Embed Size (px)
Citation preview
Modeling Risk and Reducing Liability through Better Communication and Teamwork
David P. Baker, PhDIMPAQ International, LLC
Overview
• Preparing for Demonstration Grant (R21)• Research Team
– David P. Baker, PhD (Principal Investigator)– Patrice Weiss, MD (Co-Investigator)– Laurie Spotswood, MSEd, CLS (Research Specialist)– Tony Slonim, MD, DPH (Co-Investigator)
Background
• Relations between lawsuits, payouts, and negligence is muddy at best
• The Harvard Malpractice Study – Reviewed 30,000 hospital records– Found the incidence of malpractice was much larger than the
incidence of claims
• Ineffective communication between patients/families and clinicians yield lawsuits
• Patients/families are viewed as critical members of the care team– TeamSTEPPS® introduced by AHRQ for clinician teamwork– Little work on how to include/train patients/families
Study Aims• Aim 1: To identify clinical events that are highly dependent on provider
teamwork, require patient/ families to be effective members of the team, and vary in terms of risk and liability.
• Aim 2: To identify the root causes of these events, including where critical teamwork breakdowns occur.
• Aim 3: To conduct a series of focus groups to ascertain how patient/family and provider communication should occur to mitigate risk and reduce liability and to identify TeamSTEPPS tools that could be used to enable patients/families to be more effective members of the care team.
• Aim 4: To develop and pilot test a TeamSTEPPS intervention(s) that teaches patients/families how to be members of the care team and enhances communication between patients/families and providers.
Aim 1
• Goal– Identify and select events that require teamwork and vary in
terms of risk and liability in Labor and Delivery (L&D)• Approach
– Reviewed RAND (2008) report and identified candidate events that require teamwork
– Identified 18 candidate events in L&D– Surveyed 10 clinical experts
• Degree of Risk • Likelihood of Liability• Requirement for Teamwork
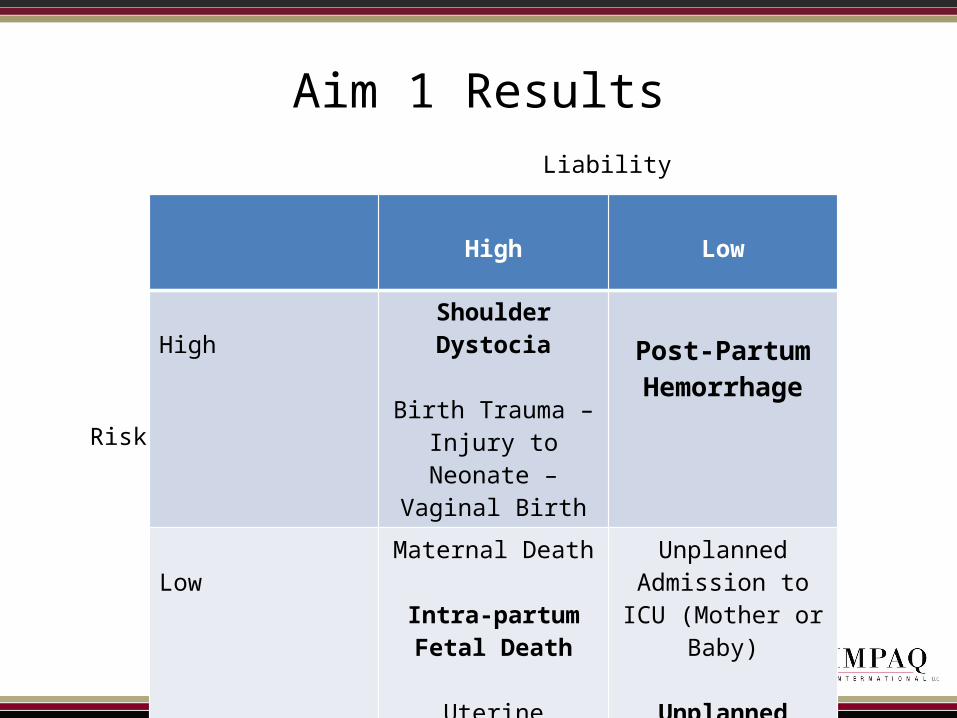
Aim 1 Results
High Low
HighShoulder Dystocia
Birth Trauma – Injury to Neonate – Vaginal
Birth
Post-Partum Hemorrhage
LowMaternal Death
Intra-partum Fetal Death
Uterine Rupture
Unplanned Admission to ICU (Mother or Baby)
Unplanned Return to LD or OR
Liability
Risk
Aim 2• Goal
– Identify the root causes of these events, including where critical teamwork breakdowns occur• Root causes included: (1) risk factors; (2) individual, team, & systems
factors; (3) clinical team members; and (4) patient and family responsibilities
• Divided L&D into six phases: (1) pre-hospital; (2) triage/ assessment; (3) monitoring/laboring; (4) delivery; (5) post-partum L&D; and (6) post-partum mother baby unit.
