Embed Size (px)
Citation preview

Module 12: Patient Support 12-1
Student Text IAFF Training for Hazardous Materials: Technician©
Module 12:
Patient Support

12-2 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Module 12: Patient Support 12-3
Student Text IAFF Training for Hazardous Materials: Technician©
Module 12: Patient Support
Module Description
This module describes how to assess, treat, and transport patients who have been exposed tohazardous materials or injured in such incidents. The first part of the module covers the assess-ment and treatment of emergency personnel as patients, while the latter part covers patients whoare not connected with the response.
Prerequisites
• Students should have completed a hazardous materials operations level training program.
• Students must be certified to the Emergency Medical Technician or Paramedic level.

12-4 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Objectives
Upon completion of this module, participants will be able to:
Instructor Preparation
• Describe the major tasks of EMS providers at a hazardous materialsincident
• List the limitations of chemical protective clothing
• Discuss health risks associated with PPE use at a hazardous materialsincident
• Describe the elements of pre- and post-entry assessments
• Describe how to perform gross decontamination on an exposed patient
• Perform a thorough assessment of patients who have been contaminatedwith hazardous materials
• Provide appropriate supportive care depending on the organ system af-fected
• Perform or describe the specific care that should be given for exposureto:• Asphyxiants• Irritants• Organophosphate insecticides• Smoke inhalation• Heat and cold injuries
• Safely transport patients who have been exposed to hazardous materials
ObjectivesNFPA
StandardsOSHA
Standards
NFPA 4733-1.3 (b)
NFPA 4724-4.2.5NFPA 4724-3.3.3.7
NFPA 4733-3.2NFPA 4733-2.2 (d) (e)3-4 (a) (b)
NFPA 4733.2.2 (b), 3-4.1,3-4.4NFPA 4732-4.2 (b)
NFPA 4733-4, 3-4.2 (c)
29 CFR 1910.120(q) (6) (iii) (C)
29 CFR 1910.120(q) (6) (iii) (C)29 CFR 1910.120(q) (6) (iii) (C)
29 CFR 1910.120(q) (6) (iii) (C)29 CFR 1910.120(q) (6) (iii) (C,G)29 CFR 1910.120(q) (6) (iii) (C)
29 CFR 1910.120(q) (6) (iii) (C, I)
29 CFR 1910.120(q) (6) (iii) (C, I)
29 CFR 1910.120(q) (6) (iii) (C)

Module 12: Patient Support 12-5
Student Text IAFF Training for Hazardous Materials: Technician©
References
Emergency Medical Response to Hazardous Materials Incidents,Richard Stilp and Armando Bevelacqua
Approximate Length
This module requires approximately eight to sixteen hours, depending on the experience level ofyour students and the activities you schedule.

12-6 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-7
Student Text IAFF Training for Hazardous Materials: Technician©
Module 12Prerequisite Quiz
1. How should a seriously injured patient who has been contaminated with a toxic chemicalbe decontaminated?A. The patient should undergo full decontamination prior to medical treatmentB. The patient should undergo full decontamination after medical treatmentC. The patient should undergo gross decontamination prior to medical treat-mentD. Medical treatment takes priority; the patient should not be decontaminated at the
scene
2. How should burns from alkali corrosive agents be treated?A. The chemical should be blotted dry and the burn covered with a dry dressingB. The chemical should be blotted dry and the burn covered with a wet dressingC. The chemical should be thoroughly flushed and the burn covered with a dry
dressingD. The chemical should be thoroughly flushed and the burn covered with a wet
dressing
3. Which of these asphyxiants carries the highest risk of secondary contamination?A. Carbon monoxideB. CyanideC. Hydrogen sulfideD. Methane
4. The acronym DUMBELS is associated with symptoms produced by exposure to which ofthe following insecticides?A. OrganophosphatesB. OrganochlorinesC. PyrethrinsD. Carbamates
5. Victims of heat stroke experience:A. Rapid, weak pulse and flushed, dry skinB. Rapid, strong pulse and flushed, dry skinC. Rapid, weak pulse and heavy perspirationD. Slow pulse and flushed, dry skin
6. Exposure to hydrogen fluoride can cause depletion of blood:A. OxygenB. NitrogenC. Red blood cellsD. Calcium

12-8 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
7. Carboxyhemoglobin occurs when carbon monoxide inhibits:A. The blood’s ability to carry oxygenB. Gas transfer through the lungsC. Blood flowD. Heart rhythm
8. Cyanide is easily absorbed through:A. InhalationB. Skin absorptionC. IngestionD. All three routes of exposure
9. How should hypothermic patients be treated?A. The patient should be warmed quickly by total immersion in warm waterB. The patient should be warmed slowly by placing heat packs close to the bodyC. The patient should be warmed quickly by placing heat packs on the extremitiesD. Extremities should be warmed quickly and the torso slowly
10. Which of the following chemicals can produce methemoglobinemia?A. Hydrogen sulfideB. Carbon monoxideC. CyanideD. Nitrates

Module 12: Patient Support 12-9
Student Text IAFF Training for Hazardous Materials: Technician©
Introduction
Questions
1. A patient contaminated with an organophosphateinsecticide is in severe respiratory distress. Should s/hebe decontaminated prior to treatment? Why or whynot?
2. For hazardous materials entry team members, what arethe exclusion criteria for vital signs (temperature,resting pulse, and blood pressure)?
3. What effect does carboxyhemoglobin have on the body?What is one chemical that can cause this?
A primary role of EMS personnel at hazardous materialsincidents is to help protect the health and safety of emer-gency responders. The safety of response personnel,however, is ultimately the responsibility of the IncidentCommander. The Incident Commander appoints an Inci-dent Safety Officer, who ensures that the following tasksare accomplished:
• Adequate personnel are on hand to safely achieveobjectives
• Personal protective equipment (PPE) is appropriate forthe tasks to be performed
• Work/rest cycles reflect on-site conditions and aresupervised and controlled
• Activities in Warm and Hot Zones are closely moni-tored and dangerous conditions are identified andcorrected
• Personnel working in the Warm and Hot Zones areproperly trained to wear PPE and receive medicalmonitoring before and after entry
• Adequate records concerning the health status of per-sonnel and incident related activities are maintained
12-10 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Emergency medical personnel can provide importantassistance in each of these areas. In doing so, they helpensure the health and safety of emergency responders.

Module 12: Patient Support 12-11
Student Text IAFF Training for Hazardous Materials: Technician©
Personal ProtectiveEquipmentThe purpose of personal protective clothing and equipmentis to protect emergency responders from chemical, physi-cal, and biological hazards they may encounter duringhazardous materials emergency response. Select PPEcarefully so that it provides adequate protection against thehazardous materials that are present, while allowing you tocomplete response tasks. For this reason, PPE can only beused in conjunction with other protective measures, includ-ing work/rest cycles and a medical surveillance program.Moreover, personnel should never don protective clothing ifthey have not been trained in its use.
The use of personal protective equipment can presentsignificant hazards. Generally, increased levels of PPE areassociated with increased risks for the wearer.
Limitations/Complications
When working in EMS, you must recognize the limitationsor complications that PPE can impose on emergencyresponders. These include:
• Limited mobility: PPE adds bulk and weight that canslow movement, restrict activity, and contribute toincreased oxygen needs and fatigue.
• Limited visibility: Face masks of SCBA and the faceshields of encapsulated suits diminish peripheral visionand can distort the wearer’s view. This compoundsvisibility problems that may already be present as aresult of smoke, darkness, or other environmentalconditions.
• Limited communication: Voice communication isimpaired or impossible unless radio transmitters areavailable within encapsulated suits. Even these radiosystems can fail or operate poorly. Hand signals areoften the only means of communication, particularly ifthe ambient sound is high.

12-12 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
• Limited dexterity: Multiple layers of gloves and bulkyprotective clothing can interfere with fine motor dexter-ity, limiting the types of work that can be safely per-formed.
• Limited endurance: The extra energy required tocarry the weight of protective clothing and the use ofSCBA reduces the wearer’s level of endurance, makingwork scheduling an important factor.
• Limited air supply: Most chemical protective fully-encapsulating clothing is worn with self-containedbreathing apparatus (PP SCBA). PP SCBA provides alimited quantity of air and this governs the amount oftime emergency responders can remain in the hazardzone. In addition, the increased exertion caused by thephysiological and psychological stress of PPE mayfurther reduce the duration of the air supply.
It is easy to see how these factors complicate the use ofPPE during emergency response. Such limitations cansubstantially impact the safety of emergency responders.Because patient assessment and treatment requires the useof the senses and fine motor dexterity, you may need tomodify your approach to health care when you are wearingPPE or assisting someone who is wearing it.
Health Risks
General Considerations
The limitations of personal protective equipment clearlyhave the potential to affect scene safety. In addition tointerfering with normal activities, the use of PPE createsphysical and psychological stresses. All responders operat-ing at the emergency incident scene must be properlytrained to detect and report these stresses.
Potential health problems should then be brought to theattention of the appropriate sector officer or EMS provider.
Examples of possible problems include:• Degradation of personal protective equipment• Perception of odors

Module 12: Patient Support 12-13
Student Text IAFF Training for Hazardous Materials: Technician©
• Skin irritation• Unusual residues on PPE• Discomfort or pain• Trouble breathing• Fatigue due to respirator use• Unexplained problems with vision or communication• Abnormal restriction of movement• Other symptoms such as rapid pulse, nausea, or chest
pain• Evidence of heat stress• Neurological problems
Hazardous Exposures
You may be exposed to hazardous materials at an incident ifyour PPE is inappropriate or it fails. Proper protectiveensemble selection is a key factor in preventing exposures.Throughout the incident, monitor the integrity of your PPEfor degradation or any damage that would allow chemicalsto breach its protective barrier.
Asphyxiation
Asphyxia is a medical condition caused by a lack of oxygenin the blood. The obvious causes of asphyxiation arerelated to oxygen-deficient atmospheres or the presence ofchemical asphyxiants such as cyanide that disrupt thebody’s ability to process oxygen and carbon dioxide. Iden-tify these conditions through proper scene assessment sothat you can use adequate respiratory protection, includingbreathing air supplied under positive pressure. Monitoryour supply of breathing air closely. Adequate breathing airmust be on hand for all phases of emergency response,including the decontamination process. The exact time anentry team member is on air must be monitored, taking intoaccount the added use rate that occurs with increasedactivity and workload.
Heat Injuries
Heat-related injuries are a serious health problem duringemergency operations, particularly when fully encapsulatingPPE is worn. Health effects due to hyperthermia or highbody temperature can range from transient fatigue to serious

12-14 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
illness or death. There is a direct relationship between theamount and type of PPE worn and reduced work toleranceand heat stress. This is because PPE adds weight and bulk,increases energy expenditure, and interferes with the body’snormal heat exchange mechanisms such as evaporation.Effective prevention of heat injuries is based on adequatehydration of personnel, control of work schedules and theirduration, and monitoring for early signs of hyperthermiaand level of fitness.
Psychological Effects of PPE
Wearing personal protective equipment can produce strongand potentially uncontrollable behavioral reactions in someemergency responders. Fully encapsulated suits, for ex-ample, can cause a sense of claustrophobia and constraint.These types of problems are often related to lack of famil-iarity with PPE and can be minimized with adequate train-ing in its use. Despite training, however, combined eventsduring an incident may bring about stress reactions that canbe manifested in various ways. As part of safety monitor-ing, watch for signs of panic or other psychological distressin those who wear PPE.
You must be constantly aware of the health and safetystatus of your partners. Monitoring for distress is part ofthat awareness.

Module 12: Patient Support 12-15
Student Text IAFF Training for Hazardous Materials: Technician©
Pre and Post EntryAssessment ofPersonnelAll responders must have a baseline assessment beforedonning chemical protective clothing. This applies tomembers of the decontamination team as well as the entryand backup teams. The assessment has two purposes. Thefirst is to determine whether the responder is fit at that timeto conduct operations while wearing the required level ofPPE. The second is to establish baseline data on physicalfactors that will be monitored for changes throughout thework period.
Prior to Entry
Only individuals who have previously been approved by aphysician for work in chemical protective clothing and theuse of self-contained breathing apparatus can be consideredfor work in such equipment. The health status of potentialmembers of the Entry Team and Backup Team must bechecked before protective clothing is donned. At a mini-mum, check and record blood pressure, pulse, respiratoryrate, oral temperature, and weight. In addition, follow achecklist to assess each individual regarding:
• Recent illness (especially with diarrhea or vomiting)• Sunburn• Recent medication use, such as antihistamines, that
might affect fluid balance
Any responder with upper respiratory tract infection orsigns of a gastrointestinal illness should not be allowed towear PPE.
Consult your department’s physician or an occupationalhealth physician regarding criteria for excluding an indi-vidual from work in chemical protective clothing based onthis pre-entry assessment. In general, it is a good idea torecheck the vital signs of any individual with an elevated

12-16 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
oral temperature (greater than 99°F), a resting pulse greaterthan 100 beats per minute, or a blood pressure in excess of150/90. If any of these vital signs remain elevated afterresting for several minutes, the individual should not donand work in protective clothing. Fluids should be taken byall members donning protective equipment to compensatefor excessive water loss through sweating. Fluid consump-tion should be about 8-16 ounces; additional fluids maycause bloating.
Each individual donning chemical protective clothing mustbe assessed before donning the suit, between any air bottlechanges and after completion of the assigned work. Yourinitial assessment must be quick but thorough and youshould have authority to make final recommendationsregarding each individual’s suitability for the work. Yourbaseline findings must be recorded so that you can comparethem with later assessments. The findings from periodicand post-entry assessments must also be recorded. Theseshould help you determine whether the responder needsfurther medical attention. If no further attention is needed,the responder can return to the staging area after adequatetime in the rehabilitation area.
Exclusion criteria for donning PPE should be establishedwell in advance. All EMS personnel should be familiarwith these criteria and should strictly follow them.
During Rehabilitation Breaks
Monitor each individual’s physical condition as early aspossible during each rest period. Observe and record thefollowing to detect early signs of heat-related injuries.
• Heart Rate: The radial pulse during a 30-secondperiod should be counted as early as possible in any restperiod. If the heart rate exceeds 110 beats per minute atthe beginning of the rest period, the next work cycleshould be shortened by one-third. Other indications thatthe work is too strenuous under ambient conditionsinclude a resting heart rate (after 3 minutes) greater than90 beats per minute. If the pulse is irregular, the firefighter should not be allowed to work and should beevaluated by a physician.

