Embed Size (px)
Citation preview

Mitochondrial dysfunction as a central event formechanisms underlying insulin resistance: theroles of long chain fatty acids
Mohamad Hafizi Abu Bakar1*Cheng Kian Kai1
Wan Najihah Wan Hassan1
Mohamad Roji Sarmidi2
Harisun Yaakob2
Hasniza Zaman Huri3,4
1Department of BioprocessEngineering, Faculty of ChemicalEngineering, Universiti TeknologiMalaysia, Skudai, Johor, Malaysia2Institute of Bioproduct Development,Universiti Teknologi Malaysia, Skudai,Johor, Malaysia3Department of Pharmacy, Faculty ofMedicine, University of Malaya, KualaLumpur, Malaysia4Clinical Investigation Centre, 13thFloor Main Tower, University MalayaMedical Centre, Lembah Pantai, KualaLumpur, Malaysia
*Correspondence to: MohamadHafizi Abu Bakar, Department ofBioprocess Engineering, Faculty ofChemical Engineering, UniversitiTeknologi Malaysia, 81310, Skudai,Johor, Malaysia.E-mail: [email protected]
Summary
Insulin resistance is characterized by hyperglycaemia, dyslipidaemia andoxidative stress prior to the development of type 2 diabetes mellitus. To date,a number of mechanisms have been proposed to link these syndromestogether, but it remains unclear what the unifying condition that triggeredthese events in the progression of this metabolic disease. There have been asteady accumulation of data in numerous experimental studies showing thestrong correlations between mitochondrial dysfunction, oxidative stress andinsulin resistance. In addition, a growing number of studies suggest that theraised plasma free fatty acid level induced insulin resistance with thesignificant alteration of oxidative metabolism in various target tissues such asskeletal muscle, liver and adipose tissue. In this review, we herein proposethe idea of long chain fatty acid-induced mitochondrial dysfunctions as oneof the key events in the pathophysiological development of insulin resistanceand type 2 diabetes. The accumulation of reactive oxygen species, lipotoxicity,inflammation-induced endoplasmic reticulum stress and alterations of mito-chondrial gene subset expressions are the most detrimental that lead to thedevelopments of aberrant intracellular insulin signalling activity in a number ofperipheral tissues, thereby leading to insulin resistance and type 2 diabetes.Copyright © 2014 John Wiley & Sons, Ltd.
Keywords long chain fatty acids; insulin resistance; mitochondrial dysfunction;inflammation; lipotoxicity; reactive oxygen species
Abbreviations DNA, deoxyribonucleic acid; LCFA, long chain fatty acid; SCFA,short chain fatty acid; MCFA, medium chain fatty acid; ETC, electron transportchain; FADH2, flavin adenine dinucleotide; mtDNA, mitochondrial DNA; IRS,insulin receptor substrate; O2
�•, superoxide radicals; NADH, a reduced form ofnicotinamide adenine dinucleotide; PI3K, phosphatidylinositol-3-kinase; PKC,protein kinase C; PPARγ, peroxisome proliferator-activated receptor γ; ROS,reactive oxygen species; TCA, tricarboxylic acid; TNF, tumour necrosis factor
Introduction
Type 2 diabetes mellitus is a devastating metabolic disorder that is characterizedby insulin resistance and linked to various metabolic syndromes such ashormonal imbalance, hypertension, hyperglycemia and excess fatty acids in
REVIEW ARTICLE
Received: 16 May 2013Revised: 19 April 2014Accepted: 23 July 2014
Copyright © 2014 John Wiley & Sons, Ltd.
DIABETES/METABOLISM RESEARCH AND REVIEWSDiabetes Metab Res Rev (2014)Published online in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/dmrr.2601

blood circulation [1]. The biological determinant such asgenetic factors is involved in the pathogenesis of type 2diabetes [2,3]. One of the first-degree relatives who hadfamily history of type 2 diabetes is conferred to havethreefold increased risk of developing the disease [3–5].However, during the last few decades, the dramaticincreases in incidence and prevalence rates are also signif-icantly observed in developed and developing countries[6], signifying that the complex synergistic roles of bothgenetic and environmental factors such as malnutritionand sedentary lifestyles are considerably involved in thedevelopment of insulin resistance and type 2 diabetes [7].
In spite of extensive researches in deciphering theassociated risk factors for insulin resistance, the exactmechanism that contributes to these metabolic perturba-tions is still largely debated. Excessive calorie intake andpoor-quality diet are attributable to one of the majorindependent risk factors underlying the events of suchdisorder. Notably, there are growing concerns thatsurround the roles of certain types of fatty acids in theprogression of various metabolic syndromes [8]. Fattyacid is regarded as one of the most important nutrientsthat are actively involved in the regulation of an energymetabolism. They are classified based on their carbonchain length as short to very long. Short chain fatty acids(SCFAs) are ranging to have aliphatic tails of two to sixcarbons, while medium chain fatty acids (MCFAs) arethe sub-class of fatty acids with aliphatic tails of 7 to 12carbons. By contrast, long chain fatty acids (LCFAs) arecomposed of 13 to 21 carbon links, and very long chainfatty acids (VLCFAs) are viewed to have more than 22carbon lengths [9]. Particularly, different types of fattyacids are metabolized in distinctive ways. It was shownthat unsaturated fatty acids are mainly catabolizedfor energy production, whereas the saturated one islikely to be oxidized with the formation of lipid interme-diates [10]. In recent years, there are certain equivocalissues regarding the metabolic roles of LCFAs in theregulation of disease processes. A couple of studiessuggested that several types of LCFAs are directed toinhibit the signalling function of thyroid hormones inthe liver, leading to the promotion of hyperinsulinemiaand fatty liver [11–13]. Accordingly, the chronicexposures of LCFA such as palmitic acid on L6 skeletalmuscle of rat increased the severity of mitochondrial su-peroxides, mtDNA damages, c-Jun N-terminal kinase-1(JNK1)-signalling activation and inhibition of intracellu-lar insulin signalling activity, resulting to mitochondrialdysfunctions and insulin resistance [14]. On the otherhand, the other type of fatty acids such as SCFA andMCFA are evidenced to enhance the insulin sensitivityand increase the mitochondrial respirations of thecell [15,16]. Therefore, the oxidation of certain types offatty acids in various peripheral tissues may affect and
behave differently in regulating biological phenomenonof the normal and disease states.
Correspondingly, there is appealing evidence that re-vealed that mitochondrial dysfunction plays a crucial rolein the central pathogenesis of insulin resistance and type 2diabetes. In fact, the causal pathogenic relationship betweenmitochondrial dysfunction and type 2 diabetes is largelybeing discussed [17–19]. Numerous findings [20–26]indicate prominent mitochondrial dysfunction in skeletalmuscle, liver and adipose tissues of obese and type 2diabetic patients with a positive family history of diabetesand in animals with obesity-associated type 2 diabetes.Although clinical investigations on how fatty acids affectthe mitochondria function are relatively scarce, compellingexperimental studies suggest that the increase of plasmafree fatty acid (FFA) induces insulin resistance with thesignificant alteration of oxidative metabolism in varioustarget tissues such as skeletal muscle, liver, adipose tissueand heart [17,18]. These metabolic impairments mostlyoccur prior to the development of insulin resistance, whichis in the pre-diabetes condition. A number of review articlesdealing with the roles of fatty acid-induced mitochondrialdysfunctions in insulin resistance and type 2 diabetes wereextensively published [27–32]. The current dogma in thefield of mitochondrial dysfunction and insulin resistance isgenerally focused around the idea that lipid overloadinduced mitochondrial dysfunction that leads to skeletalmuscle insulin resistance. However, the previous researchdirections are being descriptive to explain the mechanismof insulin resistance in the event of mitochondrial dysfunc-tions without specifically focusing on what types of fattyacids contribute to these mechanistic processes in otherperipheral tissues such as liver, heart and adipose tissue. Itis firmly believed that LCFAs play important roles withinthe disease process by exerting their detrimental effects onmitochondria functions. Thus, the purpose of this article isto provide a comprehensive overview of how LCFAs mightcontribute to the regulation of insulin resistance by propos-ing that mitochondrial dysfunction is one of the centralhallmarks that causes aberrant insulin signalling activity ina number of peripheral tissues, directing to the progressionof insulin resistance and type 2 diabetes.
Mitochondria: it is more than energyfactories of the living cells
Mitochondria have its own unique DNA (circular anddouble stranded) and contain two plasma membranes,an inner and outer membrane. Human mtDNA is mater-nally inherited and encodes 13 specific gene subunits formitochondrial biogenesis and metabolism in the electrontransport chain (Complexes I, III and IV) together with
M. H. A. Bakar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

ATP synthase, 22 tRNAs and 2 rRNAs. However, certaingenes from other specific subunits (Complex II) areencoded from the nuclear DNA [33]. Mitochondria canbe recognized as a heart of the cell that modulates variouscellular homeostasis such as cell proliferation, calciumhomeostasis, detoxification of ammonia (in the liver),programmed cell death (apoptosis), oxidative stress(a hallmark of ageing process) and other related meta-bolic processes [34,35]. Several important events suchas mitochondrial fusions and fissions are indirectlyinvolved in the programmed cell death and autophagy[36]. Without this organelle, cell would be unable toextract the significant amount of energy in order to com-ply with the metabolic requirements under conditions ofhigh energy demands. Furthermore, it was found thatmitochondria are responsible for almost 90% of the wholebody metabolism required for the sustainability of cellularprocess and its physiological components, including themaintenance of the trans-membrane ion gradients,protein synthesis and vesicular transport [37,38].
The ability of cells to perform their function is largelydependent on the amount of energy produced per seduring the hydrolysis of the terminal phosphate bond.This is generally known as the free energy of ATP hydroly-sis. The amount of ATP generated by a particular tissuedepends on the number of mitochondria that can rangefrom hundreds to thousands per cell. The amount of mito-chondria varies depending on the age and maturation ofthe cell as well as type of tissues [39]. The electrontransport chain (ETC) system can be regarded as theheart of the mitochondria where the oxidative phosphory-lation takes place. The electron transport chain is embed-ded in the inner mitochondrial membrane that comprisesfour enzymatic series complexes (Complexes I–IV)together with ATP synthase. These five complexes syner-gistically work in concert as a biological machine thatundergoes conformational changes due to the substrate-induced reduction–oxidation reactions. The electrons thatare passed down through ETC are delivered and acceptedby oxygen in order to generate an electrochemical gradi-ent that drives the phosphorylation of ATP synthesis.
During the oxidative phosphorylation, the reductionof one molecule oxygen with one electron producesfree radical and superoxide molecules. Reactive oxygenspecies (ROS) such as superoxide (O2
�•) radical isconverted to hydrogen peroxide (H2O2) by manganesesuperoxide dismutase and to water by glutathione perox-idase. Several distinct biological processes such as DNArepair, transcription, replication and protein synthesisare indirectly interacting with the mitochondrial matrix.In order to perform these cellular processes, all requiredenzymes need to be imported from cytosol into themitochondrial matrix. These complex processes signifythat mitochondrial activities require distinct mechanistic
interactions from various levels of metabolic activities inthe tissue. Thus, any impairment of these processes mightinherently affect downstream metabolic activity of thecell, as well as functional and structural behaviour ofcertain proteins and metabolites in target tissues. Inaddition, it was evidenced that human mitochondrialgenomes (size of approximately 16.5 kb) have a very highmutation rate that is 10–17-folds higher than the nucleargenomes. This could be due to the nature of humanmitochondrial structural integrity that lacks histone andmutation-suppressing elements such as intron sequences[40]. As such, it does not come as a surprise why thesebiological complex systems in the mitochondria arevulnerable to perturbations in the event of metabolicstress and disease process [41]. Because of the fragilityof the mitochondrial respiratory chain system, one simpleperturbation to the electron transport chain and its down-stream complexes might affect the nucleotide pools, tri-carboxylic acid (TCA) cycle flux, one-carbon metabolismand ROS signalling [42].
In particular, glucose, fatty acids and amino acid are theimportant substrates that have to be utilized by the bodyin order to perform the cellular functions [43]. Theseimportant substrates undergo a series of cellular metabo-lism and break down into several intermediate metabo-lites. The reducing equivalents such as nicotinamideadenine dinucleotide (NADH) and flavin adenine dinucle-otide (FADH2) and other metabolites are directly involvedtowards energy production. They are generated throughTCA cycle and β-oxidation together with the involvementof various levels of oxidative process. Highly energetictissues such as skeletal muscle, heart and liver arecritically dependent on the oxidative metabolism of mito-chondrial activities and phosphorylation of adenosinediphosphate (ADP) to ATP [44]. As the excessive energyproduction takes place, ROS are produced and may causedefects in other macromolecules such as lipid, protein andnucleic acid. Consequently, these conditions cause a seriesof modification of the mtDNA structures and affect theupper and lower levels of the mitochondrial gene expres-sion and proteins [45]. Excess FFA in blood circulationand together with hyperglycemia may also result in thedisproportionate generation of superoxide radical thatapparently affects mitochondrial integrity and plays amajor role in the pathway leading to many metabolicdisorders [46]. One study showed that in parallel withthe increase of ROS productions, other stress kinaseintracellular signalling pathways via nuclear factor-κB(NF-κB), p38 mitogen-activated protein kinase, JNK orstress-activated protein kinase, and hexosamine are alsotriggered in the disease process [47,48]. The activationof these regulatory pathways together with the elevationof ROS productions worsens the metabolic activity of thecell, causing the impaired glucose uptake and insulin
Long Chain Fatty Acids Induced Mitochondrial Dysfunction in Insulin Resistance
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

resistance. Conspicuously, the underlying mechanism ofmitochondrial dysfunction in several peripheral tissues isvery complex and intricate to be understood that itrequires synergistic analysis of both genetic (nuclear andmitochondrial genomes) and environmental factors to beperformed. Given their significance in basic biology andclinical medicine, we should agree with the assumptionsto recognize mitochondria as one of the vital organellesin regulating cellular and systemic energy homeostasisof the various metabolic disorders such as insulinresistance and type 2 diabetes.
Cellular metabolic competition of fattyacid and glucose oxidation
Historically, the research works on the metabolic competi-tion between fatty acids and glucose oxidation formitochondrial respiration were started in the early twenti-eth century [49]. Several years later, the perfused heartmuscle and diaphragm of rats were isolated to elucidatethese mechanisms of inhibition of glucose oxidation byfatty acids [50,51]. After that, the first mechanisticexplanation for the reciprocal relationship between fattyacids availability and glucose utilization was pronouncedby Randle and his colleagues. This finding is famouslyknown as the Randle cycle [52]. In their study, theybelieved that the elevation of fatty acid level supply tothe diaphragm and isolated heart was strongly associatedwith an increase of fatty acid oxidation rates towardsproducing acetyl-CoA and citrate. The availability of thesemetabolic intermediates in heart muscle essentially leadsto the impairment of glucose oxidation, glycolytic fluxand its utilization. The strong competition of substrateoxidation between fatty acid and glucose was significantlyobserved in rat heart muscle. According to their hypothe-sis, the increase of FFA oxidation directly augments themitochondrial ratio of acetyl-CoA to coenzyme A andNADH to NAD+. An elevation in these ratios results inthe increase of citrate levels in the mitochondria andcrucially inactivates the pyruvate dehydrogenase activityvia inhibition of glucose oxidation in the cytosol. In turn,glycolysis is inhibited via reduction of phosphofructoki-nase and hexokinase II activities and later contributed tothe accumulation of glucose-6 phosphate and glycogenlevels in the cytosol, thus contributing to the decrease ofbasal glucose uptake [53,54].
However, in the following years, Randle’s cycle theorywas challenged and overshadowed by numerous evi-dence [27–29,54,55]. They clearly argued that the accu-mulation of excess fatty acid intermediates such LCFA-CoA, diacylglycerol and ceramides in various peripheraltissues is noticed. Insulin resistance induced by FFA is
primarily associated with the impaired glucose uptakerather than the changes of glucose metabolism in thecytosol [54,55]. The defects in glucose transport system,phosphorylation and its disposal equally contribute tothe reduction of glycogen synthesis in rat with high-fatdiet-induced insulin resistance. The other similar reportsalso documented that the elevated level of LCFAs impairsand inhibits the process of glucose uptake rather thanaffecting the glucose metabolism [56–58]. Thus, it is note-worthy to know that Randle’s cycle does not completelyexplain and demonstrate the reciprocal relationshipbetween the glucose and fatty acid oxidation, as bothmetabolic substrate oxidations were reduced in distinctways. In fact, other intracellular mechanisms such asaccumulation of ROS and lipid intermediate metabolite-induced lipotoxicity, activation of novel protein kinaseisoforms and the effects of inflammatory mediators inthe cytosol might play the most important causative rolesin the development of insulin resistance [31,59]. On theother hand, it is speculated that LCFAs could be one ofthe ‘metabolic culprits’ that can deteriorate the efficiencyof mitochondrial activities in the long run. The emergenceof the old and new theories in these competing ideasmight warrant for numerous potential investigations andstudies to be performed in the future.
The metabolic fates of LCFA oxidationin normal and disease state
Fatty acids undergo differentmetabolic pathways dependingon the length of the carbon chain, position and geometry ofthe double bonds (cis and trans) [60]. These differencesin chemical properties might substantially affect their me-tabolism in the body. The resultant fatty acid substratessubsequently modify their properties by the actions of therespective enzymes involved in the particular metabolicpathways [61]. Physiologically, SCFAs and MCFAs are ableto diffuse directly into the plasma membrane of the livervia portal vein during lipid digestion. LCFAs are wrappedinto chylomicron and enter lymphatic capillaries via the sub-clavian vein before going into the blood circulation [62].LCFAs are subjected to undergo several distinct processesthat require protein transporter such as fatty acid translocase(FAT/CD36), fatty acid transport proteins and plasmamembrane fatty acid-binding protein in order to cross themembrane barrier of the cell. It was observed that theCD36 mRNA and its protein were significantly amplified inboth rodent and human skeletal muscle during several daysof the intervention of a high-fat diet [63,64]. Additionally,the defective uptake and utilization of LCFAs in skeletalmuscle, heart and adipocytes were observed in CD36 knock-out mice [65]. This might suggest the pivotal role of this
M. H. A. Bakar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

