¼ of this dose (1.6 mg/min) every 4 minutes up to a maximum of 3 every 4 minutes up to a maximum of 3 repeat dosesrepeat doses
– ‘‘Sedation failure’ rate of approximately Sedation failure’ rate of approximately 20%20%
– At least 15 minutes would be required to At least 15 minutes would be required to reach ‘sedation failure’ decisionreach ‘sedation failure’ decision

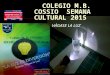
Fospropofol Sedation Success during Colonoscopy
Cohen LB. Alimentary Pharmacology & Therapeutics 27 (7), 597-608.
Figure 1. Sedation success. The primary end point of this study was sedation success, where a highly significant dose-dependent trend was observed across fospropofol dosing groups in the modified intent-to-treat population (P < 0.001 by Cochran–Armitage trend test). The sedation success rates were 24%, 35%, 69% and 96% in the FP 2.0, FP 5.0, FP 6.5 and FP 8.0 groups respectively. *P < 0.05 vs. FP 2.0 and FP 5.0.

Fospropofol Sedation during Colonoscopy - Outcomes

Patients and Physicians Patients and Physicians SatisfactionSatisfaction

Fospropofol for Colonoscopy-Fospropofol for Colonoscopy-Adverse EventsAdverse Events

Fospropofol for BronchoscopyFospropofol for Bronchoscopy

Use of fospropofol for other Use of fospropofol for other procedures requiring minimal procedures requiring minimal
to moderate sedationto moderate sedation

Modified Observer’s AssessmentModified Observer’s Assessmentof Alertness/Sedation Scale (MOAA/S)of Alertness/Sedation Scale (MOAA/S)
1Responds only after painful trapezius squeeze
0Does not respond to painful trapezius squeeze
2Responds only after mild prodding or shaking
3Responds only after name is called loudly and/or repeatedly
4Lethargic response to name spoken in normal tone
5 (Alert)Responds readily to name spoken in normal tone
ScoreResponsiveness
Dynam
ic C
onti
nuum
of
Sedati
on
Chernik DA, et al. J Clin Psychopharmacol. 1990;10:244-251.ASA Practice Guidelines. Anesthesiology. 2002;96:1004-1017.
Awake
Minimal
Moderate
Deep
Generalanesthesia

Procedure Types and Duration Procedure Types and Duration
1 (0.8)
3 (2.4)
8 (6.5)
10 (8.1)
13 (10.6)
18 (14.6)
21 (17.1)
22 (17.9)
27 (22)
Patients, n (%)N = 123
Fospropofol 6.5 mg/kg
Duration of Procedure (min)
------45Arteriovenous fistula
2678Dilatation & Curettage
562429.5Lithotripsy
32812Ureteroscopy
26414Transesophageal echocardiogram
1052643.5Bunionectomy
31312Hysteroscopy
261217.5Arthroscopy
2524Esophagogastroduodenoscopy
MaxMinMedianProcedure

Adverse Events
• Majority of adverse events (AEs) were mild to moderate• Serious AEs (n = 4)
– n=2 atrial septal defect, n=1 apnea and cardiac arrest, n=1 increased ammonia and hepatic encephalopathy
• Treatment-related AEs
– Most common were perineal paresthesias (53.7%) and pruritus (26.0%)
• Sedation-related AEs (5 patients, 4.1%)
– Hypoxemia (n=1, <1min and managed with verbal stimulation and chin lift)
– Hypotension (n=4, occurred during the dosing and recovery periods)
– Bradycardia (n=1 concurrently with hypotension and managed with atropine)
• No deaths reported and no procedure discontinued due to adverse event

Hepatic and Renal Impairment
MSURG523
•20/123 (16%) patients had previous or existing hepatic disease (minimal – severe)
•5/123 (4%) patients had severe renal impairment (creatinine clearance 11-36 mL/min)
•Adverse event rates were similar to overall population
– Treatment-related AEs were similar to other patients (paresthesia 50%, pruritus 30%)
•No sedation-related adverse events reported

"For general anesthesia or monitored anesthesia "For general anesthesia or monitored anesthesia care (MAC) sedation, DIPRIVAN Injectable care (MAC) sedation, DIPRIVAN Injectable
Emulsion should be administered only by persons Emulsion should be administered only by persons trained in the administration of general anesthesiatrained in the administration of general anesthesia
and not involved in the conduct of the and not involved in the conduct of the surgical/diagnostic procedure.” surgical/diagnostic procedure.”
Package Insert for FospropofolPackage Insert for Fospropofol
Similar to PropofolSimilar to Propofol

FutureFuture
Better pharmacological agentsBetter pharmacological agents– Better sedatives and analgesicsBetter sedatives and analgesics
Better delivery systemBetter delivery system– Patient-controlled sedationPatient-controlled sedation
Better monitoring systemBetter monitoring system– Closed-loop controlClosed-loop control

Conclusions IConclusions ISedation ensures that patients are Sedation ensures that patients are comfortable when undergoing minor comfortable when undergoing minor medical and surgical proceduresmedical and surgical proceduresConstant monitoring of patients during Constant monitoring of patients during sedation ensures safety and a good sedation ensures safety and a good outcomeoutcomePractitioners caring for patients under Practitioners caring for patients under sedation should be properly educated sedation should be properly educated on the pharmacology of the drugs used on the pharmacology of the drugs used during sedation as well as how to during sedation as well as how to combine hypnotics and analgesicscombine hypnotics and analgesics

Conclusions IIConclusions II
Minimum and moderate sedation can be safely Minimum and moderate sedation can be safely performed by sedation nurses under the performed by sedation nurses under the supervision of the physiciansupervision of the physicianDeep sedation should be cared for by medical Deep sedation should be cared for by medical personnel with the appropriate training and personnel with the appropriate training and appropriate monitoring technologyappropriate monitoring technologyPropofol and fospropfol are efficacious and Propofol and fospropfol are efficacious and safe when administered by medical personnel safe when administered by medical personnel with the appropriate training and appropriate with the appropriate training and appropriate monitoring technology.monitoring technology.

Conclusions IIIConclusions III
Even if moderate sedation is intended, Even if moderate sedation is intended, patients receiving propofol or fospropofol patients receiving propofol or fospropofol should receive care consistent with that should receive care consistent with that required for deep sedation.required for deep sedation.
This means that the clinician administering This means that the clinician administering propofol or fospropofol must be competent propofol or fospropofol must be competent to recognize a state of general anesthesia to recognize a state of general anesthesia and rescue a patient experiencing any of and rescue a patient experiencing any of the complications of general anesthesia. the complications of general anesthesia.























![Dacia Duster [M.B]](https://img.pdfslide.net/doc/110x75/5497762cac795959288b5498/dacia-duster-mb.jpg)