Embed Size (px)
Citation preview
2018 AOCOPM Midyear MeetingSan Antonio
S-1
American Osteopathic College ofOccupational and Preventive Medicine
2018 Updates by FMCSA
American Osteopathic College of Occupational and Preventive Medicine
Updated: 9/28/2013
Daniel J Callan, DO/MPH-TM, FAOCOPM, FACOFP, FASMA
423-884-6760/[email protected]
American Osteopathic College of Occupational and Preventive Medicine
Certified Medical Examiner National Course Director
AOCOPM
SCHEDULE UPDATE: TODAYWHAT WE KNOW TO DATE: 03/10/2018Learning Objectives:Understand & comprehend FMCSA Medical Standards &
Federal Regs regarding & pertaining to Commercial Motor Vehicle (CMV) driver safety.
Understand Safety reasoning behind Process & Procedural requirements for obtaining & maintaining NRCME status.
SAFETY & RISK ASSESSMENT !!!
FMCSA OVERVIEW
American Osteopathic College of Occupational and Preventive Medicine
TIPS TO REMEMBERFIRST & FOREMOST: WHILE IT IS A RIGHT TO OWN PRIVATE OR COMMERCIAL MOTOR VEHICLE; IT IS A PRIVILEGE TO DRIVE THEM ON PUBLIC ROADWAYS,
SECOND, ALWAYS REMEMBER: THAT IN ANY MEDICAL DECISION MAKING DELIBERATIONS TO DETERMINE PHYSICAL QUALIFICATION FOR A CDL MEDICAL CERTIFICATE (SAFETY SENSITIVE POSITION);= YOU MUST ALWAYS INCLUDE PSYCH, PHYSICAL &
PSYCHOMOTOR COMPONENTS OF BODY (IN TOTO) & IN RELATION TO THE JOB FUNCTIONS
= YOU MUST ALWAYS CONSIDER THE EXISTENCE OF ANY MEDICAL CONDITION ALONG WITH IT’S THERAPY FOR DISQUALIFYING FACTORS, SEPERATELY & COMBINED!
American Osteopathic College of Occupational and Preventive Medicine
American Osteopathic College of Occupational and Preventive Medicine
AOCOPM FMCSA GOAL
DO OUR BEST TO:Ensure members and participants:• Obtain and utilize the latest process, procedures,
information and guidance from FMCSA & NRCME
• ARE knowledgeable, effective & efficient in your Driver evaluations
• ARE successful in keeping the Drivers between the ditches & Ensure that each assignment ends safely at home!
MISSION AND GOALS NRCME
National Registry of Certified Medical Examiners (NRCME/National Registry) is a Federal Motor Carrier SafetyAdministration (FMCSA) program.
ON OR BEFORE THE expiration of their MEC, All CMV drivers with a current valid MEC, must be examined by a NRCME Certified Medical Professional, whose scope of practice authorizes them to perform physical examinations, as defined by the State in which they practice AND ARE LISTED on the NRCME.

2018 AOCOPM Midyear MeetingSan Antonio
S-2
MISSION AND GOALS NRCMEOnly Certified Medical Examiners (CME) that have completed training/successfully passed a test on FMCSA's physical qualification standards will be;
CERTIFIEDThen listed on the National RegistryAllowed to perform medical examinations for commercial
motor vehicle (CMV) drivers in interstate commerce (ICS). Fully understand medical standards in FMCSA Regulations, any
related guidance & how they relate to medical demands of operating a CMV.
GOAL: NRCME to promote & preserve highest level of professional standards, training and care among CMEs AND requires that CME performing CMV driver examinations be trained and certified.
NRCME OBJECTIVESObjectives of NRCME are to:
Ensure that CME understand fully the medical standards in Federal Motor Carrier Safety Regulations (FMCSRs) and related guidance and how they apply to CMV drivers
Maintain ongoing competency of CME through training, testing, certification and recertification
Promote public confidence in quality of medical examinations of CMV drivers
Ensure that the list of certified medical examiners is easily accessible
Interstate Commerce (ISC)
ISC: trade, traffic, or transportation involving crossing of a State boundary.
Either the vehicle, its passengers, or cargo must cross a State boundary, or there must be the intent to cross a State boundary to be considered an interstate carrier.
IS determined by essential character of the movement, manifested by shipper's fixed & persistent intent at time of shipment, ascertained from all of the facts & circumstances surrounding the transportation.
When intent of transportation being performed is ICS in nature, even when the route is within boundaries of a single state, the driver and CMV are subject to FMCSA Regs.
IntrAstate commerce is trade, traffic, or transportation within a single State.
THING TO REMEMBERBe aware OF ALL new meds, indications, contraindication & side
effects.
Keep your Profile up-to-date, with professional & personal contact changes. Ensure that all your NRCME credentialing data is kept up-to-date to continue to remain on the NRCME including: All renewal of medical info: state license, change of address,
name, location & contact information. ALSO, your password for access to NRCME CME website must
be changed every 90 days, a Government standard.
To determine how you stack up against other CME visit the OOIDA website at: http://www.ooida.com/ReviewDoc.You will be able to see truckers reviews of your process procedures and charges, in addition to recommendations to other truckers on use of your services.
NRCME CURRENT NUMBERS• AS OF 01/10/18 TOTAL CME = 55,311
• SINCE 05/21/14: @6M ACTIVE Drivers
– 13.5M PASSED EXAM
– 512,000 FAILED EXAM
• TOTAL EXAMS: 14M
• 100/2017:
– 550,404 PASSED
– 23,617 FAILED
TOTAL: 574,021
EXAMS/CME= @ 270/YR OR 11/MONTH
ONLINE NO COST RECERTIFICATION TO BEGIN SOON
STATS
Stats 01/17/2018: 54,311 CMEs. Continue to need CMEs due to coverage discrepancies, turnover and attrition. FMCSA is working to align the zip codes of the trucker population with the Certified CME population to determine local resource needs and coverage. This is following the FAA AME model.
