Embed Size (px)
Citation preview

MODELING OF CARDIAC BIOMARKERS IN BREAST CANCER PATIENTS
TREATED WITH ANTHRACYCLINES AND TRASTUZUMAB REGIMENS.
AURELIA DE VRIES SCHULTINK, PHD STUDENT, NKI.
ICPAD 2017

BACKGROUND – CARDIOTOXIC ANTI-CANCER DRUGS
- Anthracyclines
- Epirubicin and doxorubicin chemotherapies for breast cancer
- Cumulative lifetime doses associated with incidence CHF
- Mechanism: myocyte damage
- Irreversible
2
BACKGROUND – CARDIOTOXIC ANTI-CANCER DRUGS
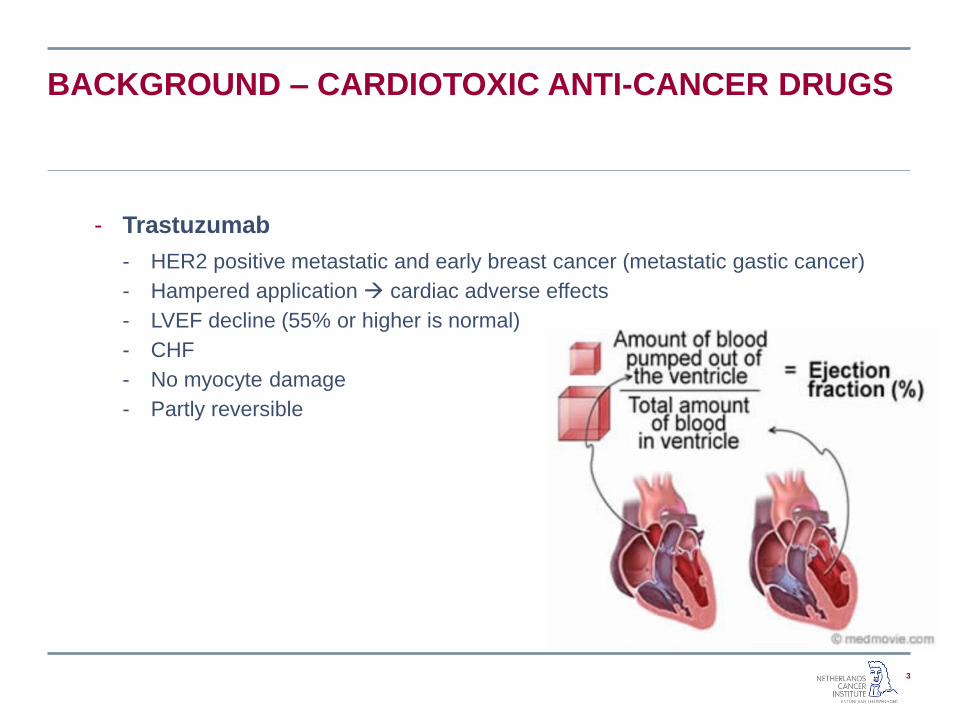
- Trastuzumab
- HER2 positive metastatic and early breast cancer (metastatic gastic cancer)
- Hampered application cardiac adverse effects
- LVEF decline (55% or higher is normal)
- CHF
- No myocyte damage
- Partly reversible
3
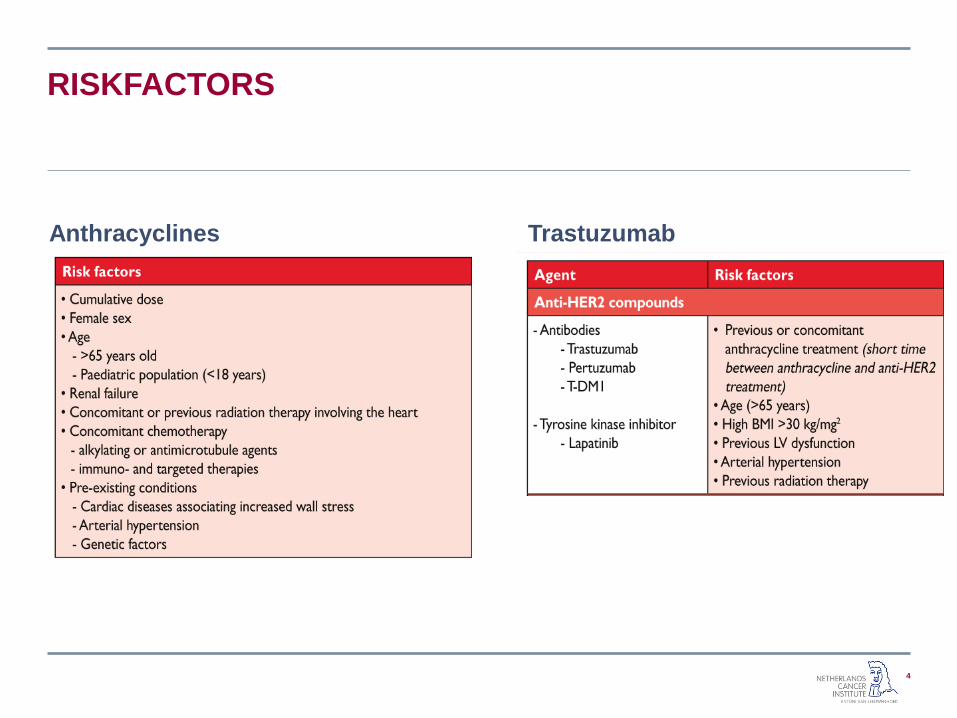
RISKFACTORS
4
Anthracyclines Trastuzumab
CURRENT CARDIAC MONITORING
5
- Anthracyclines
- Cumulative life time doses
- 550 mg/m2 doxorubicine
- 950 mg/m2 epirubicin
- Trastuzumab
- LVEF monitoring during treatment (>15% change or <45%)
- Echocardiography or MUGA scan treatment cessation
- While it is happening
CARDIAC BIOMARKERS
6
- Cardiac biomarkers- i.e. Troponin T (myocyte damage)
- or NT-proBNP (decompensation)
- Could allow for early detection of drug-induced cardiotoxicity
- Currently no evidence for management based on abnormal cardiac markers
- What’s the optimal timepoint of cardiac biomarker assessment?
AIM
7
Quantify kinetics and exposure response relationship of
LVEF, troponin T and NT-proBNP in breast cancer patients receiving anthracyclines follwed by trastuzumab.
DATA
8
- Previously published RCT
- 206 evaluable patients with early HER2-positive breast cancer
- Treated with anthracyclines followed by trastuzumab

