Embed Size (px)
Citation preview

Case Report
Minimally Invasive Unilateral Percutaneous Transfracture Fixation of a Hangman’s
Fracture Using Neuronavigation and Intraoperative Fluoroscopy
Mohamed A.R. Soliman1, Benjamin Y.M. Kwan2, Balraj S. Jhawar2
-BACKGROUND: Traumatic spondylolisthesis or hangman’s fracture is acommon cervical spine fracture. Most cases of traumatic spondylolisthesis aretreated nonoperatively with external immobilization. The indications for surgeryhave generally included fracture instability or failed nonoperative management.Operative stabilization can be performed through either anterior or posteriorapproaches and has generally required instrumentation using open methods. Wepropose a technique for surgical repair of hangman’s fracture that is minimallyinvasive and motion preserving using recent advances in 3-dimensional image-guidance technology. We believe this method represents another option in thetreatment of hangman’s fractures, because it allows for immediate stabilization,prompt recovery, and quick mobilization.
-CASE DESCRIPTION: We present the case of 2 patients with hangman’sfractures who had undergone surgical unilateral transfixation with minimallyinvasive percutaneous screw placement. In both cases, we used 3-dimensionalneuronavigation and bidirectional intraoperative fluoroscopy. The operative timefrom incision to closure was <30 minutes. Preparation and positioning afterintubation varied from 40 to 150 minutes. No intraoperative complicationsoccurred. Both patients were discharged within 48 hours postoperatively. Thefollow-up examinations at 3 months, 12 months, and 5 years revealed healthybony fusion on computed tomography imaging and an excellent clinicalrecovery.
-CONCLUSION: We have provided 2 examples in which minimally invasiveunilateral fixation of hangman’s fractures proved to be safe and effective. In bothcases, the patients were immediately relieved of their pain, quickly mobilized,and promptly discharged. The achievement of successful fusion confirmed at thefollow-up examinations.
Key words- Cervical fracture- Hangman’s fracture- Image guidance- Minimally invasive- Neuronavigation- Unilateral
Abbreviations and Acronyms3D: 3-DimensionalCT: Computed tomographyK-wire: Kirschner wire
From the 1Department of Neurosurgery, Cairo University,Cairo, Egypt; and 2Department of Neurosurgery, WindsorRegional Hospital, Western University, Windsor, Ontario,Canada
To whom correspondence should be addressed:Mohamed A.R. Soliman, M.Sc.[E-mail: [email protected]]
Citation: World Neurosurg. (2019) 122:90-95.https://doi.org/10.1016/j.wneu.2018.10.140
Journal homepage: www.journals.elsevier.com/world-neurosurgery
Available online: www.sciencedirect.com
1878-8750/$ - see front matter ª 2018 Elsevier Inc. All
INTRODUCTION
Traumatic spondylolisthesis of the axis orhangman’s fracture represents w4% of allcervical spine traumas.1 Numeroustreatments have been proposed; however,for most cases external immobilization hasremained the mainstay of treatment.1-3
Rigid halo immobilization has beenreported to achieve high fusion rates>90%.2,4-6 Cervical collars have also beenused to successfully treat hangman’sfractures.1,3 Surgery could potentiallyimprove the fusion rate1,4,5,7 but the patientmust accept the additional risk.Consequently, most clinicians haveresorted to surgery as a secondary option,when traditional management has failed.1,3
In some circumstances, surgery could beindicated as a primary treatment. Halo vestsare known to compromise pulmonary vol-umes and can compromise respiratorycapacity, which can be dangerous and lead torespiratory failure in patients withpre-existing or acquired pulmonary
rights reserved.