Enormous fraud is being perpetrated upon CMV drivers at truck stops & fly-by-night operations. If you know of someone using the state medical licensure info and a CME’s info off the FMCSA website to produce a fraudulent Medical Certificate, please call FMCSA Security Officer Alex Keenan at (202) 997-5404 or email at [email protected] IMMEDIATELY! The same applies to any Driver or company that threatens you or your staff. Call 911 and then FMCSA, provide as much information as possible. They will take care of them.

2018 AOCOPM Midyear MeetingSan Antonio
S-3
FMCSA Estimated Numbers• OVER 13 Million CDL Holders (2015)
– HEAVY TRUCK DRIVERS: 11,777,983
– 12M REGISTERED TRUCKS, 3,598 CMV FATAL Accidents, 8% INCREASE OVER 2014 (22 Fatalities/100K vs 3.4/100K FTE in
ALL other industries
– BUS DRIVERS: 691,400 to 735,300
– 843,000 REGISTERED BUSES, 261 CMV FATAL Accidents, INCREASE OF 11%
TOTAL: 4,337 FATALITIES 2015
138,000 INJURIES 2015
• Total 7 M active interstate CMV drivers needing DOT PE annual or Biannual
American Osteopathic College of Occupational and Preventive Medicine
STATSUltimate reason for regulations & recommendations, our Duty & Responsibility is to prevent, as much as reasonably possible, the road carnage for CMV drivers AND all drivers with medical conditions & on therapy!
BODY COUNT AND TREND as of 12/30/2015 FOR Large Trucks and Buses : 12M
CRASHES = 152,677 net increase of 4050 over 2014 OR 8%FATALITIES=4,311 a net increase of 11%INJURIES= 138,000 a net decrease of 1%
Large Truck Crash Causation Study (LTCCS) 78,000 CRASHESHuman Factors: DISTRACTION FATIGUE ASLEEP= 90 %Mechanical = 10% (25% due to tire or brake failure)Truck/Bus vs Auto: truck only 27%, auto 35% (cut off by distracted PDL auto)
Associated Human factors: OTC/RX MEDS, ILLEGAL DRUGS, ETOH, INT & EXT DISTRACTIONS (INTERNAL ACTIVITY, CONVERSATION, MOBILE COMMUNICATION DEVICES
COMORBIDITIES• EPI/STATS: CMV drivers constitute one of the
largest employment categories in the US.
• Controlled truck driving is hazardous and incur 22.0 fatal injuries/100k FTE compared to 3.4/100k FTE across all other industries
• 60k truck crashes past 5 yrs: cost /crash:
– $533,000 avg /injury
– $7-11M /fatality
– 30% caused by poorly functioning truck drivers
– Highest rates of chronic diseases, occupational injuries and fatalities compared with other working populations
QA/QI AUDITSPerformance Monitoring: CME
• Must provide MER & MEC to any authorized representative, special agent, or investigator of FMCSA or any authorized State or local enforcement agency representative to ensure compliance with FMCSA medical standards & guidelines in performing CMV driver medical examinations.
• FMCSA monitors medical examiner performance by: • Conducting periodic reviews of randomly selected CME listed
NRCME Website to ensure CMV driver examinations are being conducted properly.
• Periodically reviewing representative sample of the MERs associated name & numerical identifiers of applicants/drivers for errors, omissions, or other indications of improper certification.
QA/QI AUDITS
To comply with performance monitoring, you must: • Retain each original (paper or electronic) completed
MER & copy or electronic version of each MECs on file for at least 3 years from the date of the of examination.
•FMCSA will conduct annual medical examiner audits. Purpose of the audit is check percentage of CME listed on NRCME Website to obtain verification of eligibility (e.g., proof of current State medical licensure, registration, or certification to perform physical examinations & proof of completion of required training).
AUDITSRemoval from the National Registry FMCSA may remove a CME from NRCME when CME:
Fails to meet or maintain qualifications outlined in the CME Guide, requirements of other Federal regulations applicable to CME, or does not meet requirements of 49 U.S.C. 31149.
Reasons for removal may include, but are not limited to: • Failure of CME TO comply with requirements for continued listing
on NRCME.• FMCSA discovers that CME has made errors or omissions or finds
other indications of improper certification in either completed MER or MEC. (ATLANTA CHIROPRACTOR FALSIFICATION DOJ)
• FMCSA determines that CME issued a MEC to a CMV operator who failed to meet applicable standards at time of exam.
• Failure of CME to comply with FMCSA driver exam requirements.• Failure of the CME to complete training in physical & medical
examination standards.
2018 AOCOPM Midyear MeetingSan Antonio
S-4
CERTIFICATION REVIEW UPDATEMaintaining Certification: , you must:
• Be licensed, certified, and/or registered, IAW with applicable State laws & regulations to perform physical examinations in each state THE examinations are performed.
• Complete periodic training as specified by FMCSA every 5 yrs, & pass FMCSA Medical Examiner Certification Test q10 yrs.
• Agree to provide proof of eligibility upon FMCSA request.
Upon successful recertification, EFFECTIVE DATE?FMCSA WILL issue a new CME certification credential with new
expiration BUT maintain same NRCME number as long as you remain an FMCSA CME.
Continue to perform CMV driver physical examinations as long as your current certification has not expired.
If you have not passed FMCSA Certification Test by expiration of your FMCSA medical examiner certification, then you must cease performing driver exams until passing test again.
