-
7/30/2019 MIS Behavior 2012 v 7
1/22
-
7/30/2019 MIS Behavior 2012 v 7
2/22
ABSTRACT
In pediatric minimally invasive surgery (MIS), the
advantages of expert technique are demonstrable, but moving
from novice to expert often seems more the product of
fortunethanintent. Meanwhile, themodernresidencyis being
driven away from unlimited hours of direct experience and
towardformal curricula, more didactics, lessons on
simulators,
and learning metrics. Advocates and critics of these changes
probablycanagree:WeneedtoteachmoreefEiciently.Thatis,
each trainee must make more progress toward expertise
(howeverdeEined)inlesstime.InpediatricMIS,thatneedseems
magniEied, but safe surgical methodology hinges less on
contrived core competencies than on sound principles
andheuristics. Thisessaydescribesteachable principlesdesignedto
improve mechanicaladvantage inanyMIS procedure. Pediatric
surgical residents who learn these principles exhibit
easier,
faster,andsaferminimallyinvasivetechnique.
KYWORDS: laparoscopy,
thoracoscopy,minimallyinvasivesurgery,surgicaleducation,
residenttraining,heuristics
Page 2 of 22
-
7/30/2019 MIS Behavior 2012 v 7
3/22
INTRODUCTION
As tomethods theremaybeamillionandthensome,butprinciples
arefew.Themanwhograspsprinciplescansuccessfullyselecthisown
methods. Themanwho triesmethods, ignoring principles, is sure
to
havetrouble.RalphWaldoEmerson
Minimally invasivesurgery(MIS)is hardto teach. To begin
with, it is hard tolearn(1). Theskills neededfor
successfulMISare
groundedingoodopensurgicaltechnique,butexpertabilitytoperform
agivenoperationusingopentechniqueisonlytheFirstprerequisiteto
endoscopicexpertise. SuccessfulMISrequires a superset ofskills
to
perform complex procedures in small spaces with long tillers
via
remotevisualization.MISisnotareplacementforgoodsurgicalhabits
andtechniques,but is
averypowerfulextensionofsurgicaltechnique.
DespitesomeskepticismofMISinpediatricsurgery(2,3),thepotentialbeneFits
to patients are plain: smaller incisions create far less
morbidity.
Nevertheless,clumsylaparoscopictechniqueisnotminimally
invasive. Ad hoc practices and imprecise maneuvers lead to
long
operating and anesthetic times, poor mechanical results, and
return
tripstotheoperatingroom.TheserisksareampliFiedinchildren:
The variety ofcases isbroader, includingcasesin thechest,
abdomen, andpelvis associated with a very wide variety of
malformations and other problems. The scope of required
expertiseisverybroad.
Thepatientsaremuchmoredelicate,andhavemuchsmaller
structures.Therefore,precisemovementofinstrumentswithin
bodycavitiesisessentialforsafetissuemanipulationandgood
surgicalresults.
Scaling effects of biomechanical structures and essential
physiology createnewsurgicalconstraints. or example,the
abdominal wall of a baby is relatively similar in thickness
comparedto that ofa leanadult, but itsabsolutethickness is
muchsmaller,dramaticallyreducingitsabilitytoholdatrocar
in place. Technique must be speciFically adapted to
accommodate thethinabdomen. Similarly, round structures(such as
esophagus, etc) must be perfectly approximated
duringrepair, lest nonlinear increases in resistance at
small
diametersleadtopooroutcomes.
The patients are muchmore sensitive to hypothermia than
adults because of their diminished metabolic capacity,
diminished reserve, and physical characteristics allowing
greater heat loss. Poor endoscopic technique can actually
Page 3 of 22
-
7/30/2019 MIS Behavior 2012 v 7
4/22
placesmallpatientsatincreasedriskofhypothermiacompared
to open technique, as long operating times and poor
instrumentation choices force high insufFlation Flows to
maintain visualization. The energy required to heat and
humidify high-Flow insufFlation gas can easily be twice the
basalmetabolicrateofababy. The instruments are shorter,
narrower, andmore delicate.
Relativelyfewtoolsarespeciallyadaptedforpediatricuse.
Thestakesfromamisadventure canbemuchhigher(e.g.In
anadult,90mLofbloodlossistrivial;ina3kgchilditis1/3of
the total blood volume), and complications seem to be
somehowmoretragicinchildrenthaninadults.
or all of these reasons, the margin for error in small patients
is
disproportionatelysmall.
The objectiveofthis essay is to set outdiscreteprinciples of
good pediatric minimally invasive surgical techniquebeyond
simple
exercises(4,5).Theheuristicslistedhereareintendedtomaximizethe
surgeons mechanical advantageat all times, inallcases.
Maximum
mechanical advantage fosters precision and spares the
surgeon
unnecessary fatigue,keepshimaway
fromavoidableblunders,creates
optionsforrecoveringfrom
slipsorunexpectedanatomicalchallenges,
increases,shortensoperatingtime,andprotectsthepatient.
Surgery is a physical art. Surgeryis
theartofapplyingmechanicalsolutions
tomedicalproblems.Assuch,surgicalinterventionsleadtothebestresultswhen
thosemedical problems have amechanical basis. Someexamples
for
whichsurgeryisthebest interventioninclude:
repairingthedamage
from a stab incision; removing a tumor; relieving an
intestinal
blockage;reconnectingthe esophagus; restoring the insertion of
the
ureter on the bladder;repairing ameniscal tear. These,
andmany
other problems allhaveamechanicalproblemastheir source, anda
mechanicalsolutionisdemanded.However,surgerysometimesisused
for diseases that arenot strictlymechanical, but more
physiological,
somedisorder at
thecellularlevel.orexample,ulcerativecolitismaybe treated by
colectomy, but this is morepalliationthan cure: the
surgeonhasnotrepairedabiomechanicalproblem,only removedan
organ afFlicted with an inFlammatory disease that we dont
really
understand.Thesamemaybesaidforobesitysurgery.Observethatas
ageneralrule, theresultsformechanical interventions
tomechanical
problems are superior to those for physiological ones: repairing
a
Page 4 of 22
-
7/30/2019 MIS Behavior 2012 v 7
5/22
duodenum damaged by a handle-bar is better than removing the
antrumofthestomachtopreventulcersintheduodenum.
Inthis way, surgery is akind of engineering. Inorder to
achieve thebest results,surgeons must know about theirtools,
their
materials, the raw substrate they are manipulating, and what
the
mechanicalobjectiveisthattheyaretryingtoachieve.Trytostatethepurelymechanicalobjectivesof:
fundoplasty
diaphragmaticplication
appendectomy
gunshotwound
inguinalherniarepair
In diaphragmatic plication for example, there are two
objectives:
increasefunctionalresidualcapacityoftheipsilaterallung,andprovide
alesscompliantmedialborderto thecontralateralhemidiaphragmso
to increaseitsdeFlectionforthesamemuscular contraction.
Compare
mechanicalobjectiveslikethiswithpalliativeobjectivesin,forexample,
colectomyforulcerativecolitis,orpancreatectomyforhyperinsulinism.