Module 12: Patient Support 12-17
Student Text IAFF Training for Hazardous Materials: Technician©
• Temperature: A clinical thermometer should be usedto measure temperature orally or aurally at the end ofthe response activity and before fluids are taken. Iftemperature exceeds 99.5°F (37.5°C), the next workperiod should be shortened by at least one-third. Neverpermit a fire fighter to work when his or her tempera-ture exceeds 100.5°F (38°C). In addition, skin tempera-ture may be checked with a disposable, adhesive deviceapplied to the chest. As the skin temperature and oral/aural temperature approach the same value, the risk ofheat-related illnesses increases.
• Blood Pressure: Although guidelines for blood pres-sure with regard to preventing heat stress have not beenestablished, a responder should extend his or her restperiod if blood pressure exceeds 150/90. A bloodpressure of less than 90/60 may indicate a state ofdehydration in which the body is failing to compensate.In that case, additional fluids, rest, and monitoring arerequired.
• Body Water Loss: Weight should be measured on ascale accurate to + 0.25 pounds prior to any responseactivity. Compare this weight with the individual’snormal body weight to determine if enough fluids havebeen consumed to prevent dehydration. Similar cloth-ing (always dry) should be worn each time the indi-vidual is weighed. The body water lost should notexceed 1.5 percent of total body weight.
Follow the above guidelines to monitor all personnel forsigns of heat injury, even those who are not wearing protec-tive equipment but are judged to be at risk of a heat-relatedillness.
In addition to signs of heat injury, observe responders forsigns and symptoms of chemical exposure.
Activity

12-18 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Post-Entry Assessment
Everyone going through decontamination proceduresshould be assessed for signs and symptoms of exposure. Ifit appears that a worker has been exposed, inform theSafety Officer immediately since there may be an unknownor unexpected problem that is causing additional workers tobe exposed. Persons who have been exposed must then betreated as patients. If there is any possibility of secondaryexposure, EMS personnel should be appropriately pro-tected.
Post-incident assessment should include a final check ofvital signs and a comparison to baseline data as well as anevaluation of any signs of exposure or injury. It is impor-tant to do a neurological assessment to determine if level ofconsciousness has been affected. Entry team membersshould also have fluids replenished with at least eightounces of water or other hydrating liquid. Arrangementsmust be made, in consultation with the physician, to pro-vide for follow up care for any problem that has occurredand for any exposures that may result in a delayed toxicresponse.
In some cases, it may be necessary to devote time to a“Critical Incident Stress Debriefing” (CISD). The purposeof CISD is to help responders deal with traumatic events.This debriefing may be helpful in several situations, such asincidents where response personnel were exposed to haz-ardous materials with unknown effects; incidents involvingchemicals linked with long-term health effects, such ascancer; or incidents involving civilian or fire fighter death.CISD should be held within 48 hours of the event to bemost effective. Further information about stress manage-ment programs can be obtained from the U.S. Fire Admin-istration, Office of Fire Fighter Health and Safety, 16825 S.Seton Avenue, Emmitsburg, Maryland 21727.

Module 12: Patient Support 12-19
Student Text IAFF Training for Hazardous Materials: Technician©
Records
Documents of all monitoring and health care during theincident should be completed and maintained in the confi-dential health records of each individual.
It is also important to complete incident and exposurereports. These reports will help health and safety personneldetermine whether responders require follow-up or post-exposure monitoring. They will also serve as a futurereference if any health problems develop later. Records ofan incident should include the following information:
• Incident factors such as time and weather• Agent(s) involved• Measured exposure levels• On-scene action taken• Injuries sustained, treatment given• Follow-up action taken• Short term effects• Long term effects
By documenting and tracking exposures, your departmentmay be able to discover reasons for the exposures and takemeasures to prevent them in the future.

12-20 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-21
Student Text IAFF Training for Hazardous Materials: Technician©
Patient CareIn many ways, patient care at hazardous materials incidentsis similar to patient care at EMS calls. Your assessment ofthe patient is systematic. Your priorities include establish-ing an airway and ensuring breathing and circulation, thenaddressing other injuries or medical conditions in order ofseverity. Since you should already be proficient in routinepatient care, only the areas specific to hazardous materialcontamination, health effects, and treatment strategies arepresented. There are a few antidotes for specific chemicalexposures and these are discussed after general treatmentsfor each body system.
Decontamination
Typically, EMS personnel are not trained and are notexpected to perform patient decontamination. However,you should be familiar with these procedures so that youwill know what to expect at hazardous materials incidents.
Remember that exposure to a hazardous substance andcontamination with that substance are two different prob-lems. For example, a victim who has been exposed tocarbon monoxide or another simple asphyxiant must bemoved to fresh air, but does not need to be decontaminated.However, exposures to other substances are likely to resultin contamination, in which the substance clings to thepatient’s skin, clothing, or hair. In order to prevent contin-ued exposure and the risk of secondary contamination,patients must undergo decontamination prior to treatment.
If patients need immediate medical treatment, emergencydecontamination should be performed. In emergencydecontamination, the primary concern is to prevent severeinjury or loss of life. At the same time, contaminants mustbe removed to prevent ongoing exposure to the patient andexposure to response personnel through secondary contami-nation. Even in an emergency, decontamination shouldfollow a specific sequence.
Outer, more heavily contaminated items are decontami-nated and removed first, followed by less contaminated

12-22 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
articles of clothing. Gloves and boots or shoes may requiremore extensive decontamination than shirts or jackets. Incases where the victim is wearing street clothing or othermaterials that are not easily decontaminated, the outerclothing should be removed. Dry contaminants should bebrushed off the skin. Liquid contaminants can be blotteddry. Care must be taken to keep all contaminants awayfrom the face and open wounds. Affected skin and mucousmembranes (including the eyes) should be flushed withlukewarm water for at least 15 minutes. Cold water can beused if lukewarm water is not available. Large amounts ofwater must be used when corrosives are involved.
When multiple areas of the body are affected, priorityshould be given to particularly vulnerable areas, such as theeyes. If the contaminating substance is not water soluble,as with oily materials, the skin (but never the eyes) shouldbe washed gently with a solution of liquid soap in water.
The solutions and water used for decontamination shouldnot be allowed to run onto unprotected areas of the body.Used water and solutions should be contained if possible.This protects the environment and simplifies cleanup.However, individual emergency care is a high priority, sodelays in decontamination due to concern about runoffshould be avoided.
Like all standard operating procedures, decontaminationand emergency decontamination must work in a wide rangeof environments. For example, decontamination proce-dures should be written so that they are easily modifiedduring winter. All procedures, including alternative proce-dures, must be developed and practiced in cooperation withother involved organizations, such as hospital emergencydepartments.
Patients and personnel who do not need immediate medicalattention should undergo thorough decontamination. Forresponders in turnout gear, the surface of clothing should bescrubbed with a detergent solution and thoroughly rinsedwith water. The clothing is then removed so the respondercan take a personal hygiene shower at the scene to preventthe spread of offsite contamination. Protective clothing andequipment is bagged for testing and treatment or disposal.

Module 12: Patient Support 12-23
Student Text IAFF Training for Hazardous Materials: Technician©
Full Decontamination
Civilian patients are likely to have exposed skin surfacesbecause street clothing will not resist water nor penetrationof chemicals. In fact, clothing will tend to trap contami-nants close to the skin. Generally, it is most effective toremove clothing by cutting. The patient should then bewashed or allowed to shower. Special care must be taken toavoid skin abrasions that allow for easier absorption ofhazardous chemicals.
Flush any affected skin or mucous membranes (includingthe eyes) with lukewarm water. Use cold water if luke-warm water is not available. Flood with large amounts ofwater in all cases. This is especially important becausesome chemicals, such as calcium chloride (lime), form acorrosive liquid when mixed with water. Other chemicals,such as sulfuric acid, will react with water to produce heat.Using large amounts of water allows the material to bewashed away while absorbing some of the heat generatedby the reaction. Water being used for flushing should runoff the individual and not onto other areas of the body.Cover irrigated wounds with sterile towels or gauze toprevent runoff onto other areas of the body. Replace thedressing as soon as it becomes saturated or irrigation iscomplete. In any case, contain used rinse water, if possible.
When multiple areas of the body are affected, priorityshould be given to particularly vulnerable areas, such as theeyes. Flush eyes from the inside corner toward the outsidecorner, holding the eyelids open, if necessary. Flushingshould be done gently to avoid splashing or damage toburned skin. Body creases, hair, nail beds, and any openwounds must be flushed. If the contaminating substance isnot water soluble, as with oily materials, wash the skin(never the eyes) gently with a solution of liquid soap inwater. Contain any waste water for later treatment ordisposal.
When the contaminant is a dry agent, do not wet it or washthe patient until contaminants have been removed (as muchas possible) by lightly brushing the material from thesurface.

12-24 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
When a patient is contaminated with liquid materials,remove the clothing quickly and follow with a thoroughwashing using large amounts of water to dilute the material.Soap can be used as needed to remove remaining contami-nant. If contaminants on skin have any corrosive properties(such as acids or bases), continue flushing with water for atleast 20 minutes.
Patients exposed to toxic gases may still be contaminatedeven though they are no longer in the gas cloud. This isparticularly true of vapors (the gas form of a liquid) anddusts (small solid particles suspended in air). Clothingshould be removed rapidly and the patient decontaminatedby washing.
Activity
Remember to confine the runoff so it can be picked up anddisposed of, if practical. Do not delay life-saving actions tocontain run-off. Contaminated clothing and small equip-ment should be placed in plastic bags for decontaminationor disposal. The bags should be labeled as a biohazard orcontaminated and the label should describe what the bagcontains. Use transparent bags to contain items contami-nated with chemicals so cleanup and disposal personnel cansee the extent of contamination.
Like all standard operating procedures (SOPs), your depart-ment must be able to carry out decontamination and emer-gency decontamination procedures in a wide range ofenvironments. For example, decontamination proceduresmay have to be modified during the winter season. Or,alternate procedures may have to be developed in coopera-tion with other organizations, such as a specific hospitalemergency department. SOPs should also include proce-dures for collecting or containing contaminated runoff.However, since individual emergency care is a high priority,do not delay care due to concern about runoff.
All decontamination should occur in the Warm Zone. Thisremoves patients from the area of contamination (the HotZone) and prevents the spread of hazardous materials touncontaminated areas (the Cold Zone). Contaminatedvictims who are ambulatory upon arrival of emergencypersonnel should be instructed to wait in a well-ventilated,

Module 12: Patient Support 12-25
Student Text IAFF Training for Hazardous Materials: Technician©
protected area until a decontamination area is established.Responders performing decontamination must be ad-equately protected against the hazard. This may mean thatdecontamination personnel wear chemical protectiveclothing in addition to self-contained breathing apparatus(SCBA) and other routinely worn gear. Because EMSpersonnel do not typically use this equipment, your contactwith patients will probably begin after most of the hazard-ous substance has been removed.
Patient Assessment
Activity
A triage area should be established away from (and upwindof) the source of contamination. Impress upon the IncidentCommander that the triage area must be far enough fromthe incident so that it will not have to be moved if there is ashift in wind direction. Always choose security overproximity when selecting this location.
In triage, you identify the most critical injuries and estab-lish priorities for treatment. When hazardous materials areinvolved, however, all personnel must remain on guard toavoid being contaminated by the victims. Though decon-tamination should eliminate this risk, you and other person-nel in the area should be alert to any signs and symptoms ofexposure among EMS personnel.
Patient Assessment
In addition to routine triage assessment of patients, youshould determine the following:
• To what degree is each injury related to the hazardousmaterials involved?
• Which injuries are most severe and should be treatedfirst?
• What is the route of entry to the body (inhalation,ingestion, skin, eye)?
• Are delayed effects of exposure possible?

12-26 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Keep in mind that signs and symptoms related to hazardousmaterials exposure may not be obvious. Respiratorydistress may be delayed, skin may be burned or irritated inareas that are not readily apparent, or patients may notrealize they were exposed. Check with the Incident SafetyOfficer regarding the identity of all materials involved, thelikely symptoms of exposure and appropriate protectivemeasures for EMS personnel. Your patient’s condition canchange rapidly depending on the hazardous materialsinvolved. Vital signs, especially blood pressure, pulse andrespiration must be monitored frequently.
Tagging Patients
Tagging (with triage assessment) allows you to prioritizepatient care, particularly when more than one patient isinvolved. Subsequent treatment for each patient should bebased on this information.
Tag information should include:• Vital signs• Signs and symptoms• Materials the patient was exposed to• Exposure routes and duration• Treatment to date• Additional injury assessment• Chronic illness• Allergies• Current medication
Good triage assessment and tagging (even with a singlepatient) speeds admitting and treatment at the hospital.
General Treatment
Check and maintain the patient’s airway, breathing andcirculation as soon as possible. Begin other treatment onlyafter the patient is in the triage area. As with all patients,BSI (body substance isolation)—latex gloves, eye protec-tion, and fluid resistant garments—should be used toprevent exposure to blood and body fluids. Also rememberthat emesis (vomiting) can be a source of secondary con-tamination. If you are likely to need additional protectivegarments, you should be trained in their use prior to anincident.

Module 12: Patient Support 12-27
Student Text IAFF Training for Hazardous Materials: Technician©
Protect patients by clothing them in disposable gowns andslippers. If patients still have contaminated possessions,even after leaving the decontamination area, bag these forlater decontamination or disposal. Administration ofemergency medical care should be based on the type ofagent or agents involved, signs and symptoms, and thebody systems that are affected.
It is also important to prevent secondary contamination ofequipment, if possible. Contaminated equipment mustremain out of service until it is decontaminated. In somecases, contaminated equipment will have to be disposed ofand replaced. While this may limit usable equipment andhinder operations, disposal may be the only safe solution.

