Embed Size (px)
Citation preview

Calcif Tissue Int (1986) 38:175-185 Calcified Tissue International �9 1986 by Springer-Verlag
Case Report
Mixed-Sclerosing-Bone-Dystrophy: 42-Year Follow-up of a Case Reported as Osteopetrosis
Roberto Pacifici, 1 William A. Murphy, 2 Steven L. Teitelbaum, 3 and Michael P. Whyte, 1
1Division of Bone and Mineral Metabolism, Department of Medicine, The Jewish Hospital of St. Louis; 2Section of Musculoskeletal Radiology, Mallinckrodt Institute of Radiology; and 3Department of Pathology and Laboratory Medicine, The Jewish Hospital of St. Louis, Washington University School of Medicine, St. Louis, Missouri, 63110
Summary. We present a detailed metabolic investi- gation and 42-year radiological follow-up of a 52- year-old man with mixed-sclerosing-bone-dys- trophy, the rare occurrence of two or more distinct patterns of sclerosing-bone-dysplasia (e.g., osteo- pathia striata, osteopoikilosis, melorheostosis) in a single subject. Review of radiographs from 1942, when he was reported to have osteopetrosis, dem- ons t ra ted diffuse os teoscleros is , os teopath ia striata, osteopoikilosis, and focal cortical hyperos- tosis. Forty-two years later, there had been signifi- cant progression and evolution of his skeletal dis- ease with the appearance of new areas of osteo- pathia striata and osteopoikilosis and a generalized increase in skeletal mass as assessed radiograph- ically. Presence of subperiosteal bone apposition on biopsy of the iliac crest together with chronic mild hypocalcemia, secondary hyperparathyroidism, and hypophosphatemia suggested that enhanced bone formation, perhaps with defective skeletal re- sorption, is a fundamental abnormality which ac- counts for the increased bone mass of this patient.
Key words: Osteopetrosis - - Osteosclerosis - - Os- teopoikilosis - - Osteopathia striata - - Melorheos- tosis.
Send reprint requests to Dr. William A. Murphy, Mallinckrodt Institute of Radiology, 510 South Kingshighway, St. Louis, Mis- souri 63110.
The term "sclerosing-bone-dysplasia" is used to describe a group of sporadic or inherited disorders which are characterized by different patterns of in- creased bone mass that locally or diffusely involve the skeleton [1, 2]. Osteopetrosis (marble bone dis- ease) is the best known, but many others-- in- cluding osteopathia striata, osteopoikilosis, and melorheostos is- -have been recognized. Osteo- pathia striata is characterized by asymptomatic, symmetrical, dense linear striations in the long bones and pelvis. Osteopoikilosis manifests as be- nign, symmetrical , periarticular foci of osteo- sclerosis which produce a spotted appearance. Melorheostosis is an asymmetrical hyperostosis, generally of long bones, which may cause pain and deformity [1, 2]. In 1964, Walker introduced the term "mixed-sclerosing-bone-dystrophy" (MSBD) to describe two patients in whom osteopathia striata, osteopoikilosis, and melorheostosis oc- curred together [3]. MSBD has subsequently been used to indicate the extremely rare occurrence of two or more of these patterns of osteosclerosis in a single subject.
We describe herein the clinical, biochemical, ra- diological, and histopathological investigation of a patient with MSBD who was reported in 1943 as the 120th case of osteopetrosis [4]. Our study reveals that individual osteosclerotic lesions in MSBD can evolve with a progressive increase in skeletal mass, and that the pathogenesis of some cases of MSBD may involve enhanced bone formation perhaps with defective skeletal resorption.
176 R. Pacifici et al.: Mixed-Sclerosing-Bone-Dystrophy
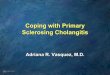
Fig. 1. At age 52, the patient had a large narrow cranium with a prominent jaw and forehead.
Case Report
This 52-year-old Caucasian man of French-English extraction was referred to the Division of Bone and Mineral Metabolism at the Washington University Medical Center, St. Louis, Missouri. A chest X-ray at this time revealed abnormal bone density. His medical history was remarkable. He was born 4 weeks prema- turely by a difficult forceps delivery. He weighed 2.3 kg at birth at which time a large head was noted. He walked at 18 months, but his gait was always stiff and awkward. At age 3 years, hearing loss was documented after he was treated for bilateral middle ear abscesses. Audiometry revealed both conduction and nerve deafness bilaterally. Adenoidectomy and tonsillectomy did not alleviate the auditory problems and he began to use a hearing aid at age 7. After head trauma, also at age 7, he developed left facial paralysis which persisted for about 1 year. At age 9, symptoms of nasal obstruction were noted and attributed to "bone thickening." In 1942, at age 10, radiological studies were first performed and a limited survey disclosed generalized os- teosclerosis. The case was reported by Dr. Carl A. W. Zim- mermann in 1943 as the 120th example of osteopetrosis [4], but the patient was then lost to follow-up.
