Embed Size (px)
Citation preview

Modulation of RANKL and OsteoprotegerinExpression in Synovial Tissue From Patients WithRheumatoid Arthritis in Response to Disease-Modifying Antirheumatic Drug Treatment andCorrelation With Radiologic OutcomeDAVID HAYNES,1 TANIA CROTTI,1 HELEN WEEDON,2 JOHN SLAVOTINEK,3 VIRGINIA AU,3
MARK COLEMAN,3 PETER J. ROBERTS-THOMSON,3 MICHAEL AHERN,2 AND MALCOLM D. SMITH4
Objective. To demonstrate the effect of treatment with disease-modifying agents on the expression of osteoprotegerin(OPG) and RANKL in the synovial tissue from rheumatoid arthritis (RA) patients and to correlate these changes withradiologic damage measured on sequential radiographs of the hands and feet.Methods. Synovial biopsy specimens were obtained at arthroscopy from 25 patients with active RA (16 of whom had adisease duration <12 months) before and at 3–6-month intervals after starting treatment with a disease-modifying agent.Immunohistologic analysis was performed using monoclonal antibodies to detect OPG and RANKL expression, withstaining quantitated using computer-assisted image analysis and semiquantitative analysis techniques. Serial radio-graphs of the hands and feet were analyzed independently by 2 radiologists and a rheumatologist using the van der Heidemodification of the Sharp scoring method.Results. Thirteen patients achieved a low disease state as defined by a disease activity score <2.6 while 19 patientsachieved an American College of Rheumatology response >20% after disease-modifying antirheumatic drug (DMARD)treatment. Successful DMARD treatment resulted in an increase in OPG expression and a decrease in RANKL expressionat the synovial tissue level, which correlated with a reduction in erosion scores measured on annual radiographs of thehands and feet.Conclusion. Successful treatment-induced modulation of OPG and RANKL expression at the synovial tissue level,resulting in a reduction in the RANKL:OPG ratio, is likely to have a significant impact on osteoclast formation and jointdamage in patients with active RA.
INTRODUCTION
Rheumatoid arthritis (RA) is characterized by inflamma-tion of the synovial membrane leading to invasion of sy-novial tissue into the adjacent cartilage matrix with deg-radation of articular cartilage and bone as a consequence.This results in erosion of bone, which is often observed as
marginal joint erosions radiographically and is predictiveof a poorer prognosis (1). Although the pathophysiologicmechanisms for cartilage and bone destruction in RA arenot yet completely understood, it is known that matrixmetalloproteinases, cathepsins, and mast cell proteinasescan contribute to cartilage and bone destruction in RA(2–4). However, it is now clear that osteoclast formation
Supported by grants from the National Health and Medi-cal Research Council of Australia, the Clive and Vera Ra-maciotti Foundation, the J. H. and J. D. Gunn Foundation,and the Rebecca L. Cooper Medical Research Foundation.
1David Haynes, PhD, Tania Crotti, BHlthSci, PhD: Univer-sity of Adelaide, Adelaide, South Australia, Australia;2Helen Weedon, BSc, Michael Ahern, MBBS, PhD, FRACP:Repatriation General Hospital, Daw Park, Adelaide, SouthAustralia, Australia; 3John Slavotinek, MBBS, FRANZCR,Virginia Au, MBBS, FACR, FRANZCR, Mark Coleman,MBBS, FRCPA, Peter J. Roberts-Thomson, DPhil(Oxon),
FRACP: Flinders Medical Centre, Adelaide, South Aus-tralia, Australia; 4Malcolm D. Smith, MBBS(Hons), PhD,FRACP: Flinders Medical Centre and Repatriation GeneralHospital, Adelaide, South Australia, Australia.
Address correspondence to Malcolm D. Smith,MBBS(Hons), PhD, FRACP, Rheumatology Research Unit,Repatriation General Hospital, Daws Road, Daw Park,SouthAustralia,5041Australia.E-mail:[email protected].
Submitted for publication September 18, 2007; acceptedin revised form February 19, 2008.
Arthritis & Rheumatism (Arthritis Care & Research)Vol. 59, No. 7, July 15, 2008, pp 911–920DOI 10.1002/art.23818© 2008, American College of Rheumatology
ORIGINAL ARTICLE
911

and activation at the cartilage–pannus junction is an es-sential step in the destruction of bone matrix in patientswith RA (5–8). A number of inflammatory cytokines foundin the synovial tissue of patients with RA (interleukin-1�[IL-1�] and IL-1�, IL-6, tumor necrosis factor �, macro-phage colony-stimulating factor [M-CSF]) have the poten-tial to promote osteoclast formation and bone resorption(9–11). However, recent evidence indicates that the inter-action between RANKL and RANK has an essential role inosteoclastogenesis (5,6,12,13). RANKL is expressed on os-teoblasts, fibroblasts, and T cells, whereas RANK is mainlyexpressed on preosteoclasts, possibly of macrophage lin-eage. There is a naturally occurring inhibitor of theRANKL interaction with RANK, called osteoprotegerin(OPG), which binds RANKL with high affinity, preventingRANKL from interacting with RANK (14).
We have previously published reports on the expressionof both RANKL (15) and OPG (16) in the synovial tissue ofpatients with inflammatory arthritis and osteoarthritis aswell as normal synovial tissue (17) and demonstrated alack of OPG expression with significant RANKL expres-sion in the synovial tissue from patients with active RA.We hypothesized that successful treatment with disease-modifying antirheumatic drugs (DMARDs) would reduceRANKL expression and increase OPG expression, alteringthe RANKL:OPG ratio and suppressing osteoclast forma-tion in the synovial tissue of patients with RA. The goal ofthe present study was to test this hypothesis in a cohort ofRA patients with active disease initiating DMARD treat-ment and to attempt to correlate the changes in synovialtissue expression of RANKL and OPG with radiologic out-comes in this patient cohort.
PATIENTS AND METHODS
Patients. Twenty-five RA patients with active synovitis,including an involved knee joint, were recruited for thestudy. All RA patients fulfilled the American College ofRheumatology (ACR; formerly the American RheumatismAssociation) criteria for RA (18). The mean age of thepatient group was 68.4 years (range 47–87 years) with 14men and 11 women. Eighteen of the 25 patients wereseropositive for rheumatoid factor, while 2 of the 7 sero-negative patients had radiologic evidence of erosions atstudy entry. The mean disease duration was 4.3 years(range 0.1–24 years); 16 patients had a disease duration �1year. Decisions about which DMARD to use to treat anindividual patient were made by the treating rheumatolo-gist and were not influenced by participation in this study.DMARDs used included methotrexate (6 patients), intra-muscular (IM) gold (6 patients), methotrexate and IM gold(9 patients), sulfasalazine (2 patients), cyclosporin A (1patient), and hydroxychloroquine (1 patient). No anti–tumor necrosis factor (anti-TNF) agents were used to treatthis patient group because the study preceded the generalavailability of these therapeutic agents in Australia. Fail-ure to respond to treatment with the original DMARDalong with clear evidence of radiologic progression led towithdrawal from the study. All patients were followed upat regular intervals (3–6 months) for clinical (tender and
swollen joint counts, visual analog scales for pain, patientand physician global assessments, and a modified HealthAssessment Questionnaire [HAQ]), laboratory (C-reactiveprotein, erythrocyte sedimentation rate, and rheumatoidfactor), and radiologic (radiographs of the hands and feettaken annually) parameters. Response to DMARD treat-ment was assessed by calculating a disease activity scorein 28 joints (DAS28) (19) and ACR response (20). Allpatients gave informed consent, and the study protocolwas approved by the research and ethics committee of theRepatriation General Hospital.
