Embed Size (px)
DESCRIPTION
kedokteran
Citation preview

UROLITHIASIS
Basuki B Purnomo, Besut Daryanto, Kurnia Penta Seputra, Paksi Satyagraha
DEPARTMENT OF UROLOGYSAIFUL ANWAR HOSPITAL/ BRAWIJAYA MEDICAL FACULTY
MALANG 2014


LEARNING OBJECTIVESAt the end of medical school, the medical student will be able to... • List risk factors for the most common types of kidney stones • Contrast differences between the clinical presentation of acute
renal colic versus an acute abdomen • Name 4 kidney stone chemical compositions • Describe the imaging study to diagnose kidney or ureteral stones • Describe 3 types of medications effective for relief of renal colic
pain • List 3 clinical situations that warrant urgent decompression of a
ureteral stone • List 2 types of medications that may help medical expulsion
therapy of a distal ureteral stone • Describe two medical prophylaxis options for hypercalciuria • List 2 common surgical techniques to manage a renal stone and a
ureteral stone that fails to pass with observation

Level of competence
Sumber: SKDI 2013

Level of competence
Sumber: SKDI 2013

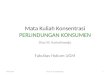
352411
101 11489 78
229
0
100
200
300
400
500
Urolithiasis BPH Urethral stricture
Malignancy Testicular disease Traumatology
Others
Urologic Operations in Saiful Anwar Hospital Oct 2001 - Sept 2006

EPIDEMIOLOGY OF UROLITHIASIS
Renal calculi are the predominant cause of urinary stone disease in the industrialized western worldAnnual incidence in U.S. up to 164 per 100,000 or 12% over lifetime (Rochester, MN, 1979)Male : female ratio = 3 : 1


Diseases Associated with Kidney Stones
Hypertension
Low Bone Density
Obesity

Epidemiologic aspects
Genetics
Age & sex
Geography
Climatic & seasonal factorsWater intake
Diet
Occupation
Stress
Intrinsic factors Extrinsic factors
(Menon & Resnick, 2002)

Urolithiasis: Composition, frequency, causes
Composition Frequency Causes & Mechanism
Calcium oxalateor calcium phosphate
70%–80% HypercalciuriaLow urine volumeHyperuricosuriaHyperoxaluriaLow urine citrate
Uric acid 10%–15% Low urine pH, defect in renal ammonium secretion
Magnesium ammoniumphosphate (struvite,infection-related)
10%–15% Urine infection (urea-splitting bacteria)
Cystine Autosomal recessive
< 1% Cystinuria, the four dibasic amino acids are cystine, ornithine, lysine, and arginine, hence the mnemonic: COLA.
Others < 1%

About 80% of stones are calcium based, and about 80% of those are calcium oxalate stones.

Etiology

(Evan et al, 2005)

(Evan et al, 2005)
Initial site of crystal deposition

Pro-Stone Forces
Stone Inhibitors• Calcium
• Uric Acid
• Oxalate
• Cystine
• Infection
• Volume (dilution)
• Citrate
• “Alkaline urine”
Pro-stone forces & inhibitors

Risk factors
History of prior calcium urolithiasis
Family history of urolithiasis
Dehydration and consequent increase urine concentration
Increase enteric absorption of oxalate
UTI
Medication that promote crystalluria (Sulfadiazine, Triamteren, Indinavir, Acetazolamide)
Urinary tract obstruction

Risk factors
Hypertension: risk of stone formation increase x 2 (hypercalciuria?)
Dietary habits soft drinks acidified with phosphoric acid increase calcium stone formation..
Coffee, tea,wine decrease risk of of stone formation
grapefruit and tomato juice increase the risk.

Pathophisiology
Stones
Infection
Obstruction

Infection StonesOften magnesium-ammonium-phosphate (MAP) or struvite.
Key is excess ammonium – NH4+.
Ammonium produced to excess due to urease (cleaves urea) which generates ammonia (NH3) and CO2.
NH3 + H+ (urine pH) NH4+.

