Embed Size (px)
Citation preview
Minimally Invasive Surgery SymposiumGut Hormones and the Medical
Management of Diabesity
Donna H. Ryan, MDPennington Biomedical Research CenterBaton Rouge, LA
Outline Physiologic abnormalities in T2DM Incretins in normal physiology and T2DM Therapeutic approaches targeting
incretins
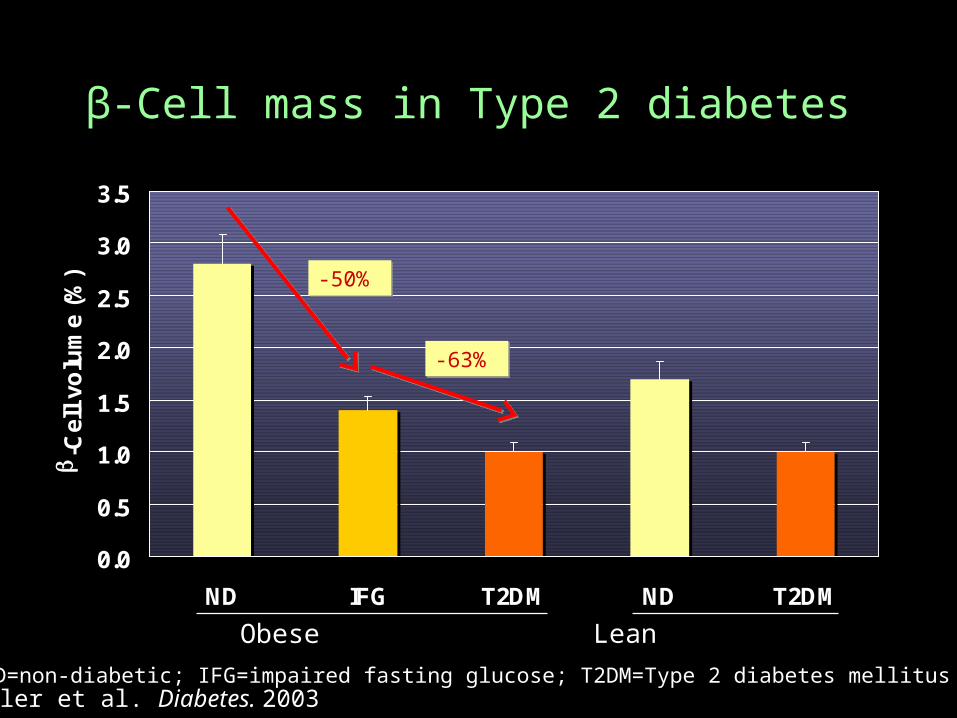
β-Cell mass in Type 2 diabetes
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
ND IFG T2DM ND T2DM
b-C
ell
volu
me
(%)
Obese Lean
-50%-50%
-63%-63%
Butler et al. Diabetes. 2003ND=non-diabetic; IFG=impaired fasting glucose; T2DM=Type 2 diabetes mellitus
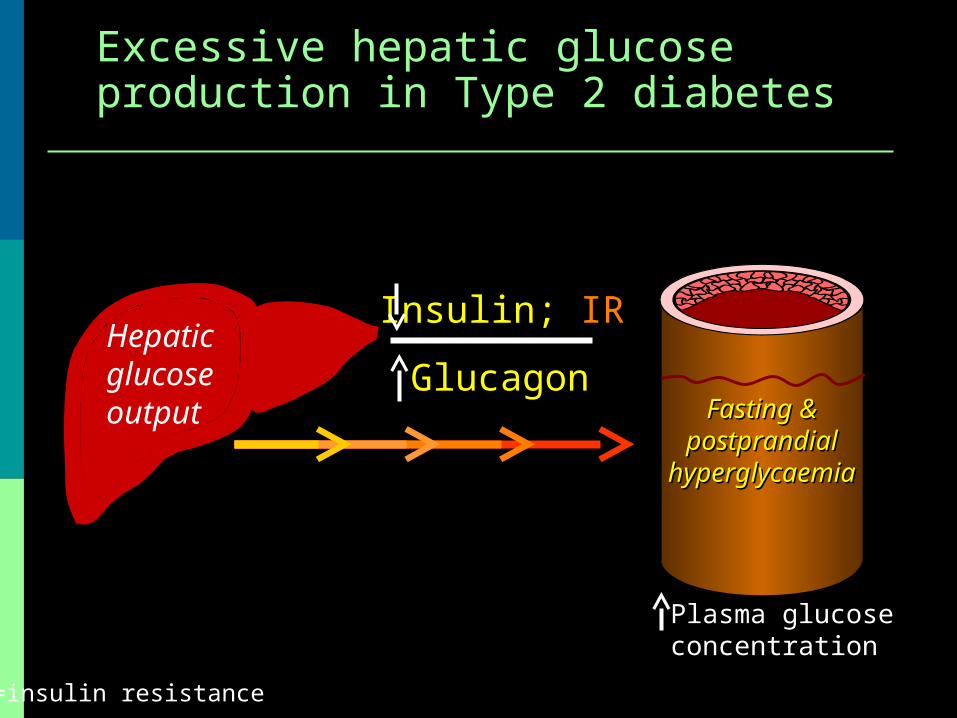
Excessive hepatic glucose production in Excessive hepatic glucose production in Type 2 diabetesType 2 diabetes
Plasma glucose concentration
Fasting & Fasting & postprandial postprandial
hyperglycaemiahyperglycaemia
Insulin; IR
GlucagonHepaticglucoseoutput
IR=insulin resistance
Outline Physiologic abnormalities in T2DM Incretins in normal physiology and T2DM Therapeutic approaches targeting
incretins
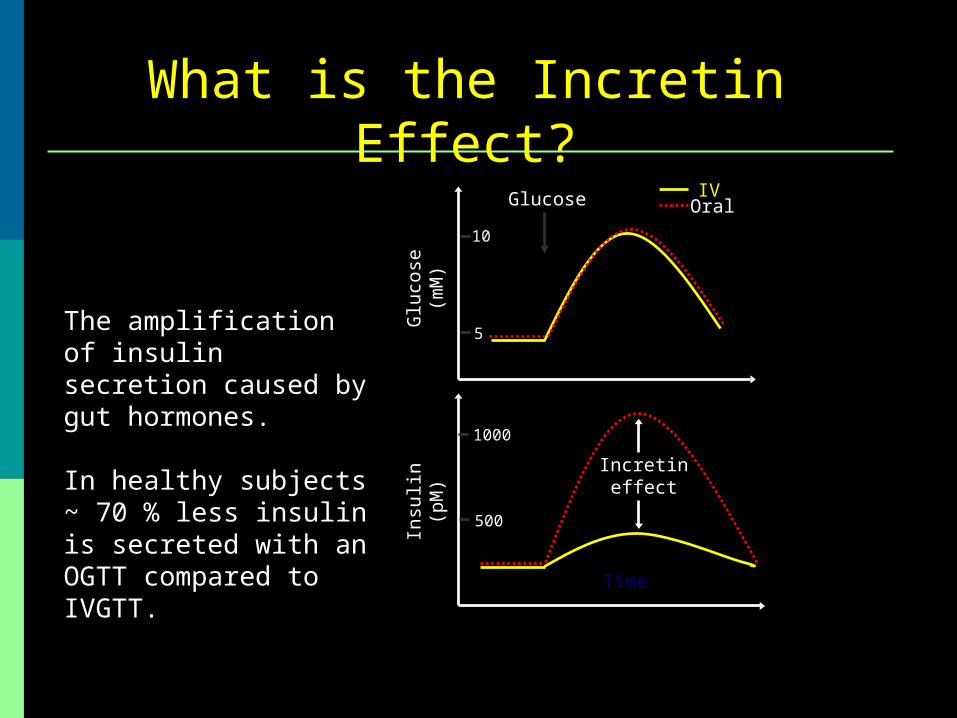
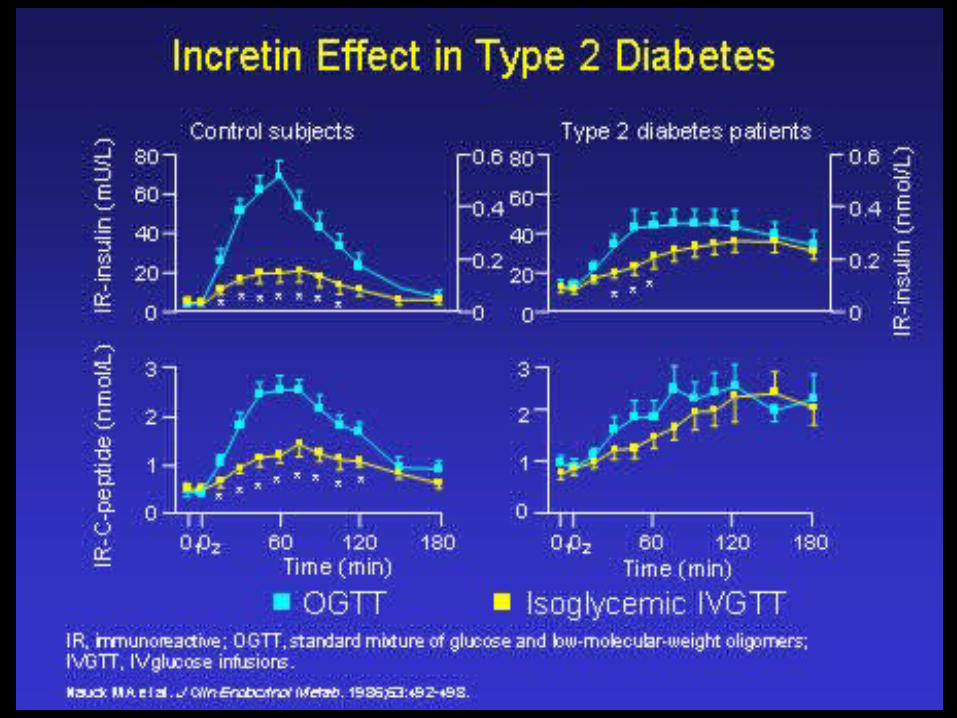
What is the Incretin Effect?
Time
Insu
lin
(pM
)G
luco
se
(mM
)1000
500
10
5
IVGlucose Oral
Incretineffect
The amplification of insulin secretion caused by gut hormones.
In healthy subjects ~ 70 % less insulin is secreted with an OGTT compared to IVGTT.
