Embed Size (px)
Citation preview
Modelling and Simulation Group, School of Pharmacy
Pharmacokinetic/Pharmacodynamic Understanding For Fentanyl IntraNasal in the Paediatric
Population
Aaron BasingSupervisors
Prof. Carl Kirkpatrick
Dr David Herd
A/Prof. Bruce Charles
Dr Ross Norris
PUFFIN
Modelling and Simulation Group, School of Pharmacy
Overview
• Why study Intranasal Fentanyl (INF) in children
• Aims and Hypothesis
• Results so far
Modelling and Simulation Group, School of Pharmacy
What is INF ?
• Fentanyl that is administered via the nasal route for analgesia
Modelling and Simulation Group, School of Pharmacy
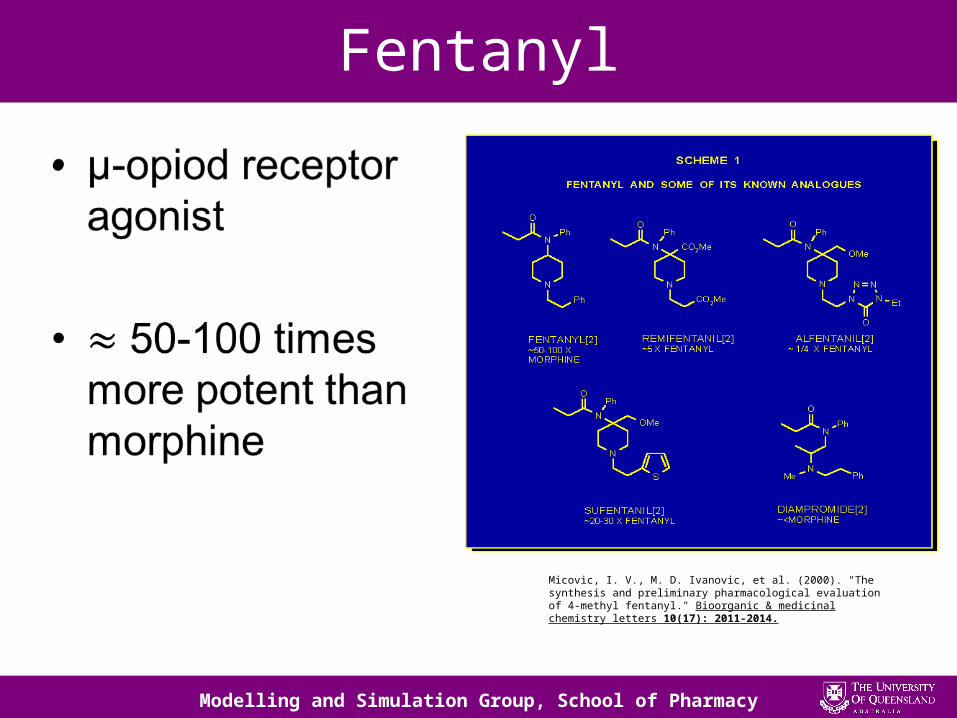
Fentanyl
Micovic, I. V., M. D. Ivanovic, et al. (2000). "The synthesis and preliminary pharmacological evaluation of 4-methyl fentanyl." Bioorganic & medicinal chemistry letters 10(17): 2011-2014.
Modelling and Simulation Group, School of Pharmacy
Medical Uses of Fentanyl
• Multiple clinical applications
– Anaesthesia• Induction• Maintenance
– Analgesia• Acute• Chronic

Modelling and Simulation Group, School of Pharmacy
Clinical Context
• Paediatric Emergency Room
– Painful injuries are common
– Painful procedures are common
Most frequent diagnoses of paediatric ED patients at PREDICT sites (n = 314 025 presentations at nine sites)2
Acworth, J., F. Babl, et al. (2009). "Patterns of presentation to the Australian and New Zealand Paediatric Emergency Research Network." Emergency medicine Australasia : EMA 21(1): 59-66.
