Embed Size (px)
DESCRIPTION
The Missouri Center for Patient Safety's Annual Report highlights achievements and growth in the area of patient safety in healthcare throughout the United States in 22007-2008.
Citation preview

2007 - 2008 Report
A health care environment safe for all patients, in all processes, all the time.
O u r M i s s i o n
“To be a leader in providing
solutions and resources to
improve patient safety and
the quality of health care
delivery by conducting
activities in collaboration
with health care providers,
physicians, purchasers,
consumers and government.”


M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y 2 0 0 7 - 2 0 0 8 R e p o r t
C o n t e n t s
A N o t e f r o m t h e E x e c u t i v e D i r e c t o r . . . . . . . . . . . . . . 1
S u m m a r y o f 2 0 0 7 - 2 0 0 8 : M o v i n g F o r w a r d . . . . . . . . . . . . 3
A c c o m p l i s h m e n t s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Certification as a Patient Safety Organization (PSO) 5
Special Initiatives 6
Education and Training 9
W h a t W e K n o w a n d D o n ’ t K n o w A b o u t T h e S a f e t y o f C a r e i n M i s s o u r i . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 5
C o m i n g i n 2 0 0 9 - 2 0 1 0 . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2
F o u n d i n g M e m b e r s a n d B o a r d o f D i r e c t o r s . . . . . . . . 2 4
A d v i s o r y P a n e l . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 5
S p o n s o r s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 6
A p p e n d i x A . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 7
R e f e r e n c e s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3


1
2 0 0 7 - 2 0 0 8 R e p o r t
ince the Center’s inception in 2005, in response to the recommendation
Sincerely,
A Note from the Executive Director
Becky Miller, MHA, CPHQ, FACHE Executive Director
Sof the Missouri Commission on Patient Safety, and with initial support of the Center’s founding members, groundbreaking work to bring together
stakeholders and establish statewide resources for patient safety has become a reality in Missouri.
I am pleased to share this report highlighting our accomplishments since our first report in 2006, our view of the safety of health care in Missouri, and our plans for the future.
In particular, we are excited to be actively moving forward as one of the first ten Patient Safety Organizations in the nation to certify and be listed by the Agency for Healthcare Research and Quality. As a federally listed PSO, the Center will implement provisions of the Patient Safety and Quality Improvement Act of 2005 – provide protection and confidentiality to providers that report errors and unsafe conditions, analyze errors, share learning from the errors, and ultimately prevent devastating and costly errors from occurring in the future.
Such exciting work can only be accomplished with ongoing funding and collaboration with Missouri’s health care providers, regulators, insurers, businesses, and other key stakeholders interested in improving the safety of health care in Missouri.
We hope you will join us in this exciting work and will join me in celebrating the progress we have made since 2005!
To meet the Commission’s recommendation and our founding members’ vision for a “private center…to act as a leadership vehicle for patient safety improvements, and be a resource for health care organizations, professionals, and consumers,” we have sought to do just that during the past three years.

“We plan to work with
providers on a voluntary
and confidential basis
to gather the necessary
data and information
about medical errors to
learn what errors occur,
why they occur, and
most importantly, to
share the learning about
how to prevent errors.”
3
2 0 0 7 - 2 0 0 8 R e p o r t
Moving ForwardDuring our first full three years of operation, the Missouri Center for Patient Safety has continued to gain recognition and participation in our work to improve the safety of health care provided in Missouri. The Center has brought together health care providers, state agencies, insurers and others with a vested interest in improving patient safety to share, learn, and facilitate improvement.
The Center has successfully implemented statewide projects – the Missouri Just Culture Collaborative to improve the culture for safety, and the Banding Together – for patient safety project to improve processes of care by decreasing the potential to confuse the use of colored wristbands.
In addition, priority issues for Missouri’s hospitals have been identified by the Center’s Hospital Advisory Committee, and two traditions have continued – the Center’s annual conference and sponsoring of Missouri Patient Safety Awareness Month.
Our most exciting venture now is to move forward as a federally listed Patient Safety Organization (PSO) to collect adverse event data and information, analyze the data for the purpose of learning, and share the learning to further improve care. Under federal legislation, the Center, as one of the first ten organizations in the nation to certify as a PSO, can offer protection and confidentiality to health care
S u m m a r y o f 2 0 0 7 - 2 0 0 8
As a PSO, the Center will continue to provide education and training, serve as a resource center, and facilitate statewide projects by working with stakeholders across Missouri to make measurable improvements in the safety of health care provided to Missourians.
providers that work with us. As a PSO, we plan to work with providers on a voluntary and confidential basis to gather the necessary data and information about medical errors to learn why they occur, and most importantly, to share the learning about how to prevent errors.