From age 10-19 years, he suffered intense headaches which lasted several days and occurred about every 2 weeks. He was generally well from age 19 until age 49 when evaluation for rectal bleeding disclosed polyps in the sigmoid colon which were re- sected but recurred. At age 51, cholecystectomy was performed after an episode of biliary colic. Diagnostic studies at that time
also revealed asymptomatic nephrolithiasis. He had experienced worsening depression since age 50 for which he received antide- pressive medication and had been hospitalized elsewhere for a 3-month history of anorexia with mild weight loss. During that hospitalization, a new colonic polyp was resected endoscopi- cally. Ostensibly, a duodenal neoplasm was suspected and he underwent an exploratory laparotomy with duodenotomy, but nothing unusual was found. Postoperatively, however, he had several episodes of ventricular tachycardia and was transferred to the Washington University Medical Center. Once the ar- rhythmia had been controlled medically, he was referred to our service. The patient was somewhat wasted, kyphotic, had a large narrow cranium, prominent brow, asymmetric large jaw, and was edentulous (Figs. 1A & B). Vital signs were normal. Rales were present bilaterally, the liver was 10 cm in span and palpable 2 cm below the right costal margin. His cranial nerves were intact except for bilateral deafness. The remainder of the physical examination was unremarkable.
Laboratory Studies
In May and July of 1984, during admissions to the Adult Clinical Research Center, Washington University Medical Center, the following studies were negative or normal: serum electrolytes, urea nitrogen, creatinine, total bilirubin, uric acid, total protein, glutamic-pyruvic transaminase, lactate dehydrogenase, caro-
R. Pacifici et al.: Mixed-Sclerosing-Bone-Dystrophy
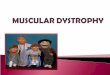
Table 1. Mineral metabolism studies in mixed-sclerosing-bone-dystrophy a
177
Date Blood
Calcium (mg/dl)
Urine
Inorganic Alkaline phosphate phosphatase 25OHD b 1,25(OH)2 Dc PTH Calcitonin b Calcium (mg/dl) (IU/L) (ng/ml) (pg/ml) p~Leq/ml (pg/ml) (mg/day)
Hydroxy- Hydroxy- proline b proline b
Phosphorus (total (free (mg/day) mg/day) mg/day)
5/81 9.2 1.8 338 2/82 9.2 1.7 380
10/83 8.9 2.2 412 4/84 8.1 1.6 346 5/84 8.0 1.7 314 7/84 8.1 1.8 286
(9.0-10.3) (2.5-4.5) (45-115)
10 60 18 <50 68 854 61 0.8 25 55 18 - - 86 282 53 0.5
(10-55) (20-76) (2-10) (0-450) (50-250) (400-1300) (25-77) (0-2)
a Normal ranges, given in parentheses at the bottom of data columns, are for the Clinical Chemistry Laboratory, Barnes Hospital, St. Louis, MO (5/84 and 7/84) b BioScience, Van Nuys, California c Consolidated Bio-Medical Labs, Wichita, Kansas
Fig. 2. Lateral skulli A. In 1942, radiographs disclosed diffuse osteosclerosis and failure of pneumatization of the paranasal sinuses. B. In 1984, there was a similar degree of osteosclerosis, edentia, and a hearing aid. The apparent difference in overall mineral content of the skull between 1942 and 1984 is a technical artifact of the 1942 exposure factors. The actual mineral content is nearly identical when exposure factors are equalized.
tene, protein electrophoresis, but serum cholesterol was low (142 and 151 mg/dl: normal 158-276). Platelet and white blood cell counts, leukocyte differential, and erythrocyte sedimenta- tion rate were normal, but he had a mild normochromic/normo- cytic anemia (Hg 10.7 g/dl; Hct 33%). Urinalysis was normal and urinary screen for aminoacids and mucopolysaccharides was negative.