Alkalinization of urine by urease producing organism
NH2-CO-NH2 + H2O 2NH3 + CO2
NH3 + H20 NH4+ + OH-
CO2 + H2O H2CO3
H2CO3 H + + HCO3- 2H + + CO3
-
(pK: 10.1)
urease


Clinical presentation
The classic presentation of a renal stone: is acute, colicky flank pain radiating to the groin or scrotum.
As the stone descends in the ureter: pain may localize to the abdomen overlying the stone.
As the stone approaches the ureterovesical junction: lower quadrant pain, urinary urgency, frequency, and dysuria are common, mimicking bacterial cystitis.

A family history of renal calculi is present in 55% of patients with recurrent stones.
Stones occur three times more frequently in men with a family history of stones.

Physical ExaminationThe physical exam typically shows a distressed patient, often writhing, while trying to find a comfortable position.
In contrast, patients with an acute abdomen typically have board-like abdominal rigidity and do not want to move.
Costovertebral angle or lower quadrant tenderness may be present.
A distal ureteral calculus at the ureterovesical junction in a woman may be palpated on vaginal exam.

Gross or microscopic hematuria is present in approximately 90% of patients.
Importantly, the absence of hematuria with acute flank pain does not preclude renal or ureteral calculi as there may be complete obstruction.
Hydronephrosis and renal capsular distension may also produce nausea and vomiting.

Differential diagnosis of acute renal colic in adults
Renal or ureteral stone
Hydronephrosis
Bacterial cystitis or pyleonephritis
Acute abdomen (bowel, biliary, pancreas or aortic abdominal aneurysm sources)
Gynecologic (ectopic pregnancy, ovarian cyst torsion or rupture)
Radicular pain (L1 herpes zoster, sciatica)
Referred pain (orchitis)

DiagnosisThe current gold standard for confirming urinary stones in the setting of acute flank pain is an unenhanced, helical computed tomography (CT) scan of the abdomen and pelvis
• CT: 100% and 91%, and• IVP: 97% and 74%
This study surpasses the intravenous pyelogram (IVP) which had been the standard imaging test for decades.
A prospective trial of 106 adult patients with acute flank pain imaged all patients with both an unenhanced helical CT and IVP.
The positive and negative predictive values for

Abdominal Plain Photo: Bilateral staghorn calculi

IVU: Left Pelvic stone with hydronephrosis

Ultrasonography CT scan
Stone

Metabolic Stone Evaluation
History and physical examination.
Urinalysis and stone analysis.
Serum CO2, potassium, calcium, magnesium, phosphorus, uric acid, creatinine, PTH.
Two 24 hr. urine collections on a normal diet for: volume, calcium, sodium, potassium, magnesium, phosphorus, citrate, uric acid, oxalate.
Urine pH.
Qualitative urine test for cystine.

Classification of Hyperoxaluria
Metabolic overproduction of oxalate.
• Hereditary• Ethylene glycol, methoxyflurane anaesthesia.
Gastrointestinal overabsorption of oxalate.
• Oxalate overingestion.• Fat malabsorption.

Uric Acid Stones
Defect in uric acid stone formers is an excessively acid urine.
Usually are not hyperuricosuric.
Treatment is urinary alkalinization.
Allopurinol only when very hyperuricosuric.