12-28 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-29
Student Text IAFF Training for Hazardous Materials: Technician©
Supportive CareOnly a few chemicals have specific antidotes that you canuse to reverse their effects. For the most part, you willinvestigate the organ systems affected by the hazardousmaterials and provide symptomatic relief for those systems.The following are general guidelines for care based onsigns and symptoms. Your department must, however,develop protocols with assistance from a medical director.
Cardiopulmonary EffectsIn hazardous materials incidents, toxic substances thataffect the heart and lungs are usually inhaled. This maycause coughing, difficulty breathing, cyanosis, abnormalpulse or respiratory rates, or chest pain. If conscious, theindividual should rest in the position where breathing ismost comfortable; often this is a sitting position. Keep theaffected individual quiet and warm, administer oxygen, andcheck vital signs frequently. Very slow or very fast restingheart rates (less than 60 or greater than 100) and irregularheart beats are particularly important. Significant changesin either systolic or diastolic blood pressure should also benoted. In all cases, watch for vomiting and never leave theaffected individual unattended.
If the patient is unconscious but breathing, your prioritiesare to maintain an airway, administer oxygen, and monitorvital signs. If breathing has stopped, administer artificialrespiration.
A bag-value mask with oxygen can be used to deliverbreaths; however, it is much more effective to deliverbreaths through an endotracheal tube. Only those individu-als trained and experienced in advanced cardiac life supportand intubation should perform such procedures. Keeping inmind the “ABCs” of basic life support—Airway, Breathing,and Circulation—it is also essential to monitor the pulseand administer chest compressions if necessary. Again, ifpersonnel trained in advanced cardiac life support areavailable, protocols for treating cardiac arrhythmias shouldbe implemented.
Activity

12-30 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Skin and Eye Effects
Pain, irritation, redness, and other observable changes areindicators of toxic effects. The decontamination proceduresalready mentioned are the first steps in caring for theseinjuries. Continued flushing of skin, eyes, and mucousmembranes requires large amounts of water in a gentlestream from any source, such as an IV setup, bulb syringe,low pressure hose, or bucket. Flushing to counteract theeffects of a corrosive or irritant should be continued for atleast 20 minutes. Flushing should begin again if burning orirritation continues.
In some cases, it may be necessary to continue flushingprocedures during transport. If the effects of the corrosiveor irritant are minimal, and you have flushed the affectedarea for at least 20 minutes, dry the area gently and apply adry sterile dressing for transport. Wet dressings should notbe applied, particularly to burns from alkali corrosiveagents such as calcium carbide, sodium hydroxide, orpotassium hydroxide. If the skin is not fully decontami-nated, application of a wet dressing could result in a reac-tion between the alkali and the water. This reaction wouldgenerate heat, increasing damage to the affected area unlessenough water was applied to draw off the heat of the reac-tion.
In case of eye exposure, thoroughly flush the eyes andcover them with moistened pads, unless the exposureinvolves alkali corrosives. Under no circumstances shouldan individual rub the eyes. Alkali burns to the eyes are aserious emergency and the eyes must be irrigated for 30 to60 minutes with normal saline solution. Water may be usedif normal saline is not available.
Activity

Module 12: Patient Support 12-31
Student Text IAFF Training for Hazardous Materials: Technician©
Gastrointestinal SystemEffects
Many toxic substances absorbed through different routes ofentry can affect the gastrointestinal system. Nausea andvomiting are frequently seen with gastrointestinal expo-sures to a wide variety of toxicants.
Supportive measures that can be given on-scene includekeeping the affected individual quiet and comfortable.Never give food or fluid to someone who is feeling verynauseated or who has vomited. There is always the riskthat the individual will vomit, then inhale the food or fluid.
If a contaminant was ingested, consult the appropriatesources for information on emergency care procedures.Sources include regional poison control centers,manufacturer’s medical staff (manufacturer’s numbers canbe obtained from Material Safety Data Sheets or throughCHEMTREC), the Agency for Toxic Substances andDisease Registry, or written references. With many toxicsubstances, particularly corrosives, vomiting should not beinduced. Rather, the material should be diluted with wateror milk. If it is not clear that a specific action is appropri-ate, it is best to simply transport the individual to an emer-gency medical care facility as soon as possible.
Activity
Neurotoxicants
Toxic substances that affect the nervous system may causesigns and symptoms that range from headache to changesin mental status, altered sensation or muscle control, sei-zures, or loss of consciousness. It is important to carefullynote all symptoms, particularly any changes from baselinebehavior or ability. Central nervous system functions suchas speech, balance, memory, and personality may be af-fected. Assess peripheral nervous system functions, includ-ing fine motor control and sensation. Keep the affected

12-32 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
individual quiet and minimize stimulus to the patient, suchas lights and noise. Since the effects may be unpredictable,take vital signs frequently.
Activities

Module 12: Patient Support 12-33
Student Text IAFF Training for Hazardous Materials: Technician©
Patient Treatment—Agent-Specific CareAs discussed so far, the overall approach to emergency careat hazardous materials incidents involves gross decontami-nation, establishing an airway, breathing, and circulationand symptomatic treatment. In addition, there are severaltoxic agents for which specific treatments or antidotes areavailable.
Asphyxiants
Simple Asphyxiants
Asphyxiants are agents that produce hypoxia (low oxygenin the body’s tissues). As mentioned earlier, asphyxiantsare divided into two groups. Simple asphyxiants producehypoxia by displacing oxygen from the environment.Simple asphyxiants cause no effect other than filling theatmosphere and pushing out the oxygen.
• Examples of simple asphyxiants are nitrogen (N2),used as an industrial inerting gas; carbon dioxide (CO2),encountered in carbohydrate fermentation sites such asbreweries, grain elevators, and winery vats; methane(CH4), found in mine tunnels and manure storage tanks;and other combustible fuels (primarily short-chainhydrocarbons, including ethane (C2H6), propane(C3H8), and butane (C4H10).
• Signs and symptoms of exposure are caused by hy-poxia alone. Symptoms include headache, nausea,confusion, collapse, seizures, and death.
• Treatment for simple asphyxiants includes removingthe affected individual from exposure and delivering100% oxygen. Do not give high concentrations ofoxygen to people with severe chronic lung disease. Inthese cases, give lower concentrations of oxygen.Simple asphyxiants work only by producing an oxygen-deficient atmosphere, so there is no potential for sec-ondary contamination.

12-34 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Chemical Asphyxiants
Chemical asphyxiants act within the body to interfere witheither oxygen delivery to cells or oxygen use by cells. Thesymptoms caused by chemical asphyxiants are similar tothose caused by simple asphyxiants, but because of thedifferent mechanisms of action, there is the added danger ofsecondary contamination. The potential for asphyxiation ofunprotected emergency care personnel exists when achemical asphyxiant is carried on the skin or clothing of theaffected individual.
Common chemical asphyxiants include carbon monoxide,cyanide, and hydrogen sulfide, with carbon monoxide beingthe most likely to be encountered by emergency responsepersonnel.
Carbon Monoxide
Carbon monoxide (CO) exposure is the leading cause offatal poisoning in the U.S. It is commonly found in the fireenvironment. Carbon monoxide acts by binding to hemo-globin, the oxygen-carrying component of red blood cells.This “carboxyhemoglobin” cannot bind with oxygen. As aresult, the exposed individual becomes hypoxic because thered blood cells are unable to deliver oxygen to the body’scells.
• Examples of other situations that may produce carbonmonoxide are those that involve poorly functioningengines or heaters, or other sources of incompletecombustion.
• Signs and symptoms of carbon monoxide poisoningvary according to the level of exposure. At low levels,symptoms include headache, nausea, and possibly chestpain due to poor oxygenation of the heart muscle.Chest pain is usually seen only in individuals withunderlying heart disease. At moderate levels of expo-sure, symptoms may include confusion, dizziness, andloss of consciousness. High-level exposures result incollapse, seizures, and coma.

Module 12: Patient Support 12-35
Student Text IAFF Training for Hazardous Materials: Technician©
You will not see the “cherry red” skin associated withcarbon monoxide poisoning until there are very highlevels of carbon monoxide in the blood. You can makethe definitive diagnosis of carbon monoxide poisoningonly by obtaining a carboxyhemoglobin blood level.
• Treatment for carbon monoxide poisoning is adminis-tration of oxygen at 100% with non-rebreather mask.The usual exception for those people with chronic lungdisease applies here as well. It will help emergencyroom personnel make the diagnosis of CO poisoningand plan the appropriate treatment if you draw a car-boxyhemoglobin blood level at the scene prior tooxygen therapy and transport it with the affected indi-vidual to the hospital. Although carbon monoxide is achemical asphyxiant, the risk of secondary contamina-tion is low. This gas easily mixes with the atmosphere,so air concentrations of carbon monoxide are likely tobe low once the affected individual is moved to freshair.
Cyanide
Cyanide (CN) is highly toxic and rapidly fatal at highdoses. It is easily absorbed through all three routes ofexposure. Since secondary contamination can occur,emergency response personnel must take appropriateprecautions.
Hydrogen cyanide (HCN) is commonly used in the produc-tion of pesticides.
• Examples of other situations involving cyanide arepolyurethane foam fires. The combustion of someplastics, such as acrylonitrile, releases cyanide onburning. Hydrogen cyanide is also formed when acidscome in contact with a cyanide compound. It is foundin insecticide production, electroplating processes,metal processing, and other industrial settings.
• Signs and symptoms of cyanide poisoning includeheadache, dizziness, and confusion. This may progressto hyperventilation and tachycardia, and eventuallycollapse, seizures, coma, or death. Diagnosing cyanide

12-36 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
poisoning may be difficult. The classic “bitter almondsmell” associated with cyanide is unreliable, and itssymptoms are similar to those of carbon monoxidepoisoning. Unlike carbon monoxide poisoning, how-ever, routine tests for cyanide poisoning are typicallynot done. Thorough pre-incident planning and hazardidentification should alert emergency response person-nel that a cyanide hazard may be present.
• Treatment of symptoms associated with cyanidepoisoning requires 100% oxygen, assisted ventilation,insertion of IV lines, and cardiac monitoring. In indi-viduals with mild symptoms, this supportive care maybe sufficient for recovery. In individuals with moderateto severe symptoms, such as deterioration in mentalstatus, start specific treatment for cyanide poisoning.
The specific treatment of cyanide poisoning involvesseveral steps. If you expect to treat patients outside ahealth care setting, protocols and standing orders mustbe established beforehand. Those responsible foradministering the medications must be thoroughlytrained in these procedures. Kits for treatment ofcyanide poisoning are available.
Hydrogen Sulfide
Hydrogen sulfide (H2S) is a colorless gas with a smell ofrotten eggs. At low levels, hydrogen sulfide is an irritantthat affects mucous membranes, the eyes, and the skin.H2S is extremely caustic even at very low concentrations.
• Examples of situations that may produce H2S aresewers, crude oil storage tanks, crude oil pipeline leaks,coal mines, or anywhere that organic material is decom-posing.
• Signs and symptoms of exposure to hydrogen sulfideat moderate levels include respiratory tract irritation,headache, and dizziness. Continued exposure at highlevels may result in pulmonary edema, collapse, coma,and death. Since hydrogen sulfide deadens the sense ofsmell, it is possible for unprotected individuals to inhalefatal amounts of the gas without realizing it. Briefexposures to high levels (greater than 300 ppm) may

Module 12: Patient Support 12-37
Student Text IAFF Training for Hazardous Materials: Technician©
cause nearly instantaneous collapse. While there islittle risk of secondary contamination to emergencyresponse personnel, the affected person must be re-moved to an area far from the hydrogen sulfide sourcebefore care is given.
• Treatment for hydrogen sulfide exposure includesadequate ventilation and circulation. As with otherasphyxiants, the individual must be given maximumoxygen flow. Supportive care and oxygen may besufficient for recovery because the life of sulfides inoxygenated blood is short.
Toxicants that Induce Methemoglobinemia
Hemoglobin carries the oxygen component in blood. Thecondition known as methemoglobinemia impairs thisfunction. Mild methemoglobinemia (a low concentrationof this altered form in the blood) can be tolerated. Moresevere methemoglobinemias (greater than 25% methemo-globin relative to normal hemoglobin) are dangerous.
• Examples of chemicals that produce methemoglobin-emia are nitrites (NO2) and nitrates (NO3). Thesechemicals convert hemoglobin into methemoglobin.Methemoglobinemia may result from a number of drugand chemical exposures involving nitrites. Methemo-globinemia has also been associated with smoke inhala-tion. Depending on the agent and route of exposure,secondary contamination may result in methemoglobinformation.
• Signs and symptoms may include headache anddifficulty breathing with exertion. Higher levels ofmethemoglobin may produce lethargy, stupor, anddeath. These symptoms are the same as those of hy-poxia, although the concentration of oxygen in theblood is normal. Nitrate or nitrite exposure is alsolikely to result in dilation of the blood vessels, thereforetachycardia, hypotension, and cardiovascular collapsemay result. Cyanosis may appear before other signsand symptoms.
12-38 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
• Treatment for methemoglobin involves improvingoxygen delivery by assisting ventilation (if necessary)and administering 100% oxygen. Intravenous methyl-ene blue may be given as directed in standing protocols;hospitalization may be required for this. Methyleneblue is a reducing agent that counteracts the effects ofthe oxidizing agent. You must be trained to provide it,because side effects include chest pain and difficultybreathing. Individuals exposed to nitrites or nitratesand who are demonstrating signs and symptoms ofhypoxia (such as difficulty breathing or confusion)should be treated with methylene blue if permitted byprotocols.
Cyanosis is likely to occur with low methemoglobinlevels, so it is not, by itself, an indication for treatment.If administration of methylene blue is not effective,transport the patient to an appropriately equippedemergency department immediately.
Respiratory Irritants
Respiratory irritants are a broad class of chemically unre-lated substances encountered regularly by emergencyresponders. These compounds produce hypoxia by causinga chemical inflammation of the trachea and bronchi, upperairway obstruction, pulmonary edema, or pneumonia. Thelocation of injury in the respiratory tract depends on theduration of exposure and how deeply the material is in-haled.
Examples of respiratory irritants include ammonia, ac-rolein/aldehydes, hydrogen halides, acetic acid, nitrogenoxides, sulfur dioxide, chlorine gas, phosgene gas, andformaldehyde. In many cases, secondary contamination ispossible. Gases can be divided into two classes, based ontheir solubility in the respiratory tract.
Highly Soluble Irritant Gases
Highly soluble gases are those that dissolve easily in themoisture of the respiratory tract mucous membranes. Likeother irritant gas exposures, lung injury from chlorine gas isdue to the formation of acids, such as hydrochloric acid(HCl), on contact with mucous membranes. This leads to

Module 12: Patient Support 12-39
Student Text IAFF Training for Hazardous Materials: Technician©
tissue inflammation and the death of cells lining the respi-ratory tract.
• Examples of highly soluble lung irritants are ammonia,sulfur dioxide, and chlorine gas. Chlorine has wide-spread industrial use in cloth and paper bleaching, andin chemical and plastic processes. Exposure may resultfrom storage or transportation incidents involving thepressurized liquid form.
• Signs and symptoms include rapid onset of upperairway irritation, cough, laryngospasm, and wheezing.Eye and mucous membrane irritation may also be seen.
• Treatment includes irrigating eyes and skin, adminis-tration of humidified oxygen, and respiratory support asneeded. In the hospital, treatment with bronchodilatingmedication may be given.
Less Soluble Irritant Gases
Irritant gases that are less soluble are likely to cause onlyminimal symptoms related to upper airway irritation.
• Examples of less soluble irritant gases are the oxides ofnitrogen, such as nitrogen dioxide (NO2), found in grainsilos. Nitrogen oxides are also used in the manufactureof dyes, fertilizers, celluloid, and lacquers. Phosgene(COCl2) can cause symptoms as described above and iscapable of producing pulmonary edema. Solvents invapor form may also cause a pneumonitis.
• Signs and symptoms may include a slight cough orsore throat after exposure. Because they are lesssoluble, they are not absorbed through the lining of theupper respiratory tract. Instead, toxicants are inhaledinto the lowest part of the respiratory tract—the bron-chioles and alveoli—causing tissue irritation andswelling, called pneumonitis. Some effects, such aspulmonary edema, may be delayed, occurring eight totwelve hours after exposure.
• Treatment immediately following exposure is support-ive. Individuals who have inhaled an irritant gas mustbe transported to a hospital for observation in case ofdelayed onset of pulmonary edema.

