Embed Size (px)
Citation preview

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
1
PATHOGENESIS AND CLINICAL ASPECTS OF RHEUMATOID ARTHRITIS
Tore K Kvien*, Hans Ulrich Scherer** and Gerd-Rüdiger Burmester**
* Dept of Rheumatology, Diakonhjemmet Hospital, Box 23 Vinderen, N-0319 Oslo, Norway. [email protected] ** Hans Ulrich Scherer and Gerd-Rüdiger Burmester Department of Rheumatology and Clinical Immunology Charité - University Medicine Berlin Charitéplatz 1, D - 10117 Berlin [email protected]

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
2
LEARNING OBJECTIVES After following this module on rheumatoid arthritis, pathogenesis and clinical aspects, the students
will be able to
• Describe how environmental, genetic and immunological mechanisms interact in the
pathogenesis of the disease
• Explain the relationship between undifferentiated arthritis and RA
• Describe the characteristic pattern of joint involvement in early and established disease
• State and describe the typical extra-articular manifestations
• Describe the most commonly used tests for assessment of disease activity and health-related
quality of life
• Use this knowledge in diagnosis and assessment of RA
I - PATHOGENESIS OF RHEUMATOID ARTHRITIS
Rheumatoid Arthritis (RA) is a chronic inflammatory disorder affecting primarily cartilage and bone of
small and middle-sized joints. In addition, larger joints and several organs such as lung, vessels and
the haematopoietic system may be involved. Locally, inflammatory cells invade the otherwise
relatively acellular synovium leading to hyperplasia and formation of pannus-tissue, which causes
destruction of cartilage, erosion of the adjacent bone and ultimately loss of function of the affected
joint. Systemic inflammation, in parallel, has long term impact on various organs, considerably
increasing the risk for atherosclerosis and lymphoma development. Combined with inevitable side
effects of year-long anti-rheumatic medication and the psychological burden of facing early invalidity
and social instability, untreated RA has an important socio-economic impact and causes a reduction
in life-expectancy of 7 years in average.
From a clinical point of view, there is considerable heterogeneity in both the clinical picture as well as
the course of disease. Although patients with longstanding disease usually present a clinical picture
characteristic of RA, overlap with other rheumatic diseases such as mixed connective tissue disease
(MCTD) exists, and RA may be accompanied by additional autoimmune diseases (e.g. Sjögren’s
syndrome, Hashimoto’s thyroiditis). For reasons largely unknown, the course of disease is highly
variable, ranging from mild cases with non-erosive, even sometimes spontaneously remitting disease,
to severe, rapidly progressive and destructive RA. Recent analysis of genetic risk factors,
autoantibody responses and therapeutic studies suggests, however, that clinical RA might consist of
pathogenetically distinct subgroups, and that different treatment strategies should be applied to
patients within these groups.
From an immunological point of view, RA is considered an autoimmune disease, implying breakdown
of immunological tolerance towards self at a given point in a patient’s life. The trigger initiating this
breakdown is so far unknown.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
3
The presence of autoantibodies and slowly rising C-reactive protein-levels several years before onset
of clinical symptoms indicate that the inflammatory process may be well underway long before
patients first consult a physician. Variations between ethnic groups in susceptibility to RA,
heterogeneity of disease course and variations in clinical, radiological and laboratory findings within
groups strongly suggest that multiple factors, both environmental and genetic, influence onset and
progression of RA, presumably with different impact during different stages of disease development.
Genetic variations, autoantibodies, cellular immune responses, hormones and gene-environment
interactions are among the most studied factors contributing to RA development, and each of these
factors shall be discussed in detail below (Figure 1).
I - 1 Epidemiology of RA
RA affects approximately 0.5-1% of European and North-American adults, with considerable regional
differences. Prevalence estimates for Southern European countries (median of 3.3 cases per 103) are
lower than for Northern Europe (5.0 per 103), and highest rates are found in North America (10.7 per
103) (1). Asian studies from China report between 2.8 and 3.5 cases per 103. The disease is absent
from certain parts of rural Africa, whereas in some Native American tribes up to 5% of individuals are
affected. Typical rheumatoid lesions in skeletal remains from these Native American populations can
be found in specimen dating back several thousand years. Such lesions, however, are absent from
European and African skeletal remains from antiquity, and evidence of RA depicted in European art
appears only from the early 17th century onwards (2).
Annual incidence rates are estimated to be 16.5 cases (per 105) in Southern Europe, 29 cases in
Northern Europe and 38 cases in North America (1). Women are more frequently affected than men,
the overall gender ratio being 0.3. Recurrence risk estimates for relatives of affected individuals are
4% for siblings, around 4.7% for first degree (parent/child) and ~1.9% for second degree relatives.
Disease severity in the index case determines recurrence risk. First degree relatives of patients with
severe erosive disease can have a risk of up to 15%, whereas the risk for relatives of mildly affected
individuals may only be minimally increased (3).

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
4
Figure 1: Schematic representation of factors relevant for the development of RA. Genetic predisposition forms the basis upon which an immune response develops. Combination of genetic
and environmental factors determines the type and specificity of the immune response (ACPA-positive or negative). When, how and why the immune response shifts to joints is unknown, but
formation of immune complexes might be involved. Once the inflammatory cascade has been started, the process is most likely self-perpetuating.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
5
I - 2 Autoantibodies in RA
Similar to Robert Koch’s postulates defining the requirements for a causal relationship between a
microbe and a disease, Witebsky postulated that a disease must fulfil three criteria to be considered
autoimmune in nature. These postulates require 1) the presence of autoantibodies or a cell-mediated
immune response against an autoantigen, 2) that the respective autoantigen is known and 3) that a
similar disease can be initiated in animals based on an analogous immune response (4).
As is the case for other autoimmune diseases, an array of antibodies targeting self-antigens (e.g.
collagen type II, calreticulin, cathepsin, BiP, CH65, etc.) has been characterized in RA. Although the
corresponding antigen is usually known, demonstrating pathogenetic relevance of the respective
autoantibody has proven far more difficult. Thus, rheumatoid arthritis has long been considered an
autoimmune disease, although evidence fulfilling the third Witebsky postulate was generally lacking.
The initial notion that mechanisms of autoimmunity might underlie RA pathogenesis came from the
discovery of autoantibodies targeting the Fc-part of human IgG (so called “rheumatoid factors” (RF))
in the blood of affected patients (5;6). RF, present mostly as IgM-RF, but detectable in subgroups of
patients also as IgG- and IgA-RF, are thought to form immune complexes activating complement in
the joint, which in turn leads to increased vascular permeability and the release of chemotactic factors
recruiting immune-competent effector cells to the joint (7). The mere presence of RF, however, is
insufficient to initiate arthritis development, as RF is also found in infectious diseases, autoimmune
diseases other than RA and in up to 15% of healthy, mostly elderly individuals. Thus, sensitivity and
specificity of RF are, depending on the population studied, 60-70% and 50-90%, respectively.
Nonetheless, the presence of RF is one of 7 diagnostic criteria for RA put forward by the American
College of Rheumatology in 1987 (2;8).