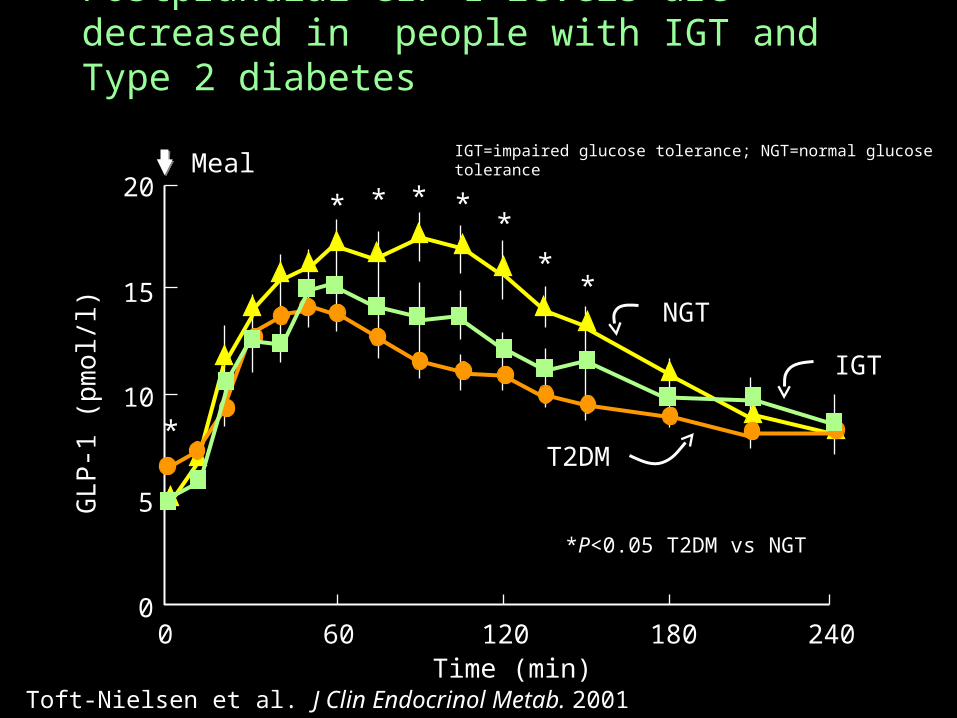
Postprandial GLP-1 levels are decreased in people with IGT and Type 2 diabetes
Toft-Nielsen et al. J Clin Endocrinol Metab. 2001
20
15
10
5
00 60 120 180 240
Time (min)
GLP
-1 (
pm
ol/l)
* * * **
**
*
Meal
NGT
T2DM
IGT
*P<0.05 T2DM vs NGT
IGT=impaired glucose tolerance; NGT=normal glucose tolerance
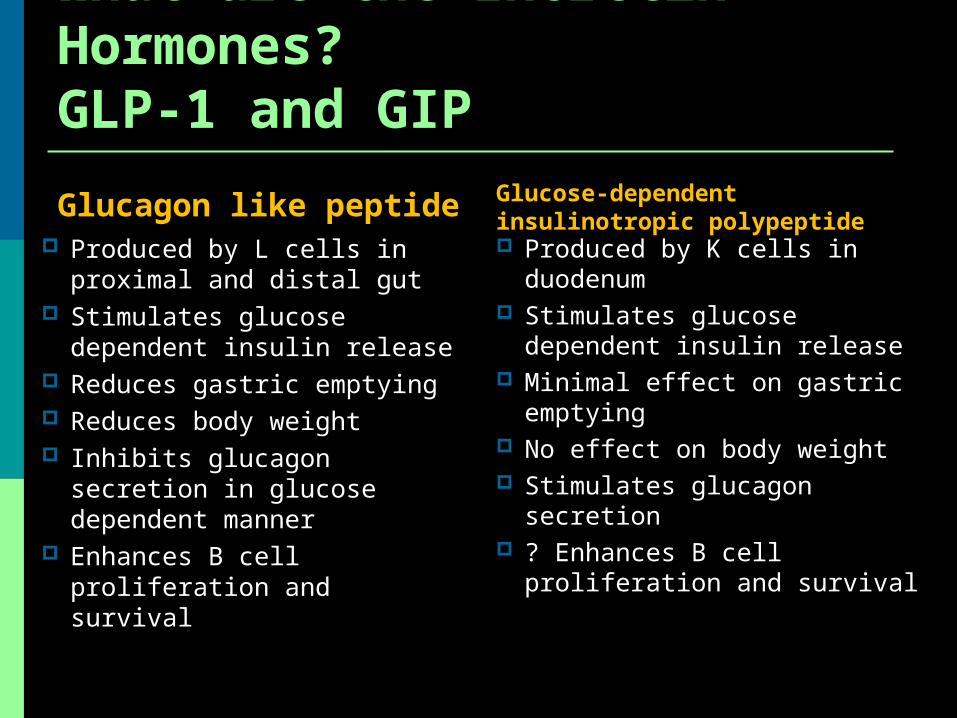
Glucagon like peptide Produced by L cells in
proximal and distal gut Stimulates glucose
dependent insulin release Reduces gastric emptying Reduces body weight Inhibits glucagon secretion
in glucose dependent manner
Enhances B cell proliferation and survival
Glucose-dependent insulinotropic polypeptide Produced by K cells in
duodenum Stimulates glucose
dependent insulin release Minimal effect on gastric
emptying No effect on body weight Stimulates glucagon
secretion ? Enhances B cell
proliferation and survival
What are the Incretin Hormones?GLP-1 and GIP
Incretin Function in T2DM Secretion of GLP-1 impaired Beta Cell sensitivity to GLP-1 decreased Secretion of GIP slightly impaired Effect of GIP abolished or grossly impaired
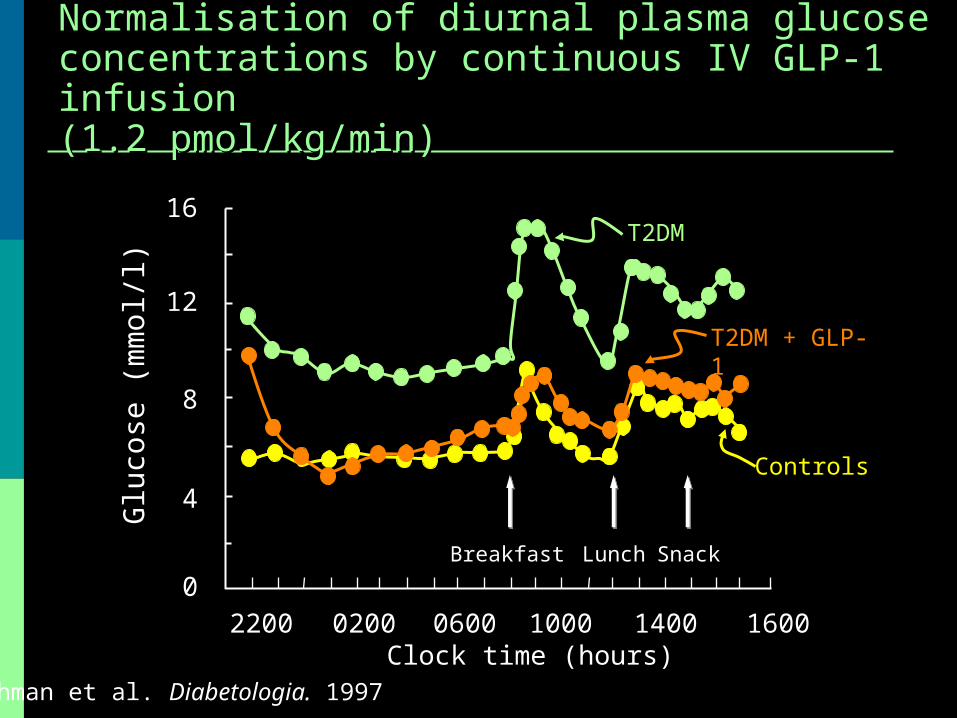
Normalisation of diurnal plasma glucose Normalisation of diurnal plasma glucose concentrations by continuous IV GLP-1 infusionconcentrations by continuous IV GLP-1 infusion(1.2 pmol/kg/min)(1.2 pmol/kg/min)
Rachman et al. Diabetologia. 1997
T2DM
T2DM + GLP-1
Controls
00600 1000 1400 1600
Glu
cose
(m
mol/l)
16
Clock time (hours)
Breakfast Lunch Snack
12
8
4
02002200
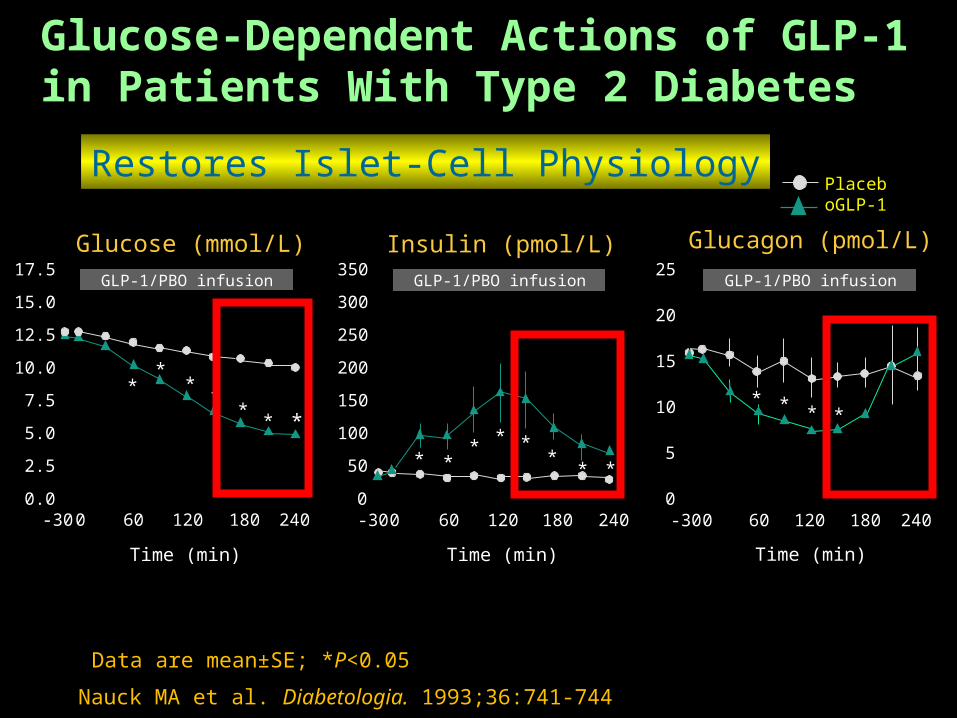
Nauck MA et al. Diabetologia. 1993;36:741-744
Data are mean±SE; *P<0.05
PlaceboGLP-1
Glucose-Dependent Actions of GLP-1in Patients With Type 2 Diabetes
350
300
250
200
150
100
50
0
Insulin (pmol/L)
* ** * *
** *
GLP-1/PBO infusion
Time (min)
-30 0 60 120 180 240 240
25
20
15
10
5
0
Glucagon (pmol/L)
Time (min)
-30 0 60 120 180
**
* *
GLP-1/PBO infusion17.5
15.0
12.5
10.0
7.5
5.0
2.5
0.0
*
Glucose (mmol/L)
GLP-1/PBO infusion
***
**
*
-30 0 60 120 180 240
Time (min)
Restores Islet-Cell Physiology
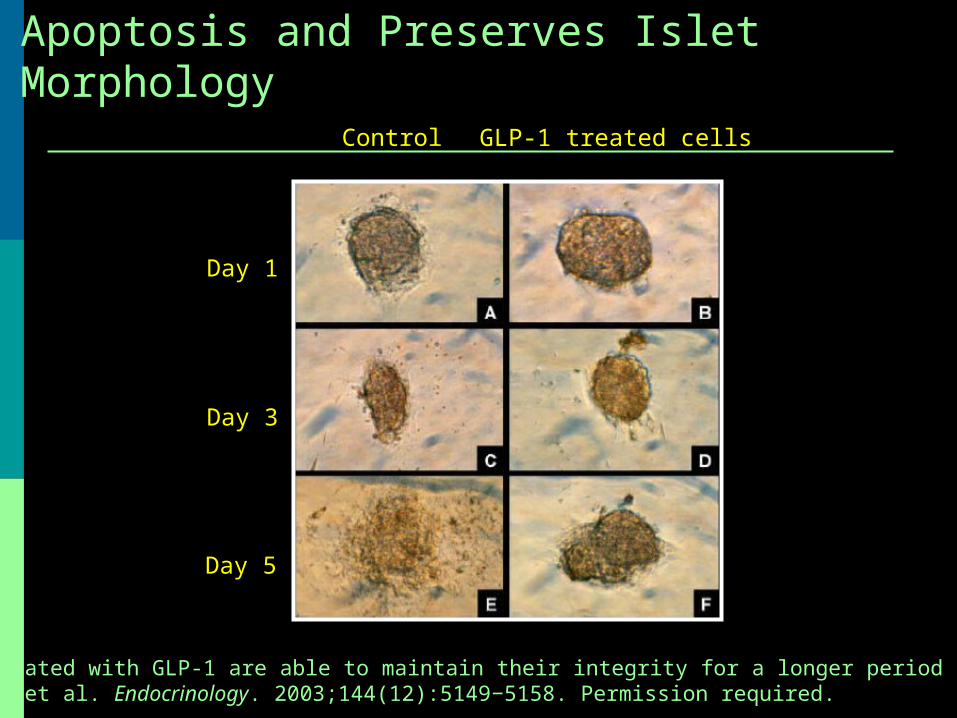
GLP-1 Inhibits Human Islet Cell Apoptosis and Preserves Islet Morphology
Day 1
GLP-1 treated cellsControl
Day 3
Day 5
Islets treated with GLP-1 are able to maintain their integrity for a longer period of time. Farilla L et al. Endocrinology. 2003;144(12):5149−5158. Permission required.