12-40 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Hydrogen Fluoride
Activity
Hydrogen fluoride (HF) (hydrofluoric acid when dissolvedin water) is a direct skin, mucous membrane, and respira-tory irritant. It also has other toxic effects, which dependon route of entry, duration of exposure, total dose, andconcentration.
There are two types of corrosive injury following contactwith hydrogen fluoride. The first is a rapid dehydratingtype of tissue destruction, resulting from the reaction ofacid with the water in skin. A secondary injury occursmore slowly, resulting from the penetration of fluoride ionsthrough the skin. This fluoride from the hydrogen fluoridemolecule reacts with the calcium in blood and other tissues.In addition to tissue destruction, this reaction uses calciumthat is required for normal body functioning. The resultingdepletion of calcium in the blood can cause life threateningcardiac arrhythmias.
• Examples of situations in which you might find HF aremetal cleaning, glass etching and some refinery pro-cesses.
• Signs and symptoms following exposure to hydrogenfluoride gas (anhydrous HF) include coughing andburning of eyes and throat. This may progress topulmonary edema within 24 hours. Skin contact causessevere burns that may result in immediate or delayedpain and lead to calcium depletion. Eye exposurecauses acute inflammation of the protective covering ofthe eye. The damage to other structures of the eyecontinues for 24 hours as fluoride ions continue topenetrate the covering of the eyes.
• Treatment for exposure to HF includes removing thepatient from the contaminated area, assessing respira-tory status, and administering humidified oxygen forrespiratory tract irritation. Since the acid may result insecondary contamination, use caution when removingcontaminated clothing and delivering care. Contami-nated skin and eyes must be irrigated immediately withlarge amounts of saline for at least 20 minutes.

Module 12: Patient Support 12-41
Student Text IAFF Training for Hazardous Materials: Technician©
Solutions to bind the fluoride ions may be given at thescene. You can use 0.03% solution of benzalkoniumchloride (Zephiran) on affected skin, but it is too toxicfor use in the eye. You may also use calcium gluconateointment on skin burns at the scene. Monitor exposedindividuals with an EKG for cardiac effects of hypocal-cemia (prolonged QT interval) throughout treatmentand transportation.
OrganophosphateInsecticides
Organophosphate insecticides are compounds containingcarbon and derivatives of phosphorous. Most organophos-phate insecticides are easily and rapidly absorbed throughthe skin, membranes of the eye, gastrointestinal tract, andlungs.
• Examples of organophosphate insecticides arediazinon, malathion, and parathion.
Organophosphate insecticides cause toxic effects bycombining with an important enzyme in the body,acetylcholinesterase. The function of this enzyme isdeactivation of acetylcholine. Acetylcholine is impor-tant in transmitting nerve impulses to skeletal muscles.Acetylcholinesterase breaks down the acetylcholineafter the impulse is transmitted. Without acetylcho-linesterase, the impulse is transmitted continuously.Clinical effects of excessive acetylcholine are compli-cated.
• Signs and symptoms that can be remembered using theacronym DUMBELS:
• Diarrhea• Urination• Miosis (pinpoint pupils)• Bronchospasm (wheezing)• Emesis (vomiting)• Lacrimation (tearing in the eyes)• Salivation
12-42 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
• Treatment of organophosphate insecticide toxicityincludes the usual measures of decontamination andrespiratory support. Clean the exposed individual’s skinand hair with green soap (a soft soap made from veg-etable oils). Be careful to avoid secondary contamina-tion.
The specific antidote for organophosphate poisonings isatropine. Atropine is probably already available onmedic units, though probably in smaller doses thanthose needed for treatment of organophosphate poison-ings. Your unit should appropriate doses of atropine ifthese poisonings are likely, such as in farming areas.Treatment protocols or emergency department physi-cians should establish atropine doses. Another antidoteis pralidoxime (2-PAM) which is usually given withatropine. Again, protocols or physicians must be con-sulted for instructions on its use.
Patients poisoned by organophosphates may havedelayed symptoms and must be transported to an appro-priate health care facility for evaluation.
Smoke Inhalation
Because many hazardous materials incidents evolve fromfires, emergency response personnel may be exposed tosmoke through inhalation. There is a wide array of airbornetoxic substances in fire smoke.
• Examples of common toxicants include the chemicalspreviously discussed, such as simple asphyxiants,chemical asphyxiants, and respiratory irritants. Othermaterials, such as vaporized metals, can become air-borne in fire smoke.
• Signs and symptoms are difficulty breathing or hoarse-ness. Other signs may include wheezing, cough, andbloody sputum.
• Treatment should focus on removing the individualfrom the smoke, establishing an adequate airway, andassisting ventilation if necessary. Deliver oxygen at100%, except as previously discussed for individuals

Module 12: Patient Support 12-43
Student Text IAFF Training for Hazardous Materials: Technician©
with chronic lung disease. Use an intravenous line andcardiac monitoring for moderate to severe exposures.Check for the presence of toxicants that cause asphyxiasuch as carbon monoxide, hydrogen cyanide, andhydrogen sulfide.
Finally, individuals exposed to smoke that depositscontaminants on the skin must be thoroughly decon-taminated at the scene.
Heat/Cold
Heat Injuries
Emergency response personnel are often at risk for heat-related health effects because of the amount of personalprotective equipment they wear. In addition, patients aswell as emergency responders are at risk for these injurieswhen environmental conditions are hot and humid. Hyper-thermia, an abnormally elevated body temperature, candevelop when the body’s normal self-cooling processes areaffected. Protective clothing, physical exertion, highambient temperatures, and high humidity—alone or incombination—can contribute to the development of hyper-thermia.
Prevention of Heat-Related Injuries
Heat-related problems among emergency responders can beprevented by maintaining an appropriate level of physicalfitness. At an incident scene, heat stress can be avoided byscheduling rest breaks that are long enough for body cool-ing to occur; by maintaining adequate fluid intake, and bymonitoring all emergency responders on an ongoing basisfor early warning signs of heat stress. In hot climates,shaded areas must be provided for rest breaks. Emergencyresponders in the Cold Zone should be encouraged to takeadvantage of shelter, such as shade or air conditionedvehicles. Water must be freely available. At ambienttemperatures exceeding 70°F, fluid replacement is essential.
The normal thirst mechanism is not sensitive enough tosignal the need to drink water to replace lost fluids. Underhot conditions, such as working in encapsulated clothing,

12-44 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
emergency responders must drink at least 8 ounces of waterevery 30 minutes. Some local protocols may include theuse of a diluted commercially-available electrolyte fluid.
It is important to be aware of conditions that make emer-gency responders and civilians especially susceptible toheat-related problems. A person who is not accustomed tohot environments will have a more difficult time adjusting.Older age, obesity, or lack of physical fitness can alsoincrease susceptibility. Particularly important are tempo-rary conditions that may unexpectedly predispose a healthyemergency responder to a heat-related emergency. Theseinclude recent alcohol or drug use, sunburn, or recentillness (especially with fever or diarrhea). Also, an emer-gency responder might arrive at the incident in a fluiddeficient state, perhaps after working out or playing sports.
Heat Cramps
Effects of heat exposure range in severity from heat crampsto heat exhaustion and heat stroke. Heat cramps are painfulmuscle cramps, usually in the legs and abdomen, caused bythe loss of large amounts of fluid and salt through perspira-tion. Individuals with heat cramps perspire heavily and areoften extremely thirsty. Exhaustion, dizziness, or faintnessmay occur.
The most important objective in treating any heat-relatedcondition is to rapidly lower body temperature and replacelost fluids. Individuals who experience heat cramps shouldbe moved to a cool place as soon as possible. After rapiddecontamination, check vital signs. Give water or half-strength commercial electrolyte fluids. Massage thecramped muscles to ease discomfort. Any individual whoexperiences a heat-related illness must be monitored forbody temperature, heart rate, respirations, and normalperspiration, as well as the more serious signs and symp-toms of heat exhaustion or heat stroke. However, heatcramps do not necessarily precede more severe effects ofheat.

Module 12: Patient Support 12-45
Student Text IAFF Training for Hazardous Materials: Technician©
Heat Exhaustion
Heat exhaustion is often seen in people who work in hotenvironments or in encapsulated protective clothing. It is aform of shock caused by excessive fluid and salt loss.Signs and symptoms of heat exhaustion include heavyperspiration, rapid weak pulse, weakness, dizziness, andsometimes unconsciousness.
The individual experiencing heat exhaustion must undergoemergency decontamination. If there has been no perceivedexposure, it is acceptable to leave on some clothing. Other-wise, appropriate decontamination procedures require thatthe patient be completely undressed for secondary decon-tamination. Protect yourself from contaminants if second-ary decontamination is postponed in favor of rapid assess-ment and treatment.
In all cases the individual experiencing heat exhaustionshould receive flooding amounts of cool water over theskin. Other means of cooling include fanning and placingcool compresses or ice packs on the head, neck, axilla,groin, wrist, and ankles. The affected individual must rest.If the individual is conscious and is not nauseated or vomit-ing, give water or half-strength electrolyte fluid. Treatmentfor shock and administration of oxygen may be necessary.Some protocols may require that intravenous fluid be given.Though recovery from heat exhaustion is usually rapid, anaffected emergency responder should not be allowed toreturn to duty. Even in the absence of other signs andsymptoms, a responder with an oral temperature more than100.6°F (38.1°C) should not be allowed back to work.
Heat Stroke
Heat stroke is a medical emergency and is fatal in up to80% of cases if immediate treatment is not given. It occurswhen the normal temperature regulating mechanism failsand the body is unable to rid itself of excessive heat. Inresponse to fluid and salt loss, sweating stops and heat canno longer be lost through evaporation. Body temperaturerises rapidly. The cessation of sweating leads to a differentset of signs and symptoms from those seen in heat exhaus-tion. Respirations are deep, then become more shallow; thepulse is full and rapid; skin is red, flushed and dry; and the

12-46 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
body temperature is very high. There may be a change inthe level of consciousness, and seizures and muscle twitch-ing can occur.
In cases of heat stroke, focus on rapidly cooling the indi-vidual. After emergency decontamination, move the af-fected individual to a cool area. Flood the individual’s skincontinuously with cold water. Place cool packs as de-scribed earlier for heat exhaustion. Begin routine treatmentfor shock, give intravenous fluids, and administer oxygen.Monitor vital signs throughout this process and transportthe individual as soon as possible to an emergency medicalcare facility. Under no circumstances should body coolingbe stopped until core body temperature is reduced.
Cold Injuries
Cold-related injuries can occur in any environment whenbody heat is lost faster than it can be generated. Thepotential for cold-related injuries is greater when clothing iswet because water conducts heat away from the body muchfaster than air. Wind increases the effects of cold tempera-tures even further. Susceptibility to cold injuries is alsoincreased in individuals who are immobile, injured, ill, orunder the influence of alcohol.
Cold injuries can be divided into those that affect specificparts of the body, and those that cause a general cooling ofthe body, known as hypothermia. Injuries that affect aspecific part of the body may occur as a result of freezing,as in frostnip or frostbite, or may occur as a result of pro-longed cold, such as chilblains or immersion injury (trenchfoot).
Prevention of Cold-Related InjuriesAmong Personnel
Although acclimatization can increase resistance to heat-related injuries, the same is not true of cold-related injuries.The main defenses against cold injury among emergencyresponders are insulation provided by effective protectiveclothing and modification of emergency scene tactics.