The so far best known candidate to fulfil all three Witebsky postulates, however, and as such the
autoantibody most likely directly related to RA-pathogenesis, targets proteins containing the atypical
amino-acid citrullin. Citrullination is a process by which arginine residues in a given protein are post-
translationally modified in the presence of relatively high calcium-concentrations by an enzyme called
PAD (peptidyl arginine deiminase). Functionally, it is believed that citrullination is important for the
degradation of intracellular proteins during apoptosis. In 1998, long-known antibodies present in RA-
sera called antiperinuclear factor (discovered already in 1964 (9)) and antibodies directed against
keratin (first described in 1979 (10)) were found to recognize a common target, namely citrullinated
fillagrin (11;12). Meanwhile, citrullin-specific reactivities against additional proteins (e.g. fibrinogen
and vimentin) have been identified, and by the use of novel assays anti-citrullinated protein antibodies
(ACPA) are now found in 60-70% of RA-patients, but hardly in other diseases or healthy subjects.
Thus, ACPA display unique specificity for RA, and ongoing studies are evaluating fine-specificity,
affinity and immunoglobulin-subtypes of the ACPA-response in individual patients (13).

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
6
ACPA can be detected in sera several years before clinical onset of arthritis, their presence predicts
progression from undifferentiated arthritis to RA and is associated with a more severe course of
disease. Active citrullination has been detected in RA synovium, whereas citrullinated proteins are
absent from healthy joints. Interestingly, the strongest genetic risk factor for the development of RA,
the presence of shared epitope alleles (see below), has been found to be associated not with RA
itself, but only with ACPA-positive RA, indicating that ACPA-status defines a specific disease-
phenotype (14). This finding strongly suggests a crucial role for ACPA in RA-pathogenesis, although
experimental evidence for the third Witebsky postulate is still scarce. Citrullination of a peptide
binding to HLA-DRB1*0401 in a HLA-DR4 transgenic mouse has been shown to increase peptide-
MHC affinity and to activate CD4+ T-cells (15). Also, monoclonal antibodies against citrullinated
fibrinogen have been shown to enhance arthritis in a mouse model of pre-existing collagen-induced
arthritis (16). Although these data using engineered ACPA or citrullinated antigens are indicative, data
showing arthritis induction by endogenously produced ACPA is still lacking.
I - 3 Genetic Risk Factors
Comparisons between concordance rates in monozygotic twins in several populations indicate that
approximately 50% of the variation in prevalence of RA is caused by genetic factors. The strongest
and most relevant genetic risk factor for the development of RA, contributing around 30% to the total
genetic effect, is found in HLA class II molecules on chromosomal location 6p21.3, and relates to
experiments first performed in 1969. In autologous mixed lymphocyte reactions, lymphocytes from
RA-patients proliferated poorly when cultured with lymphocytes from other RA-patients, whereas their
proliferative potential was normal in response to lymphocytes from healthy donors (17;18). This
finding indicated genetic similarities between RA-patients, which were subsequently found to reside in
the MHC class II locus, namely the HLA-DRB1 alleles. Several HLA-DRB1 molecules (*0101, *0102,
*0401, *0404, *0405, *0408, *1001 and *1402) share a common amino acid sequence at position 70-
74 in the third hypervariable region of the DRβ1-chain. This sequence consisting of glutamine-
leucine-arginine-alanine-alanine (QKRAA), QRRAA or RRRAA, has, therefore, been termed the
“shared epitope”. It is situated in the antigen binding cleft of the respective class II molecule and has
thus been implicated in binding of a putative arthritogenic peptide (“shared epitope hypothesis”) (19).
Multiple efforts aimed at identifying such a peptide, however, have failed, and recent availability of the
crystal structure of DR molecules indicates that the shared amino acids actually face away from the
antigen binding cleft. Thus, alternative explanations for the shared epitope effect have been put
forward, favouring a possible role of the sequence in shaping a T cell repertoire biased for
autoreactive, non-tolerogenic T-cells. More detailed analysis of the shared epitope revealed that
amino acids at position 70 and 71 flanking positions 72-74 (RAA) seem to modulate the T cell
response, thus influencing the risk conferred by the shared epitope to the development of RA.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
7
Arginine (R) or glutamine (Q) at position 70 and leucine (K) at position 71 confer a higher risk for the
development of RF and ACPA than alanine (A) or glutamic acid (E) at position 71 (see DERAA
below) (20).
Irrespective of the so far unknown mechanism by which the shared epitope contributes to the
development of RA, multiple studies underline the strong association between shared epitope and
susceptibility to as well as severity of RA. Individuals heterozygous for the shared epitope suffer from
more severe and erosive disease, an effect that is further increased by homozygosity. In addition,
homozygosity for the same HLA-DRB1 allele as well as homozygosity for two different alleles confers
a higher risk to develop extra-articular disease manifestations (e.g. vasculitis). As mentioned above,
this shared-epitope effect is in itself indirect, as it predisposes not to RA as such, but to the
development of ACPA. Importantly, the presence of two shared-epitope alleles does not induce
higher ACPA-levels than the presence of only one allele, indicating a dominant effect of the shared
epitope on the immune response (21).
In contrast to ACPA-positive RA, less genetic risk factors have been identified associating with
ACPA-negative RA. Another MHC-class II gene, HLA-DR3, predisposes to the development of this
disease variant. It is part of a conserved haplotype (A1; B8; DRB1*03) that includes the MHC class III
region encoding for e.g. proinflammatory cytokine TNF-α. Thus, this risk factor could influence the
degree of and the susceptibility to inflammation. Alternatively, HLA-DR3 could predispose to the
development of another, yet unidentified autoantibody distinct from ACPA (22).
In contrast to the shared epitope, another amino acid sequence (DERAA) shared by several HLA-
DRB1 alleles (*0103, *0402, *1102, *1103, *1301, *1302, *1304) has been found to independently
protect its carriers from the development of RA. DERAA-encoding alleles are found in approximately
30% of healthy Caucasian individuals, whereas only ~16% of RA-patients are DERAA-positive.
DERAA-positive individuals have a significantly lower risk to develop RA, both in the presence or
absence of shared-epitope alleles. In addition, DERAA-encoding alleles are associated with less
erosive disease in both ACPA-positive and negative patients. As is the case for the shared-epitope
effect, the mechanism underlying the DERAA-effect is so far unknown (23).
Next to genetic variations in HLA-class II molecules, other genetic factors have been identified as
important risk factors for RA-development. A single nucleotide polymorphism in tyrosine phosphatase
PTPN22 at position 1858 (C->T) leading to a missense mutation is associated with several
autoimmune diseases and has been found to be an HLA-independent risk factor for RF- and ACPA-
positive (but not ACPA-negative) RA. As PTPN22 is important in the inhibition of T-cell receptor
signalling, the mutation is thought to lower the threshold for T-cell activation, thus facilitating the
development of autoreactive T-lymphocytes (24).
The relative importance of polymorphisms of other candidate genes (i.e. CTLA-4, PAD4, PD-1, IL-10,
TNFRII, RUNX1) is somewhat less clear to date, as associations with RA have been found in some
populations, but not in others. Such discrepancies, however, largely depend on the size of the
respective patient cohort and on the technical approach applied.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
8
Alternatively, inconsistent findings might reflect the predominance of disease subgroups in different
populations. Thus, genetic variations in several genes which need further study might contribute to
RA susceptibility and severity independently of the strong effect exerted by HLA-class II molecules.
