Embed Size (px)
Citation preview

Mirto Foletto, MD
Bariatric Unit - Padova University Hospital (Italy)
Lessons from a Week Surgery Unit

standard of careresources
3rd millennium biggest challenge
matchin'

Mainstays of bariatric practice
• Multidisciplinary discipline
• Private or Public settings
• Community or Academic Institutions
• Dedicated or intermingled wards
• Outcomes and costs
• Covering (insurance, self payer, NHS)
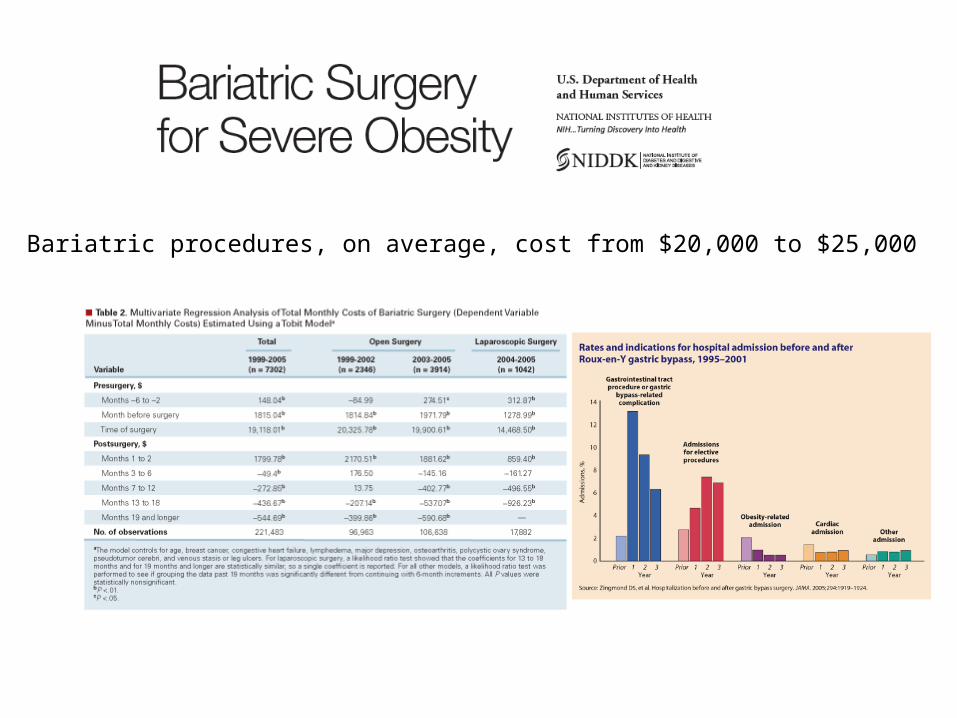
Bariatric procedures, on average, cost from $20,000 to $25,000

CoE policy
Accreditation should impact on outcomes and costs

THE SETTING IS THE KEY ISSUE !
healthcare = complexity

•Organizational pathologies (1)
•High variation of clinical processes•underuse of effective care, overuse of supply-sensitive care and misuse, i.e. failures to execute procedures properly
•Low reliability (failure-free operation over time) of clinical processes
••Trust paper tools, memory, and hard work••Ample tolerance toward clinical autonomy••Reliability goals not explicitly stated••Performance judged against (mediocre) averages of outcomes rather than benchmarks of processes

Organizational pathologies (2)
Lack of system thinking
little understanding of interactions between structures, processes,patterns and results; little involvement of keystakeholders, esp. front-line professionals
Lack of statistical thinkingoverreactions in front of common causes, i.e. thinking that change hasoccurred and decisions are necessary when infact there is no change
Lack of quality improvement methods messy use of fragments of improvement models

System thinkingAll work occurs in a system of inter-relatedprocesses, i.e. sets of sequential activities that turn inputs into outputs and outcomes, which affect customers
A system is heavily influenced by connectionsamong its parts, more than by the isolatedperformance of its elements; hence optimizingeach one independently can result in an evenpoorer performanceProcesses should be studied systematically visualizing them through flowcharts and measuring their important stepsEvery system is perfectly designed to get the results it gets. If we want different results, we must change the system
Statistical analysis is essential in order to turn data into useful knowledge

AIM
TO ASSESS WHETHER A MODIFICATION TO THE APPROACH OF A PATIENT CANDIDATE FOR BARIATRIC SURGERY CAN IMPACT ON OUTCOMES AND COSTS
setting: academic hospital
intermediate intentensity of care
"week surgery" ward
Methods•6-MONTH ACTIVITY PROSPECTIVE ANALYSIS OF
LSG •SINGLE SURGEON - SINGLE INSTITUTION BASED •BEFORE (GROUP A) AND AFTER (GROUP B) Wk
SURGERY UNIT ACTIVATION
VARIABLES
Operating Room Time (OR)
Hospital stay (HS)
Early complications rate (EC)
STATISTICSt-TEST FOR PARAMETRIC
Fisher for non parametric
set point p < 0.005
COSTSASSESSED ACCORDING ACTIVITY BASED COST MODEL