90 www.SCIENCEDIRECT.com
conditions.8,9 Certain unstable fractures,such as Effendi type III, which involve lockedand dislocated C2-C3 facets, or Levine-Edwards type IIa/III, which involve fracturedisplacement and angulation, have also beenrecognized to be insufficiently treated byexternal fixation, and experts have generallyrecommended surgery.1-3,5,10 Halo fixationcan also fail and has its own series of com-plications, including infection, nerve injury,scalp laceration, pain, and visible scarring.1,11
Although, in general, the surgical fusionrates have tended to be greater than nonop-erative procedures, they can be associatedwith significant morbidity and/or mortality.1
Traditional surgical techniques have tendedto be open, requiring extensive dissection
WORLD NEUROSURGERY, http
and lengthy procedural times. Thecomplications have included possible bloodloss requiring transfusion, infection,lengthy recovery, and nontrivial medicalrisks for elderly individuals withcomorbidities.12 Minimally invasive surgery,however, avoids many of these issues byexposing patients to less tissue invasion.13
These techniques have been increasinglyused in spinal surgery to achieve improvedoutcomes by exploiting careful preoperativeplanning and recent innovations inneuronavigation technology.14-16
With these advantages, minimallyinvasive internal fixation of a hangman’sfracture using pedicle screw insertion withneuronavigation could be another option
s://doi.org/10.1016/j.wneu.2018.10.140

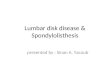
Figure 1. (AeC) Sagittal computed tomography (CT) scans of the cervicalspine showing hangman’s fracture with angulation of C2-C3 over C3. (D)Sagittal T2-weighted magnetic resonance imaging scan of the cervical spineshowing the ligamentous injury. (E,F) Sagittal CT scans of the cervical spine
showing the fixated fracture immediately postoperatively. (G,H) Sagittal CTscans of the cervical spine showing the fixated fracture at the 3-monthfollow-up visit. Sagittal CT scans of the cervical spine showing the (I) rightand (J) left sides of the fixated fracture at the 5-year follow-up visit.
CASE REPORT
MOHAMED A.R. SOLIMAN ET AL. UNILATERAL BEFORE MINIMALLY
in the management of nonangulatedhangman’s fractures in stable patients.
CASE DESCRIPTION
We present the cases of 2 patients withhangman’s fractures.
WORLD NEUROSURGERY 122: 90-95, FEB
Patient 1A 35-year-old man experienced a traumatichyperextension injury from a fall down 4stairs. He presented with neck pain and noneurological deficits. Computed tomogra-phy (CT) imaging revealed fracturesthrough both parts of C2, consistent with
RUARY 2019 www.journals.
a hangman’s fracture, type IIa (Levineclassification; Figure 1AeC). A magneticresonance imaging scan of the cervicalspine showed edema in the area of theC2-C3 interspinous ligaments, suggestingadditional ligamentous injury (Figure 1D).The patient was offered the option of
elsevier.com/world-neurosurgery 91

92 www.SCIENCEDIRECT.com WORLD NEUROSURGERY, https://doi.org/10.1016/j.wneu.2018.10.140
CASE REPORT
MOHAMED A.R. SOLIMAN ET AL. UNILATERAL BEFORE MINIMALLY

CASE REPORT
MOHAMED A.R. SOLIMAN ET AL. UNILATERAL BEFORE MINIMALLY
minimally invasive surgery, includingtransfracture fixation with the intentionto stabilize the fractured segment. Thepatient elected for surgery.The patient was brought to the oper-
ating room 4 days after injury. Afterfiberoptic intubation, he was placed inMayfield head fixation and turned tothe prone position. During the next 47minutes, the patient was positioned toachieve perfect orthogonal views withperpendicularly placed C-arms. The ante-roposterior and lateral images of the axiswere then used to calibrate our neuro-navigation system (BrainLAB, Munich,Germany) using CT fluoroscopic guidance(Figure 1C). After calibration, the potentialtrajectories were then determined on eachside through each fracture. The entrypoint was through the posterolateralportion of each facet, directedanteromedially through the pedicle andthen the fracture. For patient 1, the rightside was thought to be the idealtrajectory, and the distance from the skinto the facet was 15 cm.A 1.5-cm skin incision was made in the
posterolateral neck. A precalibrated trocarwas passed down to the facetelaminarjunction with repeated fluoroscopicimaging for guidance. Trajectories for theKirschner wire (K-wire) were then esti-mated again and confirmed. The K-wirewas inserted through the facet, pedicle,and fracture and placed as close aspossible to the anterior cortical borderwithout breaching this bone. A cannulateddrill was used to widen this trajectory withcareful attention aimed toward preventingK-wire advancement. For patient 1, a30-mm-long, 4-mm-diameter threadedscrew successfully captured the fracturedsegment and reduced the fracture(Figure 1E). The wound was closed within20 minutes of the incision.Postoperative CT imaging confirmed
excellent screw positioning and trans-fixation of the fractured segment. How-ever, a breach of the C1-C2 joint had
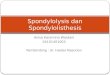
Figure 2. (A) Axial computed tomography (CT) scan ofixated fracture immediately postoperatively. Sagittal Cimmediately postoperatively. (E) Axial CT scan of thespine showing the (F) right and (G) left sides of the fifracture at the 12-month follow-up visit. Sagittal CT sfollow-up visit. (K) Axial CT scan of the cervical spinefixated fracture (left side) at the 5-year follow-up visit
WORLD NEUROSURGERY 122: 90-95, FEB
occurred, which could be avoided in futurepatients by performing 3D imaging studiesafter screw insertion. The patient hadexperienced immediate resolution of hispain on examination in the recovery roomand was discharged 2 days later.Follow-up CT imaging at 3 months
postoperatively confirmed early fusion onthe fixated right side of C2 and evidence offusion on the nonfixated left side(Figure 1G,H). At the 12-month and 5-yearfollow-up imaging studies (Figure 1I,J),fusion had occurred on both sides, withno evidence of instability.
