Embed Size (px)
Citation preview

Module 4
Infant Feeding in the Context of HIV Infection

Malawi PMTCT Training Package 2
Module Objectives
Define key infant feeding terms Describe the key infant feeding recommendations
based on National PMTCT Guidelines and Infant and Young Child Nutrition Policy and Guidelines, 2005-2010.
Give an overview of the National Code of Marketing of Infant and Young Child Foods
Give an overview of the Baby Friendly Hospital Initiative

Malawi PMTCT Training Package 3
Module Objectives (continued)
Discuss the main infant feeding options in Malawi and their advantages and disadvantages.
Demonstrate step-by-step safe preparation of commercial formula and home-modified animal milk.
Demonstrate steps in infant feeding counselling
for HIV-positive mothers.

Malawi PMTCT Training Package 4
Unit 1:
Overview of Infant Feeding Recommendations

Malawi PMTCT Training Package 5
Unit 1 Objectives Define key infant feeding terms Describe the key infant feeding recommendations
based on National PMTCT Guidelines and Infant and Young Child Nutrition Policy and Guidelines, 2005-2010.
Give an overview of the National Code of Marketing of Infant and Young Child Foods
Give an overview of the Baby Friendly Hospital Initiative
Malawi PMTCT Training Package 6
Basic Facts on Malnutrition, Infant Feeding and Child Survival
Poor nutrition is a leading cause of illness in children. In Malawi, 48% of children under the age of five years
are stunted, 22% are underweight and 5% present with wasting.
Poor feeding practices, such as early mixed feeding, inadequate complementary feeding, or poor hygiene are a major cause of low weight, and high morbidity and mortality among children
For mothers who are HIV-infected, counselling and support may lead to improved infant feeding practices that may also prevent MTCT.

Malawi PMTCT Training Package 7
Overview of Infant Feeding in the Context of HIV
Breastmilk is the ideal nourishment for infants, for the first six months of life.
ARV therapy and prophylaxis substantially reduce MTCT. However, ARV prophylaxis does NOT provide long-term protection for the infant who is breastfeeding.
Without intervention, 10% - 20% of infants breastfed by HIV-infected mothers may acquire HIV through breastfeeding.

Malawi PMTCT Training Package 8
Overview of Infant Feeding in the Context of HIV in Malawi
Breastfeeding is practiced by almost 97% of mothers
Exclusive breastfeeding (EBF) for the first 6 months of life is practiced by only 53% of mothers
Most infants are not given timely, appropriate or adequate nutrient-rich and energy-dense foods to complement breast milk from age 6 months to 24 months and older

Malawi PMTCT Training Package 9
Key Infant Feeding Terms
Exclusive breastfeeding (EBF): All infant nutrition provided by breastmilk NO other drinks (not even water) or foods
should be given to baby May receive expressed breastmilk No pacifiers, dummies, artificial teats No limits on number of breastfeeds (average 8-
12 times in 24 hours) No limits on length of breastfeed No mixed feeding

Malawi PMTCT Training Package 10
Key Infant Feeding Terms (continued)
Mixed feeding: when infant who is breastfed is also given other liquids, such as water, tea, formula, cow’s milk, or foods such as porridge or rice during first six months of life
Wet-nursing: having another woman (HIV-negative) breastfeed baby
Express and heat-treat breastmilk: removing milk from breasts manually or with a pump, then heating it to kill HIV

Malawi PMTCT Training Package 11
Key Infant Feeding Terms (continued)
Replacement feeding: Infant who is receiving NO breastmilk given a
diet that provides all required nutrients until age at which he/she can be fed on family foods.
During first 6 months of life, replacement feeding with a suitable breastmilk substitute (commercial infant formula or home-modified animal milk).
After 6 months, other foods should be offered to complement breastmilk substitute.

Malawi PMTCT Training Package 12
Key Infant Feeding Terms (continued)
Commercial infant formula: Breastmilk substitute consisting of specially-
formulated powdered milk. Made specifically for infants and sold in shops or
provided to HIV-infected mothers who choose not to breastfeed.
Home-modified animal milk: Made from fresh liquid (or full cream powder)
animal milk and modified using a standard or specific recipe.

