-
8/3/2019 Mitochondrial Disorders in Neurons 2008
1/35
Mitochondrial Disordersin the Nervous System
Salvatore DiMauro1 and Eric A. Schon1,2
Departments of Neurology1 and Genetics and Development,2
Columbia University MedCenter, New York, NY 10032; email:
[email protected], [email protected]
Annu. Rev. Neurosci. 2008. 31:91123
First published online as a Review in Advance onMarch 10,
2008
The Annual Review of Neuroscience is online
atneuro.annualreviews.org
This articles doi:10.1146/annurev.neuro.30.051606.094302
Copyright c 2008 by Annual Reviews.All rights reserved
0147-006X/08/0721-0091$20.00
Key Words
mitochondrial DNA, maternal inheritance, oxidative stress,
apoptosis
oxidative phosphorylation, aging
Abstract
Mitochondrial diseases (encephalomyopathies) have traditionally
been
ascribed to defects of therespiratory chain,whichhas
helpedresearcherexplain their genetic and clinical complexity.
However, other mitochon
drial functions are greatly important for the nervous system,
includingprotein importation, organellar dynamics, and programmed
cell death
Defects in genes controlling these functions are attracting
increasingattention as causes not only of neurological (and
psychiatric) disease
but also of age-related neurodegenerative disorders. After
discussingsome pathogenic conundrums regarding the neurological
manifestations of the respiratory chain defects, we review altered
mitochondria
dynamics in the etiology of specific neurological diseases and
in thphysiopathology of more common neurodegenerative
disorders.
91
Click here for quick links to
Annual Reviews content online,
including:
Other articles in this volume
Top cited articles
Top downloaded articles
Our comprehensive search
FurtherANNUAL
REVIEWS
http://showhidebookmarks/http://showhidebookmarks/http://showhidebookmarks/http://showhidebookmarks/http://showhidebookmarks/http://showhidebookmarks/http://showhidebookmarks/http://showhidebookmarks/http://showhidebookmarks/http://showhidebookmarks/http://showhidebookmarks/http://showhidebookmarks/
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
2/35
Contents
INTRODUCTION . . . . . . . . . . . . . . . . . . 92
DISEASES OF THEMITOCHONDRIAL
RESPIRATORY CHAIN . . . . . . . . . . 93Disorders Caused by
Mutations in
mtDNA . . . . . . . . . . . . . . . . . . . . . . . .
93Disorders Caused by Mutations in
nDNA . . . . . . . . . . . . . . . . . . . . . . . . .
97DISEASES CAUSED BY IMPAIRED
MITOCHONDRIAL PROTEINIMPORT . . . . . . . . . . . . . . . . . .
. . . . . . . 103
DISEASES CAUSED BY ABERRANTMITOCHONDRIAL
DYNAMICS . . . . . . . . . . . . . . . . . . . . . . 104AGING
AND LATE-ONSET
NEURODEGENERATIVE
DISORDERS . . . . . . . . . . . . . . . . . . . . .
106Mitochondria and
Neurodegeneration . . . . . . . . . . . . . . . .
108Neurodegenerative Diseases Caused by
Mutations in Nuclear-EncodedProteins Targeted
to Mitochondria . . . . . . . . . . . . . . . . . . .
108MITOCHONDRIAL
PSYCHIATRY . . . . . . . . . . . . . . . . . . . .
112CONCLUSIONS . . . . . . . . . . . . . . . . . . . . 113
INTRODUCTION
Mitochondrial dysfunction plays a crucial role
in neurology. This notion became apparentthree decades ago when
pediatric neurologists
Table 1 Mitochondrial respiratory chain disease targets
Mutations in mtDNA Mutations in nDNA
R.C. subunits R.C. subunits
Complex I, II, IIIProtein synthesis genes Ancillary proteins
Rearrangements Complex I, III, IV, V; CoQ
tRNAs Intergenomic communication
rRNAs Multiple mtDNA deletions
Depletion of mtDNA
Translation of mt-mRNAs
Mitochondrial lipids
coined the term mitochondrial encephalom
opathies to call attention to the frequent ocurrence of brain
disease in children w
mitochondrial alterations in their muscle biosies (Shapira et
al. 1977). The selective v
nerability of skeletal muscle and of the n vous system was
confirmed in 1988, wh
the first pathogenic mutations in the michondrions own DNA
(mtDNA) were disco
ered (Holt et al. 1988, Wallace et al. 198These discoveries
heralded the era of michondrial genetics and led to the
recogniti
of a multitude of mtDNA-related disordemostly maternally
inherited and mostly ma
ifesting as encephalomyopathies (DiMauroDavidzon 2005, DiMauro
& Schon 2003). B
cause mtDNA encodes only 13 proteins, of them subunits of the
mitochondrial respi
tory chainthe business end in terms of ATproductionanother
notionbecame widely
cepted: The term mitochondrial encephalomopathies was reserved
for defects of the res
ratory chain.Even within these boundaries, the classifi
tion of the mitochondrial encephalomyopathsoon became quite
cumbersome, including tflavors of primary mtDNA mutations
(i.e.,
impairment of global mitochondrial protsynthesis andof the
translation of specific res
ratory chain subunits) and a much larger meof Mendelian
disorders (Table 1). Also, g
netic errors in other fundamental mitochodrial functions that do
not affect the respirat
chain directly have major deleterious effects the nervous
system, including impaired imp
tation of mitochondrial proteins and defectsmitochondrial
dynamics, such as motility, fi
sion, fusion, and distribution.Another topic of current interest
is the r
of progressive mitochondrial dysfunction
normal aging and in the pathogenesis of laonset
neurodegenerative disorders.In this review, we discuss first the
nervo
system disorders caused by mitochondrial r
piratory chain defects, emphasizing how thpathogenesis is still
largely terra incognita. W
then consider the burgeoning new group of dorders attributed to
defects of mitochondr
92 DiMauro Schon
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
3/35
dynamics. Last, we review the neurodegenera-
tive disorders in which mitochondrial dysfunc-tion is either
primary or seems to be at least
involved in pathogenesis. We do not discussmitochondrial
metabolic pathway defects other
than the respiratory chain, such as pyruvate de-hydrogenase
complex (PDHC) deficiency or-
oxidation defects, although the nervous systemis frequently
affected in those disorders, too.
DISEASES OF THEMITOCHONDRIAL RESPIRATORYCHAIN
These diseases can be caused by mutationsin mtDNA (sporadic or
maternally inherited
traits)or by mutations in nuclear DNA(nDNA;Mendelian
diseases).
Disorders Caused by Mutationsin mtDNA
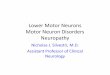
Human mtDNA (Figure 1) is a 16.6-kb cir-cular, double-stranded
molecule, which con-
tains 37 genes: 2 rRNA genes, 22 tRNA genes,and 13 structural
genes encoding subunits of
the mitochondrial respiratory chain (Andersonet al. 1981).
Reducing equivalents produced inthe Krebs cycle and in the
-oxidation spi-
ral are passed along a series of protein com-plexes embedded in
the inner mitochondrial
membrane(theelectron transportchain), whichconsists of four
multimeric complexes (I, II,
III, and IV) plus two small electron carriers,coenzyme Q (or
ubiquinone) and cytochrome c
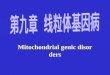
(Figure 2). The energy generated by the re-actions of the
electron transport chain is used
to pump protons from the mitochondrial ma-trix into the
intermembrane space (IMS) lo-
cated between the inner and outer mitochon-
drial membranes. This process creates an elec-trochemical proton
gradient, which is utilizedby complex V (or ATP synthase), a tiny
rotary
machine that generates ATP as protons flowback into the matrix
through its membrane-embedded F0 portion, the rotor of the
turbine.
The motors stator (called the F1 portion) pro-trudes into the
matrix and converts ADP and
mtDNA:mitochondrial DNA
PDHC: pyruvatedehydrogenasecomplex
nDNA: nuclear DN
inorganic phosphate (Pi) to ATP in a tripartite
series of catalytic reactions [three sets of/
dimeric subunits alter their conformations via
a rotating cam that connects Fo to F1 so asto bind ADP +Pi
first, then to convert ADP
and Pi to form ATP, and finally to release theATP into the
matrix, where it is exported from
the organelle into the cytoplasm via the adeninenucleotide
translocator (ANT)].
At this point, a brief reminder of the rules ofmitochondrial
genetics is de rigueur.
1. Heteroplasmy and threshold effect. Each
cell contains hundreds or thousands ofmtDNA copies, which, at
cell divi-
sion, distribute randomly among daugh-ter cells. In normal
tissues, all mtDNA
molecules are identical (homoplasmy).Deleterious mutations of
mtDNA usu-
ally affect some but not all mtDNAs (het-eroplasmy), and the
clinical expression of
a pathogenic mtDNA mutation is deter-mined largely by the
relative proportions
of normal and mutant genomes in dif-ferent tissues. A minimum
critical muta-tion load (typically above 80%90%) is
required to cause mitochondrial dysfunc-tion in a particular
organ or tissue and mi-
tochondrial disease in an individual: Thisis the threshold
effect.
2. Mitotic segregation. At cell division, theproportion of
mutant mtDNAs in daugh-ter cells may shift and the phenotype
may
change accordingly. This phenomenon,called mitotic segregation,
explains how
the clinical phenotype in patients withmtDNA-related disorders
may change as
patients grow older.3. Maternal inheritance. At fertilization,
all
mtDNA derives from the oocyte. There-
fore, themode of transmission of mtDNA
and of mtDNA point mutations (singledeletions of mtDNA are
usually sporadicevents) differs from Mendelian inheri-tance. A
mother carrying a mtDNA point
mutation will pass it on to all her children(males and females),
but only the daugh-
ters will transmit it to their progeny.Thus, a disease expressed
in both sexes
www.annualreviews.org Mitochondrial Disorders in the Nervous
System 93
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
4/35
HSP
LSP
D-Loop
T
P
E
Cyt b
ND5
ND6
ND4L
KSS
S
A
Q
OL
N
C
Y
ND4
ND3
ND2
ND1
L
V
12 S F
16 S
R
G
COX III
COX II
COX I
W
M
I
D
A6A8K
LS
H
Parkinsonism
LHONDystonia
LS, LHONDystonia
LS, LHON
LS
LSNARPMILSFBSN
MERRF
Epilepsy
Alpers-like
MNDEpilepsy
LS
MELAS
MELAS
OH
Figure 1
The human mitochondrial genome. The mtDNA-encoded gene products
for the 12S and 16S ribosomal RNAs, the subunits ofNADH-coenzyme Q
oxidoreductase (ND), cytochrome coxidase (COX), cytochrome b (Cyt
b), and ATP synthase (A), and 22 tRNA(1-letter amino acid
nomenclature) are shown, as are the origins of heavy- and
light-strand replication (OH and OL) and the promotof heavy- and
light-strand transcription (HSP and LSP). Some pathogenic mutations
(for expanded versions of all the key terms in tharticle, see
Supplemental Term List; follow the Supplemental Material linkfrom
the Annual Reviews home page athttp://www.annualreviews.org) that
affect the nervous system in particular are indicated (colors
correspond to those of the affected genes
butwithnoevidenceofpaternaltransmis-sion is strongly suggestive
of an mtDNApoint mutation.