Mineral metabolism was extensively investigated in May and July, 1984 (Table I). Hypophosphatemia, hypocalcemia, mark- edly increased circulating alkaline phosphatase activity, and in- creased immunoreactive parathyroid hormone (carboxy-ter- minal) were noted on both admissions. Phosphorus excretion appeared to be excessive for the degree of hypophosphatemia. However, circulating immunoreactive calcitonin, 25-hydroxyvi-
178 R. Pacifici et al.: Mixed-Sclerosing-Bone-Dystrophy
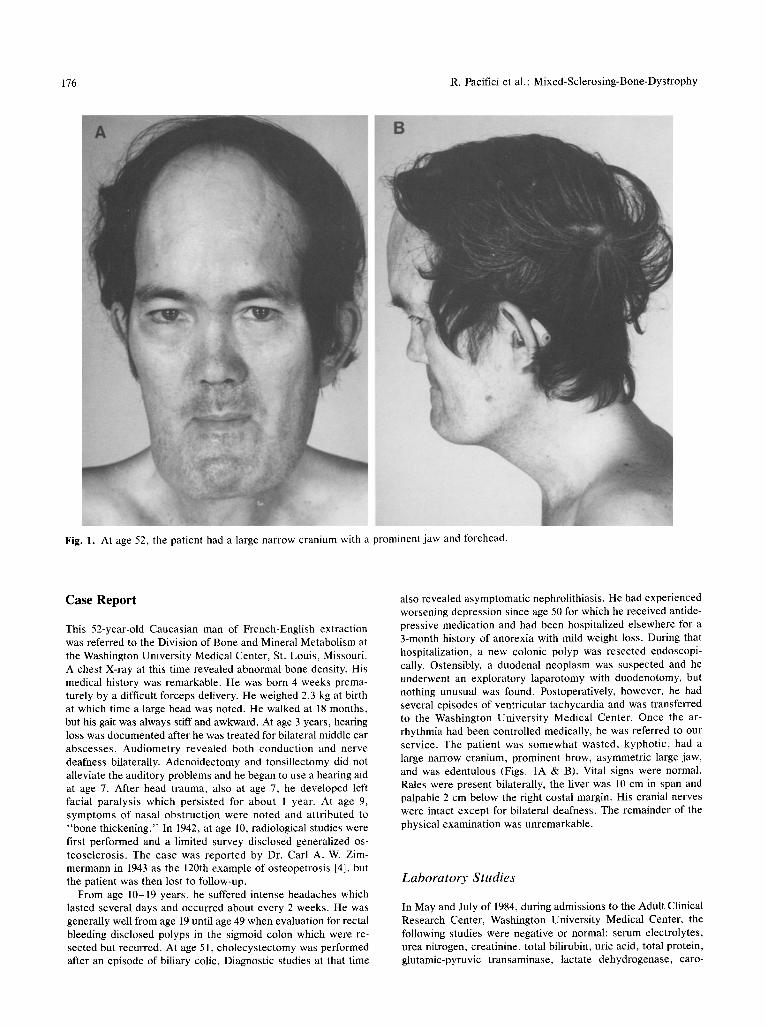
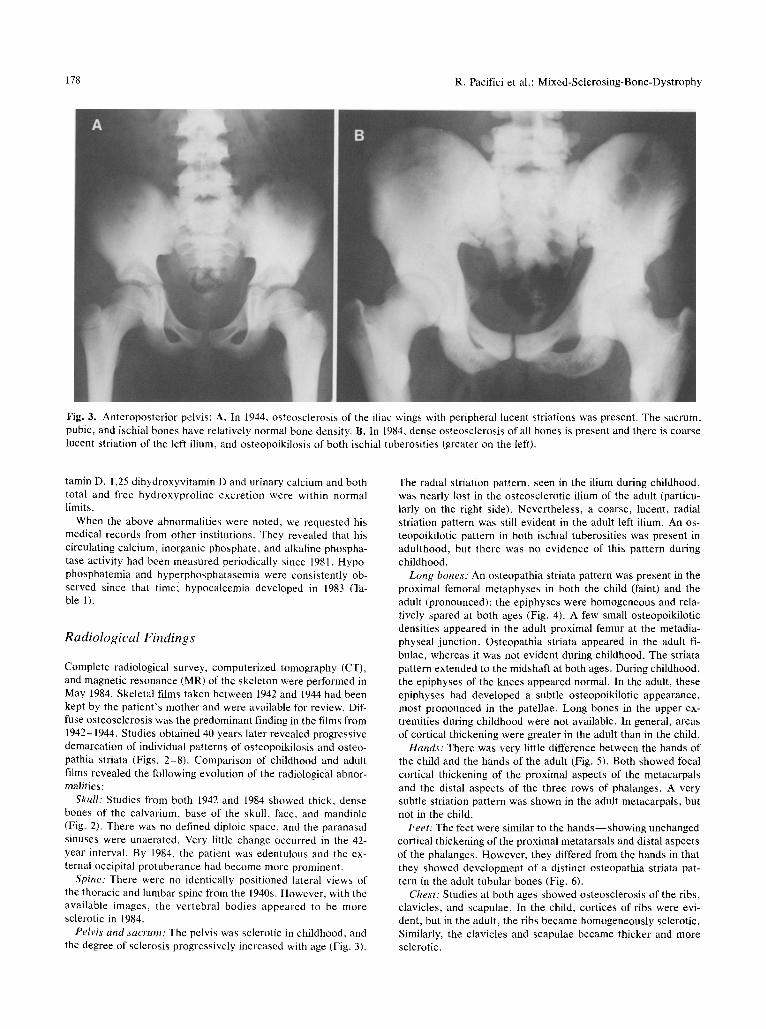
Fig. 3. Anteroposterior pelvis: A. In 1944, osteosclerosis of the iliac wings with peripheral lucent striations was present. The sacrum, pubic, and ischial bones have relatively normal bone density. B. in 1984, dense osteosclerosis of all bones is present and there is coarse lucent striation of the left ilium, and osteopoikilosis of both ischial tuberosities (greater on the left).
tamin D, 1,25 dihydroxyvitamin D and urinary calcium and both total and free hydroxyproline excretion were within normal limits.