Malawi PMTCT Training Package 13
Key Infant Feeding Terms (continued)
Complementary feeding: feeding babies who are older than 6 months of age foods and liquids in addition to breastmilk or breastmilk substitute.

Malawi PMTCT Training Package 14
Infant Feeding Recommendations
Mothers who are HIV-negative & mothers with unknown HIV status:
Breastfeed exclusively for first six (6) months of life
After age 6 months and up to 2 years or longer, continue breastfeeding while giving complementary foods.
Encourage women with unknown HIV status to test for HIV
Educate mother about risk of HIV infection during pregnancy or breastfeeding.

Malawi PMTCT Training Package 15
Infant Feeding Recommendations (continued)
Mothers who are HIV-infected: EBF is a primary feeding option and is
recommended during the first months of life To minimize HIV transmission risk, early
cessation of breastfeeding recommended at 6 months or sooner
Avoid breastfeeding when replacement feeding is AFASS.
All HIV-infected mothers should receive infant feeding counselling

Malawi PMTCT Training Package 16
Infant Feeding Recommendations (continued)
Ensure use of breastmilk substitutes is in compliance with National Code of Marketing Infants and Young Child Foods
Children 6-59 months receive Vitamin A supplementation
Growth monitoring and health promotional activities
Multimix principle - using foods from different food groups at each meal, making meals more nutritious.

Malawi PMTCT Training Package 17
AFASS: DefinitionsAcceptable: Mother perceives no barrier to replacement
feeding. Barriers may be cultural or due to fear of stigma or discrimination.
Feasible: Mother (or family) has adequate time, knowledge, skills and other resources to prepare the replacement food and feed the infant up to 12 times in 24 hours.
Affordable: Mother and family, with community or health-system support if necessary, can pay the cost of purchasing, preparing and using replacement feeding, including all ingredients, fuel, safe water, soap and equipment, without compromising the health and nutrition of the family.

Malawi PMTCT Training Package 18
AFASS: Definitions (continued)
Sustainable: The mother has access to a continuous and uninterrupted supply of all ingredients and products needed for safe replacement feeding for as long as the infant needs it, up to one year of age or longer.
Safe: Replacement foods are correctly and hygienically stored, prepared, and fed in nutritionally adequate quantities with clean hands using clean utensils, preferably by cups.

Malawi PMTCT Training Package 19
AFASS: Possible Questions to Ask Clients
AFASS Possible Questions to Ask Clients
Acceptable Of the people who live with you, who knows that you are HIV-infected? Are your partner or other family members supportive of replacement feeding and willing to help? What do people say when a baby is not breastfed?
Feasible How would you arrange night feeds? Do you work? If so, are there other caregivers that will be able to prepare the replacement feeds correctly and feed the baby as often as needed?
Affordable How much money can you afford for formula each month? If your child gets sick, will you still be able to pay for his/her medical care?
Sustainable Is the supply of replacement feeds consistent? Do the markets or stores in your area tend to run out animal milk or formula?
Safe Where do you get your drinking water? Can you prepare each feed with boiled water and clean utensils? Is there a reliable fuel source for boiling water?

Malawi PMTCT Training Package 20
Risks associated with mixed feeding before 6 months of age
The risks include: Breastmilk is replaced with less nutritious
foods. Increased risk of diarrhoea Increased risk of HIV transmission to baby
due to irritation of intestinal mucosa by other foods/liquids allowing for absorption of the HIV.
Malawi PMTCT Training Package 21
Malawi National Code of Marketing of Infant and Young Child Foods
Based on the 1981 International Code of Marketing of Breastmilk Substitutes
Bans promotion of formula feeding and sets labelling requirements
The Code: Protects and promotes breastfeeding Supports proper and informed use of
breastmilk substitutes Promotes acceptable marketing and
distribution practices

Malawi PMTCT Training Package 22
The Baby Friendly Hospital Initiative
This is a worldwide effort that aims to give every baby the best start in life by creating a healthcare environment where breastfeeding is the norm.
Goals of BFHI: To transform hospitals and maternity facilities into
breastfeeding conductive environments To end the practice of distribution of free and low
cost supplies of breastmilk substitutes to maternity wards and hospitals.