Modelling and Simulation Group, School of Pharmacy
Clinical Context
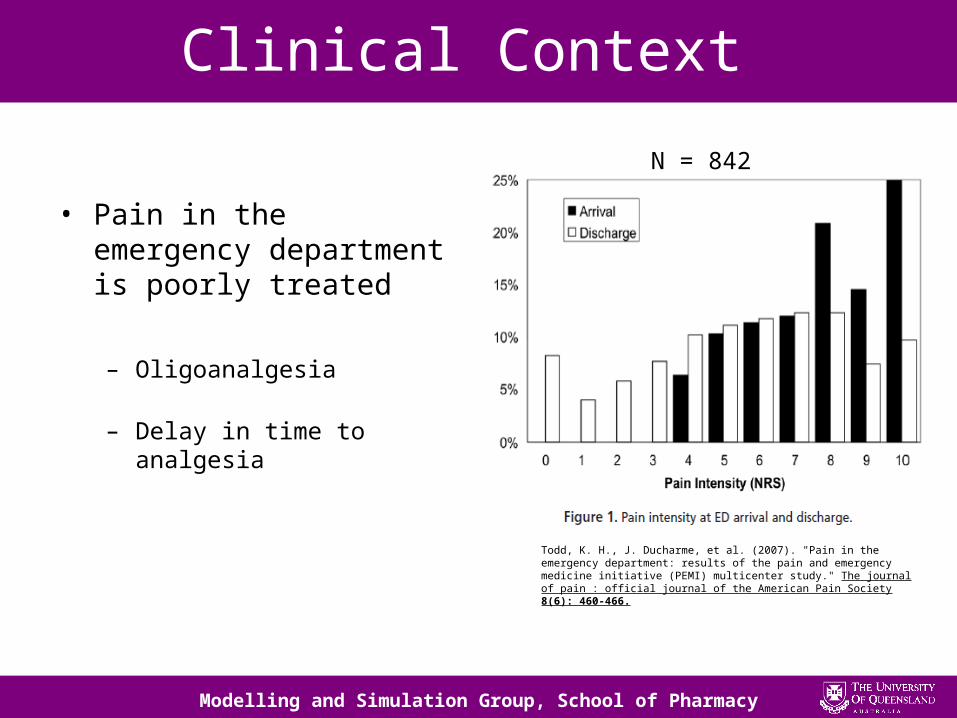
• Pain in the emergency department is poorly treated
– Oligoanalgesia
– Delay in time to analgesia
Todd, K. H., J. Ducharme, et al. (2007). "Pain in the emergency department: results of the pain and emergency medicine initiative (PEMI) multicenter study." The journal of pain : official journal of the American Pain Society 8(6): 460-466.
N = 842

Modelling and Simulation Group, School of Pharmacy
Why do we need INF ?
• Viable alternative to intravenous analgesia
– Needleless
– Rapid Absorption
– Sterile technique not
required
Modelling and Simulation Group, School of Pharmacy
What we already know about INF
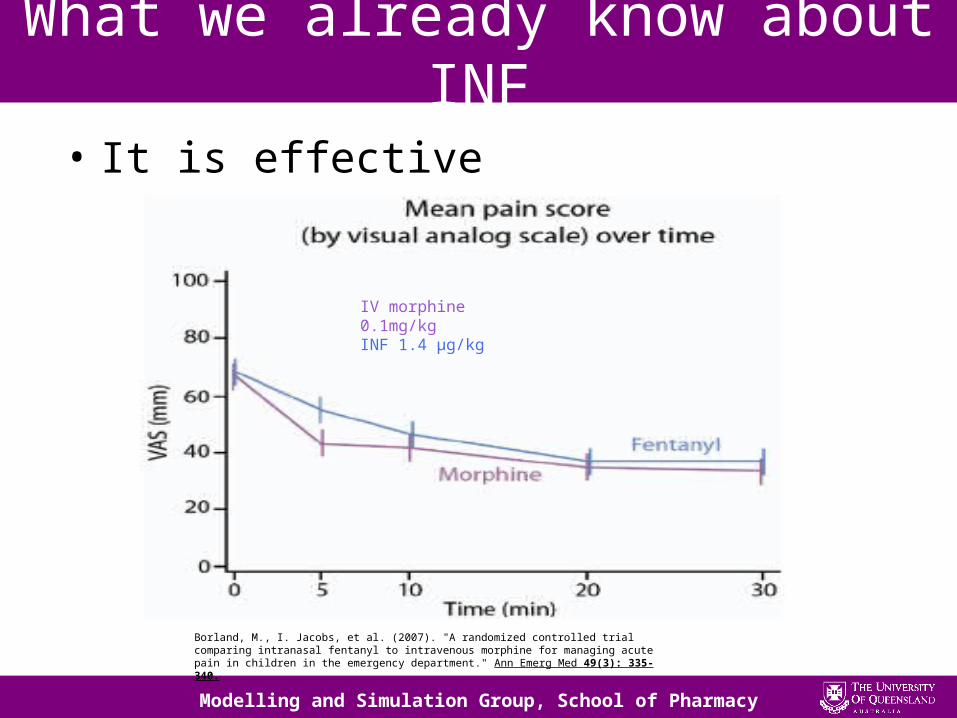
• It is effective
IV morphine 0.1mg/kgINF 1.4 µg/kg
Borland, M., I. Jacobs, et al. (2007). "A randomized controlled trial comparing intranasal fentanyl to intravenous morphine for managing acute pain in children in the emergency department." Ann Emerg Med 49(3): 335-340.
Modelling and Simulation Group, School of Pharmacy
What we already know about INF
• It can reduce time to analgesia
Modelling and Simulation Group, School of Pharmacy
Summary so far
• Painful injuries and procedures are common in paediatric emergency departments.
• INF has several features that are well suited to use within a paediatric emergency department
Modelling and Simulation Group, School of Pharmacy
What we DON’T know about INF
• The underlying pharmacokinetics for INF in the paediatric population
Modelling and Simulation Group, School of Pharmacy
What we don’t know about
• Dosing strategies have been developed empirically from adult pharmacokinetic studies
Potential for therapeutic catastrophe