In each of these later cases, the basis of the treatment
isnt
biomechanical,butsimplytoremovethedysfunctionalorgan,tradinga
diseasedphysiologytosomelesserdysfunction.
In indirect inguinal hernia repair, the objective is to
permanently close the internal ring (while avoiding damage to
the
spermatic cordstructures). What approachmostlikelyachieves
this?
Laparoscopic repairs
allowthesurgeontovisualizetheringataround
8xmagniFicationdecreasingtheprobabilityofdamagingthecord.But
early results showed a disappointingly high recurrence rate.
This
problem vanished when permanent suture was used instead of
the
moretraditionalabsorbablesutureusedinopentechnique.Itappears
that whilethemechanical objective (permanently close the
internal
ring)ofopenandlaparoscopicrepairsisthesame,the methodmaybe
different--one technique disconnects the sac, one does not--and
so
different materials must be used. Still, whatever the details of
the
method,themechanicalobjectiveisthesame,andmustbeachievedfor
a successful repair regardless of whether the approach is open
or
laparoscopic.The ten principles here increase the chances that
the mechanical
objectivesofagivenprocedurewillbeachieved.
Page 5 of 22
-
7/30/2019 MIS Behavior 2012 v 7
6/22
#1 Perfect Operations Begin With Perfect Tools
IfIhad8hourstocutdownatree,Iwouldspend6hourssharpeningmy
axe.
AbeLincoln.
Therighttoolscamera,ports,instruments,scopesmakethe
difference between a safe operation performed smoothly under
conditionsofexcellentvisualizationandaFlail.Inthisway,patient
safety is seen to begin with (but not end with) well-chosen
and
perfectlymaintainedtools.
MIS instrument maintenance and replacement is often
neglectedinhospitals eventhoughtheinstrumentshaveafar
shorter
usable lifetimethanthoseusedinopenprocedures. Astainless
steel
Kocher clamp will work reliably for generations; a Fine 3mm
endoscopic needle-driver will be sprung in a few years or less
and
endoscopic scissors may not last more than a single
operation.
OperatingroombudgetsmustreFlecttheseshorterusefullifetimesand
plan for constant replacement of defective instruments.
Clever
operatingrooms partnerwithvendorstomaintaintheinstrumentson
a constant basis, vastly extending these tools working lives.
An
operatingroom staffthatholdsoutastandardoflikenewoperation
for everyinstrument for everycase protectsbothitsownbottom
line
andits patients. Put moresimply,toolsthat
arenotgoodenoughfor
useonyourownchildarenot goodenough. It is thesurgeons job to
insistonthisstandard.
Perfectoperationsareperformedwithtoolsthathavesmooth,low-resistance
working parts, precision approximation at the tip,
reproducibleandpredictableaction.
Anexpertwieldsthesetools,the
long reach from hand to organ hardly noticed. In contrast,
poorly
functioningtools canbedeadly.Whileanexperiencedsurgeonwillbe
irritated and slowed by sticky instruments, the novice will
be
thoroughly Flummoxed, operatingwith jerkymoves
andhaltingover-
corrections. The delicate infant liver, Fine sutures, and
ephemeral
tissueplanes becomeinevitablecasualties.
Then,disruptedanatomy
and bloody, obscured views makes the operation even harder,
producing a feed-forward spiral to sub-optimal results at least,
and
disasteratworst.Wellchosen,wellfunctioningtoolsmustberegardedandbudgetedasindispensablecontributorstopatientsafety.
Animportant corollaryhereisthat theexpert knows howall
his toolswork. Heknowshowthetools Fit together, howfeedback
is
measuredbytheinsufFlator,howFlowrelatestohypothermia,howthe
variousenergysourcesworkandwhattheirlimitsandliabilitiesare.A
noviceisbafFledbypoorinsufFlation;anexpertknowshowtotrackand
disposeofproblemsinstantly,fromtheCO2source,totheinsufFlator,to
Page 6 of 22
-
7/30/2019 MIS Behavior 2012 v 7
7/22
thetubing,to thetrocars,to
theinstruments,tothelevelofanesthesia.
The expert chooses hook, or spatula, or hot scissors, or
Harmonic
Scalpel (Ethicon, Endosurgery, Cincinnati, OH), or Ligasure
(ValleyLab,Boulder,CO)accordingtothewaytheydeliverenergy,how
the shape of the business end Fits his surgical Field, and
what
problems areminimizedbychoosing oneover theother.
Thenovicehasonetoolandtries touseiteverywhere.
Anoviceblamesthetools;
theexpertstoolsservehistechnique.
In other words, MIS is not technology; it is technique.
Surgeons liketechnology. Thenumberandvarietyofinstrumentsand
devicesforuseintheoperatingroomrunsintothethousands.Withthe
spread of endoscopic methods, vendors have hugely expanded
the
available tools. Certainly technological progress in
charge-couple
devices, electronics,optics, andmaterials has helpedspur
thebroad
applicationofMISmethods,andongoingadvances(especiallyinoptics)
willcontinuetoaidtechniqueandhelppatients.Butalargenumberof
theseare meregadgets, engineered solutions to non-problems.
or
example, suture assist devices exist in order to bridge a
deFicit of
sewingandtyingskill. Vendorshavemarketedallmannerof devices
thatholdincommononlythattheyarecomplex,expensive,andtotally
unnecessarytotheexpertendoscopicsurgeon.
The tools never do theoperation. or example, thesurgical
robot is really a telemanipulator (or a waldo), andcannot make
a
novice endoscopic surgeon into an expert one. Even suture
assist
devices that use ski-needlesarenotanasset but a liability
inbabies:
Thelargesizeoftheseneedlesmakesthemclumsyinstruments,better
suited to inadvertently damaging the liver or spleen than
allowing
accuratesutureplacement. Inanycase,endoscopic
gadgetsarerarely
designedforverysmallpatients,andtryingtoforcethesedevices(e.g.
tryingtosqueezeevenasmallstaplerintoaninfantschest)isnoroute
tobetteroutcomes.Thewrongtoolsweakenthesurgeonandendanger
thepatient.
On the other hand, the expert surgeon has attended to
developing robust and general ski lls with basic endoscopic
instruments. He exhibits suture technique as precise as open
technique. Heunderstandsandcantroubleshoottheequipment. He
can safely and rapidlyperform averywidenumberofproceduresat
leastaswellas(andinmanycases betterthan)usingopentechnique.Use
of gadgets fosters shortcuts and poor methods, compromising
outcomes and lending MIS an air of risk. In cases of trouble,
the
surgeon,andhispatient,are betterservedby reliable technique
than
bytechnology.
Oneproblemwithmedicalandsurgicaldevicesistheproblem
ofimplieduse,thecuesonthedeviceitselfthatimplyhowthethinkis
intendedtobeused. These cues aresometimes called
affordances.