As outlined below, some of these effects are strongly influenced by environmental factors (gene-
environment interactions) (25).
I - 4 Environmental Risk Factors
None of the aforementioned genetic risk factors in itself is sufficient to cause RA. Carrying one or
more of these factors may predispose to either disease development or disease severity, but
additional environmental factors are needed for genetic factors to exert their impact. In the context of
RA, some environmental factors may have specific effects directly related to RA-pathogenesis (e.g.
factors promoting citrullination of proteins), whereas others might have non-specific effects promoting
inflammation in general (e.g. triggers of innate immunity). Thus, the former will only be relevant for
subtypes of RA (e.g. ACPA-positive or negative RA), whereas the latter will influence disease in a
broader sense. In addition, these factors might be relevant at distinct time-points during disease
development.
Infections are major candidates for the induction of autoimmunity and have, therefore, been
intensively studied also in RA. Several pathogens (mycobacteria, Epstein-Barr Virus, Parvovirus B19
and others) have been debated to trigger the initial immune response necessary for RA-development
in a genetically susceptible host. To date, however, no pathogen-derived antigen has been clearly
linked to RA-pathogenesis, and convincing evidence for cross-reactivity of self-antigen-specific T- or
B-cells with pathogen-derived peptides (“molecular mimicry”) in a manner relevant for RA-
development is still lacking.
The most prominent example for a gene-environment interaction in RA-pathogenesis, however, is
cigarette smoking. Several years of smoking confer an increased risk for the development of RA.
Smoking is associated with more severe disease and the risk increases proportionally with the
number of pack-years. Importantly, smoking increases the risk for the development of ACPA-positive,
but not for ACPA-negative RA. This risk is further increased in the presence of shared-epitope alleles
(up to an estimated 21-fold as compared to shared-epitope negative non-smokers) (26;27). As
shared-epitope alleles themselves also predispose to the development of ACPA-positive RA only,
cigarette smoke could be involved in the induction of protein-citrullination. Supporting this hypothesis,
citrullinated proteins have been detected in bronchoalveolar lavage fluid from smokers but not from
non-smokers (28). Thus, smoking might induce apoptosis and subsequently citrullination in alveolar
cells, which, by a mechanism so far unknown, induces an anti-citrullin specific immune response.
How and why this response eventually targets the joints, however, remains unknown and might
require additional environmental factors.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
9
Next to smoking, additional environmental factors are associated with a risk for RA-development,
albeit without necessarily a clear gene-environment interaction. Some of these should be interpreted
with caution, however, as they have only been reported in one cohort or cohorts with small sample
sizes. As for smoking, most associations underline the notion that RA can be divided in subgroups, at
least by stratifying for ACPA-status.
Coffee consumption has shown association with RA in several cohorts, although stratification for
smoking usually reduced significance of this finding. In a Danish cohort, however, coffee consumption
did show association with ACPA-positive RA after adjustment for smoking. Alcohol intake, on the
other hand, seemed to have a protective effect on the development of ACPA-positive RA, whereas no
effect was found for ACPA-negative RA (29).
Strong association with ACPA-negative RA has been shown for individuals with high body-mass
index (29). Although this finding has been questioned by other studies (30) and could have been
confounded by osteoarthritis patients within the ACPA-negative RA-group, its immunological
significance could be interesting. Adipose tissue is receiving increasing attention due to its recently
discovered immune-modulatory properties, as adipocytes are an abundant source of pro- and anti-
inflammatory cytokines.
Occupational exposure to mineral oils (e.g. motor oils, hydraulic oils etc.) was found to be a risk factor
for ACPA-positive RA in males in a Swedish cohort, independently of the presence of shared epitope
alleles. This finding is of interest, as mineral oils are arthritogenic in certain rat-strains due to a yet
unknown mechanism (31).
Female predominance in various autoimmune diseases including RA suggests that sex hormones
and reproductive factors influence both RA-development and severity. Women with lower age at
menarche have a comparatively low risk for the development of RA. In the Danish cohort, for
example, women with older age at menarche (≥15) had an almost 2-fold risk to develop RA as
compared to women aged ≤12 years at menarche. Pregnancy is in itself a risk factor for the
development of RA, as around 12% of women with RA experience disease onset within one year
after pregnancy. During pregnancy, most women with RA (in older studies up to 90%) experience a
significant reduction in disease activity (including complete remissions), but almost all patients
relapse within six months after delivery. Multiparty (>3 children) favours a more severe course of
disease, but does not additionally increase the risk for developing RA. Use of oral contraceptives, on
the other hand, lowers disease severity, but data from initial studies showing a protective effect on RA
development could not be confirmed after adjustment for age (29;32).

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
10
I - 5 Disturbances of the Immune System
During normal embryonic development the immune system is tolerized by various mechanisms
against recognizing “self” as “dangerous”. T cells, for example, are positively and negatively selected
in the thymus to only recognize non-self antigens in the context of MHC-molecules (central
tolerance). As some autoreactive T cells might escape this selection, and as some self-antigens are
only expressed later in life, additional mechanisms of tolerance exist once immune cells enter the
periphery (peripheral tolerance). Naturally occurring regulatory T cells, for example, efficiently control
autoreactive effector T cells. Consequently, lack of such regulatory T cells leads to a syndrome of
severe multiorgan autoimmunity including arthritis in both mice and humans (33).
The trigger initiating breakdown of immunological tolerance in RA is still unknown. Rheumatoid
synovitis is characterized by massive infiltration of the synovium by various immune effector cells
(mainly T- and B-lymphocytes, neutrophils, monocytes, mast cells). As these are absent from a
normally very thin synovial layer in healthy joints, the infiltration is considered to be initiated via an
active process of cellular migration. Locally, these cells may proliferate and produce inflammatory
cytokines and chemokines. Together with vascular growth factors promoting neovascularization and
vascular leakage which facilitates cellular migration, additional effector cells are recruited to the joint.
Over time, this process creates a cytokine milieu in the joint that activates synovial fibroblasts and
osteoclasts, which in turn degrade cartilage and bone. Cellular mediators as well as important
cytokines supporting this process are discussed below (Figure 2).

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
11
Figure 2: Suggested mechanism of the development of the immune response. Antigen-specific T cell activation by DC-T cell interaction usually occurs in lymph nodes. Naïve T cells thereby differentiate into effector T cells that give help to B cells, which leads to production of autoantibodies (e.g.ACPA).
These form immune complexes and accumulate in joints, activating complement. This leads to recruitment of effector cells (macrophages, neutrophils, etc.) which secrete proinflammatory cytokines
and chemokines and activate osteoclastogenesis. Note that this figure depicts a hypothesis, as a crucial pathogenetic role for ACPA has not yet been fully demonstrated. (Figure adapted with
modifications from Luross et al. (2001), Immunology 103:407-416)

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
12
I - 5 - 1 T cells T cell function in RA can be interpreted from different perspectives. Effector T cells are likely to be the
first to recognize an autoantigen as foreign, thus being antigen-specifically activated and providing
necessary help for B cells to produce autoantibodies. Upon activation, these effector cells proliferate
and produce proinflammatory cytokines, thereby driving an inflammatory immune response.