Modelling and Simulation Group, School of Pharmacy
Pharmacokinetics of Fentanyl
• ABSORPTION
• DISTRIBUTION
• METABOLISM
• EXCRETION
Modelling and Simulation Group, School of Pharmacy
Pharmacokinetics in Adults
ABSORPTION
– Rapid, Tmax approx 10 minutes
– Bioavailablity – 70-90%
Drug Administration
Drug in Blood Stream
Modelling and Simulation Group, School of Pharmacy
What we know about the pharmacokinetics of fentanyl
DISTRIBUTION
– Octanol/Water Coefficient 9550 – Adipose Tissue – some– Skeletal muscle – some– Well Perfused organs – High
Drug in Blood Stream Body Tissue
Modelling and Simulation Group, School of Pharmacy
What we know about the pharmacokinetics of fentanyl
METABOLISM
• Primarily N-Dealkylation to norfentanyl (inactive) by CYP3A4
• Large variability in clearance– Genetic variability in CYP3A4– Physiologic and pathophysiologic variability in liver blood flow
Drug in Blood Stream Metabolites
Modelling and Simulation Group, School of Pharmacy
What we know about the pharmacokinetics of fentanyl
EXCRETION
• Kidney– 10% Unchanged
• Faeces– 1% Unchanged
Drug in Blood Stream
Drug outside of body
Modelling and Simulation Group, School of Pharmacy
What we need to know INF
• Guestimate of pharmacokinetic parameters in paediatrics compared to adults
– Clearance ? ↓
– Volume of Distribution ? ↓
– Nasal absorption rate constant ???? ↑↓
Modelling and Simulation Group, School of Pharmacy
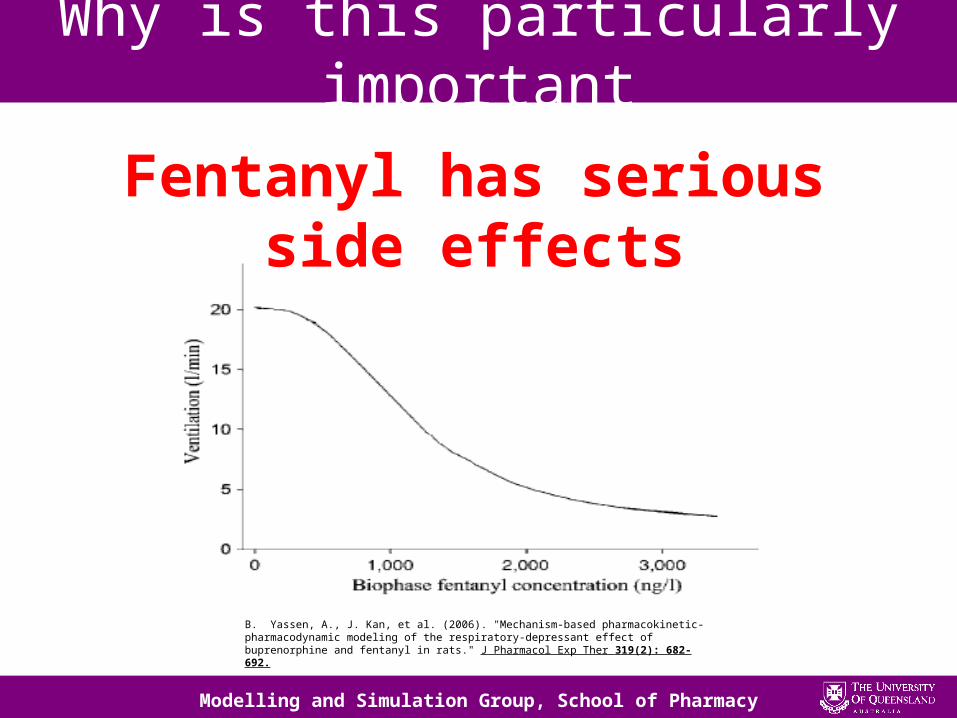
Why is this particularly important
Fentanyl has serious side effects
B. Yassen, A., J. Kan, et al. (2006). "Mechanism-based pharmacokinetic-pharmacodynamic modeling of the respiratory-depressant effect of buprenorphine and fentanyl in rats." J Pharmacol Exp Ther 319(2): 682-692.
Modelling and Simulation Group, School of Pharmacy