When the above abnormalities were noted, we requested his medical records from other institutions. They revealed that his circulating calcium, inorganic phosphate, and alkaline phospha- tase activity had been measured periodically since 1981. Hypo- phosphatemia and hyperphosphatasemia were consistently ob- served since that timei hypocalcemia developed in 1983 (Ta- ble 1).
Radiological Findings
Complete radiological survey, computerized tomography (CT), and magnetic resonance (MR) of the skeleton were performed in May 1984. Skeletal films taken between 1942 and 1944 had been kept by the patient's mother and were available for review. Dif- fuse osteosclerosis was the predominant finding in the films from 1942-1944. Studies obtained 40 years later revealed progressive demarcation of individual patterns of osteopoikilosis and osteo- pathia striata (Figs. 2-8). Comparison of childhood and adult films revealed the following evolution of the radiological abnor- malities:
Skull: Studies from both 1942 and 1984 showed thick, dense bones of the calvarium, base of the skull, face, and mandible (Fig. 2). There was no defined diploic space, and the paranasal sinuses were unaerated. Very little change occurred in the 42- year interval. By 1984, the patient was edentulous and the ex- ternal occipital protuberance had become more prominent.
Spine: There were no identically positioned lateral views of the thoracic and lumbar spine from the 1940s, However, with the available images, the vertebral bodies appeared to be more sclerotic in 1984.
Pelvis and sacrum: The pelvis was sclerotic in childhood, and the degree of sclerosis progressively increased with age (Fig. 3).
The radial striation pattern, seen in the ilium during childhood, was nearly lost in the osteosclerotic ilium of the adult (particu- larly on the right side). Nevertheless, a coarse, lucent, radial striation pattern was still evident in the adult left ilium. An os- teopoikilotic pattern in both ischial tuberosities was present in adulthood, but there was no evidence of this pattern during childhood.
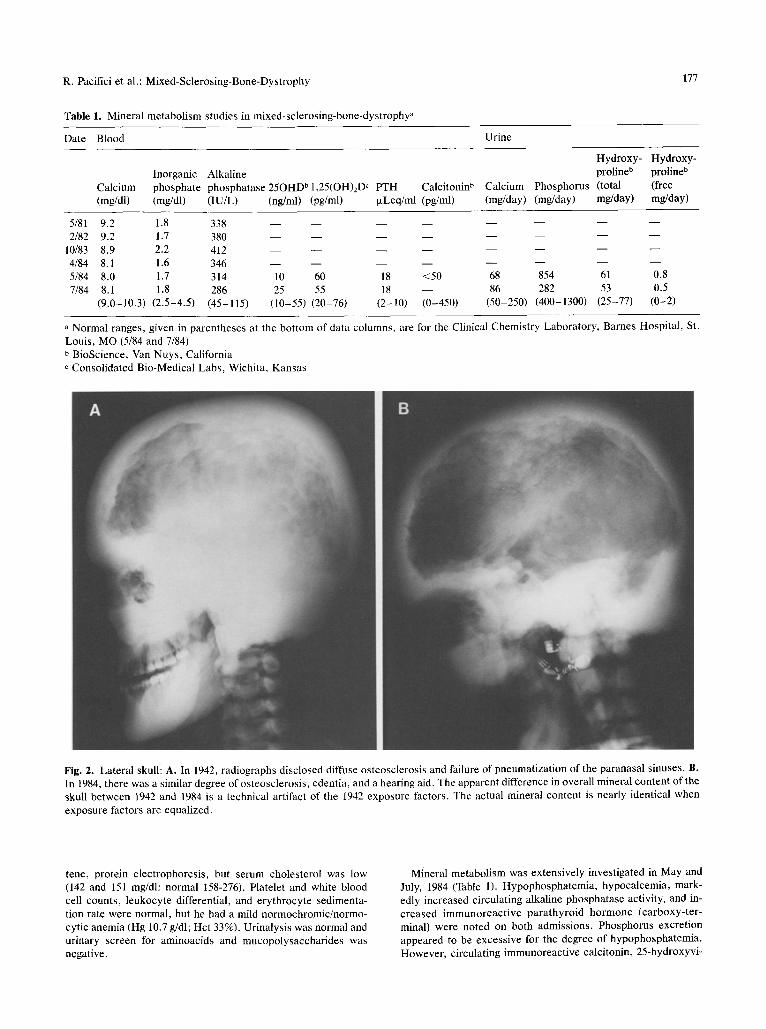
Long bones. An osteopathia striata pattern was present in the proximal femoral metaphyses in both the child (faint) and the adult (pronounced); the epiphyses were homogeneous and rela- tively spared at both ages (Fig. 4). A few small osteopoikilotic densities appeared in the adult proximal femur at the metadia- physeal junction. Osteopathia striata appeared in the adult fi- bulae, whereas it was not evident during childhood. The striata pattern extended to the midshaft at both ages. During childhood, the epiphyses of the knees appeared normal. In the adult, these epiphyses had developed a subtle osteopoikilotic appearance, most pronounced in the patellae. Long bones in the upper ex- tremities during childhood were not available. In general, areas of cortical thickening were greater in the adult than in the child.