Synovial tissue. A small-bore arthroscopy (2.7-mm ar-throscope; Dyonics, Andover, MA) was performed withpatients under local anesthesia as previously described(21) at baseline and at 3, 6, 12, 18, 24, and 36 months afterstarting DMARD treatment. Biopsy specimens of synovialtissue were obtained from all accessible regions of the kneejoint, but mainly from the suprapatellar pouch. The sam-ples were separately snap-frozen in Tissue-Tek OCT(Miles Diagnostics, Elkhart, IN) and stored at �80°C untilused. Cryostat sections (6 �m) were mounted on glassslides (Superior Marienfeld, Baden-Wurttemberg, Ger-many). The glass slides were boxed and stored at �20°Cuntil immunohistologic analysis.
Immunohistochemistry. Serial sections were stainedwith the following mouse monoclonal antibodies (mAb):anti-human OPG antibodies (mAb 805 and mAb 8051;R&D Systems, Minneapolis, MN); anti-human TRANCE(mAb 626; R&D Systems); anti-CD68 (clone EBM11; DakoAustralia, Botany Bay, New South Wales, Australia) todetect macrophages; mAb 67 (Serotec, Kidlington, Oxford,UK), which recognizes CD55, to detect fibroblast-like sy-noviocytes; anti-CD3 (BD Biosciences, San Jose, CA) andanti-CD45RO to detect T cells and memory T cells, respec-tively; anti-CD22 (Central Laboratory of the NetherlandsRed Cross Blood Transfusion Service, Amsterdam, TheNetherlands) to detect B cells; anti-CD38 (BD Biosciences)to detect plasma cells; and anti–granzyme B (Novo CastraLaboratories, Newcastle upon Tyne, UK). Endogenous per-oxidase activity was inhibited using 0.1% sodium azideand 1% hydrogen peroxide in Tris–phosphate bufferedsaline. Staining for cell markers was performed as de-scribed previously (15–17). Following a primary step ofincubation with mAb, bound antibody was detected ac-cording to a 3-step immunoperoxidase method. Horserad-ish peroxidase (HRP) activity was detected using hydrogenperoxide as substrate and aminoethylcarbazole (AEC) asdye. Slides were counterstained briefly with hematoxylinsolution and mounted in Gurr Aquamount (BDH, Poole,UK). Affinity-purified HRP-conjugated goat anti-mouseantibody was obtained from Dako, affinity-purified HRP-conjugated swine anti-goat Ig from Tago (Burlingame, CA),and AEC from Sigma (St. Louis, MO). The specificity of theantibodies against RANKL (15) and OPG (16) has previ-ously been demonstrated by absorption studies using pu-rified RANKL and OPG.
912 Haynes et al

Quantitation of immunohistochemical labeling. Afterimmunohistochemical staining, sections stained for OPG(mAb 805 and 8051) and RANKL were analyzed in a ran-dom order by computer-assisted image analysis, analyzing6 high-power fields for each section as previously de-scribed (22,23). In addition, these sections were scored bya semiquantitative method on a 5-point scale by 2 inde-pendent observers in a random order, as described previ-ously (15,16,24).
Real-time polymerase chain reaction on synovial tis-sue. Complementary DNA (cDNA) samples were preparedfrom synovial biopsy specimens from 5 RA patients usingthe initial synovial tissue obtained before starting DMARDtreatment and again using the biopsy specimens obtainedwhen there was significant improvement in disease activ-ity as defined by the DAS28. As controls for these patients,cDNA was prepared from synovial tissue obtained at ar-throscopic biopsy in 5 patients with osteoarthritis of theknee joint. Real-time polymerase chain reaction (PCR) wasperformed using Platinum SYBR Green quantitative PCRSupermix-UDG (Invitrogen Life Technologies, San Diego,CA) as per the manufacturer’s recommendations. Amplifi-cation was carried out in a Rotor-Gene 3000 (Corbett LifeScience, Mortlake, New South Wales, Australia) withSYBR Green detection and melt curve analysis. Oligonu-cleotide primers that were used have been described pre-viously, and are specific for OPG and RANKL (25). Theendogenous reference gene hARP (26) was used to normal-ize threshold cycle (Ct) data obtained from the genes in-vestigated. Reaction mixtures contained 1 �l of 1:5 dilutedcDNA, 7.5 �l Platinum SYBR Green quantitative PCR Su-permix-UDG, 300 nM each of forward and reverse primer,and diethyl pyrocarbonate–treated water to a final volumeof 15 �l. All samples were investigated in triplicate andthe melting curves obtained after each PCR amplificationconfirmed the specificity of the SYBR Green assays. Opti-mization of forward and reverse primer concentrationsbetween 50 nM and 900 nM was evaluated to obtain thecombination of primers with the lowest Ct value. For eachtarget gene (OPG and RANKL) and endogenous referencegene (hARP), a concentration of 300 nM of both forwardand reverse primers yielded the lowest Ct values, with thehighest increase in fluorescence. Validation experimentswere performed to demonstrate that amplification efficien-cies of the target genes and the endogenous reference genewere approximately equal. Complementary DNA was pre-pared from pooled RNA samples and diluted in a 2-folddilution series over 6 orders of magnitude. Target andreference genes were then amplified in separate tubes us-ing this cDNA dilution series and Ct were values obtained.The difference in Ct (�Ct) for each sample was then calcu-lated as outlined below and data were plotted against thelog cDNA dilution. If the absolute value of the slope is�0.1, the efficiencies of the target and reference genes aresimilar, and the ��Ct calculation for the relative quantifi-cation of target may be used (27). The slope for OPG hARPwas 0.078 and for RANKL hARP was 0.0125. Relativeexpression of the target genes in the studied samples wasobtained using the difference in the Ct (��Ct) method.Briefly, for each sample, a value for threshold (Ct) was
determined, defined as the mean cycle at which the fluo-rescence curve reached an arbitrary threshold. The �Ct foreach sample was then calculated according to the formulaCt target gene � Ct hARP; ��Ct values were then obtainedby subtracting the �Ct of a reference sample (the average�Ct for osteoarthritis samples) from the �Ct of the studiedsamples. Finally, the levels of expression of the targetgenes in the studied samples as compared with the refer-ence sample were calculated as 2���Ct.
Grading of serial radiographs. Radiographs of thehands and feet were obtained for all patients included inthis study �12 months apart for the duration of the studyusing a standard technique. The radiographs were gradedby 2 radiologists and a rheumatologist, using the van derHeide modification of the Sharp technique (28), after firststandardizing against each other using a series of hand andfeet radiographs from 4 RA patients not included in thisstudy. The radiographs were graded separately by the 3assessors without knowledge of the clinical outcome, butwith knowledge of the timing of the radiographs. Thescoring system results in a maximum score of 210 for jointspace narrowing and 280 for erosions. A disagreementbetween scorers of up to 5% of the maximum score wasallowed, with the final score being an average of the 3scores. Any disagreement above this level was settled byconsensus, with all 3 assessors scoring all radiographs fora single patient together in the same session. This wasnecessary for 4 of the 25 patients included in this study.