M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y
4
“As a statewide PSO, the Center will also establish an ongoing network among participants as a forum to share and learn about processes and practices to further enhance improvements.”
5
2 0 0 7 - 2 0 0 8 R e p o r t
Certification as a Patient Safety Organization (PSO)On November 5, 2008 the Center
Background and Overview of Federal Legislation Establishing PSOs
The Patient Safety and Quality Improvement Act of 2005, Public law 209-41 (the Act) was signed into law in response to the 1999 “To Err Is Human” report of the Institute of Medicine that called for Congress to establish a network of independent PSOs. The law establishes procedures for voluntary, confidential reporting of medical errors to designated PSOs and provides significant federal protection and confidentiality for entities and individuals reporting such errors.
Although clinicians have been encouraged to report safety events in the past, until implementation of the Act, two major impediments stood in the way of collecting enough information to make significant improvement in the prevention of medical
errors - fear of liability and lack of standardized data collection to truly analyze and learn about patterns and causes of errors.
Key Provisions of the Act
The Act defines requirements of PSOs to certify with the Secretary of Health and Human Services to work with any provider licensed by the state. PSOs will work with providers to collect Patient Safety Work Product within a Patient Safety Evaluation System, as defined within the law and subsequent regulation.
If working with a PSO, the Act gives providers legal protection for data, reports, records, memoranda, analyses, written or oral statements reported to or developed by a PSO to improve safety, quality or outcomes. Legal protection is also provided to those who report to a PSO.1
Benefits of PSOs
• Establishing a culture that encourages reporting and sharing of data and information about medical errors
• Participation in a national network of PSOs to further increase sharing and learning
• Comparative data and information about adverse events
• Potential to streamline adverse event reporting requirements of providers to various payers
A c c o m p l i s h m e n t s
became one of the first ten PSOs to be listed by the Agency for Healthcare Research and Quality under provisions of the federal Patient Safety andQuality Improvement Act of 2005. Being listed as such now allows the Center to fulfill the intent of the Missouri Commission for Patient Safety and the Center’s founding members.

M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y
6
• Potential to prevent 1-3% of preventable adverse events within the first five years, saving $435 million in healthcare costs nationally2
• Potential to decrease professional liability costs such as those from objects left after surgery and pressure ulcers that, alone, account for over 12% of medical professional liability costs3
Missouri Center for Patient Safety as a PSO
As a federally-designated and statewide PSO, the Center will work to identify what adverse events occur, why they occur, and facilitate the prevention of errors. Based on statistics published in the Federal Register2, low estimates reveal over 7,500 preventable adverse events could be eliminated annually, saving approximately $7.5 million in healthcare costs in Missouri alone.
To accomplish this, the Center will not only establish a data system to collect, analyze and report adverse event data, but use knowledge learned from the analysis and reporting to focus our education, training, and support to participating providers.
As a statewide PSO, the Center will also establish a network among participants as a forum to share and learn about processes and practices to further enhance improvements.
Special InitiativesBanding Together - for patient safety
Upon learning that Missouri providers were identifying at least 21 different clinical conditions using no fewer than 29 different colors of wristbands4, the Banding Together – for patient safety project was launched. The Center took leadership of this project in July 2007, which made Missouri the 7th state in the nation to voluntarily standardize the use of colored wristbands for high priority conditions in hospitals. There are now over 20 states that have implemented the same or similar recommendations.
As the result of this project, over 110 Missouri hospitals have voluntarily implemented some or all of the recommendations of Banding Together by using red wristbands to designate allergy risk, yellow to designate fall risk, and purple to designate “Do Not Resuscitate” orders. Other recommendations of the project include using text on the wristbands to reinforce quick recognition, removal of personal wristbands worn into the hospital by patients, and encouraging other healthcare providers to implement the same recommendations.
A c c o m p l i s h m e n t s

7
2 0 0 7 - 2 0 0 8 R e p o r t
Missouri Just Culture Collaborative
In September 2007, the Center, with grant funding from the National Council of State Boards of Nursing, launched the Missouri Just Culture Collaborative. The collaborative sought to establish a common understanding of Just Culture principles between health care providers and regulators – an open, learning environment, consistent management of system and human errors, and appropriately taking necessary disciplinary action.
The Collaborative, scheduled to end February 2009, led to commitment of state associations, state agencies, health systems, and healthcare providers. Sixty-seven organizations are participating in the collaborative, including hospitals, a nursing home, physician practices, a professional school, a statewide association, and state regulatory agencies.
Collaborators are participating in an assessment of organizational culture, education, and training sessions for each organization’s champion and leadership team, in addition to training of many managers and staff.
Collaborating organizations are also participating in a web community and monthly teleconferences to share information and learn additional aspects of a Just Culture.
A c c o m p l i s h m e n t s
Scott Griffith, Outcome Engineering, addressing statewide leaders about Just Culture principles
Becky Miller, MOCPS, addressing Just Culture Champions at an initial training session

M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y
8
Hospital Safety Priorities
In July 2008, with special funding provided by the Missouri Hospital Association, a Hospital Advisory Committee was established representing Missouri hospitals and health systems. The Committee identified the following priority patient safety issues for further research and potential statewide collaboration:
• Prevention of injury from falls
• Hand hygiene
• Pressure ulcer prevention
• Surgical safety
• Medication safety
• Health literacy
• Identifying opportunities for a clinical collaborative
Initially, a pilot project on fall injury reduction, is the result of this committee’s work.
Patient Safety Awareness Month
Since its inception, the Center, in collaboration with the Missouri Department of Health and Senior Services, has sponsored the first ever Missouri Patient Safety Awareness Month.
Following a focus on consumer medication safety in 2006, this special month in 2007 highlighted the Center’s “Patient Safety: Achieving Success in Missouri” conference, along with the launch of the Banding Together - for patient safety and the Missouri Just Culture Collaborative projects.
A c c o m p l i s h m e n t s
MOCPS and DHSS representatives with Gov. Blunt declaring March as Patient Safety Awareness Month

