Embed Size (px)
Citation preview

Future Generation Computer Systems 43–44 (2015) 87–98
Contents lists available at ScienceDirect
Future Generation Computer Systems
journal homepage: www.elsevier.com/locate/fgcs
Mobile cloud-based depression diagnosis using an ontology and aBayesian networkYue-Shan Chang a,∗, Chih-Tien Fan b, Win-Tsung Lo c, Wan-Chun Hung a,Shyan-Ming Yuan b
a Department of Computer Science and Information Engineering, National Taipei University, New Taipei City, Taiwanb Department of Computer Science, National Chiao Tung University, Hsinchu, Taiwanc Department of Computer Science, Tung Hai University, Taichung City, Taiwan
h i g h l i g h t s
• Integrating Ontology with Bayesian Network to predict getting depressed or not.• Using mobile agent and cloud environment to implement the diagnosis environment.• Evaluation result shown the system is feasibility for doing the prediction.
a r t i c l e i n f o
Article history:Received 1 January 2014Received in revised form3 April 2014Accepted 19 May 2014Available online 12 August 2014
Keywords:Bayesian networkDepression diagnosisMobile and ubiquitous healthcareMobile cloudOntology application
a b s t r a c t
Recently, depression has becomes a widespread disease throughout the world. However, most peopleare not aware of the possibility of becoming depressed during their daily lives. Therefore, obtaining anaccurate diagnosis of depression is an important issue in healthcare. In this study, we built an inferencemodel based on an ontology and a Bayesian network to infer the possibility of becoming depressed, andwe implemented a prototype using a mobile agent platform as a proof-of-concept in the mobile cloud.We developed an ontology model based on the terminology used to describe depression and we utilizeda Bayesian network to infer the probability of becoming depressed. We also implemented the systemusing multi-agents to run on the Android platform, thereby demonstrating the feasibility of this method,and we addressed various implementation issues. The results showed that our method may be useful forinferring a diagnosis of depression.
© 2014 Elsevier B.V. All rights reserved.
1. Introduction
Depression (or major depressive disorder) is a common illness.According to theWorld Health Organization (WHO), over 350 mil-lion people of all ages suffer from depression around the world[1,2]. In the worst case, a depressed patient will commit suicide[1,2]. To diagnose depression, various questionnaires can be ob-tained from experts or the Internet, and patient evaluations canbe made after completing the form. These questionnaires usuallyanalyze the severity of the symptoms experienced by a patientduring the past week and the scaled scores are summed to deter-mine whether the patient is becoming depressed. A disadvantage
∗ Corresponding author. Tel.: +886 2 86741111.E-mail addresses: [email protected], [email protected] (Y.-S. Chang),
[email protected] (C.-T. Fan), [email protected] (W.-T. Lo),[email protected] (S.-M. Yuan).
http://dx.doi.org/10.1016/j.future.2014.05.0040167-739X/© 2014 Elsevier B.V. All rights reserved.
of these questionnaires is that patients cannot obtain their resultsinstantly tomonitor their status. In addition, the questionnaires aredesigned in a static format, thus it is not easy to add new symp-toms related to depression. Furthermore, it is difficult to evaluatewhether a person is becoming depressed or not. Many studies haveevaluated the diagnosis of depression in the past decade [3,4].
E-health (electronic healthcare) was first proposed in 1999 [5]and it is a general model that facilitates the provision of healthinformation, products, and services, which can be delivered viatelecommunications. The concept of e-health [5–9] has been de-veloped and applied inmany practical areas. A common solution isto employ sensors with telecommunication capacities, which con-stantly transmit data observations to a database. Suitable medi-cal experts can check the patient’s data instantly, or they can benotified if a patient exhibits critical signs. However, the mood ofa patient is difficult to collect using a sensing device. Thus, somechanges must be made to the traditional e-health concept to al-low the mood states of patients to be recorded anywhere at any

88 Y.-S. Chang et al. / Future Generation Computer Systems 43–44 (2015) 87–98
time. Recently, improvements in sensor andmobile technology,m-health [6,7], and u-health [8] have been proposed, which provide amore convenient way to deliver health information to patients viaa mobile device that can be browsed instantly on mobile devices.
The cloud environment [10] provides a highly stable and less ex-pensive service, thus increasing numbers of applications are beingbuilt in the cloud [11,12]. The advances in wireless communica-tions mean that not all data need to be stored locally [13] and vari-ous data can be obtained via the cloud environment. The cloud alsoprovides computing resources that allow users to execute theirown programs. Thus, services can be built and provided to con-sumers and scientists by exploiting the resources provided by thecloud [14–20]. In addition, as described by Foster [21], the grid pro-vides power to solve deterministic problems and agents providethe brain to solve problems in flexible, uncertain, and dynamic en-vironments.
Therefore, the e-health cloud [9] offers the possibility of easyand ubiquitous access to medical data. A general solution to de-pression diagnosis is to ask patients to complete questionnairesthat ask them about their recent physical and mental state. How-ever, it is difficult to apply depression diagnosis via e-health be-cause asking a patient to complete questionnaires on a frequentbasis is not convenient, and the results cannot be sent to a databaseand checked immediately by medical experts. Thus, it is not pos-sible to notify relevant experts on the fly to give help to a patientwho is becoming depressed.
Due to the continuing advance of information technology, in-creasing numbers of studies are utilizing information technol-ogy for the automatic inference of the status of patients and toobtain results [22]. In various research areas, ontology [23] is animportant technique for representing the terminology used in cer-tain domains. Information technology can process the user’s in-put automatically, and then infer the results according to the inputbased on an ontology and related rules. However, this approach canonly infer certainties and it cannot infer various possibilities ac-curately for the uncertainties that are inevitable features of mostenvironments. A Bayesian network (BN) is a probabilistic graph-ical model that represents the conditional dependencies of eachnode as a directed acyclic graph (DAG). Each node in the DAG has arandom probability, where every directed edge represents the de-pendency between nodes. BNs have been applied to risk analysisin some medical areas [24–26,14].
Merging an ontology with a BN to infer uncertainty is a popularapproach in various domains [27–30]. Ontologies can specify ashared conceptualization in a formal and explicitmanner. They canprovide excellent representations of the organizational structureof large complex domains, where Bayesian probability allows theassignment of probabilities to other types of statement. Thesetechniques have also been applied widely in expert medicalsystems [24,31,25,26] in recent years. However, they have neverbeen applied to the diagnosis of depression.
In this study,we developed amobile cloud-based depression di-agnosis framework, which we implemented to run on amobile de-vice. This framework uses an ontology to define the terminology ofdepression and a BN is employed to infer the probability of becom-ing depressed. First, we built a depression ontology using Protégé,1which is a free and open source ontology editor that allows the ex-plicit representation of the relationships of the symptoms of de-pression, and it uses the Graphical Network Interface (GeNIe) andStructural Modeling, Inference, and Learning Engine (SMILE)2 as a
1 The Protégé Ontology Editor and Knowledge Acquisition System, seehttp://protege.stanford.edu/.2 GeNIe and SMILE were developed by the Decision Systems Laboratory,
University of Pittsburgh, and they are available at http://genie.sis.pitt.edu/.