Malawi PMTCT Training Package 23
The Baby Friendly Hospital Initiative: 10 Steps to Successful Breastfeeding
Step 1: Have a written breastfeeding policy that is routinely communicated to all healthcare staff.
Step 2: Train all healthcare staff in the skills necessary to implement this policy.
Step 3: Inform all pregnant women about the benefits and management of breastfeeding.
Step 4: Help mothers initiate breastfeeding within half an hour of birth.
Step 5: Show mothers how to breastfeed and how to maintain lactation even if they are separated from their infants.

Malawi PMTCT Training Package 24
The Baby Friendly Hospital Initiative: 10 Steps to Successful Breastfeeding (continue)
Step 6: Give newborn infants no food or drink other than breastmilk unless medically indicated.
Step 7: Practice rooming in – that is, allow mothers and infants to remain together 24 hours a day. This allows unlimited contact between mother and baby.
Step 8: Encourage breastfeeding on demand. Step 9: Give no artificial teats or pacifiers (also called
dummies and soothers) to breastfeeding infants Step 10: Foster the establishment of breastfeeding
support groups and refer mothers to them on discharge from the hospital or clinic.

Malawi PMTCT Training Package 25
Unit 2
Infant Feeding Options

Malawi PMTCT Training Package 26
Unit 2 Objectives
Discuss the main infant feeding options in Malawi and their advantages and disadvantages.
Demonstrate step-by-step safe preparation of commercial formula and home-modified animal milk.

Malawi PMTCT Training Package 27
Breastmilk Feeding Options
Breastfeeding Option 1: EBF & EBF with early cessation
Breastfeeding Option 2: Expressing & heat-treating breastmilk
Breastfeeding Option 3: Wet-nursing

Malawi PMTCT Training Package 28
Risks: Breastfeeding & MTCT
Mothers who choose to breastfeed should know:
10%-20% infants breastfed by HIV-infected mothers acquire infection through breastfeeding
ARV prophylaxis does not provide long-term protection to breastfed infant

Malawi PMTCT Training Package 29
Risks: Breastfeeding & MTCT (continued)
Risk of transmitting HIV to infant during breastfeeding is greater:
When the woman has higher viral load (by clinical or laboratory measures)
When the woman has mastitis, breast abscess or other similar conditions
When the child has ulcers or open sores in the mouth
Possibly, when the mother practices mixed-feeding
Malawi PMTCT Training Package 30
Breastfeeding Option 1:EBF
Advantages Protects babies from diseases. Improved brain growth and development. Provides all necessary nutrition and water. Always available/no special preparation Early cessation ends infant’s HIV exposure through
breastfeeding
Disadvantages Risk of MTCT. Mother needs support to EBF. Requires feeding on demand 8-10 times per day

Malawi PMTCT Training Package 31
Breastfeeding Option 1:EBF with Early Cessation
Advantages Early cessation ends the infant's exposure to HIV
through breastfeeding.Disadvantages Infants malnourishment after breastfeeding stops. Increased risk of diarrhoea for infants if breastmilk
substitutes are not prepared safely. Infants may become anxious and even dehydrated if
stop breastfeeding too rapidly. Replacement feeding requires feeding infant with a cup. Mothers' breasts may become engorged and infected
during transition.

Malawi PMTCT Training Package 32
Breastfeeding Option 2:Expressing & Heat-treating Breastmilk
Expressing milk means removing it from the breast, usually by hand. Milk heated to boiling point. Long term strategy
From birth till breastfeeding cessation
Short-term strategy: When mother is symptomatic When the mother has a breast infection While the mother is transitioning from
breastfeeding to replacement feeding

Malawi PMTCT Training Package 33
Breastfeeding Option 2:Expressing & Heat-treating Breastmilk
(continued)
Mothers should be provided with support: Taught appropriate techniques for expressing breastmilk Store expressed breastmilk in a cool place and use
within 12 hours if stored at room temperature or 72 hours if refrigerated
Heat only enough milk for one feed. Use heat-treated milk within one hour. Discard left over milk.
Always use a clean cup for feeding the infant. Express the breast frequently (8 times or more in a 24-
hour period) to maintain milk supply