Why is this important
• Besides dosage other relevant clinical questions remain to be answered with science rather than anecdote
– When should it start to work– When is it safe to re-dose

Modelling and Simulation Group, School of Pharmacy
How we will determine the parameters of interest
• Population PK/PD modelling allows:– Optimal design data– Estimation of variability and affect of
covariates– Allows “what if” experiments to be completed
in silico
Modelling and Simulation Group, School of Pharmacy
AIMS
• What we hope to achieve
Modelling and Simulation Group, School of Pharmacy
AIM 1
• Determine if varying techniques for the preparation and administration of intranasal fentanyl effect the amount of drug delivered
Modelling and Simulation Group, School of Pharmacy
AIM 2
• Using optimal design methodologies, design a trial protocol to study the population pharmacokinetics of intranasal fentanyl in paediatric patients
Modelling and Simulation Group, School of Pharmacy
AIM 3 + 4
• Determine the most appropriate model to describe the relationship between administered dose of intranasal fentanyl and observed blood concentration in paediatric patients.
• Determine the most appropriate model to describe the relationship between blood concentration of fentanyl and pain score after administration of intranasal fentanyl to the paediatric population.
Modelling and Simulation Group, School of Pharmacy
AIM 5
• Perform simulations to answer clinically relevant questions for the treatment of acute or procedural pain in paediatric patients by INF
Modelling and Simulation Group, School of Pharmacy
Results so far
• For statistical optimisation of a trial design we must have some idea of the underlying model– Problem!!!