protein transporter in the relative rate of LCFA uptake intoskeletal muscle of both rodents and humans.
The insulin resistance is also characterized by animbalance between fatty acid oxidation and its uptake incertain target tissues [66]. During fatty acid oxidation,the transport of LCFAs is generally known as the rate-limiting step. LCFAs are metabolized by the addition ofcoenzyme A by acyl-CoA synthetase in the cytoplasm,and the resultant LCFA-CoA is transported into themitochondria via carnitine palmitoyltransferase. Beforecytoplasmic LCFA-CoA undergoes fatty acid β-oxidationin the mitochondrial matrix, it must be transported intothe mitochondrial membranes. This process wouldrequire the aids of several enzymes to be highly expressedin the outer mitochondrial membranes, as they cannotfreely diffuse into the mitochondrial. Carnitine-dependenttransport system is known as a central system in regulatingandmodulating the LCFA transportation in the outer and in-ner mitochondrial membrane. The system consists of carni-tine palmitoyl-transferase I (CPT-I), carnitine-acylcarnitine
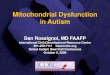
translocase (CACT) and carnitine palmitoyl-transferase II(CPT-II) [67]. CPT-I is the rate-limiting enzyme that cataly-ses the addition of carnitine into the LCFA-CoA towardsthe formation of acylcarnitine in the mitochondrial inter-membrane. Acylcarnitine is transported into the mitochon-dria matrix with the aid of shuttle transporter CACT,whereby CPT-II reverts the action of CPT-I by reconvertingthe acylcarnitine into long chain fatty acyl-CoA and carni-tine. Later, carnitine is transported back into the mitochon-dria membranes to be utilized for the subsequent reactions[67]. Lastly, LCFA-CoA enters into the β-oxidation process,producing acetyl-CoA, and enters into the TCA cycle andETC for the cellular energy generation. The overall mecha-nistic interaction of carnitine transport system in regard tothe LCFA oxidations in normal and insulin resistancesubjects is summarized in Figure 1.
The capacity of this carnitine system for the transporta-tion of LCFAs into mitochondria heavily depends upon theexpression of CPT-I enzymes, which is controlled by theallosteric inhibitor malonyl-CoA and citrate. The formation
Figure 1. Schematic representation of the long chain fatty acid (LCFA) oxidation in mitochondria for both normal and disease states.Activation of fatty acids (fatty acyl-CoA) is the rate-limiting step in β-oxidation in mitochondria. The transfer of carnitine to LCFA-CoAto form long chain acylcarnitine is catalysed by carnitine palmitoyl-transferase I (CPT-I). Once inside the mitochondria, carnitinepalmitoyl-transferase II (CPT-II) reforms LCFA-CoA, which undergoes β-oxidation generating acetyl-CoA molecules. However, anaccumulation of LCFA in the cytosol required high amounts of the carnitine transport system to be expressed in mitochondrial mem-branes. Besides, in the events of abnormal accumulation of LCFAs, malonyl CoAs are synthesized by carboxylation of acetyl-CoAcarboxylase irreversibly that inhibits CPT-I activity, thus inhibiting β-oxidation by preventing entry of activated fatty acids into themitochondria. As a result, these mechanisms lead to the build-up of lipid intermediates that can exert their deleterious effects onmitochondrial membranes. CACT, carnitine-acylcarnitine translocase; CAT, carnitine-acetyl transferase; ACC: acetyl-CoA carboxylase;CoA: coenzyme A
Long Chain Fatty Acids Induced Mitochondrial Dysfunction in Insulin Resistance
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

of malonyl-CoA in the cytosol is catalysed by acetyl-CoAcarboxylase (ACC) via carboxylation of cytosolic acetyl-CoA. Thus, in order to increase the transportation of LCFAsinto mitochondria, the inhibition of the CPT-I enzyme mustbe resolved first. This can be achieved via direct phosphory-lation of ACC and the reduction of malonyl-CoA synthesiswith highly expressed of CPT-I enzyme activities [68]. Inobese and insulin-resistant individuals, the relative rate ofmitochondrial LCFA uptakes in the number of peripheraltissues such as skeletal muscles and liver is significantlyreduced. As compared with the healthy control, obesegroups exhibit almost 35% lower CPT-I activity withprofound 50% decrease of fatty acid oxidations [69]. In ad-dition, the increased expression of ACC activity at the basallevel was reported in insulin-resistant subjects. The high-level expressions of this enzyme later stimulate the synthe-sis of malonyl-CoA to inhibit CPT-I activity, resulting in theaccumulation of lipid intermediates in the cytosol [70].
β-oxidation is one of the important processes in mito-chondrial fatty acid catabolism to produce acetyl-CoAand shortened fatty acyl-CoA towards energy productionin mitochondria. A concept of the incomplete β-oxidationcycle was introduced to manifest the condition of lipidoversupply that increased fatty acid oxidation withoutthe activation of the TCA cycle and ETC in the process[71,72]. This process promotes the unusual accumulationof lipid intermediates such as acylcarnitine in the mito-chondrial membrane and exerts its damaging effects intovarious metabolic signalling activities of mitochondriametabolism. Several experimental and clinical studiesrevealed that the acylcarnitine profile of marker incom-plete β-oxidation in the blood and urine is significantlyamplified in both animal and type 2 diabetic patients com-pared with control [71,73,74]. Acylcarnitine is known toaffect the mitochondrial protein within the plasma mem-brane by acylation and acetylation [75,76]. Additionally,incomplete β-oxidation may also lead to the accumulationof reactive oxygen species (ROS) that exacerbate the lipidperoxidation rates towards damaging the mitochondrialprotein and DNA [77]. The inflammatory responsethrough the activation of JNK and IKKβ protein isactivated with the increases of ROS production in themitochondrial membrane [48]. In spite of that, the exactmechanism by which this aberrant process in β-oxidationleads to insulin resistance remained to be elucidated.
LCFA-inducedmitochondrial dysfunctionleads to insulin resistance
Themetabolic associations betweenmitochondrial dysfunc-tion and insulin resistance were studied as early as in the1963 [78]. Later in 2000, it was found that elder people
exhibited skeletal muscle insulin resistance with the signif-icant decrease (~40% lower) of the mitochondrial oxida-tive phosphorylation level compared with the younggroup [79]. Mounting evidence indicates that the circulat-ing FFAs in the blood play a vital role in the developmentof insulin resistance [8,80,81]. Insulin responsive tissuessuch as skeletal muscle and adipose tissue metabolize bothglucose and FFAs for energy production. In the cell, glucoseis broken down into pyruvate, which is converted to acetyl-CoA, by the enzyme pyruvate dehydrogenase in themitochondria. Fatty acids are first metabolized to severallipid intermediates in the cytosol in order to be transportedintomitochondria and catabolized towards the formation ofacetyl-CoA via β-oxidation. Later, acetyl-CoA is converted tometabolic intermediates in the TCA cycle with the genera-tion of several reducing equivalents such as NADH andFADH2. The regulation of these metabolic activities in fattyacids and glucosemetabolism is tightly coordinated in orderto prevent any development of metabolic defects. Theability of various peripheral tissues to switch from fatoxidation during fasting to glucose oxidation after a mealis referred to as metabolic flexibility [82]. Insulin resistanceand obesity are characterized by the ‘metabolic inflexibility’due to the total impairment of substrate preference betweenglucose and fatty acids in fasting and insulin-stimulatedconditions [83].
Insulin resistance is an integral event to the pathophys-iology of obesity-related metabolic abnormalities and type2 diabetes [84]. This metabolic impairment is defined asone of the systemic adaptations of the body in the formof underutilized glucose uptake in specific tissues suchas liver, adipose tissue and skeletal muscles [85]. Obeseindividuals are at an increased risk of developing a rangeof chronic health problems such as cardiovascular disease,diabetes, hypertension, non-alcoholic fatty liver andcertain cancers [86]. The influence of obesity on the riskof type 2 diabetes is determined not only by the degreeof obesity but also by the site where the fat accumulates[87]. The excess accumulation of FFAs in the adiposetissue may systematically lead to the increased rate oflipolysis in the body. In the event of increased lipolysis,there is an augmented flow of non-esterified LCFAs intoskeletal muscle, resulting in the excessive muscular fatstorage, associated with the insulin resistance [88].Prolonged exposure of LCFAs into numerous targettissues activates deleterious mechanisms of the glucose–fatty acid vicious cycle that inherently lead to the mito-chondrial dysfunction and insulin resistance [66]. Thepresent research study provides additional evidence withrespect to the role of LCFA-induced mitochondrial dys-function via several adaptive mechanisms of metabolicdysfunctions in cellular and systemic profiles of the hu-man body. Therefore, we proposed the idea that LCFAsmay synergistically induce these intricate mechanisms
M. H. A. Bakar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

towards the notions of ROS-induced oxidative stress,lipotoxicity, significant alterations of mitochondrial geneexpression and activation of inflammatory signallingpathways in the development of insulin resistance andtype 2 diabetes.
High level of reactive oxygen species
One of the popular postulations underlying mechanismsof diabetic complications is oxidative stress, which arisesfrom the excessive production of free radicals from avariety of sources, especially from the diet. It is estimatedthat 57.9% of diabetes subjects experience microvascularor macrovascular complications that are significantlyrelated to the oxidative stress [89]. The oxidative stressis the cellular adaptation of certain target tissues inresponse to the overproduction of ROS. The cross-talkbetween the oxidative stress and insulin resistance hasbecome one of the central issues in diabetes complications[90,91]. ROS can rapidly react with a wide range of mac-romolecules such as lipid, amino acid, carbohydrate andmtDNA. The resultant molecules are produced throughsevere modifications in the chemical structure to becomehighly cytotoxic and reactive. Consequently, these mole-cules may exert their biological effects in intracellularinsulin signalling activity, which lead to the irreversibledestruction of the cell functions [92,93].
Generally, LCFAs alter the mitochondrial respirationtowards producing excessive ROS via two ways: (1)partial blocking of mitochondrial respiratory chain activi-ties and (2) depolarization of mitochondrial inner mem-brane (the uncoupling effects) [94]. The stimulatorymechanism of these processes is believed to be regulatedthrough the damage of cytochrome c from the externalside of the mitochondrial inner membrane. In case ofoxidative stress, previous studies showed that the impair-ment of mitochondrial ETC Complexes I and III is themajor source of the free radical superoxide production indiabetes [95]. These superoxide molecules are releasedinto mitochondrial intra-membrane space and matrix.When the level of these reactive superoxide moleculesexceeds antioxidant capacity of the cell to neutralizethese free radicals, cellular damage may occur. Theaccumulation of oxidized product of lipids, DNA andrelated glycolytic products is prominent to be detectedin the plasma, urine and various target tissues, suggestingthat the systemic and local manifestation of these condi-tions has exacerbated the diabetes complication with direconsequences [96,97].
The production of ROS in mitochondria is stimulatedfrom a variety of complex biological processes by involv-ing certain activation of enzyme kinases such as NADPHoxidase and nitric oxide synthase in the mitochondria
[77,98–100]. The elevation of ROS production by themitochondria is usually followed by the increased concen-tration of plasma FFAs that are highly susceptible to alterthe oxidative metabolism of numerous insulin responsivetissues [101,102]. Indeed, LCFAs, especially the unsatu-rated ones, are prone to oxidative damage [103]. Severallines of studies have identified that the chronic elevationof lipid intermediates is implicated with the increaseof ROS production [104,105]. The accumulation ofROS may worsen the inner membrane of mitochondria(cardiolipin-enriched in polyunsatutared fatty acids)[106]. These accumulations consequently cause damageto the mitochondrial machinery that consists of theelectron transport chain and their downstream effectors.This condition indirectly activates the negative feedbackmechanism via lowering the expression of various mito-chondrial gene expressions and proteins. Eventually, thiscellular behaviour results in the decline of mitochondrialactivities to metabolize lipid efficiently, giving rise to anabnormal accumulation of lipid intermediates in the innermembrane of mitochondria and cytosol. This metabolicadaptation is usually observed in pre-diabetes patients,as their skeletal muscles and liver contain a high amountof lipid intermediates and increased rate of lipid peroxida-tion [20,107,108]. Besides, the oxidative stress alsoactivates several oxidation and reduction processes ofcellular protein via sulfhydryl groups of cysteine inproteins and later affects several major functions of theperipheral cells in regulating the cellular homeostasisand numerous biological pathways [109]. Thus, it is notsurprising to know that the imbalance of these redoxreactions inherently exacerbates the cellular function inthe intracellular signalling process, hence contributing tothe development of the disease.
Works by Anderson and colleagues have identified thatthe level of mitochondrial H2O2 was significantlyaugmented in both human and rodents following a high-fat diet meal [110]. They also observed several significantchanges through the reduction of the mitochondrial redoxbuffering capacity after a high-fat diet meal. In addition,the 6-week attenuation of these superoxide moleculeswith mitochondrial targeted-antioxidant resulted in theimprovement of glycaemic control and insulin sensitivity,and ameliorates the detrimental effects by high-fat diet.However, in overweight Zucker rats, the emissions ofmitochondrial H2O2 were significantly increased in ratskeletal muscle. The study also found that in vivometformin(anti-diabetic drug) treatment that was continued for about4 weeks altered the mitochondrial respiration rate throughsignificant decline of mitochondrial H2O2 emission inskeletal muscle of obese rats [111], signifying that thepotential antioxidant-attenuated ROS is directed via theimprovement of mitochondrial functions. Furthermore,in vitro studies that utilized LCFAs as substrate oxidation
Long Chain Fatty Acids Induced Mitochondrial Dysfunction in Insulin Resistance
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