BN inference engine. Both run in the backend cloud environment.In addition, at the front end of the mobile cloud, a mobile agentplatform is deployed on the patient’s mobile device to collect andtransmit health information to the backend cloud platform. Userscan input their personal feelings into the mobile device. The useragent then sends these inputs to the backend cloud environmentto infer the possibility of becoming depressed. A prototype of thisframeworkwas also implemented to demonstrate the feasibility ofthe proposedmethod. Our results indicate that this method can bean effective and efficient tool for inferring the diagnosis of depres-sion.
This study makes three major contributions compared withprevious methods.
• A mobile cloud-based depression diagnosis framework wasdeveloped to evaluatewhether a person is becoming depressed.
• No previousmethods have used an ontology and a BN for the di-agnosis of depression. Thus, we constructed a depression ontol-ogy model (DOM), which we integrated with the BN techniqueto build a model to infer the possibility of becoming depressed.
• We used mobile agent technology to implement a readily ac-cessible interface on a mobile device to evaluate the likelihoodof becoming depressed anytime and anywhere.
The remainder of this paper is organized as follows. In Section 2,weprovide some background knowledge and discuss related research.Section 3 mainly describes the construction of the proposed DOMusing Web Ontology Language-Description Logics (OWL-DL). Sec-tion 4 shows how the probability of becoming depressed is inferredusing the BN technique. Section 5 addresses the implementationissues encountered when utilizing the techniques. Finally, we pro-vide our concluding remarks and suggest future work in Section 6.
2. Background and related work
In this section, we discuss the background of this study and re-lated research. In Section 2.1, we present a preliminary descriptionof the ontology and the BN. A definition of mobile and ubiquitoushealthcare is provided in Section 2.2. Finally, previous research re-lated to our proposed approach is discussed in Section 2.3.
2.1. Preliminaries
The concept of an ontology [32,33] is derived from philoso-phy. In computer science, an ontology is a formal representationof knowledge as a set of concepts within a domain, and the re-lationships between pairs of concepts. Ontologies are one of themost widely used approaches for enabling system intelligence andfor improving the capacity to automate a system by obtaining thesystem’s semantics [34–37]. An ontologymay take a various forms,but itmust include a vocabulary of terms and specifications of theirmeaning. In general, an ontology is the manifestation of a sharedunderstanding of a domain, which has been agreed by a numbersof parties.
Different ontology languages have various specific characteris-tics. The most recent development in standard ontology languagesis OWL,3 which is endorsed by the World Wide Web consortium(W3C) to promote the Semantic Web Vision. OWL provides a lan-guage with a rich vocabulary for describing properties and classes,including the relations between classes, cardinality, equality, richtyping of properties, the characteristics of properties, and enumer-ated classes. An OWL ontology comprises Individuals, Properties,
3 http://www.w3.org/TR/2004/REC-owl-features-20040210/.

Y.-S. Chang et al. / Future Generation Computer Systems 43–44 (2015) 87–98 89
and Classes. Individuals indicate the object of a specific field. Proper-ties represent the relationships between two individuals. There aretwo properties: an Object property and a Datatype property. TheObject property connects two individuals and the Datatype prop-erty connects one individual to an XML schema Datatype value or aresource description framework (RDF) literal, which is a label lan-guage proposed by W3C. Classes are interpreted as containing acollection of many individuals.
An ontology defines the conceptual model of knowledge, thusa BN can provide a probabilistic graphical model (a type ofstatistical model) that represents a set of random variables andtheir conditional dependencies via aDAG [38]. The basic element ofthe Bayesian probability is a random variable, which is consideredto refer to an event in an initially unknown environment [27].
In the BN, each node represents a random variable in theBayesian sense, which may be observable quantities, latentvariables, unknown parameters, or hypotheses. Edges representconditional dependencies, where unconnected nodes representvariables that are conditionally independent of each other. Eachnode is associated with a probability function, the input of whichis a particular set of values for the node’s parent variables andthe output is the probability of the variable represented bythe node. The conditional dependencies in the graph are oftenestimated using known statistical and computationalmethods. Fordiscrete random variables, the conditional probabilities are oftenrepresented by a table, which lists the local probability that a childnode takes each of the feasible values for each combination of thevalues of its parents. The unique joint distribution of a collectionof variables can be determined using these local conditionalprobability tables (CPTs). The joint probability is defined as theprobability that a series of events will happen concurrently. Thejoint probability of several variables can be calculated from theproduct of the individual probabilities of the nodes, according toformula (1). A more formal definition of a BN is given in [39].
P(X1, . . . , Xn) =
ni=1
P(Xi|parent(Xi)). (1)
An ontology allows the representation of background knowl-edge about a domain in amachine understandable form,while a BNis a probabilistic model that represents uncertainty. Several stud-ies have shown that it is possible to combine these two models toprovide richer knowledge [27–30,24,40].
In [28], a method was proposed for the ontology-basedgeneration of a BN. This ontologywasused to provide the necessaryknowledge related to the nodes of the BN, including various factors,relationships, weights, and the scale, which represented thepotential states of identified influential factors. A security ontologywas used to demonstrate the feasibility of the proposed method.
An ontology-driven uncertainty model called OntoBayes wasproposed in [27], where a probability-annotated OWL was pro-posed to represent probabilities in the ontology. The OWL classesof PriorProb, CondProb, and FullProbDist were defined to specifythe prior probability. The OWL properties of hasPrior and hasCondwere also defined to describe the properties of an OWL object.Dependency-annotated OWL was also introduced to specify thedependency relations.
Gu et al. [40] also proposed an approach for handling uncertaincontexts, where an ontology markup language was introduced asa probabilistic extension to OWL. This markup language allowedthe context to be translated into a DAG, where the correspondingrandom variable was present on each node. Using the DAG, theuncertainty of the context could be evaluated with a BN.
2.2. Mobile and ubiquitous healthcare
Mobile cloud computing [41–43] was introduced after theconcept of ‘‘cloud computing’’ was proposed. In general, it refersto the operation of a resource-rich server on a remote cloud site,while a mobile device has client applications that allow contentsto be obtained from the server via telecommunications (e.g., fordisplay on a screen). Mobile cloud computing can be defined asfollows. (1) A remote cloud server provides a service to mobiledevices via the internet. (2) A virtual resource cloud is formed bythe mobile devices in the vicinity. (3) A cloudlet allows mobiledevices to bypass latency and bandwidth issues, while benefittingfrom its resources. A more detailed definition can found in [41]. Inall cases, the architecture usually comprises the cloud architecture,the end user device, and the telecommunications infrastructure.Our system conforms to the second definition.
Mobile computing has also been applied successfully to varioushealthcare applications [8,44–46]. In [8], a mobile u-health (ubiq-uitous e-health) service system was introduced called THE-MUSS.The authors focused on the usability of the system, where the testscenario was divided into five components: data acquisition, datastorage, data analysis, decision and delivery, and user feedback. Al-though this technique is not used in the present study, we employa similar architecture. In addition, healthcare technology based onagents has been used for many years. For example, a multime-dia healthcare system (MHS) was presented in [46], which facili-tated continuous medication monitoring, context-aware prompt-ing, adaptivemultimedia presentation, and flexiblemedicineman-agement. Older patients could use MHS to view their medicationplan and diary. They could also obtain advice from the MHS advi-sory service based on their medication plan and diary.