Statistical analysis. Results are presented as themean � SD. Tests for normality were applied to the data.Semiquantitative scores were treated as nonparametricdata. Data generated by computer-assisted digital imageanalysis (integrated optical density [IOD]) were generallynormally distributed. Changes within the groups were an-alyzed using Wilcoxon’s signed rank test for data that werenot normally distributed (semiquantitative scores) andStudent’s paired t-test for normally distributed continuousdata (IOD). Separate linear regressions of each parameterversus time in months were performed. To account for thecorrelation between repeated observations on the samepatient in the analyses, generalized estimating equations,assuming an exchangeable correlation structure, wereused in the regressions. The analyses were also carried outfor the differenced data, in which the first synovial biopsyresult was subtracted from each subsequent synovial bi-opsy result for each of the variables.
RESULTS
Clinical and demographic features. All patients in-cluded in this study had active RA, with a mean tenderjoint count of 17.7 (range 5–26), mean swollen joint countof 13.8 (range 3–27), mean modified HAQ score of 2.3(range 1.3–3.0), and mean DAS28 of 5.9 (range 4.4–7).There was a significant decrease in DAS28 with treatment(P � 0.000). Thirteen patients attained a low disease ac-tivity state as defined by a DAS28 score �2.6 following
RANKL and OPG in RA Synovial Tissue 913
DMARD treatment. Nineteen patients attained a significantACR response to treatment, defined as a �20% ACR re-sponse to treatment, but 6 of these patients did not achievea low disease activity score as defined by a DAS28 �2.6.
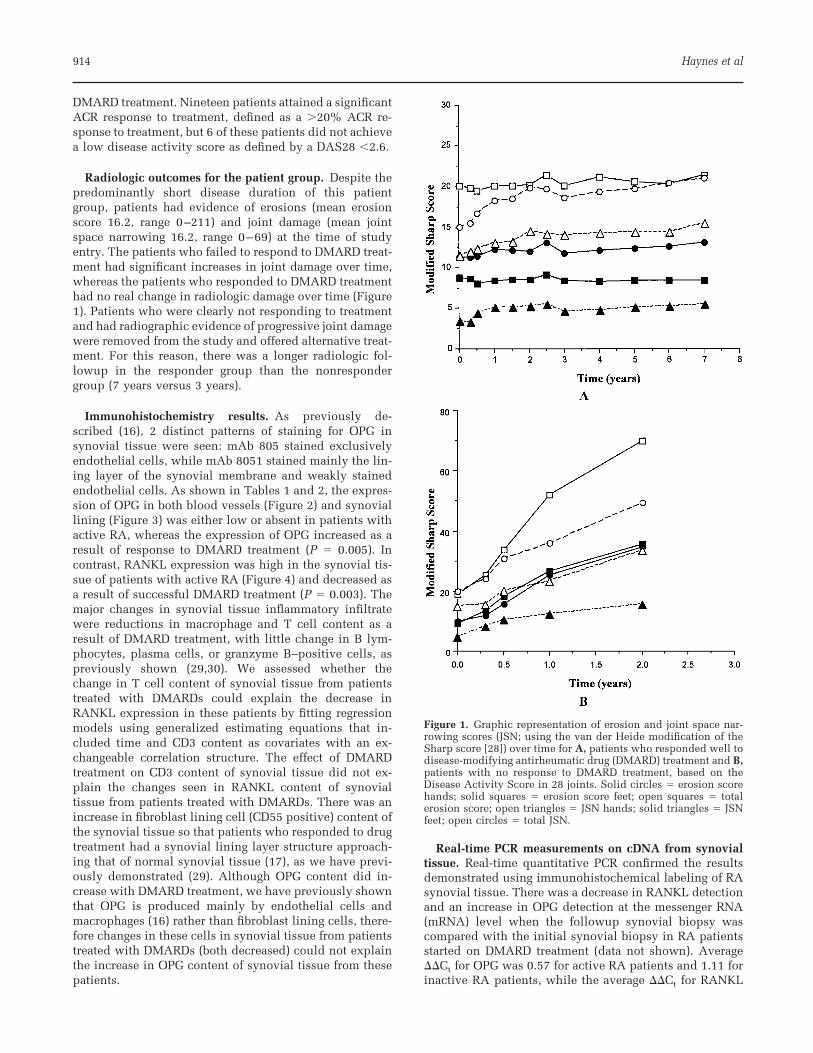
Radiologic outcomes for the patient group. Despite thepredominantly short disease duration of this patientgroup, patients had evidence of erosions (mean erosionscore 16.2, range 0–211) and joint damage (mean jointspace narrowing 16.2, range 0–69) at the time of studyentry. The patients who failed to respond to DMARD treat-ment had significant increases in joint damage over time,whereas the patients who responded to DMARD treatmenthad no real change in radiologic damage over time (Figure1). Patients who were clearly not responding to treatmentand had radiographic evidence of progressive joint damagewere removed from the study and offered alternative treat-ment. For this reason, there was a longer radiologic fol-lowup in the responder group than the nonrespondergroup (7 years versus 3 years).