• No studies report the pharmacokinetics of INF in children
Modelling and Simulation Group, School of Pharmacy
Results so far
• However we do have • Adult INF studies
• Expolate using a linear relationship between weight and dose
Modelling and Simulation Group, School of Pharmacy
How do we use adult data
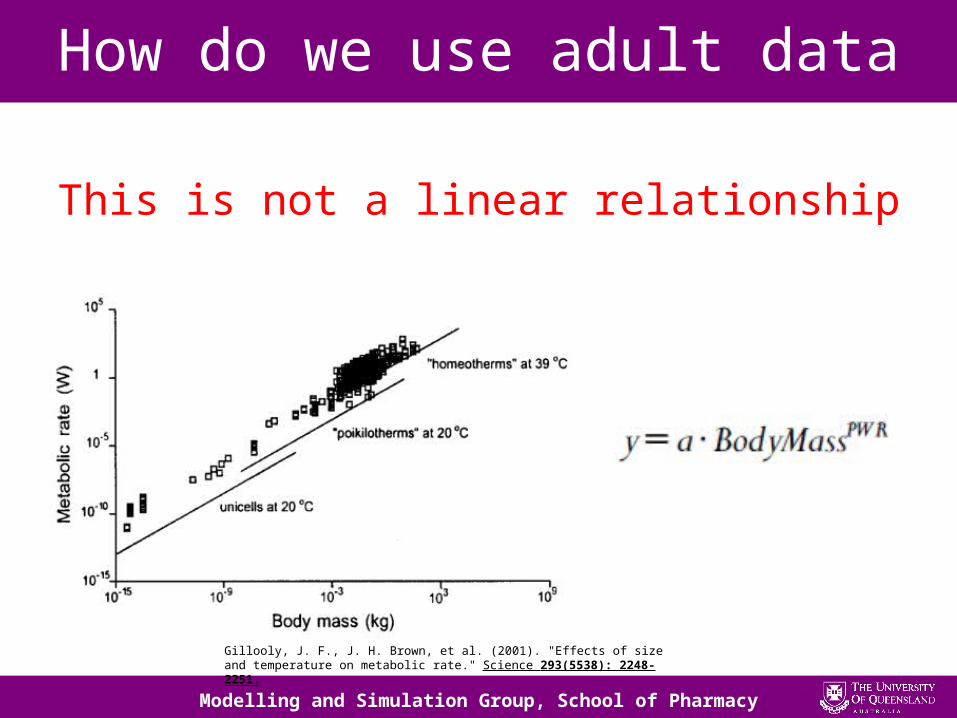
This is not a linear relationship
Gillooly, J. F., J. H. Brown, et al. (2001). "Effects of size and temperature on metabolic rate." Science 293(5538): 2248-2251.