Module 12: Patient Support 12-47
Student Text IAFF Training for Hazardous Materials: Technician©
Personnel must wear layers of insulating clothing andwaterproof gloves and boots. Because the environment ofan incident may make it impossible to keep gloves, socks,and other clothing dry, spare gloves and socks should beprovided at the scene during cold conditions. Betweencalls, wet clothing should be dried, or spare garmentsshould be available.
At the emergency scene, personnel should be rotated toallow rewarming. Because cold exposure greatly reducesthe touch sensation and normal endurance, work periodsmay have to be shortened. Since heat energy is producedby working muscles, sudden changes from high physicalactivity to inactivity may be accompanied by a dramaticdrop in body temperature. Under these conditions, be alertfor symptoms of hypothermia.
Freezing Injuries
Frostnip is the first stage of frostbite and tends to strike thenose, tips of ears, cheeks, toes, and fingers. It may berecognized more easily by someone other than the affectedindividual. The area first reddens, then turns pale or gray-white. The site is usually numb, though it may also ache ortingle.
If the exposure to cold is more prolonged and signs offrostnip are ignored, the area may develop a superficialfrostbite. The affected skin appears white and waxy andfeels frozen on the surface. If the deeper tissues are frozen,then deep frostbite, or freezing, has occurred. In suchcases, the skin can appear blotchy, grayish-yellow orgrayish-blue. This serious stage indicates tissue death andmay lead to loss of the body part.
The initial care for all freezing injuries is the same. Afterdecontamination, move the person to a warm area. Handlethe affected area very gently and carefully. Remove cloth-ing and jewelry from the site. Smoking cannot be permit-ted since this constricts blood vessels and delays warmingof extremities. If transport to an emergency medical carefacility is to be delayed for any reason, immerse the af-fected site in warm water (100°F to 105°F) without allow-ing it to touch the sides or bottom of the container. Keepthe person warm, without overheating, and watch the

12-48 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
affected area for the return of color. After the area is re-warmed, it should be dried gently and kept warm withoutapplying pressure to the site. Take extreme care to preventrefreezing the affected area. If the feet are affected, theindividual must not be permitted to walk. It is also veryimportant to avoid rubbing the affected site at any time afterfrostbite has been recognized.
Hypothermia
Hypothermia can be a very serious condition, leading todeath if untreated. Signs and symptoms progress fromearly shivering to feelings of numbness, drowsiness, slowedrespiratory and heart rates, visual deficits, uncoordinatedmovements, and unconsciousness. Core body temperaturesfall.
Hypothermia cases encountered by emergency responderswill probably be relatively mild, and can be treated bymoving the individual to a warm area following decontami-nation. Remove wet clothing and rewarm the individualslowly, using such measures as hot packs, hot water bottles,or hot air. Apply heat to the trunk, armpits, and groin. Heatshould not be applied to the extremities because this cancause blood to pool, leading to shock. If the individual isalert, give him or her warm liquids to drink slowly. Keepthe patient at rest. Administer oxygen if indicated. Monitorvital signs, including oral body temperature, during trans-port to an emergency medical care facility.

Module 12: Patient Support 12-49
Student Text IAFF Training for Hazardous Materials: Technician©
Transportation
Preparing for PatientTransportation
All emergency transport vehicles are kept in an uncontami-nated area to minimize the risk of contaminating the crew.All affected individuals must be decontaminated priorto being transported to a health care facility. Transport-ing contaminated individuals could create serious healthrisks for the transport crew and for the staff at the receivinghealth care facility. It is unlikely that the transport crew orhospital staff could be adequately protected from secondarycontamination. In addition, the seriousness of the incidentcould escalate with the continued contamination of newgroups of people remote from the incident scene.
After the patient is grossly decontaminated and treated,take added precautions to limit the spread of any con-taminants left on the patient. For example, the patientmay be clothed in a disposable gown, or placed on dispos-able (plastic coated) blankets. Supplies or equipment thatcome in contact with contaminated areas of the patient(such as blood pressure cuffs and stethoscope) should alsobe disposable. The patient should be wrapped in a dispos-able blanket, sheeting, or commercially-prepared victimtransport bag so that the contaminating substance cannotcome into contact with medical personnel, the ground, orthe ambulance.
Some departments have SOPs that require covering allexposed surfaces in the interior of the ambulance transportcompartment with plastic sheeting in cases where second-ary exposure is a possibility. A heavy gauge (3 to 4 mmthickness) plastic is typically used to minimize the possibil-ity of ripping or tearing. Alternatively, a pre-shaped remov-able protective housing may be prepared for use duringhazardous materials incidents. This program emphasizeseffective decontamination, making draping the inside oftransport vehicles unnecessary. Covering an ambulanceinterior should not be a routine procedure.

12-50 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Modes of Transportation
SOPs for transporting patients exposed to hazardous mate-rials must be developed in cooperation with the health carefacilities involved. Some emergency departments are betterequipped than others to handle patients who have beenexposed to hazardous materials. When preparing to trans-port patients, keep in mind the following:
• Any patients or personnel who may have becomecontaminated must go through decontamination beforeleaving the scene. This may require that the patient betransported in a second ambulance with an uncontami-nated crew.
• Any equipment that may have become contaminatedmust not be removed from the scene until it has beendecontaminated.
• Fax to the receiving facility (or send with the patient)any pertinent information, such as MSDSs or shippingpapers.
Whether air or ground transport is used, make sure theadmitting hospital is properly informed in advance and isprepared to treat victims of the specific hazardous materialsinvolved in the incident. The hospital should be updatedperiodically while the patient is being prepared and trans-ported. Hospitals should be informed of the following:
• The number of victims• The nature of exposure• Types of injuries• Treatment on-scene• Level of patient decontamination• Estimated time of arrival
The EMS unit should also verify with the hospital wherethe patient should be taken. Some hospitals have estab-lished special areas outside the emergency room that areequipped to handle potentially contaminated patients.

Module 12: Patient Support 12-51
Student Text IAFF Training for Hazardous Materials: Technician©
Ground Transport
Your vehicle must be considered contaminated as soon as ithas been used to transport victims. After arrival at a treat-ment facility, the vehicle must not be left unattended be-cause of the possibility that unauthorized persons will comein contact with contamination on the vehicle. All emer-gency personnel who were in the ambulance with thepatient must also be considered contaminated, and mustundergo proper decontamination procedures for theirprotection.
Air Transport
Patients who may still be contaminated (even after fielddecontamination) should not be transported by air. Ifpatients from a hazardous materials incident are transportedby helicopter, several precautions should be observed.
• The helicopter agency should be contacted well inadvance to determine procedures regarding patienttransport
• Landing sites should be as far from the incident aspractical and should not cause air movement toward thetriage area
• The landing zone must be a minimum of 100 feet indiameter
• The pilot’s radio frequency should be known to theIncident Commander and flight paths should be down-wind of the incident when entering and upwind whenleaving
While En Route• Continue to monitor symptoms and make physical
assessments of victims
• Continue to irrigate eyes or affected skin as necessary,although this may be difficult while in motion
• Continue oxygen administration as indicated

12-52 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
• Start recommended treatment communicated by physi-cians at the admitting hospital
• Update triage tags with all treatment to date
• Verify where to take the patient
Clearance for Return to Scene
If the ambulance has not been decontaminated, you may ormay not be able to return to the scene to transport morepatients. You must consider the following:
• Risk of additional crew exposure during travel
• Risk of contaminating other patients
• Availability of additional emergency vehicles if possi-bly contaminated vehicles are not reused
• Minimization of the number of vehicles used (andtherefore, needing decontamination) at the end of theincident
Activity

Module 12: Patient Support 12-53
Student Text IAFF Training for Hazardous Materials: Technician©
Termination andPost-Incident Phase
Post-Event Considerations
Personal Cleanup
The experienced professional never assumes he or she is“free” of contamination after an incident. Medical person-nel must be decontaminated according to the establishedpolicies of the environmental agencies and industry experts.Sometimes clothing and jewelry must be discarded if theycannot be decontaminated. Contact your local departmentof environmental protection, the product manufacturer, orother sources for specific decontamination procedures.
Be careful removing protective outerwear so you do notcontaminate yourself. Be especially careful of the soles ofshoes, cuffs on pants, and other crevices in clothing. Ingeneral, do not wear home any potentially contaminatedarticle of clothing (including underwear) that has not firstbeen laundered. All clothing worn at the emergency sitemust be decontaminated and laundered before being wornagain. Remember that contaminated clothing may be a firehazard if not washed immediately.
All EMS personnel involved in the incident must showerand change clothes. Head and body hair should be thor-oughly cleaned when showering to remove any fine con-taminants such as dusts. If possible, this shower should beset up at the scene to minimize the potential spread ofcontaminants.
Vehicle Cleanup
The response vehicle and equipment must be decontami-nated according to the established policies of environmentalagencies and industry experts. Decontamination must takeplace before the vehicle returns to service. Resources suchas your local department of environmental protection,health department, or product manufacturer can providespecific decontamination procedures.

12-54 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Review
Hold an EMS review session immediately following theincident to cover the following topics:
• The need for a Critical Incident Stress Debriefing
• Areas of strongest performance
• Areas needing additional work
• Additional personnel and equipment needed for futureincidents
• Equipment that was unnecessary
• Restocking requirements
Activity

Module 12: Patient Support 12-55
Student Text IAFF Training for Hazardous Materials: Technician©
Application Exercise

12-56 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-57
Student Text IAFF Training for Hazardous Materials: Technician©
Application Exercise
You will need
• EMS units and equipment• A “scenario and symptom” index card for each student (described below)• Departmental medical protocols• A copy of departmental patient assessment forms• A copy of the Competency Checklist for each student
Preparation
This exercise is intended to give students hands-on experience in identifying symptoms of chemi-cal exposures and administering the most appropriate treatment. The specific procedures you useshould follow departmental medical protocols.
In advance of the exercise you will need to prepare “scenario and symptom” cards for eachstudent. On each card describe:• A hazardous materials incident with identified or unidentified chemical(s). There will be two
“patients” for every “incident”, so prepare two cards describing the same incident.• Signs and symptoms of possible chemical exposure, heat stress, or cold stress (based on the
incident described). Vary the signs and symptoms for the two patients in the scenario.• Condition of the patient (e.g., conscious and ambulatory; unconscious with no pulse). Vary
the condition of the two patients in the scenario.
At the beginning of the exercise, position the EMS unit and supplies. Divide the class intogroups of four; assign two to act as patients and two to act as EMS personnel. (Have the otherstudents observe, unless additional EMS units and instructors are available to conduct more thanone group at a time). Distribute a “scenario and symptom” card to the two patients. Instructthem to read their cards then pass them to the EMS personnel in their group.
Instruct the EMS personnel to read the cards and take action as they would in an actual incident;for example, they should administer the appropriate treatment, complete the patient assessmentforms, notify the receiving hospital, etc. (They should assume emergency decontamination hasbeen performed). In some cases EMS personnel may want or need additional information. Beprepared to give additional details as necessary (e.g., weather conditions).
Have the members of the group switch roles and repeat the exercise. Then assign another groupto carry out their scenarios. Continue until each student has had an opportunity to serve as bothpatient and EMS provider. Complete the Competency Checklist on the following page for eachstudent.

12-58 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Competency Checklist
Name of Student:
_________________________________________________________________
Indicate student competency in the following areas.
Did the student:Yes No
Accurately assess the patient, based on the situation and symptoms?
Prioritize patients, if one was more severely injured than the other?
Check patient vital signs?
Ask questions for additional information?
Take steps to avoid secondary contamination?
Administer the appropriate treatment, based on the situation and symptoms?
Contact the receiving hospital?
Supply all pertinent information to the receiving hospital?
Follow all medical protocols as required by SOPs?
Remarks (including skills to be improved):
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________

Module 12: Patient Support 12-59
Student Text IAFF Training for Hazardous Materials: Technician©
Action Statement

12-60 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-61
Student Text IAFF Training for Hazardous Materials: Technician©
Action Statement
You have just completed the twelfth module of the Hazardous Materials Technician course. Thetopics included:
• Personal Protective Equipment• Pre and Post Entry Assessment of Personnel• Patient Care• Support Care• Patient Treatment—Agent-Specific Care• Transportation• Termination and Post-Incident Phase
Knowing how you respond to emergencies in your first due areas, would you change your actionsor habits based on the information covered in this module? Listed below are some suggestedactions. Some you may already do, and others may not fit your work environment. If there areactions you have not done in the past, do you think you will begin doing them as a result of thistraining?
As a result of this training I will:
1. Refresh my EMT skills2. Take more care to avoid secondary contamination when treating patients3. Read my department medical protocols for patient support4. Research or practice patient support in special situations, such as for exposure to radia-
tion or infectious agents5. (Create my own action statement)
______________________________________________________________________________

12-62 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-63
Student Text IAFF Training for Hazardous Materials: Technician©
Appendix A
Activities

12-64 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-65
Student Text IAFF Training for Hazardous Materials: Technician©
Entry Team Assessments Activity 1
Student Instructions
Conduct a physical assessment of your assigned entry team member. Use the form on the fol-lowing page or one provided by your instructor.

12-66 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-67
Student Text IAFF Training for Hazardous Materials: Technician©
Decontamination Activity 2
Instructor Notes
Verbally describe the following scenarios to the students and discuss the treatment and methodsfor preventing secondary contamination.
1. A cargo tank rolls over on an interstate. The driver is unconscious, lying outside the cab,and is drenched in diesel fuel. No other chemical hazards are present.
2. A forklift operator carrying a drum of sodium hydroxide powder accidently drops thedrum. The lower half of his body is contaminated.
3. A hardware store employee is splashed on the face and arms with an organophosphatepesticide when a shelf collapses.
4. Three chemistry students are splashed in the eyes with sulfuric acid during a chemistrydemonstration.
5. A fire fighter complains of shortness of breath after a fire involving polyurethane foammattresses.
6. A fire fighter in turnout gear but no SCBA is exposed to sodium hydroxide. Emergencymedical personnel treating the fire fighter receive secondary contamination.