Hands: There was very little difference between the hands of the child and the hands of the adult (Fig. 5). Both showed focal cortical thickening of the proximal aspects of the metacarpals and the distal aspects of the three rows of phalanges. A very subtle striation pattern was shown in the adult metacarpals, but not in the child.
Feet: The feet were similar to the hands--showing unchanged cortical thickening of the proximal metatarsals and distal aspects of the phalanges. However, they differed from the hands in that they showed development of a distinct osteopathia striata pat- tern in the adult tubular bones (Fig. 6).
Chest: Studies at both ages showed osteosclerosis of the ribs, clavicles, and scapulae. In the child, cortices of ribs were evi- dent, but in the adult, the ribs became homogeneously sclerotic. Similarly, the clavicles and scapulae became thicker and more sclerotic.

R. Pacifici et al.: Mixed-Sclerosing-Bone-Dystrophy 179
striata pattern (Fig. 7D). A sagittal MR image of the head and neck clearly demonstrated the thickened bone as well as entrap- ment of the spinal cord and cerebellar tonsils at the foramen magnum (Fig. 8).
Bone scintigraphy--performed with 20 mCi Tc-99m meth- ylene diphosphonate given intravenously--showed strikingly uniform uptake throughout the long bones with lack of the usual distinction between the cortex and medullary cavity. The skull had an unusual appearance with a dense calvarium, large man- dible, and flattened facial bones. The appearance of the other bones were relatively unremarkable except for mild generalized increased activity with reduced soft tissue uptake.
Fig. 4. Anteroposterior knees: A. In 1944, there was faint os- teopathia striata only of the femoral and tibial metadiaphyses, but all epiphyses were normal. B. In 1984, distinct osteopathia striata is present in the femur, tibia, and fibula (a very faint os- teopoikilotic pattern of the epiphyses has appeared).
CT, MR, and Bone Scintigraphy Imaging
CT examinations were performed with a Siemens DR3 scanner; sections were 8 mm thick. In general, the CT images of the ex- tremities showed dense epiphyseal and metaphyseal medullary canals (Fig. 7A). The metaphyses had an alternating pattern of round radiolucencies and radiodensities. The epiphyses were more homogeneous and of more normal pattern (Fig. 7B). The surrounding cortex was normal in pattern and thickness. Head CT showed thickened bone and unpneumatized maxillary and sphenoid sinuses. The brain parenchyma had normal anatomy, but the ventricles were large.
Magnetic resonance examinations were performed with a su- perconductive system operating at 0.35 Tesla (15 MHz). Spin- echo pulse sequences were utilized with multisection, dual-echo parameters. One centimeter-thick sections were obtained in transverse, coronal, and sagittal planes depending on the region studied. In general, the MR images showed a low signal from cortical and medullary bone, with some sparing of the epiphyses where a greater signal was generated because of a greater amount of bone marrow (Fig. 7C). The metaphyses produced an alternating pattern of low signal areas (corresponding to the dense osseous striations) and high signal areas (corresponding to areas of residual marrow in the restricted spaces between the bony striata). Coronal images of the distal femora revealed the
Pathologic Findings
Trephine biopsy of the right iliac crest was performed with diffi- culty in May 1984. The microscopic appearance of this espe- cially hard specimen suggested that it consisted of two pieces of cortical bone. The thickness of the cortex was markedly in- creased, yet its porosity appeared to be unremarkable (Fig. 9A). Haversian channels were numerous and lined by osteoid seams, most of which were covered by large and fusiform osteoblasts. Osteoclasts were unremarkable in number and appearance. By polarizing microscopy, the bone was completely lamellar in ap- pearance (Fig. 9B) except for a thick periosteal band of woven bone (which demonstrated no secondary remodeling) in the peri- osteal region. Prior to the iliac crest biopsy, the patient had been instructed to take two 3-day courses of oxytetracycline (1 gram daily) separated by 2 weeks, with the last dose 4 days before biopsy. However, by ultraviolet microscopy, tetracycline fluo- rescence was not observed (Fig. 9C).