in endothelial tissue and skeletal muscle also resulted in theincrease of ROS productions in mitochondria [112,113].Current studies also documented that the treatment ofLCFA such as linoleic acid on 3T3-L1 adipocytes contributesto the excessive accumulation of ROS with the significantdecrease of glucose uptakes/utilizations as well as acti-vates various levels of inflammatory signalling cascadepathways [114]. As diabetes is strongly associated withother complications such as neuropathy, it was observedthat the human neuronal SK-NB-E cells treated withVLCFAs (C22:0, C24:0 or C26:0) for 48 h result in severemodifications of mitochondrial integrity and morphol-ogy, resulting in the development of oxidative stress andmitochondrial dysfunctions [115].
Several studies suggest that oxidative stress also af-fects the mitochondrial activities and its morphology.The oxidative damage induces an accumulation of cell-damaged mitochondria and blocks various distinct pro-cesses in mitochondrial activity such as the electrontransport chain, β-oxidation and TCA cycle [91]. Theimpairment of mitochondrial function causes a reducedactivity of rotenone-sensitive NADH: O2 oxidoreductase,citrate synthase and creatine kinase activity [116]. Thesame study also observed that mitochondria in skeletalmuscle of patients with type 2 diabetes were muchsmaller, and abnormal morphology was clearly observedcompared with the control group. The impaired mito-chondria functions directly contribute to insulin resis-tance with a couple of defects in glucose and lipidmetabolisms because of the disturbed oxidative phos-phorylation capacity as well as the inefficient provisionof ATP for hexokinase activity [117]. An in vitro cell-based assay study indicates that chronic exposure of3T3-L1 adipocytes to high concentrations of glucoseand fatty acids caused a decrease in the mitochondrialmembrane potential, morphology changes and down-regulation of peroxisome proliferator-activated receptorgamma (PPARγ) co-activator 1-alpha (PGC-1α) with thesignificant increase of ROS [24]. In 3T3-L1 pre-adipocyte,several mitochondrial inhibitors impaired mitochondrialrespiration, leading to the abnormal triglyceride accumu-lation. High levels of ROS concentrations in mitochondriaby respiratory chain were reported to exert several delete-rious effects on the adipocyte proliferation and differentia-tion [118].
A damaged mitochondria membrane induces accumula-tion of ROS in the cell and may indirectly affect mitochon-drial DNA, RNA and proteins [93]. As a result, theactivation of the chronic inflammatory pathways is directedto signal the event of these oxidative damages. Increase ofan electrochemical gradient across the membrane exacer-bates the cell to undergo oxidative damage by elevatingthe ROS production. Clearly, these findings suggest a roleof a high level of ROS that is highly dependent on the
proton gradients over the inner membrane of mitochondriathat consists of ATP synthase for ATP production. However,in spite of accumulating findings for the role of LCFA-induced ROS accumulation in the development of suchdisorder, there are also several lines of studies depictingthat insulin resistance can occur without any exacerbationsof mitochondrial oxidative properties [20,119–121]. Thus,further studies are strongly needed to be performed inorder to enhance our understandings related to the exactroles of LCFA-induced oxidative stress in the developmentof such impairments. Taken altogether, these studies mightsubstantially add into our current understanding of patho-physiological mechanisms underlying insulin resistanceand type 2 diabetes pertaining to the interaction betweenmitochondrial functions and LCFA availability.
Altered pattern of mitochondrial geneexpression
Mitochondrial activity is a highly coordinated process thatrequires a considerable amount of controlled signals inthe forms of enzyme and growth factors from bothmitochondria and nuclear genomes. These complexsignals can act as metabolic sensors that mediate anyvariation in biological perturbations of cellular and sys-temic profiles of the human body. The metabolic activitiesin mitochondria such as β-oxidation, the TCA cycle andelectron transport chains are heavily dependent uponthe regulation of these cellular machinery genes andproteins. Previous studies reported that a significantamount of deletion andmutation inmtDNA (m.3243A>G)and its related nuclear encoded proteins is criticallyassociated with the development of insulin resistance andtype 2 diabetes [122–125]. Several distinct mitochondrialsingle nucleotide polymorphisms are also linked with suchperturbation [126]. Any deficiency or disturbance in thesemitochondrial genes and protein networks may contributeto the dysregulation of mitochondrial gene expressionsand affects the integrity of the mitochondrial dynamicprocess. Indeed, the reduction of these key proteins isimplicated in the pathogenesis of insulin resistance andendothelial dysfunction in diabetes [127]. In the event ofmetabolic defects such as type 2 diabetes, insulin resistanceand ageing, the integrity of these machinery genes andproteins involved in the mitochondrial biogenesis andmetabolism is totally diminished at various levels of adisease process [17,20,128].
Recent review from Joseph and his colleagues highlightedseveral important issues concerning the dysregulated mito-chondrial gene expression networks and its protein variousmetabolic defects in the progression of insulin resistanceand type 2 diabetes [129]. A number of experimentalstudies also showed that the cellular mechanistic
M. H. A. Bakar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

adaptations of skeletal muscle in obese and type 2 diabe-tes subjects concomitantly alter the integrity of severalvital genes responsible for glucose metabolism, fatty acidoxidation and oxidative phosphorylation [21,22]. Worksby Turner groups have compared the effects of fatty acidswith different carbon chain lengths (LCFA vs MCFA) inrodents by evaluating their insulin actions and mitochon-drial functions [16]. They have found that rodents thatwere fed with MCFAs exhibited an increase of themarkers in mitochondrial metabolism up to 50–140%(vs low fat-fed controls, p< 0.01) while groups that weretreated with LCFA diet only increased 20–50% (p< 0.05)of markers for mitochondrial metabolism in skeletalmuscle compared with low-fat diet-fed controls. Inaddition, mice fed with MCFA diet did not suffer fromsevere triglyceride accumulation in skeletal muscle com-pared with mice groups fed with LCFAs that exhibitedthe lipotoxocity properties with a significant increase of77% intramuscular triglycerides. The same study alsofound that the mice treated with MCFA diet led to theimprovement of insulin sensitivity in skeletal muscleand adipose tissue. In addition, glucose tolerance in thisgroup treated with MCFA was significantly improved ascompared with the other group that was fed with LCFA-rich diets [16], indicating the possible roles of LCFAs inthe regulation of insulin resistance and lipotoxicity-related events.
The PGC-1 family is a member of the nuclear receptor su-perfamily that is mainly responsible for the mitochondrialbiogenesis andmetabolism. This protein is metabolically in-volved in various biological regulations co-activated withother key transcription factors such as nuclear respiratoryfactor-1 (NRF-1), estrogen-related receptor-α (ERRα) andPPARβ or PPARγ [130,131]. The following studies alsoidentified that PPARs directly participate in regulating themitochondrial gene subsets and fatty acid oxidation as wellas becoming one of the inducers for the uncoupling mecha-nism [130,132]. The increase of LCFA concentration in anumber of peripheral tissues stimulates these receptorsand numerous biological signalling activities throughdirect inhibitions of intracellular insulin signalling andAMP-protein kinase (AMPK) phosphorylation [133].PPARα is ubiquitously expressed in liver, heart, kidney,intestine, pancreas, skeletal muscle and brown adiposetissue. It is responsible for the expression of diverse mito-chondrial genes that are essentially involved in fatty acidsand glucose metabolism. This protein is also recognizedas one of the molecular sensor for various types of fattyacids and other lipid derivatives – due to its naturalligands that include polyunsaturated fatty acids. Theaction of this protein is stimulated through various multi-ple target genes that are strongly correlated with theincrease of CPT-1a expression, the rate-limiting enzymeof β-oxidation in mitochondria. It is also a regulator of
CD36, lipoprotein lipase, UCP-3 and potentially pyruvatedehydrogenase kinase-4 (PDK-4) [134].
Long chain fatty acids activate the expression ofseveral genes involved in the lipid and glucose metabo-lism via stimulation of CPT-1 and PDK-4 [135]. How-ever, the elevated level of plasma FFA may inducedetrimental effects on the expression of these enzymesto cause loss-of-functions due to the heavy metabolicdemands. Corroborating with these facts, it was dem-onstrated that the chronic exposure of LCFAs inskeletal muscle apparently results in significant alter-ation of PGC-1 functions [104,105,136,137]. In healthymales, 3 days of high-fat feeding resulted in a signifi-cant decline of PGC-1α and PGC-1β expression [138],while similar effects were also observed in 6-h lipidinfusion into healthy subjects that resulted in thedown-regulation of PGC-1α, PGC-1β and PPARα expres-sion [139]. Another study reported that 3 weeks ofhigh-fat diet in healthy mice led to the down-regu-lation of mitochondrial genes and enzyme expressionsuch as PGC-1α and several protein components of themitochondrial ETC [140]. To strengthen this finding,the same study also observed that the treatment ofTroglitazone (an insulin sensitizer) in Zucker rat showeda significant increase of PGC-1α and NADH dehydroge-nase subunit 1 expression level, indicating that the regu-lation of mitochondrial genes subsets is considerablyimplicated in the development of insulin resistance andtype 2 diabetes.
Furthermore, a high amount of intramyocellular lipidcontent is linked to the down-regulation of PGC-1αexpression and other gene-encoding protein for mitochon-drial respiratory chain complexes I, II, III and IV [138]. Inadipose tissues, the reduced expression of PGC-1α inwhite adipose tissue of rat also leads to the accumulationof lipid intermediates that is concomitantly associatedwith a significant reduction of gene expression regulatinglipid and glucose metabolism in the respected tissue[141]. One study confirmed that the NRF-1 is a down-stream target transcription of mitochondrial genesresponsible for the mitochondrial dysfunction in insulinresistance. The authors found that NRF-1 expression wassignificantly reduced as parallel with the lowered level ofmitochondrial genes and protein expression [142,143].Besides, these metabolic changes in gene expression alsocontribute to the accumulation of intramyocellular lipidcontent in the mitochondrial matrix that leads to theinsulin resistance [17,21]. As PGC-1α is a transcriptionalco-activator of NRF-1, PPAR and growth associated-bindingprotein in the mitochondria, it is tempting to hypothesizethat any alteration of PGC-1α gene expression mayregulate other mitochondrial genes and proteins. There-fore, any suppression or loss-of-function of these vitalgenes may result in the impairment of fatty acids and
Long Chain Fatty Acids Induced Mitochondrial Dysfunction in Insulin Resistance
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

glucose oxidation that leads to the development of mito-chondrial dysfunction and insulin resistance.
Nevertheless, all the studies reviewed so far in regardto the dysregulated mitochondrial genes and proteinnetworks in the development of insulin resistance sufferfrom conflicting results, which indicate that the improve-ment of insulin sensitivity was not necessary to beaccompanied by an increase of mitochondrial geneexpression and proteins. Oikari et al. (2008) have suc-cessfully shown that 4-week treatment of LCFAs in ratsincreased mRNA expression (1.5–3.5-folds) of liverPPARs and sterol regulatory element-binding transcrip-tion factor-1 (SREBP-1) compared with the controlgroups [144]. However, as compared with control, theprotein levels of AMPKα were depleted by 48% with nosignificant changes observed in glucose and insulin levelsof rat fed with LCFA diets. This study indicates that anyenhancement of insulin sensitivity is not necessarilyaccompanied with the up-regulated mitochondrial geneexpressions. Similarly, the same study also observed thata diet with MCFAs reduced liver PPARγ and SREBP-1mRNA levels by 43% and 35%, respectively, while themRNA level of PPARγ expression in adipose tissue wasup-regulated by 31%. An improved glucose toleranceand lower serum insulin level were reported in thisgroup compared with the control, signifying that thedecreases of several mitochondrial gene expression andproteins were not necessarily associated to the evolve-ment of insulin resistance. In addition, another studyfound that the reduced mitochondrial protein contentsof transcription factors including PGC-1α and PGC-1βand proteins associated with mitochondrial fusion eventsin skeletal muscle are not correlated with the progres-sion of insulin resistance and obesity [145], clearlywarranting further detailed investigations to elucidateand understand these complex mechanisms underlyingthe disease.
Mitofusin 2 (Mfn2) is known as one of the key proteinsthat are directly involved in the biological process of mito-chondrial membrane metabolism. The expression of Mfn2genes and its proteins was reduced in the human skeletalmuscle of insulin and diabetic Zucker rat (ob/ob) with thesignificant decrease of glucose oxidation rate [146].Another study confirmed that the Mfn2loxP/loxP miceexhibit insulin resistance with a profound increase ofendoplasmic reticulum stress and enhanced inflammatorysignalling pathways [147]. The study was then furtherverified in rats that were fed with a high-fat diet rich withsaturated LCFAs that exhibit insulin resistance withlowered expression of Mfn2 in the skeletal muscle [148].Furthermore, in agreement with the aforementionedstudies, Gan and colleagues identified that the over-expression of Mfn2 genes in a group of rats showedameliorative properties against a high-fat diet-induced
insulin resistance [149]. The study also specifically ob-served that the glucose infusion rate was also improvedbecause of the increase of expression and phosphoryla-tion of insulin receptors that lead to the stimulation ofglucose transporter synthesis within the liver. Neverthe-less, the specific role of Mfn2 in the regulation of energymetabolism of lipid-induced insulin resistance and type 2diabetes is not well understood. In spite of severalconflicting results in the studies, these observations havefostered our understanding by supporting the ideas thataccumulation of FFA especially LCFAs may have severaldetrimental effects via rigorous alteration in geneexpression of mitochondrial biogenesis and metabolismthat become one of the principal contributors to theobesity-associated diminished insulin sensitivity in vari-ous peripheral tissues.
Accumulation of lipid intermediatesinduced lipotoxicity
Obesity is one of the major risk factors involved in theprogression of insulin resistance and type 2 diabetes[8,87]. An inverse relationship between insulin sensitiv-ity and adipose tissue mass was critically reviewed[150,151], indicating the roles of adipose tissue func-tions in regulating lipid and glucose metabolism. Inhealthy humans, the dynamic amount of fatty acidstorage and its release into the blood circulation is tightlycoordinated based on metabolic demands. Excess accu-mulation of LCFAs in adipose tissues may lead to thehypertrophic adipocytes. These conditions exert aphysiological stress on their cellular functions and laterinduce them to transform into inflamed adipocytes withthe activation of inflammatory response via recruitmentof tumour necrosis factors-α (TNF-α) and macrophage-migration-inhibitory-factor and nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB). Thedownstream effects of these mediators lead to variouscellular dysregulation including apoptosis, mitochon-drial dysfunctions, endoplasmic reticulum (ER) stressand insulin resistance [152–154]. Because of these cellu-lar consequences, the inflamed adipocytes exhibitvarious metabolic malfunctions in terms of glucose andlipid oxidation, storage and uptake that lead to thehigher rate of lipolysis and excess non-esterified LCFAs[155]. In these conditions, the accumulation of theseLCFAs is directed to be catabolized in the other periph-eral tissues such as skeletal muscle and liver that havea very limited storage capacity for lipid [156]. It usuallyoccurred when the amount of lipid intermediates isamplified in adipose tissue and exceeds its own capacityto store and metabolize lipid for energy production.Lipotoxicity is defined as the accumulation of excess lipids
M. H. A. Bakar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