12-68 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-69
Student Text IAFF Training for Hazardous Materials: Technician©
Triage Activity 3
Student Notes
Your instructor will divide you into two groups. Half of you will be “patients” and receive anindex card with specific information. The other half will act as EMS personnel and prioritize thepatients, based on the information they give you. Interview all the patients and complete thetriage form below. Give a brief reason why each patient is prioritized as such.
Patient Triage Reason/Description Number Priority

12-70 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Module 12: Patient Support 12-71
Student Text IAFF Training for Hazardous Materials: Technician©
Activity 4Cardiopulmonary Effects Worksheet
Sign
s an
d Sy
mpt
oms
Tre
atm
ent
T
reat
men
t
Tre
atm
ent
(
pati
ent
cons
ciou
s)
(p
atie
nt u
ncon
scio
us
(p
atie
nt n
ot b
r eat
hing
) b
ut b
reat
hing
)

12-72 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-73
Student Text IAFF Training for Hazardous Materials: Technician©
Activity 5Skin and Eye Effects Worksheet
Sig
ns a
nd S
ympt
oms
Tre
atm
ent
(gen
eral
)T
reat
men
t (c
orro
sive
s in
volv
ed)

12-74 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-75
Student Text IAFF Training for Hazardous Materials: Technician©
Activity 6Gastrointestinal Effects Worksheet
S
igns
and
Sym
ptom
s
T
reat
men
t
Tre
atm
ent
(if
no
naus
ea/v
omit
ing)
(if
naus
ea/v
omit
ing
is p
rese
nt)

12-76 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-77
Student Text IAFF Training for Hazardous Materials: Technician©
Activity 7Neurotoxicant Effects Worksheet
S
igns
and
Sym
ptom
s S
igns
and
Sym
ptom
s
Tre
atm
ent
(C
NS)
(P
NS)

12-78 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-79
Student Text IAFF Training for Hazardous Materials: Technician©
Supportive Care Activity 8
Complete the matrix below for each chemical. Use only the reference books given to you byyour instructor.
Compare your answers with the rest of the class and discuss the differences among referencesources.
Chemical Effect Supportive treatment
Cardio- Skin/ Gastro- Nervous pulmonary Eyes intestinal System
Picric acid
Ethylene
Hydrogenperoxide
Mercurymetal
Liquid phenol

12-80 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-81
Student Text IAFF Training for Hazardous Materials: Technician©
Hydrofluoric Acid Case Study Activity 9
NEW YORK--A city sanitation worker died after inhaling the fumes of a corrosive acid from adiscarded container that burst under the compacting blades of a garbage truck making routinecollections in Brooklyn.
Fire Department hazardous materials experts identified the substance as hydrofluoric acid, oftenused to etch glass.
A second sanitation worker was injured in the incident, which touched off an investigation bypolice and sanitation departments and raised the possibility of homicide charges against thoseresponsible for leaving the acid to be picked up.
A spokesperson for the Department of Sanitation said the incident was avoidable. “The appro-priate procedure in this case would have been to notify the Department of Environmental Protec-tion, and they will then recommend the proper procedure for disposal,” he said.
The dead man was identified as Michael Hanly, 49, of Brooklyn, a Sanitation Department workerfor 22 years. His injured partner, who suffered burns on the face and hands when he came toHanly’s aid, was identified as Thomas Giammarino of Staten Island, a member of the departmentfor 15 years who was listed in stable condition at the burn unit, where he was held for furtherobservation.
“People are unaware of what they dispose of and how they dispose of things,” the spokespersonsaid. “Frequently, sanitation workers are stuck by needles. People many times dispose of liquidthinners and paints and so forth. When the cans break open, they spatter. In this case, this is avery caustic acid.”
The incident began around 9:00 a.m. when Hanly and Giammarino were working their regularcollection route. Their truck was nearly loaded when one of them picked up a parcel and threw itin the back. One of the workers was cycling the blades to compact. The other turned away topick up the hydrofluoric acid which sprayed out.
Hydrofluoric acid burns are like fire, dehydrating the skin. As little as a drop generates extremepain. Hanly inhaled the acid, leading to his death in the emergency room of New York Hospital.Giammarino, who was 10 or 15 feet away collecting other refuse when the acid container burst,rushed to his aid and pulled his partner away from the truck.
The injured workers were taken to the Manhattan hospital in a Fire Department ambulance, whilea Fire Department hazardous materials team set about identifying the volatile material. The FireDepartment ordered and took part in the detoxification of the emergency room, hospital crew, itsown personnel, and members of the ambulance crew. For a time, the hospital’s emergencyentrance was closed off for decontamination.
Edited from The New York Times, November, 1996

12-82 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Questions
Using the resources you have available, answer the following questions.
1. How toxic is hydrofluoric acid?
2. What are the health effects of exposure to hydrofluoric acid?

Module 12: Patient Support 12-83
Student Text IAFF Training for Hazardous Materials: Technician©
Patient Assessment Activity 10
You arrive at the scene of a major accident at a water treatment plant. Apparently, three employ-ees were working in an underground tank when two collapsed. The third collapsed as he wastrying to climb to the manhole. None was wearing breathing apparatus. A fire fighter whoattempted a rescue entered the tank, but temporarily removed his breathing apparatus in order tofit through the manhole. Although his buddy handed him the SCBA after he entered the tank, thefire fighter was overcome by vapors before he could put it on.
When your EMS unit arrives at the scene, the four victims have been removed from the tank. Asyou prepare to treat the patients, what are three important questions you should be asking your-self?

12-84 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-85
Student Text IAFF Training for Hazardous Materials: Technician©
The Medical Team Activity 11
On arrival at the scene of a hazardous materials accident, you and two other EMTs are assignedto treat two victims of a corrosive spill. Command places you in charge of the medical treatmentsector. He informs you that both victims were splashed on the legs when a 55-gallon drum ofphosphoric acid (technical grade) was dropped from a pallet. After receiving gross decontamina-tion, the victims are carried by backboard from the site of the accident to your location, approxi-mately 300 feet from the spill. When the patients arrive at the treatment area, they present in thefollowing manner:
Patient #1 is experiencing respiratory distress and has a decreased level of consciousness. Hehas chemical burns over thirty percent of his body; both legs and abdomen are involved. Thehead, neck and chest seem unaffected. This patient is a 45-year old male with a history ofasthma. His vitals are:1. B.P. = 110/602. Pulse = 120 (weak)3. Skin = pale and wet (discolored in the burned area)4. Respirations = 30 (w/wheezes)5. Pupils = midpoint and reactive
Patient #2 is in severe pain, but is alert and oriented. He has severe chemical burns covering bothfeet with some burn areas on the lower parts of both legs. The rest of his body seems unaffected.He is also complaining of breathing difficulty. This patient is a 26 year old male with no pastmedical history. His vitals are:1. B.P. = 140/802. Pulse = 110 (strong)3. Skin = warm and wet (discolored in the burned areas)4. Respirations = 2455. Pupils = midpoint and reactive
Using the above information, answer these questions:
1. What level of protective clothing would you require for your medical team?
2. How would you assign your personnel?

12-86 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
3. How would you treat patient #1?
4. How would you treat patient #2?
5. What requests would you make of Command?
6. Describe the communications that would take place (who and what) in order to provideappropriate medical care for these patients?

Module 12: Patient Support 12-87
Student Text IAFF Training for Hazardous Materials: Technician©
Appendix B
Entry Team Assessment FormsExposure Report Forms

12-88 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-89
Student Text IAFF Training for Hazardous Materials: Technician©
Entry Team Assessment Form (Example 1)

12-90 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-91
Student Text IAFF Training for Hazardous Materials: Technician©
Entry Team Assessment Form (Example 2)

12-92 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-93
Student Text IAFF Training for Hazardous Materials: Technician©
Pre-Incident Entry Survey (Example 3)
Prior to entry evolutions, a pre-incident entry physical examination must be completed. Theseexams will be performed by EMS personnel. The results of this survey will indicate whichfunctions, if any, the hazardous materials team member may perform. In order to adequatelytrack each member’s condition, each section of the exam has been developed to place the hazard-ous materials responder into one of four possible categories as listed below:
Status 0 The responder can perform any task on a hazardous materials incident.
Status 1 A minor condition exists that will need to be reevaluated in 15 - 20 minutes.During this time period, the responder will stay at rest and have no assignment. Ifafter 15 - 20 minutes this evaluation does not improve or worsens, the responderwill be placed into Status 2.
Status 2 A condition is present that will not allow a responder to perform any physicallydemanding or stressful work. This person will be reevaluated in 15-20 minutes toassure that the condition does not worsen. If after 15 - 20 minutes the conditiondoes not improve or worsens, the responder will be placed into Status 3.
Status 3 A serious condition exists that excludes the responder from any activity. TheEMS personnel should consider whether this person should be transported to thehospital. If a question exists, the Medical Surveillance Officer or Medical Controlshould be consulted. Any person placed in this status will have at least a 24 hourperiod of no hazardous materials activity. At that time, he/she may be reevaluatedand appropriate assignments made.

12-94 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Pre-Incident Entry Survey ComponentsA. Blood Pressure B. PulseSystolic: Diastolic:100 -150 Status 0 Less than 90 Status 0 50 - 110 Status 0*Less than 100 Status 1 95 - 100 Status 1 *Less than 50 Status 1Greater than 150 Status 1 Greater than 100 Status 2 Greater than 110 Status 2
C. Respirations D. Temperature12 - 20 Status 0 96 - 100 Status 0Less than 12 Status 1 Less than 96 Status 1Greater than 20 Status 2 Greater than 100 Status 2
E. Weight To be recorded while responder is in shorts or coveralls. (Allow two pounds for coveralls.)
F. Skin Check appearance for any rashes or abnormalities. Document size and location of rashes. It will be thediscretion of the EMS personnel to determine whenever the rash, abnormality, etc. will allow the member to performcertain tasks. Personnel with open or weeping wounds should generally not be working in situations where skinabsorption of a toxin is possible.
G. Eyes Check pupils for size and reactivity. Check eyes for appropriate movement. Comparisons should be madewith the baseline exam to determine abnormalities. If gross differences exist, refer to physician. Status 3
H. Lungs Listen for wheezes, rales, bilateral equal sounds. If wheezes, rales, unequal breath sounds exist, theresponder will be placed in Status 2 or Status 3 per the discretion of EMS personnel.
I. Heart Any chest pain Cardiac arrhythmia (with the exception of sinus arrhythmia) Status 3
J. Abdomen Any abdominal pain/cramping Status 2Nausea or vomiting Status 2Diarrhea Status 2
K. Musculoskeletal At the discretion of the EMS personnel, any member with a recent or ongoing injury may beplaced into Status 2.
L. Recent Medical History If a member has had a condition that required absence from work within 48 hours ofthe response, a Status 2 is indicated.
M. Current Medications If a member is taking one of the following medications he/she will not be allowed towear encapsulated clothing: Phenothiazines, bronchodilator, narcotics, antihistamine, decongestants or antibioticsfor respiratory, ear, or GI problems.
N. Other If a member is under current treatment for middle ear, respiratory, genitourinary or gastrointestinalproblems, SCBA or encapsulated clothing should not be worn. Any other components or findings not listed abovewill be categorized at the discretion of EMS personnel.
O. If a member has had a condition that prevented working for three or more days within the past seven days, thatmember shall not be put in a position that requires the use of protective clothing.
P. If a member has a condition that requires wearing a cast, brace, etc., that team member shall not participate in acombat type position (unless cleared by a physician). Consideration should be given to his/her working in a com-mand function.
Q. A pre-incident exam worksheet (attached) will be completed on all members going through the exam. It will beheld on file for comparison to the post-incident exam. All findings are to remain confidential.
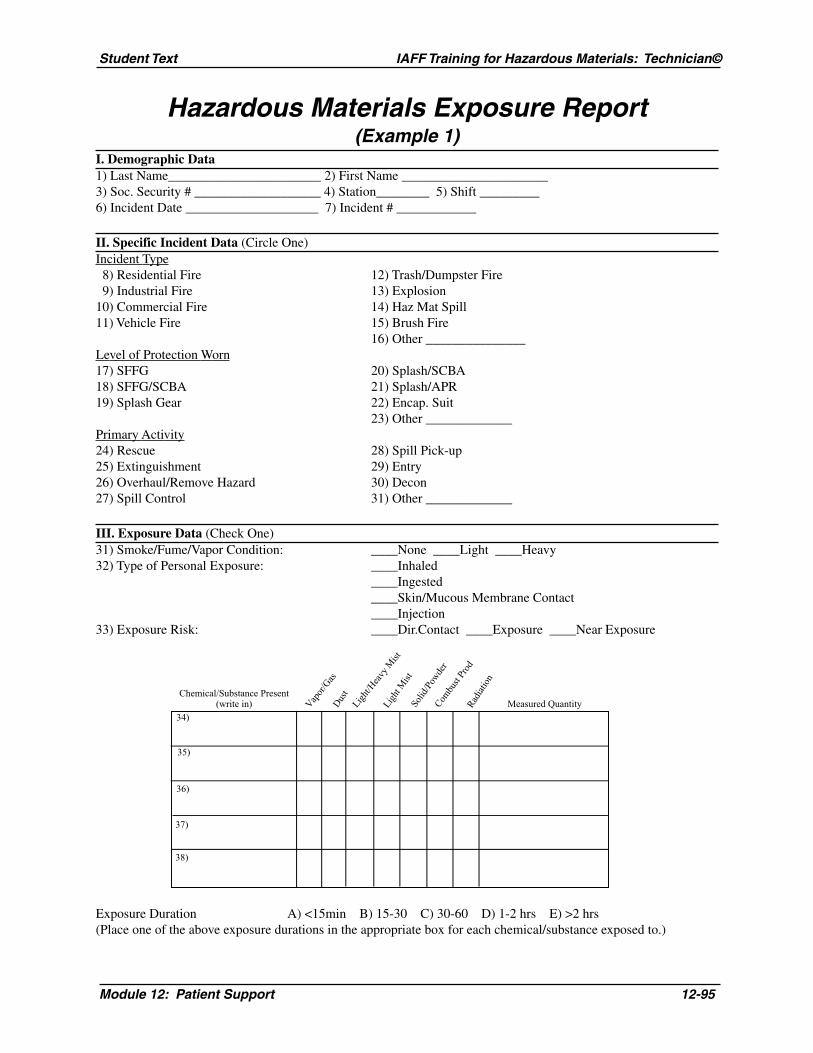
Module 12: Patient Support 12-95
Student Text IAFF Training for Hazardous Materials: Technician©
Hazardous Materials Exposure Report(Example 1)
I. Demographic Data1) Last Name_______________________ 2) First Name ______________________3) Soc. Security # ___________________ 4) Station________ 5) Shift _________6) Incident Date ____________________ 7) Incident # ____________
II. Specific Incident Data (Circle One)Incident Type 8) Residential Fire 12) Trash/Dumpster Fire 9) Industrial Fire 13) Explosion10) Commercial Fire 14) Haz Mat Spill11) Vehicle Fire 15) Brush Fire
16) Other _______________Level of Protection Worn17) SFFG 20) Splash/SCBA18) SFFG/SCBA 21) Splash/APR19) Splash Gear 22) Encap. Suit
23) Other _____________Primary Activity24) Rescue 28) Spill Pick-up25) Extinguishment 29) Entry26) Overhaul/Remove Hazard 30) Decon27) Spill Control 31) Other _____________
III. Exposure Data (Check One)31) Smoke/Fume/Vapor Condition: ____None ____Light ____Heavy32) Type of Personal Exposure: ____Inhaled
____Ingested____Skin/Mucous Membrane Contact____Injection
33) Exposure Risk: ____Dir.Contact ____Exposure ____Near Exposure
Exposure Duration A) <15min B) 15-30 C) 30-60 D) 1-2 hrs E) >2 hrs(Place one of the above exposure durations in the appropriate box for each chemical/substance exposed to.)
Chemical/Substance Present(write in)
34)
35)
36)
37)
38)
Vapor
/Gas
Dus
tLig
ht/H
eavy
Mist
Solid
/Pow
der
Combu
st Pr
od
Ligh
t Mist
Radi
atio
n
Measured Quantity

