Embed Size (px)
Citation preview
MLP ORIENTATION
WORKSHOP 1
Objectives
• Orientation overview• Department orientation• Work flow• RACE team• RME• Fast Track• Physician consults• Charting and documentation
Orientation Overview
• Business Office orientation• Hospital Orientation • New Employee Orientation (guideline)• Epic MHS training + provider oreintation• Workshop 1• Workshop 2• Shadow + Mentorship shifts
New Employee Orientation
Workflow
• Sign into Epic• ASCOM phone• Huddle with charge RN and attendings• Objectives shift specific / location specific
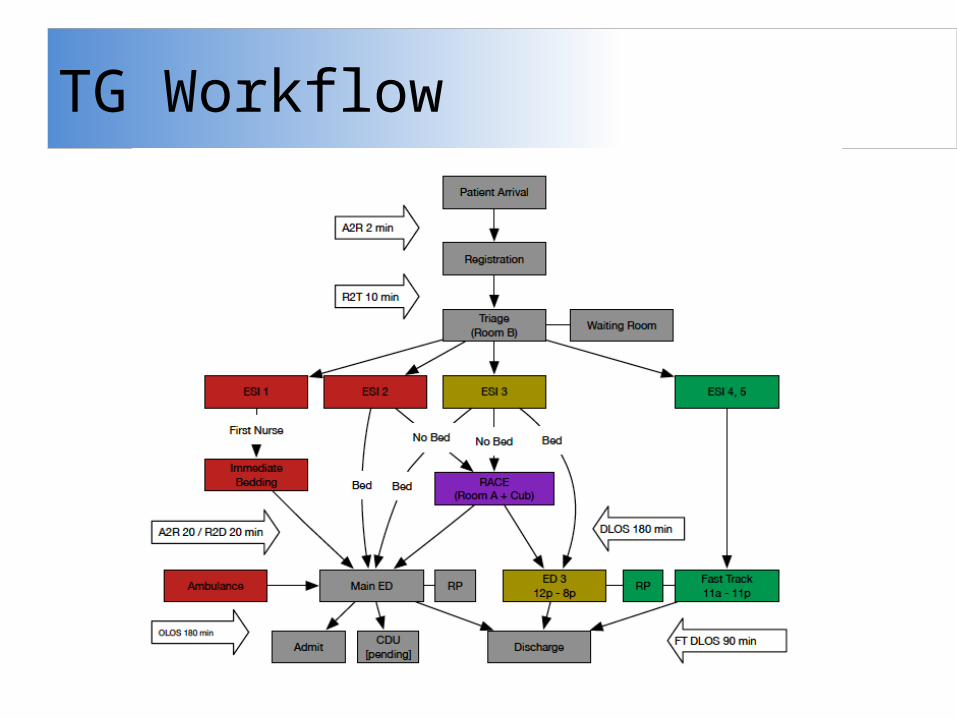
TG Workflow
Tacoma General 10-8p
• 1000 – 2000• ESI 4 and 5 patients in Fast Track
– Signs up as attending • Waiting room RME of patients
– Signs up as attending then “end assignment” in Treatment Team tab– Turns patient RME status on track board
• Physician extension tasks – Laceration repair– Procedures– Consultation– Dispositions– Re-assessments
Tacoma General 2p-12a• 1400 – 0000 (Huddle) • RME WTBS patients in main ED (sickest first) if unable to be seen
by physician – Signs up as attending, gets taken over by attending
• RACE Team– Signs up as attending then “end assignment” in Treatment Team tab– Turns patient RME status on track board– ESI 2, then 3 by LOS– If all 2 and 3 done, treat and street ESI 5
• Assist with Fast Track ESI 4 and 5 patients • Co-management of patients with physician in main ED • MLP signs up as PA or ARNP in MLP column
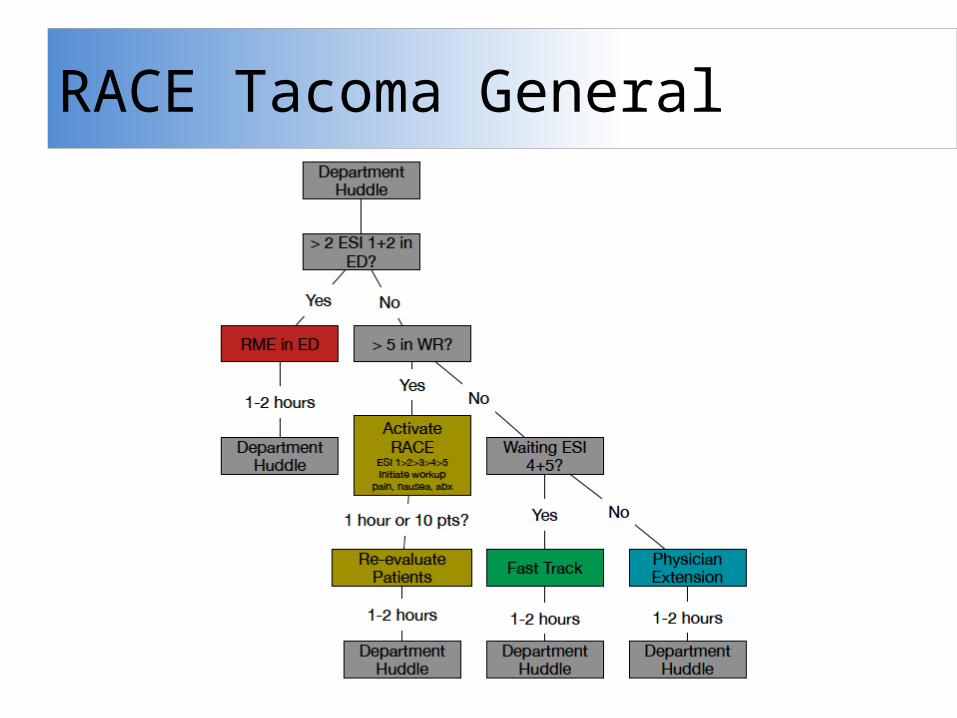
RACE Tacoma General
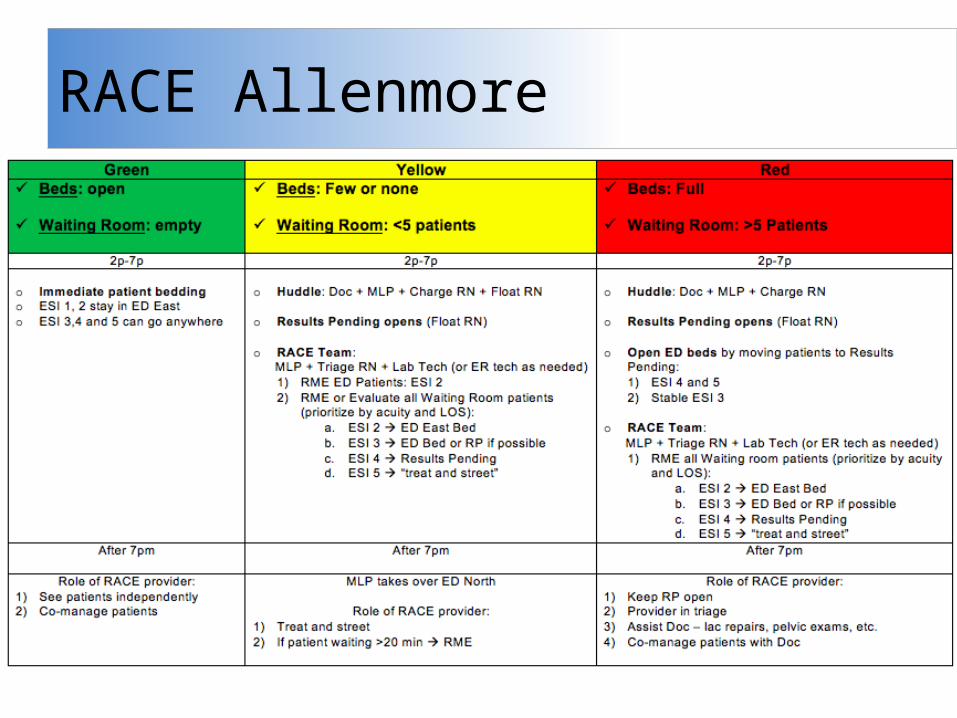
RACE Allenmore
RACE Covington
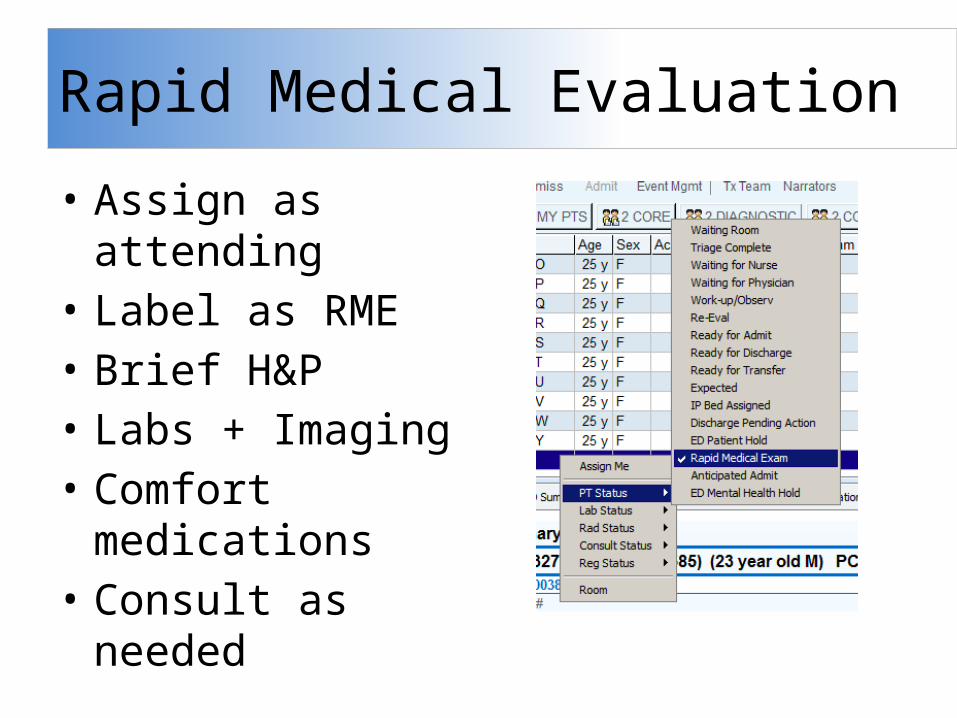
Rapid Medical Evaluation
• Assign as attending• Label as RME• Brief H&P• Labs + Imaging• Comfort
medications• Consult as needed
Fast Track
• Verb… not noun• Goal evaluation <80 min• ESI 4 + 5• Seen independently, consult prn • RN + tech• Focus on oral medications and limited