9
2 0 0 7 - 2 0 0 8 R e p o r t
In 2008, this month highlighted the “Ask Me 3™” campaign of the National Patient Safety Foundation encouraging consumers to always ask three questions to ensure successful communication with their health care professionals:
• “What is my main problem?”
• “What do I need to do?”
• “Why is it important for me to do that?”
Institute for Healthcare Improvement Node
In 2007, the Center joined with the Missouri Hospital Association and Primaris to support the efforts of Missouri hospitals in IHI’s Saving 5 Million Lives from Harm campaign. These efforts resulted in 86 hospitals participating in the initiative to continue the six interventions of the IHI’s 100,000 Lives Campaign (rapid response teams, acute myocardial infarction care, prevention of adverse drug events, central line infections, surgical site infections, and ventilator-associated pneumonia) and new interventions (preventing harm from high-alert medications, reducing surgical complications, preventing pressure ulcers, reducing MRSA infections, care for congestive heart failure, and engaging boards in safety efforts).5
Education and TrainingAnnual Conferences
A c c o m p l i s h m e n t s
Jonah Borrelli, IHI, speaking at the launch of the Missouri Node’s 5 Million Lives campaign. Sharon Burnett, Missouri Hospital Association, in the background
Attendees participating in break-out sessions at the “Patient Safety: Achieving Success in Missouri” conference

M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y
10
In 2007, the Center held its first conference, “Patient Safety: Achieving Success in Missouri.” followed by “The Art and Science of Patient Safety” in April 2008. Approximately 350 individuals have participated in these conferences.
As a result of conference successes, the Center plans to hold annual conferences bringing national speakers to Missouri to share successful efforts that tangibly improve patient safety, highlight successes in other states, and showcase safety practices occurring right here in Missouri.
Education and Training
A c c o m p l i s h m e n t s
Participants acknowledging speakers at “The Art and Science of Patient Safety” conference
Attendees enjoying poster displays of patient safety practices during the annual conferences
James Saxton, Esq. and Doug Wojcieszak, Sorry Works Coalition, greet Kathy Butler of Greensfelder, Hemker and Gale during a book signing at “The Art and Science of Patient Safety” conference

11
2 0 0 7 - 2 0 0 8 R e p o r t
Attendees have commented:
“Awesome benefits from both days – it gave me great ideas!”
“Excellent speakers comparable to some national conferences.”
“Excellent conference! Excellent speakers!”
“This was well worth the time and money.”
“Thank you for providing the great opportunity of networking!”
A four member team sponsored by the Center was accepted to participate in the Agency for Healthcare Research and Quality
A c c o m p l i s h m e n t s
The MOCPS PSIC team: Janet Schaffner, HSG; Sharon Burnett, MHA; Becky Miller, MOCPS, and Dana Lammert, Primaris
™
and the Veterans Administration Center for Patient Safety’s Patient Safety Improvement Corp (PSIC). The team participated in three weeks of intense training by national leaders in patient safety from August 2007 through May 2008.
As a result of the training, this team now brings nationally renowned training and expertise in patient safety to Missouri, including four TeamSTEPPS™ master trainers. The team is working to establish a modular safety training program on aspects of safety important for individuals responsible for organization-wide patient safety.
Patient Safety Improvement Corp.

M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y
12
Resource Center
The Center provides patient safety resources through its web site, responding to media inquiries, and by presenting to various audiences about the Center’s work and health care safety issues.
As the public face of the Center, its web site provides information and resources for health care providers, consumers, and the media, resulting in an estimated 35,000 annual hits. The site:
• Delivers the latest patient safety news
• Provides information about the Center’s activities and projects
• Houses a growing collection of patient safety related tools and resources
• Includes medication safety resources, “My Medicine List” for consumers and a medication safety brochure and poster for download
• Provides an opportunity for individuals to sign up to receive Center updates
• Provides background information about the Center, including contact information
• Lists educational and training opportunities, including the ability to register online for Center programs
• Enables users to submit sponsorships to the Center to support statewide patient safety work
The Center, through media sources has reached an estimated 723,000 individuals to educate them about the Center and our work to improve the safety of care in Missouri.
Center staff has also provided information and presentations to various audiences over the past two years, including clinical groups, nursing groups, healthcare associations, nursing home audiences, regulatory bodies, health systems, and hospitals in Missouri and other states.
Funding
The Center has been successful in obtaining financial support for its work, through the following sources:
• A 3-year grant from the Missouri Foundation for Health to support aspects of PSO implementation
• An 18-month grant from the National Council of State Boards of Nursing to support the Missouri Just Culture Collaborative
A c c o m p l i s h m e n t s
13
2 0 0 7 - 2 0 0 8 R e p o r t
• Financial support from Laserband®, Precision Dynamics Corporation®, St. Johns Companies™, and University of Missouri Health Care for the Banding Together - for patient safety project
• Funding from the Missouri Hospital Association to support work and projects specific to hospital safety
• Conference sponsors
• Individual and organizational sponsorships
With support from the Nonprofit Services Consortium, the Center has also established a Fund Development Plan to guide future work and to seek and maintain necessary funding.
A c c o m p l i s h m e n t s

M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y
14
“A health care
environment
safe for all
patients, in all
processes, all
the time.”