CERTIFICATION REVIEW UPDATETo ensure uninterrupted certification: Complete training requirement Pass the Recertification test within 1 year prior to certification
expiration date. Definitely not later than the end of 30-day grace period
following your certification expiration date. Failure to successful recertify within 1-yr (plus 30-day grace
period) timeframe, the following occurs: • Your certification expires; • Your information remains on the National Registry with a date of removal; and • CMV driver physical examinations performed after certification has expired are not recognized as valid by FMCSA
MORE THINGS1. UNSURE IF THERE ARE ANY HCP at FMCSA Medical
Programs Office A Non HCP was filling in until a replacement is
found. Further complicates communication and leadership
problems.
2. FMCSA allows drivers, who think a CME certification is wrong, to
seek a second exam from another certified CME, providing all
historical information is the full, the honest truth, and they do not
Doctor Shop. If Med certificate is different when entered into
NRCME system suppose to be red flagged, & reviewed to
determine if information provided to both CMEs is same, & be
investigated by the originating FMCSA state office.
COMORBIDITIES• N=38,184 DRIVERS
• Total crashes: 13,472
• Preventable crashes: 10,350
• Multiple Comorbid medical conditions results in 2-3X INCREASE CRASH RISK ESTIMATE
• SOURCE:
• JOEM, VOL 59, NO2 FEB 2017, Page 205 RESEARCH ARTICLE “Multiple Conditions Increase Preventable Crash Risks Among Truck Drivers in a Cohort Study” Retrospective
OSAOSA SPECIFICS:
a. NTSB 2017 Most Wanted List includes OSA for FFD, for 10 yrs
in a row. FAA has issued new guidelines for AME also.
b. FMCSA issued bulletin to CME/Training Organizations on
OSA: See link:
https://nationalregistry.fmcsa.dot.gov/NRPublicUI/documents/O
SA%20to%20MEs%20and%20Training%20Organizations-
01122015.pdf
c. NEW Regulation WAS working it’s way through Rule Making
Process as required by law. After the comment gathering stage
OFFICIAL’S HAVE WITHDRAWN THE NPRM!
FMCSA/NRCME OSA recommendations ARE still to use
current best medical practice and evidenced based guidelines.
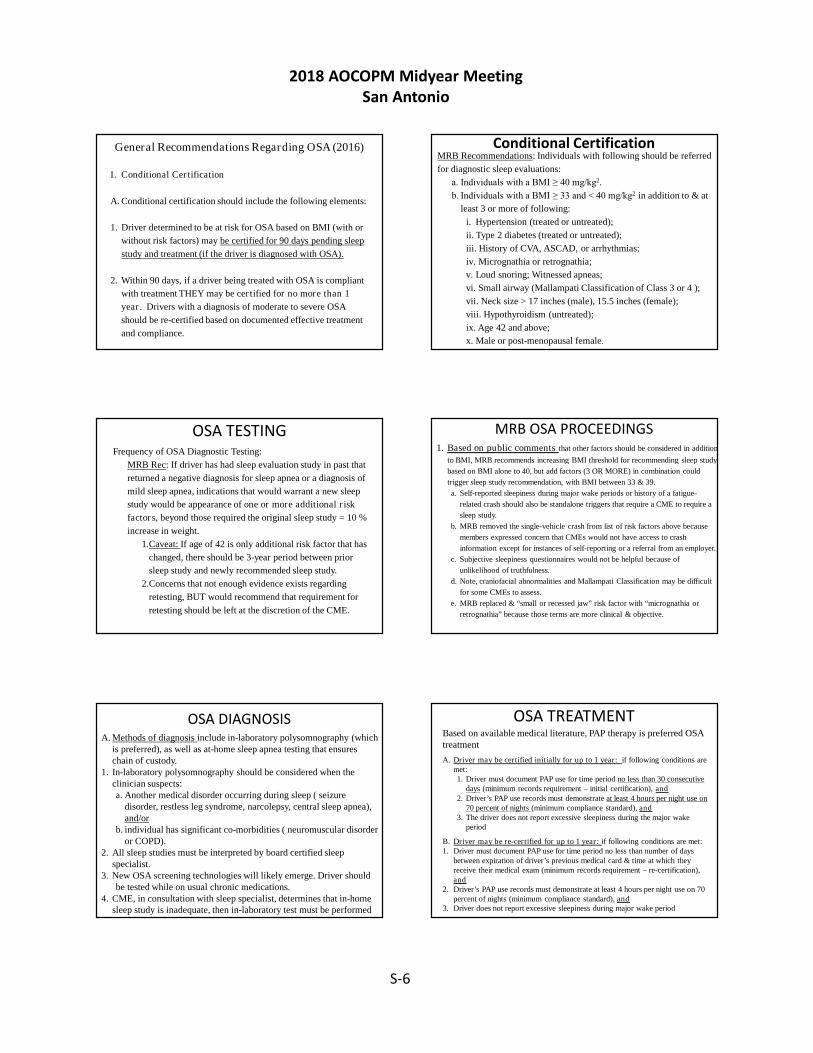
$30 billion
2018 AOCOPM Midyear MeetingSan Antonio
S-5
FMCSA OSA RULE MAKING TASKING
Agency received more than 600 comments to the ANPRM. In an effort to have MRB assist Agencies in furthering this rulemaking, we ask members to review & analyze all comments from medical professionals & associations & identify factors Agency should consider with regard to making a decision about next step in OSA rulemaking.
Additionally, given MRB & Motor Carrier Safety Advisory Committee’s (MCSAC) previous report on OSA from 2012, we request that MRB review that report to ensure that it addresses most current medical standards & practice & that it reflects comments received from listening sessions and in the docket.