• Approach– Two phases of key informant interviews with clinical staff
• Phase I – Identify events (12 interviews)• Phase II – Validate events (11 interviews)
– Identified common root causes across all four events (identified during Aim 1)
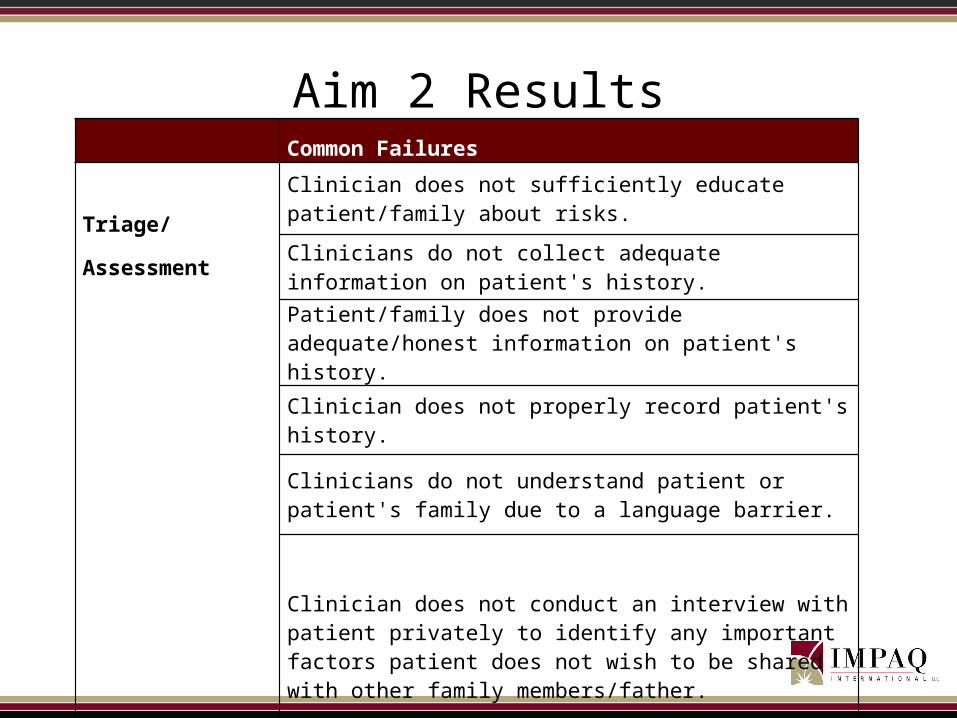
Aim 2 Results Common Failures
Triage/Assessment
Clinician does not sufficiently educate patient/family about risks.
Clinicians do not collect adequate information on patient's history.
Patient/family does not provide adequate/honest information on patient's history.
Clinician does not properly record patient's history.
Clinicians do not understand patient or patient's family due to a language barrier.
Clinician does not conduct an interview with patient privately to identify any important factors patient does not wish to be shared with other family members/father.