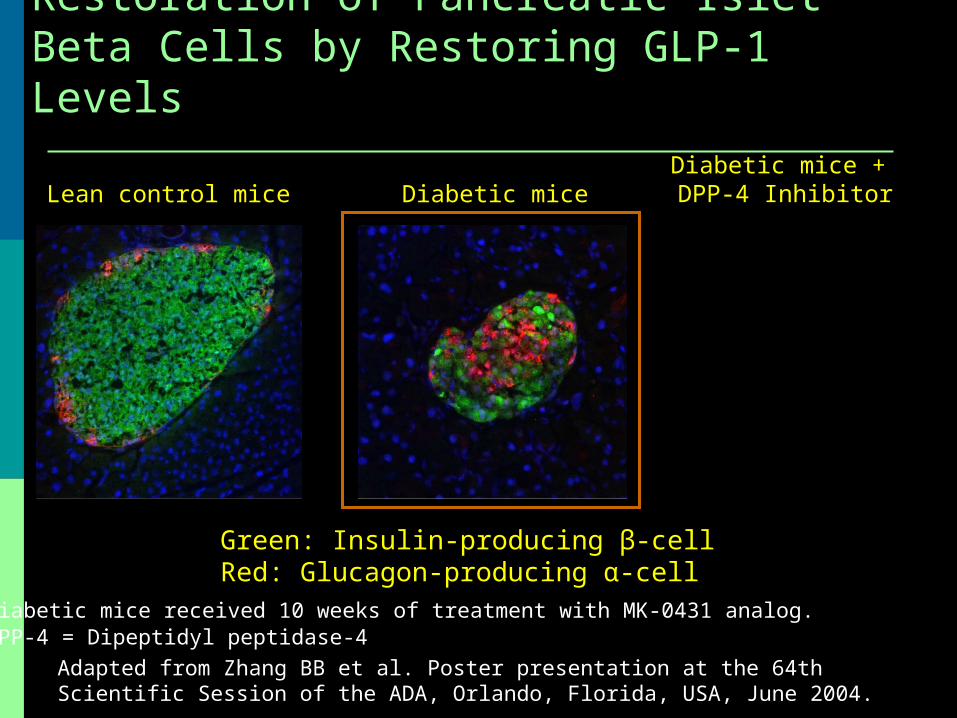
Restoration of Pancreatic Islet Beta Cells by Restoring GLP-1 Levels
Diabetic miceDiabetic mice + DPP-4 InhibitorLean control mice
Green: Insulin-producing β-cellRed: Glucagon-producing α-cell
Adapted from Zhang BB et al. Poster presentation at the 64th Scientific Session of the ADA, Orlando, Florida, USA, June 2004.
Diabetic mice received 10 weeks of treatment with MK-0431 analog.DPP-4 = Dipeptidyl peptidase-4
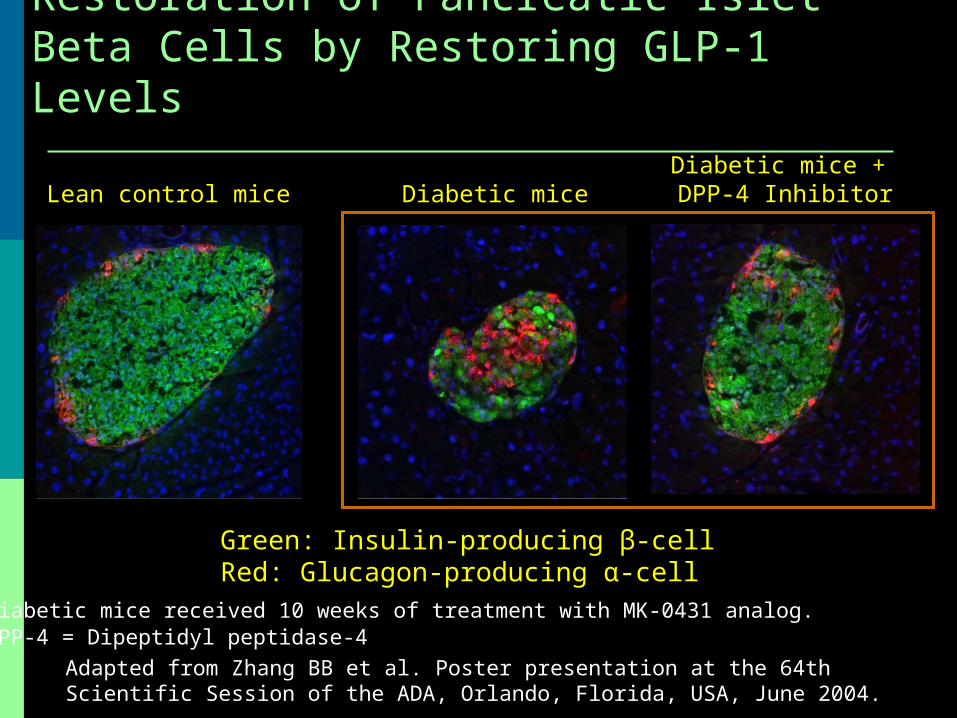
Restoration of Pancreatic Islet Beta Cells by Restoring GLP-1 Levels
Diabetic miceDiabetic mice + DPP-4 InhibitorLean control mice
Green: Insulin-producing β-cellRed: Glucagon-producing α-cell
Adapted from Zhang BB et al. Poster presentation at the 64th Scientific Session of the ADA, Orlando, Florida, USA, June 2004.
Diabetic mice received 10 weeks of treatment with MK-0431 analog.DPP-4 = Dipeptidyl peptidase-4
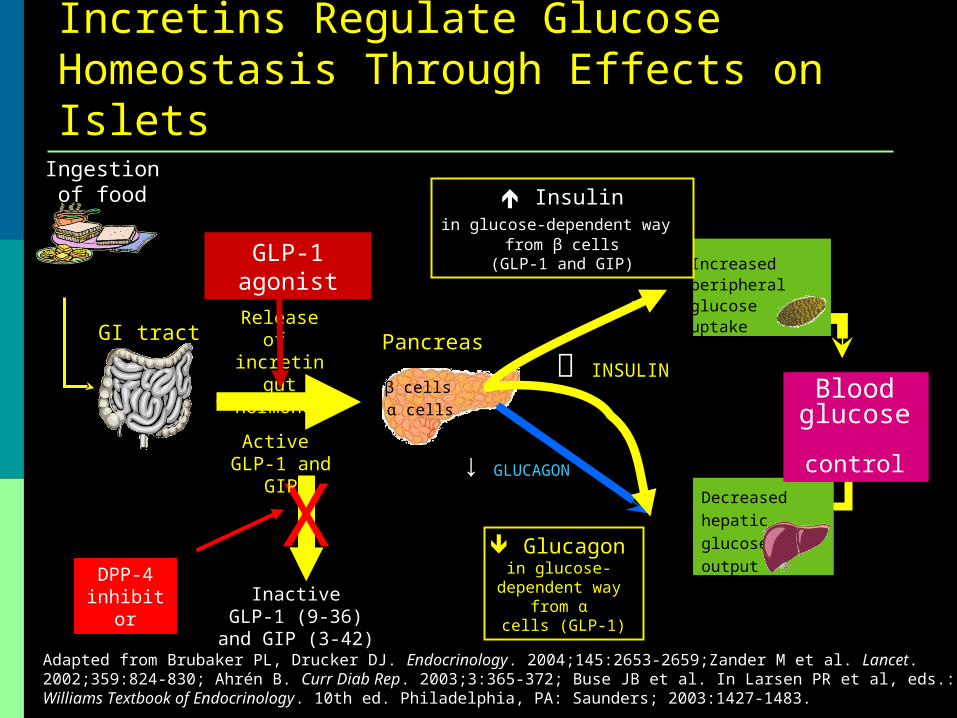
Decreasedhepatic glucose output
Increased peripheral glucose uptakeGI tract Pancreas
Incretins Regulate Glucose Homeostasis Through Effects on Islets
Glucagon in glucose-
dependent way from αα
cells (GLP-1)
α cells
Insulinin glucose-dependent way
from β cells(GLP-1 and GIP)
β cells
Ingestion of food
Adapted from Brubaker PL, Drucker DJ. Endocrinology. 2004;145:2653-2659;Zander M et al. Lancet. 2002;359:824-830; Ahrén B. Curr Diab Rep. 2003;3:365-372; Buse JB et al. In Larsen PR et al, eds.: Williams Textbook of Endocrinology. 10th ed. Philadelphia, PA: Saunders; 2003:1427-1483.