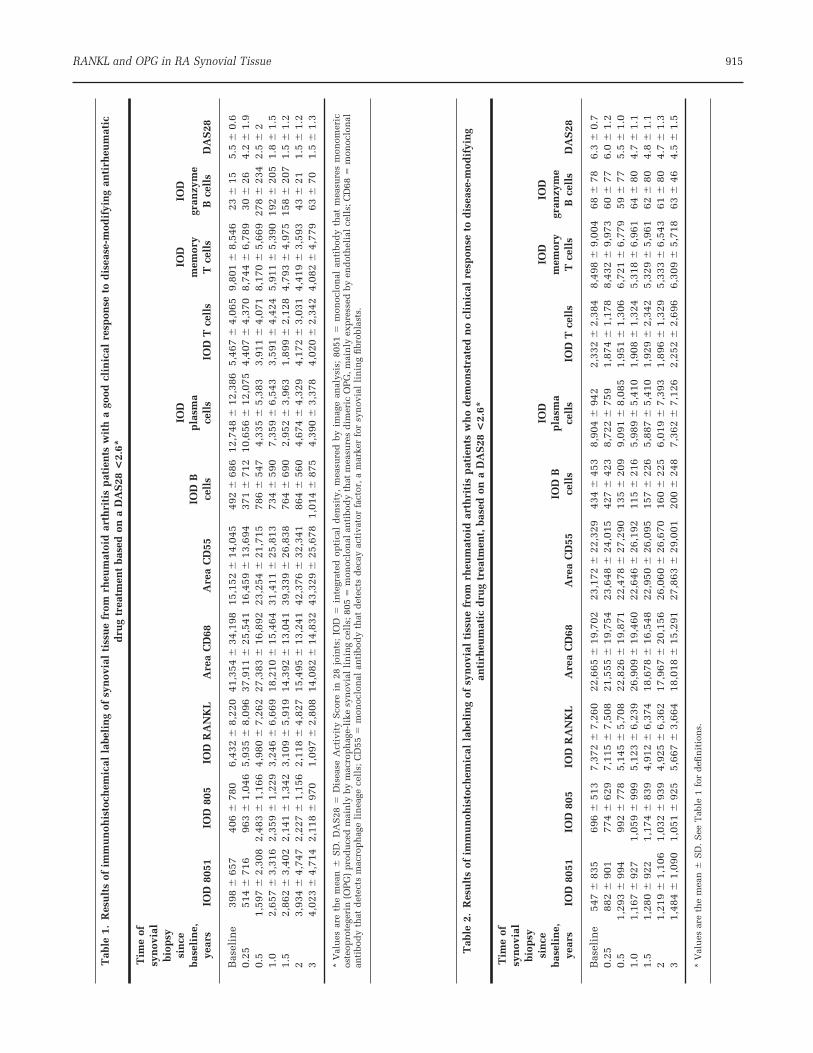
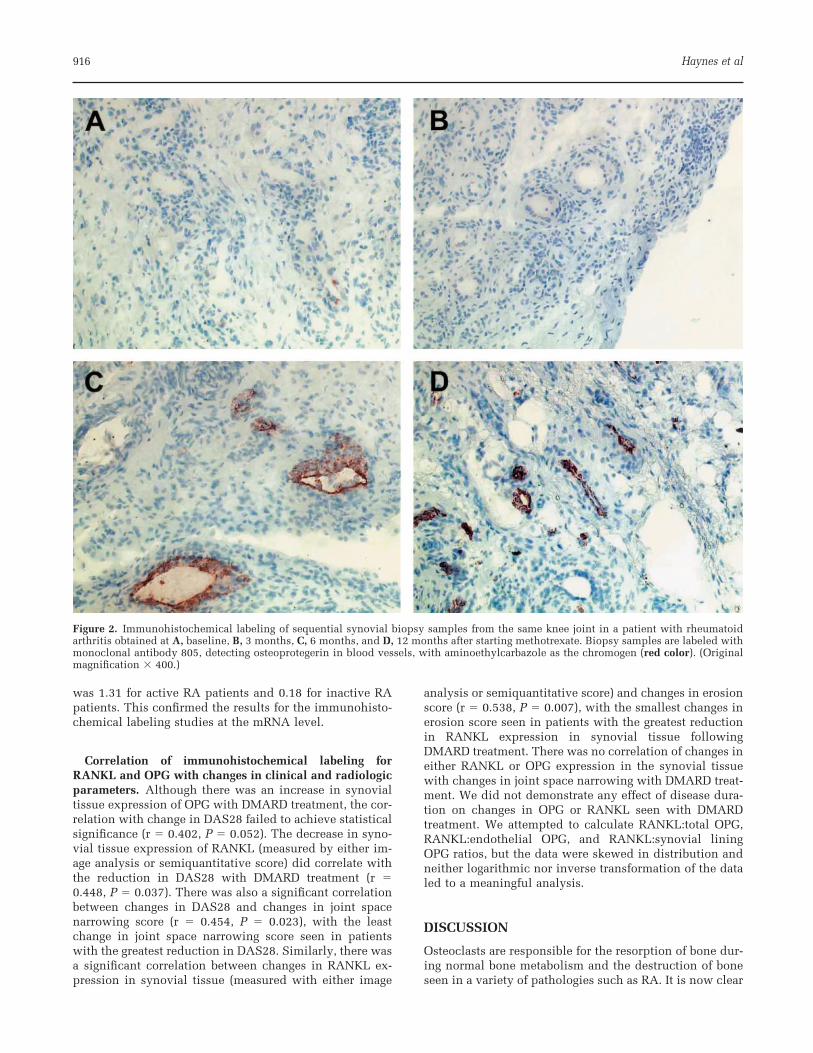
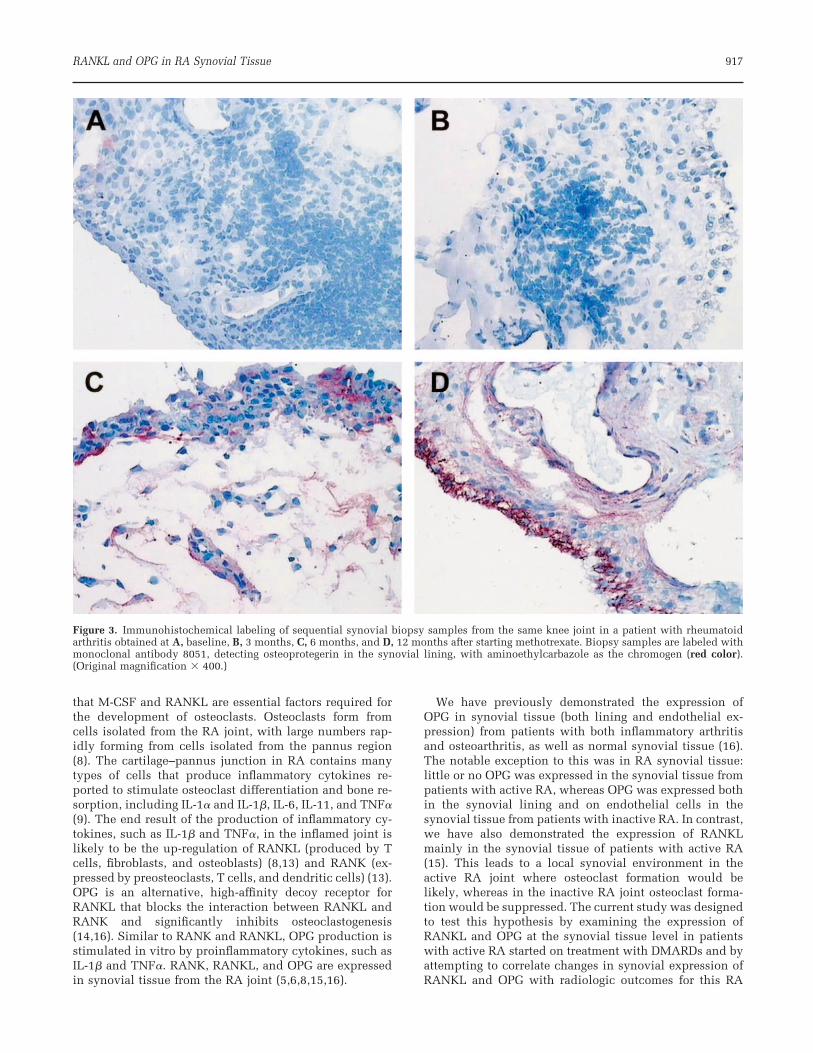
Immunohistochemistry results. As previously de-scribed (16), 2 distinct patterns of staining for OPG insynovial tissue were seen: mAb 805 stained exclusivelyendothelial cells, while mAb 8051 stained mainly the lin-ing layer of the synovial membrane and weakly stainedendothelial cells. As shown in Tables 1 and 2, the expres-sion of OPG in both blood vessels (Figure 2) and synoviallining (Figure 3) was either low or absent in patients withactive RA, whereas the expression of OPG increased as aresult of response to DMARD treatment (P � 0.005). Incontrast, RANKL expression was high in the synovial tis-sue of patients with active RA (Figure 4) and decreased asa result of successful DMARD treatment (P � 0.003). Themajor changes in synovial tissue inflammatory infiltratewere reductions in macrophage and T cell content as aresult of DMARD treatment, with little change in B lym-phocytes, plasma cells, or granzyme B–positive cells, aspreviously shown (29,30). We assessed whether thechange in T cell content of synovial tissue from patientstreated with DMARDs could explain the decrease inRANKL expression in these patients by fitting regressionmodels using generalized estimating equations that in-cluded time and CD3 content as covariates with an ex-changeable correlation structure. The effect of DMARDtreatment on CD3 content of synovial tissue did not ex-plain the changes seen in RANKL content of synovialtissue from patients treated with DMARDs. There was anincrease in fibroblast lining cell (CD55 positive) content ofthe synovial tissue so that patients who responded to drugtreatment had a synovial lining layer structure approach-ing that of normal synovial tissue (17), as we have previ-ously demonstrated (29). Although OPG content did in-crease with DMARD treatment, we have previously shownthat OPG is produced mainly by endothelial cells andmacrophages (16) rather than fibroblast lining cells, there-fore changes in these cells in synovial tissue from patientstreated with DMARDs (both decreased) could not explainthe increase in OPG content of synovial tissue from thesepatients.