About 200 mtDNA point mutations andinnumerable single
large-scale (kilobase-sized)
partial deletions have been associated with h
man diseases, most of which affect the centandperipheral nervous
system, especiallyif m
opathies are consideredas they shouldtdomain of peripheral
neurology. This conc
94 DiMauro Schon
Supplemental Material
http://arjournals.annualreviews.org/doi/suppl/10.1146/annurev.neuro.30.051606.094302http://arjournals.annualreviews.org/doi/suppl/10.1146/annurev.neuro.30.051606.094302
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
5/35
Succinate Fumarate
Diseases
Diseases
LHON
MELAS
LHON + dystonia
Leigh syndrome
Leighsyndrome
Leukodystrophy
Leighsyndrome
Encephalo-myopathy
Leighsyndrome
Cardioencephalo-myopathy
Leukodystrophy/tubulopathy
Fatal infantileencephalomyopathy
Leighsyndrome
Encephalo-myopathy
Nephrosis
NDUFA1
NDUFS1
NDUFS2
NDUFS3
NDUFS4
NDUFS6
NDUFS7
NDUFS8
NDUFV1
NDUFV2
NDUFA12L
SDHA
SDHB
SDHC
SDHD
7 0
4
1 3 2
~39
APTX
COQ2
PDSS1
PDSS2
BCS1L
UQCRB
COX10
COX15
LRPPRC
SCO1
SCO2
SURF1
ATPAF2
ND1 ND6
Encephalomyopathy
Cyt b
ALSlike syndrome
Encephalomyopathy
COX I COX III ATPase 6
NARP
MILS
FBSN
Mutated genes
Mutatedgenes
IMM
IMS
mtDNA-encoded subunits
nDNA-encoded subunits
Matrix
e
e ee
O2
e
H2O
ADP AT
Complex I Complex II Complex III Complex IV Complex V
COX ICOX II
COX III
A8
A6
ND1 ND2ND3
ND4Cyt b
ND6
ND5 ND4L CoQ
Cyt c
10 10 ~16
Figure 2The mitochondrial respiratory chain (RC), showing
nDNA-encoded subunits (blue) and mtDNA-encoded subunits (colors
correspondinto the genes in the map in Figure 1). Protons are
pumped from the matrix to the intermembrane space through complexes
I, III, and IVand are pumped back to the matrix through complex V
to produce ATP. Coenzyme Q and cytochrome care electron (e)
transfercarriers. Diseases (see Supplemental Term List) caused by
mutations in mtDNA (above the RC) and in nDNA (below the RC)
arelisted according to the correspondingly affected RC complex.
Genes in bold encode RC subunits; those in plain text encode
ancillary assembly proteins.
is illustrated in Figure 1 and, in more de-tail, in Table 2,
which highlights the typical
clinical features of the five most commonmtDNA-related syndromes
of neurological in-
terest.Thesearenotdescribedhere in anymoredetail because the
features can be found in text-
book reviews (Hays et al. 2006, Hirano et al.2006a).
The human mitochondrial genome is satu-rated with mutations.
Does this mean that weare scraping the bottom of the barrel as
far
as our understanding of mtDNA-related dis-eases is concerned?
Not by a long stretch. Al-
though, understandably, the pace at which newpathogenic
mutations are discovered has slack-
ened in recent years, novel mutations are stillbeing reported,
and several questions still awaitanswers in the field of
mitochondrial genetics.
For example, whereas mostpathogenicmtDNAmutations are
heteroplasmic and clinical sever-
ity is usually relatedto mutation load, some mu-tations are
homoplasmic, and yet the severity
www.annualreviews.org Mitochondrial Disorders in the Nervous
System 95
Supplementa
http://arjournals.annualreviews.org/doi/suppl/10.1146/annurev.neuro.30.051606.094302http://arjournals.annualreviews.org/doi/suppl/10.1146/annurev.neuro.30.051606.094302
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
6/35
Table 2 Clinical features in diseases associated with mtDNA
mutations
-mtDNA tRNA ATPase6
TISSUE SYMPTOM/SIGN KSS MERRF MELAS NARP M
of the syndromes they cause differs in different
families or even in members of the same fam-ily. A related
question concerns the functionalsignificance of mtDNA haplotypes.
In the mi-
gration out of Africa, human beings have accu-mulated
distinctive variationson the mtDNA of
the ancestral mitochondrial Eve, resulting inseveral haplotypes
characteristic of different
ethnic groups (Wallace et al. 1999). Differ-ent mtDNA haplotypes
may modulate oxida-
tive phosphorylation, thus influencingthe over-all physiology of
individuals and predisposing
them toor protecting them fromcertaindiseases (Carelli et al.
2006). Clearly, much
work remains to be done to define better boththe pathogenic role
of homoplasmic mutations
and the modulatory role of haplotypes in hea
and disease.A major problem in mtDNA-related neu
logical diseases is our woeful ignorance abo
genotype-phenotype correlations. In fact, isurprising that mtDNA
mutations should ca
different syndromes in the first place. If,conventional wisdom
dictates, both large-sc
mtDNA rearrangements and point mutatioin rRNA or tRNA genes
impair mitochondr
protein synthesis and ATP production, it wobe logical to expect
a clinical swamp of
defined andoverlapping symptoms andsignsoriginally predicted by
the lumpers (Rowla
1994). Although clinical overlap does occurmtDNA-related
diseases, it is fair to say th
96 DiMauro Schon
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
7/35
the splitters won the day, in that most muta-
tions result in well-defined syndromes, includ-ing mutations
associated with KSS/PEO, DAD,
MERRF, MELAS, NARP/MILS, LHON, andSNHL.
To explain the distinctive brain symp-toms in patients with KSS,
MERRF, and
MELAS, the different mutations have beenmapped indirectly
through immunohisto-
chemical techniques. Consistent with clin-ical symptoms and
laboratory data, im-munohistochemical evidence suggests that
the
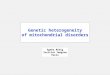
mtDNA deletion (-mtDNA) of KSS aboundsin the choroid plexus
(Tanji et al. 2000)
(Figure 3ad), the 3243-MELAS mutationis abundant in the walls of
cerebral arteri-
oles (Betts et al. 2006) (Figure 3ef), andthe 8344-MERRF
mutation is abundant in
the olivary nucleus of the cerebellum (Tanjiet al. 2001) (Figure
3gj). Direct evidence
of the accumulation of -mtDNA in thechoroid plexus of KSS
patients was provided
by Tanji et al. (2000) using in situ hybridization(Figure 4).
However, these data fail to explain
what directs each mutation to a particular areaof the brain, how
the mutation correlates withthe clinical syndrome, or why the
syndromes
differ from each other. That mutations in different tRNA
genes
may have different mechanisms of action is sug-gested by the
apparently selective tissue vul-
nerability associated with mutations in sometRNAs: For example,
cardiomyopathy is often
associated with mutations in tRNAIle, diabetesis a frequent
manifestation of theT14709C mu-
tation in tRNAGlu, and multiple lipomas havebeen reported only
in patients with mutations
in tRNALys. However these are mere associa-tions,not
explanations. It is fair to conclude that
the pathogenesis of mtDNA-related disordersis still largely
unexplained.
Disorders Caused by Mutationsin nDNA
During the many millennia of symbiotic re-
lation with the nDNA, the mtDNA has lostmore than 99% of its
original genes and most
a b
c d
e f
g h
i j
COX II
Control
KSS
Control
MERRF
MELAS
FES
Figure 3
Immunohistochemistry to detect the mtDNA-encoded COX II subunit
ofcomplex IV (left panels) and the nDNA-encoded FeS subunit of
complex III(right panels) in brain structures in three
mtDNA-related diseases. Choroidplexus from a control (A, B) and a
KSS patient (C, D). Sub-pial arterioles froa MELAS patient (E, F).
Olivary nucleus from a control (G, H) and a MERRpatient (I, J).
Courtesy of Drs. Eduardo Bonilla and Kurenai Tanji,
ColumbiaUniversity Medical Center.
www.annualreviews.org Mitochondrial Disorders in the Nervous
System 97
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
8/35
Probe 1
Probe 1
wt-mtDNA
Normal
KSS
-mtDNA Deletion
Probe 2
Probe 2
a
b
Figure 4
In-situ hybridization to detect mtDNAs in the choroid plexus
from a KSSpatient. (a) Map of wt- and -mtDNAs from the patient
showing the twoprobes: Probe 1 (red) detects both wt- and -mtDNAs;
probe 2 (blue) detectsonly wt-mtDNA. (b) As opposed to the uniform
signal with both probes in thecontrol (upper panels), there is a
much stronger signal in the patient with probe1 than with probe 2
(lower panels), indicating a massive accumulation of-mtDNAs.
Courtesy of Drs. Eduardo Bonilla and Kurenai Tanji,
ColumbiaUniversity Medical Center.
of its autonomy, and it now depends on
nuclearfactorsforallitsbasicfunctions,includingrepli-
cation, translation, synthesis of most respira-tory chain
subunits, and assembly of respira-
tory chain complexes, and for the synthesisof the phospholipids
that constitute the inner
mitochondrial membrane (IMM). This is whythe Mendelian defects
of the respiratory chain
can be divided into at least four subgrou
(Table 1).
Mutations in genes encoding respirat
chain subunits. These mutations (direct hhave been found
predominantly in the first t
complexes of the respiratory chain, sugge
ing that deleterious mutations in the termincomplexes are either
rare or incompatible w
life. One explanation suggests that complexeand II are in
parallel, allowing for some res
ual electron transport even when one compis out of commission,
whereas complexes I
IV, and V are in series (Figure 2). Althoudirect hits do occur
in the mtDNA-encod
subunits of complexes III (cytochrome b), (COX I, II, or III),
and V (ATPase 6), the h
eroplasmic nature of these mutations may p
mit some residual activity. However, the ries/parallel
hypothesis has been undercutthe finding of a homozygous frameshift
mu
tion in the ubiquinone-binding subunit of coplex III UQCRB (Haut
et al. 2003), which is
cated at the C-terminus of the protein and sallows for some
residual complex III activiIt is more difficult to explain why
severe CO
deficiency with recessive mutations in assemproteins (for
example SCO2) is still compati
with life, albeit a very abbreviated life.