Page 7 of 22
-
7/30/2019 MIS Behavior 2012 v 7
8/22
Rarelyaresurgeonsgiveninstructionon theelements ofhowdevices
are designed, and user manuals are an early casualty of a
busy
operatingroom,evenifthesurgeonwasinterested.Instead,surgeons
duringtheirtrainingtypicallyreceivesomelessons asmemesor
lore,
oftenpassedfromaseniorresident,alessontheywillpasstotheirown
trainees. Often, those lessons are little more than
someonesworkaroundwhentryingtousethedeviceforacertainpurpose(e.g.a
malecot drain repurposed as a gastrostomy tube, now
virtually
standardofcareinpediatricsurgery).Othertimes,theuseissimply
amisunderstandingofa designthat implies,byitsshapeor
structure,
thatitshouldbeusedaparticularway(e.g.thesutureholesonmany
gastrostomytubeswhicharein fact merelyventilationholes,
andnot
designedorintendedforsecuringatube).
Sometimes,thesehintsforuseareaccurate,butoftennot,and
the novice may have no basis onwhich to tell the difference.
or
example, novice operators very commonly pick up instruments
and
holdthem inthumb and index Finger, a gripthat puts the userat
a
disadvantageintermsoftorqueandprecision. Thesurgeonmustpay
attention to how devices were actually engineered to be used,
but
hemustgofurther:hemustunderstandwhenthedesigndoesnotquite
servehis need,and bewareof how theseshortcomings canincrease
risks.orexample,it is
commonforsurgicalstaplerstorequireavery
stronggripinorderto Fire. Asurgeonwithsmallerhandsmaybeata
mechanical disadvantage and struggle with the Firing, which
can
translateto jarringorshakingatthebusiness endofthestapler.
One
way around this is to turn the handle upside downwhich acts
to
lengthen themoment arm, thereby decreasing the force required
to
exertthesametorqueontheFiringmechanism.
Expert minimally invasive surgery is technology wielded
accordingtoproFicienttechnique.
#2 Face the Organ
Positioning the patient properly begins withpositioning
thesurgeon.oranyendoscopicprocedure,thesurgeonmuststandfacing
the organ of interest. Too often, surgeons are seen
operating
backwards,strickenbyparadoxicalactionoftheirtoolsonthescreen.
Precisionmotionis impossible when the surgeon cannot even
intuitright andleft,upanddown. Ofcourse,itsnot funnyif
thesurgeonis
you.
Meanwhile, operatinginpoor position is very tiring to the
surgeon. As the surgeon fatigues, the muscles responsible for
Fine
movements fail First. In this way, fatigue hugely
compromises
precision.orexample,asurgeonwhoattemptstooperateonaspleen
from the leftsideofthetablenot onlyhasa poorangleofattack
and
Page 8 of 22
The wrong hold. It canseem like the right
way to grasp the instrument, but this hold
destroys control at the tip and leaves the
user unable to spin the shaft.
Stand up. No one can maintain precise
technique if hunched over, twisted, or
awkwardly positioned. The surgeon is the
first surgical instrument, and must be
used properly like all the others.
-
7/30/2019 MIS Behavior 2012 v 7
9/22
someparadoxicalmotiontocontendwith,butawkwardbodyposition
that quickly leads to fatigue. If you are shaking and sore after
an
endoscopicprocedure,yourset-upwasprobablysuboptimal.
Perfectpositionallowsthesurgeontooperatewithlittleeffort.
The most important principleforgoodpositionis for the surgeon
to
facetheorgan heisoperatingon.
Inotherwords,thesurgeonshouldplacethemonitor(ideallymountedontheceiling,butthepracticecan
bemaintainedwithtowers)inalinewithhimself, thecamera,andthe
organofinterest. Agoodmnemonic that somesurgeonsteachisS-C-
O-P, or surgeoncameraorganpicture(6). or example, with
appendectomy,thesurgeonstandstothepatientsleft,facingtheright
lowerquadrantwiththescreenonthepatientsright.Ifthesurgeonis
operatingontheGE junction, heshould standat the foot of the
bed
(withbabies frog-leggedat the endofthebed, larger patients
inlow
lithotomy position) facing the epigastrium, with the monitor
hung
directlyoverthepatients chest.
ThisistheFirstprinciplethatallows
thesurgeontouseallavailabledegreesoffreedom.
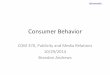
Implicitinthisruleisknowingwhattheorganis.orexample,
whenperformingathoracoscopiclobectomy,theorganisnotthelung
or the lobe, but themajor Fissure, the placewheremost of the
Fine
dissectionoccurs(seeigure1,above),andthesurgeonshouldstandin
linewithit. Similarly, inlaparoscopic
pullthroughforHirschprungs,
theareawheretheFinedissectionoccursistherectum,andthesurgeon
shouldstandatthebabyshead.
Onementalbarrier tofacethe organ istheimplicit rulethata
surgeonandhisassistantmustoperateoppositeeachother. Innearly
everyopenproceduresurgeonandassistant faceeachother,andany
other arrangement seems wrong, even taboo. But what brings
advantageinopencases may bringdisadvantagein endoscopic
cases.
Itisabsurdforeithersurgeonorassistantto
strugglewithparadoxical
motion,but this
foolishpracticeistoleratedbecauseofthebeliefthat
anoperatormust standon each sideof thepatient regardlessof
the
surgical objective. ace the organ goes for surgeonand
assistant,
evenifbothstandonthesamesideofapatient(astheyoftenshould).
Only when facing the organ can the other aspect of good
positioningbeemployed,thePianistPosition.
Virtuosopianistshold
theirarms loose at theshoulder,armsbent
attheelbow,wristsloose
and Fingersonthekeys. Virtuosoendoscopic surgeons
operatewiththebedatalevelthatallowsthemthesameposition:headuprightand
level with the screen, shoulders relaxed, elbows bent at 90
120degrees,wristsloose,andactionontheinstrumentscontrolledwith
Fingertips. The novicecan beseenwithback bent, arms
abducted,
elbowsaskew,wristsstiff,instrumentsheldinadeathgrip.
The comfortable surgeon attends to surgical detail; the
uncomfortablesurgeonthinksabouthissoreback.
Page 9 of 22
In lobectomy, the organ is not the lobe
being removed, but the fissure. The
surgeon gets best advantage by aligning
tools and his body along its axis.
-
7/30/2019 MIS Behavior 2012 v 7
10/22
#3 Triangulate the Ports
Positioningtheportswellalsocontributestothesurgeonscomfortandprecision.Cameraandworkinghandsshouldforma
triangle,likethebroadendofakitewheretheorganofinterestisthepointedtail(igure2).Ingeneral,thecameraisinthecenter(butnot
always,seebelow).
Eveninsmallpatientsthekiteallowswideenoughseparation
between ports that the operator will not cross the streams
and
impedehisownwork. Equalspacingallows bothhands tocontribute
similarly(seePrinciple#6).Noticethattriangulationallowsmaximum
motionthrough all available degrees of freedom (DO). Degrees
of
freedom in mechanics are the parameters required to specify
an
objectspositioninspace.InMIS,thereare6:
(1) Sidetoside
(2) Upanddown
(3) Inandoutthroughthetrocar
(4) Rotationoftheinstrument
(5) Opening/Closing the instrument (e.g. a marylands working
tip)
(6) Translationofthebodywall(whatCO2insufFlationgives)
Evenif fourormoreportsare needed,thepositionofall theports
is
determinedbytheworkingtriangle,andthe prinicipleofmaximizing
allavailabledegreesoffreedom.