MRB Task Statement 16–1
Recommendations to the Agency on disposition of comments from medical professionals & associations to Agency’s & Federal Railroad Administration’s (FRA) Advance Notice of Proposed Rulemaking (ANPRM) on safety-sensitive rail & commercial motor vehicle (CMV) drivers with moderate to severe Obstructive Sleep Apnea (OSA).
In 2012, FMCSA tasked its MRB & MCSAC with reviewing & recommending medical standards for identifying and treating CMV drivers with OSA.
In 2015, as a result of several high profile accidents involving untreated sleep apnea across several different modes of transportation, Office, Secretary of Transportation convened panel of representatives from several DOT modes to discuss broader development & application of standards for all transportation safety workers. As a result, FMCSA & FRA began working together on this issue of mutual safety concern & published the joint NPRM in March 2016. As part of effort to garner as much information from medical experts and drivers on OSA, we convened a series of listening sessions, which took place in Washington, DC, Chicago, IL, and Los Angeles. These sessions took place within comment period, which closed on July 8, providing agencies opportunity to hear first-hand information on this important safety topic.
2013-2016 Changes & Clarifications:
Obstructive Sleep Apnea (OSA): Bill signed by President in October 2013 mandates: that “any new or revised requirement providing for the
screening testing or treatment of individuals operating CMV for sleep disorders is adopted pursuant to a rulemaking proceedings (3-5 yrs). SAME FOR THE FAA POLICY.
FMCSA guidance is NOT a requirement, thus only requirement is the “drivers meet the medical standard (has no established medical history or clinical diagnosis of respiratory dysfunction) likely to interfere with their ability to control & drive a CMV safely”! All else is guidance!
CME use current best evidence based medical clinical judgment & practice in fitness to drive, risk for insidious or sudden incapacitation, and obtain or review any appropriate diagnostic studies. If high risk for OSA withhold certificate until tested and treated.
Remember it is the medical condition and medication treatment in Risk Assessment!
MRB ONGOING RESEARCH
a. Sleep Apnea & HTN and Heart Disease
b. ID Sleep Disorders in CMV Drivers using On Board Monitoring
Systems (OBMSS)
c. Effects of Detention Times on CMV Driver Fatigue
d. Advanced Fatigue Modeling for Individual differences
e. Driver Distractions: Eye Glance Analysis & Conversation
Workload
f. Methodologies & Statistical Approaches to Understanding Driver
Fatigue Factors in Motor Carrier Safety & Driver Health
g. Restorative Rest for Motor Coach Drivers
h. Conference on Transportation Operators’ Health/Wellness and
Fatigue
i. Drowsy Driver mitigation System
j. North American Fatigue Management Program
OSA
General Recommendations Regarding OSA (2016)A. CMEs must screen drivers presenting for medical certification for
OSA diagnostic testing.B. CMEs cannot issue a medical card for more than 1 year to a
driver with an established diagnosis of OSA, regardless of severity.
C. A CME may certify a driver with an OSA diagnosis if the driver is being treated effectively.
D. For certification purposes, “effective treatment” or “treated effectively” is defined as the resolution of moderate to severe OSA to mild or better, as determined by a board-certified sleep specialist.
General Recommendations Regarding OSA (2016)
Immediate Disqualification
A. Drivers should be disqualified immediately and referred for OSA diagnostic testing if any of the following conditions exist:
1. Individuals who have admitted fatigue or sleepiness during the
wake period.
2. Individuals who have been involved in a sleep-related motor
vehicle crash or accident or near crash.
B. Drivers found non-compliant with treatment should be disqualified
immediately until evaluated and treated effectively.
C. The CME should have the discretion to disqualify any driver who
appears to be at extremely high risk.
D. Drivers disqualified for any of the above reasons must remain
disqualified until evaluated and treated effectively.
2018 AOCOPM Midyear MeetingSan Antonio
S-6
General Recommendations Regarding OSA (2016)
I. Conditional Certification
A. Conditional certification should include the following elements:
1. Driver determined to be at risk for OSA based on BMI (with or
without risk factors) may be certified for 90 days pending sleep
study and treatment (if the driver is diagnosed with OSA).
2. Within 90 days, if a driver being treated with OSA is compliant
with treatment THEY may be certified for no more than 1
year. Drivers with a diagnosis of moderate to severe OSA
should be re-certified based on documented effective treatment
and compliance.
Conditional Certification MRB Recommendations: Individuals with following should be referred
for diagnostic sleep evaluations:
a. Individuals with a BMI ≥ 40 mg/kg2.
b. Individuals with a BMI ≥ 33 and < 40 mg/kg2 in addition to & at
least 3 or more of following:
i. Hypertension (treated or untreated);
ii. Type 2 diabetes (treated or untreated);
iii. History of CVA, ASCAD, or arrhythmias;
iv. Micrognathia or retrognathia;
v. Loud snoring; Witnessed apneas;
vi. Small airway (Mallampati Classification of Class 3 or 4 );
vii. Neck size > 17 inches (male), 15.5 inches (female);
viii. Hypothyroidism (untreated);
ix. Age 42 and above;
x. Male or post-menopausal female.
OSA TESTINGFrequency of OSA Diagnostic Testing:
MRB Rec: If driver has had sleep evaluation study in past that
returned a negative diagnosis for sleep apnea or a diagnosis of
mild sleep apnea, indications that would warrant a new sleep
study would be appearance of one or more additional risk
factors, beyond those required the original sleep study = 10 %
increase in weight.
1.Caveat: If age of 42 is only additional risk factor that has
changed, there should be 3-year period between prior
sleep study and newly recommended sleep study.