Most mutations in nDNA-encoded coplex I or in complex II
subunits cause Leisyndrome (LS) (Table 3). The hallm
neuropathological lesions of this devastatneurodegenerative
disorder of infancy or ea
Table 3 Causes of Leigh syndromea
Defect Transmission Frequency
Complex I AR, M +++
Complex II AR +
Complex IV AR +++
Complex V M ++tRNALeu(UUR) M +
tRNALys M +
CoQ10 AR +
PDHC XR, AR +++
aAbbreviations: AR, autosomal recessive; M, maternal;
X, X-linked.
98 DiMauro Schon
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
9/35
ba
Figure 5
Typical brain lesionsLeigh syndrome.(a) Coronal sectionshowing
bilateral
symmetrical cavitatinlesions in the basalganglia (arrows).(b)
T2-weighted MRshowing abnormalbilateral symmetricahyperintense
signalsthe lenticular nuclei(arrowheads).
childhood [bilaterally symmetrical foci of cys-tic cavitation
(Figure 5), vascular proliferation,
neuronal loss, and demyelination in the basal
ganglia, brainstem, and posterior columns ofthe spinal cord]
probably reflect the stereo-typical ravages caused by defective
oxidative
metabolism on the developing nervous system.This concept is
supported by the observationthat LS is also caused by mtDNA
mutations
when they are sufficiently abundant (MILS;Table 2) or severe
enough to impair oxidative
phosphorylation early in life (Kirby et al. 2003,Sarzi et al.
2007, Tatuch et al. 1992).
Although some mutations in mtDNA com-
plex I genes cause LS, most do not, butrather cause Leber
hereditary optic neuropathy(LHON), a maternally inherited optic
atrophy
that causes blindness in young adults with chal-lenging
contradictions. First, all pathogenic
LHON mutations are in complex I genes, and yet the complex I
deficiency is not particu-
larly severe. Second, whereas some LHONmutations are
heteroplasmic (as in most mi-
tochondrial diseases), most are homoplasmic,and yet the
pathology is confined, on the
whole, to the retinal ganglion cells (Carelliet al. 2007).
Third, even though the mu-tation is often homoplasmic, the
blindness
usually does not occur until the patient isolder than age 20,
and then each eye is af-
fected sequentially within months. Fourth, al-though LHON is
maternally inherited, men
KSS: Kearns-Sayresyndrome
PEO: progressiveexternalophthalmoplegia
MERRF: Myoclonuepilepsy ragged-redfibers
MELAS:mitochondrialencephalomyopathy,lactic acidosis,
andstrokelike episodes
NARP: Neuropathyataxia, retinitispigmentosa
LS: Leigh syndromMILS: Maternallyinherited Leighsyndrome
LHON: Leberhereditary opticneuropathy
are affected far more frequently, and moreseverely, than are
women, implying an X-linked
modifier effect (Hudson et al. 2005). Also,
rarely, the blindness is partially reversible.
Mutations in genes encoding ancillary pro-
teins. This group of disorders is caused by in-direct hits, that
is, mutations in proteins that
are not part of any complex but are neededto synthesize and
direct the proper assembly
of the various nDNA- and mtDNA-encodedsubunits, together with
their prosthetic groups.
Important clues to the molecular etiology of
these disorders, and especially COX deficiency,came from yeast
genetics because most genesneeded for COX assembly in yeast have
hu-
man homologues. Another shortcut to find-ing mutant genes
without sequencing multiple
candidate COX-assembly genes was the searchfor complementation
in COX-deficient cul-
turedcells from patients via monochromosomalhybrid fusion or
microcell-mediated chromo-
some transfer, which led to the identification ofthe most common
gene responsible for COX-
deficient LS, SURF1 (Tiranti et al. 1998, Zhuet al. 1998).
Integrative genomics, on the basisof information derived from DNA,
mRNA, and
proteomics studies, led to the identification ofLRPPRC, the gene
responsible for LS-French-
Canadian type (LSFC), another COX-deficientform of LS associated
with liver diseases and
www.annualreviews.org Mitochondrial Disorders in the Nervous
System 99
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
10/35
prevalent in the Saguenay-Lac Saint-Jean re-
gionof Quebec (Mootha et al. 2003, Morin etal.1993). A
bioinformatics approach was also used
to identify the first mutant assembly gene re-sponsible for
complex I deficiency,NDUFA12L
(formerly called B17.2L), in a child with severecavitating
leukoencephalopathy (Ogilvie et al.
2005). Knowledge of the molecular defects inthese fatal
infantile neurological disorders of-
fers young parents who have lost one child theoption of prenatal
diagnosis.
Primary coenzyme Q10 (CoQ10) deficiency
encompasses disorders caused by blocks in thebiosynthetic
pathway of this small ubiquinone
carrier. CoQ10 transfers electrons from com-plexes I and II to
complex III and receives
electrons from the -oxidation pathway
the electron transfer flavoprotein dehydrognase (ETF-DH) (Figure
6). Mutations in t
CoQ10 biosynthetic enzymes (in the PDSand PDSS2 subunits of of
COQ1, and
COQ2) have been identified in infants or chdren with
encephalomyopathy (one of them h
LS)and nephrotic syndrome (Lopez et al. 20Mollet et al. 2007,
Quinzii et al. 2006). Becau
at least nine enzymes are needed to synthsize CoQ10, mutations
in the other seven ezymes will probably also be associated with
e
cephalomyopathic syndromes (DiMauro et2007). Several syndromes
have also been
sociated with a presumed secondary CoQdeficiency. These include
autosomal recess
Pyruvate
PDHC
Acetyl-CoA -oxidation
Fatty acids
Krebs cycle
OMM
IMS
IMM
Matrix
ND1 ND2
ND4Cyt b
COX ICOX II
COX III
A8ND6
ND5 ND4L CoQ
Cyt c
A6
ND3
SDH
ETF-DH
ETF
Figure 6
Schematic of mitochondrial intermediate metabolism showing the
relationships between pyruvate and fatty acid metabolism and
ATsynthesis. Note that the electron-transfer flavoprotein (ETF)
delivers electrons from the -oxidation pathway to CoQ10 via
theETF-dehydrogenase (ETF-DH).
100 DiMauro Schon
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
11/35
cerebellar ataxia of unknown etiology in chil-
dren, the syndrome of ataxia and oculomo-tor apraxia (AOA1)
caused by mutations in the
aprataxin gene (APTX) (Quinzii et al. 2005),and a predominantly
myopathic form of glu-
taric aciduria type II (GAII) caused by muta-tions in the
electron transfer flavoprotein dehy-
drogenase gene (ETFDH) (Gempel et al. 2007)(Figure 6). Aside
from its scientificimportance,
knowledge of CoQ10 deficiency syndromes isimportant for
physicians because most patientsimprove with CoQ10
supplementation.
The other respiratory complexes obviouslyalso require assembly,
and mutations in assem-
bly factor BCS1L for complex III (Visapaa et al.2002) and ATPAF2
for complex V (De Meirleir
et al. 2004) have also been found. Clearly, thepool of available
candidate genes has yet to be
exhausted (DiMauro & Hirano 2005).
Defects of intergenomic communication.
The alterations of mtDNA of some disor-
ders are not caused by primary mutations ofthe mitochondrial
genome, but rather are theresult of garbled messages from the
nuclear
genome, which controls mtDNA replication,
maintenance, and translation. The resultingMendelian disorders
are characterized by qual-
itative (multiple deletions) or quantitative (de-pletion)
alterations of mtDNA, or by defec-
tive translation of mtDNA-encoded respiratorychain components.
Of note, most of these dis-
orders are caused by alterations in the pools ofnucleotides
required to synthesize mtDNA, orin enzymes associated with mtDNA
replication
itself (Spinazzola & Zeviani 2005) (Figure 7).
Multiple mtDNA deletions. From the clini-cal point of view,
multiple mtDNA deletion
syndromes share the cardinal features of oc-ular and limb
myopathy (PEO, ptosis, prox-
imal weakness), which are almost invariablyassociated with
extramuscular system involve-
ment, including peripheral nerves (sensorimo-tor neuropathy),
the brain (ataxia, dementia,
psychosis), the ear (sensorineural hearing loss),and the eye
(cataracts). Mutations in sev-eral genes, all involved in the
homeostasis of
the mitochondrial nucleotide pools, have beenassociated with PEO
and multiple mtDNA
dA dAMPdGMP
dADPdGDP
dATP
mtDNA
PEO1,
POLG,
POLG2
NME4, NME6
SUCLA2, SUCLG1AK2, UCK
dGTPDGUOK
dG
dC dCMPdTMP
dCDPdTDP
dCTPdTTP
ADP
ATPdNTPdNDPrNDP
TK2
RRM2B
ANT1
NT5MdT
IMM
OMM
IMS
dAdG
ETN1
Thymine
dCdT
TP
Figure 7
Schematic of nucleotide metabolism for mtDNA synthesis and
replication. Genes in bold have been associated with
diseasescharacterized by multiple mtDNA deletions and/or with mtDNA
depletion.
www.annualreviews.org Mitochondrial Disorders in the Nervous
System 101
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
12/35
MNGIE:mitochondrialneurogastrointestinalencephalomyopathy
deletions. These include ANT1, which en-
codes the adenosine nucleoside translocator;PEO1, which encodes
a helicase called Twinkle;
ECGF1, which encodes the cytosolic enzymethymidine phosphorylase
(TP); POLG, which
encodes the mitochondrial polymerase cat-alytic subunit; and
POLG2, which encodes the
dimeric accessory subunit of POLG (Spinaz-zola & Zeviani
2005). Two of these disorders
are of special interest to neurologists.The first is MNGIE
(mitochondrial neuro-
gastrointestinal encephalomyopathy), an auto-
somal recessive multisystem disease of youngadults caused by
mutations in TP (Nishino
et al. 1999) andcharacterized clinically by PEO,neuropathy,
leukoencephalopathy, and intesti-
nal dysmotility leading to cachexia and earlydeath. Thelack of
TP activity damages mtDNA
synthesis, causing not only multiple deletions,but also
depletion and point mutations, which
are evident in skeletal muscle, although mus-cle expresses
little TP (Hirano et al. 2005).
This muscle paradox suggests that TP defi-ciency acts through
toxic intermediates. Two
such toxic intermediates, thymidine and de-oxyuridine,
accumulate massively in the bloodof MNGIE patients. Hemodialysis,
an obvious
therapeutic approach, has only transient effects,as do platelet
infusions, but allogeneic bone
marrow transplantation in one patient restoredTP activity in
buffy coat cells and normalized
blood levels of thymidine and deoxyuridine. Al-thoughthe patient
hasimproved subjectively 18
months after the procedure, clinical efficacy re-mains to be
firmly documented (Hirano et al.