InactiveGLP-1 (9-36)
and GIP (3-42)
↓ GLUCAGON
INSULIN
DPP-4 inhibitor
X
Bloodglucose control
Release of incretin gut hormones
Active GLP-1 and
GIP
Bloodglucose control
GLP-1 agonist
Outline Physiologic abnormalities in T2DM Incretins in normal physiology and T2DM Therapeutic approaches targeting
incretins
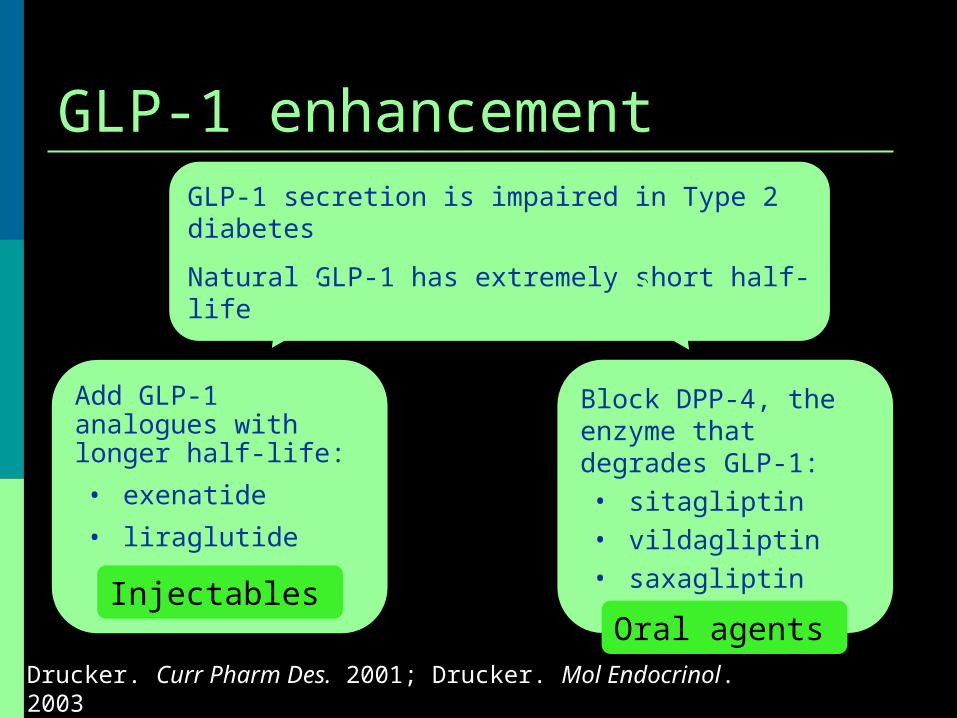
GLP-1 enhancement
Drucker. Curr Pharm Des. 2001; Drucker. Mol Endocrinol. 2003
GLP-1 secretion is impaired in Type 2 diabetes
Natural GLP-1 has extremely short half-life
Add GLP-1 analogues with longer half-life:
• exenatide
• liraglutide
Injectables
Block DPP-4, the enzyme that degrades GLP-1:• sitagliptin• vildagliptin• saxagliptin
Oral agents
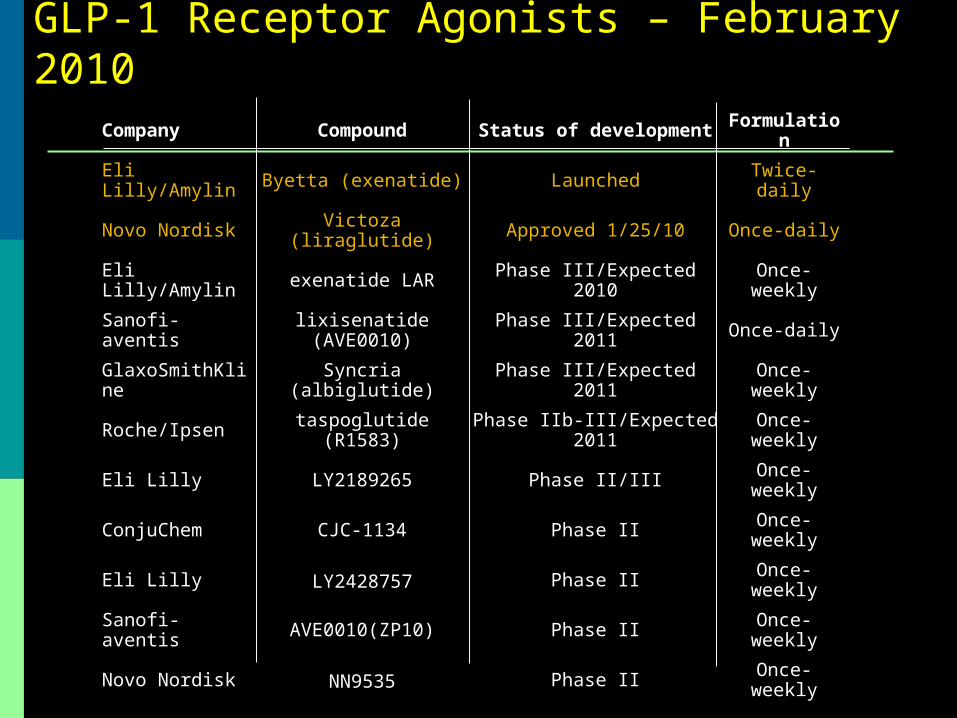
GLP-1 Receptor Agonists – February 2010Company Compound Status of development Formulation
Eli Lilly/Amylin Byetta (exenatide) Launched Twice-daily
Novo Nordisk Victoza (liraglutide) Approved 1/25/10 Once-daily
Eli Lilly/Amylin exenatide LAR Phase III/Expected 2010 Once-weekly
Sanofi-aventis lixisenatide (AVE0010) Phase III/Expected 2011 Once-daily
GlaxoSmithKline Syncria (albiglutide) Phase III/Expected 2011 Once-weekly
Roche/Ipsen taspoglutide (R1583) Phase IIb-III/Expected 2011 Once-weekly
Eli Lilly LY2189265 Phase II/III Once-weekly
ConjuChem CJC-1134 Phase II Once-weekly
Eli Lilly LY2428757 Phase II Once-weekly
Sanofi-aventis AVE0010(ZP10) Phase II Once-weekly
Novo Nordisk NN9535 Phase II Once-weekly
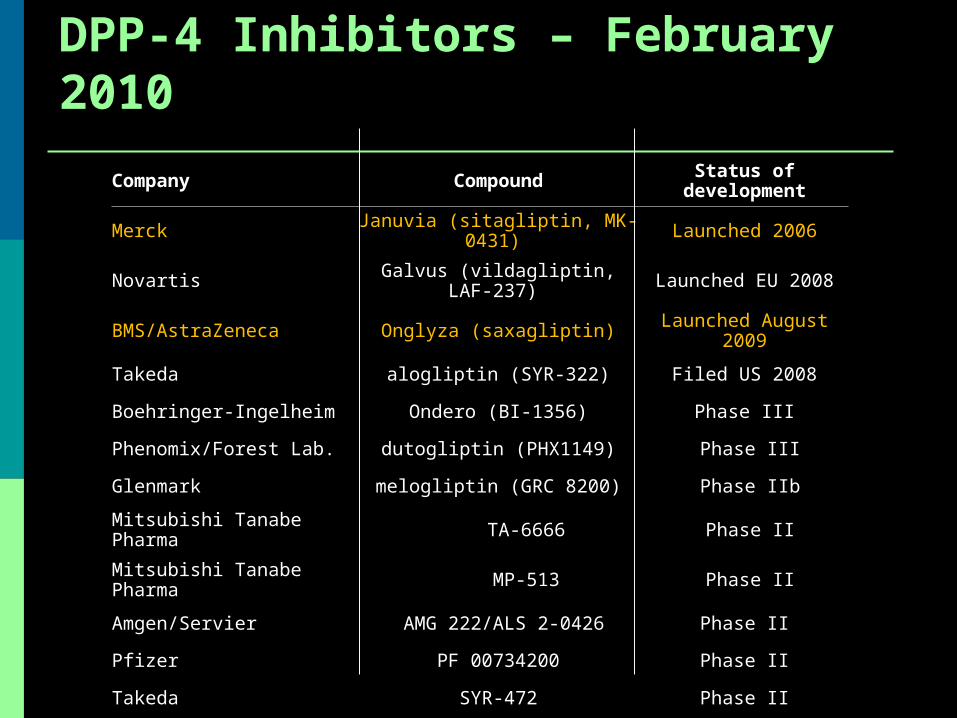
DPP-4 Inhibitors – February 2010
Company Compound Status of development
Merck Januvia (sitagliptin, MK-0431) Launched 2006
Novartis Galvus (vildagliptin, LAF-237) Launched EU 2008
BMS/AstraZeneca Onglyza (saxagliptin) Launched August 2009
Takeda alogliptin (SYR-322) Filed US 2008
Boehringer-Ingelheim Ondero (BI-1356) Phase III
Phenomix/Forest Lab. dutogliptin (PHX1149) Phase III
Glenmark melogliptin (GRC 8200) Phase IIb
Mitsubishi Tanabe Pharma TA-6666 Phase II
Mitsubishi Tanabe Pharma MP-513 Phase II
Amgen/Servier AMG 222/ALS 2-0426 Phase II
Pfizer PF 00734200 Phase II
Takeda SYR-472 Phase II
Abbott Laboratories ABT-279 Phase II
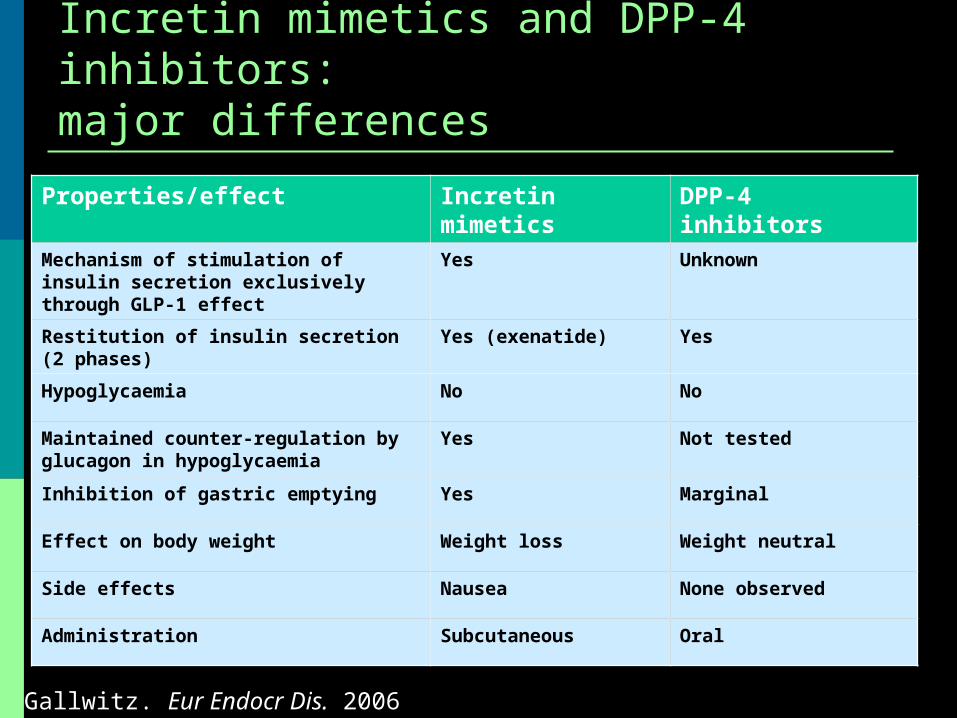
Incretin mimetics and DPP-4 inhibitors:major differences
Properties/effect Incretin mimetics DPP-4 inhibitors
Mechanism of stimulation of insulin secretion exclusively through GLP-1 effect
Yes Unknown
Restitution of insulin secretion (2 phases) Yes (exenatide) Yes
Hypoglycaemia No No
Maintained counter-regulation by glucagon in hypoglycaemia
Yes Not tested