2.Concerns that not enough evidence exists regarding
retesting, BUT would recommend that requirement for
retesting should be left at the discretion of the CME.
MRB OSA PROCEEDINGS1. Based on public comments that other factors should be considered in addition
to BMI, MRB recommends increasing BMI threshold for recommending sleep study
based on BMI alone to 40, but add factors (3 OR MORE) in combination could
trigger sleep study recommendation, with BMI between 33 & 39.
a. Self-reported sleepiness during major wake periods or history of a fatigue-
related crash should also be standalone triggers that require a CME to require a
sleep study.
b. MRB removed the single-vehicle crash from list of risk factors above because
members expressed concern that CMEs would not have access to crash
information except for instances of self-reporting or a referral from an employer.
c. Subjective sleepiness questionnaires would not be helpful because of
unlikelihood of truthfulness.
d. Note, craniofacial abnormalities and Mallampati Classification may be difficult
for some CMEs to assess.
e. MRB replaced & “small or recessed jaw” risk factor with “micrognathia or
retrognathia” because those terms are more clinical & objective.
OSA DIAGNOSISA. Methods of diagnosis include in-laboratory polysomnography (which
is preferred), as well as at-home sleep apnea testing that ensures chain of custody.
1. In-laboratory polysomnography should be considered when the clinician suspects: a. Another medical disorder occurring during sleep ( seizure
disorder, restless leg syndrome, narcolepsy, central sleep apnea), and/or
b. individual has significant co-morbidities ( neuromuscular disorder or COPD).
2. All sleep studies must be interpreted by board certified sleep specialist.
3. New OSA screening technologies will likely emerge. Driver should be tested while on usual chronic medications.
4. CME, in consultation with sleep specialist, determines that in-home sleep study is inadequate, then in-laboratory test must be performed
OSA TREATMENTBased on available medical literature, PAP therapy is preferred OSA treatment
A. Driver may be certified initially for up to 1 year: if following conditions are met:1. Driver must document PAP use for time period no less than 30 consecutive
days (minimum records requirement – initial certification), and2. Driver’s PAP use records must demonstrate at least 4 hours per night use on
70 percent of nights (minimum compliance standard), and3. The driver does not report excessive sleepiness during the major wake
period
B. Driver may be re-certified for up to 1 year: if following conditions are met: 1. Driver must document PAP use for time period no less than number of days
between expiration of driver’s previous medical card & time at which they receive their medical exam (minimum records requirement – re-certification), and
2. Driver’s PAP use records must demonstrate at least 4 hours per night use on 70 percent of nights (minimum compliance standard), and
3. Driver does not report excessive sleepiness during major wake period

2018 AOCOPM Midyear MeetingSan Antonio
S-7
OSA CERTIFICATIONDriver fails to meet compliance standards, CME may provide a 30-day certification to allow driver to produce 30 days of consecutive PAP use data that meets the minimum compliance standard.
1. After driver demonstrates compliance with 30 days of PAP use data, CME may issue a 60-day certification to allow driver to produce 60 days of consecutive PAP use data that meets minimum compliance standard.
2. After driver demonstrates compliance with 60 days of PAP use data, CME may issue 90-day certification to allow driver to produce 90 days of consecutive PAP use data that meets minimum compliance standard.
3. After driver demonstrates compliance with 90 days of PAP use data, CME may issue a 1-year certification.
If driver cannot produce 30 days of consecutive PAP use data, driver must be disqualified & cannot be re-certified until THEY are able to provide 30 days of compliant PAP use data
OSA RESEARCH
DOT, DOD, NASA AGREEMENT ON PRINCIPLES OF OSA; Insufficient &/or disordered sleep jeopardizes the health,
wellbeing and safety of military, space and commercial personnel. Transient sleep difficulties often become tomorrows persistent sleep disorders.
Restorative sleep is a vital physiological function, and it’s failure to obtain sufficient sleep has been linked to adverse outcomes including degradation in cognition and compromised mental and physical health.
Sleep deprivation and sleep disorders appear to be common in many work professions
More understanding is needed to safeguard military, space and commercial readiness, safety and health throughout all American.
OSA RESEARCH
DOT, DOD, NASA AGREEMENT ON PRINCIPLES OF OSA;
Consequences of insufficient/disrupted sleep has shown an upward trend in sleep disorders & comorbidities, with utilization of coping strategies (stimulants, hypnotics and alcohol) for sleep and fatigue related concerns, but ultimately can fail, exacerbating sleep disturbances and setting the stage for PTSD, anxiety, depression and suicide.
Stress of having to do more with less, new regulations (HOS), adequate off duty rest, less than optimal sleeping environment, insufficient understanding of the importance and sleep.
Policies required to mitigate the negative consequences od insufficient/poor sleep and promote greater sleep health among employers and employees, from pre-diagnosis education, self recognition through sustained best treatment outcomes and quality of life.
FMCSA DISCLAIMER
Role of CME’ Clinical Judgment in Medical Certification Process :
FMCSA’s physical qualifications standards & advisory criteria do not provide OSA screening, diagnosis or treatment guidelines for CMEs to use in determining whether an individual should be issued a medical certificate.
CMEs may exercise their medical judgment & expertise in determining;
whether a driver exhibits risk factors for having OSA, & whether additional information is needed before making
a decision whether to issue the driver a medical certificate & duration
of medical certification.
THE WAY AHEAD: 2018Provide Driver with MECMEs are required to provide medically qualified CMV drivers with a paper copy of the MEC, Form MCSA5876 so that Commercial Learner’s Permit (CLP)/Commercial Driver’s License (CDL) applicants/holders are able to provide a copy to the State Driver’s Licensing Agency (SDLA), and the non-CDL drivers are able to provide the documentation to their employers and Federal and State enforcement officials.