15
2 0 0 7 - 2 0 0 8 R e p o r t
W h a t W e K n o w a n d D o n ’ t K n o w A b o u t t h e S a f e t y o f C a r e i n M i s s o u r i
Publicly Available Data and Information Some data and information is available about the safety of care provided in Missouri, however, unlike over 20 states with some type of mandated adverse event reporting, Missouri does not have sufficient data and information to answer the following questions:
• What types of medical errors occur in Missouri?
• Why do these errors occur?
• What can be done to prevent errors from occurring?
• How is the safety of care improved over time?
• What events require special alerts to inform providers about potential risk and how to prevent it?
• What are the safety priorities for Missouri providers?
This section is an overview of the data publicly available about quality and safety of care, which is evidence of the need for more defined patient safety reporting in Missouri. Caution is needed in interpreting the data as each data set and reporting organization define indicators differently, use different data sets, and analyze the data in different ways.
What is important is that we are seeking well-defined, useful data to tell us the level of safe care provided in Missouri. While the data sets discussed below are pieces to the puzzle, the Center, now as a federally-listed PSO, will define reporting parameters, consistently analyze and report the data and information, and strive to answer these important questions for Missouri’s consumers and providers.
We need to learn much more, collectively, across the state for the Center to achieve its vision of “an environment safe for all patients, in all processes, all the time.”
See Appendix A for additional details of the data and information discussed below.
Centers for Medicare & Medicaid Services (CMS)
The CMS collects and reports certain nationally defined quality indicators for hospitals, nursing homes, home health agencies, and other providers. This information is available on the CMS web site, including organization-specific data.6
Although not defined as safety of care indicators, the CMS indicators reflect a component of the safety of care provided in these health care settings. There is also debate about these indicators relating to the accuracy of the data source, complexity of the calculations, usefulness to consumers, and

M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y
16
value of comparing average rates when most providers strive to provide better than average care. However, the measures do indicate failures to provide appropriate care - care that should have been given but was not, or care given in the incorrect manner – in addition to indicators of hospital patient satisfaction and outcomes, which are impacted by the quality and safety of care.
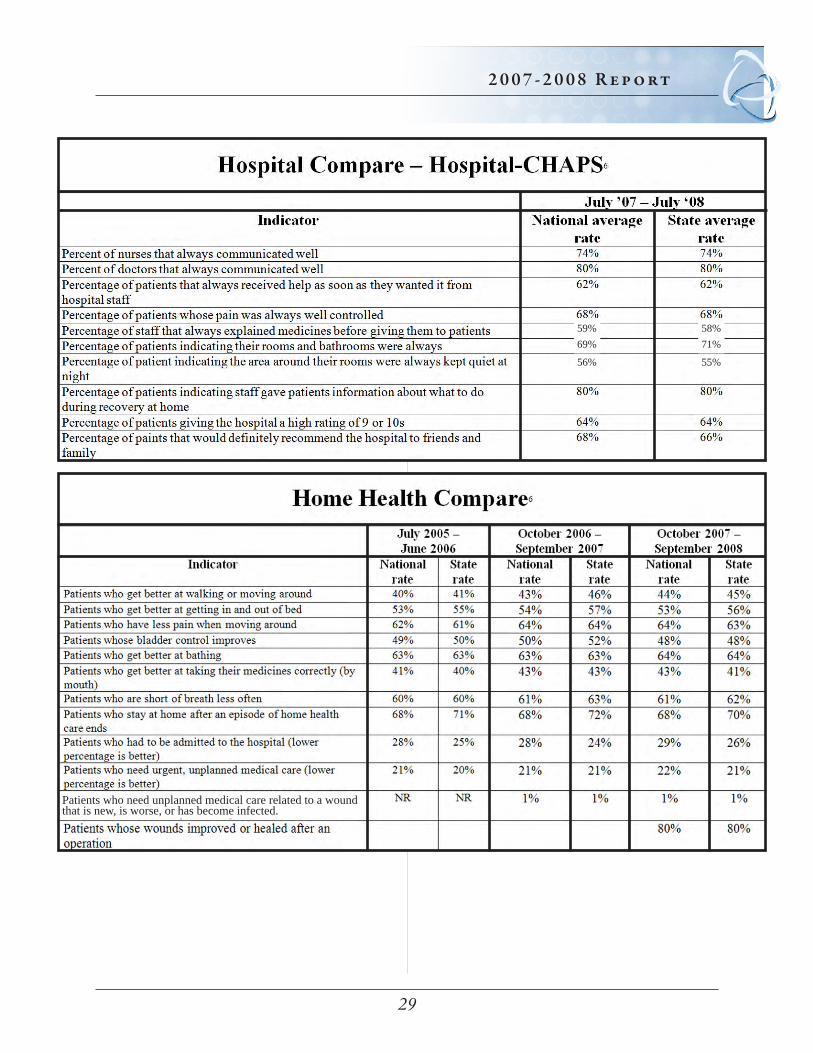
Hospital Compare, based on data collected and submitted by Medicare-certified hospitals, compares hospital clinical care processes for heart attack, heart failure, pneumonia, surgery and children’s asthma; 30-day mortality for heart attack, heart failure and pneumonia; and patient perceptions of care.
Through June 2008, Missouri data reveals the following compared to national averages:
• A better rate for three of the seven heart attack indicators (rates for percutaneous coronary intervention within 120 minutes and fibrinolytic treatment within 30 minutes of arrival being considerably better), one indicator the same and three worse
• A slightly better rate for one of the heart failure indicators and slightly worse for three
• A slightly better rate for four of the pneumonia measures, one slightly worse, and two equal to national rates
• For surgical indicators, five of seven indicators being slightly better and two being equal
• The mortality rate for heart attack, heart failure and pneumonia for most Missouri hospitals is similar to the national rate with the exception of five hospitals; one with a higher mortality for heart failure, two with a higher rate, and two with a mortality rate for pneumonia
• No state data is available for the children’s asthma measures
• Satisfaction with care indicators reveal Missouri with a slightly better rating on one indicator, three slightly worse, and the remaining six equal to national ratings
Home Health Compare compares indicators from the Outcomes & Assessment Information Set (OASIS) submitted to CMS by Medicare-certified home health providers. The most recent data, submitted through September 2008, reflects national and state rates for 12 indicators. Compared to national rates, Missouri’s rate is slightly better for six indicators, the same for four indicators, and slightly worse for the two indicators. Of the 11 indicators reported for the past two reports, eight are slightly worse than the previous year, two are equal, and one is slightly better.
Nursing Home Compare compares long-term care indicators as reported to CMS from the Minimum Data Set (MDS) by Medicare-certified long-term care providers. Data submitted on 19 indicators, reveals Missouri’s
W h a t W e K n o w a n d D o n ’ t K n o w A b o u t t h e S a f e t y o f C a r e i n M i s s o u r i