workups
Co-manage patients
• Initially assigns as attending• Perform H&P• Initiate labs + imaging• Consult attending early• Change assignment to PA
or ARNP once consulted• Re-consult after workup
complete to discuss management
Mandatory Consultation
• ESI 1 or 2• Unstable VS – HR >110 or <50– SBP <100 or >220/120– RR >24 or <8– Pulse ox <95% (unless baseline)– Abdominal pain >50 yrs old– Altered mental status
• Active / uncontrolled bleeding• Anaphylaxis• Chest pain >35 yrs old• CVA / TIA• Joint dislocation (other than digits)• Falls associated with near syncope / syncope• Open fractures
Mandatory Consultation
• Pregnancy with abdominal pain or bleeding• Post surgical complications• Procedural sedation• SOB with abnormal vital signs• Telemetry indicated• Unexpected (non-follow up) return visit• Pediatrics <12 mo, or <3 yr with fever
Mandatory Consultation

Consultation
• Start with reason for consult: run it by you, ED consult, asking for admit.
• ED presentations: ok to not be sure• Concise presentations• Other consultants: specific questions.• Know what you want
Consult case 1
• 22yo M c/o abdominal pain. Constant, began 4 hours ago, radiates to R testicle.
• No PMH/PSH/meds/allergies• VS 140/92, HR 115, RR 30, T 37• Exam: R testicle swollen and painful.• Labs: normal. US no flow to R testicle
Consult case 1
Dx:• HPI:• Plan for care?• Reason for consult?• Present to the ED attending• Present to consultant.
Consultation case 2
• 51 yo man c/o left lower leg pain and swelling for 4 days.
• PMH: DM, HTN• PSH: none• Meds: insulin, lisinopril• VS: 130/80, HR 130, RR 22, T 38.2• Left leg swollen, red, hot to touch. • WBC 20, lactate 4, glucose 600, AG 30, Co2 10
Consult case 2
DX:• HPI:• Plan for care?• Reason for consult?• Present to the ED attending• Present to Consultant. Recommends discharge
after insulin bolus and single dose of IV antibiotics.