2006b).Disorders associated with mutations in
POLG are inherited as either autosomal-recessive or
autosomal-dominant traits. Both
forms of inheritance are encountered in adults
with PEO and multiple mtDNA deletions:Clinical manifestations
include ataxia, periph-eral neuropathy, parkinsonism, psychiatric
dis-orders, myoclonus epilepsy, and gastrointesti-
nal symptoms (DiMauro et al. 2006a). Autoso-mal recessive
inheritance of mutations in POLG
is the rule in children with Alpers syndrome,a severe
hepatocerebral disease associated with
mtDNA depletion and extreme vulnerability
valproate administration (Naviaux & Nguy2004). This clinical
heterogeneity can, at le
in part, be attributed to the site of the mution in the
catalytic subunit, which has a po
merase (i.e., replicating) domain and an exonclease (i.e.,
proofreading) domain joined b
linker region: Most patients with Alpers sydrome have at least
one mutation in the linregion and another in the polymerase
doma
whereas adults with PEO tend to have mutions solely in the
polymerase domain. To co
plicate matters further, mutations in the dimeaccessory subunit
POLG2,which is responsi
for processive DNA synthesis and tight bining of the POLG
complex to DNA, can a
cause autosomal dominant PEO (Longley et2006).
Depletion of mtDNA. We have seen h
some mutations in POLG predominantly camtDNA depletion and
result in a severe infatile hepatocerebral disorder (Alpers
syndrom
In fact, mutations in other proteins contrling the mitochondrial
nucleotide pool a
cause mtDNA depletion. For reasons that not completely clear,
the degree of depleti
varies in different tissues, but two major sydromes have
emerged: (a) hepatocerebral sy
drome, caused by mutation either in POLGin DGUOK, which encodes
the enzyme d
oxyguanosine kinase (dGK); and (b) a puror predominantly
myopathic syndrome asso
ated with mutations in TK2, which encodes tmitochondrial form of
the enzyme thymid
kinase, with mutations in SUCLA2, encodthe subunit of the
mitochondrial matrix e
zyme succinyl-CoA synthetase (Elpeleg et2005), and with
mutations in RRM2B, encoing the cytosolic p53-inducible
ribonucleot
reductase small subunit (p53R2) (Bourdon et2007). However, not
all cases of mtDNA d
pletion are explained by mutations in thfour genes, and not all
mutated genes are
volved in nucleotide pool homeostasis. For ample, some children
with hepatocerebral sy
drome harbored pathogenic mutations in a geon chromosome 2,
MPV17, which encodes
102 DiMauro Schon
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
13/35
IMM protein of unknown function (Spinazzola
et al. 2006). The importance of this gene wasbolstered by the
finding that the same homozy-
gous mutation encountered in a southern
Ital-ianfamilyisthecauseofadiseaseendemicinthe
Navajo population of the American southwest(Karadimas et al.
2006). The disease is called
Navajo neurohepatopathy (NNH) to stress thatneuropathy rather
than encephalopathy accom-
panies the liver dysfunction in this condition,probably because
of some as-yet-unknown ge-netic modifier. We can now provide sound
ge-
netic counseling to the Navajo population inthe hopes of
eradicating this dreadful disease.
Defects of mtDNA translation. Faithful trans-
lation of the 13 mtDNA-encoded subunits ofthe respiratory chain
requires not only intact
mtDNA, a trustworthy polymerase, and theavailability of
nucleotide building blocks, but
also ribosomal proteins, RNA modificationenzymes, and
initiation, elongation, and termi-
nation factors, all encoded by nDNA. Defectsin mtDNA translation
result in severe com-
bined respiratory chain complex defects, and itis important to
think of this pathogenic mecha-nism in infants or children with
hepatocerebral
syndrome, encephalopathy, infantile
cavitatingleukoencephalopathy, or cardiomyopathy and
otherwise unexplained multiple respiratorychain defects. Thus
far, investigators have
described mutations in four genes, but thisnumber will certainly
increase in the years
to come. The first gene, GFM1, encodes oneof four ribosomal
elongation factors (Coenen
et al. 2004, Valente et al. 2007); the second,MRPS16, encodes
the mitochondrial riboso-
mal protein subunit 16 (Miller et al. 2004);the third, TSFM,
encodes the mitochondrial
elongation factor EFTs (Smeitink et al. 2006);
and the fourth gene, TUFM, encodes theelongation factor Tu
(Valente et al. 2007). Adifferent syndrome is caused by defective
pseu-douridylation of mitochondrial tRNAs and is
characterized by myopathy, lactic acidosis, andsideroblastic
anemia (MLASA): Mutations in
this gene, PUS1, which encodes the mitochon-drial enzyme
pseudouridine synthase 1, have
been identified in three families (Bykhovskaya
et al. 2004, Fernandez-Vizarra et al. 2006).
Mutations affecting the lipid milieu of the
respiratory chain. The complexes of the res-
piratory chain are embedded in the lipid milieuof the IMM, whose
major component is cardi-
olipin, an acidic phospholipid. Cardiolipin doesnot have merely
a scaffolding function, but alsoparticipates in the formation of
supercomplexes
(stoichiometric assemblies of individual respi-ratory chain
complexes into functional units)
(Zhang et al. 2005b) and interacts directly withCOX(Sedlak et
al. 2006); conversely, intact res-
piratory chain function is essential for cardi-olipin
biosynthesis (Gohil et al. 2004). There-
fore, genetic abnormalities of cardiolipin couldimpair
respiratory chain function in humans.
The best candidate for this role is Barth syn-drome, an X-linked
recessive disorder charac-
terized by mitochondrial myopathy, cardiomy-opathy, and growth
retardation, and caused by
mutations in the gene encoding a phospholipidacyltransferase
called tafazzin (TAZ) (Schlame& Ren 2006). Tafazzin promotes
structural uni-
formity and molecular symmetry among cardi-olipin molecular
species, and mutations in TAZ
alter the concentration and composition of car-diolipin, leading
to altered mitochondrial ar-
chitecture and function. Some TAZmutationscause mislocalization
of cardiolipin from the
outer mitochondrial membrane (OMM) andIMM to the mitochondrial
matrix (Claypool
et al. 2006).
DISEASES CAUSED BYIMPAIRED MITOCHONDRIALPROTEIN IMPORT
Of the 1300+ proteins found in mammalian
mitochondria (Schon 2007), only 13 areencoded by mtDNA. All
others are encodedby nDNA genes, synthesized in the cytoplasm,
and imported into the organelle. Mitochon-drial import is a
complex process, with differentpathways for protein targeting and
sorting to
each of the four mitochondrial compartments(OMM, IMM, IMS, and
the matrix enveloped
www.annualreviews.org Mitochondrial Disorders in the Nervous
System 103
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
14/35
HSP: hereditaryspastic paraplegia
SPG: spasticparaplegia
by the IMM). Among the components of the
import machinery, composed of nearly 60polypeptides, are members
of the heat shock
protein (HSP) family, chaperones needed forthe unfolding and
refolding of mitochondrially
targeted proteins as they transit throughthe import receptors
and are directed to the
appropriate compartment. Most, but notall, mitochondrial
proteins (especially those
destined for the IMM and the matrix) havewell-defined targeting
signals, usually locatedat the N-terminus of the protein. Once
inside
the mitochondrion, the mitochondrial target-ing signal (MTS, or
leader peptide) is cleaved
to release the mature protein. The importmachinery consists of
polymeric translocases
in the outer membrane (TOM) or the innermembrane (TIM). In
collaboration with a
sorting and assembly machinery (SAM), apresequence
translocation-associated motor
(PAM), and a mitochondrial import and assem-bly (MIA) pathway
specific for a subset of IMS
proteins (Gabriel et al. 2006), TOM and TIMsort out incoming
polypeptides to the proper
compartments (Chacinska & Rehling 2004).Although a few
mutations in leader peptides
have been associated with specific enzyme de-
fects, such as methylmalonic acidemia (Ledleyet al. 1990) and
PDHC deficiency (Takakubo
et al. 1995), remarkably few human diseaseshave been attributed
to genetic defects of the
general importation machinery. One of theseis an X-linked
recessive deafness-dystonia syn-
drome (Mohr-Tranebjaerg syndrome) causedby mutations in the gene
(TIMM8A) encoding
the deafness/dystonia protein (DDP), an MIApathway protein
located in the IMS (Roesch
et al. 2002). Another is an autosomal dom-inant form of
hereditary spastic paraplegia
(HSP type 13; SPG13) caused by mutations in
the import chaperonin HSP60 (Hansen et al.2002).Unless most
disorders caused by disruption
of the general importation machinery are in-
compatible with life, as suggested by Fenton(1995), we can
expect more such disorders to
be identified in the near future.
DISEASES CAUSED BY ABERRANMITOCHONDRIAL DYNAMICSThis relatively
new area of interest for cli
cal neuroscientists has already yielded instrutive results and
is sure to provide many mo
in the coming years. Remembering their bacrial origin,
mitochondria move, fuse, and div
within cells, where they often form tubular nworks that may
favor the delivery of organel
to areas of high energy demand (Bossy-Wetet al. 2003). The need
for mitochondrial mo
ity is nowhere more evident than in motor nrons of the anterior
horn cells, where mi
chondria must travel a huge distance from tcell soma to the
neuromuscular junction. Michondria travel on microtubular rails,
propel
by motor proteins, usually GTPases, called nesins (when
mitochondria travel downstrea
or dyneins (when they travel upstream). Tfirst mitochondrial
motility defect was iden
fiedin a family with autosomaldominant hereitary spastic
paraplegia type 10 (SPG10) a
mutations in a gene encoding one of the nesins (KIF5A): The
mutation affects a regi
of the protein involved in microtubule bindi(Fichera et al.
2004) (Figure 8).
In yeast, at least four proteins are requirfor mitochondrial
fission: Dnm1p (dynam
related protein), Fis1p (fission-related prote
Mdv1p (mitochondrial division protein), aCaf4p (carbon
catabolite repression-associa
factor). Of the four, only Fis1p is an integpart of
mitochondria, located in theouter me
brane. Upon a signal to divide, Fis1p recruDnm1p to the
organelle via the bridge protei
Mdv1p and Caf4p; Dnm1p then forms an evtightening spiral collar
around the organe
which severs the mitochondrion by stranglation (Chan 2006). For
the opposite proc
of mitochondrial fusion, two proteins are
quired in yeast: Fzo1p (the yeast homologthe Drosophila fuzzy
onion protein) and Ugo(ugo is Japanese for fusion). For fission to
o
cur, the OMM and IMM must establish cotact sites, apparently
through the action of
another protein called Mgm1p (mitochondrgenome maintenance
protein 1).