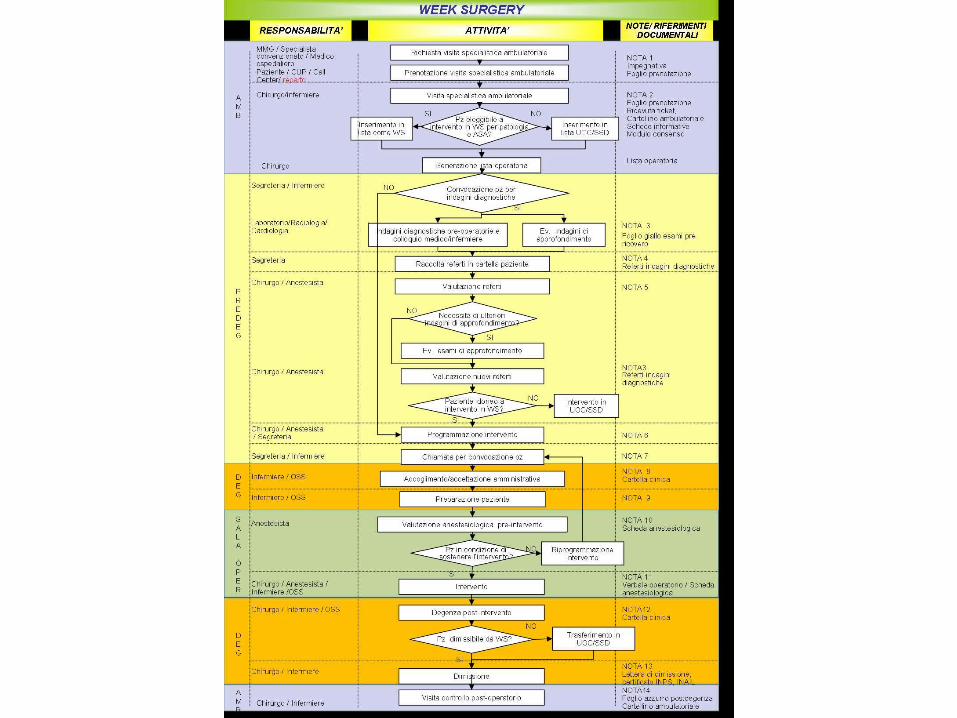
The "Week Surgery" model Improving care through affordability
what we had
standardized clinical pathwaypatients' selection health professionals
24-bed ward
2 ORs 8-14
10 scrub nurses
10 ward nurses
0-24 Mo-Th
Gates closed Fr 20
patients surgeons
anesthesiologists

The "Week Surgery" model Improving care through affordability
OR SLOTSwk surgerystakeholders
bariatric unit endocrine surg E-G junctionbreast unit
miscellaneousskin and SQgall bladderhernia surg
mo-wed
thu-fri



standard of care
who does what
risk management

Group AGroup A
ord wardord ward
(55 pts)(55 pts)
Group BGroup B
WS wardWS ward
(67 pts)(67 pts)
•F F 32 (58,2%)32 (58,2%) 47 (70,1%)47 (70,1%)
•M M 23 (41,8%)23 (41,8%) 20 (29,9%)20 (29,9%)
Age (anni)Age (anni) 47,2 ± 10,447,2 ± 10,4 45,5 ± 9,845,5 ± 9,8
BMI (kg/mBMI (kg/m22)) 48,4 ± 7,848,4 ± 7,8 46,9 ± 7,746,9 ± 7,7
•comorbiditiescomorbidities 7 (12,7%)7 (12,7%) 10 (14,9%)10 (14,9%)
•morbid obesitymorbid obesity 25 (45,5%)25 (45,5%) 35 (52,2%)35 (52,2%)
•Super obese Super obese 23 (41,8%)23 (41,8%) 22 (32,8%)22 (32,8%)
Previous bariatric Previous bariatric surgerysurgery
16 (29,1%)16 (29,1%) 8 (11,9%)*8 (11,9%)*
6-mos LSG outcomes by ward

Results Results
Group AGroup A
55 pts55 pts
Group BGroup B
67 pts67 pts
Operative time (min)Operative time (min) 89,3 ± 2989,3 ± 29 57,9 ± 12*57,9 ± 12*
early complicationsearly complications 10 (18,2%)10 (18,2%) 4 (6%)4 (6%)§§
Hospital Stay (days)Hospital Stay (days) 5,3 ± 2,65,3 ± 2,6 3,4 ± 0,5*3,4 ± 0,5*
** p<0,0001 p<0,0001
§§ p<0,04 p<0,04

COSTSCOSTS
OR + EC + HS
=
2000 Euros
Group A vs Group B

CONCLUSIONSCONCLUSIONS
Bariatric Surg A MODEL for elective Surgery
Patterns of care IMPACT ON:
• OUTCOMES
• PERFORMANCE
• COSTS
COE accreditation alone is not enough





