Calcium Infection Urate
Etio Oxalate ↑ Urea-splitter bacteri Urate ↑
Urine pH ↑ ↓
Ro (opacity) ↑↑ ↑ Non opaque
Medical treatment Oxalate ↓ AB, urine
acidificationPurine ↓, urine alkalinization

Dietary Characteristics of Patients with Renal Stones
Urine volume - patients with renal stones have lower fluid intakes. Dietary sodium is higher; dietary potassium is lower.
Dietary calcium - lower in patients with kidney stones.
Vitamin B6 (40 mg/day) confers RR for stones of 0.66 (0.44-0.98).
Vitamin C does not appear to confer an increased risk for kidney stones.
Dietary phytate appears to decrease risk of kidney stones (Curhan, 2004)

Urolithiasis: Dietary Factors “The Busch Bonus”
Beer drinking results in a 53%
reduction in risk for urinary calculi
(*N.B.: unrelated to amount consumed!)
Kueger, JN et al: AJKD 28:195, 1996

Urolithiasis
Prevention
Treatment

INDICATIONS FOR URGENT INTERVENTION WITH URINARY STONES
Obstructed upper tract with infection
Impending renal deterioration
pain refractory to analgesics Intractable nausea/vomiting
Patient preference

Expectant management
When urgent intervention is unnecessary, and the patients may be followed expectantly in anticipation of passing their stone spontaneously
The stone size and location are key determinants to predict spontaneous stone passage.
The majority of stones < 5 mm in diameter are likely to pass spontaneously and the likelihood of spontaneous stone passage decreases as stone size increases

Spontaneous stone passage within the distal ureter may be facilitated with drugs that enhance expulsion. Such medical expulsion therapy (MET) includes alpha-blockers and calcium channel blockers, typically used in combination with NSAIDs.

Medical TreatmentsDietary modification.
Thiazides for hypercalciuria.
Potassium citrate for hypocitraturia.
Allopurinol for hyperuricosuria.
Magnesium for hypomagnesuria.
Tiopronin for cystinuria.
Pyridoxine for primary hyperoxaluria.

Dietary Modification
Increasing urine volume decreases the incidence of kidney stones (intake ~ 80 oz./day).
Normal calcium (30 mmol/day); low animal protein (52 g/day); low salt diet (50 mmol/day).
We tend to restrict dietary oxalate in hyperoxaluric patients.

Citrate Therapy for Hypocitraturia
Reduces calcium oxalate aggregation.
Several studies document effectiveness in preventing stone recurrences.
Given as potassium citrate.
Citrate is form of alkali and when given as potassium citrate can decrease urinary calcium.

Invasive and minimally invasive management

Treatment: ESWL

Treatment: Lithotripsy

URS: Ureterorenoscopy

Treatment: PCNL

Stone Fragments

Treatment: open surgery

Recurrency
About 10% of people will experience Urolithiasis in their lifetime, and about 70% of those will have recurrences.
The interval between recurrences ± 10% within one year,± 35% in five years, and± 50% by 10 years

Preventing Recurrent Stones
Stone form when the urine is supersaturated
The aim of medical management of stone disease is to decrease the supersaturation of the crystal components in urine.
Urine concentration of stone-forming salts is strongly affected by daily urine volume, so increasing daily fluid intake is important in preventing recurrent stone disease

Increased fluid consumption
Reduction in the five year recurrence rates
The simplest and most difficult intervention to implement is to encourage greater fluid intake.
It is easy to advise patients to drink more, but it is often difficult to achieve the target of drinking sufficient to produce at least 2 litres of urine daily
This is further complicated by the effects of heavy exercise, hot weather, and long distance travel.
The recommendation should be to have colourles urine because yellow or brown urine is too concentrated.

Calcium diet???
Reduce/avoid dairy produce consumption??
Calcium binds oxalate in the gut, preventing its absorption.
A reduction in dietary calcium can cause hyperoxaluria, with resultant increased stone formation.
Observational studies have suggested that calcium restriction may increase stone formation and that calcium supplementation may be beneficial

SUMMARY
Urinary calculi typically present with renal colic and hematuria.
The unenhanced CT is the best initial diagnostic test.
Clinicians should assess the need for urgent intervention and the likelihood for spontaneous stone passage.
Urologic intervention must be individualized.
Metabolic risk of stone recurrences should be addressed in repeat stone formers, and in some first-time stone formers.

“I will not cut persons labouring under the stone, but will leave this to be done by men who are practitioners of this work.”
Hippocrates