17
2 0 0 7 - 2 0 0 8 R e p o r t
rate, compared to the national rate, to be better for 10 indicators, the same for five indicators, and worse for four indicators.6
Missouri Nosocomial Infection Reporting
In response to state legislation, the “Missouri Nosocomial Infection Reporting Act of 2004,” the Missouri Department of Health and Senior Services began reporting health care acquired infection rates in December 2006.
The most recent report reflects central line associated blood stream infections for 106 ICUs in 72 hospitals for April 2007-March 2008, and surgical site infections reported from 65 hospitals and 26 ambulatory surgery centers (ASC).
Missouri’s bloodstream infection rate has decreased for all types of ICUs since reporting began in 2005 through March 2008. Missouri rates are also lower than the national rate of infection per 1,000 central line days. In addition, Missouri’s surgical site infection rates for hip repairs, abdominal hysterectomy, and coronary artery bypass surgery are lower than national rates.
Missouri’s reporting system is one of the few
collecting surgical site infection data for hernia repairs and breast surgery from ambulatory surgery centers, for which there is no national comparison. Missouri’s rates are 0.1 and 0.23 per 100 surgeries respectively as reported by the 26 ASCs.7
The DHSS Web site provides organization-specific rates.
Joint Commission
The Joint Commission’s Sentinel Event Policy calls for voluntary reporting of certain adverse events from its accredited facilities - unexpected occurrences involving death or serious physical or psychological injury, or the risk thereof.
The Joint Commission reports that 5,632 sentinel events have been reported from January 1995 through December 2008, the majority resulting in death. Of the 5,632 reported, 96 events were reported from Missouri (16 events per million population), 59 percent being self-reported to the Joint Commission by the accredited provider.8
Detailed information about the types of events, outcomes of the events, and causes of the events reported from Missouri are not available.
W h a t W e K n o w a n d D o n ’ t K n o w A b o u t t h e S a f e t y o f C a r e i n M i s s o u r i

M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y
18
Institute for Healthcare Improvement, Protecting 5 Million Lives from Harm Campaign
Eighty-six of the total 4,050 hospitals participating in the Protecting 5 Million Lives from Harm Campaign working to implement some or all of the following interventions are Missouri hospitals.
• Prevention of pressure ulcers
• Reduction in methicillin-resistant staphylococcus aureus infection
• Prevention of harm from high-alert medications
• Reduction in surgical complications
• Delivery of reliable, evidence-based care for congestive heart failure
• Getting boards engaged in patient safety
• Interventions from the 100,000 Lives Campaign (rapid response teams; acute myocardial infarction care; and preventing adverse drug events, central line infections, surgical site infections and ventilator-associated pneumonia).
Three of Missouri’s hospitals are designated as mentors for campaign focus areas - acute myocardial infarction, high alert medications, and ventilator-associated pneumonia.
Although individual participants have likely assessed their participation in these projects and improvements attributed to the project, this information is not known for the state as a whole.
A list of participating hospitals is available on the IHI web site.5
The Agency for Healthcare Research and Quality (AHRQ) Patient Safety Indicators (PSIs)
The AHRQ PSIs are indicators developed from claims data for certain safety events that occur in hospitals. The PSIs provide a snapshot of possible safety events to assist providers in further evaluation of safety issues.
Of the 20 PSIs reported, 19 are compared for Missouri’s hospitals, using 2005 national data and 2007 state data, the most recent comparative data available. Of these 19 indicators, Missouri’s rates are slightly better for eight of the indicators - death in low mortality DRGs, decubitus ulcer, postoperative hip fracture, postoperative physiologic and metabolic derangements, postoperative wound dehiscence, and all three OB trauma indicators; slightly worse on eight indicators - anesthesia complications; death of surgical inpatients with serious treatable complications; postoperative hemorrhage or hematoma, respiratory failure, pulmonary embolism, sepsis; accidental
W h a t W e K n o w a n d D o n ’ t K n o w A b o u t t h e S a f e t y o f C a r e i n M i s s o u r i