Noticethat poor triangulationdestroys aDO. or example,trocars
positioned too close together, or too far from the organwill
maketheinstrumentsworknearlyinparallel,constrainingthe#1.Itis
nearlyimpossibletotiesuturesinthiscircumstance.Similarly,putting
trocars too lateral (where the bodywall begins to curveback
down
towardthebed),orbumpingthepatients legsupbothcanimpede#2,
makinganterior anatomyimpossible toreach,or awkwardto
handle.
Morefamiliarly,whenCO2insufFlationisinadequatefromleaksorpoor
settings or a bucking patient, #6 is constrained, destroying
the
surgeonsviewandmakingprogress impossible. But anyreductionof
DO(suchasforgettingtheavailableinstrumentrotation,#4)seriously
degradesthesurgeonsabilitytomovefreelyandwithprecision.Goodmechanicalresultscannotbeattainedthisway.
Centering the cameraalsokeeps paradoxical motion to the
minimum.Paradoxicalmotionisattemptingtooperatewhentheimage
isreversed, fromthesurgeonsperspective. It
istheoppositeofface
the organ. or example if the camera was looking toward the
appendix,butthesurgeonwasstandingonthepatientsright,hewould
Page 10 of 22
In general, trocars should be placed so
that right and left hand instruments
approach the organ of interest separated
by approximately 90 degrees. Meanwhile,
the camera port should (usually) be offset
from the two main working ports such that
the three ports form a triangle, not a line.
These four pointsthe three main ports
and the organform a kite shape, a
configuration that generally allows the
best view, comfort, and maneuverability.
-
7/30/2019 MIS Behavior 2012 v 7
11/22
be working paradoxically. All moves would feel backwards,
and
unintuitive.Noonecanoperatewithprecisionthisway.
But rigidly keeping the camera in a center port is
disadvantageous. Occasionally, operations are better performed
(at
least in part) by placing the camera to one side, as an
outrigger
camera. orexample,inappendectomy,
itmaybeeasiertoplacethecameraattheumbilicus
andworkthroughsuprapubicand left-lower-
quadrantports.Inthoracoscopicdiaphragmaticherniarepairwiththe
patient in decubitus position, it may be advantageous to have
the
camera(andthecameraoperator)intheportnearestthepatientsback
andtheoperatorusingtheports
inthemidandanterioraxillarylines.
In other cases, the peculiarities of the anatomy (e.g. some
thoracic
masses) may require the camera to occupy any of the ports as
the
procedureprogresses.Observethatwhenusingtheoutriggercamera
technique, advantagecan be gainedby using anangledscopewhich
allows the viewing angle to approach (if not perfectly achieve)
a
centeredview.Triangulatingtheportsallowsthefreedomtomovethe
camera whenever needed, without creating distortions in
working
mechanicaladvantage.
#4 Do The Same Operation
Somehavetheimpressionthatendoscopicmethodsarenotasreliable,
safe,oreffectiveas opentechnique,thatsomehowtheresults
arelessrobustandthepatientswellbeinglesswellinhand.Certainly
the novice feels unnaturally constrained by the tools and
the
visualization, andoftenisconfusedby theorientation.
Struggleswiththeanatomyandwithbasicskillssuchasendoscopicsuturingcanlead
somesurgeons into doingan operationthatis
prettyclose,nearlyas
good, a fair approximation, etc. Stitches are placed,
workaround
methodswithclipsorothergadgetsareemployed,anddissectionsare
fudgedin ways that thesamesurgeonwouldnever accept were the
casebeingdoneinstandardopenfashion.Whocouldbesurprisedthen
when outcomes are not as good, especially early in a
surgeons
experience?
Dothesameoperationmeans:Performanoperationwithat
leastasgoodamechanicalresult aswouldbeachievedwithclassic
opentechnique. This does notmeanthat
everystepusedinanopenprocedureshouldbereplicatedendoscopically.
Instead,oneis aiming
atthesameFinalmechanicalproduct:
Use thesame suture. If youare repairingduodenalatresia,
and youwould perform the duodenoduodenostomy with a
series of Fine interruptedmonoFilament sutures ina double-
d iamond ana s tomos is , d o t he s ame ana s tomosi s
Page 11 of 22
Surgeryistheapplicationofmechanicalsolutionstomedicalproblems.
-
7/30/2019 MIS Behavior 2012 v 7
12/22
laparoscopically. Alternatively, if you would never use a
braided2-0ona skineedle for this anastomosis, dontuse it
laparoscopicallysimplybecausethatistheonlysutureyoucan
usewiththescope.
Dothesamedissection. orexample, ifyoucarefullyisolate
andvisualizethesplenicvesselsandclearlyvisualizethetailofthe
pancreas during splenectomy, you should do the same
laparoscopically rather than Firing a stapler semi-blindly
acrossthesplenichilum.
Completeatleastthesamemechanicalrepair. Ifyoustick-
tie the appendiceal base during open appendectomy, you
should do this (or amechanical equivalent, like staples) ina
laparoscopicappendectomy.Ifyouwouldplaceastitchinthat
serosal tear inanopencase,put a suturein laparoscopically
too. Ifyouwouldmobilizethecolonmoretodecreasetension
duringanopenpull-through,youshouldmobilizeitprecisely
the same amount when per forming the procedure
laparoscopically.
The ideais toperformatleastasgoodanoperation.Inskilled
handsofcourse,endoscopicproceduresmayproducesuperiorresults:
alaparoscopicNissendonewellwillhaveaffordedabetterviewof the
vagusnervesandabetter,saferwrap;alaparoscopicpyloromyotomyis
faster; a laparoscopicduodenoduodenostomyallows
theanastomosis
dobedonelargely insitu,decreasingtheamountofdissectionneeded
and possibly leading to faster resolution of gastric i leus;
a
thoracoscopic esophageal atresia repairallows less dissection of
the
distalsegmentanddissectionunderveryhighmagniFicationapparently
leading to measurably lower stricture and leak rate(7).
Better
visualizationcancertainlyallowtheendoscopicexperttodoasuperior
procedure. But theessentialprinciple is a cognitive commitment
to
doingthesameexcellentoperationonewoulddousingopentechnique.