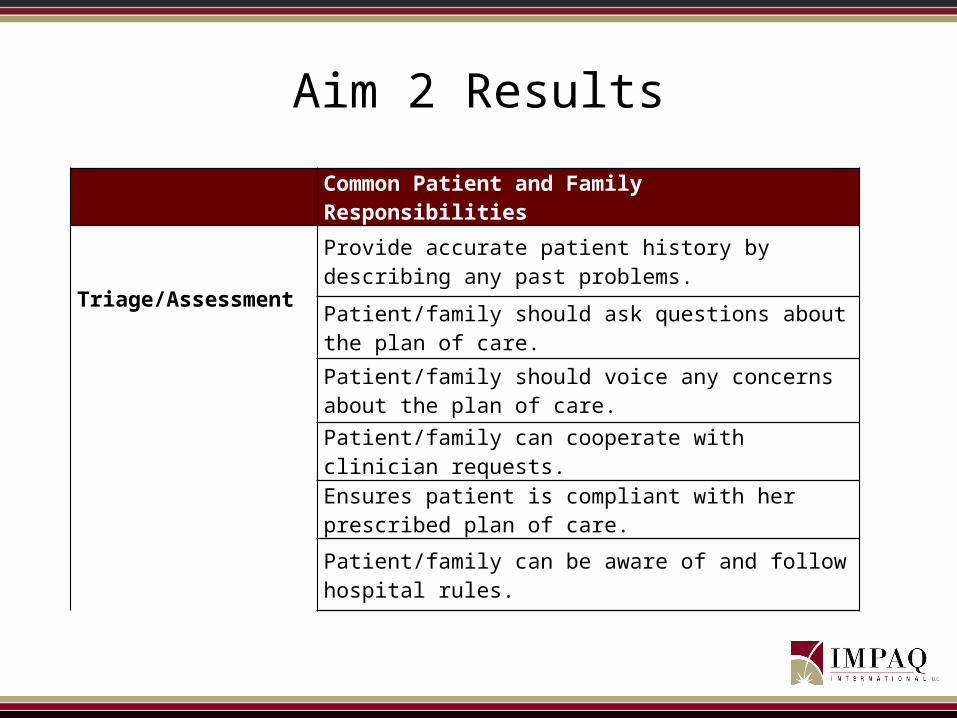
Aim 2 Results
Common Patient and Family Responsibilities
Triage/Assessment
Provide accurate patient history by describing any past problems.
Patient/family should ask questions about the plan of care.
Patient/family should voice any concerns about the plan of care.
Patient/family can cooperate with clinician requests.
Ensures patient is compliant with her prescribed plan of care.
Patient/family can be aware of and follow hospital rules.
Aim 3• Goal
– Collect information from patients and family members in order to:• Verify patient and family responsibilities• Identify the root causes per event that patients would want disclosed and
clinical staff would feel should be disclosed• Identify TeamSTEPPS tools and strategies patients would find useful
• Approach– Four patient and family focus groups; one per L&D event
• Verified the patient and family responsibilities clinicians identified• Facilitated discussion about what patients and families want clinicians to
disclose• Conducted disclosure survey of patients and providers focused on the
different events• Reviewed and discussed TeamSTEPPS tools
– 47 patient and family members; 13 clinicians
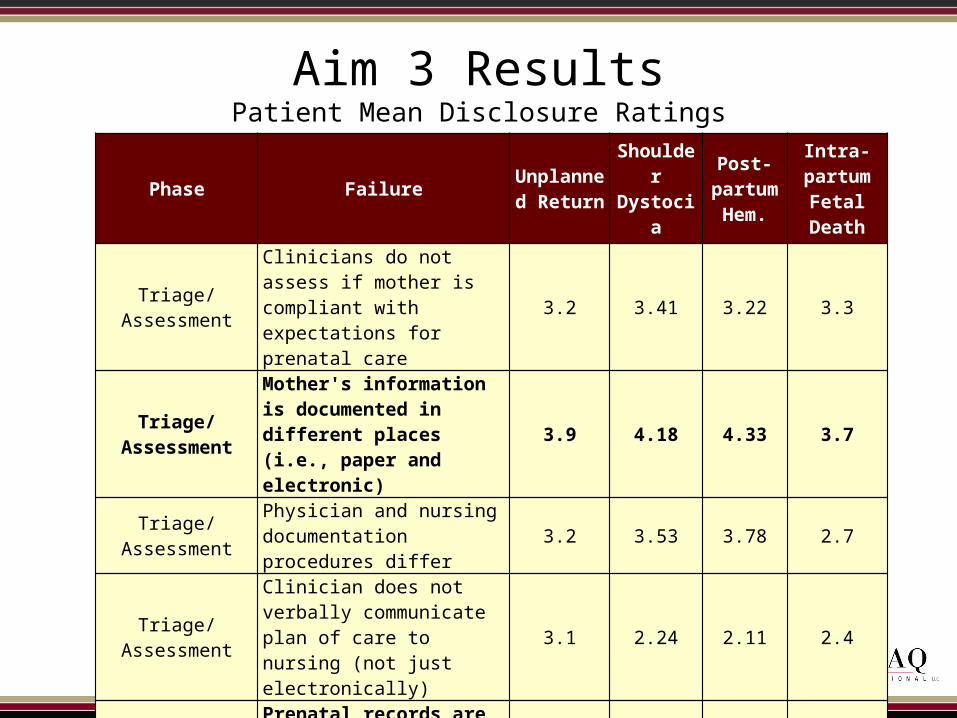
Aim 3 ResultsPatient Mean Disclosure Ratings
Phase Failure Unplanned Return
Shoulder Dystocia
Post-partum Hem.