Inhibition of gastric emptying Yes Marginal
Effect on body weight Weight loss Weight neutral
Side effects Nausea None observed
Administration Subcutaneous Oral
Gallwitz. Eur Endocr Dis. 2006
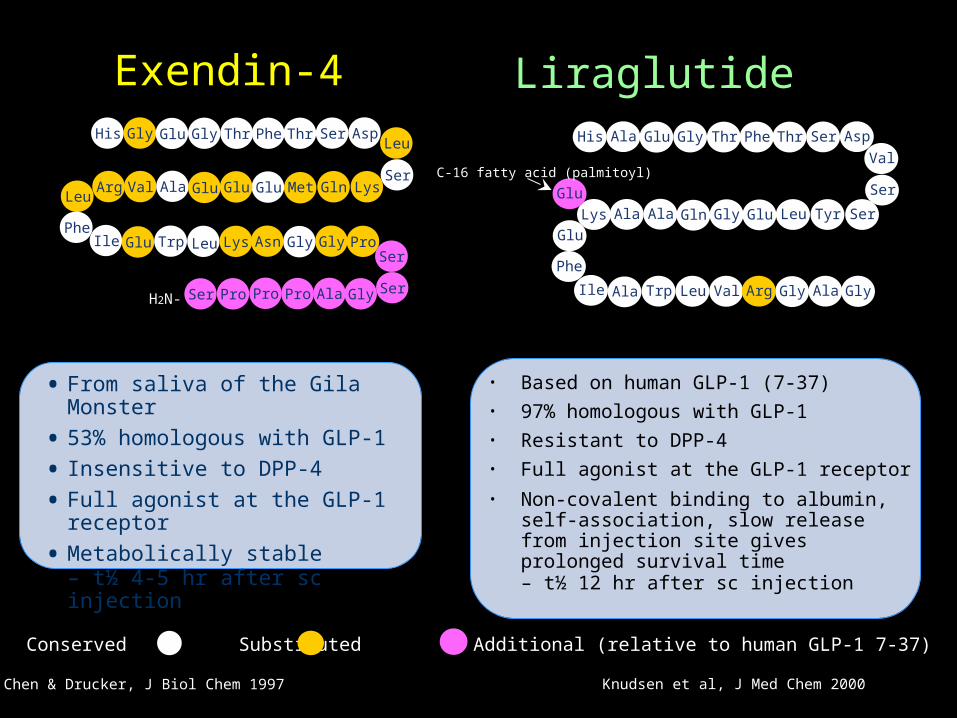
Exendin-4
Chen & Drucker, J Biol Chem 1997
GlyHis
Val Ala
Glu
Glu
Glu
Gly
Glu
Gly
Leu
Thr Phe Thr
Phe
Ser
LysSer
AspLeu
GlnMet
Leu Lys
GluArg
AsnIle Trp Gly ProSer
SerGlyPro AlaProSer ProH2N-
His Ala
Ala Ala
Ala
Glu
Glu
Gly
Gly
Gly
Glu
Thr Phe Thr
Phe
Ser
Ser
Ser
Asp
Val
TyrLeu
Leu Val
GlnLys
ArgIle Trp Ala Gly
Glu
C-16 fatty acid (palmitoyl)
• Based on human GLP-1 (7-37)• 97% homologous with GLP-1• Resistant to DPP-4• Full agonist at the GLP-1 receptor
• Non-covalent binding to albumin, self-association, slow release from injection site gives prolonged survival time– t½ 12 hr after sc injection
• From saliva of the Gila Monster
• 53% homologous with GLP-1
• Insensitive to DPP-4
• Full agonist at the GLP-1 receptor
• Metabolically stable – t½ 4-5 hr after sc injection
Liraglutide
Knudsen et al, J Med Chem 2000
Conserved Substituted Additional (relative to human GLP-1 7-37)
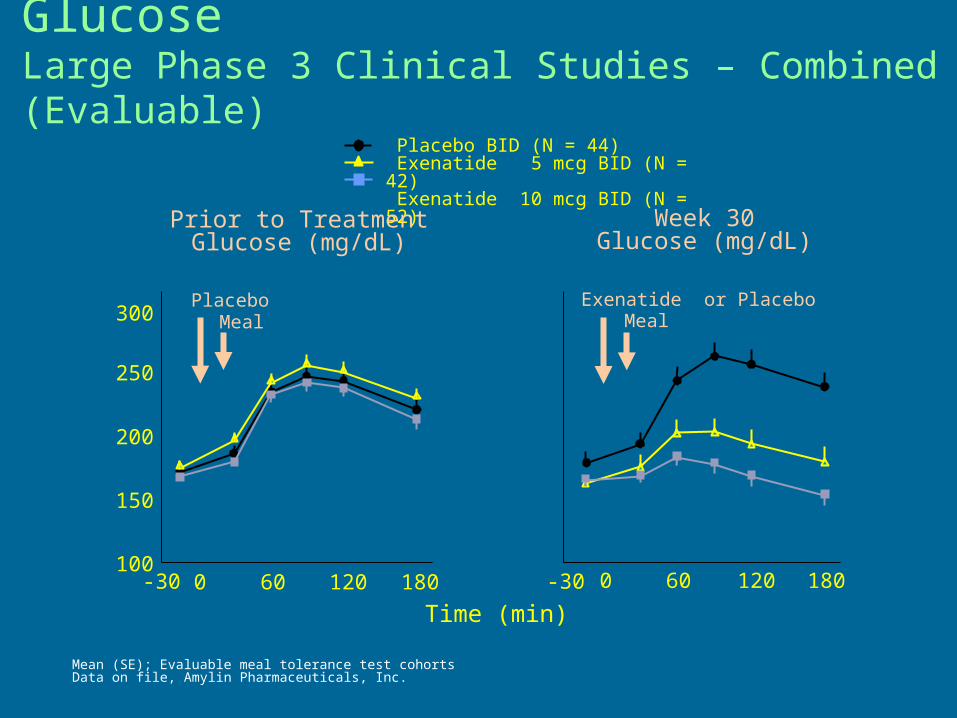
Exenatide Lowers Postprandial Glucose Large Phase 3 Clinical Studies – Combined (Evaluable)
Placebo BID (N = 44) Exenatide 5 mcg BID (N = 42) Exenatide 10 mcg BID (N = 52)
Time (min)
Prior to Treatment Glucose (mg/dL)
1000 60 120 180
150
200
250
300Placebo
Meal
Mean (SE); Evaluable meal tolerance test cohortsData on file, Amylin Pharmaceuticals, Inc.
Week 30Glucose (mg/dL)
0 60 120 180
Exenatide or PlaceboMeal
-30 -30
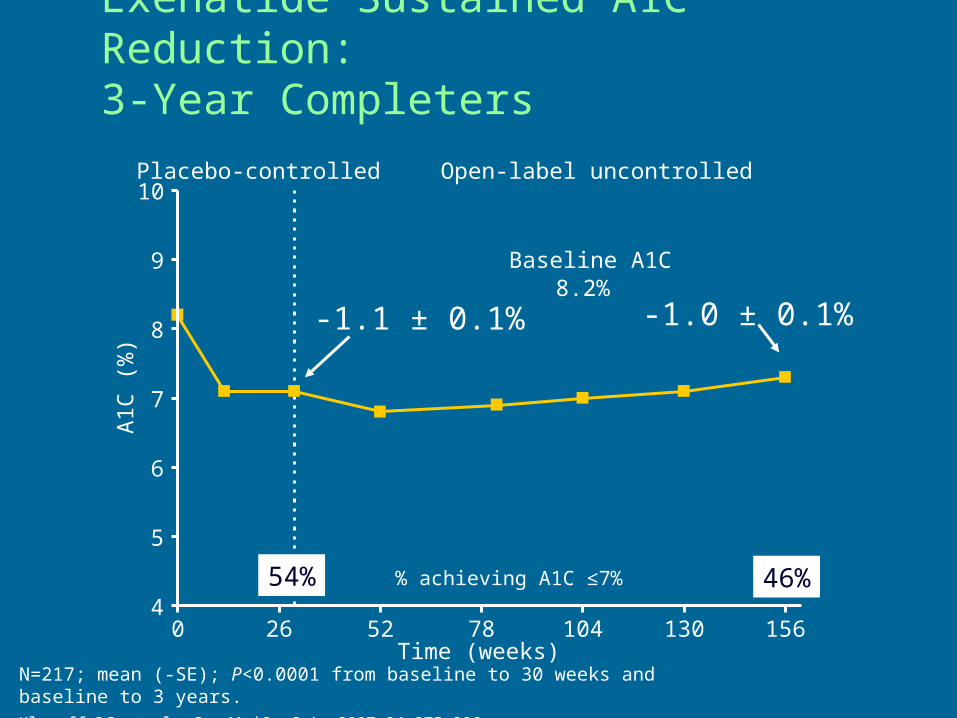
N=217; mean (-SE); P<0.0001 from baseline to 30 weeks and baseline to 3 years.Klonoff DC et al. Curr Med Res Opin. 2007;24:275-286.
Exenatide Sustained A1C Reduction:3-Year Completers
0 26 52 78 104 130 1564
5
6
7
8
9
10
Time (weeks)
Baseline A1C8.2%
Placebo-controlled Open-label uncontrolled
-1.1 ± 0.1%
% achieving A1C ≤7%
A1
C (
%)
-1.0 ± 0.1%
46%54%
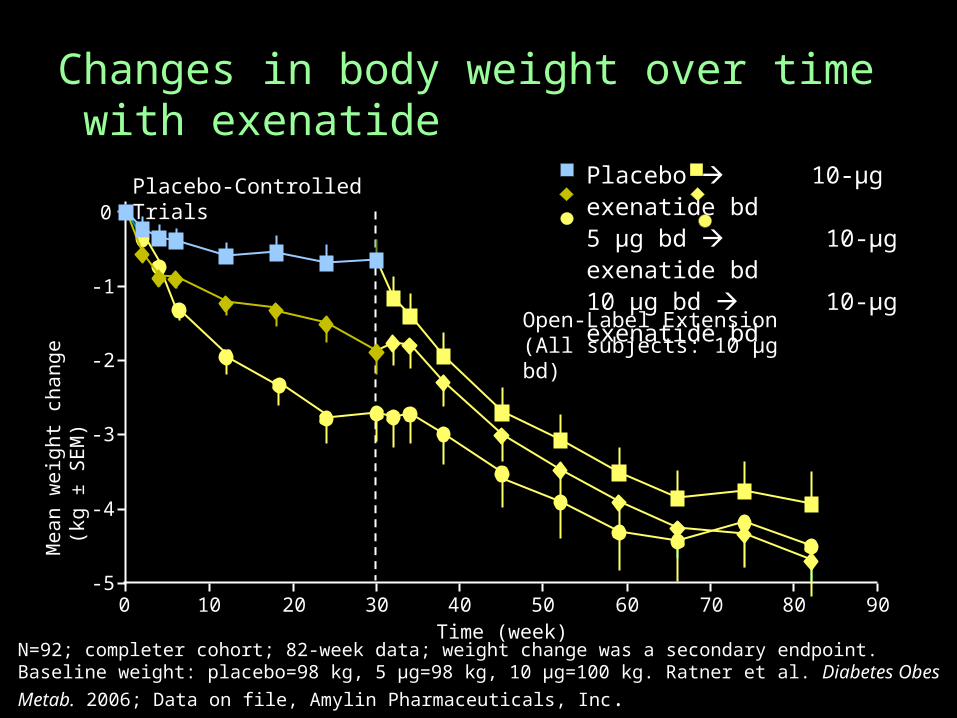
Changes in body weight over time with exenatide
Mean w
eig
ht
change
(kg
± S
EM
)
Time (week)
Placebo-ControlledTrials
0 10 20 30 40 50 60 70 80 90-5
-4
-3
-2
-1
0
Placebo 10-μg exenatide bd5 μg bd 10-μg exenatide bd10 μg bd 10-μg
exenatide bdOpen-Label Extension(All subjects: 10 μg bd)
N=92; completer cohort; 82-week data; weight change was a secondary endpoint. Baseline weight: placebo=98 kg, 5 μg=98 kg, 10 μg=100 kg. Ratner et al. Diabetes Obes Metab. 2006;
Data on file, Amylin Pharmaceuticals, Inc.