Modelling and Simulation Group, School of Pharmacy
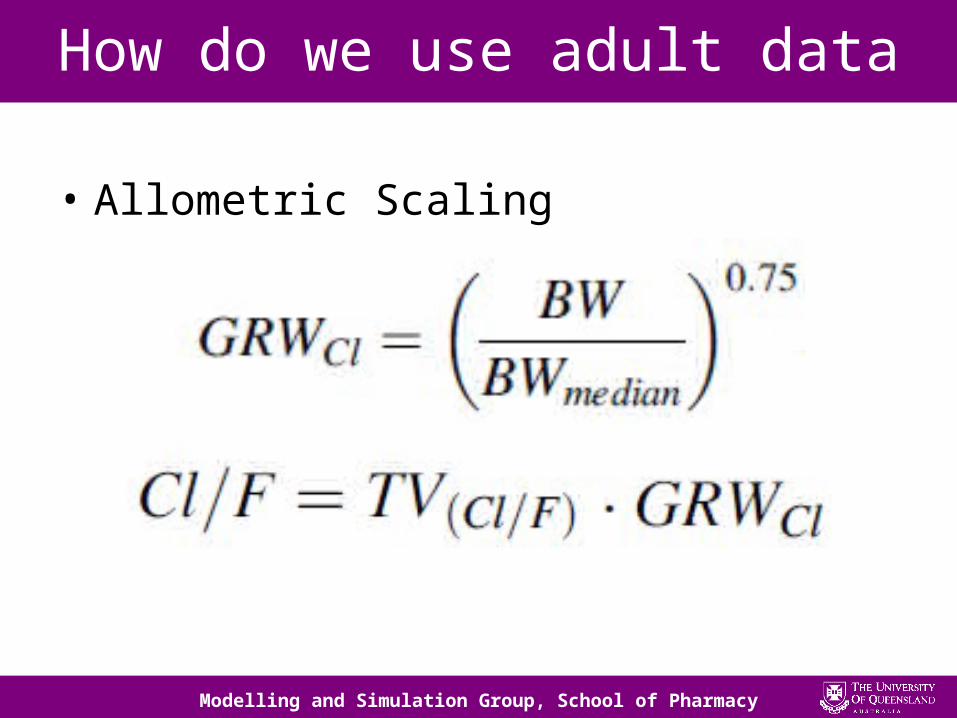
How do we use adult data
• Allometric Scaling
Modelling and Simulation Group, School of Pharmacy
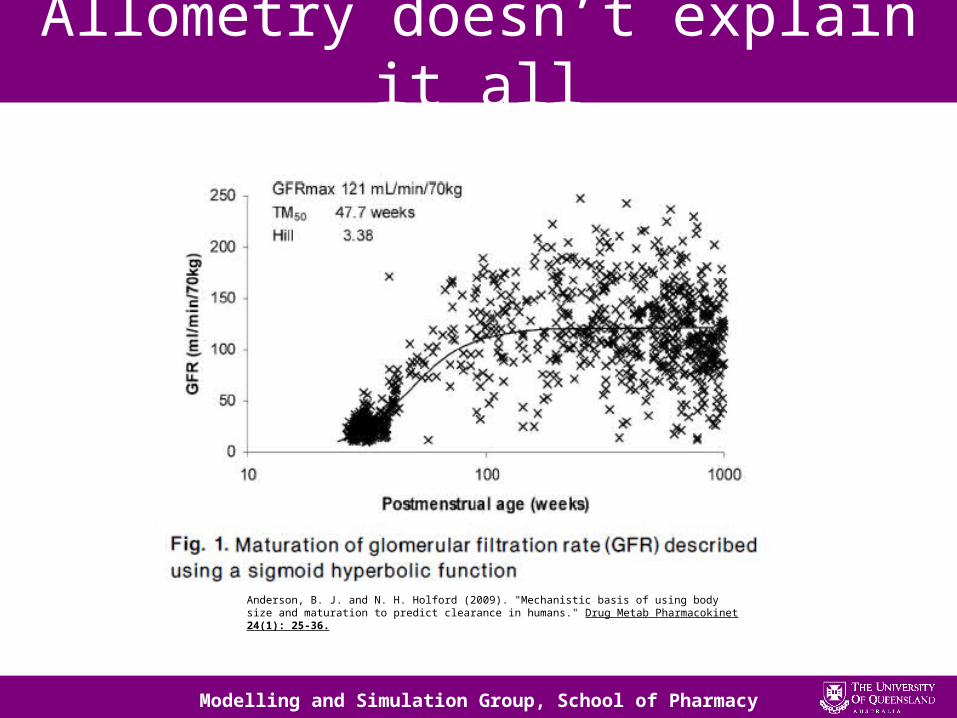
Allometry doesn’t explain it all
Anderson, B. J. and N. H. Holford (2009). "Mechanistic basis of using body size and maturation to predict clearance in humans." Drug Metab Pharmacokinet 24(1): 25-36.