Regulatory T cells (Treg), on the other hand, appear to be incapable of controlling this autoreactive
immune response. Whether Treg are functionally defective in RA is still a matter of debate, but data
indicate that TNF-α is involved in downregulation of Treg-cell function (Figure 3).
Figure 3: Defective regulation of T-cell immunity leads to chronic inflammation. Regulatory mechanisms normally control and terminate T cell activation (lower pathway). In (genetically) susceptible hosts, however, these mechanisms fail, leading to chronic T cell activation and
subsequently to inflammation (upper pathway).
For many years, rheumatoid arthritis was considered to be a mainly Th1-mediated autoimmune
disease. The abundance of Th1-cytokines (especially IFN-γ) and the relative lack of Th2-cytokines
(IL-4, IL-5, IL-10) in RA-patients favoured this notion, and the ability of Th1-cells to activate
monocytes, the main source of TNF-α in RA, further supported the concept. This view has
considerably changed over the last years, mainly due to a new understanding of the original Th1/Th2
paradigm (34).
IL-12, the cytokine driving Th1-development and IFN-γ production, was found to share a common
subunit (IL-12p40) with recently discovered cytokine IL-23 (consisting of IL-12p40 and IL23p19). IL-
23, in turn, is important for IL-17 production by a new subclass of T helper cells termed Th17.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
13
Previous models investigating the role of IL-12 in knock-out models of IL-12p40, therefore, not only
exhibited IL-12 deficiency, but also lack of IL-23. Importantly, IL-17 producing, but not IFN-γ
producing CD4+ T cells proved to be pathogenetically relevant in the murine collagen induced arthritis
model (CIA). In line with this observation, mice deficient in IL-23 only (p19-/-) were shown to be
resistant to CIA, whereas lack of IL-12 (p35-/-) induced more severe disease (35). Further
experiments showed that differentiation of naïve CD4+ T cells into Th17 cells is driven by TGF-β, IL-6
and IL-1 and inhibited by IFN-γ and IL-4. Apart from IL-17, Th17 cells themselves produce TNF-α, IL-
6, IL-22 and GM-CSF (36).
Although these findings were obtained in mice, increasing evidence supports an important role for IL-
17 also in the human system. In RA-patients, both IL-17 and IL23p19 are found in sera, synovial fluid
and synovial biopsies, whereas these cytokines are mostly absent from osteoarthritis patients. IL-17
strongly stimulates macrophages to produce TNF-α as well as IL-1 and has been implicated in the
induction of osteoclastogenesis. It also enhances IL-6 production, collagen destruction and collagen
synthesis by RA synovial explants. In addition, synovial mRNA levels of IL-17, TNF-α, IL-1β and IL-10
correlate with progressive joint damage. Finally, IL-17 induces production of IL-1β, IL-6, IL-23, IL-8,
G-CSF, GM-CSF, VEGF, Cox2 and PGE2 by fibroblast-like synoviocytes (37). Thus, IL-17 has
become an interesting novel therapeutic target in RA, and the efficacy of tocilizumab, an IL-6
antagonist currently evaluated in RA, might in part be explained by an influence on Th17-
development and function.
Naïve T cells develop into effector T cells upon antigen recognition, while the cytokine milieu they
encounter during development influences lineage specificity. Recognition of antigen by naive T cells
in the context of MHC-molecules, however, requires additional costimulatory signals for efficient T cell
activation. Without costimulatory signals, T cells become anergic. Interaction of CD28 and CD80/86
generates one of the most important costimulatory signals, which is controlled by expression of the
natural inhibitor CTLA-4. This mechanism is exploited therapeutically by an engineered CTLA4-Ig
fusion protein (Abatacept), which efficiently inhibits disease activity in RA. Next to cytokine
production, CD4+ effector T cells have been attributed additional functions in RA synovium. By means
of direct cell-to-cell contact they provide crucial help to B cells for antibody production, and by the
expression of RANKL they can directly induce osteoclastogenesis (34).
Detailed analysis of human regulatory T cell function in RA is hampered by difficulties in defining a
consistent phenotype for these cells. Initially non-regulatory T cells can acquire a regulatory
phenotype in the periphery upon stimulation with specific cytokines (“inducible Treg”). “Naturally
occurring” regulatory T cells (Treg that have developed in the thymus), on the other hand, also do not
form a homogeneous population in the human. This might explain, why conflicting data on functional
integrity of Treg cells in RA patients have been published. Whereas an initial report did not find
functional impairment of RA-derived Treg cells (38), later work claimed that Treg cells of RA-patients
fail to suppress cytokine production by effector T cells. Interestingly, the functional deficit was
restored following treatment with TNF-antagonists (39).

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
14
This study was later extended to show that treatment with TNF-antagonists gives rise to a newly
generated, functionally distinct Treg-cell population that secretes TGF-β and IL-10 (40). Treg cells
express TNFR-II, which makes them susceptible to deleterious effects of TNF-α. Indeed, TNF-α was
experimentally shown to inhibit Treg-cell function, and treatment of RA-patients with TNF-antagonists
restored Treg cell function also in a second study (41). The relevance of functionally intact Treg-cells
for RA has clearly been shown in murine CIA. Mice depleted of Treg developed more severe disease,
and adoptive transfer of Treg in mice with established disease could lower disease severity (42).
I - 5 - 2 B cells The importance of B cells in RA-pathogenesis has only recently received adequate appreciation. The
presence of RF and ACPA years before clinical onset of arthritis implicates early involvement of
autoantigen-specific B cell activation and plasma cell differentiation. ACPA show high specificity for
RA, strong genetic association with shared-epitope alleles and clearly associate with disease
progression and severity. RA synovium frequently exhibits formation of lymphoid follicles with
germinal centre-like structure, indicating involvement of B cells in the local immune response. Indeed,
T cell activation in RA synovium has recently been shown to be B cell dependent. Finally, depletion of
peripheral B cells has proven to be highly effective even in patients with inadequate response to TNF-
antagonists.
The role of B cells in RA is multifactorial, including cytokine production (e.g. TNF-α, IL-6, IL-10),
antigen presentation, modulation of T cell responses and (auto-) antibody production (43). In addition,
B cells are responsive to triggers of innate immunity (e.g. immune complexes, bacterial DNA), thus
bridging non-specific and specific immune responses.
By producing TNF-α and IL-6, B cells contribute to the activation of macrophages and directly
participate in inflammation. IL-6 is also an important differentiation factor for B cells themselves. IL-10
producing B cells have been implicated in downregulation of the immune response possibly by
tolerizing T cells, but their exact phenotype and role in RA is less well understood.
During inflammation, B cells infiltrate RA synovium, although the degree of infiltration and local
structural organization varies significantly between patients. Fibroblast-like synoviocytes and dendritic
cells in synovium secrete factors attracting B cells and influencing their differentiation and survival
(e.g. BAFF, CXCL12, CXCL13, APRIL). Some of these factors are currently evaluated as therapeutic
targets. In some but not all patients formation of tertiary lymphoid structures, consisting mainly of B
cells, T cells and follicular dendritic cells is observed. Locally, interaction of B cells with T cells is
important for adequate function of both cell types as both provide help to each other.