19
2 0 0 7 - 2 0 0 8 R e p o r t
puncture or laceration and birth trauma; and the same for three indicators - iatrogenic pneumothorax, infections due to medical care, and transfusion reactions.9
W h a t W e K n o w a n d D o n ’ t K n o w A b o u t t h e S a f e t y o f C a r e i n M i s s o u r i
HealthGrades.com
HealthGrades uses publicly available data sets to calculate quality and patient safety ratings for various types of health care providers. The most recent report analyzes over 41 million Medicare discharges from US hospitals from 2005-2007 to calculate mortality and complication rates for 27 diagnoses and procedures. HealthGrades also ranks providers using a star system, five stars being the best.
The report finds that mortality rates of five-star rated hospitals continue to improve at a faster rate than other hospitals. In addition, the report indicates that over 230,000 Medicare lives, associated with 17 procedures and conditions, could have been saved in the 2 years covered by the report if all hospitals performed at a five-star level.
Although state-specific data and ranking is not reported, Missouri is included in the West North Central region. This region was given a five-star rating for critical care and heart attack care; three stars for cardiac surgery and coronary interventional procedures; and one star for gastrointestinal, heart failure, pulmonary and stroke. Although Missouri is included in the category of having the least
improvement and the greatest three year-risk adjusted mortality; improvement was noted in scores for cardiac surgery, coronary interventional procedures, critical care, gastrointestinal, heart attack, heart failure, pulmonary, stroke and the overall composite score.
Individual facility results are posted on the web site in addition to ratings of physicians and nursing homes.10
AHRQ National Quality Report, Patient Safety
The Agency for Healthcare Research and Quality provides an annual report to Congress on quality, including patient safety, and disparity in health care. The most recent report identifies patient safety as the only measure set seen to decline, at a one percent rate. The quality measure sets showed improvement by three percent. Improvement in quality measures was greater in hospitals than in home health, long-term care and ambulatory care settings. Hospital improvements are attributed to the national focus and public reporting of quality indicators by the CMS and Hospital Quality Alliance.
The importance of patient safety is evidenced from the statistics used in the report: Up to 98,000 Americans die each year from medical errors,11 and at least 32,000 Americans die in the hospital each year due to 18 types of

M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y
20
W h a t W e K n o w a n d D o n ’ t K n o w A b o u t t h e S a f e t y o f C a r e i n M i s s o u r i
medical injuries.12 Costs attributable to medical errors is up to $29 billion,11 with the annual cost attributable to surgical errors alonebeing $1.47 billion.15
Only 17 of the 38 patient safety indicators showed any improvement. An overview of the indicator sets and changes reported is provided below.
• Postoperative care, pneumonia or venous thromboembolic event (improved)
• Timing of antibiotics for surgical patients (improved)
• Adverse events associated with central venous catheters (more events occurred)
• Potentially inappropriate prescription medications in adults age 65 and over (more events occurred)
• Catheter-associated urinary tract infections (no comparisons reported)
• Accidental puncture or laceration (more events occurred)
• Postoperative wound separation (more events occurred)
• Iatrogenic pneumothorax (slightly improved)
• Deaths following complications of care (improved)
• Deaths in low mortality diagnosis-related groups (improved)
• Adverse drug events in hospitals (more events occurred for intravenous heparin and insulin/hypoglycemic)
• Hospitalized patients with one or more adverse events (slightly improved; however, one in seven Medicare patients hospitalized are noted to experience one or more adverse events)
Information specific to Missouri for the patient safety indicators is not reported.
The report indicates the development of Patient Safety Organizations is expected to improve these overall measures of patient safety nationwide.13
The Leapfrog Group
The Leapfrog Group, a coalition of health care purchasers who advocate for transparency of the quality and safety of care and reward providers through payment for achieving certain goals, target certain areas of the United States. Missouri target regions are the Kansas City and St. Louis metropolitan areas. Hospitals in the target areas are asked to voluntarily implement the Leapfrog recommendations and participate in an annual survey.