104 DiMauro Schon
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
15/35
AtlastinSPG3A
SpastinSPG4
SpastinSPG4
Dynein/dynactin
DYNCL1LI2
HAP1
Kinesins
Milton
MFN1 MFN2
CMT6CMT2A
Miro
HTTHD
DNCH1
DISC1SCZD KIF5A
SPG10SynucleinFPD
PARKINFPD
LRRK2FPD
PINK1FPD
DJ-1FPD
HSPD1SPG13
HTRA2FPD
GDAP1CMT4A
Para-pleginSPG7
OPA1(large)DOA
YWHAEMDS
NUDEL
YWHAZ
AFG3L1AFG3L2
PARLOPA1(small)DOA
IMM
Microtubule
Cytosol
OMM
IMS
Matrix
Figure 8
Selected genes associated with mitochondrial dynamics. Genes
boxed in yellow have been associated with neurodegenerative
orpsychiatric diseases (disease abbreviations in red).
Mitochondrially targeted gene products are in bold. Black dots
denote reportedinteractions between proteins.
Mutations in the human orthologs ofMgm1p (OPA1) and Fzo1p (MFN2
or mito-
fusin 2) have been associated with human dis-eases. Mutations in
OPA1 cause autosomal
dominant optic atrophy (DOA), the Mendeliancounterpart, as it
were, of LHON and are char-
acterized by maldistribution of mitochondriain affected cells
(Alexander et al. 2000, Delet-tre et al. 2000). Notably, OPA1
interacts with
mitofusin1(MFN1)topromotefusion(Cipolatet al. 2004). However,
beyond its role in fusion,
OPA1, an IMM protein, is also required for re-modeling the
cristae (Cipolat et al. 2006) to-
gether with PARL (presenilin-associated rhom-boid like), an
IMS-localized protein (Pellegrini
& Scorrano 2007). Mutations in the second mitofusin
gene,
MFN2, cause an autosomal dominant axonalvariant of
Charcot-Marie-Tooth disease (CMT
type 2A) (Lawson et al. 2005, Zuchner et al.2004). A recent
review of 62 unrelated axonal
CMT families revealed MFN2 mutations in 26patients from 15
families, which suggests that
this is a major cause of axonal CMT2A (Chung
CMT: Charcot-MaTooth
et al. 2006). In addition, mutations in GDAP1,the gene encoding
ganglioside-induced differ-
entiation protein 1, which is located in theOMM and which
regulates the mitochondrial
network (Niemann et al. 2005), cause CMTtype 4A, an autosomal
recessive, severe, early-
onset form of either demyelinating or axonalneuropathy (Pedrola
et al. 2005) (Figure 8).
A remarkable example of the underlying
connections between mitochondrial movementand ostensibly
disparate diseases is Charcot-
Marie-Tooth disease type 6 (CMT6), which ischaracterized by the
coexistence of peripheral
neuropathy and optic atrophy. Moreover, op-tic atrophy onset is
followed in many patients
by slow vision recovery, as sometimes seen inLHON patients.
Suchner et al. (2006a) found
mutations in MFN2 in affected members of sixunrelated families
with CMT6; one of them
had a missense mutation (R94W) identical tothat in some patients
with CMT2A. An un-
derlying problem in mitochondrial movementpresumably causes both
peripheral and optic
neuropathy, even though most patients with
www.annualreviews.org Mitochondrial Disorders in the Nervous
System 105
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
16/35
MFN2 mutations do not have optic atrophy,
and most patients with OPA1 mutations do nothave CMT. The
patients nuclear background
may influence the penetrance of the mitochon-drial trafficking
defect.
Because mitochondria are not the only car-goes to be moved
around the cell, it is not
too surprising that mutations in genes con-trolling
mitochondrial motility may also affect
other organelles. Both mitochondria and per-oxisomes had
abnormal size, shape, and distri-bution in fibroblasts from an
infant with a syn-
drome of encephalopathy, optic atrophy, lacticacidosis, and a
heterozygous dominant muta-
tion in the human ortholog of yeast Dnm1pcalleddynamin-like or
dynamin-relatedprotein
1 (DLP1/DRP1; gene DNM1L) (Waterhamet al. 2007).
A mitochondrial import defect may berelated to impaired neuronal
migration
(Figure 8). Two neuronal migration disorders,isolated
lissencephaly sequence (ILS) and
the Miller-Dieker syndrome (MDS), areassociated with deletions
on chromosome
17p13.3. Mutations in LIS1 (gene PAFAH1B1)cause ILS, whereas a
second gene at thislocus, encoding the 14-3-3 protein isoform
(YWHAE), is invariably deleted in patients with MDS
lissencephaly (Toyo-oka et al. 2003).
YWHAE is a cytoplasmic chaperone thattargets precursor proteins
to the mitochondria,
which is why it is also called the mitochondrialimport
stimulating factor subunit L (MSFL)
(Alam et al. 1994). YWHAE interacts withthree other proteins
that not only are required
for neuronal migration but also are known toassociate with
mitochondria: NUDEL (nuclear
distribution protein nudE-like 1) (Brandonet al. 2005, Ikuta et
al. 2007), FEZ1 (fascicula-
tion and elongation protein zeta-1) (Ikuta et al.
2007), and DISC1 (deleted in schizophrenia 1)(Millar et al.
2005). NUDEL targets dynein tomicrotubule ends through LIS1 (Li et
al. 2005),whereas altered expression of both FEZ1 and
DISC1 caused mitochondrial morphologyand mobility defects (Ikuta
et al. 2007, Millar
et al. 2005). In yeast, the homolog of humanYWHAE (Bmh1p;
14-3-3) interacts with
the homolog of human YWHAZ (Bmh
14-3-3) (Chaudhri et al. 2003); YWHAZin fact, present in
mitochondria (Schind
et al. 2006, Taylor et al. 2003). Thus, lossYWHAE may well
affect neuronal migrati
either by disrupting the trafficking of these lter proteins to
mitochondria or by interdicti
the binding of mitochondria to dynein.These diseases are only
the proverbial tip
what will be found to be an iceberg of hum
neurodegenerative disorders directly or inrectly linked to
abnormal mitochondrial mo
ity, fusion, or fission (Table 4).
AGING AND LATE-ONSETNEURODEGENERATIVEDISORDERS
In the title of a 1992 News & Viewsarticle Nature Genetics,
the late Anita Harding posi
the role of mitochondria in normal aging wher usual wit: Growing
Old: The Most Co
mon Mitochondrial Disease of All? (Hardi1992). Her comments
concernedan article d
umenting the age-related accumulation of common 4977-bp mtDNA
deletion (Sch
et al. 1989) in human brain, but especiain the caudate, putamen,
and substantia nig(Soong et al. 1992). Last year, using more
phisticated techniques (laser microdissectiosingle-molecule PCR,
long-range PCR), t
groups confirmed the age-related accumution of somatic and
clonal mtDNA deletio
in substantia nigra and showed that neurowith high mutation
loads were COX-negat
(Bender et al. 2006, Kraytsberg et al. 200These findings are
consistent with the alm
40-year-old mitochondrial theory of agin(Harman 1972), which
postulates a vicious
cle whereby somatic mtDNA mutations [p
dominantly deletions (Pallotti et al. 1996)] gerate excessive
reactive oxygen species (ROand these, in turn, further damage mtDN
The main objection to this hypothesis ca
from clinical experience because the mution loads recorded in
most postmitotic t
sues during normal aging are at least oorder of magnitude lower
than those fou
106 DiMauro Schon
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
17/35
Table 4 Diseases associated with defects in mitochondrial
dynamicsa
Disease Gene Protein
Dominant optic atrophy (DOA) OPA1 Dynamin-related GTPase
CMT type 2A MFN2 Mitofusin 2
CMT type 4A GDAP1 Ganglioside-induced differentiation protein
1
CMT type 6 MFN2 Mitofusin 2
AD-HDP type 3A SPG3A Atlastin (associated with spastin)
AD-HSP type 4 SPAST Spastin (microtubule severing protein)
AR-HSP type 7 SPG7 Paraplegin (AAA protease)
AD-HSP type 10 KIF5A Kinesin heavy chain
AR-HSP type 20 SPG20 Spartin (microtubule-interacting
protein?)
AD-HSP type 31 REEP1 Receptor expression-enhancing protein
Infantile microcephaly DNM1L Dynamin-related protein DLP1
Huntington disease HD Huntingtin (binds HAP1)
Lissencephaly (Miller-Dieker) YWHAE 14-3-3 protein
aGenes encoding mitochondrially targeted proteins are in
bold.
in patients with primary pathogenic mtDNAdeletions (e.g., KSS;
Table 2). However, theproportion of-mtDNA measured in single
neurons of the substantia nigra from aged nor-mal individuals
approaches or surpasses the es-timated pathogenic threshold (Bender
et al.
2006, Kraytsberg et al. 2006), although neu-rons from patients
with Parkinson disease do
not contain significantly more-mtDNAs thandid age-matched
controls (Bender et al. 2006).
The observation that many of these neurons are
functionally impaired (COX-negative) makesconceivable the second
step in the vicious cy-cle: excessive ROS generation. Although
the
mitochondrial theory of aging in and by it-self does not explain
either natural aging or
late-onset neurodegenerative diseases, it almostcertainly plays
a role in both conditions, to-
gether with nuclear genetic factors. A dra-matic example of the
importance (but not nec-essarily the functional significance) of
nuclear
factors is the precocious, in fact precipitous,
aging of transgenic mice that express aproofreading-deficient
POLG (Khrapko et al.2006, Kujoth et al. 2005, Trifunovic et al.
2004).The role of nuclear-encoded mitochondrial
factors in neurodegenerative disorders can beapproached by
considering first the general re-
YOU CAN PAY ME NOW OR YOU CAN PAYME LATER
The classic mitochondrial diseases known as the
mitochondrialencephalomyopathies are caused by mutations in the
mitochon-
drial or nuclear genome that affect the respiratory chain
directly.Overall, these disorders cause acute (e.g., seizures,
strokes) or
subacute (e.g., ataxia, neuropathy) clinical problems that
mani-fest early in life, in children or in young adults. However,
as a
general rule, genetic defects in mitochondrial functions that
do
notdirectly impactthe respiratory chainsuch as
proteinimport,organellar dynamics, and programmed cell deathcause
chronicclinical problems of much later onset, highly reminiscent of
the
three more common age-related and apparently sporadic
neu-rodegenerative disorders, Parkinson disease, Alzheimer
disease,and amyotrophic lateral sclerosis. In fact, now that we
have begun
to appreciate that the familial forms of the Big Three involve
mi-tochondrial function in the guise of altered organellar
dynamics,
it is no stretch of the imagination to envision the same kinds
ofmitochondrial involvement even in the far-more-common spo-
radic presentations of these devastating disorders.
lationship of mitochondrial biology to neu-
rodegeneration and then the specific diseasesattributed to
mutations in nuclear-encoded
proteins, most of them targeted to the mito-chondria (Tieu &
Przedborski 2006).
www.annualreviews.org Mitochondrial Disorders in the Nervous
System 107
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
18/35
FRDA: Friedreichataxia
Mitochondria and Neurodegeneration
Cell death in neurodegenerative diseases usu-
ally occurs by apoptosis, more commonly bythe intrinsic
mitochondrial pathway than by
the extrinsic cell-signaling pathway. The in-trinsic pathway
controls activation of caspase
9, through the adaptor molecule Apaf-1, by
regulating the release of cytochrome c fromthe IMS to the
cytosol. Proapoptotic and an-tiapoptotic members of the Bcl-2
family, and
also stress and survival signals, regulate therelease of
cytochrome c from the ISS into
the cytoplasm. Proapoptotic signals can alsorelease proteins
such as Smac/DIABLO and
Omi/HTRA2, which block IAP (inhibitor ofapoptosis) proteins to
activate cell death cas-
pases. However, in the intrinsic pathway ofapoptosis,
mitochondria are not merely passive
containers capable of leaking cytochrome c:Rather, their
life-supporting functions areclearly linkedto their death-promoting
activity.