#5 Operate with Two Hands
Humansalmostalwaysdotaskswithadominanthand. Whenlearninganew
task, thenaturaltendencyis tofocuson
thedominanthand,unconsciouslyneglectingthenon-dominant hand. If
thetask is
very new andvery difFicult, this unilateral neglect almost seems
to
approachthat ofstrokepatients. Eventhedexterityof
thedominant
handsuffers(8). Whendoctors attemptlaparoscopy fortheFirst
time,
nearly all exhibit unilateral neglect (and it is not conFined
to
laparoscopicsurgery;everyonetendstoignorethenon-dominanthand
whenFirst learningopensuturing). Allattentionseemsto
befocused
Page 12 of 22
-
7/30/2019 MIS Behavior 2012 v 7
13/22
on the unusual tiller-action-at-a-distance that is
laparoscopic
manipulation,
channelingandtruncatingattentionintonarrowtunnel
vision. Novice operators struggle to manipulate aneedleor
cautery
one-handedly,whentheycouldeasilyhelpthemselveswiththeirnon-
dominanthand.Instead,theinstrumentheld inthenon-dominanthand
driftsoutofview,islost,beginsgraspingwithawhite-knuckleddeathgrip,etc.Nearbyorgansandstructuresareatgreat,butunrecognized,
riskfrominstrumentclutchedintheneglectedhand.
Good teachers will stress non-dominant hand awareness,
boringtheirstudentswiththerefrainWhatisyourotherhanddoing?
Onlybyrepeatedlyredirectingattentiontobothhandscanonelearnto
usebothhandseffectively,andautomatically.
Evenseasonedsurgeon
needtoexplicitlyremindthemselves.
Non-dominanthandawarenessisimportantnotonlyforspeed
andefFiciency,butbecausehumansaremorecoordinatedinFinemotor
taskswhenbothhandsappearintheirvisualField,evenifonehandis
not participating in the action(9). You can verify this
yourself; try
cuttingsuturewithonehandonyourchestversuswithbothhands in
theField. Withbothhands inview,thecuttinghandwillbesmoother
andmoreprecise.ThesameeffectholdsinMIS.
Endoscopic methods always impose constraints on
manipulation, since thenumber ofhands inthe Fieldare always
one
fewer than the number of trocars (unless one has an
experimental
camera/manipulatorcombinationinstrument).So,onemustmaximize
what hecandowithwhathehas. Neglectingthenon-dominanthand
halvesanalready-restricteddexterity(byremovingdegreesoffreedom
grantedbythathand).Somemayboastthattheycanoperatewithone
hand tied behind their back, but this is no road to precision
and
accuracyfor the rest of us. Precisionendoscopyis a
two-handed
proposition.
Thisdiscussionbringsuponecommonbut verypoorpractice.
In general surgery, training cases (l ike cholecystectomy,
appendectomy,or evensplenectomy)arecommonlyset upin sucha
waythat theattendingmanipulatesorganswithone instrument, and
has the trainee try to operate with the dominant while the
non-
dominanthandmoves thecamera. Therearenaturalreasonsforthis:
Attending surgeonstire of (andare notoriouslyunskilledat)
running
thecamera(see#8,below),theyarenervousaboutthedexterityofthetrainee,
feel the need to have a hand in the action as ameans of
exertingcontrol,andtheyworry that
thetraineeisnotskillfulenough
tousebothhands.
However,this practicealways puts the trainee(and thus the
patient) at a disadvantage since he is forced to divide
attention
between two very different tasks, camerawork and Fine
dissection.
Meanwhile,removing thenon-dominant handfromviewdegradesthe
Page 13 of 22
-
7/30/2019 MIS Behavior 2012 v 7
14/22
coordination of theoperatinghand as described above. inally,
no
degree of simpatico between teacher and student will allow
good
coordination between two different operators single hands.
This
attempted coordination almost always resembles fencing more
than
operating. Instead, the teacher is always better having the
learner
operatewithtwohands fromtheirFirst case, just aswe
teachinopencases.
Iftheteacherfeelsheneedsmorecontrol,thesolutionistoadd
aport(see#7below)andaninstrument,nottotakeoneawayfromthe
learningoperator.
But there is moreto theskillful use of two-handed surgery
thanmerely remembering to use two hands. The skillful
operator
moves his instruments the way a geisha walks, with small,
even
mincing, but highly-controlled steps. The tips of the
instruments
remaininviewofthecamera(reducingtheneedtorelyon#9,below),
and eachmove is slow,smooth,controlled. urthermore, the
skilled
endoscopicsurgeonis ambidextrous. Therewillbetimeswhenit is
bettertohavetheenergysourceenterfroma left-handedport, anda
retractor from the right. One should be able to readily
switch
instruments fromhand tohand, always keeping thehighest
possible
mechanicaladvantage.
Those Fine, measured movements also apply to the use of
energysources likemonopolarelectrosurgery(thebovie). Energy
sources in babies not only require lower power settings, but
the
mannerofapplyingtheseinstrumentsisdifferent.
Inparticular,when
using the hook cautery, energy should never be engaged unless
in
contact with the tissue to be divided or fulgurated (Swinging
the
activatedhookaroundlikealightsaberriskscauteryinjury).
Also,it
is bad practice to work in a hole; keeping a wide working
front
maximizes visualizationandminimizescollateraldamage.
Allenergy
sourcescertainlyperformbetteriftheoperatoravoidsgettinggreedy,
e.g.takinglargebites oftissuetodivide,apracticethat
leadstoexcess
char, incompletehemostasis,andbroadcollateral burns.
inally,and
mostimportantly,precisiontechniquebeneFitsfromalight footon
the
pedal.MostdivisionandcoagulationcanbeachievedwithFinetapsof
thepedal,whereas long continuous burns produce char anda
wide
penumbraofthermaldamage.
Ofcourse,nocuttingcanoccurwithout propertensiononthe
tissue. Perhapsthemostimportant
roleofthenon-dominanthandiscreationoftensiononwhateverareaistobecut.Withoutgoodtension
applied to it,the tissuewillmerelycontract andcharwhenenergy
is
applied. It willnot separate,
butthermalspreadwilltakeoverasthe
operator vainlyappliesmoreelectricity. Insmallspaces,
unintended
tissuedamagebecomesinevitable.Novicesoftencannotseethatwhile
theymaybe creatingtensioninthetissue,thefocus ofthetensionis
away from where it is that they want to be cutting. But
careful
Page 14 of 22
Puttensionwhereyouarecutting;
cutwherethetensionis.
-
7/30/2019 MIS Behavior 2012 v 7
15/22
attentionto tensionlinescombinedwithanunconstraineduseof the
non-dominant hand will allow the operator to recognize where
the
tissue tension lies within the tissueplain. Moreover, the
non-
dominant handmust continue to adjust tobring newtension to
the
working plane as attachments are cut and tension is released.
In
general, theprincipleis: Put tensionwhereyouarecutting, and
cutwhere the tension is. This sounds hilariously obvious, but
is
notoriouslydifFiculttoapplyinpracticewithoutanexpliciteffort.
SuchdaintyuseofenergyusuallyseemsoddatFirst,butthese
habits lower energy settings, no lightsabers, no holes, no
greediness,no Bovie pedalleadfoot, andattentionto tension
translateinto Fine, efFicient dissectionwithless smoke, less
char, less
bleeding,andlessriskofunintentionaldamage.
The surgeon who always operates with two hands has the
fullestpossiblecontroloverthesurgicalField.