B cells can take up antigen via surface Ig and are able to very efficiently process and present antigen
loaded on MHC class II molecules to T cells. Indeed, T cell priming by B cells was demonstrated to
be of prime importance in a mouse arthritis model, although the relative contribution of this
mechanism to RA in the human is less clear. T cells, on the other hand, provide help to B cells for
sufficient antigen production.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
15
Ig-class switching and somatic hypermutation are usually dependent on the presence of T cells and
require CD40-CD40L interaction. Recent findings, however, indicate that Ig class switching in B cells
can also occur independently of T cells. This process requires BAFF, which is present in elevated
amounts in RA synovium and additionally prolongs B cell survival (43;44).
Another important feature of B cells is the expression of several toll-like receptors (TLRs) which
provides an important link between innate and adaptive immunity. TLRs preferentially transmit
“danger signals” by binding bacterial cell wall components and DNA (so called “pathogen associated
molecular patterns”). TLR-9, for example, detects microbial DNA with hypomethylated CpG motifs. In
murine models of RA, immune complexes containing IgG bound to mammalian chromatin were
shown to activate B cells via sequential engagement of B cell receptor and TLR-9 (45). A similar
mechanism has been proposed for antigens associated with single-stranded RNA via engagement of
BCR and TLR-7 (46). These findings are important, as hypomethylated mitochondrial DNA released
from dead cells is abundantly present in RA-synovium. Triggering of TLR-9 has recently been shown
to initiate transcription of germline genes involved in class switching, although subsequent IgG-
production required BCR signalling and presence of BAFF (47). This indicates that non-protein
components contained within synovial fluid are intimately involved in activation of potentially
autoreactive B cells, thus driving antibody production and immune complex formation.
The role of autoantibodies in RA is still incompletely understood. As mentioned above, ACPA are very
likely to be directly involved in the pathogenesis of shared-epitope positive RA, although the exact
mechanism remains elusive. RF, on the other hand, also associate with disease severity and
progression, but have less specificity for RA and are thus thought to rather drive inflammation than
initiate disease. RF form immune complexes that can induce tissue damage and efficiently activate
complement. They can also be taken up by macrophages and induce inflammatory cytokine secretion
(48) (see below).
I - 5 - 3 Mast cells Mast cells are a rather neglected cell type in RA-research. They might, however, be strongly involved
in driving local synovial inflammation. Experiments from mice emphasize this potential involvement,
as mice deficient in mast cells are resistant to arthritis (49). Mast cells are abundantly present in RA
synovium in the human, and their presence correlates with disease progression. Fibroblasts, stromal
cells and epithelial cells secrete stem-cell factor, an important differentiation factor for mast cells.
TGF-β, complement components C3a and C5a, serum amyloid A and platelet activating factor are
important for mast cell recruitment.
Mast cells are loaded with granules full of cytokines, proteases, biogenic amines and proteoglycans.
Upon cross-linking of FcεReceptor I by IgE antibodies, mast cells release large amounts of these
effector molecules. In addition, they are sensitive to many cytokines (e.g. IL-4), chemokines, bacterial
components (via TLRs) due to expression of specific receptors.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
16
While mast cells degranulate very rapidly during type I hypersensitivity reactions, chronic
inflammation might induce a functional change towards more selective secretion of inflammatory
mediators. Many of the mediators produced by mast cells directly influence other cell types important
in RA-pathogenesis. Next to histamine, mast cells release heparin, chymase, tryptase, IL-5, IL-6, IL-8,
TNF-α, RANTES, leukotriene C4, prostaglandin D2, vascular endothelial growth factor and fibroblast
growth factor. Mast cells are also considered to play a vital role in driving (neo-) angiogenesis,
thereby facilitating migration of immune effector cells and contributing to pannus formation. Chymase
and tryptase secretion, on the other hand, activate matrix-metalloproteinase production by fibroblasts,
thus driving cartilage and bone degradation (see below) (50;51).
I - 5 - 4 Monocytes/Macrophages The role of activated macrophages in RA synovium is central to driving and maintaining chronic
inflammation. Macrophages are multipotent effector cells that very efficiently integrate innate and
adaptive immune responses. They are abundantly present in the rheumatoid synovial membrane and
at the cartilage/pannus junction. Important functions include strong phagocytic activity, antigen
processing and presentation, secretion of proinflammatory cytokines, expression of Fc-receptors
responsive to (auto-) antibodies and immune complexes, complement activation and regulation, toll-
like receptor (TLR) expression, tissue degradation and remodelling, and direct interaction with mainly
fibroblasts and T cells.
So far, no direct causal relationship between macrophages and the initiation of rheumatoid
inflammation has been established. However, as macrophages are tissue-resident in most organs,
they are likely to be the first to encounter non-self antigen. Thus, macrophages could be involved in
presenting pathogen-derived antigen to autoreactive T cells, thereby providing the initial trigger
necessary to start an immune response on the basis of genetic predisposition. Alveolar
macrophages, for example, could play a role in presenting smoke-induced citrullinated peptides, as
macrophages are responsible for the clearance of apoptotic cells. So far, however, direct evidence for
such a crucial, early pathogenetic role for macrophages is missing. In addition, the relative
importance of different macrophage functions during the course of disease may change over time
(52).
Synovial macrophages respond to direct cell-contact with T cells and fibroblasts. Co-culture with
fibroblasts not only induces secretion of IL-6, IL-8 and GM-CSF, but also enhances cartilage
degradation in vitro (53). Bacterial cell wall (e.g. LPS) and nuclear (e.g. DNA) components, but also
cartilage degradation products such as hyaluronic acid, are strong macrophage activators. Among the
most important cytokines secreted by activated macrophages in RA are TNF-α, IL-1, IL-6, IL-12, IL-
15, IL-18 and IL-27. In addition, macrophages produce MMP-9 and -12, macrophage migration
inhibitory factor (MIF), GM-CSF and thrombospondin (54).

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
17
Macrophages are also responsive to oestrogens, a finding that could explain changes in disease
activity during pregnancy. Interestingly, physiological oestrogen levels induce IL-1 expression,
whereas higher levels (as occur in pregnancy) inhibit IL-1 secretion (55).
Macrophage function is in itself regulated by various cytokines that in some cases have autocrine
effects. IL-4, for example, downregulates macrophage function by reducing the expression of TNF-α,
IL-1β and PGE2. IL-10 lowers the expression of HLA-DR and reduces antigen processing and the
expression of Fc-receptors. Both IL-4 and IL-10 have strong anti-arthritic properties in murine models
of arthritis, and some studies have linked polymorphisms in the IL-10 gene to disease susceptibility
(56;57).
I - 5 - 5 Inflammatory cytokines In many ways, the cytokine profile of RA synovium reflects the relative contribution of different cell-
types to the inflammatory state. Studies evaluating cytokine profiles have tried to assess which cell
type predominates during different stages of disease development. Especially the initiation phase of
inflammation is thought to be distinct from a chronic, self-perpetuating phase. While studies in long-
standing disease are hampered by the effects of therapy, assessment of cytokine profiles in early,
even undifferentiated arthritis are more suggestive. Recently, patients with early arthritis (symptom
duration less than 3 months) that progressed to RA were shown to exhibit a different synovial
cytokine profile than patients that remitted or developed other arthritides. Patients prone to develop
RA showed elevated levels of T cell-derived cytokines IL-2, IL-4, IL-13 and IL-17 and of stromal and
macrophage related cytokines EGF, βFGF, IL-1 and IL-15. IFN-γ was not detected in these samples,
and IL-6 seemed to be associated with inflammation independent of underlying disease phenotype.