Modelling and Simulation Group, School of Pharmacy
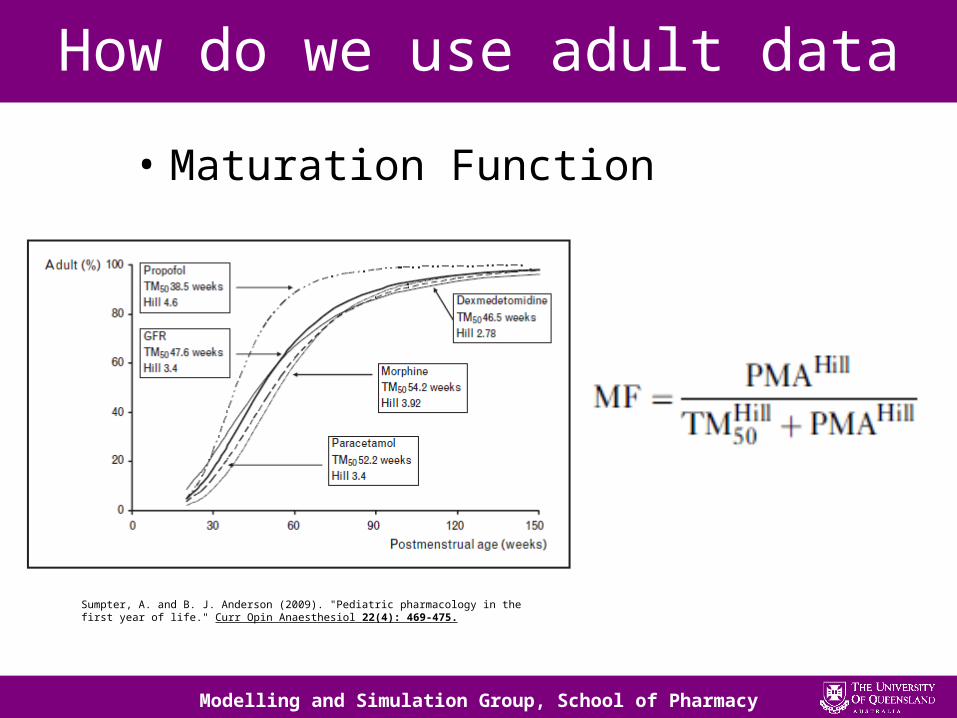
How do we use adult data
• Maturation Function
Sumpter, A. and B. J. Anderson (2009). "Pediatric pharmacology in the first year of life." Curr Opin Anaesthesiol 22(4): 469-475.
Modelling and Simulation Group, School of Pharmacy
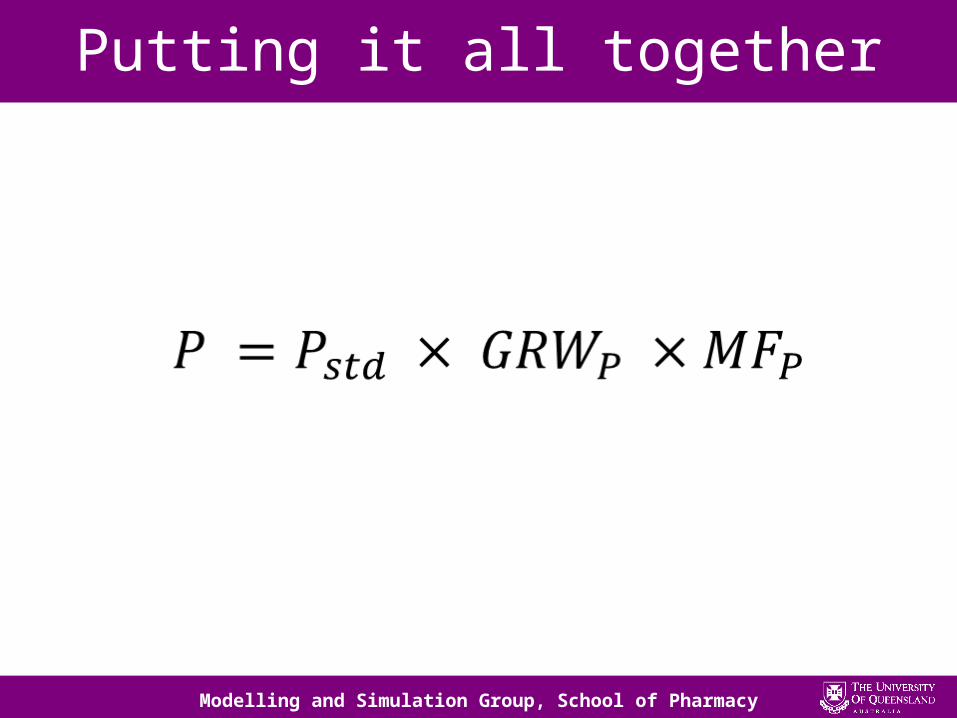
Putting it all together
Modelling and Simulation Group, School of Pharmacy
Sampling times and windows
• Run competing maturation models and varying allometric exponents for varying age.Database of different sampling times for
different ages
Do the sampling windows overlap???