in non-adipose tissues such as skeletal muscle and liver,resulting in an increase of mitochondrial stress, activationof inflammatory pathways, reduced glucose uptakes and in-sulin resistance [86]. Numerous evidence indicated that theaccumulation of non-esterified LCFAs is strongly associatedwith the insulin resistance [157,158]. Indeed, high levels ofectopic lipid accumulation are concomitantly associatedwith type 2 diabetes and lipotoxicity [159,160].
It was scientifically observed that plasma FFA levelswere augmented in obese and diabetic patients [101,161].In the long run, high amounts of FFA levels together withdiminished fat oxidative capacity contribute to the accumu-lation of LCFA intermediates in several insulin responsivetissues other than adipocytes [156]. On the other hand,the consumptions of other types of fatty acids such asMCFAs were not led to the ectopic accumulation of lipidintermediates in the liver and skeletal muscle of rat andmice [162,163]. Intracellular fatty acid intermediates accu-mulate in myocytes, mainly in the form of LCFA-CoA,monoacylglycerol, diacylglycerol, phosphatidic acid, triac-ylglycerol and ceramide [18,32,143,164,165]. Theprimary defects in the metabolic capacity of mitochondrialfatty acid oxidation may result to the accumulation ofthese lipid intermediates [166]. Numerous studies werepublished in regard to the obvious observations of non-esterified LCFA build-up in skeletal muscle and liver thatcan essentially contribute to the development of insulinresistance [29,164,167].
Ceramide and diacylglycerol are believed to be themost deleterious mediators that can interfere and inhibitvarious levels of insulin signalling cascade pathwaysthrough the decrease of mitochondria functions [31].The elevated concentration of LCFAs within the cellexacerbates the abnormal accumulation of diacylglyceroland ceramide to activate protein kinase C theta thatinherently results in the phosphorylation of serine 307residue of insulin receptor substrate 1 (IRS-1). Intrinsi-cally, this occurrence is directed towards the inhibitionof tyrosine phosphorylation and impaired insulin signal-ling [168]. According to these crucial insights, recentwork also supports several issues pertaining to the roleof PKC in LCFA intermediate-induced insulin resistancevia inhibition of insulin-stimulated phosphatidylinositol-3-kinase activity [169]. Nevertheless, there is no reliableevidence that explained on how the activation of PKC isrelated to serine phosphorylation of IRS-1 in inhibitingthe phosphorylation of tyrosine residues [164], suggest-ing well-designed experimental studies to be furtherimplemented.
Ceramide is a family of intermediate lipid species thatprofoundly functions as signalling molecules to signalapoptosis and inhibit cell division [170]. There is anexpanding amount of studies that indicate the reciprocalrelationship between the ceramide contents and the
development of insulin resistance [169,171,172]. Pro-longed exposure of ceramide in skeletal muscle, liverand heart tissues may directly suppress the activity ofComplexes I and III in the mitochondrial electron trans-port chain system [173,174]. A study confirmed that cer-amide treatment affects the mitochondrial integrity viareduced mitochondrial respiration and Akt/PKB phos-phorylation in the skeletal muscle [175]. While in liver,it was showed that the excessive formation of ceramidein mitochondria is directly derived from LCFA intermedi-ates such as sphingosine and palmitate [176]. The eleva-tion of ceramide contents in skeletal muscle of obesesubjects was also accompanied by a deterioration of oxi-dative capacity via reduced fatty acid oxidation and mito-chondrial functions [177]. Importantly, an excessiveaccumulation of ceramide contents was reported in theskeletal muscle of insulin-resistant animals [157], obeseinsulin-resistant humans [161] and lipid infused humans[178]. High amount of ceramide level in various periph-eral tissues is a consequence of sphingomyelin hydrolysis(a plasma membrane constituent), which is catalysed bysphingomyelinase [179]. Alternatively, ceramide can beformed via a series of metabolic reactions between twofatty acids and serine in four enzymatic steps [180]. Thefirst step is rate limiting, catalysed by serine palmitoy-ltransferase, which specifically entails LCFAs as the sub-strate. Thus, the increase of LCFA uptake by the skeletalmuscle or inhibition of stearoyl-CoA desaturase-1 activitymay promote the accumulation of ceramide in the skeletalmuscle [181,182] and exert their effects on mitochondrialfunctions. Moreover, other studies have shown that a dietrich in LCFAs especially palmitic acids significantly leadsto the abnormal accumulation of ceramide contents in theskeletal muscle of mice and rats [183,184]. In human, theconsumption of polyunsaturated LCFAs such as conjugatedlinoleic acid (CLA) as a weight-loss supplement is alsocontroversial [185]. The study observed that 4 g/day ofmixed CLA isomers given to the subjects for 12 weeksaffects the insulin signalling activity via the elevation ofintramuscular ceramide contents. The accumulation of cer-amide content causes a significant decrease of insulin sensi-tivity in skeletal muscle of overweight subjects (p≤ 0.05)compared with controls [185], implying the roles of LCFAsthat significantly contribute to a high amount of ceramidecontents in this peripheral tissue.
A number of studies have found that the diacylglycerollevel in the skeletal muscle of obese and insulin-resistantsubjects is negatively correlated with the improvement ofinsulin sensitivity and glucose uptake [168,172,186,187].The accumulation of diacylglycerol content in hearttissues of C57BL/6 mice that were fed with a high-fatdiet was also found to affect the insulin signalling path-ways via phosphorylation of p70s6 kinase and transloca-tion of PKC-α [188]. The intravenous lipid infusion
Long Chain Fatty Acids Induced Mitochondrial Dysfunction in Insulin Resistance
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

into12 healthy men over 6 h results in the total reductionof the whole body insulin sensitivity because of abnor-mal accumulation of diacylglycerol in the skeletal muscle[168]. Surprisingly, a diet rich in unsaturated LCFAssuch as oleic and linoleic acids also contribute to the sig-nificant accumulation of diacylglycerol contents [186].Another report by employing 12 lean male offspring oftype 2 diabetic patients and 21 men with overweight orobesity found that the elevations of intramuscular diacyl-glycerol contents are strongly associated with the devel-opment of insulin resistance [172]. These findings arealso supported by Todd and colleagues who observedthat the rats that were fed with a high-fat diet result indecreased insulin-stimulated glucose uptake togetherwith the augmented diacylglycerol contents in skeletalmuscle [189]. Additionally, these detrimental effects ofincreased diacylglycerol level in the peripheral tissueon insulin signalling transduction pathways were associ-ated with the activation of inflammatory response viaactivation of novel protein kinase C. Later, this metabolicconsequence activates the signalling pathways of NF-κβand insulin-dependent activation of mTOR/p70s6k,causing the phosphorylation of serine residues of IRS-1 as well as inhibition of the PI3K/AKT pathway [190–192]. All in all, high amounts of LCFA intermediatessuch as LCFA-CoAs, diacylglycerol and ceramides in cy-tosol may synergistically act towards diminished oxida-tive capacity of various peripheral tissues via reducedmitochondrial respirations.
Activation of inflammatory signallingpathways and endoplasmic reticulumstress
The links between the inflammation and insulin resistancein studying the roles of LCFA-induced insulin resistance arerecently emerged in numerous publications [193–195].Obesity has been well recognized as the low grade ofsystemic chronic inflammatory conditions that activatethe metabolic activity of a number of circulating cytokinesin the body. The activation of these inflammatory signalsin various peripheral tissues may interfere with the intra-cellular insulin signalling actions and inherently lead tothe disruptions of metabolic homeostasis as a whole. Inparticular, these signals are directed towards the stimula-tion and activation of JNK isoforms in macrophage anddirectly induce posttranslational modification of IRS mole-cules via direct activation of serine residues in liver andskeletal muscle [196]. It has become increasingly apparentthat the activations of these signalling pathways are clearlyoriginated from accumulation of LCFAs and lead to theformation of lipid intermediates such as diacylglyceroland ceramides in adipocytes and skeletal muscle and result
in the excessive stimulations of pro-inflammatory media-tors [152,197,198].
The intracellular inflammatory signalling pathways areactivated by LCFAs by their binding into Toll-like receptorfamily, especially TLR-4 [199,200]. TLRs are a family ofevolutionary conserved receptors that specifically recog-nize pathogen-associated molecular patterns by facilitatingthe presence of microbes. A number of studies indicate thatthe TLR-4 is one of the key regulators of insulin resis-tance that contributes to the stimulation of these inflam-matory signalling pathways in obesity and insulinresistance. The activation of TLR-4 acts as a metabolicsensor that is capable to detect high amounts of plasmanon-esterified LCFAs and exogenous ligands from vari-ous dietary fatty acids that are profoundly present inobese states [201,202]. In particular, the possible mech-anism of TLR-4 activation in the mammalian system issuggested through binding to a ligand of lipopolysaccha-rides (LPS) in the cell wall of gram-negative bacteria.LCFA is one of the main components of the lipid part ofLPS, which is Lipid A. The presence of Lipid A could bedetected by TLR-4 and sufficiently enough to triggerthe TLR-4 activation and its downstream signallingcascade in a macrophage cell line [203]. The release ofTLR-4 in skeletal muscle directly activates the c-Jun NH(2)-terminal kinase (JNK) and Iκb kinase (IKK) com-plexes that inherently lead to the down-regulation ofthe inhibitor of κB (IκBα) and NF-κB. As a result, theseconditions drive the transcription of a variety of pro-inflammatory genes and proteins [204,205]. Furtheron, another study also showed that the LCFAs and lipidinfusion through in vitro and in vivo observed thesignificant activation of TLR-4/NF-κB in the skeletalmuscle [195].
Long chain fatty acids initiate the activation of TLR-4via direct stimulation of JNK and IKKβ signalling path-ways with the alteration of intracellular insulin signallingand inhibition of phosphorylation in tyrosine residues ofIRS-1 [195,206]. Consequently, the serine phosphoryla-tion is significantly activated to signal the inhibition ofglucose transporter, GLUT4, to the cell membrane. Theseobservations are in accord with one study to understandthese metabolic impairments through lipid infusion into.They have found that the TLR-4 knockout mice did notexhibit insulin resistance in the skeletal muscle, which ap-parently pointed out to an important role of the activationof TLR-4 in LCFA-induced insulin resistance in vivo [207].Similarly, mutated mice with the loss-of-function in TLR-4genes escaped from developing any condition of insulinresistance and accompanied by the reduced NF-κB andJNK activation, although feeding with high-fat diet[208]. In addition, the isolated muscles from these micewere protected from the saturated LCFA-induced insulinresistance by deactivating the TLR family [209–211]. An
M. H. A. Bakar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

in vitro study also showed that the insulin signalling path-way was not altered by deleterious effects of palmiticacids in L6 myotubes by blocking TLR-4 protein, indicat-ing that this fatty acid requires TLR-4 protein to be signif-icantly expressed in various peripheral tissues [210].Thus, it can be postulated that to hold the idea of TLR-4activation by LCFAs might be one of the particular eventsthat lead to the activation of inflammatory signallingpathways.
Furthermore, several studies have indicated that LCFAsalso facilitate the secretion of several other cytokines,including TNF-α, interleukin-1β, plasminogen activatorinhibitor-1, C-reactive protein and interleukin-6 (IL-6)[212–214]. These reports are in accordance with anotherstudy where it was clearly observed that the concentra-tion levels of these inflammatory mediators significantlyamplified in obese and insulin-resistant individuals, whichcould be predictive inflammatory markers for type 2diabetes [215]. The mitochondrial membrane potentialand cellular ATP contents were also significantly reducedin 3T3-L1 adipocytes exposed to IL-6 inflammatorycytokines [216]. TNF-α is found to play their metabolicfunction via direct and indirect inhibition of certain regu-latory pathways that are responsible for the glucose andfatty acid oxidations in the skeletal muscle and adiposetissues [154,217]. Similar to the aforementioned mecha-nisms, the possible mechanism involved in the activationof these inflammatory mediators is adapted via the activa-tion of PKC isoform and NF-κB, which stimulates the ser-ine kinase cascade event in the myocytes [217]. Tocorroborate with these defined mechanisms of inflamma-tory cytokines in the development of mitochondrial dys-function and insulin resistance, recent investigationssuggest that the activation of inflammatory cytokinesmay indirectly cause physiological stress in the mitochon-dria and substantially contribute to the mitochondrialdysfunction [218,219]. The release of these inflammatorycytokines leads to the advancement of aberrant mitochon-drial function as LCFAs may stimulate the release of thesecytokines in leukocytes [193,220].
Moreover, the metabolic association between theactivation of ER signalling pathways and the inflamma-tory response in people with obesity and type 2 diabetesis emerging as one of the critical risk factor componentsthat contribute to the hallmarks of such metabolicdisease [221–223]. The close interactions of mitochon-dria and ER functions are observed in modulatingvarious cellular such as mitochondrial fission, calciumsignalling and lipid flux [224]. ER is a membranous net-work that is intrinsically functioning as one of the impor-tant organelles involved in trafficking of a wide range ofproteins. Therefore, the enhancement of the metabolicsignals critical in maintaining cellular homeostasisthrough proper ER functions is necessary to modulate
the metabolic capacity of tissue during the developmentof metabolic disorders such as insulin resistance and type2 diabetes. ER stress is linked to various inflammatorysignalling pathways because of the failure of ER func-tions, particularly its folding capacity, thus triggeringthe activation of unfolded protein response (UPR)[225]. The activation of UPR may exacerbate the meta-bolic conditions via the stimulation of inert physiologicalstress and activate multiple inflammatory signals via in-flammatory NF-κB/IKK pathways in various peripheraltissues [226]. The role of LCFA-induced mitochondrialdysfunctions in regard to the activation of the UPRand ER stress is implicated in insulin resistance andtype 2 diabetes [224,227]. The activation of the UPRand ER stress is strongly associated with the excessiveproduction of ROS molecules in various peripheraltissues, leading to the development of oxidative stressand diminished mitochondrial functions [98].
Several genetic and dietary animal models that in-duced insulin resistance were used to study the roles ofER stress in the pathophysiological mechanism underly-ing these complex diseases [98,228]. To several extents,it was reported that several ER stress markers such as thephosphorylated protein kinase-like endoplasmic reticu-lum kinase and inositol-requiring enzyme 1α were ele-vated in these animal models of insulin resistance,indicating that these metabolic pathways of ER stressmay play a role for the promotion of inflammatory path-ways, insulin resistance and type 2 diabetes. The recentfindings demonstrated that obesity and type 2 diabetesare strongly associated with the compromising ER func-tions via the activation of JNK signalling pathways[226]. The activation of these pathways during ER stressdirectly regulates the expression of various inflammatorygenes in response to these adaptive mechanisms. It wasclearly showed that JNK knockout mice were beingprotected against a high-fat diet-induced insulin resis-tance. Besides, the induction of pro-inflammatory genesand cytokines such as interleukin-6 and monocyte che-motactic protein-1 in these mice also were blunted[229,230]. Current analysis highlighted several findingspertaining to the metabolic fate of LCFAs such as palmiticacid on skeletal muscle that apparently contributes to-wards the amplification of the ER stress marker level[231]. Another report showed that the 16-week treat-ment of high-fat diet-induced insulin resistance inC57BL/6J male mice significantly increased the mtDNAdamage, oxidative stress and mitochondrial dysfunctionin various peripheral tissues [232]. In addition, the studyalso found that high-fat diet in mice also contributed tothe activation of ER stress, apoptosis and inhibition ofintracellular insulin signalling pathways in both liverand skeletal muscle, implying that these synergistic ef-fects are accordingly activated to signal the metabolic
Long Chain Fatty Acids Induced Mitochondrial Dysfunction in Insulin Resistance
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