Real-time PCR measurements on cDNA from synovialtissue. Real-time quantitative PCR confirmed the resultsdemonstrated using immunohistochemical labeling of RAsynovial tissue. There was a decrease in RANKL detectionand an increase in OPG detection at the messenger RNA(mRNA) level when the followup synovial biopsy wascompared with the initial synovial biopsy in RA patientsstarted on DMARD treatment (data not shown). Average��Ct for OPG was 0.57 for active RA patients and 1.11 forinactive RA patients, while the average ��Ct for RANKL
Figure 1. Graphic representation of erosion and joint space nar-rowing scores (JSN; using the van der Heide modification of theSharp score [28]) over time for A, patients who responded well todisease-modifying antirheumatic drug (DMARD) treatment and B,patients with no response to DMARD treatment, based on theDisease Activity Score in 28 joints. Solid circles � erosion scorehands; solid squares � erosion score feet; open squares � totalerosion score; open triangles � JSN hands; solid triangles � JSNfeet; open circles � total JSN.
914 Haynes et al
Tab
le1.
Res
ult
sof
imm
un
ohis
toch
emic
alla
beli
ng
ofsy
nov
ial
tiss
ue
from
rheu
mat
oid
arth
riti
sp
atie
nts
wit
ha
good
clin
ical
resp
onse
tod
isea
se-m
odif
yin
gan
tirh
eum
atic
dru
gtr
eatm
ent
base
don
aD
AS
28<
2.6*
Tim
eof
syn
ovia
lbi
opsy
sin
ceba
seli
ne,
year
sIO
D80
51IO
D80
5IO
DR
AN
KL
Are
aC
D68
Are
aC
D55
IOD
Bce
lls
IOD
pla
sma
cell
sIO
DT
cell
s
IOD
mem
ory
Tce
lls
IOD
gran
zym
eB
cell
sD
AS
28
Bas
elin
e39
8�
657
406
�78
06,
432
�8,
220
41,3
54�
34,1
9815
,152
�14
,045
492
�68
612
,748
�12
,386
5,46
7�
4,06
59,
801
�8,
546
23�
155.
5�
0.6
0.25
514
�71
696
3�
1,04
65,
935
�8,
096
37,9
11�
25,5
4116
,459
�13
,694
371
�71
210
,656
�12
,075
4,40
7�
4,37
08,
744
�6,
789
30�
264.
2�
1.9
0.5
1,59
7�
2,30
82,
483
�1,
166
4,98
0�
7,26
227
,383
�16
,892
23,2
54�
21,7
1578
6�
547
4,33
5�
5,38
33,
911
�4,
071
8,17
0�
5,66
927
8�
234
2.5
�2
1.0
2,65
7�
3,31
62,
359
�1,
229
3,24
6�
6,66
918
,210
�15
,464
31,4
11�
25,8
1373
4�
590
7,35
9�
6,54
33,
591
�4,
424
5,91
1�
5,39
019
2�
205
1.8
�1.
51.
52,
862
�3,
402
2,14
1�
1,34
23,
109
�5,
919
14,3
92�
13,0
4139
,339
�26
,838
764
�69
02,
952
�3,
963
1,89
9�
2,12
84,
793
�4,
975
158
�20
71.
5�
1.2
23,
934
�4,
747
2,22
7�
1,15
62,
118
�4,
827
15,4
95�
13,2
4142
,376
�32
,341
864
�56
04,
674
�4,
329
4,17
2�
3,03
14,
419
�3,
593
43�
211.
5�
1.2
34,
023
�4,
714
2,11
8�
970
1,09
7�
2,80
814
,082
�14
,832
43,3
29�
25,6
781,
014
�87
54,
390
�3,
378
4,02
0�
2,34
24,
082
�4,
779
63�
701.
5�
1.3
*V
alu
esar
eth
em
ean
�S
D.
DA
S28
�D
isea
seA
ctiv
ity
Sco
rein
28jo
ints
;IO
D�
inte
grat
edop
tica
ld
ensi
ty,
mea
sure
dby
imag
ean
alys
is;
8051
�m
onoc
lon
alan
tibo
dy
that
mea
sure
sm
onom
eric
oste
opro
tege
rin
(OP
G)
pro
du
ced
mai
nly
bym
acro
ph
age-
like
syn
ovia
lli
nin
gce
lls;
805
�m
onoc
lon
alan
tibo
dy
that
mea
sure
sd
imer
icO
PG
,mai
nly
exp
ress
edby
end
oth
elia
lce
lls;
CD
68�
mon
oclo
nal
anti
bod
yth
atd
etec
tsm
acro
ph
age
lin
eage
cell
s;C
D55
�m
onoc
lon
alan
tibo
dy
that
det
ects
dec
ayac
tiva
tor
fact
or,
am
arke
rfo
rsy
nov
ial
lin
ing
fibr
obla
sts.
Tab
le2.
Res
ult
sof
imm
un
ohis
toch
emic
alla
beli
ng
ofsy
nov
ial
tiss
ue
from
rheu
mat
oid
arth
riti
sp
atie
nts
wh
od
emon
stra
ted
no
clin
ical
resp
onse
tod
isea
se-m
odif
yin
gan
tirh
eum
atic
dru
gtr
eatm
ent,
base
don
aD
AS
28<
2.6*
Tim
eof
syn
ovia
lbi
opsy
sin
ceba
seli
ne,
year
sIO
D80
51IO
D80
5IO
DR
AN
KL
Are
aC
D68
Are
aC
D55
IOD
Bce
lls
IOD
pla
sma
cell
sIO
DT
cell
s
IOD
mem
ory
Tce
lls
IOD
gran
zym
eB
cell
sD
AS
28
Bas
elin
e54
7�
835
696
�51
37,
372
�7,
260
22,6
65�
19,7
0223
,172
�22
,329
434
�45
38,
904
�94
22,
332
�2,
384
8,49
8�
9,00
468
�78
6.3
�0.
70.
2588
2�
901
774
�62
97,
115
�7,
508
21,5
55�
19,7
5423
,648
�24
,015
427
�42
38,
722
�75
91,
874
�1,
178
8,43
2�
9,97
360
�77
6.0
�1.
20.
51,
293
�99
499
2�
778
5,14
5�
5,70
822
,826
�19
,871
22,4
78�
27,2
9013
5�
209
9,09
1�
8,08
51,
951
�1,
306
6,72
1�
6,77
959
�77
5.5
�1.
01.
01,
167
�92
71,
059
�99
95,
123
�6,
239
26,9
09�
19,4
6022
,646
�26
,192
115
�21
65,
989
�5,
410
1,90
8�
1,32
45,
318
�6,
961
64�
804.
7�
1.1
1.5
1,28
0�
922
1,17
4�
839
4,91
2�
6,37
418
,678
�16
,548
22,9
50�
26,0
9515
7�
226
5,88
7�
5,41
01,
929
�2,
342
5,32
9�
5,96
162
�80
4.8
�1.
12
1,21
9�
1,10
61,
032
�93
94,
925
�6,
362
17,9
67�
20,1
5626
,060
�26
,670
160
�22
56,
019
�7,
393
1,89
6�
1,32
95,
333
�6,
543
61�
804.