0
5
10
15
20
25
30
35
0-4 >4-8 >8-12 >12-16 >16-20 >20-24 >24-28 >28
Time (week)
% I
ncid
ence
of
naus
ea
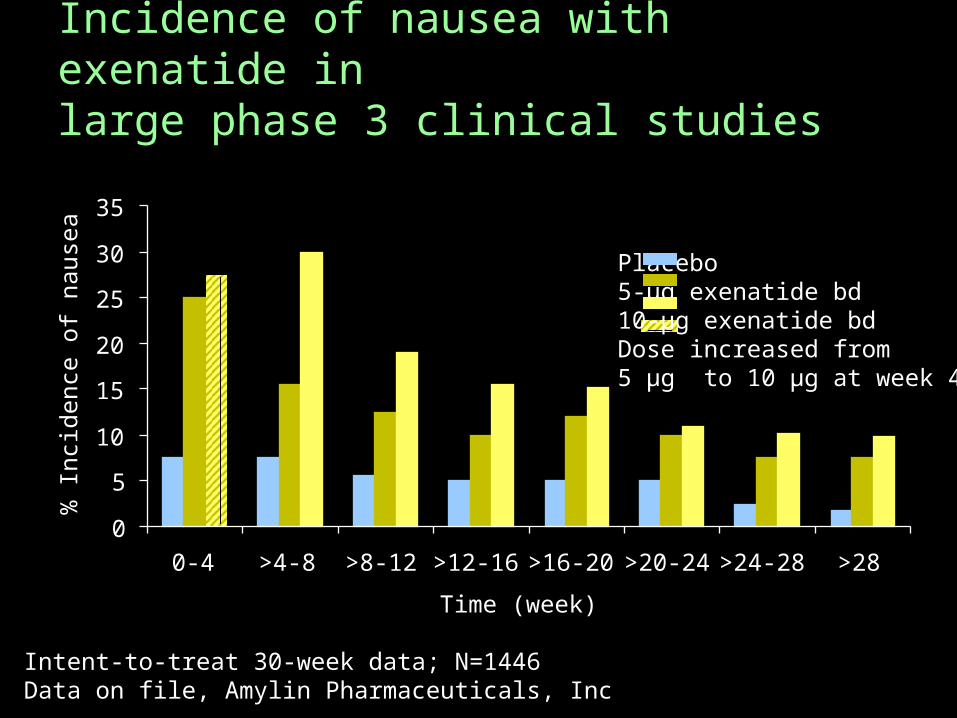
Intent-to-treat 30-week data; N=1446Data on file, Amylin Pharmaceuticals, Inc
Incidence of nausea with exenatide inlarge phase 3 clinical studies
Placebo5-μg exenatide bd10-μg exenatide bdDose increased from 5 μg to 10 μg at week 4
26 Week LEAD-6 Trial of Liraglutide vs Exenatide
Liraglutide is GLP-1 analog with a single amino acid substitution and a fatty acid to slow absorption – 97% homology
Half life 13 h. Dose 1.8 mg/d Exenatide has 57% homology Liraglutide lowered HgbA1, FPG and
HOMA-B more than exenatide. Weight loss about 2 kg
Buse J Lancet 2009;May 23
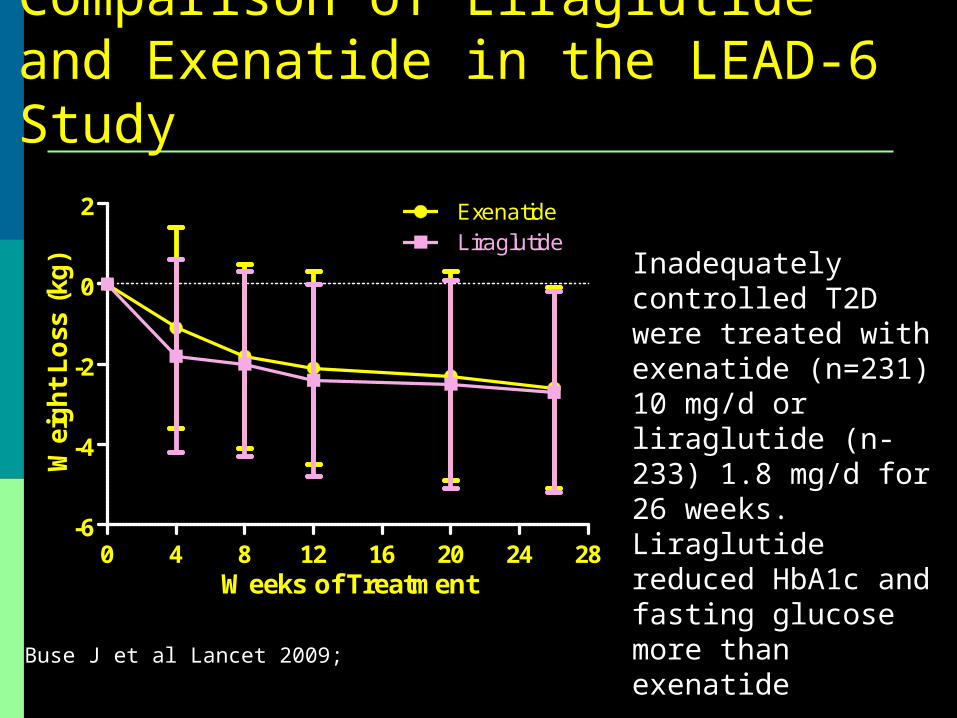
Comparison of Liraglutide and Exenatide in the LEAD-6 Study
0 4 8 12 16 20 24 28-6
-4
-2
0
2 ExenatideLiraglutide
Weeks of Treatment
Wei
gh
t L
oss
(kg
)
Buse J et al Lancet 2009;
Inadequately controlled T2D were treated with exenatide (n=231) 10 mg/d or liraglutide (n-233) 1.8 mg/d for 26 weeks. Liraglutide reduced HbA1c and fasting glucose more than exenatide
24 Week Study of Liraglutide in Obesity
20 week multi-center clinical trial with 564 obese subjects randomized to placebo, orlistat or 4 doses of liraglutide
75 subjects had prediabetes Screening and 2 week run-in prior to
randomization followed by 20 weeks of therapy
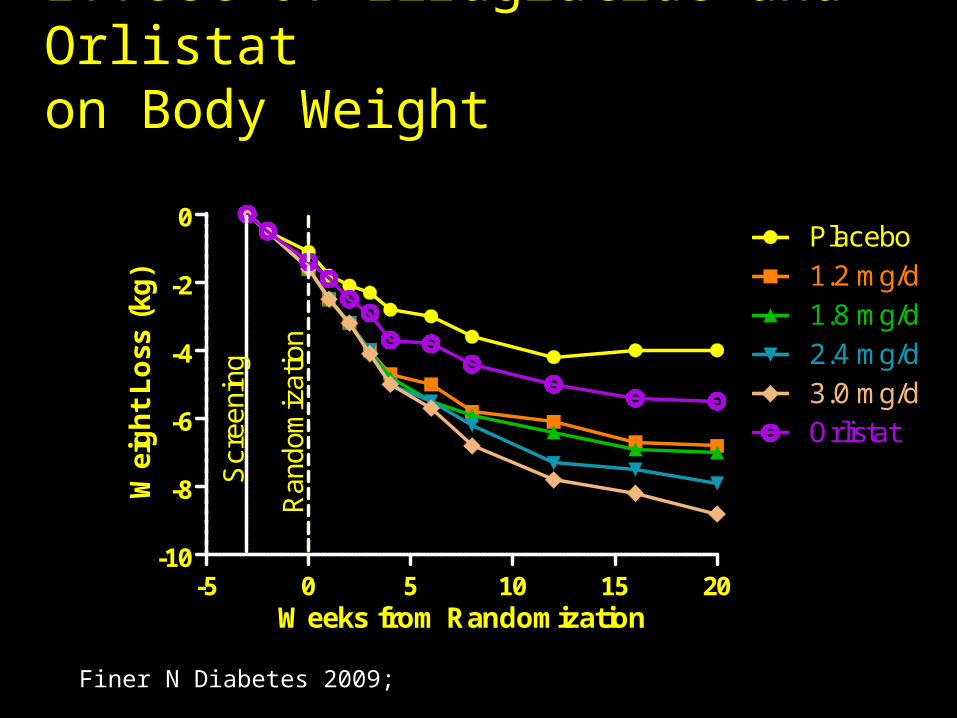
Effect of Liraglutide and Orlistaton Body Weight
-5 0 5 10 15 20-10
-8
-6
-4
-2
0Placebo1.2 mg/d1.8 mg/d2.4 mg/d3.0 mg/dOrlistat
Ran
dom
izat
ion
Scr
eeni
ng
Weeks from Randomization
Wei
gh
t L
oss
(kg
)
Finer N Diabetes 2009;
Time will tell… Liraglutide is once daily, exenatide is twice
daily, with once weekly due soon. Both liraglutide and exenatide are
associated with nausea, vomiting and diarrhea.
Will liraglutide have the side effect of pancreatitis that is seen with exenatide?