Malawi PMTCT Training Package 34
Breastfeeding Option 2:Expressing & Heat-treating Breastmilk
(continued)Advantages HIV killed by heating the milk. Most nutrients remain in breastmilk after heating. Others can help feed infant.Disadvantages May not be as effective (as unheated breastmilk) for
protecting baby from other infectious diseases. Time-consuming and must be done frequently Baby will need to drink from a cup. Need safe water and soap to was containers and cups Need fuel to heat the breastmilk Others may suspect mother has HIV

Malawi PMTCT Training Package 35
Breastfeeding Option 3: Wet-nursing
A wet-nurse is a woman who breastfeeds another woman’s baby with consent of the baby’s parent or principal guardian. Acceptable in some communities, but not in others. Mothers must receive counselling about potential risk of HIV transmission from a wet-nursing mother who is HIV-infected or a wet-nursing mother whose HIV status is unknown.

Malawi PMTCT Training Package 36
Breastfeeding Option 3: Wet-nursing
Advantages Carries no risk of HIV transmission for the
baby, as long as the wet-nursing mother is not infected with the virus.
Breastmilk is the perfect food for babies and can protect them from diseases.
Disadvantages Wet-nursing mother must be confirmed HIV-
negative. Wet-nursing mother must be able to protect
herself from HIV infection the entire time she is breastfeeding.

Malawi PMTCT Training Package 37
Breastfeeding Option 3: Wet-nursing
Disadvantages (continued) The wet-nursing mother must be available to
breastfeed the baby frequently day and night. Small risk HIV-infected infant can pass HIV to
wet-nursing mother while breastfeeding. Others may suspect mother has HIV. The mother may get pregnant again too soon.

Malawi PMTCT Training Package 38
Breastfeeding by Mothers on ARV Therapy
Clear evidence exists that women on ARV prophylaxis and ARV therapy have reduced risk of HIV transmission during pregnancy and labour
Currently no evidence that either ARV therapy or prophylaxis reduces HIV transmission through breastfeeding.
Infant feeding counselling and advice should be the same for all women, whether or not they are/were on ARV therapy or ARV prophylaxis.

Malawi PMTCT Training Package 39
Replacement Feeding During First 6 Months of Life
Infants receive no breastmilk Does not provide immune protection against
other diseases. During first 6 months of life, replacement
feeding should be with suitable breastmilk substitute (commercial infant formula, home-modified animal milk with micronutrient supplements).
After six months, suitable breastmilk substitute should be complemented with other foods.

Malawi PMTCT Training Package 40
Replacement Feeding Option 1: Commercial Infant Formula
Advantages No risk of transmitting HIV to the infant. Includes most nutrients an infant needs. Others can help feed infant.Disadvantages Does not contain protective antibodies Infant more likely to get diarrhoea, chest infections and
malnutrition Mother must stop breastfeeding completely, or the risk
of transmitting HIV will continue. Expensive

Malawi PMTCT Training Package 41
Replacement Feeding Option 1: Commercial Infant Formula
Disadvantages (continued) Safer preparation requires fuel & clean
water. Others may suspect mother has HIV. Must be made fresh for each feed. Continuous, reliable formula supply
required. Baby must drink from a cup. Mother may get pregnant again too soon.

Malawi PMTCT Training Package 42
Commercial Infant Formula Requirements in First 6 months
Month 500 g
Tins/Month**
450 g
Tins/Month** First month (0-30 days) 4 5
Second month 6 6
Third month 7 8
Fourth month 7 8
Fifth month 8 8
Sixth month 8 9
Total 40 44

Malawi PMTCT Training Package 43
Replacement Feeding Option 2: Home-Modified Animal Milk
Animal milk that is diluted and enriched to ensure nutritional suitability for infants.
Modifications include diluting milk with boiled water in precise amounts to reduce formula's concentration and adding sugar to increase the number of calories in the milk.
Fewer micronutrients than commercial formula. Baby should take micronutrient supplement