7�
1.3
31,
484
�1,
090
1,05
1�
925
5,66
7�
3,66
418
,018
�15
,291
27,8
63�
29,0
0120
0�
248
7,36
2�
7,12
62,
252
�2,
696
6,30
9�
5,71
863
�46
4.5
�1.
5
*V
alu
esar
eth
em
ean
�S
D.
See
Tab
le1
for
defi
nit
ion
s.
RANKL and OPG in RA Synovial Tissue 915
was 1.31 for active RA patients and 0.18 for inactive RApatients. This confirmed the results for the immunohisto-chemical labeling studies at the mRNA level.
Correlation of immunohistochemical labeling forRANKL and OPG with changes in clinical and radiologicparameters. Although there was an increase in synovialtissue expression of OPG with DMARD treatment, the cor-relation with change in DAS28 failed to achieve statisticalsignificance (r � 0.402, P � 0.052). The decrease in syno-vial tissue expression of RANKL (measured by either im-age analysis or semiquantitative score) did correlate withthe reduction in DAS28 with DMARD treatment (r �0.448, P � 0.037). There was also a significant correlationbetween changes in DAS28 and changes in joint spacenarrowing score (r � 0.454, P � 0.023), with the leastchange in joint space narrowing score seen in patientswith the greatest reduction in DAS28. Similarly, there wasa significant correlation between changes in RANKL ex-pression in synovial tissue (measured with either image
analysis or semiquantitative score) and changes in erosionscore (r � 0.538, P � 0.007), with the smallest changes inerosion score seen in patients with the greatest reductionin RANKL expression in synovial tissue followingDMARD treatment. There was no correlation of changes ineither RANKL or OPG expression in the synovial tissuewith changes in joint space narrowing with DMARD treat-ment. We did not demonstrate any effect of disease dura-tion on changes in OPG or RANKL seen with DMARDtreatment. We attempted to calculate RANKL:total OPG,RANKL:endothelial OPG, and RANKL:synovial liningOPG ratios, but the data were skewed in distribution andneither logarithmic nor inverse transformation of the dataled to a meaningful analysis.
DISCUSSION
Osteoclasts are responsible for the resorption of bone dur-ing normal bone metabolism and the destruction of boneseen in a variety of pathologies such as RA. It is now clear
Figure 2. Immunohistochemical labeling of sequential synovial biopsy samples from the same knee joint in a patient with rheumatoidarthritis obtained at A, baseline, B, 3 months, C, 6 months, and D, 12 months after starting methotrexate. Biopsy samples are labeled withmonoclonal antibody 805, detecting osteoprotegerin in blood vessels, with aminoethylcarbazole as the chromogen (red color). (Originalmagnification � 400.)
916 Haynes et al
that M-CSF and RANKL are essential factors required forthe development of osteoclasts. Osteoclasts form fromcells isolated from the RA joint, with large numbers rap-idly forming from cells isolated from the pannus region(8). The cartilage–pannus junction in RA contains manytypes of cells that produce inflammatory cytokines re-ported to stimulate osteoclast differentiation and bone re-sorption, including IL-1� and IL-1�, IL-6, IL-11, and TNF�(9). The end result of the production of inflammatory cy-tokines, such as IL-1� and TNF�, in the inflamed joint islikely to be the up-regulation of RANKL (produced by Tcells, fibroblasts, and osteoblasts) (8,13) and RANK (ex-pressed by preosteoclasts, T cells, and dendritic cells) (13).OPG is an alternative, high-affinity decoy receptor forRANKL that blocks the interaction between RANKL andRANK and significantly inhibits osteoclastogenesis(14,16). Similar to RANK and RANKL, OPG production isstimulated in vitro by proinflammatory cytokines, such asIL-1� and TNF�. RANK, RANKL, and OPG are expressedin synovial tissue from the RA joint (5,6,8,15,16).
We have previously demonstrated the expression ofOPG in synovial tissue (both lining and endothelial ex-pression) from patients with both inflammatory arthritisand osteoarthritis, as well as normal synovial tissue (16).The notable exception to this was in RA synovial tissue:little or no OPG was expressed in the synovial tissue frompatients with active RA, whereas OPG was expressed bothin the synovial lining and on endothelial cells in thesynovial tissue from patients with inactive RA. In contrast,we have also demonstrated the expression of RANKLmainly in the synovial tissue of patients with active RA(15). This leads to a local synovial environment in theactive RA joint where osteoclast formation would belikely, whereas in the inactive RA joint osteoclast forma-tion would be suppressed. The current study was designedto test this hypothesis by examining the expression ofRANKL and OPG at the synovial tissue level in patientswith active RA started on treatment with DMARDs and byattempting to correlate changes in synovial expression ofRANKL and OPG with radiologic outcomes for this RA
Figure 3. Immunohistochemical labeling of sequential synovial biopsy samples from the same knee joint in a patient with rheumatoidarthritis obtained at A, baseline, B, 3 months, C, 6 months, and D, 12 months after starting methotrexate. Biopsy samples are labeled withmonoclonal antibody 8051, detecting osteoprotegerin in the synovial lining, with aminoethylcarbazole as the chromogen (red color).(Original magnification � 400.)
RANKL and OPG in RA Synovial Tissue 917
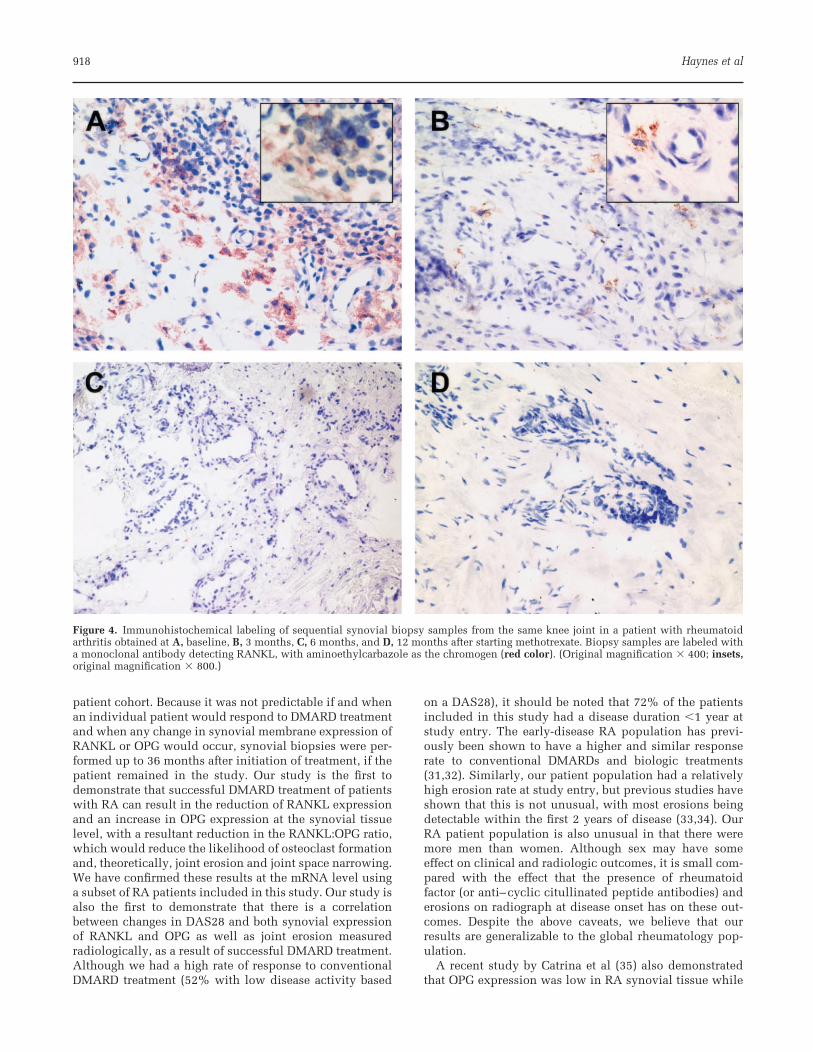
patient cohort. Because it was not predictable if and whenan individual patient would respond to DMARD treatmentand when any change in synovial membrane expression ofRANKL or OPG would occur, synovial biopsies were per-formed up to 36 months after initiation of treatment, if thepatient remained in the study. Our study is the first todemonstrate that successful DMARD treatment of patientswith RA can result in the reduction of RANKL expressionand an increase in OPG expression at the synovial tissuelevel, with a resultant reduction in the RANKL:OPG ratio,which would reduce the likelihood of osteoclast formationand, theoretically, joint erosion and joint space narrowing.We have confirmed these results at the mRNA level usinga subset of RA patients included in this study. Our study isalso the first to demonstrate that there is a correlationbetween changes in DAS28 and both synovial expressionof RANKL and OPG as well as joint erosion measuredradiologically, as a result of successful DMARD treatment.Although we had a high rate of response to conventionalDMARD treatment (52% with low disease activity based
on a DAS28), it should be noted that 72% of the patientsincluded in this study had a disease duration �1 year atstudy entry. The early-disease RA population has previ-ously been shown to have a higher and similar responserate to conventional DMARDs and biologic treatments(31,32). Similarly, our patient population had a relativelyhigh erosion rate at study entry, but previous studies haveshown that this is not unusual, with most erosions beingdetectable within the first 2 years of disease (33,34). OurRA patient population is also unusual in that there weremore men than women. Although sex may have someeffect on clinical and radiologic outcomes, it is small com-pared with the effect that the presence of rheumatoidfactor (or anti–cyclic citullinated peptide antibodies) anderosions on radiograph at disease onset has on these out-comes. Despite the above caveats, we believe that ourresults are generalizable to the global rheumatology pop-ulation.