Consult case 3
• 25yoF presents to c/o back and leg pain that began several hours after an intense crossfit workout.
• No PMH/PSH/meds/allergies• HR 90, BP 120/80, RR 18, T 37• Exam: uncomfortable. Moderate paraspinous
tenderness. Neuro exam normal.• Labs: CBC/CMP normal. UA +heme, no RBC, CK
4,000
Consult case 3
DDX:• HPI:• Plan for care?• Reason for consult?• Present to the ED attending
Consult case 4
• 45F HA x3 days. Sudden onset 12 hours ago. +vomiting and photophobia. Worst HA of life
• PMH: migraines• VS: 192/120, HR 88, RR 20, T 37• Exam: uncomfortable, otherwise normal• CT head: negative• LP: +xantochromia, + 100,000 RBC
Consult case 4
Dx:• HPI:• Plan for care?• Reason for consult?• Present to the ED attending• Present to consultant.
Specialist Consult
• Consult ED attending first• Medicine– More detailed information– Tell the story of the patient’s problem– Review recent admissions, clinic visits, imaging
• Surgery– Ask your question first– Brief presentations– Review prior surgeries, admissions– Cedar group is different than ACSS
Charting and Documentation
• Chart at appropriate level (3 – critical care)• Don’t forget PMH, PSH, FH, Soc, etc…• HPI: OPQRST• MDM– Initial impression, DDx– Workup and impression of objective data– How this supports / refuts your DDx– reassessment– Final impression and treatment plan
Resources
• PSR website– EGO charting tips and tricks– Pdf of previous education lectures
• Textbook– An Introduction to Clinical Emergency Medicine
• Education Website– Tecpedu.net
• Fundamentals of Emergency Medicine• Resident Page• Procedures• CME• Blog
From Here
• Workshop 2– Procedural
• Select evaluation dates– 30 day, 90 day
• Reach out to mentors / sponsors – Set date and agenda
• Review onboarding materials
Questions
• Epic questions– Dot phrases– Preferences– Macros
• Workflow





