Patient 2After an all-terrain vehicle injury, a 76-year-old man (a farmer) experiencedfractures of C1, C2, and C3. The C2 frac-ture was a hangman’s fracture type I(Levine classification) and was throughboth pars. The C1 fracture was a bilateralposterior laminar fracture, and at C3, thefracture was through the spinous process.He also had coexisting pulmonary in-juries but had no neurological deficits.The patient was offered the option ofminimally invasive surgery, includingtransfracture fixation, with the intentionto stabilize the fractured segment. Thepatient elected for surgery.The same operative method for our first
patient was used for patient 2. The prep-aration time before surgery, but afterintubation, was 150 minutes. The trajec-tory from the skin to the facet was 50 mm.The threaded screw length was 34 mm andthe diameter was 4 mm. The total surgicalcut time was 25 minutes. Postoperative CTimaging of the cervical spine showedexcellent screw positioning (Figure 2C).The patient had experienced almost
complete relief of pain postoperatively.The patient was quickly mobilized anddischarged home 2 days later. Follow-upCT imaging of the cervical spine scan at3 months postoperatively showed sub-stantial healing (Figure 2E). The right sideof the C2 vertebra where the transarticular
f the cervical spine showing the hangman’s fracture. (BT scans of the cervical spine showing the (C) fixated frac
cervical spine showing the fixated fracture at the 3-montxated fracture at the 3-month follow-up visit. (H) Axial Ccans of the cervical spine showing the (I) right and (J) leshowing the fixated fracture at the 5-year follow-up visi.
RUARY 2019 www.journals.
screw was inserted showed further union.At the 12 month follow-up study, CT im-aging showed partial union of the fractureand good apposition of the bony struc-tures (Figure 2I). No evidence of instabilitywas seen.
DISCUSSION
We have reported 2 patients who haddeveloped hangman’s fractures that weresuccessfully managed with minimallyinvasive neuronavigation-assisted instru-mented fixation. The technique allowedfor anatomical joint preservation, minimaltissue disruption, and relatively shortoperative times. We believe that with therecent advances in accuracy and reliabilityin neuronavigation technology,16-18 it isnow safer than previously to be able topercutaneously fixate fractures throughoutthe entire spine, without the need toperform extensive and potentiallydangerous dissection. Under certain cir-cumstances, in appropriate patients, andwith adequate training, we believe that theindications for surgical management ofhangman’s fractures can be widened.Hangman’s fractures are frequently
managed with conservative treatment us-ing a rigid cervical collar or halo immo-bilization device for 12 weeks, because itresults in high fusion rates and, in gen-eral, has a low rate of complications.1-3,11
However, external immobilization willnot be appropriate for all cases, inparticular, those with unstable C2 frac-tures, halo intolerance, and/or coexistingtrauma and many elderly in-dividuals.1,2,8,11,19 Complications resultingfrom external immobilization have beenreported in previous studies and havedescribed cases of pin site infection,pressure sores, and aspiration pneu-monia.8,11 Hangman’s fractures are alsopainful, with many patients requiringopioids to manage their pain. Suchtreatment can be necessary for manyweeks when patients are managed
) Axial CT scan of the cervical spine showing theture (right side) and (D) fixated fracture (left side)h follow-up visit. Sagittal CT scans of the cervicalT scan of the cervical spine showing the fixatedft sides of the fixated fracture at the 12-montht. (L) Sagittal CT scan of the cervical spine of the
elsevier.com/world-neurosurgery 93

CASE REPORT
MOHAMED A.R. SOLIMAN ET AL. UNILATERAL BEFORE MINIMALLY
nonoperatively. Our 2 patients were able tobe weaned off opioids rapidly. Theyexperienced immediate pain controlwithin hours after surgery. Cervical collarswere not necessary.Traditional open surgical techniques in