Family Study
The patient 's parents and three brothers are alive and well. Family history is negative for bone disease. Assay of blood and urine for calcium and inorganic phosphate, and a limited radio- logical survey were nnremarkable in the mother and one of the brothers. The patient's two brothers and father have had radio- graphs of the chest which were ostensibly normal.
Discussion
Although our patient was reported in the medical literature in 1943 as the 120th example of osteope- trosis [4], review of the original radiographs from the 1940s revealed areas of osteopathia striata and focal cortical hyperostosis--features not in keeping with that diagnosis. Furthermore, a specimen of his iliac crest obtained during our investigation showed histopathological changes which were inconsistent with osteopetrosis; i.e., there were no areas of car- tilage within mature bone--changes which would be reflective of a failure of osteoclasts to resorb the primary spongiosa of endochondral bone formation [5]. Alternatively, it is clear from the radiological

180 R. Pacifici et al.: Mixed-Sclerosing-Bone-Dystrophy
Fig. 5. Posteroanterior hands: A. In 1942, cortical thickening (but no osteopathia striata or osteopoikilosis) was present, B. In 1984, faint osteopathia striata of the metacarpals has appeared.
features, that our patient had a mixed-sclerosing- bone-dystrophy (MSBD).
Natural History of MSBD
Previous reports concerning isolated cases of os- teopoikilosis and osteopathia striata generally have not reported an evolutionary pattern for the radio- logical abnormalities [6], possibly because patient follow-up was brief. In our patient, comparison of the childhood and adult radiographs disclosed inter- esting changes in the patterns of osteosclerosis. Osteopathia striata, in particular, became more pro- nounced in some regions (femoral and tibial me- taphyses) and appeared elsewhere in new areas (fibulae, hands, feet). Similarly a faint pattern of osteopoikilosis developed at several new sites (is- chial tuberosities, femoral epiphyses). Further-
more, cancellous sclerosis progressed in some areas (vertebral bodies, sacrum, and ribs) and even- tually obscured the osteopathia striata pattern in portions of the pelvis. These findings demonstrated that a developmental and evolutionary behavior of the osteopoikilosis, osteopathia striata, and gener- alized sclerosis can occur in MSBD.
Our study provided some new information con- cerning the anatomy of MSBD. CT and the MR ex- aminations revealed that the dense metaphyseal striations of osteopathia striata are not cortical ab- normalities, but occur in the medullary space of long bones. The MR coronal images showed these striations to be low signal, sharp, columnar areas of dense bone. In general, CT and MR imaging showed the same anatomical features, i.e., that os- teopathia striata and osteopoikilosis patterns are not cortical abnormalities (periosteal and/or sub- periosteal), but are within the medullary space.

R. Pacifici et al.: Mixed-Sclerosing-Bone-Dystrophy 181
Fig. 6. Anteroposterior feet: A. In 1942, cortical thickening, but no osteopathia striata or osteopoikilosis, was noted. B. In 1984, there is pronounced osteopathia striata of the tubular bones.
Classification of MSBD
The term MSBD was coined by Walker in 1964 to describe 2 patients with osteopathia striata, osteo- poikilosis, and melorheostosis [3]. Subsequently, several similar cases have been reported [7-11]. In a recent review, we cautioned that the term MSBD has been used to describe cases in which the radio- logical features actually differ [11], but that tenta- tive classification of at least four sub-types of MSBD--each characterized by specific associa- tions of two or more osteosclerotic pa t te rns- - seemed helpful [11]. The patient reported herein had all of the radiological features of MSBD type III, yet did not fit satisfactorially into this group ei- ther, since he also displayed diffuse osteosclerosis. However, we documented that his skeletal lesions evolved. We conclude, therefore, that a definitive classification and understanding of patients with MSBD may require serial radiographic study. We continue to suggest, however, that the term MSBD be used "generically" to describe the occurrence
of two or more of the distinct sclerotic bone dys- plasias in a single patient; our suggested classifica- tion should remain tentative, and any attempt to re- fine the nosology of MSBD will require study of additional cases and delineation of their natural his- tory.
Pathogenesis of MSBD
Although we were able to investigate only our pa- tient's mother and one of his two brothers--his fa- ther and other brother also have negative histories for skeletal disease and have had ostensibly normal radiographs of the chest. This would suggest that our patient's bone dysplasia occurred sporadically, a finding in keeping with all previously reported cases of MSBD [11].
Several mechanisms could account for the skel- etal sclerosis in our patient. The complex associa- tion of osteosclerotic patterns could, in theory, re- sult from localized increases in bone formation and/

182 R. Pacifici et al.: Mixed-Sclerosing-Bone-Dystrophy
Fig. 7. Sectional imaging of long bones: A. CT (transverse image) of the distal femora shows dense metaphyseal spots which are cross-sections of the longitudinal striations. B. CT image through the proximal tibiae shows a nearly normal epiphysis on the right, but dense metaphyseal spots on the left. C. MR (transverse image, TR 500/TE 30) of the distal femora--corresponding to CT image (A)--shows striations and residual marrow as black and white areas, respectively. D. Coronal MR image (TR 500/TE 30) of the knees revealed striations (longitudinal black bands) of the metadiaphyseal regions, and relative sparing of the epiphyses (nearly homogeneous high signals from the marrow).