Mobile devices are often used to help collect data from patients.In [44], the authors proposed a networked multi-agent architec-ture for monitoring human health conditions based on emergingwireless mobile technologies. The patient’s agent collected theirbodily signs and uploaded them to a static server, while otheragents, including those related to doctors or paramedics, could ac-cess them constantly or notifications were received in certain situ-ations. In [45], the authors used mobile devices to recognize theactivities of users, where a hierarchical recognition scheme wasproposed to reduce the energy consumption ofmobile devices. Thisscheme facilitated the accurate recognition of activities by mobiledevices, even at a low sampling frequency.
2.3. Ontology and BN applications for diagnosis
Several previous studies [24,31,25,26] employed methods sim-ilar to that proposed in the present study. In [24], the authors pro-posed an approach that employed an ontology and a BN inmedicaldiagnosis. Two levels of the ontology were defined: the ‘‘Knowl-edge’’ level represented the specialist’s medical knowledge; andthe ‘‘Operational’’ level helped the physician to collect useful datawith the support of the Knowledge level, thereby formulating theirpersonal diagnosis. A two-level BN and a predefined structure fordecisionnetworkswere used to perform theBayesian analysis. Thisscheme allowed only limited extension into the domain ontology,but it facilitated probabilistic analysis. The algorithmestimated theprobability that a patient was affected by a given pathology and itwas also capable of suggesting possible additional tests, as well ascomputing their usefulness.
In [31], the authors proposed an ontology-enhanced ubiqui-tous monitoring and treatment model to help people overcomethe challenges of mental disorders. The authors proposed a con-text ontology for mental disorders, which was based on semantic-enhanced methods developed for collecting, formalizing, and ma-nipulating patient data. The proposed framework was imple-mented to facilitate online cognitive behavioral therapy to treat de-pression in the current stage,which combined talk/chat/messaging

90 Y.-S. Chang et al. / Future Generation Computer Systems 43–44 (2015) 87–98
Table 1Comparison of the proposed method and previous studies.
Our proposed method Bucci et al. [24] Hu et al. [31] Arsene et al. [25] Zheng et al. [26]
Diseaseconsidered
Depression Flu Mental disorder Heart disease Not specified (Clinical Practice Guidelines)
Platform Mobile cloud, JADE +
AndroidNot specified Mobile device (not
specified)Personal computer Not specified
Diagnosismethod
Ontology and Bayesiannetwork
Ontology and Bayesiannetwork
Multi-layeredontology
Ontology and Bayesiannetwork
CPG ontology and Bayesian network
Userinterface
Rich interface onmobile device
Not specified Rich interface onmobile device
Personal computer Not specified
services, help to retrieve neurofeedback, and support for collabo-rative diagnosis when necessary.
In [25], the authors proposed a general model for an applica-tion framework called the Dynamic Bayesian Network Ontology(DBNO), which was designed to obtain a medical-assisted diagno-sis based on an ontology and a BN. In the proposed scheme, theknowledge domain was separated from probabilistic information,which made the proposed framework more flexible. The domainknowledge and probabilities were provided by medical experts,and they were ready for use as a medical ontology and an uncer-tainty profile, respectively. The diagnostician employed the userinterface to access the ontology domain and an uncertainty pro-file. The application was tested on a sample medical model for thediagnosis of heart disease.
An ontology-based representation of uncertainty in clinicalpractice guidelines (CPGs) was proposed in [26], where the ontol-ogy model was built as an activity graph based on the guidelinesspecified in the CPGs. The activity graph contained three types ofactivity: context activity, decision activity, and action activity. Toalleviate restrictions on the internal conditions of an activity, a BNwas used to obtain the uncertainty features of conditions. The ef-fect on the overall clinical process could be evaluated when an ac-tivity occurred. The evaluation results could help doctors to assessthe risk of uncertainty for other activities and to make decisions.A variable elimination algorithm was used to infer the BN and avalidation scenario was presented based on aspirin therapy for di-abetic patients.
Table 1 compares our proposed method and previous re-search [24,31,25,26]. Themethod reported by Hu et al. [31] is mostsimilar to that proposed in the current study because both employa user interface (UI) on a mobile device. However, Hu et al. onlyused an ontology to infer whether someone had a mental disor-der or not, and a BNwas not employed to obtain the probability. Inaddition, Hu et al. focused on the development of an e-health envi-ronment that allowed patients to obtain help directly frommedicalexperts via their mobile phones. However, the system did not ex-ploit an inferencemodel and the actions could only be activated byhumans.
Other studies have focused on the diagnosis of differentdiseases. However, most of these studies only provided a modeland UIs were not developed to allow patients to access their data,except for [31,25]. Thus, these studies focused only on how toobtain the probabilities of patients having certain diseases. Bycontrast, in our study, we developed a readily accessible UI forpatients to use on a handy mobile device, but we also exploitedthe mobile cloud andmobile agents to facilitate the deployment ofan e-health system in a cloud environment.
3. Building the DOM
In general, an ontology is used to represent knowledge in aspecific domain. In this study, we employed OWL-DL to constructan ontology model for depression, because it supports users whorequire maximum expressiveness without losing computational
Fig. 1. Basic ontology model for depression.
Fig. 2. Relationship between two individuals.
completeness to build a DOM for their framework. We utilizedProtégé to construct the DOM and to edit the ontology model,which is a free and open source ontology editor and knowledgebase framework. In addition, the rules used for inferring ontologieswere constructed with the GeNNe & SMILE reasoning engine,which is a Semantic Web framework for Java that supportsemantics for defining rules. In general, the ontology does notinclude any probabilities in the node. The ontology model isintroduced in Section 3.1. The definitions and properties thatconnect the class and instances used in theDOMare also presented.The DOM inference rules are described in Section 3.2. The DOMenhanced with a BN is explained in Section 4.
3.1. Ontology model
Fig. 1 shows the DOM, where Thing class is a system class,which is defined as the root of the ontology. The DOM canbe classified into three main classes: Patient, Disease, andDepression. The Patient class is used to represent a patientinstance, which can store the patient’s symptoms and othermedical history. The Disease class represents the super-classof all diseases, i.e., all diseases are its sub-classes. There is onlyone disease class in our DOM: the Depression class. The thirdclass is the Depression_Symptom, which is the super-class thatcontains all the symptoms of depression.
There are also several instances in the proposed DOM, wheresome instances can only be used by specific classes. An exampleis shown in Fig. 2, where the instance (or the individual inProtégé) Fatigue is the subclass Dysthymia_Symptom, whichis shown as a solid line ‘‘is_a’’. By contrast, the sub-classof Dysthymia_Symptom has an individual Fatigue, which isshown by the dashed line ‘‘has_individual’’ in the figure.