Intra-partum
Fetal Death
Triage/AssessmentClinicians do not assess if mother is compliant with expectations for prenatal care
3.2 3.41 3.22 3.3
Triage/AssessmentMother's information is documented in different places (i.e., paper and electronic)
3.9 4.18 4.33 3.7
Triage/AssessmentPhysician and nursing documentation procedures differ
3.2 3.53 3.78 2.7
Triage/AssessmentClinician does not verbally communicate plan of care to nursing (not just electronically)
3.1 2.24 2.11 2.4
Triage/Assessment Prenatal records are not available or missing 2.6 1.35 1.56 2.2
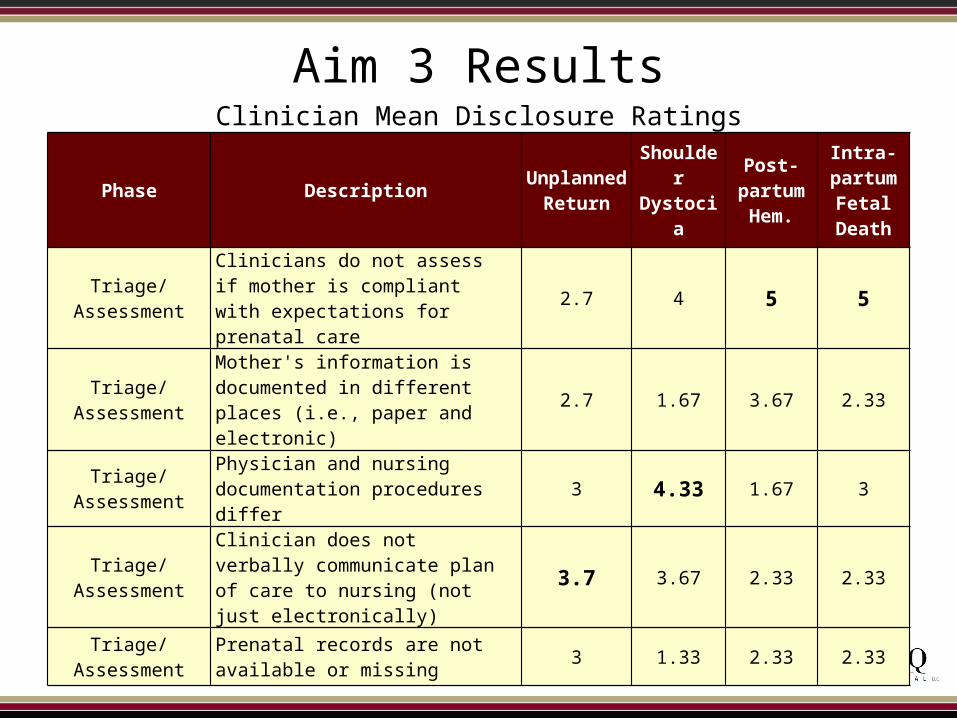
Aim 3 ResultsClinician Mean Disclosure Ratings
Phase Description Unplanned Return
Shoulder Dystocia
Post-partum Hem.