METHODS
10
- Develop anthracycline-troponin T model
- Develop trastuzumab LVEF model
- Evaluate models NT-proBNP- Anthracyclines-NT-proBNP
- Trastuzumab-NT-proBNP
- LVEF-NT-proBNP: inverse, delayed inverse etc.
- Evaluate covariates (forward inclusion/backward elimination)
Anthracyclines Trastuzumab
Age Age
Radiotherapy of the chest and
laterality
Radiotherapy of the chest and
laterality
Hypertension Hypertension
Type of anthraycline Baseline LVEF
dTIME last ANT dose, first TT dose

RESULTS ANTHRACYCLINES-TROPONINE T
11
- K-PD model
- Baseline model for anthracycline—troponin T
𝑇𝑅𝑃 = 𝑇𝑅𝑃0 ∙ (1 + 𝑠𝑙𝑜𝑝𝑒 ∙ 𝐶𝑎𝑛𝑡)
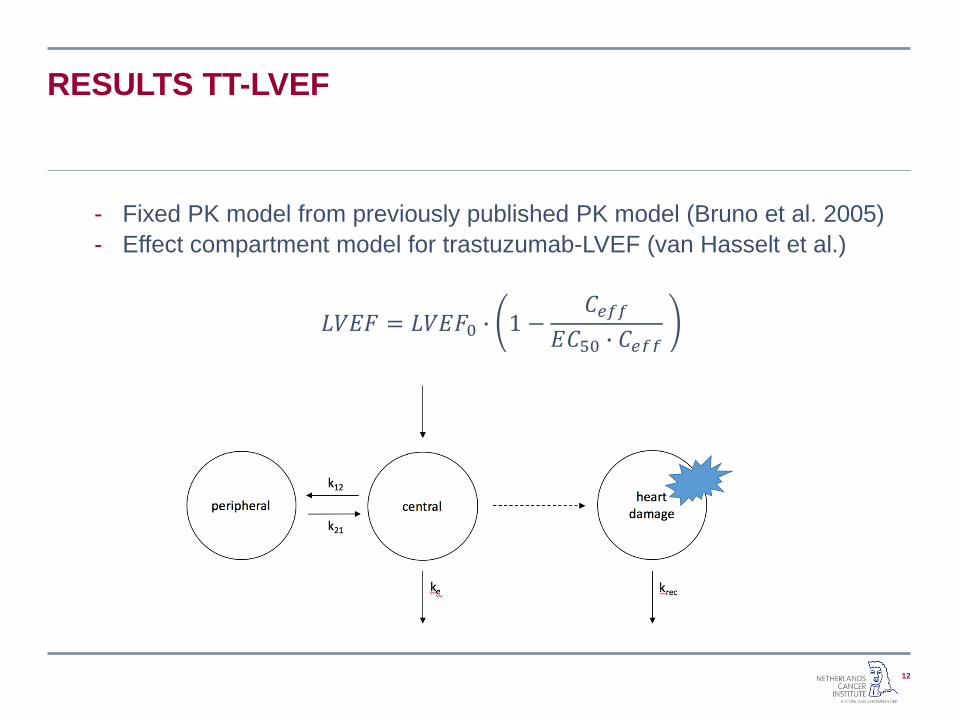
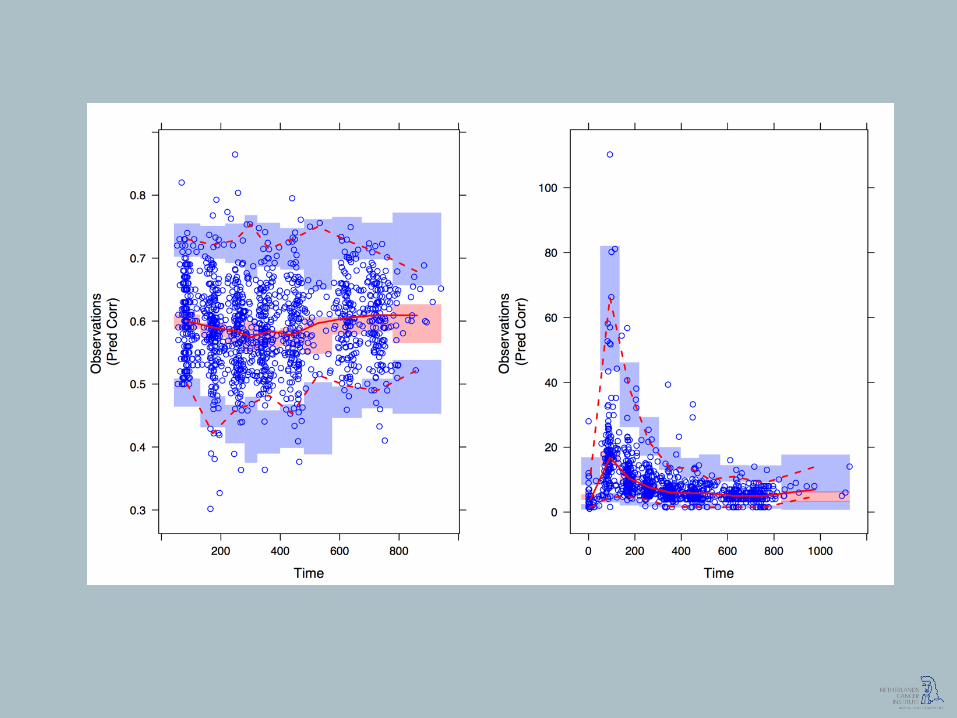
RESULTS TT-LVEF
12
- Fixed PK model from previously published PK model (Bruno et al. 2005)
- Effect compartment model for trastuzumab-LVEF (van Hasselt et al.)
𝐿𝑉𝐸𝐹 = 𝐿𝑉𝐸𝐹0 ∙ 1 −𝐶𝑒𝑓𝑓
𝐸𝐶50 ∙ 𝐶𝑒𝑓𝑓
RESULTS NT-PROBNP
13
- No inverse of LVEF decline,
- No unified trends or changes during ant or TT
- Baseline NT-proBNP tested as covariates no significance
- 4 patients with significant decline in LVEF have late onset peaks of NTproBNP > 1000 pmol/L
- Result of LVEF decline or other underlying disease.