Fig. 3 shows all the symptoms in our DOM, which demon-strates that there are many types of depressions. For example,

Y.-S. Chang et al. / Future Generation Computer Systems 43–44 (2015) 87–98 91
Fig. 3. Extended depression ontology model.
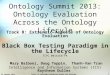
Fig. 4. One of the rules used to infer Dysthymia in the depression ontology model. The first line shows the rule’s name: Dysthymia. Lines 2–7 show the conditions ofthe dysthymia rule, while the last line shows the outcome applied to the inference system if all the conditions are true. In this example, the rule can be represented as: ifa patient has the symptoms of sadness, fatigue, sleep disturbance, eating disturbance, low self-esteem, and anxiety, the patient may have dysthymia. This rule is written inthe Apache Jena reasoner’s simplified text rule syntax.4
Dysthymia is one of the types of depression that is relatedmainly to the mood of the patient, thus if a patient has the dis-ease dysthymia, he must also have the disease depression. There-fore, as shown in Fig. 3, the instance Dysthymia is a sub-class ofDepression, while the classDysthymia_Symptom is a sub-classof Depression_Symptom. In Protégé, an ontology can also be ex-tended to show that it contains more subclasses. For example, thesymptoms of depression may include Suicide, Frustrated, and LowSelf-esteem, as shown in Fig. 3.
3.2. Inference rules
An ontology is used to formalize a specific concept, where eachnode represents an individual. In order to deduce the relationshipsbetween individuals, we need to define inference rules, which canbe executed by the SMILE inference engine. Therefore, we con-structed inference rules to infer the desired information. To explainthe inference rules, we utilize a simple example to demonstratepartial inference rules, as shown in Fig. 4.
The inference rule can deduce the relationships between everyindividual. An inference rule is definedwith three tuples: the nameof the rule, the conditions, and the outcomes. As shown in Fig. 4, arule called Dysthymia is defined in the DOM. The rule indicatesthat if a patient has the symptoms of ‘‘Sadness’’, ‘‘Fatigue’’, etc., thenthe outcome for the patient may be ‘‘Dysthymia’’. The inferencerules can be updated by medical experts at any time, thereby en-suring that advanced research results are used to diagnose the pa-tient. It is obvious that the inference rule cannot obtain the proba-bility ofDysthymia occurring as an outcome andwe only know thatthere is a possibility of the disease. Therefore, the BN technique canbe used to calculate the probability of having the disease.
3.3. Representation of a patient’s ontology
In addition, as mentioned above, the ontology model includes aPatient class for recording the patient’s symptomwhile the patientuses the system. For example, a patient A utilizes the ontologyand inference rules are used to infer the possible disease. Thesystem then constructs the user’s symptoms for Patient_A in theontology model, as shown in Fig. 5. The patient has the symptomsof Fatigue, Low Self-esteem, and Anxiety. These patientdisease ontology features can be stored in the backend cloud.In the ontology model, the accumulated user symptoms can beused to adjust the inference rule progressively in the future. Thecorresponding ontology graph is shown in Fig. 6.
4. Probability inference using a BN
In the previous section, we defined the DOM with inferencerules. An example of Patient_A’s ontology was also presented.However, the DOM cannot represent the probability of an instance.For example, when Patient_A’s ontology shown in Fig. 5 wasreasoned using the Dysthymia rule defined in Fig. 4, the resultonly showed that Patient_A did not have Dysthymia, butthere was no indication of the probability of Patient_A havingDysthymia.
Another issue is the unpredictability of the patient. For example,a patient may become ‘‘silent’’ about their feelings at some times,whereas they may have ‘‘an angry spell’’ for just a few minuteson other occasions. Some symptoms occur more frequently than
4 ‘‘Apache Jena – Home,’’ see http://jena.apache.org/.

92 Y.-S. Chang et al. / Future Generation Computer Systems 43–44 (2015) 87–98
Fig. 5. Example of a patient’s disease ontology.
Fig. 6. Patient’s ontology graph.
Fig. 7. Example showing the transformation of an ontology model into a Bayesian network.
others. This information is very useful when medical experts wantto diagnose whether a patient has depression.
In this section, we describe how the BN [40] technique is usedto produce a possibility model in the DOM. OntoBayes, whichwas proposed in [27], is utilized to add this important feature.Section 4.1 describes how the DOM is transformed into a BN. TheCPT of the BN is shown in Section 4.2. Finally, we show how the BNis evaluated in Section 4.3.
4.1. Merging the DOM with the BN
It is necessary to merge the model with the BN to makethe DOM accept probabilities. We used OntoBayes [27] to mergethe DOM with the BN to infer the probabilities of node. Fig. 7shows a simple example of a DOM merged with a BN. For everyindividual in a DOM, a directed edge may connect them. Thedirected edges can be obtained from the properties of classes orthe inference rules. For example, a property shows that SymptomAMay_Cause SymptomB, and the corresponding directed edgeis also shown in BN. For both SymptomA and SymptomBMay_Cause_This_Disease of DiseaseA, the matcheddirected edges are also shown in BN. Because the inference rulescan be updated at any moment, the BN is generated on the fly.
The next integration step involved probabilistic extension toexpress the inference results using a Bayesian probability model.Thus, we also needed an extension of OWL that allowed us tospecify probability-annotated classes or properties. Therefore, thevalue of a probability is inferred by the Bayesian probabilitymodel.
In Fig. 7, we add a probabilistic property to the inference results.The inference process is described in the next section.
4.2. Conditional probability table of the BN
A CPT needs to be defined to utilize the BN. The CPT needs to becorrect to facilitate precise inference of the BN. A possible solutionto this problem is to allow the CPT to be edited by medical expertsbased on their knowledge. This approach appears to be feasible,but the statistics might not be correct due to a lack of sufficienthistorical records for patients or the results may be out-of-date.
All of the patients’ record are stored in the backend clouddatabase, so a possible solution is to periodically run a distributedmining program, such as the Message Passing Interface (MPI)5program or Hadoop MapReduce,6 to calculate each probability.After performing the calculations, the results can be applied to theCPT directly, or sent to medical experts as a reference to makefurther improvements to the system. Finally, all patients can infertheir probability of depression based on the most advanced data.
A simple example of a CPT is shown as Fig. 8, which has threenodes: Sleep_Disturbance, Fatigue, and Dysthymia. ThesymptomofSleep Disturbancemaybe the cause the symptomof Fatigue, while both symptoms may cause Dysthymia. How
5 MPI Documents, see http://www.mpi-forum.org/docs/.6 Welcome to ApacheTMHadoop R⃝!, see http://hadoop.apache.org/.

Y.-S. Chang et al. / Future Generation Computer Systems 43–44 (2015) 87–98 93
Fig. 8. Example of a Bayesian network. The conditional probability tables areshown next to each corresponding node.
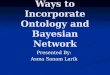
do we infer the probability of a disease occurring? First, we need aCPT to express the local probability that a child node takes each ofthe feasible values for each combination of the values of its parents.Fig. 8 shows an example of the CPT in the BN, where the CPT onthe edges represents the probability of the parent symptom giventhe child symptom. For example, there are three nodes in the BN:Sleep_Disturbance, Fatigue and Dysthymia. Each nodehas a CPT that is dependent on causality. The CPT of Fatiguemeans that when the patient has Sleep_Disturbance, it setsSleep Disturbance as True and there is a 65% possibility ofFatigue. If the patient does not have Sleep_Disturbance, itsets Sleep_Disturbance as False and there is a 15% possibilityof Fatigue.