A recent study by Catrina et al (35) also demonstratedthat OPG expression was low in RA synovial tissue while
Figure 4. Immunohistochemical labeling of sequential synovial biopsy samples from the same knee joint in a patient with rheumatoidarthritis obtained at A, baseline, B, 3 months, C, 6 months, and D, 12 months after starting methotrexate. Biopsy samples are labeled witha monoclonal antibody detecting RANKL, with aminoethylcarbazole as the chromogen (red color). (Original magnification � 400; insets,original magnification � 800.)
918 Haynes et al

RANKL expression was high in patients with active dis-ease, and that treatment with TNF blockers (either etaner-cept or infliximab) altered the RANKL:OPG ratio in favorof a reduction in osteoclast formation. However, unlikeour previous findings, these authors failed to find anycorrelation between changes in disease activity andchanges in synovial tissue expression of RANKL and OPG,and suggested that the changes they observed were a directresult of TNF blockade. The patient group included in thestudy by Catrina et al was similar to that used in our study,but Catrina et al did not indicate the disease duration oftheir patient group, so it is not possible to establishwhether the RA patients they studied had early RA, as didthe majority of the patients included in our study. Inaddition, there was considerable coprescription of bothcorticosteroids and DMARDs (mainly methotrexate) withinfliximab and etanercept in their study, so it is unclearwhether the effects on OPG and RANKL expression in RAsynovial tissue were solely due to TNF inhibitors. Finally,Catrina et al only followed patients for 8 weeks and theclinical responses seen in these patients (ACR20 responsesand reduction in DAS28 scores to mean levels of 3.8 [et-anercept] and 4.2 [infliximab]) were inferior to those seenin the patients included in our study. A further study bythe same research group (36) demonstrated that intraartic-ular corticosteroids could significantly reduce the synovialcontent of CD3-positive T lymphocytes and the expressionof RANKL by these cells without affecting synovial expres-sion of OPG, potentially reducing the risk of erosions inthe RA joint, although the researchers did not measure theeffect on radiologic outcomes. While these authors did notdemonstrate any effect of intraarticular corticosteroids onsynovial tissue OPG expression, the antibody they useddetects only OPG on endothelial cells and not on macro-phages, as we have previously demonstrated (16).
The results of our study suggest that a deficiency in OPGexpression may have a role in the pathogenesis of boneerosions, which characterize RA, and suggest that OPGmay well have a therapeutic role in the future managementof RA. Standard DMARD treatment of patients with RAcan down-regulate RANKL expression in RA synovial tis-sue with significant implications for progression of erosivedamage within joints over time. The development of treat-ments for RA that modulate both the inflammatory milieuof the synovial tissue and the mediators of osteoclast for-mation is likely to result in significant improvement in theclinical, functional, and radiologic outcomes for patientswith RA.
AUTHOR CONTRIBUTIONS
Dr. Smith had full access to all of the data in the study and takesresponsibility for the integrity of the data and the accuracy of thedata analysis.Study design. Haynes, Crotti, Smith.Acquisition of data. Haynes, Crotti, Weedon, Slavotinek, Au,Ahern, Smith.Analysis and interpretation of data. Haynes, Crotti, Coleman,Ahern, Smith.Manuscript preparation. Haynes, Crotti, Roberts-Thomson,Ahern, Smith.Statistical analysis. Ahern.
REFERENCES
1. Van Zeben D, Hazes JM, Zwinderman AH, Vandenbroucke JP,Breedveld FC. Factors predicting outcome of rheumatoidarthritis: results of a followup study [published erratum ap-pears in J Rheumatol 1993;20:2179]. J Rheumatol 1993;20:1288–96.
2. Woolley DE, Crossley MJ, Evanson JM. Collagenase at sites ofcartilage erosion in the rheumatoid joint. Arthritis Rheum1977;20:1231–9.
3. Trabant A, Gay RE, Fassbender HG, Gay S. Cathepsin B insynovial cells at the site of joint destruction in rheumatoidarthritis. Arthritis Rheum 1991;34:1444–51.
4. Tetlow LC, Woolley DE. Mast cells, cytokines, and metallo-proteinases at the rheumatoid lesion: dual immunolocalisa-tion studies. Ann Rheum Dis 1995;54:896–903.
5. Gravallese EM, Manning C, Tsay A, Naito A, Pan C, Amento E,et al. Synovial tissue in rheumatoid arthritis is a source ofosteoclast differentiation factor. Arthritis Rheum 2000;43:250–8.
6. Takayanagi H, Iizuka H, Juji T, Nakagawa T, Yamamoto A,Miyazaki T, et al. Involvement of receptor activator of nuclearfactor �B ligand/osteoclast differentiation factor in osteoclas-togenesis from synoviocytes in rheumatoid arthritis. ArthritisRheum 2000;43:259–69.
7. Romas E, Bakharevski O, Hards DK, Kartsogiannis V, QuinnJM, Ryan PF, et al. Expression of osteoclast differentiationfactor at sites of bone erosion in collagen-induced arthritis.Arthritis Rheum 2000;43:821–6.
8. Haynes DR, Crotti TN, Loric M, Bain GI, Atkins GJ, FindlayDM. Osteoprotegerin and receptor activator of nuclear factor�B ligand (RANKL) regulate osteoclast formation by cells inthe human rheumatoid arthritic joint. Rheumatology (Oxford)2001;40:623–30.