Intra-partum
Fetal Death
Triage/ AssessmentClinicians do not assess if mother is compliant with expectations for prenatal care
2.7 4 5 5
Triage/ AssessmentMother's information is documented in different places (i.e., paper and electronic)
2.7 1.67 3.67 2.33
Triage/ Assessment Physician and nursing documentation procedures differ 3 4.33 1.67 3
Triage/ AssessmentClinician does not verbally communicate plan of care to nursing (not just electronically)
3.7 3.67 2.33 2.33
Triage/ Assessment Prenatal records are not available or missing 3 1.33 2.33 2.33
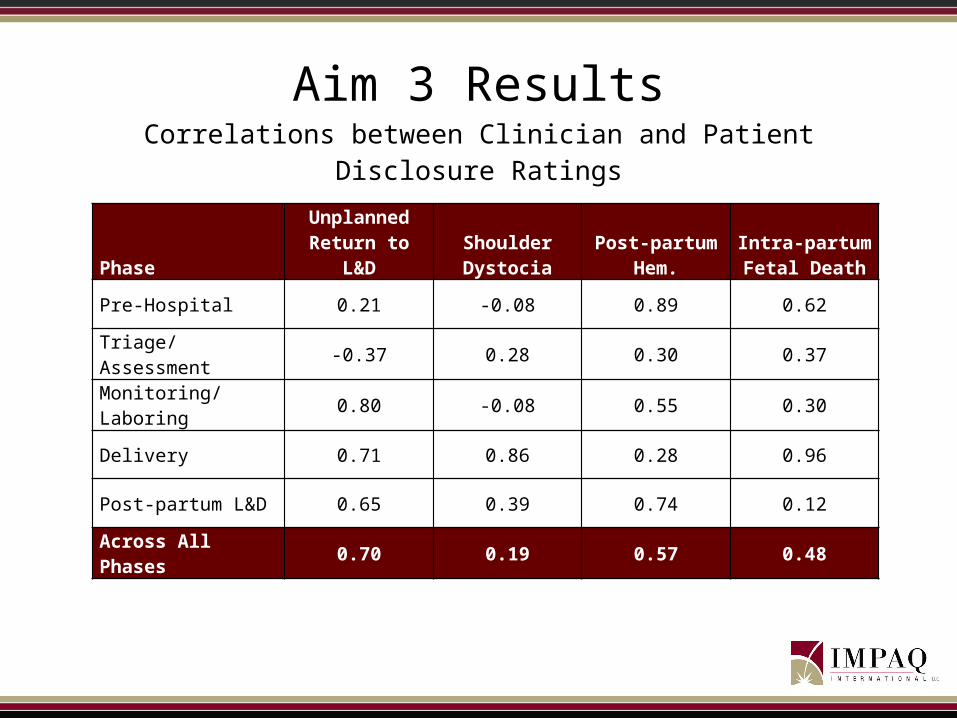
Aim 3 ResultsCorrelations between Clinician and Patient Disclosure Ratings
PhaseUnplanned
Return to L&DShoulder Dystocia
Post-partum Hem.
Intra-partum Fetal Death
Pre-Hospital 0.21 -0.08 0.89 0.62
Triage/Assessment -0.37 0.28 0.30 0.37
Monitoring/Laboring 0.80 -0.08 0.55 0.30
Delivery 0.71 0.86 0.28 0.96
Post-partum L&D 0.65 0.39 0.74 0.12
Across All Phases 0.70 0.19 0.57 0.48

Aim 4
• Goal– To develop and pilot test a TeamSTEPPS intervention(s) that
teaches patients/families how to be members of the care team and enhances communication between patients/families and providers
• Approach– Developed a 45-minute, patient and family oriented
TeamSTEPPS module for L&D– 28 participants– Collected pre-post data on participant reactions and learning
• Reactions: instrumentality and affective• Learning: attitudes (T-TAQ) and knowledge (Learning Benchmarks)
TeamSTEPPS Training Objectives
• Describe how the patient and family fits into the clinical team
• Describe the patient and family responsibilities as team members
• Describe the clinical team member roles and responsibilities• Describe the core components of team leadership,
assertion, and communication• Describe TeamSTEPPS tools that can be used by patients
– Briefs, Huddles and Debriefs– Assertive Statement and Two-Challenge Rule– SBAR and Check Back

Aim 4 - Results
• Reactions– Overall mean rating was 4.18, on a 5-point scale
• “This training would be appropriate for patients in all care settings”
• “This training should be offered by …. in the future”
• Learning– Attitudes
• Pre-training Mean (4.51)• Post-training Mean (4.55)
– Learning• Pre-training Mean (10.86 items correct)• Post-training Mean (12.28 items correct)

Conclusions• Clinicians generally showed high agreement when assessing the degree of
risk, liability, and teamwork associated with specific clinical events in L&D• Regardless how events varied in terms of risk and liability, the individual,
team, and system failures were generally common across events• Patients/family members were found to agree about which failures were
important to disclose, and type of adverse event did not affect these results
• Clinicians on the other hand showed far more variability regarding what should be disclosed, and these results did appear to be affected by adverse event type
• Patients/families like TeamSTEPPS, intended to use the tools taught, would recommend the training to others, and showed gains in knowledge

Next Steps
• Negotiating with an implementation site• Examine transfer of the trained skills• Determine if there is a relation to clinical outcomes




















![Teamwork [1]](https://img.pdfslide.net/doc/110x75/55625904d8b42aa52d8b577e/teamwork-1.jpg)