Malawi PMTCT Training Package 44
Replacement Feeding Option 2: Home-Modified Animal Milk (continued)
Not all milks are suitable for use in home-modified animal milk.
Suitable Milks Fresh cow’s milk Fresh goat’s milk Fresh sheep’s milk Full-cream milk (pasteurized) Ultra high temperature (UHT) milk Full-cream milk (powdered) Evaporated (unsweetened) milk

Malawi PMTCT Training Package 45
Replacement Feeding Option 2: Home-Modified Animal Milk (continued)
Not suitable: Fresh animal milk already diluted by an
unknown amount Skimmed milk or low-fat milk powder Sweetened or condensed milk Thin cereal-based gruels or porridge Fruit juice, teas, sugar drinks, or sodas Flavoured milk drinks or coconut milk
Malawi PMTCT Training Package 46
Replacement Feeding Option 2: Home-Modified Animal Milk (continued)
Important to observe strict hygiene in preparing the milk.
Should be used within 2 hours or 24 hours if stored in refrigeration at 5˚C or less.
Should only be considered when commercial formula not available or not affordable.

Malawi PMTCT Training Package 47
Replacement Feeding Option 2: Home-Modified Animal Milk
Advantages No risk of HIV transmission. May be less expensive than commercial formula and is
readily available if the family has milk-producing animals.
Can be used when commercial formula is not available. Other family members can help feed the infant.Disadvantages Does not contain antibodies, which protect infants from
infection. Hard for babies to digest and does not contain all the
nutrients that babies need. Needs to be mixed with water and sugar. The baby will
need a micronutrient supplement.

Malawi PMTCT Training Package 48
Replacement Feeding Option 2: Home-Modified Animal Milk
Disadvantages (continued) Higher risk of diarrhoea, chest infections and
malnutrition. Mother must stop breastfeeding. Need to make fresh for each feeding, unless refrigerator
available. Baby needs about 15 litres of milk per month for first 6
months. Sugar and a micronutrient supplement also needed
Baby will need to drink from a cup. Clean water needed to prepare formula and soap to wash
the baby’s cup. Others may suspect mother has HIV The mother may get pregnant again too soon.

Malawi PMTCT Training Package 49
Replacement feeding 6-24 months
After six months of age, milk alone not adequate for baby’s nutritional requirements.
Introduce complementary foods gradually in addition to: For HIV-negative or those with unknown
status: breastmilk For HIV-positive: replacement feed if
AFASS (or breastmilk if not AFASS)
Malawi PMTCT Training Package 50
Replacement feeding 6-24 months (continued)
For mothers for whom replacement feeding is AFASS, this means: Commercial formula: prepared as instructed on the tin. Fresh animal milk: boil milk. Do not dilute and do not add
sugar; the child will need an iron-containing supplement. Powdered or evaporated milk: add clean boiled water
according to the directions on the tin to make full strength milk. Do not dilute and do not add sugar; the child will need an iron-containing supplement.
Processed/pasteurized or UHT milk: no preparation needed; if it has been open more than an hour, it will need to be boiled. Do not dilute and do not add sugar; the child will need an iron-containing supplement.
Do not use condensed milk as the main source of milk.

Malawi PMTCT Training Package 51
Prevention of Spill-Over
Spill-over: With increased availability of formula, there is
risk that women who are HIV-negative or those who do not know their status will use it. They may lose confidence in breastfeeding and decide to feed their babies infant formula.
HCWs should take measures to minimize this.

Malawi PMTCT Training Package 52
Exercise 4.1
Demonstration of Preparation of Commercial Infant Formula and Home-Modified Animal
Milk

Malawi PMTCT Training Package 53
Unit 3
Supportive Counselling for Safer Infant Feeding Choices

Malawi PMTCT Training Package 54
Unit 3 Objective
Demonstrate steps in infant feeding counselling for HIV-positive mothers
Malawi PMTCT Training Package 55
Counselling about Infant Feeding
HIV-positive women should receive counselling that includes:
Information about the risk of HIV transmission through breastfeeding
Information on advantages and disadvantages of feeding options
Recommendations based on the woman's individual circumstances, including her health, social, and financial status, as well as local customs and beliefs