Determination Pending The determination pending status allows the ME up to 45 days to obtain additional medical information and/or examination results in order to make a determination as to whether or not the driver is physically qualified to drive a CMV in accordance with § 391.41(b). If used the ME is required to inform the driver that:
• Additional information must be provided or further examination must be completed within 45 days.
• The Determination Pending status will be reported to FMCSA.
The driver may continue to operate a CMV if he/she has a current valid MEC.
If the requested information and examination results are not completed andprovided to the ME within 45 days:
• The examination will no longer be valid.
The driver is required to obtain a new examination in order to obtain a MEC, Form 5876
New Form (MCSA-5875)
• MUST use after April 20, 2016• More Extensive History• Required testing identical• Exam about the same• Outcomes quite different• Added options so same form can be
used for intrastate-only drivers
American Osteopathic College of Occupational and Preventive Medicine

2018 AOCOPM Midyear MeetingSan Antonio
S-8
LOOK BACK: “Old” outcome options
• Qualified – 2 Years
• Qualified – Less than 2 years
• Qualified with waiver or SPE
• Qualified 3 months (i.e. while BP fixed)
–Then we could issue card for rest of year
• Unqualified
American Osteopathic College of Occupational and Preventive Medicine
CURRENT “New” outcome options
• Qualified – 2 Years
• Qualified – Less than 2 years
• Determination Pending (45 days)
–Neither approved nor disqualified
• Unqualified
American Osteopathic College of Occupational and Preventive Medicine
2015-8 Change in the Spirit of the program
This will make your head hurt . . .
American Osteopathic College of Occupational and Preventive Medicine
• About 2008 FMCSA wanted to standardize the CDL Driver medical approval process
American Osteopathic College of Occupational and Preventive Medicine
• By 2012 FMCSA had a medical manual and a test for providers based on the manual and conference reports
MEDICAL EXAMINER HANDBOOK• Good news as the Medical Examiner Handbook WAS available as a
single PDF file to be downloaded. Bad news it has been removed from website for updating (11/2014). A copy can still be found in our dropbox on our website for use until new one published or use our MED DOT APP.
• As you are aware the HANDBOOK reference has been removed from NRCME and FMCSA websites with no instructions on what to do in the interim until the new hand book is posted. Date ?. I still use the old handbook and we have it posted on our AOCOPM website to download or use. Also refer to MEDDOT app.
• Really bad news is the elimination of essentially all references for OSA/chronic sleep disorders (except narcolepsy), and FAQ # 26, #57 & #60. Since the Medical Review Board (MRB) along with the FAA OSA recommendations have been forced into the Regulation (RULE) Making process,
• I use and recommend using Best Clinical Evidence Based Practice Guidelines.
• In a conference call about the new form FMCSA made it clear that everything they had produced to that point were general references (not rules), and that at all determinations are entirely up to the provider, and thus your liability
American Osteopathic College of Occupational and Preventive Medicine

2018 AOCOPM Midyear MeetingSan Antonio
S-9
American Osteopathic College of Occupational and Preventive Medicine
Remaining Absolute “No”• Vision
– Monocular Vision
– Visual Acuity
• Hearing
• Methadone, Marijuana
• Epilepsy
• Diabetes using Insulin
• FAQ: By regulation, Specific Medically Disqualifying Conditions Found Under 49 CFR 391.41 are Hearing Loss, Vision Loss, Epilepsy and Insulin Use.
American Osteopathic College of Occupational and Preventive Medicine
So . . . What about all the existing references?
• The resources still provide useful information
• You CAN deviate from those guidelines
• You will need to be able to justify your reasons in your documentation
American Osteopathic College of Occupational and Preventive Medicine
OTHER THINGSNEW INTEGRATION REGULATION: New software updated exam and medical certificate online forms were effective and available on 12/22/2015.
ALL NEW MEDICAL CERTIFICATES MUST BE ELECTRONICALLY TRANSMITTED WITHIN 24 HRS OF EXAM, EFFECTIVE 06/22/2018.
Current official FMCSA H&P exam and Medical Certifications formsare online available for download as a PDF file. If you use the current online electronic forms, only the 5850 form must be submitted, the exam long form and medical certificate copy must be kept on file in your office (electronic/paper formats for 3 years).
NEW MER Form, MCSA–5875• Make info collected on driver health history more comprehensive,
streamline format, strengthen efficiency of frequently used clinical processes & tools for performing driver physical exams
• Expand CME determination section, add statement for CME Signature, add NRCME Number, add section for amending CME determination.
• No longer include info about driver’s role, a listing of physical qualification standards for drivers, detailed instructions for performing exam, & medical advisory criteria, WILL be published in
FMCSA Guidance Documents & covered in training required for CME
to be listed on the NRCME.
• LATEST VERSION, WITH ALL REVISIONS, EFFECTIVE 09/2016
NEW MER Form, MCSA–5875• Expand CME determination section by eliminating
‘‘Temporarily Disqualified’’ option & adding ‘‘Pending Determination’’ option to defer decision temporarily for up to 45 days, if the CME requires additional info to make determination of whether driver was Qualified.
• Add place for CME to amend certification decision if driver did not require completely new exam. FMCSA
would consider any CMV Driver MER Form, MCSA–5850, displaying a ‘‘Pending Determination’’ status as
incomplete exam.
2018 AOCOPM Midyear MeetingSan Antonio
S-10
NEW MER FORM, MCSA–5875
• Information will be submitted & stored only in NRCME system.
• If disposition of Pending Determination exam is not updated by CME before 45 day expiration date, FMCSA would notify CME & driver in writing that exam is no longer valid & driver is required to be reexamined.