9. Chu CQ, Field M, Allard S, Abney E, Feldmann M, Maini RN.Detection of cytokines at the cartilage/pannus junction inpatients with rheumatoid arthritis: implications for the role ofcytokines in cartilage destruction and repair. Br J Rheumatol1992;31:653–61.
10. Deleuran BW, Chu CQ, Field M, Brennan FM, Katsikis P,Feldmann M, et al. Localization of interleukin-1 �, type 1interleukin-1 receptor and interleukin-1 receptor antagonistin the synovial membrane and cartilage/pannus junction inrheumatoid arthritis. Br J Rheumatol 1992;31:801–9.
11. Chu CQ, Field M, Feldmann M, Maini RN. Localization oftumor necrosis factor � in synovial tissues and at thecartilage–pannus junction in patients with rheumatoid arthri-tis. Arthritis Rheum 1991;34:1125–32.
12. Yasuda H, Shima N, Nakagawa N, Yamaguchi K, Kinosaki M,Mochizuki S, et al. Osteoclast differentiation factor is a ligandfor osteoprotegerin/osteoclastogenesis-inhibitory factor and isidentical to TRANCE/RANKL. Proc Natl Acad Sci U S A1998;95:3597–602.
13. Gravallese EM, Galson DL, Goldring SR, Auron PE. The role ofTNF-receptor family members and other TRAF-dependentreceptors in bone resorption. Arthritis Res 2001;3:6–12.
14. Lacey DL, Timms E, Tan HL, Kelley MJ, Dunstan CR, BurgessT, et al. Osteoprotegerin ligand is a cytokine that regulatesosteoclast differentiation and activation. Cell 1998;9:165–76.
15. Crotti TN, Smith MD, Weedon H, Ahern MJ, Findlay DM,Kraan M, et al. Receptor activator NF-�B ligand (RANKL)expression in synovial tissue from patients with rheumatoidarthritis, spondyloarthropathy, osteoarthritis, and from nor-mal patients: semiquantitative and quantitative analysis. AnnRheum Dis 2002;61:1047–54.
16. Haynes DR, Barg E, Crotti TN, Holding C, Weedon H, AtkinsGJ, et al. Osteoprotegerin expression in synovial tissue frompatients with rheumatoid arthritis, spondyloarthropathiesand osteoarthritis and normal controls. Rheumatology (Ox-ford) 2003;42:123–34.
17. Smith MD, Barg E, Weedon H, Papangelis V, Smeets T, TakPP, et al. The microarchitecture and protective mechanismsin synovial tissue from clinically and arthroscopically normalknee joints. Ann Rheum Dis 2003;62:303–7.
RANKL and OPG in RA Synovial Tissue 919
18. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF,Cooper NS, et al. The American Rheumatism Association1987 revised criteria for the classification of rheumatoid ar-thritis. Arthritis Rheum 1988;31:315–24.
19. Prevoo ML, van ’t Hof MA, Kuper HH, van Leeuwen MA, vande Putte LB, van Riel PL. Modified disease activity scores thatinclude twenty-eight–joint counts: development and valida-tion in a prospective longitudinal study of patients with rheu-matoid arthritis. Arthritis Rheum 1995;38:44–8.
20. Felson DT, Anderson JJ, Boers M, Bombardier C, Chernoff M,Fried B, et al. The American College of Rheumatology prelim-inary core set of disease activity measures for rheumatoidarthritis clinical trials. Arthritis Rheum 1993;36:729–40.
21. Smith MD, Chandran G, Youssef PP, Darby T, Ahern MJ. Daycase knee arthroscopy under regional anesthesia, performedby rheumatologists. Aust N Z J Med 1996;26:108–9.
22. Kraan MC, Haringman JJ, Ahern MJ, Breedveld FC, Smith MD,Tak PP. Quantification of the cell infiltrate in synovial tissueby digital image analysis. Rheumatology (Oxford) 2000;39:43–9.
23. Kraan MC, Smith MD, Weedon H, Ahern MJ, Breedveld FC,Tak PP. Measurement of cytokine and cell adhesion moleculeexpression in synovial issue by digital image analysis. AnnRheum Dis 2001;60:296–8..
24. Tak PP, van der Lubbe PA, Cauli A, Daha MR, Smeets TJ,Kluin PM, et al. Reduction of synovial inflammation afteranti-CD4 monoclonal antibody treatment in early rheumatoidarthritis. Arthritis Rheum 1995;38:1457–65.
25. Welldon KJ, Atkins GJ, Howie DW, Findlay DM. Primaryhuman osteoblasts grow into porous tantalum and maintainan osteoblastic phenotype. J Biomed Mater Res A 2008;84:691–701.
26. Franssen ME, Zeeuwen PL, Vierwinden G, van de Kerkhof PC,Schalkwijk J, van Erp PE. Phenotypical and functional differ-ences in germinative subpopulations derived from normaland psoriatic epidermis. J Invest Dermatol 2005;124:373–83.
27. Livak KJ, Schmittgen TD. Analysis of relative gene expression
data using real-time quantitative PCR and the 2��(�Ct) method.Methods 2001;25:402–8.
28. Van der Heide A, Remme CA, Hofman DM, Jacobs JW, BijlsmaJW. Prediction of progression of radiologic damage in newlydiagnosed rheumatoid arthritis. Arthritis Rheum 1995;38:1466–74.
29. Smith MD, Kraan MC, Slavotinek J, Au V, Weedon H, ParkerA, et al. Treatment induced remission in rheumatoid arthritispatients is characterised by a reduction in macrophage con-tent of synovial biopsies. Rheumatology (Oxford) 2001;40:367–74.
30. Kraan MC, Haringman JJ, Weedon H, Barg EC, Smith MD,Ahern MJ, et al. T cells, fibroblast-like synoviocytes, andgranzyme B cytotoxic cells are associated with joint damagein patients with recent onset rheumatoid arthritis. AnnRheum Dis 2004;63:483–5.
31. Cush JJ. Early rheumatoid arthritis: is there a window ofopportunity? J Rheumatol Suppl 2007;34:1–7.
32. Mitchell KL, Pisetsky DS. Early rheumatoid arthritis. CurrOpin Rheumatol 2007;19:278–83.
33. Richi P, Balsa A, Munoz-Fernandez S, Villaverde V, Fernan-dez-Prada M, Vicario JL, et al. Factors related to radiologicaldamage in 61 Spaniards with early rheumatoid arthritis. AnnRheum Dis 2002;61:270–2.
34. Wick MC, Lindblad S, Weiss RJ, Klareskog L, van Vollen-hoven RF. Estimated prediagnosis radiological progression:an important tool for studying the effects of early diseasemodifying antirheumatic drug treatment in rheumatoid ar-thritis. Ann Rheum Dis 2005;64:134–7.
35. Catrina AI, Klint EA, Ernestam S, Catrina SB, MakrygiannakisD, Botusan IR, et al. Anti–tumor necrosis factor therapy in-creases synovial osteoprotegerin expression in rheumatoidarthritis. Arthritis Rheum 2006;54:76–81.
36. Makrygiannakis D, Klint EA, Catrina SB, Botusan IR, Klares-kog E, Klareskog L, et al. Intraarticular corticosteroids de-crease synovial RANKL expression in inflammatory arthritis.Arthritis Rheum 2006;54:1463–72.
920 Haynes et al





