These modulating factors include the respira-tory chain
activity, with the unavoidably associ-
ated generation of ROS; mitochondrial fusionand fission; calcium
homeostasis; the lipid com-
position of the mitochondrial membranes; andthe mitochondrial
permeability transition.
As an obvious example of the respiratorychain influence,
cytochrome c is a vital water-
soluble electron carrier, not just an executionerin
apoptosis.
Also, ROS are normal byproducts of the res-piratory chain
activity, and their concentrationis controlled by mitochondrial
antioxidant en-
zymes, such as manganese superoxide dismu-tase (SOD2) and
glutathione peroxidase. Ex-
cessive ROS production (oxidative stress) isconsidered a central
feature in the pathogen-
esis of all neurodegenerative disorders (Beal2005), which
explains the popularity of ROS-
scavenging compounds, such as CoQ10 or anal-ogous molecules, in
therapeutic trials (Di-
Mauro et al. 2006c, Shults & Schapira 2001).A pathogenic
role for ROS in age-related neu-
rodegeneration is also suggested by the cor-relation between
rates of formation of mito-
chondrial reactive oxygen and nitrogen species
(RONS), rates of neurodegeneration in br
and retina, and maximum lifespan potentialsfive different
mammalian species (Wright et
2004).The observation that during apoptosis
normally tubular mitochondrial network bcomes fragmented, and
that the proapopto
molecule Bax colocalizes with the fusiorelated proteins DRP1 and
MFN2 (Newme& Ferguson-Miller 2003), suggests a regulato
role for mitochondrial fission and fusion. mentioned above,
cardiolipin has many fun
tions beyond being a scaffold for the respitory chain: One such
function may be to fav
apoptosis through Bax-mediated permeabilition of the OMM.
Although cardiolipin is p
dominantly a component of the IMM, it mbe present in the OMM at
sites of contact w
the IMM, where Bid and Bcl-2 also clus(Newmeyer &
Ferguson-Miller 2003).
The permeability transition (PT) refersa still largely
hypothetical pore composed
cyclophilin D and the ANT1 protein in tIMMand of the
voltage-dependent anion ch
nel (VDAC) and the peripheral benzodiazepreceptor in the OMM.
Sustained openingthe PT pore is considered an obligatory step
apoptosis.
Neurodegenerative Diseases Causedby Mutations in
Nuclear-EncodedProteins Targeted to Mitochondria
Friedreich ataxia (FRDA) is an autosomal cessive disorder
characterized clinically by ea
onset (before 25 years of age), progressive limand gait ataxia,
peripheral neuropathy with a
flexia, pyramidal signs, hypertrophic cardiomopathy, and
increased incidence of diabe
The hallmark neuropathology of FRDA is d
generation of the spinocerebellar tracts alarge sensory neurons.
The mutated mitochodrial protein, frataxin, is encoded by a ge
(FXN) on chromosome 9q13, andmost patieare homozygous for a GAA
trinucleotide rep
expansion in the first intron of FXN. Thare loss-of-function
mutations, and resid
108 DiMauro Schon
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
19/35
frataxin expression level correlates with the
severity of the clinical phenotype.FRDA pathogenesis is
controversial because
frataxin is involved in the formation of non-heme iron-sulfur
clusters (ISCs), heme biosyn-
thesis, and the detoxification of iron. Loss offrataxin causes
impaired mitochondrial iron
storage and metabolism and defects in mito-chondrial enzymes
containing ISCs, including
aconitase and complexes I, II, and III. Iron ac-cumulation
increases ROS generation by theFenton reaction, causing oxidative
damage and
further mitochondrial enzyme inactivation. Toworsen the
situation, antioxidant defenses are
decreased in cultured cells from FRDA
patients(Chantrel-Groussard et al. 2001). Although the
pathogenic role of oxidative stress in FRDAseemed bolstered by
the beneficial effects of
the antioxidant idebenone, at least on the car-diopathy (Schulz
et al. 2000), paradoxically, a
conditional neuronal frataxin knockout mouseshowed neither
evidence of oxidative stress nor
improvement with antioxidants (Seznec et al.2005).
Hereditary spastic paraplegia (HSP) is theterm for a group of
clinically similar disordersrather than a specific clinical entity.
We have
already discussed two different mitochondrialcauses of autosomal
dominant HSP: one a
defect in mitochondrial protein importationcaused by mutations
in SPG13, encoding
the chaperonin HSP60 (HSP here stands forheat shock protein),
and the other a defect of
mitochondrial behavior caused by mutations inthe kinesin KIF5A.
More controversial is the
pathogenesis of an autosomal recessive formof HSP caused by
mutations in a gene (SPG7)
encoding paraplegin, a protein highly homol-ogous to the AAA
family of mitochondrial
proteases (Casari et al. 1998).Because AAApro-
teases have a quality control function ensuringthat unassembled
respiratory chain subunits aredegraded, a mutatedparaplegin
mayresult in anaccumulation of defective subunits choking
the importation machinery (similar to muta-tions in HSP60) and,
ultimately, the respiratory
chain (Claypool et al. 2006). However, anotherfunction of
paraplegin seems to involve process-
PD: Parkinson dise
ing MRPL32, a component of the large riboso-
mal subunit tightly bound to the IMM (Clay-pool et al. 2006,
Nolden et al. 2005). Thus, a
mutated paraplegin may impair mtDNA trans-lation, in which case
this form of HSP would
belong with the subgroup of intergenomiccommunication disorders
discussed above.
Autosomal dominant HSP type 4 (SPG4) iscaused by mutations in
spastin (gene SPAST),
a microtubule-severing protein located in thecytoplasm. Because
mitochondria must be at-tached to microtubules for them to travel
down
axons, disruption of this connection should af-fect
mitochondrial mobility, and indeed, cells
of SPG4 patients showed an abnormal perinu-clear clustering of
mitochondria, presumably a
consequence of an inability of mutated spastinto sever
microtubules (McDermott et al. 2003).
Spastins binding partner is known as atlastin(Sanderson et al.
2006), and mutations in the
gene encoding this protein (SPG3A) also causeHSP (autosomal
dominant HSP type 3A), again
implicating cargo traffic on microtubules (andalmost certainly
mitochondria) in the patho-
genesis of the disorder. Autosomal recessive HSP type 20
(also
called Troyer syndrome) is due to mutations
in spartin (gene SPG20), an OMM protein(Lu et al. 2006). Spartin
has a microtubule
interacting and trafficking (MIT) domain atits N-terminus
(interestingly, its mitochondrial
targeting signal is located at the C-terminus),implying yet
again the role of mitochondrial
trafficking in thepathogenesisof this syndromicgroup (Lu et al.
2006).
Finally, autosomal dominant HSP type 31(SPG31) is caused by
mutations in recep-
tor expression-enhancing protein 1 (REEP1),a mitochondrial
protein of unknown function
(Zuchner et al. 2006b).
Parkinson disease (PD) is a predominantlysporadic late-onset
disorder, and the mito-chondrial theory of aging, with its
nonfamilial,age-related accumulation of somatic mtDNA
deletions in the substantia nigra (coupled withbiochemical
evidence of complex I deficiency),
provided an attractive pathogenic explanation.Although, as
discussed above, this mechanism
www.annualreviews.org Mitochondrial Disorders in the Nervous
System 109
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
20/35
HD: Huntingtondisease
per se is not sufficient to explain sporadic PD,
PD (or parkinsonism, if the diagnostic criteriaof the London
Brain Bank areapplied strictly) is
familial more often than thought until five yearsago (Hardy et
al. 2006). To date, six nuclear
genes have been implicated: PARK2 (disease lo-cus PARK2),
encoding parkin; PINK1 (locus
PARK6), encoding PTEN-induced putative ki-nase 1, or PINK1;
PARK7 (locus PARK7), en-
coding DJ-1 (Hardy et al. 2006); SNCA (locusPARK1/4), encoding
-synuclein; LRRK2 (lo-cus PARK8), encoding dardarin; and HTRA2
(locus PARK13) encoding Omi/HTRA2. Allthese proteins interact
directly or indirectly
with mitochondriaandseemto affect apoptosis.Mutations in PARK2
have been associated
with autosomal recessive PD. Parkin is a ubiq-uitin E3 ligase
associatedwith theOMM, where
it has a protective role against mitochondrialswelling caused by
ceramide-induced apopto-
sis (Darios et al. 2003). As further evidence of amitochondrial
role for parkin, patients with PD
and parkin mutations have decreased complexI in leukocytes
(Muftuoglu et al. 2003).
PINK1 is a mitochondrial kinase (Silvestriet al. 2005) whose
precise function is unknown,but which, when mutated, causes
early-onset
recessive PD and, when overexpressed, protectsagainst neuronal
apoptosis (Petit et al. 2005).
Omi/HTRA2 is a serine protease localizedto the mitochondrial IMS
and released into the
cytosol upon apoptosis induction. Strauss et al.(2005) found a
mutation inHTRA2 in four spo-
radic patients with PD, and a polymorphismin the same gene seems
to predispose to PD
development.Although mutations in DJ-1 were thought
to abolish the oxidation-induced localization ofthe protein to
mitochondria (Canet-Aviles et al.
2004), good evidence demonstrates that both
wild-type and mutant DJ-1 proteins are presentin mitochondria
(matrix and IMS) (Zhang et al.2005a), where they likely have an
antiapoptoticfunction.