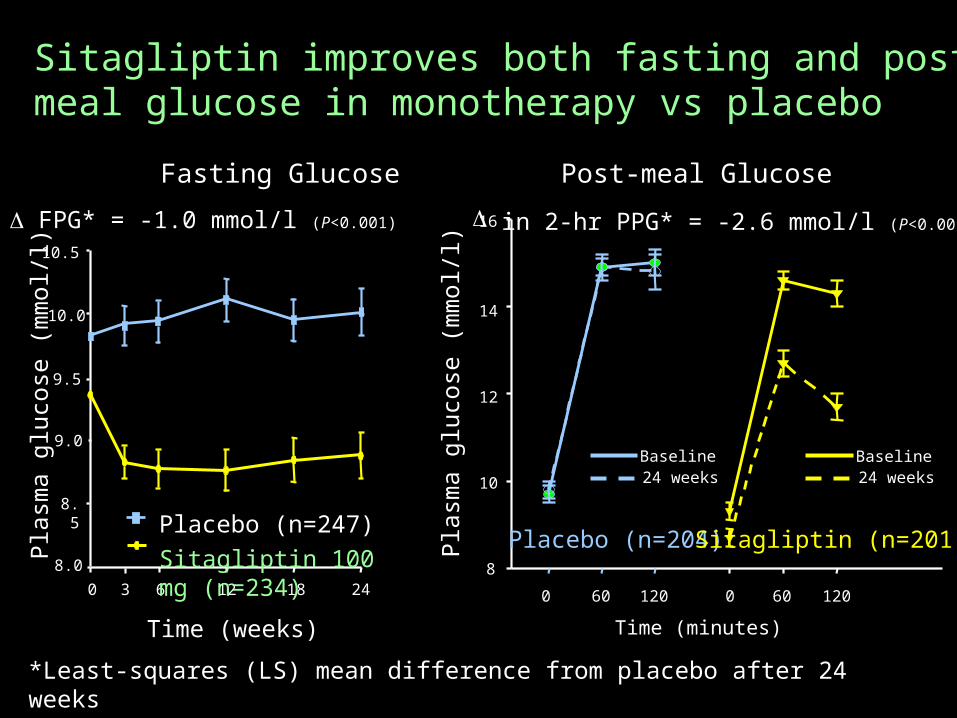
Sitagliptin improves both fasting and post-meal glucose in monotherapy vs placebo
*Least-squares (LS) mean difference from placebo after 24 weeks Aschner et al. Diabetes Care. 2006
Fasting Glucose
Pla
sma g
luco
se (
mm
ol/l)
Time (weeks)
0 6 123 18 24
Placebo (n=247)Sitagliptin 100 mg (n=234)
FPG* = -1.0 mmol/l (P<0.001)
Post-meal Glucose
Time (minutes)
Pla
sma g
luco
se (
mm
ol/l)
in 2-hr PPG* = -2.6 mmol/l (P<0.001)
0 60 120 0 60 120
8
10
12
14
16
Placebo (n=204)Sitagliptin (n=201)
Baseline24 weeks
Baseline24 weeks
9.0
9.5
8.5
10.0
10.5
8.0
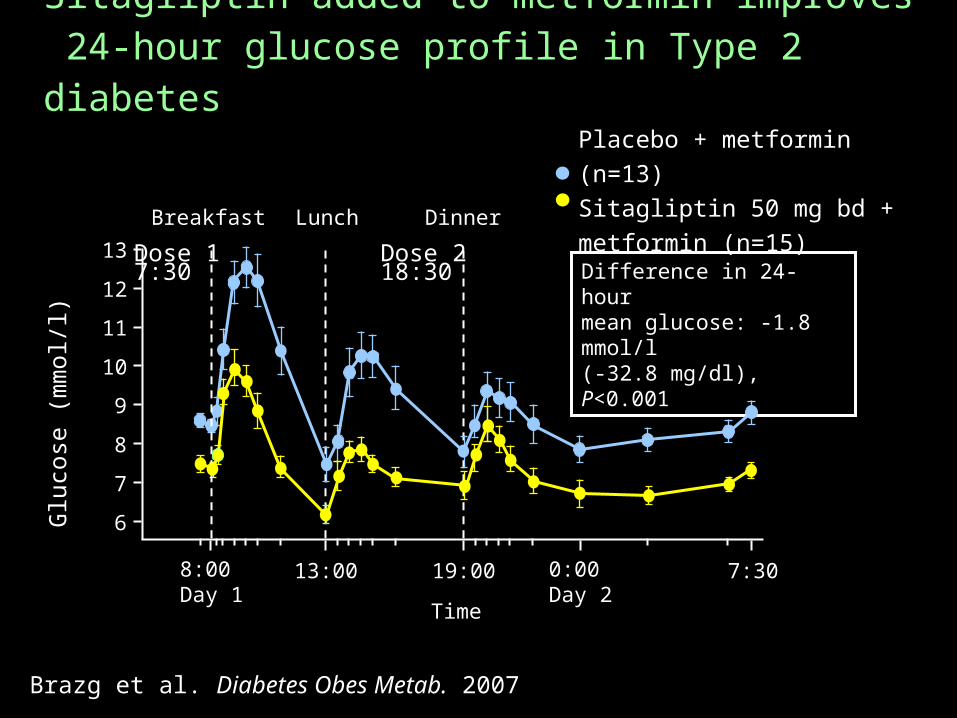
Difference in 24-hourmean glucose: -1.8 mmol/l(-32.8 mg/dl), P<0.001
Brazg et al. Diabetes Obes Metab. 2007
Sitagliptin added to metformin improves 24-hour glucose profile in Type 2 diabetes
Glu
cose
(m
mol/l)
8:00 Day 1
13:00 19:00 0:00Day 2
7:30
6
7
8
9
10
13
11
12
Dose 17:30
Dose 218:30
Breakfast Lunch Dinner
Placebo + metformin (n=13)Sitagliptin 50 mg bd + metformin (n=15)
Time
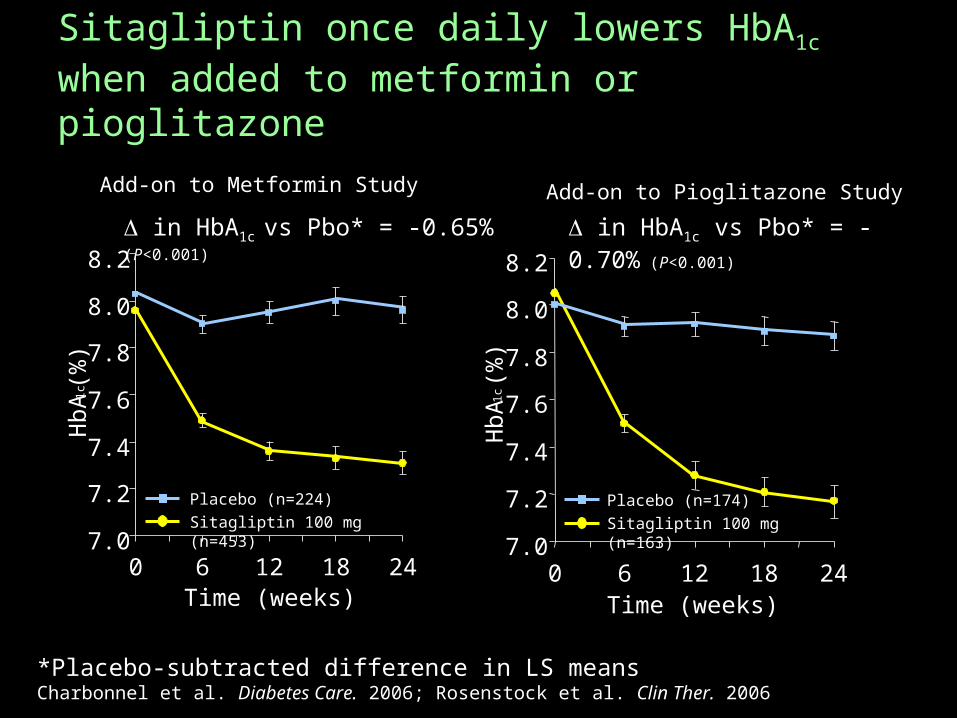
Sitagliptin once daily lowers HbA1c when added to metformin or pioglitazone
*Placebo-subtracted difference in LS meansCharbonnel et al. Diabetes Care. 2006; Rosenstock et al. Clin Ther. 2006
in HbA1c vs Pbo* = -0.65%
(P<0.001)
in HbA1c vs Pbo* = -0.70% (P<0.001)
Placebo (n=224)Sitagliptin 100 mg (n=453)
Add-on to Pioglitazone Study
Placebo (n=174)Sitagliptin 100 mg (n=163)7.0
7.2
7.4
7.6
7.8
8.0
8.2
0 6 12 18 24Time (weeks)
Hb
A1c (%
)
Add-on to Metformin Study
7.0
7.2
7.4
7.6
7.8
8.0
8.2
0 6 12 18 24Time (weeks)
Hb
A1c (%
)
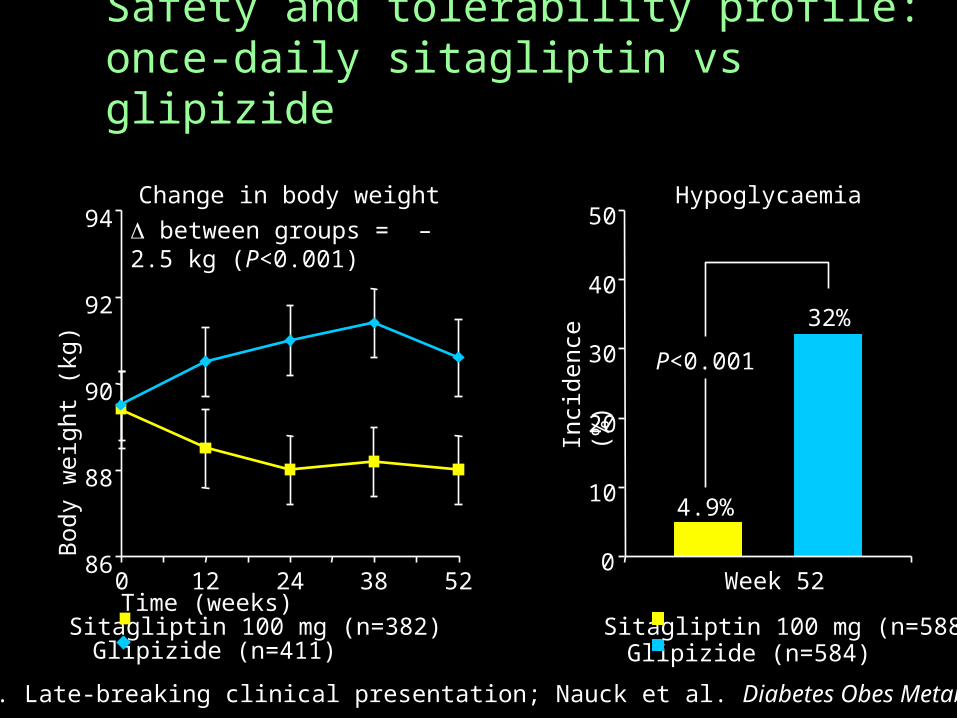
Safety and tolerability profile: once-daily sitagliptin vs glipizide
between groups = –2.5 kg (P<0.001)
Change in body weight
86
88
90
92
94
0 12 24 38 52Time (weeks)
Body w
eig
ht
(kg)
Sitagliptin 100 mg (n=382)Glipizide (n=411)
4.9%
32%
0
10
20
30
40
50Hypoglycaemia
P<0.001
Week 52In
cid
ence
(%
)
Glipizide (n=584)Sitagliptin 100 mg (n=588)
Stein. ADA. 2006. Late-breaking clinical presentation; Nauck et al. Diabetes Obes Metab. 2007
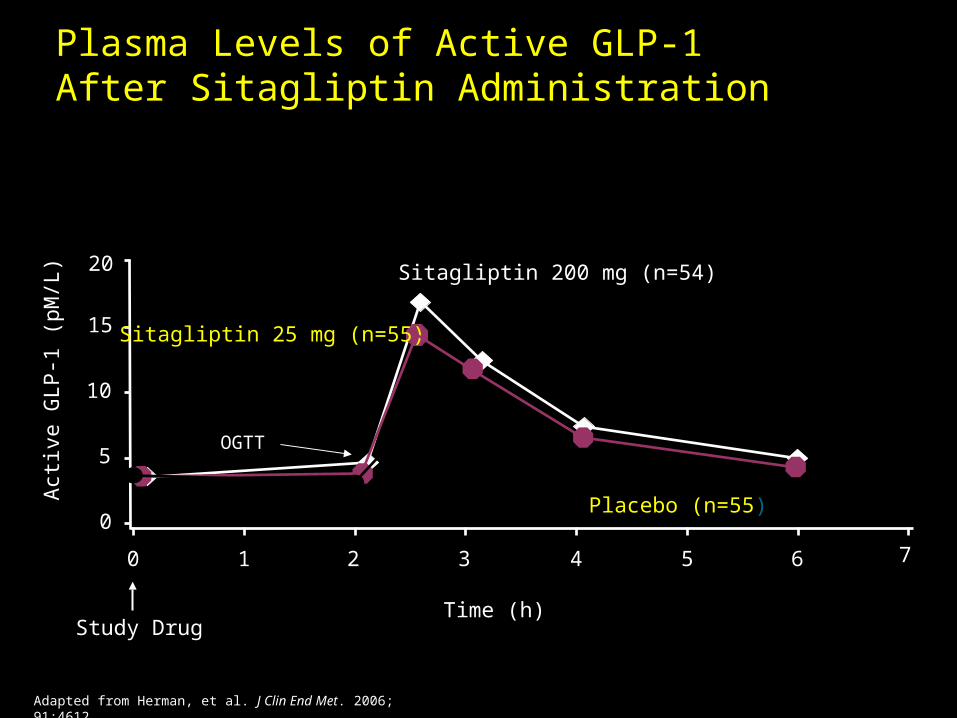
Adapted from Herman, et al. J Clin End Met. 2006; 91:4612.