FMCSA will retain invalidated examination info in the NRCME Registry System.
NEW MER Form, MCSA–5875• FMCSA MAY 10, 2013: issued 49 CFR Parts 383,
384 and 391
• Medical Examiner’s Certification Integration
Eliminates advisory criteria (guidance) contained in current MER Form that has been sometimes misinterpreted when applying regulatory standards.
Permissible changes to 5875 & 5876, clarified 12/2016
CME can make more accurate decisions regarding
the physical qualification of CMV drivers.
NEW MER MCSA–5875• No longer include:
– Info on CMV drivers role,
– Instructions to the CME
– Statement for CME to review medications
– Now 38 numbered items under Health History
– Any illness or injury in past 5 yrs now in #32 “other health conditions not described above”.
• Questions added on: “ever had sleep study spent a night in hospital, had a broken bone, High Cholesterol, ever or current use of tobacco, illegal substances in past 2 yrs, or failed a drug test”
• Testing section will include Neck Circumference & BMI
• Attestation statement at end of form for CME sig and info.
2018 AOCOPM Midyear MeetingSan Antonio
S-11
INSULIN TREATED DIABETES MELLITUS PROPOSED CHANGES TO WAIVER EXEMPTIONSThe MRB recommended that ITDM drivers be medically disqualified unless they meet the following requirements demonstrating their stable, well controlled ITDM:
1. Driver must provide an FMCSA Drivers With Insulin Treated Diabetes Mellitus
Assessment Form (set out in the recommendations) to CME that has been
completed and signed by the treating clinician.
Treating clinician must be a Doctor of Medicine, a Doctor of Osteopathy, a Nurse
Practitioner or a Physician’s Assistant who prescribed insulin to the driver and is
knowledgeable regarding the treatment of diabetes.
2. Driver must receive a complete ophthalmology or optometry exam, including
dilated retinal exam, at least every 2 years documenting the presence or absence
of retinopathy/macular edema and the degree of retinopathy and/or macular
edema if present (using the International Classification of Diabetic Retinopathy and
Diabetic Macular Edema).
3. In addition, the MRB stated that, if a driver is medically disqualified due to not
meeting the ITDM criteria listed above & BELOW, the driver should remain
disqualified for at least 6 months.
MRB recommended that CME be allowed to certify an ITDM driver as medically qualified for a time period of no longer than 1 year only if the driver has not experienced any of the 8 disqualifying factors below(which the MRB believes should be listed in 49 CFR 391.46):1. Any episode of severe hypoglycemia within the previous 6 months.
2. Blood sugar less than 60 milligrams per deciliter (mg/dL) demonstrated in
current glucose logs.
3. Hypoglycemia appearing in the absence of warning symptoms (i.e.,
hypoglycemic unawareness).
4. An episode of severe hypoglycemia, blood sugar less than 60 mg/dl, or
hypoglycemic unawareness within the previous 6 months; the driver should be
medically disqualified and must remain disqualified for at least 6 months.
5. Uncontrolled diabetes, as evidenced by Hemoglobin A1c (HbA1c) level greater
than 10 percent. A driver could be reinstated when HbA1c level is less than or
equal to 10 percent.
6. Stage 3 or 4 diabetic retinopathy; a driver should be permanently disqualified.
7. Signs of target organ damage; a driver should be disqualified until the matter is
resolved by treatment, if possible.
8. Inadequate record of self monitoring of blood glucose; a driver should be
disqualified for inadequate records until the driver can demonstrate adequate
evidence of glucose records (minimum 1 month).
OTHER ISSUESWhat happens if a CMV driver is not truthful about his/her health
history on the medical examination form? FMCSA medical certification process is designed to ensure drivers are
PQ to operate CMV safely. Driver is required to complete Health History section of the
examination report & certify responses are complete & true.Driver must also certify that THEY understand that inaccurate, false or
misleading information may invalidate examination & CME's certificate.
FMCSA relies on CME's clinical judgment to decide whether additional information should be obtained from driver's treating physician.
Deliberate omission or falsification of information may invalidate the examination and any certificate issued based on it.
A civil penalty may also be levied against the driver under 49 U.S.C. 521(b)(2)(b), either for making false statement for concealing a disqualifying condition USAG OFFICE
DOT CDL DRUG & ALCOHOL CLEARINGHOUSEEFFECTIVE DATE 2016: data base under FMCSA admin that will
contain controlled substance & alcohol test result information for holders of CDLS
REQUIRES REGULATED MOTOR CARRIER EMPLOYERS, MRO, SAP & CONSORTIA/3RD PARTY ADMINISTRATORS TO REPORT:
verified positive (non-negative), adulterated & substituted drug test results, positive alcohol, test refusals, negative RTD test results, & information on f/u testing.
actual knowledge of traffic citations for driving cmv while under influence of alcohol or drugs.
TERMS OF ACCESS TO DATABASE, including conditions under which information would be submitted, accessed, maintained, updated, removed & released to prospective employers, current employers & other authorised entities.
REQUIRE LABORATORIES that provide FMCSA regulated motor carrier employers with DOT drug testing services to report annual summary of information about their testing activities
DOT CDL DRUG & ALCOHOL CLEARINGHOUSE
CLEARINGHOUSE REQUIRES EMPLOYERS TO QUERY THE DATABASE:Annually for each driver they currently employ for current &
prospective employees drug & alcohol violations before permitting those employees to operate CMVs.
SDLA REQUIRED TO QUERY DBASE WHENEVER A CDL IS ISSURED, RENEWED, TRANSFERRED OR UPGRADED.