A
B

SENSITIVITY TO LVEF DECLINE
16
- Maximum concentration of troponin T measure for cardiac damage during anthracycline treatment
- LVEF baseline before start trastuzumab
- 14.2% and 22.4% of IIV in EC50
A
B
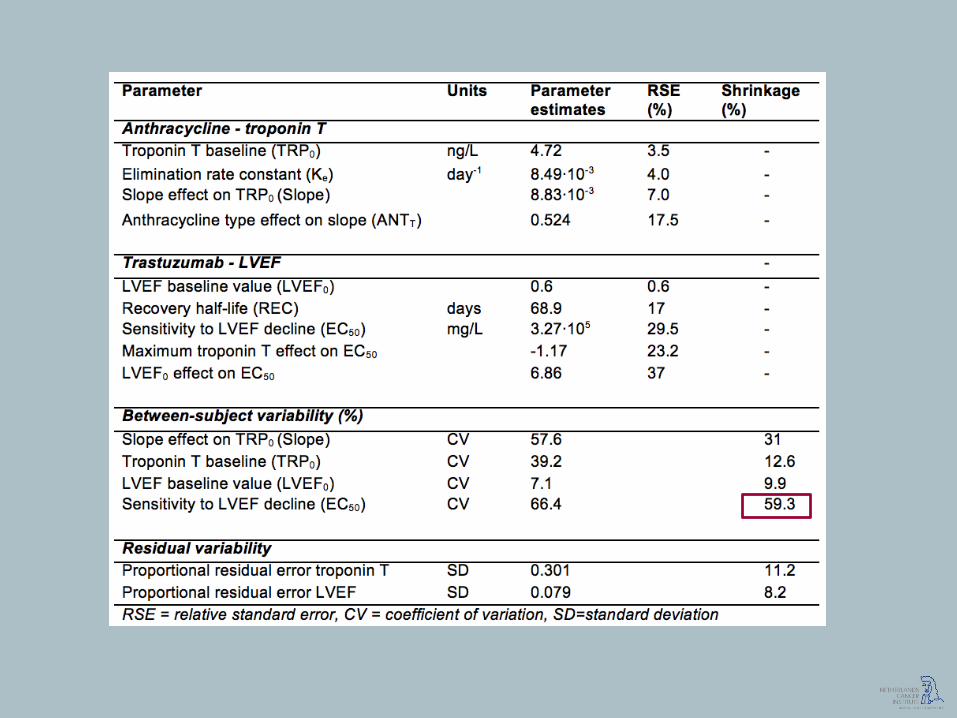
EC50 PARAMETER
20
- By adding covariates shrinkage is increased from 33% to 59%
- Small subgroup of patients is very sensitive for LVEF decline- Partly explained by covariates- Increased shrinkage
- Other patients are not sensitive for LVEF decline
- Left skewedness of EC50 IIV is improved by adding covariates PPC

DISCUSSION
21
- Small group of patient is sensitive to LVEF decline;- Inclusion criteria of RCT patients with low cardiac risk
- Exclusion criteria of RCT exclude patients with high risk
- Previously reported risk factors could not be identified- Age: Highest age 69 (13% > 60 years)
- Cardiac history: relavitely low risk patients
- Radiotherapy: medistinal RT excluded
- dTIME ANT-TT: 6% > 30 days
- NT-proBNP- Peak in patients with cardiac “event”
- Related to LVEF decline?
- Related to late onset cardiac effects?
CONCLUSIONS
22
- Troponin T and LVEF baseline can possibly be used as a biomarkers for LVEF decline
- Troponin T max: 23 days after last ANT infusion.
- NT-proBNP
- Hetereogeneous data is needed for evaluation in high risk patients
- Improve cardiac monitoring strategies- Evaluation with simulations

ACKNOWLEDGMENTS
23
Netherlands Cancer Institute Leiden University
Alwin Huitema Coen van Hasselt
Annelies Boekhout
Thomas Dorlo
Jan Schellens
QUESTIONS
24