Fig. 8. Sagittal MR image (TR 300/TE 30) of the head shows a very thick skull and entrapment of the spinal cord and cerebellar tonsils at the foramen magnum.
or decreased bone resorption. The appearance of the osteoclasts in our patient's dense iliac crest bone was normal, and biochemical indices of os- teoclast activity (such as serum acid phosphatase activity and urinary hydroxyproline excretion) were also unremarkable. Furthermore, the histo- pathological paradigm of life-long osteoclast dys- funct ion-presence of cartilage within mature bone as found in osteopetrosis [5]--was also absent in this patient and one other with MSBD [I1]. Carti- lage within trabecular bone in osteopetrosis reflects the failure of osteoclasts to resorb endochondral skeletal tissue. Thus, a profound life-long defect in osteoclastic bone resorption does not appear to ex- plain the pathogenesis of MSBD.
Although medical information relevant to our pa- tient's mineral metabolism was limited to the 3-year period prior to his referral, there appeared to be some consistent biochemical abnormalities. Hypo- phosphatemia and hyperphosphatasemia were always present. Despite hypophosphatemia, his

R. Pacifici et al.: Mixed-Sclerosing-Bone-Dystrophy 183
4"," , ~ :i~ �84 "> "'~ :j: iii{
~: �9 ~�9 :�9 �84
Fig. 9. Histopathological studies of mixed- sclerosing-bone-dystrophy: A. Undecalcified section of iliac crest (Masson tr ichrome stain, 39 x ) reveals a markedly increased mineralized bone mass (staining blue) wherein the entire specimen appears as cortex; no corticomedullary junct ion is apparent (P = periosteal surface). Haversian canals (arrows) are numerous and generally lined by osteoid seams (staining red) of unremarkable thickness. B. Decalcified section of iliac crest examined by polarizing microscopy (156 x ) revealed a normal pattern of lamellar bone (L) within deeper areas of the cortex. However, a thick band of woven collagen (which demonstrates no secondary bone remodeling) is also present (delineated by the arrows) in the subperiosteal region. C. Fluorescence microscopy of the pat ient 's bone (A) failed to show discrete yellow "tetracycl ine labels" indicative of active bone formation (B = control subject; arrows illustrate discrete bands of tetracycline; MB = mineralized bone) [magnification • 160].

184 R. Pacifici et al.: Mixed-Sclerosing-Bone-Dystrophy
urinary phosphorus levels were normal during the first clinical research center admission when his nutritional status was poor, but improving. Phos- phaturia in the presence of hypophosphatemia may, in part, be explained by a secondary hyperpara- thyroidism; his circulating calcium concentration was at the lower range of normal (from 1981 to 1982) and clearly subnormal (since 1983). Although his caloric intake was probably poor for about 3 months prior to our studies, circulating 25(OH)D and 1,25(OH)2D levels were normal. Perhaps our observation of normal vitamin D status could be ex- plained by the fact that his nutritional status was recovering in hospital. Poor nutrition with vitamin D deficiency, however, is an unlikely explanation for our patient's chronic (at least 3 years) hypocal- cemia or hypophosphatemia. Dietary malabsorp- tion was unlikely, since we found his serum caro- tene concentration and absorption of d-xylose to be normal. Furthermore, iliac crest biopsy showed no evidence of osteomalacia. Since our patient's bone density increased significantly with time (as ob- served radiologically), his chronic hypocalcemia and secondary hyperparathyroidism might reflect, instead, increased skeletal avidity for calcium. His- topathological studies were especially interesting in this regard, since iliac crest biopsy revealed a thick subperiosteal band of woven bone. This was a striking finding since periosteal bone apposition is usually inactive after the third decade of life [12]. Our patient's markedly increased circulating alka- line phosphatase activity (an index of osteoblast ac- tivity) is in keeping with an enhanced rate of bone formation. A perplexing finding in our patient, however, was that tetracycline "labels" were not present on ultraviolet m i c r o s c o p y - - a feature present in bone of patients with normal or in- creased rates of skeletal mineralization [13]. We are unable to conciliate the absence of tetracycline labels with the hypothesis that increased bone for- mation accounts for the progression of osteoscle- rosis. Perhaps our patient had defective tetracy- cline absorption from the GI tract, was not com- pliant in taking the drug, or was experiencing a period of quiescent bone formation at the time of biopsy. We feel that he was deeply interested in our studies and, therefore, believe he took the oxyte- tracycline. We have no evidence for gastrointes- tinal malabsorption and therefore feel that at the time of iliac crest biopsy, bone formation was qui- escent. The explanation for quiescent bone forma- tion at the time we performed the iliac crest biopsy may be in the period of poor nutrition which our patient suffered prior to our studies. In rats, semis- tarvation has been found to profoundly suppress
bone formation and result in a failure of bone to assume tetracycline labels [14].