#6 Gravity is the Third Hand
Gravity can be a tremendous hindrance if ignored. On
theotherhand,usinggravitytoones advantagecandramaticallyimprove
visibility, decrease the need for manipulating the organs, and
cut
anesthetictime. orexample,whenoperatinginthepelvis, theworst
possible position would be reverse-Trendelenberg; all of the
small
bowel would slide to the pelvis, hopelessly obscuring all
other
structures.Ontheotherhand,whenoperatingintheupperquadrants,
especially, for example, during a fundoplasty or a gastric
bypass,
reverse-Trendelenberg is crucial topullthe colonand fatty
omentumoutoftheway. Even routine cases such as appendectomy
beneFit
from simple positioning changes: rolling thepatient to the left,
and
placinghiminslightTrendelenbergelevates thececum
andallowsthe
ileumtofalldownandbackfromtheFieldofview.Inallofthesecases,
gravity is like a third hand holding a retractor for the
surgeon,
keepingother organsout ofthe Fieldofview. Thisisalwaysa
better
methodthanconstantlytryingtosweeptheboweloromentumawayso
onecanseetheoperativeField.
But tousegravity effectively, one must planthepositioning
carefully.Inparticular,onehastokeepinmindtwostrategies:
Set up thetrocarandpatientpositionssothat gravitycanbe used.
or
example,onewouldnotwanttoapproachtheposteriorleftlower lobe
witha patient supinesinceno amountofturningthe
tablewillallow
thelungto fallawayfrom the chestwall.
Ontheotherhand,anterior
mediastinalmassesarebestapproachedwiththepatientsupinesince
inthis position the lung is already pulleddown and away from
the
Page 15 of 22
-
7/30/2019 MIS Behavior 2012 v 7
16/22
operativetargetbygravity. Obviously,partof
thisset-updependson
Principle#2:acetheorgan.
Secureand pad thepatientproperly to restrain gravity.
orexample,
oneofthemostcommonpositionswhenoperatingonbabiesistoplace
themat the foot of the table,with legs frog-legged,
andthemonitorhanging above the patients head or chest (lower
picture). This
position is excellent for Nissen, Ladds, duodenal atresia
repair,
abdominal approach to CDH/eventration, Morgagni hernia
repair,
choledochal cyst excision, etc. But the samegravity that pulls
the
omentumdowncanpullthewholepatientdownaswell. Indeed,ina
baby, even a short slide downthe table, say 1-2 cm, is enough
to
dislodge the endotracheal tube, creatingunintended extubation.
To
avoidthiskindofproblem,carefulpaddingandtapingareessential.In
addition,theuseofasmallbumpundertheabdomenactsasakindof
skid-stoptoretardsliding.
The pictures show two well-positioned patients, top, for
laparoscopic right nephrectomy, and, bottom, for
laparoscopic
fundoplasty (or duodenal atresia, or choledochal cyst, or
others).
Observethatthereisnostretchontheextremities that
couldproduce
nerve injuries, and that good padding is placed everywhere.
No
undercrossinglinesor tubes snakebeneaththebodyor limbs(these
couldquicklycreatepressureinjuriesinchildren).Also,notethattape
with adequate tensile strength is used; it is a common blunder
in
pediatricsurgerytorelyonclearplasticorpapertapeinanattemptto
begentle. But there isnothinggentleabout
fallingofftheoperating
table.
#7 Add a Port
It is anerrortosacriFiceprecision,mechanicaladvantage,andspeed
in the nameof making fewer port incisions. Occasionally, a
perverse sort of macho ethic sneaks
intoa surgeonsmentalhabits,likethe
s u r ge o n w h o r a c es t h r ou g h
laparoscopiccholecystectomies aiming
for personal best skin-to-skin times.Here the error is to
replace effect as
cause: It is from precision and
efFiciency that a speedy operation
results. ocusing on speed will not
improve precision, but precision
always bringsspeed. Astitchintime
reallydoessavenine.Similarly,adding
Page 16 of 22
Using gravity well also means protecting
from gravity. These patients are properly
padded and secured.
-
7/30/2019 MIS Behavior 2012 v 7
17/22
a port in a casewhere exposure or counter-tension is difFicult
can
dramatically improve theoverall precisionof thecase,
andallowits
completionspeedily.Regardingtheadditionofatrocarassomesortof
failing,as a loss insomekindofNameThat Tunetypeof numerical
contest(Icantakeout thatspleenwithonlythreetrocarsWellIcan
doitwithonlytwo!)doesnotservethepatient. One of the worries
about adding trocars is that the addition
couldaddsigniFicantly tothemorbidity oftheoperation.
However,a
fourthorFifth3or5mmtrocarwill not contribute substantially to
a
patientspainorscarring.Experienceshowsthattheextratrocarsite
adds trivially to the patients pain. But if the operative time
is
shortenedfrom3hours ofstrugglewithgrasping andregrasping the
bowel toa smooth1 hour casewiththeleastamountofmanipulation
necessary,thepatientisplainlywellserved.
Considerationoftrocarincisionlengthsbringsustooneofthe
primefallacies inendoscopic surgery. It isinevitable that
onehears
the argument that surgical technique is not improved if an
open
operationcanbedonethroughalinearincisionwhoselengthissimilar
to thesum lengthofall trocarsiteincisions.
orexample,itisargued
thata2.5cmincisionisnodifferentthanFive5mm incisions,withthe
implication that the endoscopic method is somehow a fancy
waste.
However, it is not true that the lengths of trocar incisions sum
to
similaropenincisionlengthsintermsofpain,scar,disability,etc.
or
example,itisintuitivelyobviousthat5incisionsdistributedaroundthe
abdomen have a very lowor zero risk of dehiscence, but a
2.5-3cm
linear incision is vulnerable to this complication. urthermore,
the
mathematics of woundtensionshow that thetotal tension across
an
incision varies as a function of the square of its length, so
the total
tensionof a longincisionis greaterthan
thesummedtensionsacross
several very smallincisions ofthe sameaggregate length(10).
Pain
and scarring plainly depend on tension(11). The smaller
tensions
across trocar incisions are the origin of the minimally
invasive
moniker,butthereisno reasonfor thesurgeonto endurea minimal
accessdisadvantage.
Dontstruggle.Addaport.
#8 Tai Chi Camera Ironically, camerawork, one of the tougher
tasks, is oftendelegated to the least experienced person around the
table. The
cameraoperatormust keepanupright imagecenteredon theaction
withtherightzoom andleastmovementatalltimes.Often,theintern
ormedicalstudentisaskedtorunthecameraandhasno ideahowthe
operation is done, what needs tobe seen, or evenexactlywhathe
is
Page 17 of 22
A TROCAR OF DIAMETER D...
...REQUIRES AN INCISION
OF LENGTH
L=r2D
OR ONE HALF THE
CIRCUMFERENCE!