21
2 0 0 7 - 2 0 0 8 R e p o r t
Highlights of the 2008 Leapfrog Hospital Survey Results, completed by 1,276 hospitals reveals:
• Only 7 percent of all hospitals responding to the survey fully meet the group’s recommendation to use computerized physician order entry
• Low percentages of hospitals fully meet the volume and mortality standards or adhere to evidence-based practices and guidelines for heart bypass, heart angioplasty, high-risk deliveries, pancreatic resections, bariatric surgery, esophagectomy, aortic valve replacement, and abdominal aortic aneurysm repair
• 65 percent do not have recommended policies for the prevention of hospital-acquired infections
• 75 percent do not fully meet standards for 13 evidence-based safety practices
• Only 26 percent fully meet standards for treatment of heart attacks, 34 percent fully meet standards for treatment of pneumonia, 30 percent for prevention of hospital-acquired pressure ulcers, 25 percent for preventing hospital-acquired injuries
W h a t W e K n o w a n d D o n ’ t K n o w A b o u t t h e S a f e t y o f C a r e i n M i s s o u r i
The report also identifies that more hospitals now meet the Group’s ICU staffing standard, have the recommended policies in place to prevent hospital acquired infections, and have implemented the policy of not charging for care involved with certain adverse events.
Sixteen of the targeted 53 hospitals in Missouri participated in the annual survey and are included in the report.
Information about the Group’s focus areas, reports, and hospital-specific information is available at www.leapfroggroup.org.14

M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y
22
C o m i n g i n 2 0 0 9 - 2 0 1 0As evidenced above, while we know some information about the safety of care provided in Missouri, many questions remain - questions we hope to answer through the Center’s efforts as a federally-designated Patient Safety Organization.
By providing federal protections to Missouri’s health care providers to share, analyze, and report safety data and information, the Center will begin to answer the following important questions, questions that are, to some extent, currently available in over 20 other states.
• What types of medical errors occur in Missouri?
• Why do these errors occur?
• What can be done to prevent errors from occurring?
• How is the safety of care improved over time?
• What events require special alerts to inform providers about potential risk and how to prevent it?
• What are the safety priorities for Missouri providers?
As a PSO, the Center will provide the following services for participating providers:
• Federally-designated legal protections
• Access to a web-based data platform to submit data, analyze, and report defined adverse event data
• Potential to interface with current automated reporting systems
• Real-time reports of facility-specific data and information entered into the system
• Comparative reports
• Technical assistance for establishing patient safety processes
• Assistance in defining policies and procedures to address PSO participation
• Networking opportunities within the state and nationally on patient safety improvement
• User group meetings
Through this work, we will establish a basis of knowledge about the events that occur in Missouri and move toward sharing the learning obtained about error prevention strategies.
This work will no doubt lead to informing of health policy, consumer choice, and provider practice, and ultimately safer care for Missourians.
23
2 0 0 7 - 2 0 0 8 R e p o r t
Also in 2009, the work of the Hospital Advisory Committee will expand as a result of the Center’s PSO designation to focus its work on priority projects, initially in the area of preventing injury from falls.
Activities that are now traditions will also continue - hosting of the annual conference to bring national and local safety experts to Missouri to share and learn about safety successes, sponsoring Missouri Patient Safety Awareness Month highlighting key messages for consumers and providers, and collaboration with the MHA and Primaris as Missouri’s Institute for Healthcare Improvement node.
All of this in addition to the Center’s web site, www.mocps.org, and serving as a statewide resource will continue to be enhanced and expanded.
The work accomplished by the Center during its first years of operation continues to serve as a basis to build upon to further the Center’s mission “to be a leader in providing solutions and resources to improve patient safety and the quality of health care delivery by conducting activities in collaboration with health care providers, physicians, purchasers, consumers and government.”
We hope that Missouri’s healthcare providers, consumers, regulators, insurers, and businesses will join us in our efforts.
C o m i n g i n 2 0 0 9 - 2 0 1 0

M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y
24
M O C P S F o u n d i n g M e m b e r s
Officers
Board MembersEdward Cabbabe, MD, St. Louis
Joseph Crossett, Liberty Hospital, Liberty
Dwight L. Fine, Missouri Hospital Association, Jefferson City (2007)
Daniel Landon, Missouri Hospital Association, Jefferson City (2008)
S. Gordon Jones, Jr., MD, Sikeston
Paula Nickelson, Missouri Department of Health and Senior Services, Jefferson City
C.C. Swarens, Missouri State Medical Association, Jefferson City
Coreen Vlodarchyk, BSN, Barnes Jewish Hospital, St. Louis
Joseph M. Yasso, Jr., DO, FACOFP, Grain Valley
Ex-OfficioBecky Miller, MHA, CPHQ, FACHE, Executive Director
H. Jerry Murrell, M.D.Secretary/Treasurer (2007),Vice-chair (2008)Columbia
Richard A. RoyerChair (2007),Secretary/Treasurer (2008)Columbia
Steve Bjelich, FACHEVice-chair (2008),Chair (2008)Cape Girardeau
M O C P S B oa r d o f D i r ec to r s ( 2 0 0 7 - 2 0 0 8 )