Interestingly, this profile was absent from patients with established RA and seemed to be present only
transiently (58). These findings point towards an important role for T cells in the initiation phase of
RA. The absence of Th1-cytokine IFN-γ and the presence of Th2-cytokines IL-4 and IL-13 together
with (presumably) Th17-derived IL-17 are in favour of the recently revised Th1/Th2-paradigm
described above.
T cells, macrophages and stromal cells are also the main source of cytokines in established RA.
Macrophage derived cytokines, however, predominate, and T cell derived cytokines become less
abundant. Examination of synovial biopsies indicates that disease-subtype specific patterns might
exist. Distinct cytokine profiles were found to correlate with subtypes of lymphocyte infiltration in
active RA. In this study, diffuse lymphocytic infiltrates was associated with RF-negative RA and
displayed low levels of IFN-γ, IL-4, IL-1β und TNF-α. Germinal centre formation, on the other hand,
correlated with high levels of IFN-γ and IL-10, and absence of IL-4. Patients with extra-articular
disease manifestations showed synovial granuloma formation associated with high levels of IFN-γ, IL-
4, IL-1β and TNF-α (59).

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
18
The therapeutic success of monoclonal antibody therapies underlines the importance of pleiotropic
cytokines TNF-α, IL-1 and IL-6 in maintaining chronic inflammation. Other cytokines such as IL-12, IL-
17, IL-23, IFN-γ, IL-4 and IL-10 have been discussed above. IL-18 needs consideration as
proinflammatory cytokine driving macrophage activation together with IL-12 and IL-15. IL-18 is over
expressed in RA synovium, it induces RANKL-expression in T cells (see below) and strongly
aggravates experimental arthritis. The existence of a natural inhibitor, IL-18 binding protein, makes IL-
18 an interesting therapeutic target (60). IL-15 attracts T cells and IL-15 activated T cells in turn
activate macrophages. It is expressed in the synovial membrane and by macrophages themselves.
Finally, TGF-β is an important regulator of tissue degradation and remodelling and displays pro- and
anti-inflammatory properties. It is produced by macrophages in RA synovium, and low expression of
TGF-β due to genetic polymorphisms is associated with disease severity. In addition, TGF-β drives
development of regulatory T cells, but can also enhance Th17-development in the presence of IL-6
(61).
I - 6 Cartilage and Bone Degradation – The Role of Fibroblast and Osteoclasts
While immune effector cells discussed above are responsible for initiating and maintaining
inflammation, two cell types are of prime importance for destruction of cartilage and bone. Synovial
fibroblasts (SF) adhere to cartilage and degrade the extracellular matrix. Osteoclasts, on the other
hand, are mainly involved in bone destruction. Both cell types closely interact with cells of the immune
system and, by secreting large amounts of cytokines, participate themselves in the maintenance of
inflammation.
Synovial fibroblasts in RA are commonly found in the sub-lining layer of the synovium. Expression of
various transcription factors indicates that they proliferate locally, thus contributing to synovial
hyperplasia. SF in RA-patients show prolonged survival and resistance to apoptosis. Functionally,
they adhere to cartilage via attachment to fibronectin, collagen type VI and cartilage oligomeric matrix
protein (COMP), and display an aggressive invasive behaviour. Synovial fibroblasts are an abundant
source of IL-15, -16 and -17. They also secrete CXCL12, CXCL13 and members of the IL-6 family
(e.g. IL-11). These cytokines activate T cells and influence B cell migration and survival. Large
amounts of PGE2 additionally support inflammation. Degradation of cartilage is due to the secretion of
matrix metalloproteinases (MMPs) and cathepsins. Specifically, SF produce MMP-1, -3, -13, -14 and -
15 as well as cathepsins B, K and L. These enzymes degrade extracellular matrix which generates
almost indefinite amounts of potential (neo-) antigens for T and B cell polyclonal proliferation (62).
Bone degradation in RA is mainly mediated by osteoclasts. Osteoclastogenesis, i.e. the differentiation
of osteoclasts from precursor cells, requires M-CSF and the presence of an osteoclast differentiation
factor (ODF).

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
19
Identification of this factor marked an important step in understanding osteoclast differentiation, as it
was found that ODF and osteoprotegrin ligand (OPG-L) are identical to RANKL (receptor activator of
NFkB ligand) and TRANCE (TNF-related activation induced cytokine), molecules first identified in
activated T cells (63). Meanwhile, RANKL has been found to be specifically expressed in RA
synovium, and RANKL-deficient mice are protected from bone destruction in experimental arthritis
despite active inflammation. RANKL is expressed not only by T cells, which thereby directly drive
osteoclastogenesis, but also by neutrophils and in large amounts by synovial fibroblasts (64). TNF-α
accelerates this process by inducing RANKL-expression and enhancing RANKL-signalling.
Interestingly, Th1- and Th2-cytokines (IFN-γ, IL-4, IL-10) as well as IL-12 and IL-18 inhibit
osteoclastogenesis. IL-17, however, induces RANKL-expression in osteoblasts and might significantly
contribute to osteoclast formation (Figure 4).
Figure 4: Factors contributing to osteoclastogenesis. Macrophages, synovial fibroblasts and T cells express IL-1, TNF-α and RANKL, factors important for differentiation of osteoblasts to osteoclasts. Multinucleated osteoclasts degrade bone, thereby creating radiographically detectable erosions.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
20
II - CLINICAL ASPECTS OF RHEUMATOID ARTHRITIS
II - 1 Introduction The mode of disease onset and the course of the disease may be extremely variable. Some patients
have a very acute disease onset with dramatic symptoms with fever, polyarthritis and extra-articular
manifestations, whereas a gradual and insidious onset is more common. Typical articular symptoms
and findings include pain, stiffness and swelling. Concomitant tenosynovitis, bursitis and even carpal
tunnel syndrome may be present. Extra-articular features are also rather common, especially
generalized weakness, weight loss or low-graded fever.
A special type of RA has been called palindromic rheumatism. This clinical picture includes variable
episodes of polyarthritis which suddenly may affect one or more large or peripheral joints. The
duration may be hours or a few days and then spontaneous improvement with complete
disappearance of all rheumatic signs between attacks. About one third of these palindromic cases will
eventually evolve into typical RA.
Both prevalence and incidence rates are about 2- to 4-fold higher in women, and symptoms appear to
be more severe than in men (65). The female/male ratio decreases with age. The reasons for the
greater prevalence of RA among women have not been firmly established.
A decline in the incidence of RA over recent decades has been reported in a number of countries
(e.g. Finland, England/Wales, United States and Japan). The decreasing incidence has been
especially apparent in women possibly as a consequence of some environmental factor such as the
introduction of oral contraceptives in the 1960s (66). A shift in the incidence towards the higher age
at disease onset has been observed across several cohorts. The incidence rate seems to increase
with age up to a plateau around 60 years (67).