L
D
Good trocar placement requires making
precisely sized trocar incision. The oute
diameter of a 5mm trocar is usually just ove
7 mm, but the incision needs to be a little
larger. This formula suggests an incision o
11mm for a 7mm OD trocar, but because th
skin has a small amount of elasticity, the rea
value is the formula, minus a little bit, o
closer to 9mm. If it is too small, the troca
will crush the skin edges, and the surgeon
may damage underlying structures while h
struggles to insert it. Conversely, a trocar i
too large an incision will slide in and out wit
the instruments, easily falling out, etc.
-
7/30/2019 MIS Behavior 2012 v 7
18/22
seeing. Whensternorders are barked(Look left! NO! Left! And
DOWN!)theresultisadizzyingjumpypicturelikeabad1980smusic
video.
Buteveryonemustlearncameraworksometime.ortunately,
afewsimpleideascanvastlyhelpthelearnermentallypicturewhatit
is heneeds to do. irst, takeone minuteto show(or to learn)
thecameracontrols,lensconnection,andlighthookup.Explaintheuseof
theextradegreeof freedom one gains withanangled telescope,
and
howtouseittoadvantage(forexample,twistthescopesotheobjective
pointsupwardwhenplacingtrocars,etc.). Demystify it,so that
the
cameraoperatorwillnotbedistractedbyapprehension.
Next,thelearnermustunderstandthattheimagemustalways
becenteredontheaction,andkeptupright. Novices tendtoallowthe
camerato drift away from center, andoff kilter. Ifyou
Findyourself
tryingtolookaroundthecornerofthescreen,oraretiltingyourhead,
check your cameraman. Most learners need to be reminded of
this
multiple times. Even seasoned surgeons can be pulled into
this
tendency to look aroundcorners of a two-dimensional image, but
a
goodcameraoperatorwillnottempttheoperator.
Notonlyshouldthecamerabecenteredontheaction,butthe
picturemust bekept upright. It is amatterof simple
demonstration
that task precisionradicallydegrades iftheimagetilts relativeto
the
surgeonssenseofupanddown.Itispossible(althoughnotoptimal)to
worksemi-paradoxically,that iswithonesbodyorienteduptonearly
90degreesoffthelinebetweencameraandorganofinterest (that is,
partiallyviolatingtheruleto facetheorganbeingoperateon).
This
positionallows anassistanttoworkwellfromthepatients sidewhen
theoperator is at thefoot,forexample. It also make
theoutrigger
cameraaviablestrategy. But
evenaslightchangeintiltdestroysthe
surgeonsabilitytomovebecauseofhumanrelianceonanabsolutez-
axis. orbothsurgeonandassistant,theupanddownmustremaina
consistentreferenceframeinwhichtowork.
Novices also tendto jerk the camera around,makingsmall,
briskmovementswithmultipleovercorrections.Humansareknownto
performbetteratnewskillsiftheycanmentallylinkthenewactionto
animaginedactionorimagethattheyknow.Martialartsteachershave
knownthisforcenturies: Bendlikethereed inthewindorStand
likeanironhorse. Theimagesdo not needto beanactionthat thenovice
has alreadydone(althoughthatis helpful), but evocativeina
waythat pre-Fires the cerebellum ina particularway. Inthis
spirit,
teachthenewcameraoperatortomovethecameraasifsheweredoing
TaiChi.
Everyonecanpicturetheslow,graceful,highlycontrolledand
FluidmotionofsomeoldmasterpracticingTaiChi.Holdingthisimage
inmindpredisposesthenovicetorelax,breathe,andmovethecamera
slowly, precisely. The imagewillbe better thanin response to
the
Page 18 of 22
-
7/30/2019 MIS Behavior 2012 v 7
19/22
order Move slower! The novicelearns faster when primed than
whenbullied.
TheTaiChicameraisalwayscentered,upright,anddeliberate.
#9 Use Bifocals for Spatial and Situational Awareness.
It
isveryeasytoloseoneselfduringanendoscopicprocedure.Theperspectiveisdifferent,theanatomydisorienting,andtheangleof
approach of ones instruments to the surgical objective may
be
awkward. Instrumentsleavethevisualframewheneveronedoesnot
practice Geisha walkmovements, when the non-dominant hand is
neglected, or whenever an instrument must be changed or
cleaned.
Onehandcaneasily get lost,
leavingtheoperatorFlailingaroundin
anattemptto bringtheinstrumentbackintoviewofthecamera. Ina
baby,thesegross,blindmovescandamagebowel,liveror lung. Even
withoutdamage,thesestruggleswastetime.
ortunately,onecanseemorethanjustwhatisonthescreen.
Onecanseethepatientaswell.Alostinstrumentcaneasilybefound
if one looks at the patient to seewhere the camera is
pointingand
simplyaims theinstrumentfor that region. Inessence,one
triesto
focus alternately between the virtual image on the screen, and
the
realimageof theactualField.
Callingthismethodbifocalsgivesthe
techniqueaname,makingthemethodeasiertoremember.
Bifocals also improve situational awareness. It means that
not onlymust thesurgeon be able to focus onthe imagesinside
theoperatingcavity,butmustbeattunedtowhatishappeningoutsidethe
operatingFieldaswell. Istheanesthesiologistactingworried?
Isthe
pulseoxdrifting? Istheend-tidalCO2 oddly high?
Didsomeonejust
callfor blood? Haveyouprimedthescrub nurseortechtohavethe
right
stitchorcriticalendomechanicaldevicereadyforthenextmove,
andthemoveafter that? Awarenessofthesethingshelpsyousmooth
theprocedureandprotectthepatient.
Humanscannotreallymultitask. Truemultitaskingisamyth;
humans that attempt to do two jobs at once end updoing two
jobs
poorly.Instead,apparentmultitaskingdependsonatleasttwoskills.
irst,theappearanceofmultitaskingisreallythequickFlitofattentionamongdifferentobjects,justthewaysomeonewearingbifocalsquickly
adjusts his focal lengthby peering through different portions of
the
glasses. orexample, the aware surgeonmay quickly sample the
sounds around him periodically--thepulseox, theheart monitor,
the
conversations.ThisFlittingsampletakesmilliseconds,butyieldslots
ofinformation.
Page 19 of 22
-
7/30/2019 MIS Behavior 2012 v 7
20/22
The second skill is the ability to ignore details. This skill
is
familiar to anyone who has learned the automatic,
unconscious
movements of driving a car. At First, every single move
requires
deliberatethought--clutch,signal,turn,gas,clutch,brake,gas....Thenew
drivermustpaysomuchattentiontothemechanics ofthecarthat he
will not see that truck, that pedestrian, or that pothole. But
withpractice, thedriver,
andthesurgeon,movesautomatically,freeingthe
mindforotherfocus. Inthisway,practiceisreallyawayofremoving
distractions.Somewhatparadoxically,beingmoremindfulistheartof
attendingto less. Expertiseisnottheabilityto
attendtomorethings,
but the ability to be more selective in attention. The
expert
automatically pays attention to the important stuff andneglects
the
unimportant.Beinganexpertmeansbeingabletotellthedifference.
#10 Build Versatility by Analogy
Innovativenewproceduresarecreatedthesamewaythatthelearneraddstohisrepertoire.