-synuclein is a cytosolic protein, but itsfunctional
relationshipwith mitochondria is re-
vealed by several observations: (a) Overexpres-sion of mutant
-synuclein in cell cultures im-
pairs the respiratory chain and induces oxid
tive damage; (b) transgenic mice overexpress-synuclein in
neurons are overly sensitive
MPTP; (c)-synuclein-deficient mice are mresistant to respiratory
chain inhibitors; a
(d) transgenic mice expressing mutantsynuclein show neuronal
degeneration, acc
mulation of intraneural inclusions, and coplex IV deficiencyin
thespinalcord. In humamutations in the SNCA gene cause autosom
dominant PD (Polymeropoulos et al. 1997).Autosomal recessive
parkinsonism is not u
common in patients with PEO and mutatioin POLG, and it can be
seen even in young p
tients without PEO (Davidzon et al. 2006).Huntington disease
(HD), an auto
mal dominant disorder, penetrates fully mid-adult life and is
characterized by choreo
thetotic movements, emotional problems, adementia. Selective
degeneration of stria
neurons and marked atrophy of caudate aputamen occur. HD is
caused by abnormexpansion of a CAG repeat in the HD gene
chromosome 4, which encodes a protein calhuntingtin (HTT).
Although HTT is not a m
tochondrial protein, four pathogenic scenarall involve
mitochondrial dysfunction.
The first scenario postulates an
enemetabolismdefectandisbasedonmagneticr
onance spectroscopy (MRS) of the brain (shoing lactate peaks in
the occipital cortex a
basal ganglia) andof muscle(showing decreasPCr/Pi ratios). Both
direct and indirect b
chemical evidence also show impaired enerproduction because the
activities of respirato
chain complexes II and III were decreasedpostmortem HD brains,
and inhibition of co
plex II by malonate in experimental animcaused pathological
lesions resembling thosehuman HD.
The second scenario is based on evidenthat polyglutamine
accumulation impairs c
cium handling, causing calcium-induced pmeability transition and
cytochrome c rele
(Choo et al. 2004).The third pathogenic mechanism in a sen
includes the previous two andsuggests that mtant HTT impairs
mitochondrial function
110 DiMauro Schon
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
21/35
a more general way, by repressing PGC-1-
regulated gene transcription of many nucleus-encoded
mitochondrial genes; PGC-1 (perox-
isome proliferators-activated receptor- coac-tivator 1) is a
master transcriptional coactiva-
tor that controls mitochondrial biogenesis andoxidative
phosphorylation (Greenamyre 2007).
Fourth, and perhaps most provocative, aphysical interaction that
impacts organellar
mobility in this disease may exist between HTTand mitochondria.
HTT binds to huntingtin-interacting protein 1 (HAP1). HAP1 is a
cy-
tosolic protein that associates with micro-tubules and other
membranous compartments
of the cell, including mitochondria (Gutekunstet al. 1998).
However, using immuno-electron
microscopy, HAP1 was localized to smallpuncta in both the
nucleus and the mitochon-
dria (Gutekunst et al. 1998). In addition, HAP1interacts with
the p150Glued subunit of dyn-
actin (DYNC1LI2) (Engelender et al. 1997, Liet al. 1998). The
relationship between HTT,
HAP1, and dynactin may explain the observa-tion that
microtubules are destabilized in HD
(Trushina et al.2003)and that mutantHTT im-pairs axonal
trafficking in mammalian neurons(Trushina et al. 2004).
Amyotrophic lateral sclerosis (ALS) is alate-onset, sporadic
disorder typically affecting
both lower (anterior horn cells of the spinalcord) and upper
(cortical) motor neurons, caus-
ing widespread paralysis and premature death.About 5%10% of
patients have a familial form
of ALS (FALS), and 20% of these harbormutations in the
Cu,Zn-superoxide dismutase
1 (SOD1) gene. SOD1 is present in both thecytosol and in the IMS
(Sturtz et al. 2001).
Transgenic mouse models overexpressing mu-tant SOD1 also develop
motor neuron degen-
eration. Most pathogenic mutations do not im-
pair SOD1 activity, and investigators assumethat they cause a
toxic gain of function.Mitochondrial involvement in FALS is
sug-
gested by the early mitochondrial degenera-
tion observed in motor neurons from patientsand transgenic
animals, by the presence of mu-
tant SOD1 and of aggregates containing mu-tant SOD1 in the
mitochondrial matrix and
ALS: amyotrophiclateral sclerosis
FALS: Familial ALS
AD: Alzheimerdisease
FAD: familial AD
IMS (Liu et al. 2004), and by the impaired mito-
chondrial functions (respiratory chain and cal-cium homeostasis)
seen in transgenic mice.
Studies also report respiratory chain abnor-malities in spinal
cord of sporadic ALS pa-
tients (Borthwick et al. 1999, Wiedemann et al.2002).
Conversely, one patient with primary
mitochondrial disease (a microdeletion in theCOX I gene of
mtDNA) had a typical, albeit
early-onset, ALS phenotype (Comi et al. 1998).Alzheimer disease
(AD) is a neurodegener-
ative dementing disorder of late onset, with a
relatively long course (Mattson 2004). Stud-ies show progressive
neuronal loss, especially
in the cortex and the hippocampus. The twomain histopathological
hallmarks of AD are the
accumulation of extracellular neuritic plaques,consisting mainly
of -amyloid (A), and of
neurofibrillary tangles, consisting mainly of
hy-perphosphorylated forms of the microtubule-
associated protein tau (Goedert & Spillantini2006, Roberson
et al. 2007). Most AD cases are
sporadic, but three genes have been identifiedin the familial
form (FAD): amyloid precursor
protein (APP), presenilin 1 (PS1; gene PSEN1),and presenilin 2
(PS2; gene PSEN2). Vari-ants in two genes predispose people to
SAD:
apolipoprotein E isoform 4 (APOE4) (Corderet al. 1993) and
SORL1, a neuronal sorting re-
ceptor (Rogaeva et al. 2007).Abundant evidence indicates that
mitochon-
dria are affected in AD, including reductionin brain energy
metabolism shown by positron
emission tomography (Azari et al. 1993),mitochondrial metabolic
enzyme deficiency
(Mastrogiacomo et al. 1993, Sheu et al. 1985),and respiratory
chain deficiency (Bonilla et al.
1999, Kish et al. 1992), etc. However, a directrole for
mitochondria in AD pathogenesis has
been controversial, hinging mainly on findings
related to both APP and PS1. The current view is that APP is
locatedpredominantly in the plasma membrane, whereit is cleaved in
a series of proteolytic events
(e.g., by -, -, and -secretases) to releaseintra- and
extracellular fragments of uncertain
function. However, Avadhanis group showedby genetic dissection
and expression of APP
www.annualreviews.org Mitochondrial Disorders in the Nervous
System 111
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
22/35
constructs in vitro that the APP protein con-
tains a possible mitochondrial targeting signalat its N-terminus
(Anandatheerthavarada et al.
2003). They then showed that nonglycosylatedfull-length and
C-terminal truncated APP
accumulates exclusively in the mitochondrialproteinimport
channels in AD brains but not in
age-matched controls (Devi et al. 2006). Thisresult was
consistent with (a) the identification
of A42 in mitochondria (Lustbader et al.2004, Manczak et al.
2006); (b) the observationthat A binds to 17--hydroxysteroid
dehy-
drogenase, type 10 (HADH2), a mitochondrialmatrixprotein
involved in fatty acid metabolism
(Lustbader et al. 2004); and (c) the finding that-amyloid
inhibits respiratory chain function
in isolated rat brain mitochondria (Casley et al.2002). However,
it is unclear how A could
be derived from its precursor APP withinmitochondria, given that
the putative requi-
site initial processing proteases (e.g., - and-secretases) have
not been found in mitochon-
dria. A could be imported into mitochondria,but at present there
is no coherent explanation
as to how this might be accomplished.Researchers disagree with
regard to PS1.
Using immunohistochemical techniques, PS1
has been localized to numerous membranouscompartments in cells.
These include the endo-
plasmic reticulum (ER) (Walter et al. 1996), theGolgi apparatus
(Annaert et al. 1999, Siman &
Velji 2003), endosomes/lysosomes (Runz et al.2002, Vetrivel et
al. 2004), the nuclear enve-
lope (Honda et al. 2000), and the plasma mem-brane (Schwarzman
et al. 1999), where they
are especially enriched at intercellular contactsknown as
adherens junctions (Marambaud et al.
2002). PS1 hasnot been found in mitochondria,except by one group
that used Western blot-
ting and immunoelectron microscopy, not im-
munohistochemistry, to localize PS1 to the ratmitochondrial
inner membrane (Ankarcrona &Hultenby 2002, Hansson et al.
2004).
Besides PS1, the -secretase complex con-
tains at least three other proteins: APH1,PEN2, andnicastrin(De
Strooper 2003). Using
immunoelectron microscopyandWesternblot-ting, all three proteins
have been localized to rat
mitochondria (Hansson et al. 2004). Howev
localization of-secretase subunits, includiPS1, to mitochondria
has not been confirm
or demonstrated by other, more definitimethods.
Given that mitochondria play a role in tpathogenesis of several
neurodegenerative d
eases (Figure 8), it would not be unreasonato invoke similar
mechanisms for AD, and pecially a mechanism involving
mitochondr
movement and localization (Kins et al. 200This possibility is
supported by two obser
tions.First,aPS1mutation(M146V)inamouPS1 knock-in model impairs
axonal transp
and also increases tau phosphorylation (Pigiet al. 2003).
Second, axonal defects, consisti
of swellings that accumulate abnormal amouof
microtubule-associated and molecular m
tor proteins, organelles, and vesicles, have befound in both
sporadic AD patients and
transgenic mouse models of FAD (Stokin et2005).
MITOCHONDRIAL PSYCHIATRY
Given the brains high dependence on oxidat
metabolism, it is hardly surprising that primmitochondrial
disorders often cause cognitdeficits: dementia in adults and mental
retard
tion or neuropsychological regression in chdren. Researchers
have paid comparatively l
attention to the relationship between psycatric diseases and
mitochondrial dysfunctio
For the sake of order, let us consider separatthe psychiatric
manifestations of primary m
tochondrial diseases and the evidence of michondrial dysfunction
in patients with isola
primary psychiatric illnesses.Although the literature is replete
with an
dotal reports of psychiatric problems, mos
severe depression, in patients with mtDNrelated diseases
(DiMauro et al. 2006b), thhave been few systematic
neuropsychiat
studies of large cohorts of patients with knowmitochondrial
diseases. We have reported pliminary data on a large group of MELAS
a
MERRF families (102 persons from 30 kdreds), including notonly
patients but also th
112 DiMauro Schon
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
23/35
oligosymptomatic or asymptomatic maternal
relatives. In MELAS families (harboring theA3243G mutation), 42%
of fully symptomatic
carriers reported depressive symptoms, but22% of asymptomatic
and 29% of oligosymp-
tomatic carriers also had depressive traits, com-pared with only
7% of the control group
(Kaufmann et al. 2002). In MERRF familieswith the A8344G
mutation, 80% of fully symp-
tomatic patients, 20% of oligosymptomaticcar-riers, and none of
the asymptomatic carriers re-ported depressive symptoms. The
finding that
even asymptomatic carriers of the MELAS mu-tation were prone to
depression suggested that
psychiatric problems might be an early clinicalexpression of the
mutation, which is also sup-
ported by correlative neuropsychological and MRS studies,
showing cerebral lactic acido-
sis in asymptomatic MELAS relatives and acorrelation between
neuropsychological scores
and ventricular lactate levels (Kaufmann et al.2004).
