Embed Size (px)
Citation preview

Journal of Plastic, Reconstructive & Aesthetic Surgery (2011) 64, 693e702
CORRESPONDENCE AND COMMUNICATIONS
Modified Fogli temporal lift*
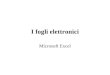
Figure 1 Spinal needle introduced above the eyebrow anddelivered into the incision site.
Elevation of the ptotic brow is an integral part of rejuve-nation of the upper third of the face. Many methods havebeen described from the direct excision of a skin ellipsefrom the forehead to the mobilisation of the forehead ina cephalic direction accessed though a coronal, endo-scopic, transblepharoplasty or combination of some or all ofthese incisions.
Fogli described an efficient and simple temporal lifttechnique that uses galeapexy to address the ptotic tail ofthe brow and crow’s feet.1 His approach consists ofa temporal incision 3 cm behind the hairline, followed bysubgaleal dissection and then a subcutaneous dissectionthat allows the freed, lifted cephalic galea, previouslyincised, to be anchored directly to the temporal aponeu-rosis. This cutaneous redraping raises the brow tail anda detachment of the orbicularis fibres. Suturing of the scalpis hence achieved without tension, without eliminating hairand prevents backward displacement of the hairline.
The senior author has modified Fogli’s lifting and fixationtechnique to achieve a more accurate lift of the mid-lateraleyebrow.
� The incision is, 3e5 cm in length, and it is made in thefronto-temporal scalp just behind the hairline (1 cmabove).
� The dissection proceeds in the subgaleal and thensubcutaneous planes as described by Fogli.
� A 6” 20G yellow spinal needle is then introduced just atthe mid-lateral eyebrow at the point where lifting isdeemed to be required to achieve an aestheticallypleasing eyebrow2 into the dissected subcutaneousplane and delivered out through the subgaleal planeinto the incision site (Figure 1).
� The thread end of a 4-0 monofilament, polydioxone(PDS), suture is then passed through the hollow spinalneedle at the sharp end to emerge out of the yellowhub. An appropriate length of suture is pulled throughand an artery clip is placed at the cephalic end of thesuture to prevent it from being pulled throughcompletely.
* This paper was presented in the 2nd Eurasian InternationalAesthetic Surgery Course (ISAPS), Istanbul, Turkey, 17-20 June 2010and 13th Turkish Society of Aesthetic Plastic Surgery Congress &ISAPS Course Istanbul, Turkey, 19-22 June 2009.
� The spinal needle is then pulled out until the tip iswithin the dermis (not being removed from the skin)and reinserted a couple of millimeters adjacent to theoriginal insertion site catching a small area of dermisand again delivered through the incision site as before.
� The PDS suture end is then pulled out of the sharp endof the spinal needle so that the suture is looped around
Figure 2 Subcutaneous suture (shown as green line) loopedthough dermis of upper eyebrow. Red arrow is pointing towardsthe suture being pulled outside of the skin.

Figure 3 Immediate postoperative view (bilateral upperblepharoplasty also performed).
694 Correspondence and communications
the dermis of the eyebrow and then pulled upwards toachieve a lift of the mid-lateral eyebrow (Figure 2).This is repeated at another point on the eyebrow ifnecessary.
� Tension on the suture is adjusted before fixing it to thefronto-temporal periosteum. The previously incised
Figure 4 (a,b) e Pre operative views of traumatic frontalnerve palsy resulting right brow ptosis.
Figure 5 (a,b) e 2 years post operative results showingeffectiveness of the technique.
galea is then anchored to the temporal aponeurosis asdescribed by Fogli.
� There is some overlap of the galea which is visible onthe upper forehead but this settles well over time(Figure 3).
This modification of Fogli’s brow lift method allows moreaccurate and effective (elastic band principle3) elevation ofthe mid-lateral eyebrow. This method has been used by thesenior author in over 50 patients over the last 5 years withgood long term results (Figure 4a, b, 5a, b).
Conflict of interest statement
None of the authors have any conflicts of interest in theform of financial or personal relationships with otherpeople or organizations that could inappropriately influ-ence (bias) this work as detailed in the JPRAS authorsinstructions.
References
1. Fogli AL. Temporal lift by galeapexy: a review of 270 cases.Aesth Plast Surg 2003;27:159e65.
2. Ellenbogen R. Transcoronal eyebrow lift with concomitant upperblepharoplasty. Plast Reconst Surg 1983;71:490.

Correspondence and communications 695
3. Flowers RS, Caputy GG, Flowers SS. The biomechanics of browand frontalis function and its effect on blepharoplasty. ClinPlast Surg 1993;20(2):255e68.
E. ErelM. Wong
D. ChesterV. Vijh
Burns and Plastic Surgery Department, University HospitalsBirmingham NHS Foundation Trust,
Queen Elizabeth Hospital Birmingham, Mindelsohn Way,Edgbaston, Birmingham B15 2WB, UK
E-mail address: [email protected]
ª 2010 British Association of Plastic, Reconstructive and AestheticSurgeons. Published by Elsevier Ltd. All rights reserved.
doi:10.1016/j.bjps.2010.09.018
Preoperative assessment of softtissue deficiency in the temporalregion with reverse engineering
Sir,
Temporal hollowing often occurs after brain surgery andcraniofacial surgery, and this deformity is a source ofcosmetic concern to patients. Therefore, augmentationsurgery is often requested.
Figure 1 The original and mirror-reversed data were synthesizepatch of the defect was created, and the volume of the patch wa
Various methods have been reported to augment thetemporal hollowing. Among them, hydroxyapatite cementpaste has the great advantage of easy molding duringsurgery.1 However, it is sometimes difficult to decide wherethe cement paste should be placed and how muchaugmentation should be performed in the operating room.If the precise volume and regions with defects can beestimated preoperatively, this information can be used toguide the surgeon.
Patient and methods
A 44-year-old woman had subarachnoid hemorrhage 4 yearsago. At the neurosurgery department of another hospital,clipping surgery was performed in the approach throughthe temporal region. The patient had temporal hollowingafter the surgery. Therefore, we planned preoperativeassessment of soft tissue deficiency with reverseengineering.
First, computed tomography (CT) scan was performed by64-slice multidetector-row computed tomography(Discovery CT750HD; GE Medical Systems, Waukesha, WI).Axial slices at 0.625-mm intervals were used for the simula-tion. Volume rendering was performed with the CT valuebelow the fat value and stereolithography (STL) data bearingskin surface information was created with DICOM manager(INTAGE Volume Editor; KGT Inc., Tokyo, Japan).2, 3
The STL data were transferred to the reverse engi-neering software (Rapidform XOS2 SP1; INUS Technology,Seoul, Korea) to repair poorly scanned data and togenerate mirror-reversed data. Then, the original dataand the mirror-reversed data were synthesized (Figure 1).
d and the deviation was visualized as a color map. Then, thes calculated.