12-96 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
IV. Scene symptoms (Check Response)AT AFTERINCIDENT INCIDENT____39) Eyes Burn ________40) Cough ________41) Nose Bleed ________42) Resp. Irritation ________43) Nausea/Queasiness ________44) Dizzy/Lt. Head ____
AT AFTERINCIDENT INCIDENT____45) Headache ________46) Skin Irritation ________47) Skin Rash ________48) Other ________49) Other ____
V. Scene Medical Surveillance (Circle One)50) Pre Entry Assessment Done NO YES Pre-entry
___BP/P ___R ___T ___EKGPost-entry
___BP/P ___R ___T ___EKG51) Decontamination Performed NO YES
52) On Scene Treatment NO YES ___Oral Fluids___O2
___IV___Other
53) Transported to ED NO YES Hospital____________
VI. Post Incident Analysis By Dept. Surveillance Officer54) Form Reviewed On ____/____/____
55) MD Physical Exam Needed NO YES DR_____________
56) LAB/X-ray Needed: NO YES DONE ON____/____/____
57) Results discussed with individual on _______________________
58) Final Disposition: Full Duty___Light Duty___Injury Leave___Other___
Signature_____________________________________________
Date_________________________________________________

Module 12: Patient Support 12-97
Student Text IAFF Training for Hazardous Materials: Technician©
Hazardous Materials Exposure Report(Example 2)

12-98 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-99
Student Text IAFF Training for Hazardous Materials: Technician©
Hazardous Materials Exposure Report(Example 3)

12-100 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Example 3 Instructions
Name/SS#/Date: Please enter your name, social security number and date in the spaces provided.
Incident #: Please enter the incident number, if appropriate, during which the exposureoccurred. If the exposure occurred at the fire station or during a drill, pleaseenter Fire Station or Training Site. (FS or TS)
Location: Enter the specific location if known.
Incident Type: Please choose the type of incident that best describes the event during which theexposure occurred. If the correct type is not listed, please choose from item 11and explain.
Primary Activity: Please choose the activity most closely responsible for the exposure. If no listedactivity is appropriate, please choose from item 12 and explain.
PPE: Place a check mark or an “X” beside each piece of Personal Protective Equip-ment that you used during the event that resulted in the exposure.
Area Exposed: Place a check mark or an “X” beside the body area(s) that was exposed.
Type of Exposure:(EMS) If the exposure is related to an EMS event, please indicate the specific type of
exposure that occurred. Please be sure a designated officer is notified.
Symptoms: If you experienced symptoms as a result of your exposure, please indicate whichones by entering a check mark or “X” beside all those that apply. You need notexperience immediate symptoms to have an exposure. Members engaged ininterior fire fighting or vehicle fire fighting receive an exposure even though theymay not experience symptoms.
Medical AttentionRequired: Please indicate whether or not medical attention was required. If medical
attention was required, please be sure to complete all other pertinent information.
Type of AgentExposed To: Place a check mark or an “X” beside the broad category that applies. For
example, interior structural fire fighting would result in a chemical exposure andcould also result in a physical exposure from heat. An EMS exposure fromvomitus would be biological exposure.
Specific Products/SubstancesToxins: If you know the material responsible for the exposure, please indicate it here.
Blood or body fluid might be appropriate for an intact skin exposure during anEMS call. Products of combustion might be available for a single-family dwellingfire when no other specific information is available.
Length ofExposure: Please estimate the amount of time you were exposed.

Module 12: Patient Support 12-101
Student Text IAFF Training for Hazardous Materials: Technician©
Appendix C
Physician Information

12-102 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-103
Student Text IAFF Training for Hazardous Materials: Technician©
Physician Information
What information should be provided to the examining physician?
Your employer must provide specific information to the health care provider conducting a medi-cal surveillance exam under the OSHA or EPA regulations. This information should help thephysician or other provider understand the nature of your work. This information includes:
A. A copy of 29 CFR 1910.120, The Hazardous Waste Operations and Emergency ResponseStandard
B. A description of the employee’s duties as they relate to his or her exposure
C. The employee’s previous exposure levels and anticipated exposure levels
D. A description of any personal protective equipment used or to be used
E. Information from the employee’s previous medical exams that is not readily available tothe examining physician
Physician’s Written Opinion
The physician writes his or her opinion regarding the employee’s fitness for duty. Copies of thewritten opinion must be sent to both the employer and the employee. Medical records regardingspecific conditions that the employee may have are confidential, so they must be maintainedseparate from personnel records.
The opinion must include:
A. Results of the medical exam and tests (available to the employee only)
B. Physician’s opinion as to whether the employee has any detected medical conditions thatcould increase risk of health impairment
C. Physician’s recommended limitation, if any, on the employee’s assigned work
D. A statement that the employee has been informed by the physician of the results of themedical exam and any medical conditions that require further exam or treatment
The written opinion obtained by the employer should not revealspecific findings or limitations unrelated to occupational exposure.
12-104 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-105
Student Text IAFF Training for Hazardous Materials: Technician©
Appendix D
Record Keeping

12-106 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-107
Student Text IAFF Training for Hazardous Materials: Technician©
Record Keeping
Maintenance and access to medical records must be performed in accordance with OccupationalSafety and Health Administration regulations. Additional guidelines can be found in NFPA1500. OSHA regulations require the employer to maintain medical records on exposed workersfor 30 years after they leave employment (29 CFR Part 1910.120). The results of medical testingand full medical records must also be available to the worker, his/her union representatives, andOSHA inspectors. To ensure confidentiality, medical records should be maintained only by thehealth care personnel who provide occupational health services to the exposed employee, ratherthan by the employer.
• The employer must retain the name and social security number of the employee, thephysician’s written opinion, any employee medical complaints related to exposureto hazardous substances, and a copy of the information provided to the examiningphysician by the employer.
• Record keeping and reporting of occupational injury and illnesses must be per-formed annually (29 CFR Part 1904).
• The medical surveillance program must be reviewed periodically. During thisreview, information on specific exposures, working conditions, and use of protectiveequipment must be incorporated into the analysis.
Exposure records or incident reports of exposures completed after each applicable responsecould be extremely important to your health care provider. These reports may also provide thelegal proof needed in a contested Worker’s Compensation claim in the future. In addition, suchrecords help health and safety representatives and medical personnel keep track of potentiallyexposed responders who may require medical follow-up. Fire fighters and paramedics arestrongly encouraged to document and keep copies of all work-related exposures.

12-108 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-109
Student Text IAFF Training for Hazardous Materials: Technician©
Appendix E
Hazardous Toxicants, Their Effects,and Medical Monitoring

12-110 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-111
Student Text IAFF Training for Hazardous Materials: Technician©
Hazardous Substanceor Chemical Group
AromaticHydrocarbons:BenzeneEthyl benzeneTolueneXylene
Asbestos (orasbestiformparticles)
HalogenatedAliphaticHydrocarbons:
Carbon tetrachlorideChloroformEthyl chlorideEthylene dibromideEthylene dichlorideMethyl chlorideMethyl chloroformMethylene chlorideTetrachloroethane
(perchloroethylene)TrichloroethyleneVinyl chloride
Target Organs
BloodBone marrowCentral Nervous System (CNS)EyesRespiratory systemSkinLiverKidney
LungsGastrointestinal system
CNSKidneyLiverSkin
Potential Health Effects
All cause:CNS depression: decreased
alertness, headache, sleepi-ness, and loss of conscious-ness.
Defatting dermatitis.
Benzene suppresses thefunctioning of bone marrow(which makes white and redblood cells). Chronic exposurecan cause leukemia.
Note: Because other aromatichydrocarbons may be contami-nated with benzene, relatedhealth effects should beconsidered when exposure toany of these agents is suspected.
Chronic effects:Lung cancerMesotheliomaAsbestosisGastrointestinal malignancies
Asbestos exposure coupled withcigarette smoke has been shownto have a synergistic effect in thedevelopment of lung cancer.
All cause:CNS depression: decreased
alertness, headache, sleepi-ness, and loss of conscious-ness.
Kidney changes: decreased urineflow, swelling (especiallyaround eyes), and anemia.
Liver changes: fatigue, malaise,dark urine, liver enlargement,and jaundice.
Vinyl chloride is a knowncarcinogen; several others in thisgroup are potential carcinogens.
Medical Monitoring
Occupational/general medicalhistory emphasizing priorexposure to these or other toxicagents.
Medical examination with focuson liver, kidney, nervous system,and skin.
Laboratory testing:Complete blood count (CBC)Platelet count
Measurement of kidney and liverfunction.
History and physical examina-tion should focus on the lungsand gastrointestinal system.
Laboratory tests should includea stool test for occult bloodevaluation as a check forpossible hidden gastrointestinalmalignancy.
A high quality chest x-ray andpulmonary function test mayhelp to identify long-termchanges associated with asbestosdiseases; however, earlyidentification of low-doseexposure is unlikely.
Occupational/general medicalhistory emphasizing priorexposure to these or otheragents.
Medical examination with focuson liver, kidney, nervous system,and skin.
Laboratory testing for liver andkidney function; carboxyhemo-globin, where relevant.

12-112 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
Hazardous Substanceor Chemical Group
Heavy Metals:
ArsenicBerylliumCadmiumLeadMercury
Herbicides:
Chlorophenoxycompounds:2,4-dichlorophenoxyacetic
acid (2,4-D)2,4,5-trichlorophenoxy-
acetic acid (2,4,5-T)Dioxin
OrganochlorineInsecticides:
Chlorinated ethanes:DDT
Cyclodienes:AldrinChlordaneDieldrinEndrin
Chlorocyclohexanes:Lindane
Target Organs
Multiple organs andsystems including:
BloodCardiopulmonaryGastrointestinalKidneyLiverLungCNSSkin
KidneyLiverCNSSkin
KidneyLiverCNS
Potential Health Effects
All are toxic to the kidneys.
Each heavy metal has its owncharacteristic symptom cluster.For example, lead causesdecreased mental ability,weakness (especially hands),headache, abdominal cramps,diarrhea, and anemia. Lead canalso affect the blood-formingmechanism, kidneys, and theperipheral nervous system.
Long-term effects (in 10 to 30years) also vary. Lead toxicitycan cause permanent kidney andbrain damage; cadmium cancause kidney or lung disease.Chromium, beryllium, arsenic,and cadmium have beenimplicated as human carcino-gens.
Chlorophenoxy compounds cancause chloracne, weakness ornumbness of the arms and legs,and may result in long-termnerve damage.
Dioxin causes chloracne andmay aggravate pre-existing liverand kidney diseases.
All cause acute symptoms ofapprehension, irritability,dizziness, disturbed equilibrium,tremor, and convulsions.
Cyclodienes may causeconvulsions without any otherinitial symptoms.
Chlorocyclohexanes can causeanemia. Cyclodienes andchlorocyclohexanes cause livertoxicity and can cause perma-nent kidney damage.
Medical Monitoring
History-taking and physical exam:Search for symptom clustersassociated with specific metalexposure (e.g. for lead, look forneurological deficit, anemia, andgastrointestinal symptoms).
Laboratory testing:Measurement of metallic content in
blood, urine, and tissues (e.g.,blood lead level; urine screen forarsenic, mercury, chromium, andcadmium).
CBCMeasurement of kidney function,
and liver function where relevant.
Chest x-ray or pulmonary functiontesting where relevant.
History and physical exam shouldfocus on the skin and nervoussystem.
Laboratory tests include:Measurement of liver and kidney
function, where relevant.Urinalysis.
History and physical exam shouldfocus on the nervous system.
Laboratory tests include:Measure of kidney and liver
function.CBC for exposure to
chlorocyclohexanes.
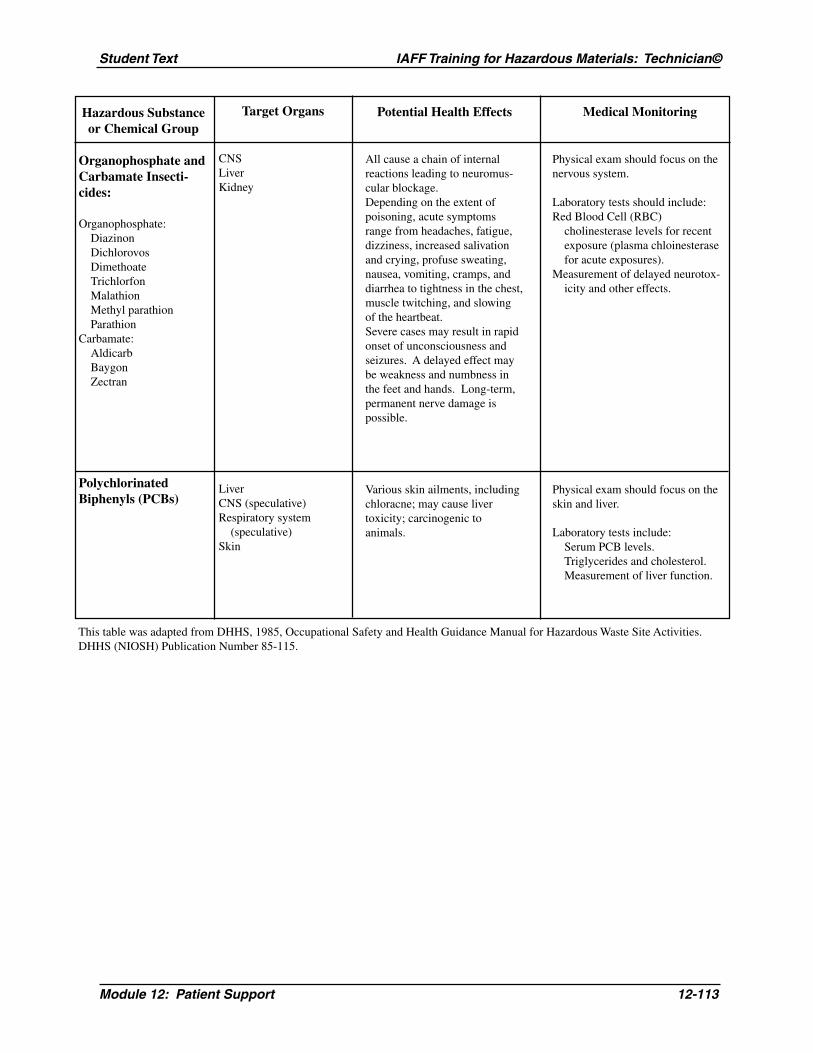
Module 12: Patient Support 12-113
Student Text IAFF Training for Hazardous Materials: Technician©
Hazardous Substanceor Chemical Group
Organophosphate andCarbamate Insecti-cides:
Organophosphate:DiazinonDichlorovosDimethoateTrichlorfonMalathionMethyl parathionParathion
Carbamate:AldicarbBaygonZectran
PolychlorinatedBiphenyls (PCBs)
Target Organs
CNSLiverKidney
LiverCNS (speculative)Respiratory system
(speculative)Skin
Potential Health Effects
All cause a chain of internalreactions leading to neuromus-cular blockage.Depending on the extent ofpoisoning, acute symptomsrange from headaches, fatigue,dizziness, increased salivationand crying, profuse sweating,nausea, vomiting, cramps, anddiarrhea to tightness in the chest,muscle twitching, and slowingof the heartbeat.Severe cases may result in rapidonset of unconsciousness andseizures. A delayed effect maybe weakness and numbness inthe feet and hands. Long-term,permanent nerve damage ispossible.
Various skin ailments, includingchloracne; may cause livertoxicity; carcinogenic toanimals.
Medical Monitoring
Physical exam should focus on thenervous system.
Laboratory tests should include:Red Blood Cell (RBC)
cholinesterase levels for recentexposure (plasma chloinesterasefor acute exposures).
Measurement of delayed neurotox-icity and other effects.
Physical exam should focus on theskin and liver.
Laboratory tests include:Serum PCB levels.Triglycerides and cholesterol.Measurement of liver function.
This table was adapted from DHHS, 1985, Occupational Safety and Health Guidance Manual for Hazardous Waste Site Activities.DHHS (NIOSH) Publication Number 85-115.