Among the Mendelian mitochondrial dis-eases, depression is
frequent in patients with
defects of intergenomic communication, PEO,and multiple mtDNA
deletions. Psychiatricproblems are especially common in
patients
harboring mutations in ANT1, PEO1, andPOLG (DiMauro et al.
2006b).
Although maternal inheritance of bipolardisorder had been
suggested by a higher-than-
expected frequency of affected mothers and in-creased risk of
illness in maternal relatives, mu-
tations in mtDNA have been excluded as causesof the disease
(Kirk et al. 1999). However, mi-
tochondrial dysfunction may still be involvedin bipolar disorder
pathogenesis through sev-
eral pathogenic mechanisms, many of which,not surprisingly, are
similar to those proposed
for neurodegenerative diseases. These include
alterations of calcium homeostasis (Kato et al.2002),
downregulation of genes controlling mi-tochondrial energy
metabolism (Konradi et al.2004), and impaired mtDNA replication
(Kaki-
uchi et al. 2005), all possibly related to a change(-116C>G)
in the promoter region ofXBP1, a
pivotal gene in theendoplasmic reticulum stressresponse
(Kakiuchi et al. 2003).
Another gene that has been highlighted
in the pathogenesis of both bipolar disorderand schizophrenia is
Disrupted in schizophre-nia 1 (DISC1), so called because a
disrup-tion of this gene by the chromosome 1 break-
point of a balanced t(1;11) translocation did,in fact,
cosegregate with schizophrenia and re-
lated mood disorders in a large Scottish family(St Clair et al.
1990). The association of DISC1and schizophrenia was confirmed in
Finnish,
American,Japanese, andTaiwanese populations(Roberts 2007) and
extended to bipolar dis-
order (Maeda et al. 2006). Although its pre-cise role remains
unclear, DISC1 bound pre-
dominantly to mitochondria (James et al. 2004)and interacted
with several proteins, including
FEZ1, LIS1, and NUDEL, which are also in-volved, at least
indirectly, in neurodegenerative
diseases (Figure 8). Overexpression of DISC1in COS-7 cells
disrupts mitochondrial orga-
nization and leads to the formation of ring-like structures,
suggesting a role of this proteinin controlling mitochondrial
dynamics (Millar
et al. 2005). The distribution of DISC1 in thedeveloping and
adult brain (frontal cortex, hip-
pocampus, thalamus) and its involvement withneuronal migration,
neurite outgrowth, and
synaptic plasticity support the pathogenic roleof genetic
variants in psychiatric disorders.
CONCLUSIONS
Two main concepts emerge from this overview
of mitochondrial disorders in the nervous sys-tem. The first is
a sense of amazement that this
small organelle, a foreign guest that took uppermanent residence
in all our cells, partici-
pates in such a wide array of neurological dis-orders, from LS
in infancy to AD in old age. A
second, and related, consideration is that there
is much more to mitochondria than the stan-dard textbook gloss
that they are the power-houses of the cell that only produce ATP.
Be-
sides ATP production, mitochondria performvaried functions that
are important for cell lifeand death, including ROS generation,
calcium
homeostasis, and programmed cell death, andthe pathogenesis of
any mitochondrial disease
www.annualreviews.org Mitochondrial Disorders in the Nervous
System 113
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
24/35
is likely to involve, at least to some extent and
at some point, all these functions. In fact, wehave seen that
even primary defects of the res-
piratory chainthe most likely causes of powerfailuresare so
diverse as to defy a unitary
mode of pathogenesis that invokes merely theloss of ATP
capacity.
In the nervous system, mitochondrial dy-namics are crucial to
guarantee long distance
delivery and balanced distribution of energy
(in addition to all the other functions) to t
farthest reaches of neurons (synapses and dedrites). Although
the concept and the rules
mitochondrial dynamics have been latecomto the field of
mitochondrial diseases, alt
ations in the topology and topography of tmost plastic of
organelles may well be the u
fying theme providing, more often than nocommon finalpathogenic
pathway for neurodgenerative and psychiatric diseases alike.
DISCLOSURE STATEMENT
The authors are not aware of any biases that might be perceived
as affecting the objectivity of t
review.
ACKNOWLEDGMENTS
This work has been supported by grants from the National
Institutes of Health (NS 11766 aHD32062), from the Muscular
Dystrophy Association, and from the Marriott Mitochondr
Disorder Clinical Research Fund (MMDCRF). The authors are
grateful to Drs. Michio Hiraand Lewis P. Rowland for revising the
manuscript and to Drs. Eduardo Bonilla and Kurenai Ta
for providing Figures 3 and 4.
LITERATURE CITED
Alam R, Hachiya N, Sakaguchi M, Kawabata S, Iwanaga S, et al.
1994. cDNA cloning and char
terization of mitochondrial import stimulation factor (MSF)
purified from rat liver cytosJ. Biochem. 116:41625
Alexander C, Votruba M, Pesch UEA, Thiselton DL, Mayer S, et al.
2000. OPA1, encodindynamin-related GTPase, is mutated in autosomal
dominant optic atrophy linked to ch
mosome 3q28. Nat. Genet. 26:21115
Anandatheerthavarada HK, Biswas G, Robin MA, Avadhani NG. 2003.
Mitochondrial targetiand a novel transmembrane arrest of Alzheimers
amyloid precursor protein impairs mi
chondrial function in neuronal cells. J. Cell. Biol.
161:4154
Anderson S, Bankier AT, Barrel BG, DeBruijn M, Coulson AR, et
al. 1981. Sequence and orgnization of the human mitochondrial
genome. Nature 290:45765
Ankarcrona M, Hultenby K. 2002. Presenilin-1 is located in rat
mitochondria. Biochem. BiophRes. Commun. 295:76670
Annaert WG, Levesque L, Craessaerts K, Dierinck I, Snellings G,
et al. 1999. Presenilin 1 co
trols -secretase processing of amyloid precursor protein in
pre-Golgi compartmentshippocampal neurons. J. Cell Biol.
147:27794
Azari NP, Pettigrew KD, Schapiro MB, Haxby JV, Grady CL, et al.
1993. Early detection
Alzheimers disease: a statistical approach using positron
emission tomographic data.J. Cer
Blood Flow Metab. 13:43847
Beal MF. 2005. Mitochondria take center stage in aging and
neurodegeneration. Ann. Neu58:495505
114 DiMauro Schon
-
8/3/2019 Mitochondrial Disorders in Neurons 2008
25/35
Bender A, Krishnan KJ, Morris CM, Taylor GA, Reeve AK, et al.
2006. High levels of mitochon-
drial DNA deletions in substantia nigra neurons in aging and
Parkinson disease. Nat. Genet.38:51517
Betts J, Jaros E, Perry RH, Schaefer AM, Taylor RW, et al. 2006.
Molecular neuropathologyof MELAS: level of heteroplasmy in
individual neurones and evidence of extensive vascular
involvement. Neuropath. Appl. Neurobiol. 32:35973Bonilla E,
Tanji K, Hirano M, Vu TH, DiMauro S, Schon EA. 1999. Mitochondrial
involvement
in Alzheimers disease. Biochim. Biophys. Acta
1410:17182Borthwick GM, Johnson MA, Ince PG, Shaw PJ, Turnbull DM.
1999. Mitochondrial enzyme
activity in amyotrophic lateral sclerosis: implications for the
role of mitochondria in neuronalcell death. Ann. Neurol.
46:78790
Bossy-Wetzel E, Barsoum MJ, Godzik A, Schwartzenbacher R, Lipton
SA. 2003. Mitochondrial
fission in apoptosis, neurodegeneration and aging. Curr. Opin.
Cell Biol. 15:70616Bourdon A, Minai L, Serre V, Jais J-P, Sarzi E,
et al. 2007. Mutation of RRM2B, encoding p53-
controlled ribonucleotide reductase (p53R2), causes severe
mitochondrial DNA depletion.Nat. Genet. 39:77680
Brandon NJ, Schurov I, Camargo LM, Handford EJ, Duran-Jimeniz B,
et al. 2005. Subcellulartargeting of DISC1 is dependent on a domain
independent from the Nudel binding site. Mol.
Cell. Neurosci. 28:61324Bykhovskaya Y, Casas KA, Mengesha E,
Inbal A, Fischel-Ghodsian N. 2004. Missense mutation
in pseudouridine synthase 1 (PUS1) causes mitochondrial myopathy
and sideroblastic anemia(MLASA). Am. J. Hum. Genet. 74:13038
Canet-Aviles RM, Wilson MA, Miller DW, Ahmad R, McLendon C, et
al. 2004. The Parkinsonsdisease protein DJ-1 is neuroprotective due
to cysteine-sulfinic acid-driven mitochondrial
localization. Proc. Natl. Acad. Sci. USA 101:91038Carelli V,
Achilli A, Valentino ML, Rengo C, Semino O, et al. 2006. Haplogroup
effects and
recombination of mitochondrial DNA: novel clues from the
analysis of Leber hereditary
optic neuropathy pedigrees. Am. J. Hum. Genet. 78:56474Carelli
V, La Morgia C, Iommarini L, Carroccia R, Mattiazzi M, et al. 2007.
Mitochondrial optic
neuropathies: how two genomes may kill the same cell type?
Biosci. Rep. 27:17384Casari G, De Fusco M, Ciarmatori S, Zeviani M,
Mora M, et al. 1998. Spastic paraplegia and
OXPHOS impairment caused by mutations in paraplegin, a
nuclear-encoded mitochondrialmetalloprotease. Cell93:97383
Casley CS, Canevari L, Land JM, Clark JB, Sharpe MA. 2002.
-amyloid inhibits integratedmitochondrial respiration and key
enzyme activities. J. Neurochem. 80:91100
Chacinska A, Rehling P. 2004. Moving proteins from the cytosol
into mitochondria. Biochem. Soc.Trans. 32:77476
![Nuclear-Mitochondrial Intergenomic Communication Disorders · Mitochondrial disorders most often refer to the ... heterogeneous, overlapping and ever expanding [10,13]: i. ... Ocular](https://img.pdfslide.net/doc/110x75/5fa879b4c3392426ac15261a/nuclear-mitochondrial-intergenomic-communication-disorders-mitochondrial-disorders.jpg)