4.3. Inference of Bayesian probability
In this section, we use the example from Fig. 5, wherePatient_A has three types of symptoms: Fatigue, Low_Self-esteem, and Anxiety. The corresponding BN based on Figs. 4and 5 is shown in Fig. 9. We assume that the patient always hasthese three symptoms, thus the probability (or the frequency) ofFatigue, Low_Self-esteem, and Anxiety are set to 100%true.
For any set of random variables, the probability of any memberof a joint distribution can be calculated from the conditionalprobabilities using the chain rule as follows:
P (X1 = Y1,X2 = Y2, . . . ,Xn = Yn)
=
i6ni=1
PXi = Yi|Xj = Yj, for each Xj which is a parent of Xi
.
(2)
According to the DOM, the symptom Sleep_Disturbance maycause Fatigue. The probability of the patient having Sleep_Disturbance can be evaluated as shown in (3) and (4). Theprobability can be looked up and evaluated using the CPT. Theother two values, Sadness and Eating_Disturbance, can alsobe looked up in the CPT. However, the the latter cannot be evalu-ated based on the information provided by the patients, whereasthe former can be calculated using the CPT to obtainmore accurateresults.
After obtaining all the probabilities that the symptoms maycause dysthymia, the BN can then be used to evaluate theprobability. The final results obtained by the BN are shown in Fig. 9,where the probability of dysthymia is evaluated with (5). Fig. 10
shows the results that are stored based on the original patient’sDOM. These results may be used for further evaluation of otherdiseases or they could checked by the doctor.P(Patient A gets Sleep Disturbance = True)
=P(SDT )P(FT |SDT )
P(SDT )P(FT |SDT ) + P(SDF )P(FT |SDF )
=0.3 ∗ 0.7
0.3 ∗ 0.7 + 0.7 ∗ 0.2= 0.6 (3)
P(Patient A gets Sleep Disturbance = False)
= 1 − P(Patient A gets Sleep Disturbance = True)
= 1 − 0.6 = 0.4 (4)P(Patient A gets Dysthymia = True)
=
s,ed,sd∈{T ,F}
P(DT , AT , FT , LT , Ss, EDed, SDsd)P(Ss)P(EDED)P(SDsd)d,s,ed,sd∈{T ,F}
P(Dd, AT , FT , LT , Ss, EDed, SDsd)P(Ss)P(EDed)P(SDsd)
=
P(DT , AT , FT , LT , ST , EDT , SDT )P(ST )P(EDT )P(SDT )
+ P(DT , AT , FT , LT , ST , EDT , SDF )P(ST )P(EDT )P(SDF )
+ P(DT , AT , FT , LT , ST , EDF , SDT )P(ST )P(EDF )P(SDT )
+ P(DT , AT , FT , LT , ST , EDF , SDF )P(ST )P(EDF )P(SDF )
+ P(DT , AT , FT , LT , SF , EDT , SDT )P(SF )P(EDT )P(SDT )
+ P(DT , AT , FT , LT , SF , EDT , SDF )P(SF )P(EDT )P(SDF )
+ P(DT , AT , FT , LT , SF , EDF , SDT )P(SF )P(EDF )P(SDT )
+ P(DT , AT , FT , LT , SF , EDF , SDF )P(SF )P(EDF )P(SDF )s,ed,sd∈{T ,F}
P(DT , AT , FT , LT , Ss, EDed, SDsd)P(Ss)P(EDed)P(SDsd)
+
s,ed,sd∈{T ,F}
P(DT , AT , FT , LT , Ss, EDed, SDsd)P(Ss)P(EDed)P(SDsd)
=
0.7 ∗ 0.5 ∗ 0.2 ∗ 0.6 + 0.65 ∗ 0.5 ∗ 0.2 ∗ 0.4+ 0.55 ∗ 0.5 ∗ 0.8 ∗ 0.6 + 0.45 ∗ 0.5 ∗ 0.8 ∗ 0.4+ 0.55 ∗ 0.5 ∗ 0.2 ∗ 0.6 + 0.5 ∗ 0.5 ∗ 0.2 ∗ 0.4+ 0.4 ∗ 0.5 ∗ 0.8 ∗ 0.6 + 0.35 ∗ 0.5 ∗ 0.8 ∗ 0.4
s,ed,sd∈{T ,F}
P(Ss)P(EDed)P(SDsd)= 0.477 (5)
whereD denotes Dysthymia,A denotes Anxiety,F denotes Fatigue,L denotes Low Self-esteem,
S denotes Sadness,ED denotes Eating Disturbance,SD denotes Sleep Disturbance.The subscript T denotes that the user has the symptom,whereas F denotes the absence of the symptom.
5. Prototyping and evaluation
In this section, we describe the implementation of the proposedsystem. Thedetailedprototyping of the system, including a brief in-troduction to the tools used, is presented in Section 5.1. After pro-totyping, we performed evaluations, as described in Section 5.2. Fi-nally, comparisons of the proposed system and previous methodsare provided in Section 5.3.
5.1. Prototyping
The DOMwas built with Protégé, which supports developmentin a variety of ontology formats, such as OWL, RDF(S), or XMLschemas. Fig. 3 shows the DOM built with Protégé.
GeNIe and SMILE provide libraries that facilitates the imple-mentation of decision-theoretic models, such as BNs, influence

94 Y.-S. Chang et al. / Future Generation Computer Systems 43–44 (2015) 87–98
Fig. 9. Inference results obtained using the Bayesian network based on the patient’s DOM.
Fig. 10. Encoding frequency and probabilistic properties in the ontology.
diagrams, and structural equation models. SMILE was originallywritten in C++ and it is also available on the Java platform via thejSMILE library. SMILE provides APIs to implement decision-theoreticmodels and GeNIe is a software package that allows usersto create decision theoretic models in an intuitive manner using agraphical click-and-drop interface. An example of the inference re-sults for the DOM and the BN is shown in Fig. 9.
We used a multi-agent system to build the proposed systemin the mobile Cloud. Java Agent Development Framework (JADE)7was used to create the multi-agent environment. JADE can createmulti-agent environments on a Java-installed machine, but it canalso run on Android mobile devices with the support of the JADEAndroid Add-On [47]. Thus, four agents were defined: User Agent(UA), Recording Agent (RA), Ontology Creation Agent (OCA), andInference Agent (IA). A database was also used to store all ofpatients’ records. The architecture of our proposed multi-agentsystem is shown in Fig. 11. Fig. 12 shows the agents running onthe agent platform during prototyping.
UA is installed on the patient’s Android mobile device and it isresponsible for interacting with the patient. During prototyping,the Android 2.3.3 emulator was used for demonstration andto obtain a proof of concept. As shown in Fig. 13(a), UA asksthe patient whether they are having a good day or not. If thepatient feels that the day is not going well, additional informationis requested. Fig. 13(b) shows an example of how UA obtainsadditional information from the patient.