Malawi PMTCT Training Package 56
Counselling about Infant Feeding (continued)
Instruction on the skills needed to feed her infant safely, including demonstrations and/or opportunities for practice
Encouragement for partner or family involvement in infant feeding decisions, when safe and appropriate
Support for disclosure of her HIV status to loved ones

Malawi PMTCT Training Package 57
Dealing with Infant Feeding Pressure
HIV-positive women who choose to breastfeed may be pressured to give their babies other fluids and foods making it hard for them to EBF.
Women who have chosen not to breastfeed may be pressured to do so.
The final decision about her infant feeding strategy should be the woman’s, and she should receive support for her choice.

Malawi PMTCT Training Package 58
Overview of Infant Feeding Counselling & Support
All mothers, regardless of HIV status, benefit from infant feeding counselling.
Infant feeding counselling should take place: Antenatal:
HIV-positive mothers should receive several infant feeding sessions antenatally.
Provided after the mother learns her test results, preferably during the first ANC visit.
Malawi PMTCT Training Package 59
Overview of Infant Feeding Counselling & Support (continued)
Postnatal: Immediately after the birth and within seven
days to monitor infant feeding progress. When the mother brings the child to the clinic
for well-baby check-ups or immunizations. During special high-risk periods, such as when
the: Child is sick Mother returns to work Mother decides to change feeding methods
Malawi PMTCT Training Package 60
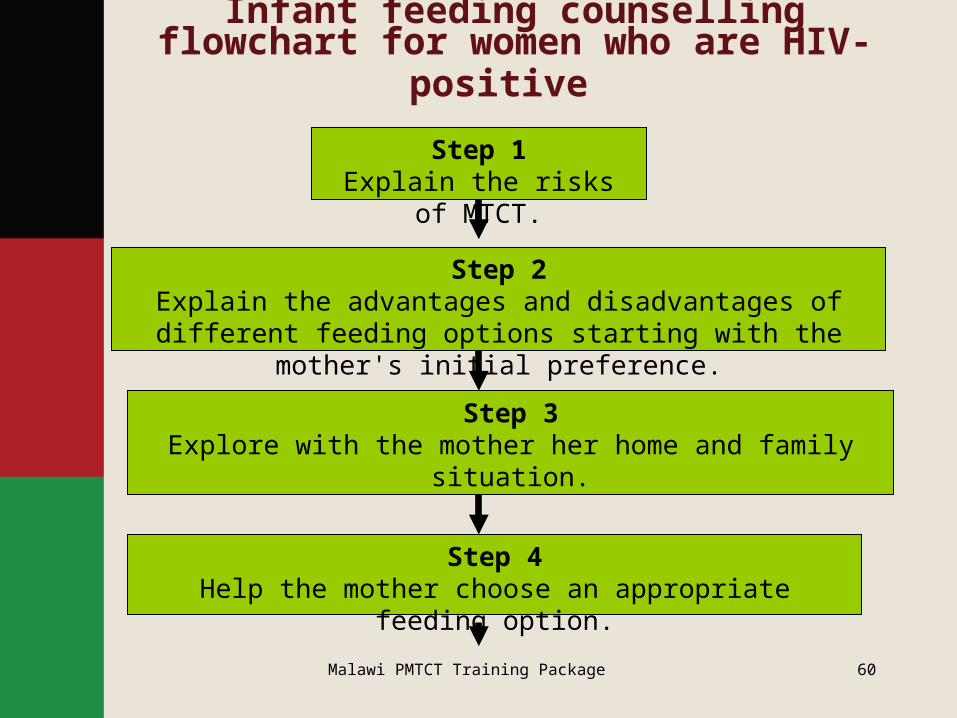
Infant feeding counselling flowchart for women who are HIV-positive
Step 3Explore with the mother her home and family situation.
Step 4Help the mother choose an appropriate feeding option.
Step 2Explain the advantages and disadvantages of different feeding
options starting with the mother's initial preference.
Step 1Explain the risks of MTCT.
Malawi PMTCT Training Package 61
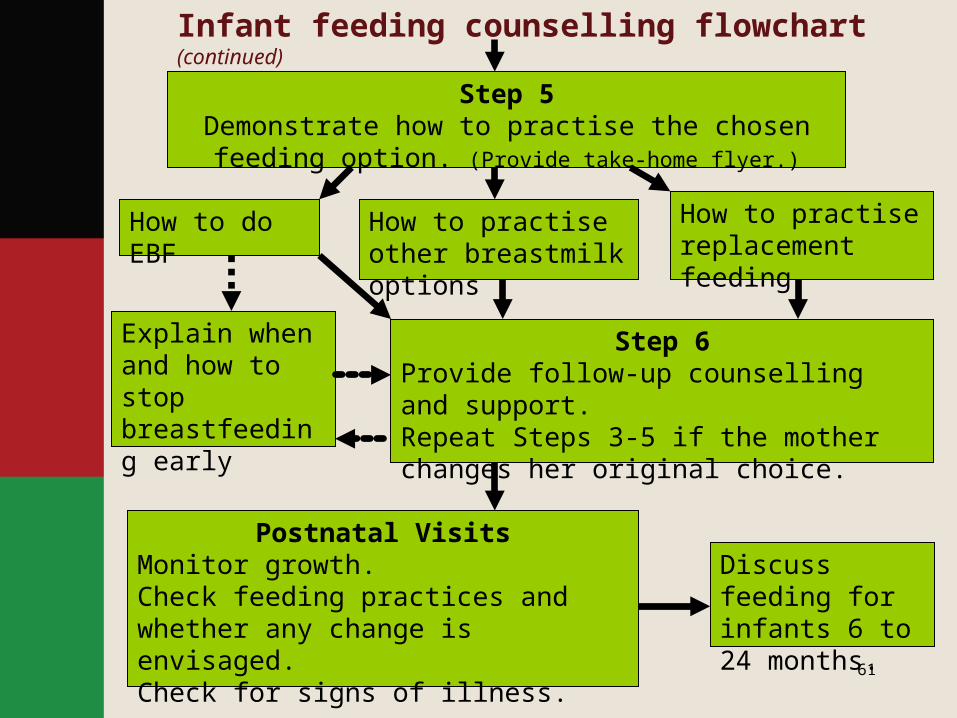
Step 5Demonstrate how to practise the chosen feeding option.
(Provide take-home flyer.)
How to do EBF How to practise other breastmilk options
How to practise replacement feeding
Step 6Provide follow-up counselling and support.Repeat Steps 3-5 if the mother changes her original choice.
Explain when and how to stop breastfeeding early
Postnatal VisitsMonitor growth.Check feeding practices and whether any change is envisaged.Check for signs of illness.
Discuss feeding for infants 6 to 24 months.
Infant feeding counselling flowchart (continued)