perturbations as a whole. Therefore, it should be con-cluded that the study has gone some ways towardsenhancing our knowledge in mechanistic understandingof the roles of LCFA-induced inflammation, ER stress,mitochondrial dysfunction and insulin resistance thatare intimately allied to each other in the disease process.
Inhibition of intracellular insulinsignalling pathways
As the nature of insulin resistance and type 2 diabetes ismultifactorial through involvement of the whole globalbody metabolism, the studies of hormone interactionand their regulatory effects in metabolic pathways are lessthan straightforward [233–235]. Insulin resistance maybe induced by the defects in hormonal actions in variousperipheral tissues such as skeletal muscle, liver andadipose tissue. Insulin plays a key role in regulating theglucose and fatty acid concentration in the blood circula-tion. The functions of insulin as a postprandial hormoneare well known to exhibit several beneficial effects incellular and systemic functions of the human body interms of cellular metabolism, division, growth, differenti-ation, survival and proliferations [236,237]. The stimula-tory mechanisms between insulin and fatty acid oxidativecapacities in various peripheral tissues are well defined.To date, the plurality of studies reported that the insulinup-regulates mitochondrial protein synthesis, enzyme ac-tivities such as citrate synthase and cytochrome c oxidase(COX). The increase of oxidative phosphorylation withenhancement of mitochondrial gene expression (NADHdehydrogenase I and cytochrome oxidase subunit) andATP content of normal skeletal muscle in miniature swineand human were also significantly observed in the eventof insulin infusion [238–240].
However, in the progression of insulin resistance andtype 2 diabetes, the stimulatory effects of insulin areblunted compared with healthy controls [241]. The studyhas found no significant effects in mitochondrial proteinsynthesis and COX activity of the disease subjects. Inanother study, the insulin-stimulated ATP synthesis wasfound to be diminished in individual and offspring of type2 diabetes patients [242,243]. Similarly, acute treatmentsof insulin for 7 h in non-obese patients with type 2 diabe-tes result in low levels of ATP synthesis [238]. Thus, it isbest to hypothesize that the action of insulin is bluntedand inhibited in various peripheral tissues, leading tothe deterioration of mitochondrial functions. This aber-rant effect might be due to the loss-of-function ofmitochondrial membrane integrity that inherently leadsto the severe inhibition of many distinct processes inmitochondrial activity such as the electron transport
chain, β-oxidation and TCA cycle. Based on previous stud-ies, they found that myocytes treated with LCFAs exhibitinsulin resistance via inhibition of intracellular insulinsignalling pathways [58,244–246]. In line with this,elevated concentrations of LCFA intermediates, especiallyin skeletal muscle and liver, which are major sites ofperipheral glucose uptake and disposal, were associatedwith insulin-resistant states such as obesity and type 2diabetes [247–250]. Figure 2 depicts the molecularmechanism of LCFA-induced mitochondrial dysfunctions,involving a number of metabolic stress pathways inskeletal muscle.
Roden and his colleagues have identified the mecha-nisms of fatty acid-induced insulin resistance by proposingthe prolonged exposures of high levels of LCFAs that leadto the insulin resistance via inhibition of insulin-mediatedglucose uptake in human skeletal muscle [58]. In theevent of aberrant mitochondrial functions, intracellularlipid metabolites such as acyl-CoAs, diacylglycerol andceramides tend to be accumulated in the cytosol. Thisaccumulation trend is due to the efficiency rate of fattyacid uptake into the cell that surpasses the oxidationcapacity of the cell to metabolize all the substrates inthe mitochondria. Subsequently, these accumulated lipidintermediates indirectly activate novel protein kinase Cand its downstream effectors [JNK and/or inhibitor ofthe NF-κB kinase (IκKβ)] through the involvement of aserine/threonine cascade signalling to stimulate the en-hancement of serine phosphorylation of IRS-1 [83,85].This in turn leads to the inhibition of IRS-1 tyrosinephosphorylation and inherently down-regulate PI3K andPKB/Akt2 isoform activities via inhibition on the translo-cation activity of GLUT4 to the plasma membrane topermeate glucose uptake [169,251,252]. The activationof protein phosphatase 2A by ceramides is also known toinhibit the intracellular signalling pathways via inhibitionof PKB/Akt2 isoform activities in C2C12 skeletal musclecell [253]. Accordingly, the glucose uptakes into the cellare inhibited and inherently resulted in high bloodglucose, leading to the hyperglycemia and insulin resis-tance. The production of ATP mainly relies on both sub-strates (glucose and fatty acids); thus, any dysregulationin their metabolic activities inherently lead to theimpairment of mitochondrial functions as a whole. There-fore, this cellular consequence may markedly affect theintegrity of cells in terms of growth, proliferation, metab-olism and survival, promoting the programmed cell death(apoptosis). The roles of the LCFAs in regulating the insu-lin resistance are heavily dependent on the activation ofthese signalling pathways. Noteworthy, these mecha-nisms strengthen the ideas of LCFA-induced mitochon-drial dysfunctions and led to the total inhibition ofinsulin signalling in various peripheral tissues, implicatingthe progression of insulin resistance and type 2 diabetes.
M. H. A. Bakar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

Mitochondrial dysfunctions as aunifying theme for LCFA-inducedinsulin resistance
A large and growing body of literature has reportedthe decreased lipid oxidation rates and reduced oxida-tive enzymes in the mitochondria of obese, insulinresistance and type 2 diabetes patients [32,254,255]. Nu-merous studies found that the mitochondrial morphologyin the skeletal muscle of insulin resistance and type 2diabetes patients was significantly altered by the smaller mi-tochondrial appearance and decreased electron transportchain activity in Complexes I and III compared with the con-trol [116]. Themitochondrial dysfunction in skeletal muscleand adipose tissues of type 2 diabetes subjects is observedconcomitantly with the reduced rate of glucose uptake andATP synthesis, while lipid deposition was greatly increased[256]. Moreover, another study evidenced that the strongpositive correlation between mitochondrial dysfunctionand insulin resistance as measured by magnetic resonancespectroscopy through in vivo and ex vivo mitochondrialrespiration [257].
The excessive accumulation of ROS is also implicated inregulating metabolic signalling in inflammatory activatedpathways. For instance, the LCFAs such as palmitic acid weredemonstrated to exert its detrimental effects onmitochondriafunctions in rat L6 skeletal muscle cell lines via significantreductions of mitochondrial respirations, mtDNA damage,activation of inflammatory signalling pathways, inducedphosphorylation of serine residues of IRS-1 and total inhibi-tion of GLUT4 translocations [258]. Moreover, the significantchanges or alterations of mitochondrial gene expression andproteins also equally contribute to the developments ofmitochondria dysfunction because of the elevated lipidintermediate-induced lipotoxicity in numerous insulinresponsive tissues such as skeletal muscle, liver, heart andadipose tissues.
As mentioned earlier, we have proposed several mecha-nisms related to the potential implications of LCFA-induced mitochondrial dysfunctions that lead to theprogression of insulin resistance in various peripheraltissues (Figure 3). In the past decade, numerous studiesshowed the strong correlation between mitochondrialdysfunction and type 2 diabetes. The defects in mitochon-drial capacity to metabolize intermediate metabolites
Figure 2. The possible mechanism of insulin resistance in skeletal muscle. Several deleterious effects of mitochondrial dysfunction areshown to exhibit such a decrease of proliferation, survival and metabolic rates of the cell (for more details, see text). PGC-1α, PPARγco-activator 1-alpha; PPARs, peroxisome proliferator-activated receptors; NRF-1, nuclear respiratory factor-1; JNK, c-JunNH (2)-terminalkinase; IKK, Iκb kinase; PKC, protein kinase C; ROS, reactive oxygen species; IRS-1, insulin receptor substrate-1; PI3-kinase,phosphoinositide 3-kinase; Akt2/PKB, protein kinase B; Gsk3β, glycogen synthase kinase 3 beta;mTOR,mammalian target of rapamycin;GLUT 4, glucose transporter type 4. , activation; , inhibition
Long Chain Fatty Acids Induced Mitochondrial Dysfunction in Insulin Resistance
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

have become one of the major drawbacks in impairedcell metabolism. Given the metabolic roles of LCFA-induced insulin resistance, it should be suggestedthat mitochondria dysfunctions might play a pivotalrole in the central pathogenesis of several metabolicdefects such as obesity and insulin resistance. In fact,there is a large volume of recent published reviewsand studies describing the role of mitochondria inthe pathogenesis of insulin resistance and type 2 diabe-tes [18,27,31,81,259].
Concluding remarks and futuredirections
To date, a number of mechanisms are postulated to eluci-date the overall pictures of insulin resistance. Neverthe-less, it remains unclear on what is the exact mechanismof actions that triggered the alteration and inhibition ofinsulin signalling the cascade events prior to the devel-opment of insulin resistance. As summarized earlier,there is accumulating evidence from previous and pres-ent studies on the roles of LCFAs in the regulation ofinsulin resistance and type 2 diabetes. Here, we furtherpostulate that the impairment of mitochondria functionsby LCFAs could be one of the causative factors in theregulation of insulin resistance. High consumption offood containing LCFAs may lead to the excessive accu-mulation of ROS, lipid-induced toxicity, alteration of mi-tochondrial genes/protein integrity and inflammation-
ER stress in various peripheral tissues, resulting in thedisturbance of mitochondria functions. Further studiesare needed in elucidating and deciphering the exactmechanism of these impairments. The studies of othersubclasses of fatty acids such as SCFAs and MCFAs inmodulating the energy metabolism and mitochondrialfunctions should be continued to explicate their amelio-rative effects on the mechanism underlying the disease.In addition, multidisciplinary studies such as the meta-bolic interaction between nutritional components indiets and other physiological factors such as hormones,gut microbiota and environmental factors are importantareas to be further investigated for better understandingin deciphering the primary mechanisms that are essen-tially involved in the pathogenesis of insulin resistanceand type 2 diabetes.
Acknowledgements
The authors would like to thank theMinistry of Education, Malaysia,under the Exploratory Research Grant Scheme (ERGS-2012–2014)and Universiti Teknologi Malaysia, Malaysia (vot. no: R.J130000.7844.4L025), for the financial and technical support.Mohamad Hafizi Abu Bakar is supported by a ‘UTM DoctoralZamalah Award’ at Universiti Teknologi Malaysia.
Conflicts of interest
The authors declare no conflicts of interest.
Figure 3. The pathophysiological events of insulin resistance by proposing mitochondrial dysfunction as a unifying theme in relationto the roles of long chain fatty acids
M. H. A. Bakar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

References
1. Leahy JL. Pathogenesis of type 2 diabetesmellitus. ArchMed Res 2005; 36: 197–209.
2. Schäfer S A, Machicao F, Fritsche A,Häring H-U, Kantartzis K. New type 2diabetes risk genes provide new insightsin insulin secretion mechanisms. DiabetesRes Clin Pract 2011; 93(Suppl 1):S9–24.
3. Barroso I. Genetics of type 2 diabetes.Diabet Med 2005; 22: 517–535.
4. Pierce M, Keen H, Bradley C. Risk ofdiabetes in offspring of parents withnon-insulin-dependent diabetes. DiabetMed 1995; 12: 6–13.
5. Weires MB, Tausch B, Haug PJ,Edwards CQ, Wetter T, Cannon-AlbrightLA. Familiality of diabetes mellitus.Exp Clin Endocrinol Diabetes 2007;115: 634–640.
6. Herman WH, Zimmet P. Type 2 diabe-tes: an epidemic requiring global atten-tion and urgent action. Diabetes Care2012; 35(5): 943–944.
7. Cornelis MC, Hu FB. Gene–environ-ment interactions in the developmentof type 2 diabetes: recent progress andcontinuing challenges. Annu Rev Nutr2012; 32: 245–259.
8. Boden G. Obesity, insulin resistance andfree fatty acids. Curr Opin EndocrinolDiabetes Obes 2011; 18: 139–143.
9. BrodyT.NutritionalBiochemistry.AcademicPress: San Diego, California, 1999; 1006.
10. Lee JS, Pinnamaneni SK, Eo SJ, et al.Saturated, but not n-6 polyunsaturated,fatty acids induce insulin resistance:role of intramuscular accumulation oflipid metabolites. J Appl Physiol 2006;100: 1467–1474.
11. Clément L, Poirier H, Niot I, et al. Die-tary trans-10,cis-12 conjugated linoleicacid induces hyperinsulinemia andfatty liver in the mouse. J Lipid Res2002; 43(9): 1400–1409.
12. Risérus U, Vessby B, Arner P, Zethelius B.Supplementation with trans10cis12-conjugated linoleic acid induces hyper-proinsulinaemia in obese men: close asso-ciation with impaired insulin sensitivity.Diabetologia 2004; 47: 1016–1019.
13. Clarke SD, Hembree J. Inhibition of tri-iodothyronine’s induction of rat liverlipogenic enzymes by dietary fat. J Nutr1990; 120(6): 625–630.
14. Yuzefovych L, Wilson G, Rachek L.Different effects of oleate vs. palmitateon mitochondrial function, apoptosis,and insulin signaling in L6 skeletalmuscle cells: role of oxidative stress.Am J Physiol - Endocrinol Metab 2010;299(6): E1096–E1105.
15. Hecker M, Sommer N, Voigtmann H,et al. Impact of short- and medium-chain fatty acids on mitochondrial func-tion in severe inflammation. J ParenterEnter Nutr 2013; 38(5): 587–594.
16. Turner N, Hariharan K, TidAng J, et al.Enhancement of muscle mitochondrialoxidative capacity and alterations in
insulin action are lipid species depen-dent: potent tissue-specific effects ofmedium-chain fatty acids. Diabetes2009; 58(11): 2547–2554.
17. Patti M-E, Corvera S. The role of mito-chondria in the pathogenesis of type 2diabetes. Endocr Rev 2010; 31: 364–95.
18. Pagel-Langenickel I, Bao J, Pang L,Sack MN. The role of mitochondria inthe pathophysiology of skeletal muscleinsulin resistance. Endocr Rev 2010;31: 25–51.
19. Martin SD, McGee SL. The role of mito-chondria in the aetiology of insulin re-sistance and type 2 diabetes. BiochimBiophys Acta 2013; 1840: 1303–1312.
20. Mogensen M, Sahlin K, Fernstro M,et al. Mitochondrial respiration isdecreased in skeletal muscle of patientswith type 2 diabetes. Diabetes 2007;56: 1592–1599.
21. Patti ME, Butte AJ, Crunkhorn S, et al.Coordinated reduction of genes of oxi-dative metabolism in humans with in-sulin resistance and diabetes: potentialrole of PGC1 and NRF1. Proc Natl AcadSci 2003; 100(14): 8466–8471.
22. Mootha VK, Lindgren CM, Eriksson K-F,et al. PGC-1α-responsive genes involvedin oxidative phosphorylation are co-ordinately downregulated in humandiabetes. Nat Genet 2003; 34:267–273.
23. Szendroedi J, Schmid AI, MeyerspeerM, et al. Impaired mitochondrial func-tion and insulin resistance of skeletalmuscle in mitochondrial diabetes. Dia-betes Care 2009; 32(4): 677–679.
24. Gao C-L, Zhu C, Zhao Y-P, et al. Mito-chondrial dysfunction is induced byhigh levels of glucose and free fattyacids in 3T3-L1 adipocytes. Mol CellEndocrinol 2010; 320: 25–33.
25. Hammarstedt A, Jansson P-A, WesslauC, Yang X, Smith U. Reduced expres-sion of PGC-1 and insulin-signalingmolecules in adipose tissue is associ-ated with insulin resistance. Bio-chem Biophys Res Commun 2003;301: 578–582.
26. Nakamura S, Takamura T, Matsuzawa-Nagata N, et al. Palmitate induces insu-lin resistance in H4IIEC3 hepatocytesthrough reactive oxygen species pro-duced by mitochondria. J Biol Chem2009; 284(22): 14809–14818.
27. Newsholme P, Gaudel C, Krause M. Mi-tochondria and diabetes. An intriguingpathogenetic role. In Adv MitochondrialMed. Volume 942. Scatena R, Bottoni P,Giardina B (eds). Springer: Netherlands,2012; 235–247. [Advances in ExperimentalMedicine and Biology]
28. Saini V. Molecular mechanisms of insu-lin resistance in type 2 diabetes mellitus.World J Diabetes 2010; 1: 68–75.
29. Kraegen EW, Cooney GJ. Free fatty acidsand skeletal muscle insulin resistance.Curr Opin Lipidol 2008; 19: 235–241.
30. Abdul-Ghani M, DeFronzo R. Mito-chondrial dysfunction, insulin resis-tance, and type 2 diabetes mellitus.Curr Diab Rep 2008; 8: 173–178.
31. Schrauwen P, Schrauwen-Hinderling V,Hoeks J, Hesselink MKC. Mitochondrialdysfunction and lipotoxicity. BiochimBiophys Acta 2010; 1801: 266–71.
32. Hoeks J, Schrauwen P. Muscle mito-chondria and insulin resistance: a hu-man perspective. Trends EndocrinolMetab 2014; 23: 444–450.
33. Pagliarini DJ, Calvo SE, Chang B, et al.A mitochondrial protein compendiumelucidates complex I disease biology.Cell 2008; 134: 112–123.
34. Soria LR, Marrone J, Calamita G,Marinelli RA. Ammonia detoxificationvia ureagenesis in rat hepatocytes involvesmitochondrial aquaporin-8 channels.Hepatology 2013; 57: 2061–2071.
35. Giorgi C, Agnoletto C, Bononi A, et al.Mitochondrial calcium homeostasis aspotential target for mitochondrial med-icine. Mitochondrion 2012; 12: 77–85.
36. Yoon Y, Galloway CA, Jhun BS, Yu T.Mitochondrial dynamics in diabetes.Antioxid Redox Signal 2011; 14: 439–457.
37. Nieminen A-L. Apoptosis and necrosisin health and disease: role of mitochon-dria. Int Rev Cytol 2003; 224: 29–55.
38. Maechler P, Wollheim CB. Mitochondrialfunction in normal and diabetic [beta]-cells. Nature 2001; 414: 807–812.
39. Amacher DE. Drug-associated mito-chondrial toxicity and its detection.Curr Med Chem 2005; 12: 1829–1839.
40. De Souza-PintoNC,MasonPA,HashiguchiK, et al. Novel DNAmismatch-repair activ-ity involving YB-1 in humanmitochondria.DNA Repair (Amst) 2009; 8: 704–719.
41. Boelsterli UA, Lim PLK. Mitochondrialabnormalities—a link to idiosyncraticdrug hepatotoxicity? Toxicol ApplPharmacol 2007; 220: 92–107.
42. Desler C, Lykke A, Rasmussen LJ.The effect of mitochondrial dysfunc-tion on cytosolic nucleotide metabo-lism. J Nucleic Acids 2010; 2010:12725–12732.
43. Spiegelman BM, Flier JS. Obesity andthe regulation of energy balance. Cell2001; 104: 531–543.
44. Lowell BB, Shulman GI. Mitochondrialdysfunction and type 2 diabetes. Sci2005; 307(5708): 384–387.
45. Jing E, Emanuelli B, Hirschey MD, et al.Sirtuin-3 (Sirt3) regulates skeletalmuscle metabolism and insulin signal-ing via altered mitochondrial oxidationand reactive oxygen species produc-tion. In Proc Natl Acad Sci USA 2011;108: 14608–14613.
46. Matsuzaki S, Szweda PA, Szweda LI,Humphries KM. Regulated productionof free radicals by the mitochondrialelectron transport chain: cardiac ische-mic preconditioning. Adv Drug DelivRev 2009; 61: 1324–1331.
Long Chain Fatty Acids Induced Mitochondrial Dysfunction in Insulin Resistance
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