Modelling and Simulation Group, School of Pharmacy
Other significant milestones
• Review paper of Transmucosal opiates in paediatrics in progress
• Competency in Assay Technique LC MS/MS
Modelling and Simulation Group, School of Pharmacy
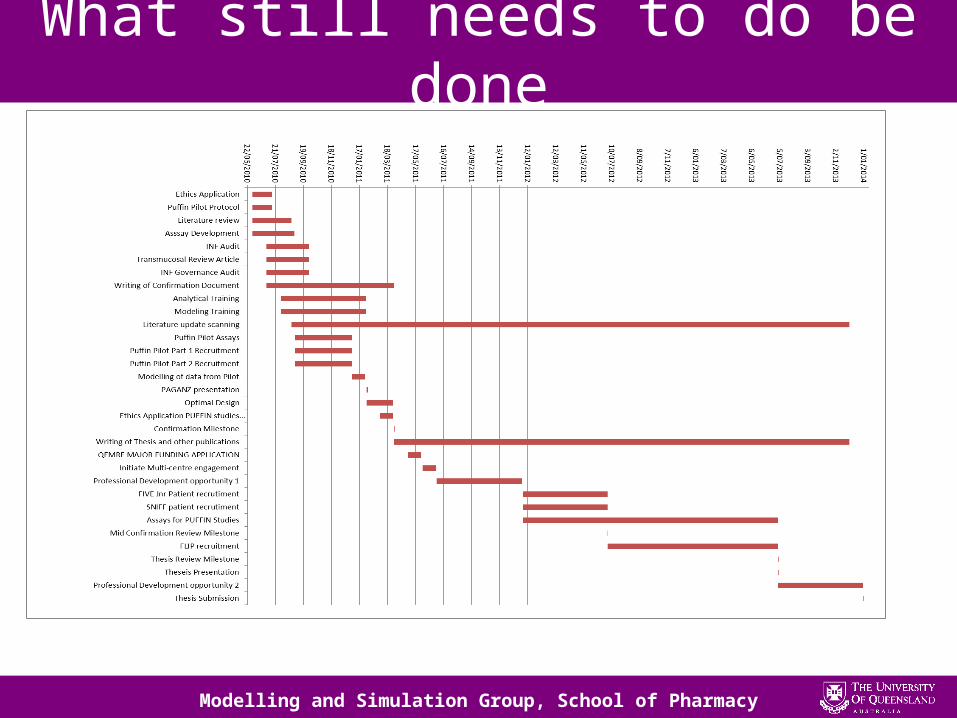
What still needs to do be done
Modelling and Simulation Group, School of Pharmacy
Acknowledgements
• Supervisors
• ACPP Laboratory staff
• Mater Children’s Emergency Department
• QUM and Medical Students
• QEMRF
• Modelling and simulation group members
Modelling and Simulation Group, School of Pharmacy
QUESTIONS
?

Modelling and Simulation Group, School of Pharmacy