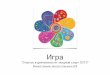
II – 2 Disease onset II - 2 - 1 Articular Manifestations The typical joint involvement at disease onset is symmetric swelling of the proximal interphalangeal
(PIP) joints, the metacarpophalangeal (MCP) joints, the wrists (Figure 5), and the metatarso-
phalangeal (MTP) joints. However, the disease may also start gradually with involvement of one or
few joints and then over time develop from undifferentiated oligo- or polyarthritis into a more
polyarticular disease with fulfilment of the RA classification criteria. Sometimes the disease also starts
with monoarthritis, e.g. of the knee. The differential diagnoses may vary according to the pattern of
joint involvement at disease onset. Sometimes the disease onset may be similar to reactive arthritis,
but generalized osteoarthritis is a more common differential diagnostic consideration with polyarticular
involvement in patients in the age of 50-60 years.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
21
Figure 5: Symmetric swelling of the proximal interphalangeal (PIP) joints, the metacarpo-phalangeal (MCP) joints, and the wrists are typical in rheumatoid arthritis
II - 2 - 2 Extra-articular Manifestations The dominating feature at disease onset is usually joint involvement. However, the disease may start
much more dramatically with fever and inflammatory manifestations of internal organs, e.g. with
pericarditis and pleuritis. In such cases, other systemic diseases may be the most important
differential diagnoses, e.g. systemic lupus erythematosus.
II - 2 - 3 Symptoms The symptoms of the patient will typically reflect the most prominent disease manifestations at
disease onset. Joints with inflammation are painful, tender and the patient perceives stiffness on
movement. The patients may also observe that the joints are swollen. A general feeling of morning
stiffness is common and typical. Other frequently occurring general symptoms include fatigue and
loss of energy.
II - 2 - 4 Clinical Findings The typical clinical finding of inflamed joints is soft tissue swelling and tenderness, and frequently also
limited motion (Figure 6). Detection of synovitis is essential for the diagnosis (Figure 7 and 8). The
joint swelling of the finger joints will often be symmetric and the same may be seen in middle sized
joints, eg the wrists, and in the forefeet. Involvement of shoulders and hips at disease onset is rare.
The clinical examination should include a general organ examination as extra-articular manifestations
may be present. In cases with serositis, clinical signs of pericarditis and pleuritis may be present. A
general organ examination is also important for the assessment of possible concomitant diseases,
since many of the relevant medications may lead to adverse reactions and interfere with existing
concurrent conditions.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
22
Figure 6: Early synovitis of PIP and MCP joints -source http://www.lecofer.org-
Figure 7: Detecting synovial effusion with two-finger technique, flexing the proximal phalanx at 30. -source http://www.lecofer.org-

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
23
Figure 8: Detecting PIP synovial effusion; four-finger technique -source http://www.lecofer.org-
II - 2 - 5 Laboratory investigations Typical findings are slightly or moderately elevated erythrocyte sedimentation rate and C-reactive
protein. Thrombocytosis and sometime leucocytosis is seen in patients with active inflammatory
disease. Reduced hemoglobin is also common. Serum iron may be lowered whereas ferritin
concentration may be elevated as a reflection of the acute phase reaction. It is important to do a
general laboratory screening including liver function test and creatinine as well as urine examination
to examine whether there are any indications of liver or kidney abnormalities.
Most importantly, tests for rheumatoid factor and/or anti-CCP are important both for the diagnosis and
for the staging of the disease since presence of rheumatoid factor and anti-CCP are associated with a
more severe disease course. Other immunological examinations may be important for differential
diagnoses. It is common to examine for the presence of antinuclear antibodies (ANA), but the value of
this test can be questioned if there is no clinical indication of any systemic connective tissue disease.
The presence of anti-nuclear antibodies has not been shown to have any prognostic value. However,
secondary Sjögren’s syndrome can be seen together with RA and in some infrequent cases the
typical immunological markers of Sjögren’s syndrome (anti-SSA and anti-SSB) may also be present
in RA.
II - 2 - 6 Imaging procedures Ultrasonography may be helpful at disease onset to demonstrate synovitis of involved joints.
Experienced ultrasonographists also claim that they can see synovitis with ultrasonography and
Doppler, which is not clinically detectable (Figure 9). More research is needed in this area.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
24
Figure 9: Ultrasonography with Doppler to detect synovitis of the MCP joints (S=synovitis, C=capsule, IP=interphalangeal) -source http://www.lecofer.org-
Ultrasonography may also be useful to detect erosions of smaller joints at an early stage of the
disease.
Conventional radiographic examinations are still the gold standard. Presence of erosions is one of the
key features of the classification criteria of rheumatoid arthritis, but diagnosis should ideally be
established before erosions are seen on radiographs. However, radiographic examinations of the
hands, wrist and feet are important as baseline examination for the subsequent monitoring of the
disease. Without the baseline radiographic assessment it will be difficult assess radiographic
progression which is considered as an unfavourable prognostic sign. Scoring systems have been
developed to assess the level of and changes in radiographic damage, e.g. the van der Heijde
modified Sharp score (68).
MRI of wrist and finger joints may be an important tool for early diagnosis and staging of the disease.
Synovitis can be seen when the imaging procedure is performed with gadolinium contrast. Bone
marrow oedema is also a typical finding, which is considered as a predictor of subsequent erosions,
but bone marrow oedema is a rather unspecific finding which may also be seen in other joint
diseases, including osteoarthritis. Erosions are seen earlier with MRI than with conventional
radiographs (69).
II - 2 - 7 Diagnosis The formal diagnosis of RA is based on presence of four out of seven items in the ACR classification
criteria from 1987 (table 1)(8). These criteria are much criticised because they are not very useful for
early disease since four of the first items reflect disease activity and the three last items reflect
disease severity and may develop with time (eg erosions and subcutaneous noduli).
Until new classification criteria have been developed the concept of undifferentiated arthritis
(persistent arthritis in patients not fulfilling the classification criteria) is important. Several studies have
shown that undifferentiated arthritis may progress into RA (70) and patients with undifferentiated
arthritis should also be considered for disease modifying therapy, also to prevent progression into RA
(71). However, this therapeutic consideration must also take individual prognostic markers into
account.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
25
Table 1: ACR classification criteria for RA (8) At least four of the following criteria
a. Morning stiffness >1 hour b. Arthritis of ≥3 joint areas c. Arthritis of hand joints d. Symmetric arthritis e. Rheumatoid nodules f. Serum rheumatoid factor g. Radiographic changes
a, b, c and d must have been present for at least 6 weeks
II - 2 - 8 Differential Diagnoses The differential diagnoses to be considered depend on the clinical picture at disease onset.
The incidence of RA increases with age and reaches a plateau around 60 years of age. This means
that hand osteoarthritis/generalized osteoarthritis often will be the most frequent differential diagnosis
to be considered in patients with a typical polyarticular disease with involvement of finger joints. The
typical clinical feature which differentiates RA from hand osteoarthritis is involvement of the MCP and
wrist joints, which are very infrequently involved in hand osteoarthritis (except in cases with
haemochromatosis). Table 2 shows the typical features that separate osteoarthritis and RA.
Polymyalgia rheumatica is also an important differential diagnosis in elderly patients. RA in the elderly
may start with polymyalgic symptoms and it may be difficult to differentiate between elderly onset RA
and polymyalgica rheumatica with concurrent arthritis. The arthritis in these cases is often rheumatoid
factor negative and large joints are more frequently involved than the small finger joints. A
differentiation between inflammatory rheumatic disease and osteoarthritis of large joints with
secondary synovitis can also be relevant in these cases.