47. Newsholme P, Haber EP, Hirabara SM,et al. Diabetes associated cell stressand dysfunction: role of mitochon-drial and non-mitochondrial ROSproduction and activity. J Physiol2007; 583(1): 9–24.
48. Wei Y, Chen K, Whaley-Connell AT,Stump CS, Ibdah JA, Sowers JR.Skeletal muscle insulin resistance:role of inflammatory cytokines andreactive oxygen species. Am JPhysiol - Regul Integr Comp Physiol2008; 23: R673–R680.
49. Muoio DM, Neufer PD. Lipid-inducedmitochondrial stress and insulinaction in muscle. Cell Metab 2012;15: 595–605.
50. Garland PB, Newsholme EA, Randle PJ.Effect of fatty acids, ketone bodies, dia-betes and starvation on pyruvate me-tabolism in rat heart and diaphragmmuscle. Nature 1962; 195: 507–520.
51. Newsholme EA, Randle PJ, ManchesterKL. Inhibition of the phosphofructo-kinase reaction in perfused rat heartby respiration of ketone bodies, fattyacids and pyruvate. Nature 1962;193: 270–271.
52. Randle PJ, Garland PB, Hales CN,Newsholme EA. The glucose fatty-acidcycle its role in insulin sensitivity andthe metabolic disturbance of diabetesmellitus. Lancet 1963; 281: 785–789.
53. Randle PJ. Regulatory interactionsbetween lipids and carbohydrates: theglucose fatty acid cycle after 35 years.Diabetes Metab Rev 1999; 14: 263–283.
54. Dresner A, Laurent D, Marcucci M,et al. Effects of free fatty acids on glu-cose transport and IRS-1-associatedphosphatidylinositol 3-kinase activity.J Clin Invest 1999; 103: 253–259.
55. Griffin ME, Marcucci MJ, Cline GW,et al. Free fatty acid-induced insulin re-sistance is associated with activation ofprotein kinase C theta and alterationsin the insulin signaling cascade. Diabe-tes 1999; 48: 1270–1274.
56. Oakes ND, Bell KS, Furler SM, et al.Diet-induced muscle insulin resistancein rats is ameliorated by acutedietary lipid withdrawal or a singlebout of exercise: parallel relationshipbetween insulin stimulation of glucoseuptake and suppression of long-chainfatty acyl-CoA. Diabetes 1997; 46(12):2022–2028.
57. Roden M. How free fatty acids inhibitglucose utilization in human skeletalmuscle. Physiol 2004; 19(3): 92–96.
58. Roden M, Price TB, Perseghin G, et al.Mechanism of free fatty acid-inducedinsulin resistance in humans. J ClinInvest 1996; 97: 2859–2865.
59. Ma ZA, Zhao Z, Turk J. Mitochondrialdysfunction and β-cell failure in type 2diabetes mellitus. Exp Diabetes Res2012; 2012: 703538.
60. Katan MB, Zock PL, Mensink RP. Ef-fects of fats and fatty acids on bloodlipids in humans: an overview. Am JClin Nutr 1994; 60(6): 1017S–1022S.
61. Gaster M, Rustan AC, Beck-Nielsen H.Differential utilization of saturatedpalmitate and unsaturated oleate: evi-dence from cultured myotubes. Diabe-tes 2005; 54(3): 648–656.
62. Vasudevan. Textbook of Biochemistryfor Dental Students (5th edn). JaypeeBrothers, Medical Publishers, 2007;1–314.
63. Cameron-Smith D, Burke LM, AngusDJ, et al. A short-term, high-fat dietup-regulates lipid metabolism andgene expression in human skeletalmuscle. Am J Clin Nutr 2003; 77(2):313–318.
64. Primeaux S, Braymer HD, Bray G.CD36 mRNA in the gastrointestinaltract is differentially regulated by die-tary fat intake in obesity-prone andobesity-resistant rats. Dig Dis Sci 2013;58: 363–370.
65. Coburn CT, Knapp FF, Febbraio M,Beets AL, Silverstein RL, Abumrad NA.Defective uptake and utilization of longchain fatty acids in muscle and adiposetissues of CD36 knockout mice. J BiolChem 2000; 275(42): 32523–32529.
66. Zhang L, Keung W, Samokhvalov V,Wang W, Lopaschuk GD. Role of fattyacid uptake and fatty acid beta-oxidation in mediating insulin resistancein heart and skeletal muscle. BiochimBiophys Acta 2010; 1801(1): 1–22.
67. Ceccarelli SM, Chomienne O, Gubler M,Arduini A. Carnitine palmitoyltransferase(CPT) modulators: a medicinal chemistryperspective on 35 years of research. J MedChem 2011; 54: 3109–3152.
68. Brownsey RW, Boone AN, Elliott JE,Kulpa JE, Lee WM. Regulation ofacetyl-CoA carboxylase. Biochem SocTrans 2006; 34(Pt 2): 223–227.
69. Kim J-Y, Hickner RC, Cortright RL,Dohm GL, Houmard JA. Lipid oxida-tion is reduced in obese human skeletalmuscle. Am J Physiol - EndocrinolMetab 2000; 279(5): E1039–E1044.
70. Bandyopadhyay GK, Yu JG, Ofrecio J,Olefsky JM. Increased malonyl-CoAlevels in muscle from obese and type2 diabetic subjects lead to decreasedfatty acid oxidation and increased lipo-genesis; thiazolidinedione treatmentreverses these defects. Diabetes 2006;55(8): 2277–2285.
71. Adams SH, Hoppel CL, Lok KH, et al.Plasma acylcarnitine profiles suggest in-complete long-chain fatty acid β-oxidationand altered tricarboxylic acid cycle activityin type 2 diabetic African-Americanwomen. J Nutr 2009; 139: 1073–1081.
72. Van Eunen K, Simons SM, Gerding A,et al. Biochemical competition makesfatty-acid β-oxidation vulnerable tosubstrate overload. PLoS Comput Biol2013; 9: e1003186.
73. Koves TR, Ussher JR, Noland RC, et al.Mitochondrial overload and incom-plete fatty acid oxidation contribute toskeletal muscle insulin resistance. CellMetab 2008; 7: 45–56.
74. Möder M, Kießling A, Löster H,Brüggemann L. The pattern of urinaryacylcarnitines determined by electrospraymass spectrometry: a new tool in the di-agnosis of diabetes mellitus. Anal BioanalChem 2003; 375: 200–210.
75. Kim SC, Sprung R, Chen Y, et al. Sub-strate and functional diversity of lysineacetylation revealed by a proteomicssurvey. Mol Cell 2006; 23: 607–618.
76. Muoio DM, Koves TR. Skeletal muscleadaptation to fatty acid depends oncoordinated actions of the PPARs andPGC1α: implications for metabolicdisease. Appl Physiol Nutr Metab 2007;32: 874–883.
77. Andreyev AY, Kushnareva YE, StarkovAA. Mitochondrial metabolism of reactiveoxygen species. Biochem Biokhimii a2005; 70: 200–14.
78. Laguens R, Bianchi N. Fine structureof the liver in human idiopathicdiabetes mellitus: I. Parenchymal cellmitochondria. Exp Mol Pathol 1963;2: 203–214.
79. Jucker BM, Dufour S, Ren J, et al.Assessment of mitochondrial energycoupling in vivo by 13C/31P NMR.Proc Natl Acad Sci 2000; 97(12):6880–6884.
80. Petersen KF, Shulman GI, Petersen KF.GIS. Etiology of insulin resistance. AmJ Med 2006; 119: S10–S16.
81. Szendroedi J, Phielix E, Roden M. Therole of mitochondria in insulin resis-tance and type 2 diabetes mellitus.Nat Rev Endocrinol 2012; 8: 92–103.
82. Galgani JE, Moro C, Ravussin E. Meta-bolic flexibility and insulin resistance.Am J Physiol - Endocrinol Metab 2008;295: E1009–E1017.
83. Corpeleijn E, Saris WHM, Blaak EE.Metabolic flexibility in the develop-ment of insulin resistance and type 2diabetes: effects of lifestyle. Obes Rev2009; 10: 178–193.
84. Kahn SE, Hull RL, Utzschneider KM.Mechanisms linking obesity to insulinresistance and type 2 diabetes. Nature2006; 444: 840–846.
85. Choi K, Kim YB. Molecular mechanismof insulin resistance in obesity and type2 diabetes. Korean J Intern Med 2010;25: 119–129.
86. Estadella D, da Penha Oller doNascimento CM, Oyama LM, Ribeiro EB,Dâmaso AR, de Piano A. Lipotoxicity:effects of dietary saturated and transfattyacids. Mediators Inflamm 2013; 2013:137579.
87. Eckel RH, Kahn SE, Ferrannini E, et al.Obesity and type 2 diabetes: what canbe unified and what needs to be indi-vidualized? Diabetes Care 2011; 34(6):1424–1430.
88. Jocken JE, Goossens G, Boon H, et al.Insulin-mediated suppression of lipoly-sis in adipose tissue and skeletal mus-cle of obese type 2 diabetic men andmen with normal glucose tolerance.Diabetologia 2013; 56: 2255–2265.
M. H. A. Bakar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

89. Friedrich N. Metabolomics in diabetes re-search. J Endocrinol 2012; 0049: 1–33.
90. Henriksen EJ, Diamond-Stanic MK,Marchionne EM. Oxidative stress andthe etiology of insulin resistance andtype 2 diabetes. Free Radic Biol Med2011; 51: 993–999.
91. Giacco F, Brownlee M. Oxidative stressand diabetic complications. Circ Res2010; 107(9): 1058–1070.
92. Brodská B, Holoubek A. Generation ofreactive oxygen species during apopto-sis induced by DNA-damaging agentsand/or histone deacetylase inhibitors.Oxid Med Cell Longev 2011; 2011:253529.
93. Indo HP, Davidson M, Yen H-C, et al.Evidence of ROS generation bymitochondria in cells with impairedelectron transport chain and mitochon-drial DNA damage. Mitochondrion2007; 7: 106–118.
94. Schönfeld P, Wojtczak L. Fatty acids de-crease mitochondrial generation of re-active oxygen species at the reverseelectron transport but increase it atthe forward transport. Biochim BiophysActa 2007; 1767: 1032–1040.
95. Barja G. Mitochondrial oxygen radicalgeneration and leak: sites of produc-tion in states 4 and 3, organ specificity,and relation to aging and longevity. JBioenerg Biomembr 1999; 31: 347–366.
96. Johannsen DL, Ravussin E. The role ofmitochondria in health and disease. CurrOpin Pharmacol 2009; 9: 780–786.
97. Warburton DER, Nicol CW, Bredin SSD.Health benefits of physical activity:the evidence. Can Med Assoc J 2006;174(6): 801–809.
98. Santos CX, Tanaka LY, Wosniak J,Laurindo FR. Mechanisms and implica-tions of reactive oxygen species genera-tion during the unfolded proteinresponse: roles of endoplasmic reticu-lum oxidoreductases, mitochondrialelectron transport, and NADPH oxi-dase. Antioxid Redox Signal 2009; 11:2409–2427.
99. Stone JR, Yang S. Hydrogen peroxide:a signaling messenger. Antioxid RedoxSignal 2006; 8: 243–270.
100. Brand MD. The sites and topology ofmitochondrial superoxide production.Exp Gerontol 2010; 45: 466–472.
101. Mensink M, Blaak EE, van Baak MA,Wagenmakers AJM, Saris WHM. Plas-ma free fatty acid uptake and oxidationare already diminished in subjects athigh risk for developing type 2 diabe-tes. Diabetes 2001; 50(11): 2548–2554.
102. Soardo G, Donnini D, Domenis L, et al.Oxidative stress is activated by freefatty acids in cultured human hepato-cytes. Metab Syndr Relat Disord 2011;9: 397–401.
103. Song JH, Fujimoto K, Miyazawa T.Polyunsaturated (n-3) fatty acids sus-ceptible to peroxidation are increasedin plasma and tissue lipids of rats feddocosahexaenoic acid-containing oils.J Nutr 2000; 130(12): 3028–3033.
104. Duval C, Cámara Y, Hondares E,Sibille B, Villarroya F. Overexpressionof mitochondrial uncoupling protein-3 does not decrease production of thereactive oxygen species, elevated bypalmitate in skeletal muscle cells.FEBS Lett 2007; 581: 955–961.
105. Lambertucci RH, Hirabara SM, SilveiraLdos R, Levada-Pires AC, Curi R,Pithon-Curi TC. Palmitate increasessuperoxide production through mito-chondrial electron transport chainand NADPH oxidase activity in skele-tal muscle cells. J Cell Physiol 2008;216: 955–961.
106. Kim J, Minkler PE, Salomon RG, AndersonVE, Hoppel CL. Cardiolipin: characteriza-tion of distinct oxidized molecularspecies. J Lipid Res 2011; 52(1): 125–135.
107. Meex RCR, Schrauwen-hinderling VB,Moonen-kornips E, et al. Restorationof muscle mitochondrial function andmetabolic flexibility in type 2 diabetesby exercise training is paralleled byincreased myocellular fat storage andimproved insulin sensitivity. Diabetes2010; 59(3): 572–579.
108. Bandeira SM, Guedes GS, da FonsecaLJ, et al. Characterization of blood oxi-dative stress in type 2 diabetes mellituspatients: increase in lipid peroxidationand SOD activity. Oxid Med Cell Longev2012; 2012: 819310.
109. Garcia J, Han D, Sancheti H, Yap LP,Kaplowitz N, Cadenas E. Regulation ofmitochondrial glutathione redox statusand protein glutathionylation by respi-ratory substrates. J Biol Chem 2010;285: 39646–39654.
110. Anderson EJ, Lustig ME, Boyle KE, et al.Mitochondrial H2O2 emission andcellular redox state link excess fatintake to insulin resistance in bothrodents and humans. J Clin Invest2009; 119: 573–581.
111. Kane DA, Anderson EJ, Price III JW,et al. Metformin selectively attenuatesmitochondrial H2O2 emission withoutaffecting respiratory capacity in skele-tal muscle of obese rats. Free Radic BiolMed 2010; 49: 1082–1087.
112. Borradaile NM, Buhman KK, ListenbergerLL, et al.A critical role for eukaryotic elon-gation factor 1A-1 in lipotoxic cell death.Mol Biol Cell 2006; 17(2): 770–778.
113. Cacicedo JM, Benjachareowong S,Chou E, Ruderman NB, Ido Y. Palmi-tate-induced apoptosis in culturedbovine retinal pericytes: roles ofNAD(P)H oxidase, oxidant stress,and ceramide. Diabetes 2005; 54(6):1838–1845.
114. Den Hartigh LJ, Han CY, Wang S, OmerM, Chait A. 10E,12Z-conjugatedlinoleic acid impairs adipocyte triglyc-eride storage by enhancing fatty acidoxidation, lipolysis, and mitochondrialreactive oxygen species. J Lipid Res2013; 54: 2964–2978.
115. Zarrouk A, Vejux A, Nury T, et al.Induction of mitochondrial changesassociated with oxidative stress on very
long chain fatty acids (C22:0, C24:0, orC26:0)-treated human neuronal cells(SK-NB-E). Oxid Med Cell Longev2012; 2012: 623257.
116. Kelley DE, He J, Menshikova EV, RitovVB. Dysfunction of mitochondria in hu-man skeletal muscle in type 2 diabetes.Diabetes 2002; 51: 2944–50.
117. Heilbronn LK, Gan SK, Turner N, CampbellLV, Chisholm DJ. Markers of mito-chondrial biogenesis and metabolism arelower in overweight and obese insulin-resistant subjects. J Clin Endocrinol Metab2007; 92(4): 1467–1473.
118. Vankoningsloo S, PiensM, Lecocq C, et al.Mitochondrial dysfunction induces tri-glyceride accumulation in 3T3-L1 cells:role of fatty acid β-oxidation and glucose.J Lipid Res 2005; 46(6): 1133–1149.
119. Furukawa S, Fujita T, ShimabukuroM, et al. Increased oxidative stressin obesity and its impact on meta-bolic syndrome. J Clin Invest 2004;114: 1752–1761.
120. Paglialunga S, Bree B, Bosma M, et al.Targeting of mitochondrial reactiveoxygen species production does notavert lipid-induced insulin resistancein muscle tissue from mice. Diabe-tologia 2012; 55: 2759–2768.
121. De Feyter HM, van den Broek NMA,Praet SFE, Nicolay K, van Loon LJC,Prompers JJ. Early or advanced stagetype 2 diabetes is not accompanied byin vivo skeletal muscle mitochondrialdysfunction. Eur J Endocrinol 2008;158(5): 643–653.
122. Barroso I, Luan J, Sandhu MS, et al.Meta-analysis of the Gly482Ser variantin PPARGC1A in type 2 diabetesand related phenotypes. Diabetologia2006; 49: 501–505.
123. Ling C, Poulsen P, Simonsson S, et al.Genetic and epigenetic factors are asso-ciated with expression of respiratorychain component NDUFB6 in humanskeletal muscle. J Clin Invest 2007;117: 3427–3435.
124. Nakanishi S, Yamane K, Ohishi W, et al.Manganese superoxide dismutaseAla16Val polymorphism is associatedwith the development of type 2 diabe-tes in Japanese-Americans. DiabetesRes Clin Pract 2008; 81: 381–385.
125. Park KS, Chan JC, Chuang L-M, et al. Amitochondrial DNA variant at position16189 is associated with type 2 diabe-tes mellitus in Asians. Diabetologia2008; 51: 602–608.
126. Guo L-J, Oshida Y, Fuku N, et al.Mitochondrial genome polymorphismsassociated with type-2 diabetes or obe-sity. Mitochondrion 2005; 5: 15–33.
127. Shenouda SM, Widlansky ME, Chen K,et al. Altered mitochondrial dynamicscontributes to endothelial dysfunctionin diabetes mellitus. Circulation 2011;124: 444–453.
128. SeoAY, JosephA-M,DuttaD,Hwang JCY,Aris JP, Leeuwenburgh C. New insightsinto the role of mitochondria in aging:
Long Chain Fatty Acids Induced Mitochondrial Dysfunction in Insulin Resistance
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