Study Drug
10 2 3 4 5 6
0
5
10
15
20
OGTT
Sitagliptin 200 mg (n=54)
Sitagliptin 25 mg (n=55)
Placebo (n=55)
Act
ive
GLP
-1 (
pM/L
)Plasma Levels of Active GLP-1After Sitagliptin Administration
Time (h)
7
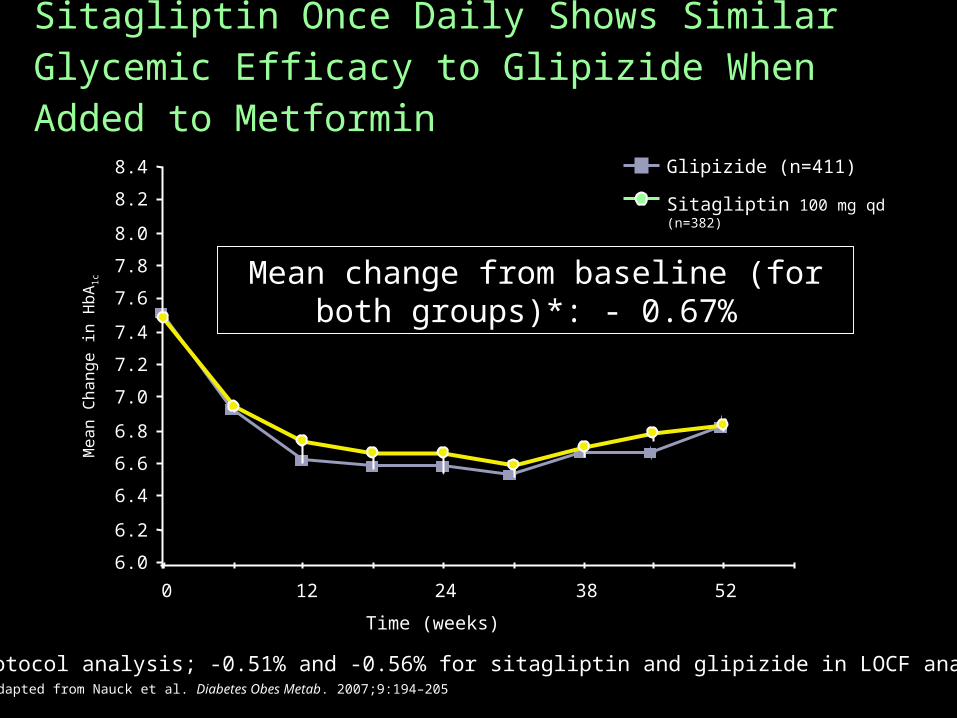
Sitagliptin Once Daily Shows Similar Glycemic Efficacy to Glipizide When Added to Metformin
Sitagliptin 100 mg qd (n=382)
Glipizide (n=411)
Mean C
hange in H
bA
1c Mean change from baseline (for both
groups)*: - 0.67%
6.0
6.2
6.4
6.6
6.8
7.0
7.2
7.4
7.6
7.8
8.0
8.2
8.4
0 12 24 38 52
Time (weeks)
*per-protocol analysis; -0.51% and -0.56% for sitagliptin and glipizide in LOCF analysis Adapted from Nauck et al. Diabetes Obes Metab. 2007;9:194–205
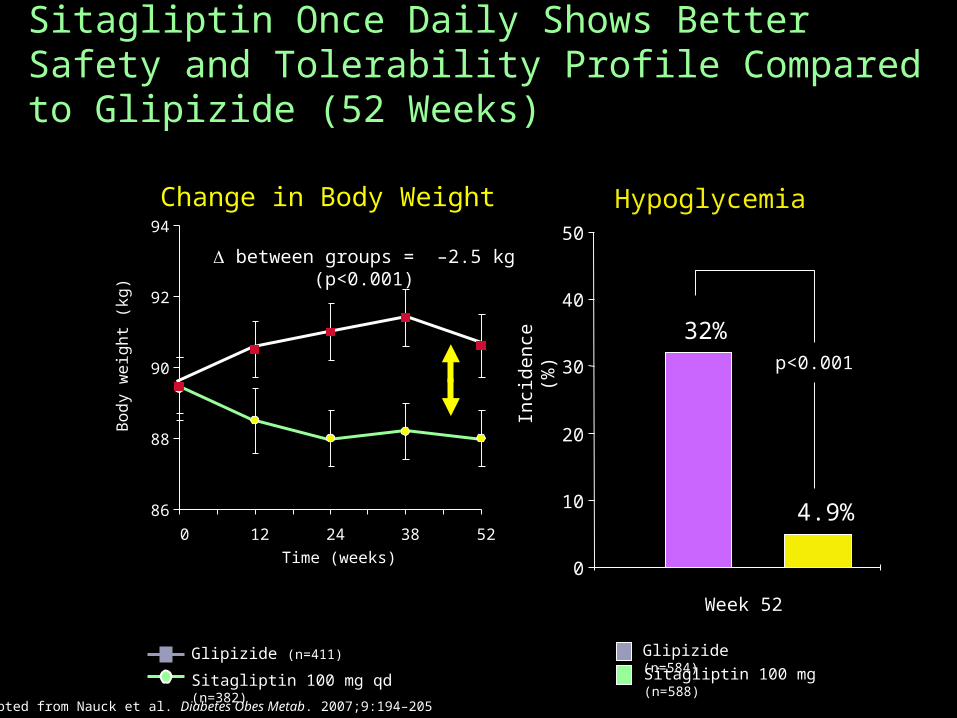
Hypoglycemia
0
10
20
30
40
50
Week 52
Inci
denc
e (%
)
Glipizide (n=584)
Sitagliptin 100 mg (n=588)
Sitagliptin Once Daily Shows Better Safety and Tolerability Profile Compared to Glipizide (52 Weeks)
p<0.001
Sitagliptin 100 mg qd (n=382)
Glipizide (n=411)
between groups = –2.5 kg (p<0.001)
32%
4.9%
Adapted from Nauck et al. Diabetes Obes Metab. 2007;9:194–205
Change in Body Weight
86
88
90
92
94
0 12 24 38 52
Time (weeks)
Bo
dy
we
igh
t (k
g)
DPP IV inhibitors – the down side DPP IV is important in the immune system
regulation. DPP IV has been reported to be a tumor
suppressor Rare reports of Stevens-Johnsons
Syndrome with sitagliptin
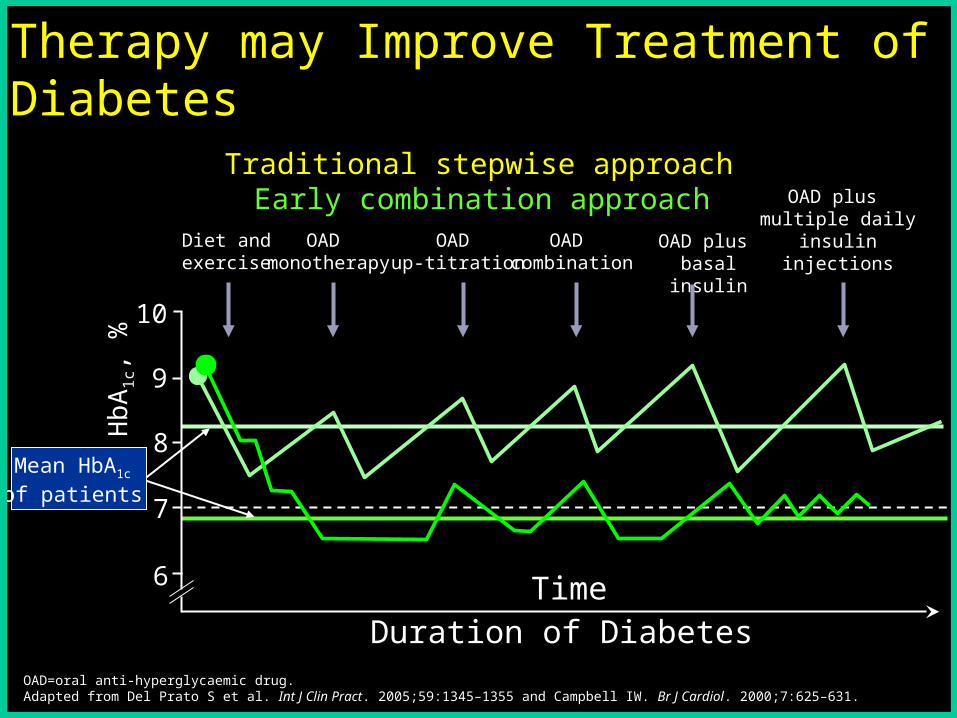
Mean HbA1c of patients
7
6
9
8
10
Hb
A1
c, %
OAD monotherapy
Diet andexercise
OAD combination
OAD up-titration
OAD plus multiple daily
insulininjections
OAD plus basal insulin
Traditional stepwise approach
Earlier Use of Combination Therapy may Improve Treatment of Diabetes
Early combination approach
Duration of DiabetesTime
OAD=oral anti-hyperglycaemic drug.Adapted from Del Prato S et al. Int J Clin Pract. 2005;59:1345–1355 and Campbell IW. Br J Cardiol. 2000;7:625–631.
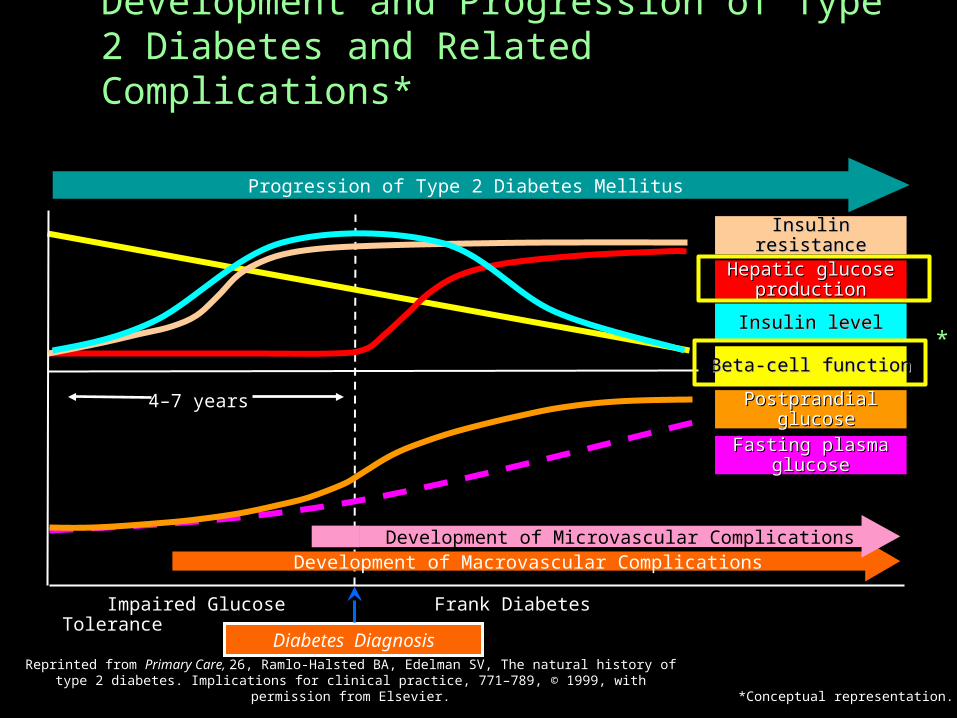
Reprinted from Primary Care, 26, Ramlo-Halsted BA, Edelman SV, The natural history of type 2 diabetes. Implications for clinical practice, 771–789, © 1999, with permission from Elsevier.
Development and Progression of Type 2 Diabetes and Related Complications*
*Conceptual representation.
Insulin levelInsulin level
Insulin resistanceInsulin resistance
Hepatic glucose Hepatic glucose productionproduction
PostprandialPostprandial glucoseglucose
Fasting plasma Fasting plasma glucoseglucose
BBetaeta-cell function-cell function
Progression of Type 2 Diabetes Mellitus
Impaired Glucose Tolerance
Diabetes Diagnosis
Frank Diabetes
4–7 years
Development of Macrovascular ComplicationsDevelopment of Microvascular Complications
*