While the UA interacts with the patient, it also transmits thepatient’s information (e.g., symptoms of the patient) to the RA. RAis responsible for updating the patient’s record in the database. Be-cause the RA is separated from theUA, there is no restriction on thedatabase that is used. Thus, different types of RA can be employedto allow the system to support multiple types of database system.
When a patient or doctor requires the probability of depressionin the patient, UA notifies the OCA to create the patient’s personalontology. First, the OCA check whether there are any new patientrecords in the database. If there are new records, a new patientontology is generated. An example of the ontology generated isshown in Fig. 5. The newly generated ontology is then stored inthe database to facilitate rapid access in the future. Next, the OCAsends the patient’s personal ontology to the IA.
After the IA receives the patient’s personal ontology, theinference model is built for the BN, as described in Section 4.The inference model is then fed to the SMILE library to infer the
7 ‘‘Jade—Java Agent DEvelopment Framework’’, see http://jade.tilab.com/.
Fig. 11. Prototyping using a multi-agent system.
Fig. 12. Snapshot of the JADE platform running the prototype. The containersdenoted as green folders act as the agent environment. The Main-Containeracts as the Cloud environment, which comprises the BNAgent, OntoAgent, andManager agent, i.e., the proposed Inference Agent, Ontology Creation Agent, andRecording Agent, respectively. The container BE-192.168.443.124_1099-1 is theagent environment on the patient’s mobile device, where the PatientA agent actsas the User Agent in the proposed system. (For interpretation of the references tocolour in this figure legend, the reader is referred to the web version of this article.)
patient’s probability of depression. The inference result is sent backto the UA and it is displayed on the mobile device, as shown inFig. 13(c).

Y.-S. Chang et al. / Future Generation Computer Systems 43–44 (2015) 87–98 95
Fig. 13. Snapshot of the User Agent using the JADE platform. The User Agent (a) asks whether the patient is having a good day, (b) it then asks how the patient feels today,and (c) the inference results are shown by the inference agent.
5.2. Evaluation
Two evaluations were conducted to evaluate the quality of theproposed system. The first evaluation tested the latency of the sys-tem. The latency was measured the time from the moment theuser’s mood was input via the UA until the response was providedby the UA. In order to eliminate the transmission overheads due tothe communication between agents over the Wide Area Network(WAN), all agentswere implementedon the same computer. Fig. 14shows the latency test results after 100 runs, where 46 inferencerules were used. The average latency was about 50 ms and it didnot exceed 80 ms. The latency increased with the number of infer-ence rules.
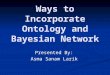
A systematic survey was also conducted to evaluate thesatisfaction of users with the system. In total, 21 interviewees aged20–25 years participated, who comprised females and 15 males.Four types of satisfaction were assessed: Usability, Convenience,Readability, and Accuracy. For each satisfaction question, fiveoptions were available to the interviewees: Excellent, Good,Average, Fair, and Poor. The survey results are shown in Fig. 15.
The first assessment considered the Usability of the system. Asshown in Fig. 15(a), over 60% of the participants considered thatthe system was ‘‘Good’’ for users or patients. In terms of Conve-nience, Fig. 15(b), shows that over 90% of the participants consid-ered that the systemwas ‘‘Good’’. Fig. 15(c) shows that over 85% ofthe participants considered that the system was ‘‘Good’’ in termsof Readability. Finally, over 75% of the participants considered thatthe systemwas ‘‘Good’’ in terms of Accuracy, as shown in Fig. 15(d).
It was notable that the satisfaction in terms of Usability waslower than that for other factors. Some of the intervieweesconsidered that this environment is not necessary to evaluate thelikelihood of becoming depressed. However, we consider that itis useful for people who need to determine whether they areexperiencingmore stress than previously, because daily life is nowincreasingly competitive in various areas at all times.
5.3. Comparison and discussion
In this section, we compared the proposed method with pre-vious approaches, including the well-known Goldberg DepressionQuestionnaire and other research. The Goldberg Depression Ques-tionnaire is a traditional approach that uses questionnaires to helpthe patient determine whether they need to consult a mentalhealth professional for the diagnosis and treatment of depression,or simply for monitoring mood. The questionnaire can be obtained
Fig. 14. Evaluation of the performance of the Inference Agent. The x-axis shows theith inference, while the y-axis indicates the time required to obtain the inference.The Depression Ontology Model had 46 inference rules and the experiment wasconducted 100 times.
online or from medical experts. The disadvantage of the question-naire is that the latest research cannot be integrated immediately.In addition, when a patient is completing the questionnaire, theyare asked to answer each question based on their feelings or be-havior during the past week. Thus, if a patient has amnesia, it isdifficult for them to answer the questions. By contrast, using theproposed method, patients can enter their state anytime and any-where, and the agents can automatically infer the probability ofbecoming depressed based on the patient’s records stored in theCloud. Additional comparisons are shown in Table 2.
6. Conclusions and future work
In this study, we developed a mobile cloud-based depressiondiagnosis framework to evaluate whether a person is becomingdepressed. This framework exploits the ontology technique toconstruct a DOM and it utilizes a BN to build a model to infer theprobability of becoming depressed. We referred to the OntoBayesmodel proposed by Yang and Calmet [27] to build the DOM, whichallowed it to be integrated with the BN to infer the probabilityof depression. We also introduced an extension to integrate thefrequency property into the Bayesian inference approach.
We implemented a prototype as a proof of concept and wedemonstrated the feasibility of the proposedmethod using a cloudenvironment and mobile agents, which can be run on the Android

96 Y.-S. Chang et al. / Future Generation Computer Systems 43–44 (2015) 87–98
(a) Usability. (b) Convenience.
(c) Readability. (d) Accuracy.
Fig. 15. Results of the satisfaction evaluation using a questionnaire-based survey. The results showed that the proposed method was considered to be acceptable.
Table 2Comparison with the Goldberg Depression Questionnaire.8
Proposed system Goldberg Depression Questionnaire[Online Version]
Goldberg Depression Questionnaire [Printed Version]
System latency Within one second. Can be calculated within onesecond.
Needs to calculate the score based on the patient orothers, which may take seconds to minutes.
Convenience Can be accessed anywhere after theAPP has been installed on the mobiledevice.
Can be accessed via a web browser. Can be used after the questionnaire is obtained by thepatient.
Readability Readily accessible user interface. Theuser can enter their state via a mobiledevice at anytime and anywhere.
Depends on the website layout. Thewebsite may not be suitable forreading on mobile devices. Inaddition, more sentences needs tobe read compared with theproposed method.
Easy to read on paper, but more sentences needs to beread compared with the proposed method.
Accuracy High. The model can be updatedinstantly by medical experts.
Medium. It may out-of-date if thewebsite is not updated with thelatest research results.