Theskills andlessons fromothercases
arecarriedover to newapplications. orexample,whenconsidering
the repair of duodenal atresia, one can reuse the setup for
pyloromyotomy. Later, familiarity with the right upper
quadrant
allows better exposure and understanding of the twisted
duodenum
seen in correction of malrotation. Similarly, when confronting
the
biopsy of a pelvic mass, one can re-use the set-up for
laparoscopicrectalpullthrough.
Or,ifoneneedstorepairaMorgagniorBochdalek
herniafrom theabdomen,
familiaritywiththesetupandmanipulation
oftheupperabdomenanddiaphragmasinaNissencanbebrought to
bear. Eachsurgeonbecomesmoreversatileby
reusingdiscreteskills
fromotheroperationstobuildanewone(evenifmerelynewtohim).
Anotherway to saythis isIfyoucanmakea pizza, you canmakea
calzone.
Versatility allows the surgeon to operate better in several
ways. Theability to adapt analogousmethodstonew
circumstances
allows thesurgeontogetoutoftrouble
(possiblyavoidingconversion
to opentechnique). Italsoallows
thesurgeontoapplyoldtechniquestonewproblems.
inally,movementanalogyhelpsreinforcetheskills
heusesforwhateverprocedureheisdoingrightthen:movesarewell-
practiced and less dangerous when used in many contexts. or
example, easy facility with an endo-loop type device for
common
procedures like appendectomy extends that facility to
unfamiliar
contextswithrarecaseslikecholedochalcyst.
Page 20 of 22
-
7/30/2019 MIS Behavior 2012 v 7
21/22
Explicitly noting the reused movement objects (the small
movesfromwhichmore complexactionsarebuilt) indifferent cases
allows thesurgeon to move up learning curves much more
quickly.
Everyendoscopic case reinforces theothers,eventhe easy
onesif
good principles are always followed. or example, safe trocar
placement,non-dominant handattention, cameramovement,and
useofgravityforretractionareusedineverylaparoscopicorthoracoscopic
case, andthe lessons
andskillsbuilthereareactuallymorecriticalin
hardercases. Inthis way,as casesarebuiltfrom skillblocks
(like
classes in object-oriented computer programming), the
learner
discovers thattherearenohard cases,only caseswith a greater
numberofeasymoves.
Conclusion
The principles describedherecanbeappliedinany pediatric
MIS case. They are intended to help maximize the surgeons
mechanicaladvantageanywhereminimallyinvasivemethodsareused.
Each of these is intendedto dealwith thescaling problemsof
small
patients,tohelpthesurgeonwieldratherthansimplyusethedevices,
topromoteprecisionbymaximizingavailabledegreesoffreedom,orto
workwith(orovercome)inherenthumanstrengths(andweaknesses):
1. Perfect tools are perfectly maintained...and understood
2. Face the organ
3. Triangulate the ports
4. Do the same operation
5. Operate with two hands
6. Gravity is the third hand
7. Add a port
8. Tai Chi Camera
9. Bifocals for Spatial and Situational Awareness
10. Analogy builds versatility
Maximizingmechanicaladvantageaidsprecision,
speed,andsafetyin
MIS, a technological extension of surgery that, perhaps
ironically,
presents severalmechanical disadvantages (andsomeadvantages,
of
course)to thesurgeon. Strugglingwiththesedisadvantages
putsthe
patient at unnecessary risk, risk that is magniFied in babies
and
children. ortunately,practicedapplicationof
theheuristicsherecan
help the surgeon create the superset of skills needed to
obviate
commonhazards.
But principles can go too far. Regarding the principles
presented here as rigid or exhaustive misses the principle
behind
principles:Principlesaretobeused,notblindlyobeyed.TAB
Page 21 of 22
The learning curve: proficiency with any sk
requires practice. But it is not true that each ne
operation starts the surgeon at the bottom of th
curve. Instead, specific abilities--good set-u
two handed action, small moves, comfortab
facility with electrosurgical devices, etc--are a
objects that port easily to new procedures. Bthe surgeon must
see the analogies to apply o
methods to new circumstances!
-
7/30/2019 MIS Behavior 2012 v 7
22/22
SELECTED CITATIONS
1. Morgenstern, L. Warning! Dangerous curve ahead: the
learning
curve. Surgical innovation12: 101-103, 2005.
2. Rangel, S. J., Henry, M. C., Brindle, M., and Moss, R. L.
Small
evidence for small incisions: pediatric laparoscopy and the need
for morerigorous evaluation of novel surgical therapies. Journal of
pediatric surgery
38: 1429-1433, 2003.
3. Rogers, D. A., Lobe, T. E., and Schropp, K. P. Evolving uses
of
laparoscopy in children. The Surgical clinics of North America
72:
1299-1313, 1992.
4. Madan, A. K., and Frantzides, C. T. Prospective
randomized
controlled trial of laparoscopic trainers for basic laparoscopic
skills
acquisition. Surgical endoscopy21: 209-213, 2007.
5. Van Sickle, K. R., Ritter, E. M., McClusky, D. A., 3rd,
Lederman, A.,
Baghai, M., Gallagher, A. G., and Smith, C. D. Attempted
establishment of
proficiency levels for laparoscopic performance on a national
scale using
simulation: the results from the 2004 SAGES Minimally Invasive
SurgicalTrainer-Virtual Reality (MIST-VR) learning center study.
Surgical endoscopy
21: 5-10, 2007.
6. Najmaldin, A. (Ed.) Operative Endoscopy and Endoscopic
Surgery
in Infants and Children. New York: Oxford University Press,
2005.
7. Holcomb, G. W., 3rd, Rothenberg, S. S., Bax, K. M.,
Martinez-
Ferro, M., Albanese, C. T., Ostlie, D. J., van Der Zee, D. C.,
and Yeung, C. K.
Thoracoscopic repair of esophageal atresia and tracheoesophageal
fistula:
a multi-institutional analysis. Annals of surgery 242: 422-428;
discussion
428-430, 2005.
8. Desrosiers, J., Bourbonnais, D., Bravo, G., Roy, P. M., and
Guay,
M. Performance of the 'unaffected' upper extremity of elderly
stroke
patients. Stroke; a journal of cerebral circulation27:
1564-1570, 1996.
9. Georgopoulos, A. P., and Grillner, S. Visuomotor coordination
in
reaching and locomotion. Science (New York, N.Y245:
1209-1210,
1989.
10. Blinman T Incisions do not simply sum. Surg Endosc. 2010
Jul;24(7):
1746-51. Epub 2010 Jan 7.
11. Burgess, L. P., Morin, G. V., Rand, M., Vossoughi, J., and
Hollinger,
J. O. Wound healing. Relationship of wound closing tension to
scar width in
rats.Archives of otolaryngology--head & neck surgery116:
798-802, 1990.
P 22 f 22
http://www.ncbi.nlm.nih.gov/pubmed?term=%22Blinman%20T%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Blinman%20T%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Blinman%20T%22%5BAuthor%5D