We are unable to assess the impact of our pa- tient's secondary hyperparathyroidism on his bone disease. Indeed, the duration of this metabolic ab- normality is uncertain. However, the evolution of his MSBD--wi th appearance of osteopoikilosis and intensification of the osteopathia striata pat- tern--cannot be attributed to enhanced PTH effect as these radiographic findings have not been re- ported in hyperparathyroidism. Furthermore, we have observed osteopathia striata to be a develop- mental finding in one kindred wherein no metabolic abnormalities were noted [15]. Finally, no evidence of PTH excess was noted on histological examina- tion of iliac crest bone from our patient.
In summary, therefore, our detailed study of one patient with MSBD reveals that this sclerosing bone dysplasia, unlike osteopetrosis, does not ap- pear to be the result of a life-long defect in resorp- tion of endochondral bone. Although not supported by the finding of tetracycline labels on bone his- tology, our observations of subperiosteal new bone, which did not appear to be undergoing active bone remodeling, together with chronic hypocalcemia, secondary hyperparathyroidism, and hypophos- phatemia suggest that periods of enhanced bone formation, perhaps with some component of re- duced bone resorption, is a possible pathogenetic mechanism for MSBD.
Acknowledgment. We are indebted to the nursing and dietary staffs of the Adult Clinical Research Center at the Washington University Medical Center for making this study possible, to Mrs. Michele A. Bergfeld for processing the iliac crest spec- imens, and to Bernice Kaplan and Frances Ledbetter for secre- tarial assistance. This study was supported in part by grant RR-00036 for the General Clinical Research Center Branch, Di- vision of Research Facilities and Resources, National Institutes of Health and a grant-in-aid from the Shriners Hospitals for Crippled Children.
References
1. Beighton P, Cremin B (1980) Sclerosing bone dysplasias. Springer-Verlag, Berlin, Heidelberg, New York
2. Resnick D, Niwayama G (1981) Diagnosis of bone and joint disorders. W. B. Saunders, Philadelphia, pp 2972-2973
3. Walker GF (1964) Mixed sclerosing bone dystrophies. J Bone Joint Surg (Br) 46:546-552
4. Zimmermann CAW (1943) Osteopetrosis (Albers-Schonberg Disease), with case report. Radiology 40:155-162
5. Jowsey J (1977) Metabol ic d iseases of bone . W. B. Saunders, Philadelphia, p. 174
6. Horan FT, Beighton PH (1978) Osteopathia striata with c r a -

R. Pacifici et al.: MiXed-Sclerosing-Bone-Dystrophy 185
nial sclerosis. An autosomal dominant entity. Clin Genet 13:201-206
7. Abrahamson MN (1968) Disseminated asymptomatic os- teosclerosis with features resembling melorheostosis, osteo- poikilosis, and osteopathia striata. J Bone Joint Surg (Am) 50:991-996
8. Elkeles A (1976) Mixed sclerosing bone dystrophy with re- gression of melorheostosis (Letter) Br J Radiol 49:97
9. Ewald FC (1972) Unilateral mixed sclerosing bone dys- trophy associated with unilateral lymphangiectasis and cap- illary hemangioma. J Bone Joint Surg (Am) 54:878-880
10. Kanis JA, Thomson JG (1975) Mixed sclerosing bone dys- t rophy with regression of melorheostosis . Br J Radiol 48:400-402
11. Wbyte MP, Murphy WA, Fallon MD, Hahn TJ (1981) Mixed-sclerosing-bone-dystrophy: report of a case and re- view of the literature. Skeletal Radiol 6:95-102
12. Epker BN, Frost HM (1965) A histological study of remod- eling at the periosteal, haversian canal, cortical endosteal, and trabecular endosteal surfaces in human rib. Anatomical Record 152:129-136
13. Shires R, Avioli Lu Bergfeld MA, Fallon MD, Slatopolsky E, Teitelbaum SL (1980) Effects of semistarvation on skel- etal homeostasis. Endocrinology 107:1530-1535
14. Fallon MD, Teitelbaum SL (1982) The interpretation of fluo- rescent tetracycline marking in the diagnosis of metabolic bone disease. Human Pathol 13:416-418
15. Whyte MP, Murphy WA (1979) Osteopathia striata asso- ciated with familial dermopathy and white forelock: evi- dence for postnatal development of osteopathia striata. Am J Medical Genetics 5:227-234
Received July 9, 1985, and in revised form September 6, 1985