the management of hangman’s fracturescan be fairly invasive and associated withsmall, but significant, risks of injury to thevertebral artery, spinal cord, and nearbyneural structures.1,12 Commonly usedsurgical methods have included anteriorfusion of C2 and C3 with interpositionalbone grafts and cervical plating, which hasrisks such as injury to the facial nerve orexternal carotid artery branches and lossof range of motion.10,15,20 Posteriorsegmental fusion has also been proposedas a treatment of hangman’s fracture withalmost perfect fusion rates.15,21 However,posterior segmental fusion results in sig-nificant reduction in rotational move-ment.15 Furthermore, the extensivedissection results in a more difficultrecovery than with anterior procedures.16
Judet et al.22 in 1970 proposedtranspedicular osteosynthesis, which is a“physiological” operation, because itleads to direct fixation of the fractureand preservation of the range of motion,does not lead to segmental fusion, andallows for anatomic healing.14 However,their method of pedicle screw fixationdoes have important risks such astrauma to the vertebral artery and/orspinal cord.23 Minimally invasive versionsof their method have since beenproposed to help limit the risks oftrauma to neurovascular structures byallowing for preoperative assessment ofthe fracture path using neuronavigation.The use of neuronavigation includes theability to select the best screw trajectory,screw placement point, and screwlength.14,15,20 Intraoperative assessmentcan also be obtained through C-armfluoroscopy, allowing for live imaging ofthe screw insertion.14,15,20
In the past, neuronavigation had majorinaccuracies, with numerous examples ofmisplaced screws.16,24,25 However, thetechnology has continued to advance andhas matured to a level of clinical accept-ability.16 Recent advances inneuronavigation have increased theaccuracy substantially, and the presenttechnologies are capable of use tocannulate small pedicles.13,26 A review by
94 www.SCIENCEDIRECT.com
Tjardes et al.27 on neuronavigation forspinal surgery highlighted the use ofCT-guided, 2-dimensional and 3D fluo-roscopy usage during surgery throughoutthe cervical spine, including odontoidfractures, atlantoaxial instability, C6-C7subluxation, and hangman’s fractures.Image-guided variants of the approachreported by Judet et al.22 are becomingmore common and have been describedusing both intraoperative CT guidance byTaller et al.14 and isocentric mobile C-arm 3D navigation navigation byRajasekaran et al.15,20
We have proposed the use of 2 C-armsto take both anteroposterior and lateralradiographs with neuronavigation forunilateral minimally invasive percutaneoustransarticular screw fixation of a hang-man’s fracture.15 This surgical operationdoes have important risks, includingvertebral artery injury, cervical nerveinjury, spinal cord injury, and pediclecompromise during insertion. Excessiveadvancement of K-wires andmisadvancement of K-wires must bemonitored constantly.18 Although in our2 patients, the position of the vertebralartery was inferred by the location of theforamen transversarium, angiographicstudies such as CT angiography ormagnetic resonance angiography couldaid surgical planning and decrease therisk by choosing to fixate the side withthe nondominant vertebral artery.Complications will be minimized,however, using the percutaneousapproach, which helps to limit bloodloss and injuries to the vertebral artery.This technique might also be more cost
effective than nonoperative care becausethe discharge for our patients was prompt.Another novel aspect of our approach wasthe decision to perform only unilateralscrew fixation. We believe that unilateralfixation is sufficient to achieve fusionbecause both of our patients had experi-enced immediate pain relief after surgery,suggesting that the fractured segment hadbeen stabilized. Under such circum-stances, bony fusion should occur, giventhe appropriate passage of time. Unilateralfixation has the obvious advantage ofreducing risk by �50%. Should failureoccur, the contralateral pedicle will remainfor repeated surgery.28 In addition, thistechnique offers another treatmentoption for nonangulated hangman’s
WORLD NEUROSURGERY, http
fractures in stable patients and reducibleangulated fractures in the absence ofC2-C3 disc herniation. The use of preop-erative CT angiography or magnetic reso-nance angiography in future cases to selectthe nondominant vertebral artery couldfurther decrease the risk of vertebral arteryinjury.