Low. It may out-of-date if the patient does not obtain thelatest version.
platform. We also evaluated the system’s latency and feasibility,including its Usability, Convenience, Readability, and Accuracy.The prototyping and evaluation results showed that the proposedsystemcan obtain effective and efficient predictions formost users.We also performed a comparison with previous methods andresearch, which showed that the proposed framework and systemhave the following advantages. First, the simple UI allows patientsto input their mood states via a mobile device to determine theirprobability of becoming depressed. Second, we used the mobilecloud to allow the result to be accessed anywhere and at anytime. Finally, integrating the ontology with the BN facilitatedthe accurate inference of the probability of a patient becomingdepressed.
In future research, we aim to perform a sensitivity analysisusing the BN to evaluate the proposed framework. We also plan toextend the proposed system to handle inputs from the user’s diary,such as themicroblogging and social network services provided by
Facebook9 or Twitter,10 thereby allowing the automatic analysisof the user’s mood to predict the likelihood of depression withoutuser interactions.
Acknowledgments
This research was supported by the National Science Councilof Taiwan, Republic of China under Grant No. NSC No. 100-2221-E-305-013 and Grant No. 101-2221-E-305-009. We would like toexpress our deep appreciation of the anonymous reviewers fortheir kind comments. In addition, we would also like to express
8 This questionnaire is used to determine whether you need to see a mentalhealth professional for the diagnosis and treatment of depression, or to monitoryour mood. http://www.mentalhelp.net/poc/view_doc.php?type=doc&id=973.9 Facebook, http://www.facebook.com.
10 Twitter, http://www.twitter.com.

Y.-S. Chang et al. / Future Generation Computer Systems 43–44 (2015) 87–98 97
our appreciation to the efforts made by open source softwaredevelopers, such as the producers of Protégé, GeNIe and SMILE, andJADE, without which this project would not have been possible.
References
[1] World Health Organization Media Centre (2012, Oct.), Depression is acommon illness and people suffering from depression need support andtreatment [online]. Available: http://www.who.int/mediacentre/news/notes/2012/mental_health_day_20121009/en/.
[2] World Health Organization Media Centre, Fact sheet No. 369 (2012, Oct.),Depression, [online] Available: http://www.who.int/mediacentre/factsheets/fs369/en/.
[3] S. Crystal, U. Sambamoorthi, J.T. Walkup, A. Akıncıgil, Diagnosis and treatmentof depression in the elderly Medicare population: predictors, disparities, andtrends, J. Am. Geriatr. Soc. 51 (12) (2003) 1718–1728.
[4] B. ZadJabbari, P. Wongthongtham, F.K. Hussain, Ontology based approach inknowledge sharing measurement, J. UCS 16 (6) (2010) 956–982.
[5] G. Eysenbach, What is e-health? J. Med. Internet Res. 3 (2) (2001).[6] R.S.H. Istepanian, S. Laxminarayan, C. Pattichis (Eds.), M-health: Emerging
Mobile Health Systems, Springer, 2005.[7] R.S.H. Istepanian, E. Jovanov, Y.T. Zhang, Guest editorial introduction to the
special section on M-health: beyond seamless mobility and global wirelesshealth-care connectivity, IEEE Trans. Inform. Technol. Biomed. 8 (2) (2004)405–414.
[8] D. Han, M. Lee, S. Park, THE-MUSS: Mobile u-health service system, Comput.Methods Programs Biomed. 97 (2010) 178–188.
[9] H. Löhr, A.-R. Sadeghi, M. Winandy, Securing the E-Health cloud, in: Proceed-ings of the 1st ACM International Health Informatics Symposium, ACM, 2010,pp. 220–229.
[10] L. Wang, G. Laszewski, A. Younge, X. He, M. Kunze, J. Tao, C. Fu, Cloudcomputing: a perspective study, New Gener. Comput. 28 (2) (2010) 137–146.
[11] L.Wang, D. Chen, Y. Hu, Y.Ma, J.Wa, Towards enabling cyberinfrastructure as aservice in Clouds, Special issue on Recent Advanced Technologies and Theoriesfor Grid and Cloud Computing and Bio-engineering, 39 (1) 2013, pp. 3–14.
[12] L. Wang, T. Kurze, J. Tao, M. Kunze, G. Laszewski, On-demand service hostingon production grid infrastructures, J. Supercomput. 66 (3) (2013) 1193–1788.
[13] K. Bilal, S.U. Khan, L. Zhang, H. Li, K. Hayat, S.A. Madani, N. Min-Allan, L. Wang,D. Chen, M. Iqbal, C.-Z. X, A.Y. Zomaya, Quantitative comparisons of the state-of-the-art data center architectures, Future Gener. Comput. Syst. 29 (3) (2013)739–750.
[14] I. Maglogiannis, E. Zafiropoulos, A. Platis, C. Lambrinoudakis, Risk analysis ofa patient monitoring system using Bayesian network modeling, J. Biomed.Inform. 39 (6) (2006) 637–647.
[15] Y. Ma, L. Wang, A.Y. Zomaya, D. Chen, R. Ranjan, Task-tree based large-scale mosaicking for massive remote sensed imageries with dynamic DAGscheduling, IEEE Trans. Parallel Distrib. Syst. 25 (8) (2014) 2126–2137.
[16] Y. Ma, L. Wang, D. Liu, T. Yuan, P. Liu, W. Zhang, Distributed data structuretemplates for data-intensive remote sensing applications, ConcurrencyComput.: Pract. Exp. 25 (12) (2013) 1784–1797.
[17] W. Zhang, L. Wang, D. Liu, W. Song, Y. Ma, P. Liu, D. Chen, Towards building amulti-datacenter infrastructure for massive remote sensing image processing,Concurrency Comput.: Pract. Exp. 25 (12) (2013) 1798–1812.
[18] L. Wang, J. Tao, R. Ranjan, H. Marten, A. Streit, J. Chen, D. Chen, G-Hadoop:MapReduce across distributed data centers for data-intensive computing,Future Gener. Comput. Syst. 29 (3) (2013) 739–750.
[19] L. Wang, M. Kunze, J. Tao, G. von Laszewski, Towards building a cloud forscientific applications, Adv. Eng. Softw. 42 (9) (2011) 714–722.
[20] F. Huang, D. Liu, X. Li, L. Wang, W. Xu, Preliminary study of a cluster-basedopen-source parallel GIS based on the GRASS GIS, Int. J. Digital Earth 4 (5)(2011) 402–420.
[21] I. Foster, C. Kesselman, N. Jennings, Brain meets brawn: why grid and agentsneed each other, in: Proceedings of the Third International Joint Conferenceon Autonomous Agents and Multiagent Systems, vol. 1, 2004, pp. 8–15.
[22] G. Quellec, M. Lamard, G. Cazuguel, C. Roux, B. Cochener, Case retrieval inmedical databases by fusing heterogeneous information, IEEE Trans. Med.Imaging 30 (1) (2011) 108–118.
[23] P. Chen, R. Verma, A query-based medical information summarizationsystem using ontology knowledge, in: 19th IEEE International Symposium onComputer-Based Medical Systems, 2006, pp. 37–42.
[24] G. Bucci, V. Sandrucci, E. Vicario, Ontologies and Bayesian networks inmedicaldiagnosis, in: 44th Hawaii International Conference on System Sciences(HICSS), 2011, pp. 1–8.