12-114 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-115
Student Text IAFF Training for Hazardous Materials: Technician©
Appendix F
Video Exercises

12-116 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-117
Student Text IAFF Training for Hazardous Materials: Technician©
Video Exercise 1Instructor Answer Sheet
In March of 1995, a tanker filled with 8,900 gallons of gasoline overturned on a major highwaysurrounding Washington, D.C. After the rollover, the tank spilled most of the product. Thedriver was taken to the hospital with injuries. Meanwhile, rush hour traffic came to a standstill.The incident occurred at Route 236 on an entrance ramp to I-495. Because there have beenseveral major incidents at this location in recent years, the intersection was preplanned. Re-sponding fire fighters could assume certain conditions even before they arrived at the scene.Based on the preplan, they knew that there was a large tank farm to the west of the intersection.So tankers exiting I-495 at this location would be empty since they were going to the tank farm,while tankers entering I-495 would be full, since they were coming from the tank farm. Firefighters also knew the exact location of hydrants near the intersection, as well as the best areasfor staging and command.
Identify a transportation corridor in your own area that has been — or is likely to be — the sceneof a hazardous materials incident.
1. Briefly describe the transportation corridor and draw a rough diagram of intersecting roads.
2. What makes this location dangerous? (List any nearby manufacturing or storage facilities thatmay ship chemicals in and out).
3. How would you preplan this location?

12-118 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-119
Student Text IAFF Training for Hazardous Materials: Technician©
Video Exercise 2Instructor Answer Sheet
Your first due area is a typical suburban community near a large city. While the area includessome light industry and a number of commercial businesses, it’s primarily residential. Oneafternoon you respond to a call reporting an injured person at one of the industrial facilities — amanufacturer of cleaning products. It’s a new company that hasn’t been preplanned yet. Em-ployees meet you at the entrance and explain that a forklift operator has collapsed in the ware-house. A witness tells you that a chemical drum was punctured by a forklift tine as the operatorwas attempting to move it. “Stuff gushed all over the floor,” the witness says. “Sam got off theforklift to take a look and boom! — down he went.” The forklift operator has fallen near anexterior door just a few feet inside the building. Based on this information and other details inyour text, should you risk a quick entry to rescue the victim or not?
1. What are some clues that the chemical in the drum might be toxic?
2. What is the first thing you should find out before making a decision about entry?
3. Suppose the drum contained methylene chloride, a solvent. Using reference sources, researchthis chemical and decide what your action should be.

12-120 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
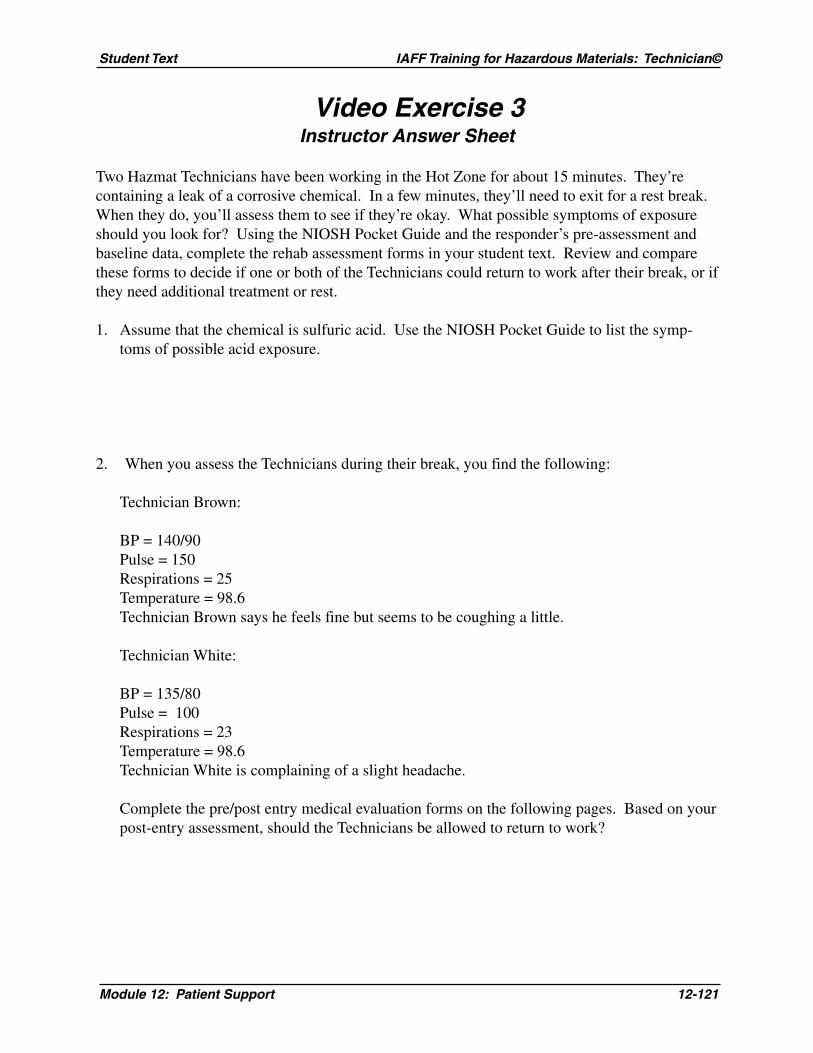
Module 12: Patient Support 12-121
Student Text IAFF Training for Hazardous Materials: Technician©
Video Exercise 3Instructor Answer Sheet
Two Hazmat Technicians have been working in the Hot Zone for about 15 minutes. They’recontaining a leak of a corrosive chemical. In a few minutes, they’ll need to exit for a rest break.When they do, you’ll assess them to see if they’re okay. What possible symptoms of exposureshould you look for? Using the NIOSH Pocket Guide and the responder’s pre-assessment andbaseline data, complete the rehab assessment forms in your student text. Review and comparethese forms to decide if one or both of the Technicians could return to work after their break, or ifthey need additional treatment or rest.
1. Assume that the chemical is sulfuric acid. Use the NIOSH Pocket Guide to list the symp-toms of possible acid exposure.
2. When you assess the Technicians during their break, you find the following:
Technician Brown:
BP = 140/90Pulse = 150Respirations = 25Temperature = 98.6Technician Brown says he feels fine but seems to be coughing a little.
Technician White:
BP = 135/80Pulse = 100Respirations = 23Temperature = 98.6Technician White is complaining of a slight headache.
Complete the pre/post entry medical evaluation forms on the following pages. Based on yourpost-entry assessment, should the Technicians be allowed to return to work?

12-122 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-123
Student Text IAFF Training for Hazardous Materials: Technician©
12-124 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text
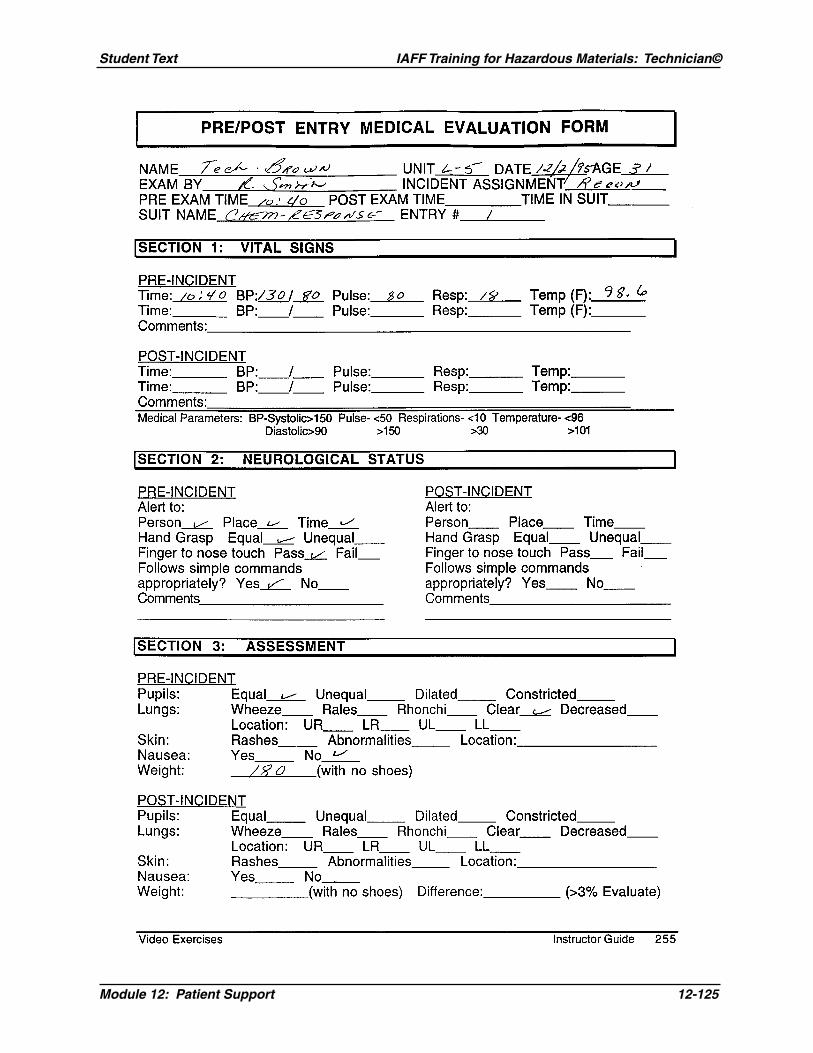
Module 12: Patient Support 12-125
Student Text IAFF Training for Hazardous Materials: Technician©

12-126 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text

Module 12: Patient Support 12-127
Student Text IAFF Training for Hazardous Materials: Technician©
Video Exercise 4Instructor Answer Sheet
In December of 1994, an oil company in Virginia reported a chemical incident. The spill in-volved a 10% chlorine solution that had reacted with an unknown product in several 50-gallondrums. The unknown product was possibly an acid. Large amounts of vapor were released. Thecall came in about 10:40. Employees in one of the oil company’s buildings were reporting noseand throat irritation from chemical fumes. Several fire department vehicles were initially dis-patched, including three EMS units. On arrival, the hazardous materials team met with theincident commander, established control zones, and began researching the chemical. Theyimmediately requested more assistance, including another EMS unit to be assigned to the hazard-ous materials team. The fire department set up primary decontamination at the incident scene asrequested by the local hospital. The hazardous materials team donned fully encapsulated vapor-protective suits. The decon team wore splash-protective gear. As more employees began com-plaining of respiratory irritation, dizziness and headaches, additional EMS units were dispatched.The incident was terminated about three hours later. In all, 13 EMS and paramedic engine unitsresponded. Twenty-one oil company employees were decontaminated, treated at the scene forrespiratory problems, and taken to area hospitals. None of the injuries was life-threatening. Thespill was contained in the immediate area and neutralized with soda ash. Could your departmenthandle a similar incident?
1. Does your fire department have a hazardous materials team? If not, who would you contact tohandle an incident such as this?
2. In this incident, a total of 21 employees were treated and transported to hospitals. Is yourdepartment equipped with a sufficient number of EMS units to handle this many victims ofexposure? If not, who would you call for assistance?
3. Using your NIOSH Pocket Guide or other resource material, what is the recommendedtreatment for exposure to chlorine?

12-128 Module 12: Patient Support
IAFF Training for Hazardous Materials: Technician© Student Text





