CONCLUSION
Although external immobilization remainsan important treatment modality, it is notwithout complications or impair-ment.1-3,8,9 We have proposed a novelmethod of fixation of nonangulatedhangman’s fracture in stable patients andin patients with reducible unstable frac-tures in the absence of C2-C3 disc herni-ation. Our method is minimally invasive,with a short operative time, allows forquick mobilization, preserves the range ofmotion, and offers a short recoverytime.14,15,20,28 We believe that withadequate training and experience, thismethod can be safely used to improveoutcomes and achieve high rates of fusion.As advancements in intraoperative imag-ing and navigation continue, thesemethods will be increasingly used to treatspinal injuries.16,29 However, our studywas small. We encourage further evalua-tion with larger patient series andthoughtful analysis before general recom-mendations are made.
REFERENCES
1. Pryputniewicz D, Hadley M. Axis fractures.Neurosurgery. 2010;66:A68-A82.
2. Li X, Dai L, Lu H, Chen X. A systematic review ofthe management of hangman’s fractures. Eur SpineJ. 2006;15:257-269.
3. Hadley MN, Walters BC, Grabb PA, Oyesiku NM,Przybylski GJ, Resnick DK, et al. Isolated fracturesof the axis in adults. Neurosurgery. 2002;50(suppl):S125-S139.
4. Francis W, Fielding J, Hawkins R, Pepin J,Hensinger R. Traumatic spondylolisthesis of theaxis. J Bone Joint Surg Br. 1981;63B:313-318.
5. Effendi B, Roy D, Cornish B, Dussault RG,Laurin CA. Fractures of the ring of the axis: aclassification based on the analysis of 131 cases.J Bone Joint Surg Br. 1981;63:319-327.
6. Greene KA, Dickman CA, Marciano FF,Drabier JB, Hadley MN, Sonntag VK. Acute axisfractures: analysis of management and outcomein 340 consecutive cases. Spine (Phila Pa 1976).1997;22:1843-1852.
s://doi.org/10.1016/j.wneu.2018.10.140

CASE REPORT
MOHAMED A.R. SOLIMAN ET AL. UNILATERAL BEFORE MINIMALLY
7. Borne G, Bedou G, Pinaudeau M. Treatment ofpedicular fractures of the axis: a clinical study andscrew fixation technique. J Neurosurg. 1984;60:88-93.
8. Taitsman LA, Altaman DT, Hecht AC, Pedlow FX.Complications of cervical halo-vest orthoses inelderly patients. Orthopedics. 2008;31:446.
9. Lind B, Bake B, Lundqvist C, Nordwall A. Influ-ence of halo vest treatment on vital capacity. Spine(Phila Pa 1976). 1987;12:449-452.
10. Xu H, Zhao J, Yuan J, Wang C. Anterior disectomyand fusion with internal fixation for unstablehangman’s fracture. Int Orthop. 2010;34:85-88.
11. Longo UG, Denaro L, Campi S, Maffulii N,Denaro V. Upper cervical spine injuries: in-dications and limits of the conservative manage-ment in halo vest. A systematic review of efficacyand safety. Injury. 2010;41:1127-1135.
12. Dekutoski M, Norvell D, Dettori J, Fehlings M,Chapman J. Surgeon perceptions and reportedcomplications in spine surgery. Spine (Phila Pa1976). 2010;35:S9-S21.
13. Jaikumar S, Kim DH, Kam AC. History of mini-mally invasive spine surgery. Neurosurgery. 2002;51(suppl 2):1-14.
14. Taller S, Suchomel P, Lukas R, Beran J. CT-guidedinternal fixation of a hangman’s fracture. Eur SpineJ. 2000;9:393-397.