mitochondrial dynamics and more. J CellSci 2010; 123(15): 2533–2542.
129. Joseph AM, Joanisse DR, Baillot RG,Hood DA. Mitochondrial dysregulationin the pathogenesis of diabetes: potentialfor mitochondrial biogenesis-mediatedinterventions. Exp Diabetes Res 2012;2012: 642038.
130. Scarpulla RC. Transcriptional para-digms in mammalian mitochondrialbiogenesis and function. Physiol Rev2008; 88: 611–638.
131. Arany Z. PGC-1 coactivators and skele-tal muscle adaptations in health anddisease. Curr Opin Genet Dev 2008;18: 426–434.
132. Evans RM, Barish GD, Wang Y-X.PPARs and the complex journey toobesity. Nat Med 2004; 10: 355–361.
133. Diradourian C, Girard J, Pégorier J-P.Phosphorylation of PPARs: from molec-ular characterization to physiologicalrelevance. Biochimie 2005; 87: 33–38.
134. Zhang J, Phillips DIW, Wang C, ByrneCD. Human skeletal muscle PPARα ex-pression correlates with fat metabolismgene expression but not BMI or insulinsensitivity. Am J Physiol - EndocrinolMetab 2004; 286(2): E168–E175.
135. Song S, Attia RR, Connaughton S, et al.Peroxisome proliferator activated re-ceptor α (PPARα) and PPAR gamma co-activator (PGC-1α) induce carnitinepalmitoyltransferase IA (CPT-1A) viaindependent gene elements. Mol CellEndocrinol 2010; 325: 54–63.
136. Coll T, Jové M, Rodríguez-Calvo R,et al. Palmitate-mediated downregula-tion of peroxisome proliferator-activatedreceptor-γ coactivator 1α in skeletalmuscle cells involves MEK1/2 andnuclear factor-κB activation. Diabetes2006; 55: 2779–2787.
137. Pimenta AS, Gaidhu MP, Habib S, et al.Prolonged exposure to palmitate im-pairs fatty acid oxidation despite activa-tion of AMP-activated protein kinase inskeletal muscle cells. J Cell Physiol2008; 217: 478–485.
138. Sparks LM, Xie H, Koza RA, et al. A high-fat diet coordinately downregulates genesrequired formitochondrial oxidative phos-phorylation in skeletal muscle. Diabetes2005; 54(7): 1926–1933.
139. Hoeks J, Hesselink MKC, Russell AP,et al. Peroxisome proliferator-activatedreceptor-γ coactivator-1 and insulin re-sistance: acute effect of fatty acids.Diabetologia 2006; 49: 2419–2426.
140. Jové M, Salla J, Planavila A, et al. Im-paired expression of NADH dehydroge-nase subunit 1 and PPARγ coactivator-1in skeletal muscle of ZDF rats: restora-tion by troglitazone. J Lipid Res 2004;45(1): 113–123.
141. Kleiner S, Mepani RJ, Laznik D, et al. De-velopment of insulin resistance in micelacking PGC-1α in adipose tissues. ProcNatl Acad Sci 2012; 109(24): 9635–9640.
142. Arany Z, Lebrasseur N, Morris C, et al.The transcriptional coactivator PGC-1
drives the formation of oxidative typeIIX fibers in skeletal muscle. Cell Metab2007; 5: 35–46.
143. Kim J-A, Wei Y, Sowers JR. Role of mi-tochondrial dysfunction in insulinresistance. Circ Res 2008; 102: 401–14.
144. Oikari S, Ahtialansaari T, Huotari A,et al. Effect of medium- and long-chain fatty acid diets on PPAR andSREBP-1 expression and glucose ho-meostasis in ACBP-overexpressingtransgenic rats. Acta Physiol 2008;194: 57–65.
145. Holloway GP, Perry CGR, Thrush AB,et al. PGC-1alpha’s relationship withskeletal muscle palmitate oxidation isnot present with obesity despite main-tained PGC-1alpha and PGC-1betaprotein. Am J Physiol Endocrinol Metab2008; 294: E1060–E1069.
146. Bach D, Pich S, Soriano FX, et al.Mitofusin-2 determines mitochondrialnetwork architecture and mitochon-drial metabolism: a novel regulatorymechanism altered in obesity. J BiolChem 2003; 278: 17190–17197.
147. Sebastián D, Hernández-Alvarez MI,Segalés J, et al. Mitofusin 2 (Mfn2)links mitochondrial and endoplasmicreticulum function with insulin signal-ing and is essential for normal glucosehomeostasis. Proc Natl Acad Sci 2012;109(14): 5523–5528.
148. Kong D, Song G, Wang C, et al. Over-expression of mitofusin 2 improvestranslocation of glucose transporter 4in skeletal muscle of high-fat diet-fedrats through AMP-activated proteinkinase signaling. Mol Med Rep 2013;8: 205–210.
149. Gan KX, Wang C, Chen JH, Zhu CJ,Song GY. Mitofusin-2 ameliorateshigh-fat diet-induced insulin resistancein liver of rats. World J Gastroenterol2013; 19: 1572–1581.
150. Gutierrez D, Puglisi M, Hasty A.Impact of increased adipose tissuemass on inflammation, insulin resis-tance, and dyslipidemia. Curr DiabRep 2009; 9: 26–32.
151. Ouchi N, Parker JL, Lugus JJ, Walsh K.Adipokines in inflammation and meta-bolic disease. Nat Rev Immunol 2011;11: 85–97.
152. Kennedy A, Martinez K, Chuang C-C,LaPoint K, McIntosh M. Saturated fattyacid-mediated inflammation and insu-lin resistance in adipose tissue: mecha-nisms of action and implications. J Nutr2009; 139(1): 1–4.
153. Gustafson B, Gogg S, Hedjazifar S,Jenndahl L, Hammarstedt A, Smith U.Inflammation and impaired adipogene-sis in hypertrophic obesity in man. AmJ Physiol - Endocrinol Metab 2009;297: E999–E1003.
154. Tourniaire F, Romier-Crouzet B, Lee JH,et al. Chemokine expression in inflamedadipose tissue is mainly mediated byNF-κB. PLoS One 2013; 8: e66515.
155. Xu L, Spinas GA, Niessen M. ER stressin adipocytes inhibits insulin signaling,
represses lipolysis, and alters the secre-tion of adipokines without inhibitingglucose transport. Horm Metab Res2010; 42: 643–651.
156. Szendroedi J, Frossard M, Klein N,et al. Lipid-induced insulin resistanceis not mediated by impaired trans-capillary transport of insulin andglucose in humans. Diabetes 2012;61(12): 3176–3180.
157. Consitt LA, Bell JA, Houmard JA. Intra-muscular lipid metabolism, insulinaction, and obesity. IUBMB Life 2009;61: 47–55.
158. Samuel VT. Fructose induced lipogene-sis: from sugar to fat to insulin resis-tance. Trends Endocrinol Metab 2011;22: 60–65.
159. Unger RH, Clark GO, Scherer PE, OrciL. Lipid homeostasis, lipotoxicity andthe metabolic syndrome. BiochimBiophys Acta - Mol Cell Biol Lipids2010; 1801: 209–214.
160. DeFronzo RA. Insulin resistance, lipo-toxicity, type 2 diabetes and atheroscle-rosis: the missing links. The ClaudeBernard Lecture 2009. Diabetologia2010; 53: 1270–1287.
161. Adams JM, Pratipanawatr T, Berria R,et al. Ceramide content is increased inskeletal muscle from obese insulin-resistant humans. Diabetes 2004; 53(1):25–31.
162. De Vogel-van den Bosch J, Hoeks J,Timmers S, et al. The effects of long-or medium-chain fat diets on glucosetolerance and myocellular content oflipid intermediates in rats. Obesity2011; 19: 792–799.
163. De Vogel-van den Bosch J, van denBerg SAA, Bijland S, et al. High-fat di-ets rich in medium- versus long-chainfatty acids induce distinct patterns oftissue specific insulin resistance. J NutrBiochem 2011; 22: 366–371.
164. Samuel VT, Petersen KF, Shulman GI.Lipid-induced insulin resistance:unravelling the mechanism. Lancet2010; 375: 2267–2277.
165. Nagle CA, Klett EL, Coleman RA.Hepatic triacylglycerol accumulationand insulin resistance. J Lipid Res2009; 50(Supplement): S74–S79.
166. Zhang D, Liu Z-X, Choi CS, et al. Mito-chondrial dysfunction due to long-chain Acyl-CoA dehydrogenase defi-ciency causes hepatic steatosis and he-patic insulin resistance. Proc Natl AcadSci 2007; 104(43): 17075–17080.
167. Timmers S, Schrauwen P, de Vogel J.Muscular diacylglycerol metabolismand insulin resistance. Physiol Behav2008; 94: 242–251.
168. Itani SI, Ruderman NB, Schmieder F,Boden G. Lipid-induced insulin resis-tance in human muscle is associatedwith changes in diacylglycerol, pro-tein kinase C, and IκB-α. Diabetes2002; 51(7): 2005–2011.
169. Galadari S, Rahman A, PallichankandyS, Galadari A, Thayyullathil F. Role ofceramide in diabetes mellitus: evidence
M. H. A. Bakar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