25
2 0 0 7 - 2 0 0 8 R e p o r t
Chair—Susan Kendig College of Nursing, University of Missouri, St. Louis
Brian Bowles (2008) Missouri Association of Osteopathic Physicians and Surgeons
Sharon Burnett Missouri Hospital Association
Jacque Christmas (2008) Missouri Department of Mental Health
Thomas Cartmell Wagstaff and Cartmell, LLP
Denise Clemonds Missouri Association of Homes for the Aging
Christine Crouch (2008) Bethesda Southgate
Erma Cunningham Consumer, AARP
Mike Delaney Healthcare Services Group
Jon Dolan Missouri Health Care Association
Ron Fitzwater Missouri Pharmacy Association
Kimberly O’ Brien (2008) Missouri Department of Health and Senior Services
Sharon Hoffarth, MD Primaris
Melissa Hogan - Watts (2008) St. Louis Area Business Health Coalition
Glen Jett President, Missouri Nurses Association
M O C P S A d v i s o r y P a n e l ( 2 0 0 7 - 2 0 0 8 )Ron Meyer Missouri Consolidated Health Care Plan
Pat Mills Missouri State Medical Association
Glenn Mitchell, MD (2007) Sisters of Mercy Health System
Shelley Neimeier SSM Health Care
Michael Perry, MD University of Missouri-Columbia
Deborah Ringenberger Missouri Board of Pharmacy
Janet Schaffner Healthcare Services Group
Mary Schantz Missouri Alliance for Home Care
Lori Scheidt Missouri State Board of Nursing
Robert Schwab, MD (2007) St. Lukes Hospital of Kansas City
Terry Seaton St. Louis College of Pharmacy
Tina Steinman Missouri State Board of Healing Arts
Douglas Wakefield, PhD University of Missouri-Columbia Center for Health Care Quality
Deborah Zimmerman, MD Mercy Health Plans
The Missouri Center for Patient Safety also thanks the organizations and individuals that support our projects by serving on advisory committees and work groups during 2007 and 2008, including the Hospital Advisory Committee, Consumer Advisory Committee, and PSO Data Work Group.
Bonnie Bowles (2007)
Lynn Carter (2007)
Laurie Hines (2007)

M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y
26
The Missouri Center for Patient Safety thanks the following sponsors for their support of the Center’s work and its mission and vision.
Platinum Healthcare Services Group (2006-2008)
Silver Missouri State Medical Foundation (2006-2008)
Bronze Missouri Organization of Nurse Leaders (2007)
Missouri Nurses Association (2007)
Missouri Association for Healthcare Quality (2007)
To support ongoing operations, the Center offers individual and organizational sponsorships. Sponsorships are also available for special projects undertaken by the Center.
S p o n s o r s
Sponsorship details are available at www.mocps.org/sponsors/ or by calling the Center at
(573) 636-1014

27
2 0 0 7 - 2 0 0 8 R e p o r t
A p p e n d i x A

M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y
28
hospitals, all are
s are
29
2 0 0 7 - 2 0 0 8 R e p o r t
59%69%
56%
58%71%
55%
Patients who need unplanned medical care related to a wound that is new, is worse, or has become infected.

M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y
30
(lower percentage is better)

31
2 0 0 7 - 2 0 0 8 R e p o r t

M i s s o u r i C e n t e r f o r Pat i e n t S a f e t y
32

33
2 0 0 7 - 2 0 0 8 R e p o r t
R e f e r e n c e s1 The Patient Safety and Quality Improvement Act of 2005, Public law 109-41; July 29, 2005
2 Federal Register, 42 CFR, Part 3, Patient Safety and Quality Improvement; Proposed Rule, Department of Health and Human Services, Tuesday, February 12, 2008
3 AON 2008 Liability Benchmark Analysis, September 2008
4 Use of Colored Wristbands Survey Results, Missouri Center for Patient Safety, December 2006
5 Institute for Healthcare Improvement, www.ihi.org/IHI/Programs/Campaign/, March 2009
6 Department of Health and Human Services, Centers for Medicare & Medicaid Services, www.medicare.gov, February 2009
7 Missouri Nosocomial Infection Reporting Data, Report to the Governor and General Assembly 2008, www.dhss.mo.gov/HAI/index.html?target=reports.html, February 2009
8 Sentinel Event Trends Reported by Year Updated Through 2008, Sentinel Event Additional Statistics, Updated Through 2008; www.jointcommission.org/SentinelEvents/Statistics/, April 2009
9 Missouri Hospital Performance Project, Missouri Hospital Association, June 2008
10 The Eleventh Annual HealthGrades Hospital Quality in America Study; October 2008; http://healthgrades.com, February 2009
11 Kohn, LT, Corrigan JM, Donaldson MS, eds. Institute of Medicine. Committee on Quality of Health in America. To err is human: building a safer health system. Washington, DC; National Academies Press; 1999
12 Zahn C, Miller MR. Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization. JAMA 2003 Oct 8;290(14):1868-74
13 National Healthcare Quality Report, 2008; Agency for Healthcare Research and Quality, AHRQ Publication No. 09-0001; www.ahrq.gov/qual/qrdr08.htm, April 2009
14 Leapfrog Hospital Survey Results, 2008, www.leapfroggroup.org/media/file/leapfrogreportfinal.pdf, March 2009
15 Encinosa WE, Hellinger FJ. The impact of medical errors on ninety-day costs and outcomes: an examination of surgical patients. Health Serv Res 2008 July 25 (Epub ahead of print). Available at www3.interscience.wiley.com/dgi-bin-fulltext/120855828/HTMLSTART
16 National Healthcare Safety Network (NHSN) Report, June 2007
17 National Nosocomial Infection Surveillance System Report; January, 1992 - June 2004



