Malawi PMTCT Training Package 62
Exercise 4.2
Infant Feeding Counselling and Support Role Play

Malawi PMTCT Training Package 63
Module 4: Key Points Without interventions, 10-20% of infants born to
mothers infected with HIV may become HIV-infected during breastfeeding.
National recommendations not only defend the right of the mother to choose how to feed her infant but also uphold her right to counselling and support.
When replacement feeding is acceptable, feasible, affordable, sustainable, and safe, mothers who are HIV-infected should avoid all breastfeeding; otherwise, EBF is recommended during the first months of life.

Malawi PMTCT Training Package 64
Module 4: Key Points (continued)
Mixed feeding is strongly discouraged as it displaces breastmilk, which is more nutritious, and may be associated with an increased risk of HIV transmission to the baby.
Replacement feeding includes commercial infant formula and home-modified animal milk with micronutrient supplementation.
Breastfeeding options include EBF with early
cessation, expressing and heat-treating breastmilk and wet-nursing.

Malawi PMTCT Training Package 65
Module 4: Key Points (continued)
Each of the infant feeding options has disadvantages and advantages. A woman will benefit from the support of an infant feeding counsellor to make the decision that is right for her and to learn how to implement that decision.
Infant feeding counselling should be offered before the woman gives birth and postpartum with additional session during high-risk periods such as when the child is sick, when the mother returns to work and when the mother is transitioning to a new feeding method.





