RECORDS OF DRUG & ALCOHOL VIOLATIONS WILL REMAIN IN THE DBASE FOR 5 YEARS
CONTROLLED SUBSTANCE RANDOM TESTING RATE REMAIN 25% FOR CALENDAR YEAR 2017
2018 AOCOPM Midyear MeetingSan Antonio
S-12
AUDIO BOOTH TESTING EQUIPEMENT
What is the ANSI Standard?
When the audiometric device is calibrated to the American National Standard (formerly the American Standard Association (ASA) Z24.5-11951. Since the prescribed standard under the FMCSRs is the American National Standards Institute (ANSI), it may be necessary to convert the audiometric results from the ISO standard to the ANSI standard. Instructions are included on the Medical Examination Report form.
WAIVER VS EXEMPTIONWhat is a waiver? An exemption? Waiver/Exemption is temporary regulatory relief from one or more of the FMCSRs given to a person subject to the regulations, or a person who intends to engage in an activity that would be subject to the regulations.
Waiver provides the person with relief from the regulation for up to three months. 49 CFR 391.64 provides waivers to CMV drivers who were in the initial vision and insulin programs in the early 1990's. A waiver is intended for unique, non-emergency events and is subject to conditions imposed by the Administrator.
Exemption provides the person or class of persons with relief from the regulations for up to two years, but may be renewed.Exemption programs are for drivers of CMVs that intend to operate in interstate commerce in US, which FMCSA Regulations define as 50 states & DC. (VISION, DM,
FINAL THOUGHTSPhysical qualifications and examinations
§391.45 Persons who must be medically examined and certified.
Except as provided in §391.67, the following persons must be medically examined and certified in accordance with §391.43 as physically qualified to operate a commercial motor vehicle:
(a) Any person who has not been medically examined and certified as physically qualified to operate a commercial motor vehicle;
(b)(1) Any driver who has not been medically examined and certified as qualified to operate a commercial motor vehicle during the preceding 24 months; or
(b) (2) Any driver authorized to operate a commercial motor vehicle only with an exempt intra city zone pursuant to §391.62, or only by operation of the exemption in §391.64, if such driver has not been medically examined and certified as qualified to drive in such zone during the preceding 12 months; and
(c) Any driver whose ability to perform his/her normal duties has been impaired by a physical or mental injury or disease.
[35 FR 6460, Apr. 22, 1970, as amended at 36 FR 223, Jan. 7, 1971; 54 FR 12202, Mar. 24, 1989]
FINAL THOUGHTS
Finally, drivers whose ability to perform their normal SAFETY SENSITIVE driving duties has been impaired by injury or disease are required by Sec. 391.45 to be reexamined before resuming such duties.
THUS RTW/FFD EXAMS SHOULD BE FMCSA PE
AFTER THOUGHTS396.41 CMV medication questionnaire draft/optional available
on line
REGULATION RESEARCH TO UPDATE “LICIT USE OF SCHEDULE II MEDICATIONS”
3rd party organization reporting services, find guidance on website.
No use of SAMSUNG GALAXY NOTE 7 SMARTPHONE IN CMV 10/2016FMCSA ALTERNATIVE TRAINING & TESTING CME EMPLOYED BY VA
TN TRUCK DRIVER imminent hazard to public safety posting on website under newsroom, 2x in 4 days, DUI, domestic violence both alcohol related
2018 UPDATESMRB PROPOSED MODIFICATION TO ITDM FORM IN PREPARATION TO
ELIMINATE THE BLANKET PROHIBITION AGAINST INSULIN TREATED DIABETICS MELLITUS ASSESSMENT TO BE COMPLETED BY PCP AND SENT TO CME.
EMPLOYER LARGE SCALE MANDATED OSA PROGRAM RESULTS FOUND DRIVERS HAD PREVENTABLE CRASH RATE 5 X THAN THOSE WHO ADHERENT, AND WERE NOT RETAINED IN THEIR JOB.
RESEARCH FOUND NO CONSISTENT SET OF GUIDELINES EXIST THAT ADDRESS THE RISK OF A 2ND CATASTROPHIC EVENT AFTER AN INITIAL CVA IN SAFETY CRITICAL OCCUPATIONS.
NRCME WEBSITE DOWN FOR UPGRADE X3 MONTHS, MUCH LIKE THE CME HAND BOOK (2YRS),MUST KEEP MED LICENSE UTD/CURRENT
MEDICAL EXAMINER RECERTIFICATION: CANDIDATES FOR CME ARE UNABLE TO ACCESS, CREATE PROFILE, OBTAIN
UNIQUE ID NUMBER, FOR TRAINING COURSE AND TESTING.CURRENT CME UNABLE TO SEND EXAM INFO, MUST SAND BAG AND
UPLOAD WHEN ALLOWED, UNABLE TO RECERT, OR UPDATE PROFILEENSURE YOU ARE ON THE NRCME LISTSERVE TO GET UPDATES

2018 AOCOPM Midyear MeetingSan Antonio
S-13
2018 UPDATE• OSA: NO RULE/REGULATIONS PROMULGATED
REQUIRING MEDICAL EVAL AND COMPLIANCE WITH TREATMENT
• USE BEST MEDICAL PRACTICE• MAKE PART OF FATIGUE RISK MANAGEMENT
PROGRAM• CAN USE AVAILABLE RESOURCES
– 2015 BULLETIN REGARDING OSA– 2016 MRB RECOMMENDATION TO TREAT OSA
“THE ONLY INCORRECT THING IS TO DO NOTHING”DRIVER MEDICATION FORM FOR PCP TO COMPLETE
AVAILABLE ONLINEAmerican Osteopathic College of Occupational and Preventive Medicine




