[25] O. Arsene, I. Dumitrache, I. Mihu, Medicine expert system dynamic Bayesiannetwork and ontology based, Expert Syst. Appl. 38 (12) (2011) 15253–15261.
[26] H.T. Zheng, B.Y. Kang, H.G. Kim, An Ontology-based Bayesian NetworkApproach for Representing Uncertainty in Clinical Practice Guidelines,in: Lecture Notes in Comput. Sci., vol. 5327, 2008, pp. 161–173.
[27] Y. Yang, J. Calmet, Ontobayes an ontology-driven uncertainty model, in:International Conference onComputational Intelligence forModelling, Controland Automation, 28–30 Nov. 2005, pp. 457–463.
[28] S. Fenz, AM. Tjoa,M. Hudec, Ontology-based generation of Bayesian networks,in: International Conference on Complex, Intelligent and Software IntensiveSystems, 2009, pp. 712–717.
[29] F. Colace,M.De Santo, Ontology for E-learning a Bayesian approach, IEEE Trans.Educ. 52 (1) (2010) 223–233.
[30] S. Sadeghi, A. Barzi, J.W. Smith, Ontology driven construction of a knowledge-base for Bayesian decisionmodels based on UMLS, in: Proceedings ofMIE2005- The XIXth International Congress of the European Federation for Medical In-formatics, 2005, pp. 223–228.
[31] B. Hu, B. Hu, J. Wan, M. Dennis, H.H. Chen, L. Li, Q. Zhou, Ontology basedubiquitous monitoring and treatment against depression, Wirel. Commun.Mobile Comput. 10 (10) (2010) 1303–1319.
[32] B. ZadJabbari, P. Wongthongtham, F.K. Hussain, Ontology based approach inknowledge sharing measurement, J. UCS 16 (6) (2010) 956–982.
[33] N.F. Noy, D.L. McGuinness, Ontology Development 101: A Guideto Creating Your First Ontology, Stanford Knowledge Systems Lab-oratory Technical Report KSL-01-05 and Stanford Medical Infor-matics Technical Report SMI-2001-0880, 2001, Accessed fromhttp://www.ksl.stanford.edu/people/dlm/papers/ontology-tutorial-noy-mcguinness-abstract.html.
[34] B.D. Martino, Semantic web services discovery based on structural ontologymatching, Int. J. Web Grid Serv. 5 (1) (2009) 46–65.
[35] M. Lanzenberger, J. Sampson, M. Rester, Ontology visualization: tools andtechniques for visual representation of semi-structured meta-data, J. UCS 16(7) (2010) 1036–1054.
[36] J.J. Jung, Semantic wiki-based knowledgemanagement system by interleavingontology mapping tool, Int. J. Softw. Eng. Knowl. Eng. 23 (1) (2013) 51–63.
[37] J.J. Jung, Ontology mapping composition for query transformation ondistributed environments, Expert Syst. Appl. 37 (12) (2010) 8401–8405.
[38] Wikipedia, Bayesian network—Wikipedia, the free encyclopedia, [online].Available: http://en.wikipedia.org/wiki/Bayesian_network.
[39] N. Friedman, D. Geiger, M. Goldszmidt, Bayesian network classifiers, Mach.Learn. 29 (1997) 131–163.
[40] T. Gu, H.K. Pung, D.Q. Zhang, H.K. Pung, D.Q. Zhang, A Bayesian Approach ForDealing With Uncertain Contexts, 2004.
[41] N. Fernando, S.W. Loke, W. Rahayu, Mobile cloud computing: a survey, FutureGener. Comput. Syst. 29 (2013) 84–106.
[42] H.T. Dinh, C. Lee, D. Niyato, P. Wang, A survey of mobile cloud computing:architecture, applications, and approaches, Wirel. Commun. Mobile Comput.(2011).
[43] F. Liu, P. Shu, H. Jin, L. Ding, J. Yu, Gearing resource-poor mobile deviceswith powerful clouds: architectures, challenges, and applications, IEEE Wirel.Commun.Mag. 20 (3) (2013) 14–22. Special Issue onMobile Cloud Computing.
[44] V. Chan, P. Ray, N. Parameswaran,Mobile e-Healthmonitoring: an agent-basedapproach, IET Commun. 2 (2) (2008) 223–230.
[45] Y. Liang, X. Zhou, Z. Yu, B. Guo, Energy-efficient motion related activityrecognition on mobile devices for pervasive healthcare, in: Mobile Networksand Applications, Springer Press, 2014.
[46] L. Tang, X. Zhou, Z. Yu, Y. Liang, D. Zhang, H. Ni, MHS: a multimedia systemfor improving medication adherence in elderly care, IEEE Syst. J. 5 (4) (2011)506–517.
[47] D. Gotta, T. Trucco, M. Ughetti, S. Semeria, C. Cuce, A.M. Porcino, JadeAndroid Add-On Guide, Available at http://jade.tilab.com/doc/tutorials/JADE_ANDROID_Guide.pdf.
Yue-Shan Chang received his Ph.D. Degree from theDepartment of Computer and Information Science atthe National Chiao Tung University in 2001. He joinedthe Department of Electronic Engineering at Ming HsingUniversity of Science and Technology in August 1992.In August 2004, he joined the Department of ComputerScience and Information Engineering, National TaipeiUniversity, Taipei County, Taiwan. In August 2010, hebecame a Professor. His research interests are distributedsystems, web service composition, information retrieval,mobile computing, and grid computing.
Chih-Tien Fan received his M.Sc. degree in computerscience and information engineering from National TaipeiUniversity, New Taipei city, Taiwan, in 2010. He is agraduate student on the Ph.D. program. His researchinterests are ubiquitous and intelligent computing, cloudcomputing, and agent technology.

98 Y.-S. Chang et al. / Future Generation Computer Systems 43–44 (2015) 87–98
Win-Tsung Lo received his B.S. and M.S. degrees inapplied mathematics from National Tsing Hua University,Taiwan, Republic of China, and M.S. and Ph.D. degreesin computer science from the University of Maryland.He is now a vice president of Tung Hai University,Taiwan, Republic of China. His research interests includedistributed systems, data exchange in heterogeneousenvironments, and recommendation systems.
Wan-Chun Hung received his M.Sc. degree in computerscience and information engineering from National TaipeiUniversity, New Taipei city, Taiwan, in 2013. His researchinterests are ontology, mobile computing, cloud comput-ing, and agent techniques.
Shyan-Ming Yuan received his BSEE degree from NationalTaiwan University in 1981, his M.S. degree in ComputerScience from University of Maryland, Baltimore Countyin 1985, and his Ph.D. degree in Computer Science fromthe University of Maryland College Park in 1989. Dr Yuanjoined the Electronics Research and Service Organization,Industrial Technology Research Institute as a ResearchMember in October 1989. Since September 1990, he hasbeen an Associate Professor in the Department of Computerand Information Science, National Chiao Tung University,Hsinchu, Taiwan. He became a Professor in June 1995. His
current research interests include distributed objects, internet technologies, andsoftware system integration. Dr Yuan is a member of ACM and IEEE.