andmechanisms. Lipids Health Dis 2013;12: 98.
170. Haimovitz-Friedman A, Kolesnick RN,Fuks Z. Ceramide signaling in apopto-sis. Br Med Bull 1997; 53(3): 539–553.
171. Górski J. Ceramide and insulinresistance: how should the issue beapproached? Diabetes 2012; 61(12):3081–3083.
172. StraczkowskiM, Kowalska I, BaranowskiM, et al. Increased skeletal muscleceramide level in men at risk of develop-ing type 2 diabetes. Diabetologia 2007;50: 2366–2373.
173. Di Paola M, Cocco T, Lorusso M. Cer-amide interaction with the respiratorychain of heart mitochondria†. Biochem-istry 2000; 39: 6660–6668.
174. Gudz TI, Tserng K-Y, Hoppel CL. Directinhibition of mitochondrial respiratorychain complex III by cell-permeableceramide. J Biol Chem 1997; 272(39):24154–24158.
175. Melissa ES, Trevor ST, Eric SB, et al.Mi-tochondrial fission mediates ceramide-induced metabolic disruption in skeletalmuscle. Biochem J 2013; 456: 427–439.
176. Novgorodov SA, Wu BX, Gudz TI, et al.Novel pathway of ceramide productionin mitochondria: thioesterase and neu-tral ceramidase produce ceramide fromsphingosine and acyl-CoA. J Biol Chem2011; 286(28): 25352–25362.
177. Coen PM, Hames KC, Leachman EM,et al. Reduced skeletal muscle oxidativecapacity and elevated ceramide but notdiacylglycerol content in severe obesity.Obesity 2013; 21: 2362–2371.
178. Straczkowski M, Kowalska I, NikolajukA, et al. Relationship between insulinsensitivity and sphingomyelin signalingpathway in human skeletal muscle.Diabetes 2004; 53(5): 1215–1221.
179. Hannun YA, Obeid LM. The ceramide-centric universe of lipid-mediated cellregulation: stress encounters of thelipid kind. J Biol Chem 2002; 277(29):25847–25850.
180. Merrill AH Jr, Jones DD. An update ofthe enzymology and regulation ofsphingomyelin metabolism. BiochimBiophys Acta - Lipids Lipid Metab1990; 1044: 1–12.
181. Pickersgill L, Litherland GJ, GreenbergAS, Walker M, Yeaman SJ. Key rolefor ceramides in mediating insulinresistance in human muscle cells. J BiolChem 2007; 282(17): 12583–12589.
182. Pinnamaneni SK, Southgate RJ,Febbraio MA, Watt MJ. Stearoyl CoAdesaturase 1 is elevated in obesity butprotects against fatty acid-induced skel-etal muscle insulin resistance in vitro.Diabetologia 2006; 49: 3027–3037.
183. Holland WL, Brozinick JT, Wang L-P,et al. Inhibition of ceramide synthesisameliorates glucocorticoid-, saturated-fat-, and obesity-induced insulin resis-tance. Cell Metab 2007; 5: 167–179.
184. Ussher JR, Koves TR, Cadete VJJ, et al.Inhibition of de novo ceramide synthesisreverses diet-induced insulin resistance
and enhances whole-body oxygenconsumption. Diabetes 2010; 59(1):2453–2464.
185. Thrush AB, Chabowski A, HeigenhauserGJ, McBride BW, Or-Rashid M, Dyck DJ.Conjugated linoleic acid increasesskeletal muscle ceramide content and de-creases insulin sensitivity in overweight,non-diabetic humans. Appl Physiol NutrMetab 2007; 32: 372–382.
186. Yu C, Chen Y, Cline GW, et al. Mecha-nism by which fatty acids inhibitinsulin activation of insulin receptorsubstrate-1 (IRS-1)-associated phos-phatidylinositol 3-kinase activity inmuscle. J Biol Chem 2002; 277(52):50230–50236.
187. Erion DM, Shulman GI. Diacylglycerol-mediated insulin resistance. Nat Med2010; 16: 400–402.
188. Zhang L, Ussher JR, Oka T, Cadete VJJ,Wagg C, Lopaschuk GD. Cardiac diacyl-glycerol accumulation in high fat-fedmice is associated with impairedinsulin-stimulated glucose oxidation.Cardiovasc Res 2011; 89(1): 148–156.
189. Todd MK, Watt MJ, Le J, Hevener AL,Turcotte LP. Thiazolidinediones en-hance skeletal muscle triacylglycerolsynthesis while protecting against fattyacid-induced inflammation and insulinresistance. Am J Physiol - EndocrinolMetab 2007; 292: E485–E493.
190. Holden NS, Squires PE, Kaur M, Bland R,Jones CE, Newton R. Phorbol ester-stimulated NF-κB-dependent transcrip-tion: roles for isoforms of novel protein ki-nase C. Cell Signal 2008; 20: 1338–1348.
191. Lee DF, Kuo HP, Chen CT, et al. IKKbetasuppression of TSC1 function links themTOR pathway with insulin resistance.Int J Mol Med 2008; 22: 633–638.
192. Zhang J, Gao Z, Yin J, Quon MJ, Ye J.S6K directly phosphorylates IRS-1 onSer-270 to promote insulin resistancein response to TNF-α signaling throughIKK2. J Biol Chem 2008; 283(51):35375–35382.
193. Bunn RC, Cockrell GE, Ou Y, ThrailkillKM, Lumpkin CK, Fowlkes JL. Palmi-tate and insulin synergistically induceIL-6 expression in human monocytes.Cardiovasc Diabetol 2010; 9: 73.
194. Emanuela F, Grazia M, de Marco R,Maria Paola L, Giorgio F, Marco B. In-flammation as a link between obesityand metabolic syndrome. J Nutr Metab2012; 2012: 476380.
195. Holland WL, Bikman BT, Wang L-P,et al. Lipid-induced insulin resistancemediated by the proinflammatoryreceptor TLR4 requires saturatedfatty acid-induced ceramide biosyn-thesis in mice. J Clin Invest 2011;121: 1858–1870.
196. Hotamisligil GS. Inflammation and en-doplasmic reticulum stress in obesityand diabetes. Int J Obes (Lond) 2008;32(Suppl 7): S52–4.
197. Hotamisligil GS. Inflammation andmetabolic disorders. Nature 2006;444: 860–867.
198. Arkan MC, Hevener AL, Greten FR,et al. IKK-[beta] links inflammation toobesity-induced insulin resistance. NatMed 2005; 11: 191–198.
199. Reyna SM, Ghosh S, Tantiwong P, et al.Elevated Toll-like receptor 4 expressionand signaling in muscle from insulin-resistant subjects. Diabetes 2008; 57:2595–2602.
200. Frisard MI, McMillan RP, Marchand J,et al. Toll-like receptor 4 modulatesskeletal muscle substrate metabolism.Am J Physiol - Endocrinol Metab 2010;298: E988–E998.
201. Barton GM, Medzhitov R. Toll-like recep-tor signaling pathways the signal tomove: D. discoideum go orienteering.Science (80-) 2003; 300(6): 1524–1525.
202. Takeda K, Akira S. Toll-like receptorsin innate immunity. Int Immunol2005; 17(1): 1–14.
203. Lee JY, Sohn KH, Rhee SH, Hwang D.Saturated fatty acids, but not unsatu-rated fatty acids, induce the expressionof cyclooxygenase-2 mediated throughtoll-like receptor 4. J Biol Chem 2001;276(20): 16683–16689.
204. Frost RA, Nystrom G, Burrows PV, LangCH. Temporal differences in the abilityof ethanol to modulate endotoxin-induced increases in inflammatorycytokines in muscle under in vivoconditions. Alcohol Clin Exp Res 2005;29: 1247–1256.
205. Frost RA, Nystrom GJ, Lang CH.Multiple Toll-like receptor ligandsinduce an IL-6 transcriptional re-sponse in skeletal myocytes. Am JPhysiol - Regul Integr Comp Physiol2006; 290: 773–784.
206. Chavez JA, Summers SA. A ceramide-centric view of insulin resistance. CellMetab 2012; 15: 585–594.
207. Davis JE, Gabler NK, Walker-Daniels J,Spurlock ME. Tlr-4 deficiency selec-tively protects against obesity inducedby diets high in saturated fat. Obesity2008; 16: 1248–1255.
208. Poggi M, Bastelica D, Gual P, et al.C3H/HeJ mice carrying a Toll-likereceptor 4 mutation are protectedagainst the development of insulinresistance in white adipose tissue inresponse to a high-fat diet. Diabetologia2007; 50: 1267–1276.
209. Shi H, Kokoeva MV, Inouye K, TzameliI, Yin H, Flier JS. TLR4 links innateimmunity and fatty acid-inducedinsulin resistance. J Clin Invest 2006;116: 3015–3025.
210. Radin MS, Sinha S, Bhatt BA, DedousisN, O’Doherty RM. Inhibition or dele-tion of the lipopolysaccharide receptorToll-like receptor-4 confers partialprotection against lipid-induced insulinresistance in rodent skeletal muscle.Diabetologia 2008; 51: 336–346.
211. Tsukumo DML, Carvalho-Filho MA,Carvalheira JBC, et al. Loss-of-functionmutation in Toll-like receptor 4 preventsdiet-induced obesity and insulin resis-tance. Diabetes 2007; 56: 1986–1998.
Long Chain Fatty Acids Induced Mitochondrial Dysfunction in Insulin Resistance
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

212. Qatanani M, Lazar MA. Mechanisms ofobesity-associated insulin resistance:many choices on the menu. Genes Dev2007; 21(12): 1443–1455.
213. Abedini A, Shoelson SE. Inflammationand obesity: STAMPing out insulinresistance? Immunol Cell Biol 2007;85: 399–400.
214. Shoelson SE, Lee J, Goldfine AB. In-flammation and insulin resistance. JClin Invest 2006; 116: 1793–1801.
215. Spranger J, Kroke A, Mohlig M, et al.Inflammatory cytokines and the riskto develop type 2 diabetes: results ofthe prospective population-basedEuropean Prospective Investigationinto Cancer and Nutrition (EPIC)-Pots-dam Study. Diabetes 2003; 52: 812–817.
216. Ji C, Chen X, Gao C, et al. IL-6 induceslipolysis and mitochondrial dysfunc-tion, but does not affect insulin-mediated glucose transport in 3T3-L1adipocytes. J Bioenerg Biomembr 2011;43: 367–375 LA – English.
217. Jové M, Planavila A, Sánchez RM,Merlos M, Laguna JC, Vázquez-CarreraM. Palmitate induces tumor necrosisfactor-α expression in C2C12 skeletalmuscle cells by a mechanism involvingprotein kinase c and nuclear factor-κBactivation. Endocrinol 2006; 147(1):552–561.
218. Coletta DK, Mandarino LJ. Mitochon-drial dysfunction and insulin resistancefrom the outside in: extracellular ma-trix, the cytoskeleton, and mitochon-dria. Am J Physiol - Endocrinol Metab2011; 301(5): E749–E755.
219. Vaamonde-García C, Valcarcel-Ares N,Riveiro-Naveira R, Lema B, Blanco FJ,López-Armada MJ. Inflammatory re-sponse is modulated by mitochondrialdysfunction in cultured normal humanchondrocytes. Ann Rheum Dis 2010;69(Suppl 2): A15–A16.
220. Håversen L, Danielsson KN, FogelstrandL, Wiklund O. Induction of proinflam-matory cytokines by long-chain saturatedfatty acids in human macrophages. Ath-erosclerosis 2009; 202: 382–393.
221. Garg AD, Kaczmarek A, Krysko O,Vandenabeele P, Krysko DV, AgostinisP. ER stress-induced inflammation:does it aid or impede disease pro-gression? Trends Mol Med 2012; 18:589–598.
222. Hummasti S, Hotamisligil GS. Endo-plasmic reticulum stress and inflamma-tion in obesity and diabetes. Circ Res2010; 107(5): 579–591.
223. Boden G. Endoplasmic reticulumstress: another link between obesityand insulin resistance/inflammation?Diabetes 2009; 58(3): 518–519.
224. Leem J, Koh EH. Interaction betweenmitochondria and the endoplasmicreticulum: implications for the patho-genesis of type 2 diabetes mellitus.Exp Diabetes Res 2012; 2012: 242984.
225. Gregor MF, Hotamisligil GS. Thematicreview series: adipocyte biology. Adipo-cyte stress: the endoplasmic reticulum
and metabolic disease. J Lipid Res2007; 48(9): 1905–1914.
226. Hotamisligil GS. Endoplasmic reticu-lum stress and the inflammatory basisof metabolic disease. Cell 2010; 140:900–917.
227. Diakogiannaki E, Morgan NG. Differen-tial regulation of the ER stress responseby long-chain fatty acids in the pancre-atic beta-cell. Biochem Soc Trans 2008;36(Pt 5): 959–962.
228. Ozcan U, Cao Q, Yilmaz E, et al. Endo-plasmic reticulum stress links obesity,insulin action, and type 2 diabetes.Science 2004; 306: 457–461.
229. Tuncman G, Hirosumi J, Solinas G,Chang L, Karin M, Hotamisligil GS.Functional in vivo interactions betweenJNK1 and JNK2 isoforms in obesity andinsulin resistance. Proc Natl Acad Sci2006; 103(28): 10741–10746.
230. Vallerie SN, Furuhashi M, Fucho R,Hotamisligil GS. A predominant rolefor parenchymal c-Jun amino terminalkinase (JNK) in the regulation of sys-temic insulin sensitivity. PLoS One2008; 3: e3151.
231. Salvadó L, Coll T, Gómez-Foix AM, et al.Oleate prevents saturated-fatty-acid-induced ER stress, inflammation and in-sulin resistance in skeletal muscle cellsthrough an AMPK-dependent mecha-nism. Diabetologia 2013; 56: 1372–1382.
232. Yuzefovych LV, Musiyenko SI, WilsonGL, Rachek LI. Mitochondrial DNAdamage and dysfunction, and oxidativestress are associated with endoplasmicreticulum stress, protein degradationand apoptosis in high fat diet-inducedinsulin resistance mice. PLoS One2013; 8: e54059.
233. Corbould A, Kim YB, Youngren JF, et al.Insulin resistance in the skeletal mus-cle of women with PCOS involves in-trinsic and acquired defects in insulinsignaling. Am J Physiol EndocrinolMetab 2005; 288: E1047–54.
234. Moura Neto A, Parisi MCR, TambasciaMA, Pavin EJ, Alegre SM, Zantut-Wittmann DE. Relationship of thyroidhormone levels and cardiovascularevents in patients with type 2 diabetes.Endocrine 2013: 1–8.
235. Brown JE. Dysregulated adipokines inthe pathogenesis of type 2 diabetesand vascular disease. Br J Diabetes VascDis 2012; 12(5): 249–254.
236. Taniguchi CM, Emanuelli B, Kahn CR.Critical nodes in signalling pathways:insights into insulin action. Nat RevMol Cell Biol 2006; 7: 85–96.
237. Cohen P. The twentieth century strug-gle to decipher insulin signalling. NatRev Mol Cell Biol 2006; 7: 867–873.
238. Stump CS, Short KR, Bigelow ML,Schimke JM, Nair KS. Effect of insulinon human skeletal muscle mitochon-drial ATP production, protein synthe-sis, and mRNA transcripts. Proc NatlAcad Sci U S A 2003; 100: 7996–8001.
239. Boirie Y, Short KR, Ahlman B, CharltonM, Nair KS. Tissue-specific regulation
of mitochondrial and cytoplasmic pro-tein synthesis rates by insulin. Diabetes2001; 50(12): 2652–2658.
240. Huang X, Eriksson KF, Vaag A, et al. In-sulin-regulated mitochondrial geneexpression is associated with glucoseflux in human skeletal muscle. Diabetes1999; 48: 1508–14.
241. Halvatsiotis PG, Turk D, Alzaid A,Dinneen S, Rizza RA, Nair KS. Insulineffect on leucine kinetics in type 2diabetes mellitus. Diabetes Nutr Metab2002; 15: 136–142.
242. Petersen KF, Dufour S, Shulman GI.Decreased insulin-stimulated ATPsynthesis and phosphate transport inmuscle of insulin-resistant offspring oftype 2 diabetic parents. PLoS Med2005; 2: e233.
243. Lanza IR, Sreekumaran Nair K. Regula-tion of skeletal muscle mitochondrialfunction: genes to proteins. Acta Phys-iol 2010; 199: 529–547.
244. Hirabara SM, Curi R, Maechler P. Satu-rated fatty acid-induced insulin resis-tance is associated with mitochondrialdysfunction in skeletal muscle cells. JCell Physiol 2010; 222: 187–194.
245. Hawley JA, Burke LM, Angus DJ,Fallon KE, Martin DT, Febbraio MA.Effect of altering substrate availabilityon metabolism and performance dur-ing intense exercise. Br J Nutr 2000;84: 829–838.
246. Savage DB, Petersen KF, Shulman GI.Disordered lipid metabolism and thepathogenesis of insulin resistance.Physiol Rev 2007; 87: 507–520.
247. Kelley DE, Mandarino LJ. Fuel selectionin human skeletal muscle in insulinresistance: a reexamination. Diabetes2000; 49(5): 677–683.
248. Koonen DPY, Glatz JFC, Bonen A,Luiken JJFP. Long-chain fatty acid up-take and FAT/CD36 translocation inheart and skeletal muscle. BiochimBiophys Acta - Mol Cell Biol Lipids2005; 1736: 163–180.
249. Watt MJ, Steinberg GR, Chen Z-P,Kemp BE, Febbraio MA. Fatty acidsstimulate AMP-activated protein kinaseand enhance fatty acid oxidation in L6myotubes. J Physiol 2006; 574(1):139–147.
250. Glatz JFC, Luiken JJFP, Bonen A.Long-chain fatty acid uptake andFAT/CD36 translocation in heartand skeletal muscle. Physiol Rev2010; 90: 367–417.
251. Cooney GJ, Lyons RJ, Crew AJ, et al.Long-chain fatty acid uptake andFAT/CD36 translocation in heartand skeletal muscle. EMBO J 2004;23: 582–593.
252. Chavez JA, Summers SA. Characteriz-ing the effects of saturated fatty acidson insulin signaling and ceramide anddiacylglycerol accumulation in 3T3-L1 adipocytes and C2C12 myotubes.Arch Biochem Biophys 2003; 419:101–109.
M. H. A. Bakar et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr

253. Schmitz-peiffer C, Craig DL, Biden TJ.Ceramide generation is sufficient to ac-count for the inhibition of the insulin-stimulated PKB pathway in C2C12 skele-tal muscle cells pretreatedwith palmitate.J Biol Chem 1999; 274: 24202–24210.
254. Chavez JA, Summers SA. Lipid over-supply, selective insulin resistance,and lipotoxicity: molecular mecha-nisms. Biochim Biophys Acta - Mol CellBiol Lipids 2010; 1801: 252–265.
255. Schrauwen P, Hesselink MKC. Oxidativecapacity, lipotoxicity, and mitochondrial
damage in type 2 diabetes. Diabetes2004; 53(6): 1412–1417.
256. Möhlig M, Isken F, Ristow M. Impairedmitochondrial activity and insulin-resistant offspring of patients withtype 2 diabetes. N Engl J Med 2004;350: 664–671.
257. Phielix E, Schrauwen-Hinderling VB,Mensink M, et al. Lower intrinsic ADP-stimulated mitochondrial respiration un-derlies in vivo mitochondrial dysfunctionin muscle of male type 2 diabetic pa-tients. Diabetes 2008; 57: 2943–2949.
258. Yuzefovych LV, Solodushko VA, WilsonGL, Rachek LI. Protection from palmitate-induced mitochondrial DNA damageprevents from mitochondrial oxidativestress, mitochondrial dysfunction, apopto-sis, and impaired insulin signaling in rat L6skeletal muscle cells. Endocrinol 2012;153(1): 92–100.
259. Wang C-H, Wang C-C, Wei Y-H. Mito-chondrial dysfunction in insulin insen-sitivity: implication of mitochondrialrole in type 2 diabetes. Ann N Y AcadSci 2010; 1201: 157–65.
Long Chain Fatty Acids Induced Mitochondrial Dysfunction in Insulin Resistance
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev (2014)DOI: 10.1002/dmrr