15. Rajasekaran S, Vidyadhara S, Shetty A. Iso-C3Dfluoroscopy-based navigation in direct pediclescrew fixation of hangman fracture. J Spinal DisordTech. 2007;20:616-619.
16. Foley KT, Holly LT. Image guidance in spinesurgery. Orthop Clin North Am. 2007;38:451-461.
WORLD NEUROSURGERY 122: 90-95, FEB
17. Papadopoulos EC, Girardi FP, Sama A,Sandhu HS, Cammisa FP Jr. Accuracy of single-time, multilevel registration in image-guided spi-nal surgery. Spine J. 2005;5:263-268.
18. Scheufler KM, Franke J, Eckardt A, Dohmen H.Accuracy of image-guided pedicle screw place-ment using intraoperative computed tomography-based navigation with automated referencing, partI: cervicothoracic spine. Neurosurgery. 2011;69:782-795.
19. Tashjian RZ, Majercik S, Biffl WL, Palumbo MA,Cioffi WG. Halo-vest immobilization increasesearly morbidity and mortality in elderly odontoidfractures. J Trauma. 2006;60:199-203.
20. Rajasekaran S, Vidyadhara S, Shetty A. Intra-operative Iso-C3D navigation for pedicle screwinstrumentation of hangman’s fracture: a casereport. J Orthop Surg. 2007;15:73-77.
21. Ma W, Xu R, Liu J, Sun S, Zhao L, Hu Y, et al.Posterior short-segment fixation and fusion inunstable hangman’s fractures. Spine (Phila Pa 1976).2011;36:529-533.
22. Judet R, Roy-Camille R, Saillant G. Actualites dechirurgie orthopedique de l'Hospital Raymond-Poincare. In: Judet R, ed. Fractures du rachis cervical.8th ed. Paris: Masson; 1970:174-195.
23. Abumi K, Shono Y, Ito M, Taneichi H, Kotani Y,Kaneda K. Complications of pedicle screw fixationin reconstructive surgery of the cervical spine.Spine (Phila Pa 1976). 2000;25:962-969.
24. Holly LT, Foley KT. Intraoperative spinal naviga-tion. Spine (Phila Pa 1976). 2003;28:S54-S61.
25. Francesco C, Andrea C, Ortolina A, Fabio G,Alberto Z, Maurizio F. Spinal navigation: standardpre-operative versus intra-operative computed to-mography data set acquisition for computer-
RUARY 2019 www.journals.
guidance system. Radiological and clinical studyin 100 consecutive patients. Spine (Phila Pa 1976).2011;36:2094-2098.
26. von Jako R, Finn MA, Yonemura KS, Araghi A,Khoo LT, Carrino JA, et al. Minimally invasivepercutaneous transpedicular screw fixation:increased accuracy and reduced radiation expo-sure by means of a novel electromagnetic navi-gation system. Acta Neurochir. 2011;153:589-596.
27. Tjardes T, Shafizadeh S, Rixen D, Paffrath T,Bouillon B, Steinhausen ES, et al. Image-guidedspine surgery: state of the art and future direction.Eur Spine J. 2010;19:25-45.
28. Song GS, Theodore N, Dickman CA, Sonntag VK.Unilateral posterior atlantoaxial transarticularscrew fixation. J Neurosurg. 1997;87:851-855.
29. Park P, Foley KT, Cowan JA Jr, La Marca F.Minimally invasive pedicle screw fixation utilizingO-arm fluoroscopy with computer-assisted navi-gation: feasibility, technique, and preliminary re-sults. Surg Neurol Int. 2010;1:44.
Conflict of interest statement: The authors declare that thearticle content was composed in the absence of anycommercial or financial relationships that could be construedas a potential conflict of interest.
Received 11 July 2018; accepted 22 October 2018
Citation: World Neurosurg. (2019) 122:90-95.https://doi.org/10.1016/j.wneu.2018.10.140
Journal homepage: www.journals.elsevier.com/world-neurosurgery
Available online: www.sciencedirect.com
1878-8750/$ - see front matter ª 2018 Elsevier Inc. Allrights reserved.
elsevier.com/world-neurosurgery 95