In younger patients it is more likely that the clinician has to differentiate between RA and other
inflammatory rheumatic diseases. Another important differential diagnosis is reactive arthritis. Knees,
ankles and MTP-joints are more frequently involved in reactive arthritis whereas finger joints and
wrists are infrequently affected. Among the connective tissue diseases systemic lupus erythematosus
is the most frequent differential diagnosis.
Psoriatic arthritis and rheumatoid factor negative RA can also be difficult to differentiate. It is common
to classify polyarthritis combined with the presence of rheumatoid factor as RA even if the patient has
psoriasis whereas rheumatoid factor negative arthritis combined with psoriasis is classified as
psoriatic arthritis.
The incidence of various inflammatory arthropathies has been examined in Southern Sweden (72) and in Finland (73) and these results highlight that many inflammatory arthropathies have to be
considered in patients with recent onset joint swelling.
(Table 3).

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
26
Table 2: Typical features of osteoarthritis versus rheumatoid arthritis OA RA Disease characteristic Cartilage degeneration with
mild inflammation Synvial inflammation leading to damage of cartilage and bone
Age of onset Usually 50-60+ All ages Joint involvement hands DIP, PIP, CMC joints PIP, MCP, wrist joint Joint involvement feet MTP I All MTP Synovial fluid Low cell count, high viscosity High cell count, low viscosity Synvial fluid, predominant cell Mononuclear Polymorphnuclear Radiographic abnormalities Joint space narrowing,
osteophytes, bony sclerosis Joint space narrowing, erosions
Blood tests Normal Elevated acute phase reactants, rheumatoid factor
DIP=distal interphalangeal PIP=proximal interphalangeal MCP=meatcarpophalangeal CMC=carpo-metacapal MTP=metatarsophalangeal
Table 3: The most common inflammatory joint diseases that have be considered as differential diagnoses to rheumatoid arthritis (72, 73)
Psoriatic arthritis Spondylarthopathies Polymyalgia rheumatica with peripheral arthritisReactive arthritis Acute sarcoid athropathy (Löfgren’s syndrome) Systemic Lupus Erythematosus Other connective tissue diseases
II - 2 - 9 Disease Assessment Several quantitative measures can be used to evaluate the activity and severity of the disease, as
well as the disease consequences for the individual.
Core measures of disease activity include tender and swollen joint counts, patient and investigator
global assessments of disease activity on a visual analogue scale (VAS), intensity of joint pain on a
VAS, a patient-reported measure of physical disability (usually health assessment questionnaire) and
acute phase reactants (erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)).
These individual disease activity measures can be combined into composite measures. The Disease
Activity Score-28 (DAS28) includes 28-swollen joint counts (28-SJC) and 28-tender joint counts (28-
TJC) in addition to patient global assessments of disease activity on a visual analogue scale (VAS)
and erythrocyte sedimentation rate (ESR). Predefined cut-offs for remission, low and moderate
disease activity are 2.6, 3.2 and 5.1, respectively (74).
Simplified Disease Activity Index (SDAI) (75) employs a linear sum of 5 untransformed, not weighted
variables, including 28-SJC and 28-TJC, patient and investigator global assessments of disease
activity on a VAS and C-reactive protein (CRP). Predefined thresholds for remission, low and
moderate levels of disease activity are 3.3, 11 and 26, respectively.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
27
Clinical Disease Activity Index (CDAI) (76) is a modification of SDAI sparing laboratory evaluation
(CRP) to allow immediate clinical assessment. Thresholds for separating remission, low and
moderate levels of disease activity are at 2.8, 10 and 22.
The algorithms for calculation of the composite scores in SPSS are shown in Table 4.
The Ritchie articular index was widely used before and is based on the assessment of joint
tenderness in several joints and joint areas.
Functional disability is most commonly measured by the Stanford Health Assessment Questionnaire
(HAQ), which is the most widely used instrument measuring disability in RA. The shortened version,
the Modified Health Assessment Questionnaire (MHAQ), reduces the number of items from 20 to 8,
one for each of the eight components, and does not allow upgrading of scores by use of technical
devices or help by another person. However, several other generic and disease specific measures
are available for assessment of physical disability and other important dimensions of health related
quality of life (see separate in depth discussion).
Joint damage is usually assessed by imaging modalities, using one of the accepted scoring systems
to assess erosions and joint space narrowing. The most widely used systems are the Larsen score
and the Sharp score (with modifications by Genant or van der Heijde). Clinical scores of deformities
are also available (77).
Table 4: SPSS Syntax for calculation of DAS28, CDAI and SDAI COMPUTE sdai = SUM.5(SJC28,TJC28,(Physgloba/10),(Patglobal/10),(CRP/10)). EXECUTE . COMPUTE cdaiV1s = SUM.5 (SJC28,TJC28,(Physgloba/10),(Patglobal/10),). EXECUTE . DAS28 = 0.555 * (SQRT(TJC28))+0.284*(SQRT(SJC28))+0.70*LN(ESR)+0.0142*Patglobal. EXECUTE .
II - 2 - 10 Identification of Prognostic Markers Since RA can have a variable disease course, it is of particular importance and relevance to identify
markers that may predict the disease course. The ideal situation is to be able to tailor treatment
according to such indicators, ie to treat patients with predictors of severe disease course
aggressively, and to protect patients with a potentially mild disease from drugs that are associated
with severe adverse reactions.
Three different outcomes can be considered to be of particular relevance; radiographic damage,
functional disability, and mortality. Table 5 shows known predictors for these long-term outcomes.
Radiographic progression is considered a key outcome variable, as it is thought to reflect the
cumulative effect of inflammation on bone and cartilage. Further, joint damage accounts for a
considerable amount of the disability in RA, both in established and in earlier phases of the disease
(78).

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
28
An optimal treatment strategy should include considerations on the presence or absence of predictors
of joint damage, since prevention of such damage is a major treatment goal. Several studies have
shown that female gender and the presence of erosions are predictors of progressive radiographic
abnormalities in RA.
The markers that are most relevant to consider in clinical practice are one of the composite disease
activity scores and laboratory markers. IgM serum rheumatoid factor (IgM-RF) has consistently been
shown to predict radiographic damage. Recent studies have shown that antibodies to cyclic
citrullinated peptide (Anti-CCP) is the strongest independent predictor of radiographic damage and
also that radiographic progression is associated with the level of antibodies. Several studies have
also shown that ESR and CRP are independent predictors of radiographic damage.
One recent Norwegian study showed that anti-CCP, IgM RF, ESR and female gender all were
independent predictors of radiographic progression and could be combined into an algorithm for
better prediction. Anti-CCP was the strongest contributor to the overall prediction model. In this study,
patients with high levels of anti-CCP were 10 times more likely than anti-CCP negative patients to
develop radiographic progression, and about 5 times more likely than patients with low-moderate
levels (79).
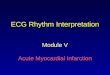
The algorithm with anti-CCP, IgM RF, high ESR and female gender predicted radiographic
progression on the individual level with good accuracy (Figure 10). Prediction of mild disease
(specificity) however, is more difficult than prediction of progressive disease (sensitivity).
In summary, an appropriate work-up in early RA should include both the evaluation of diagnosis and
also the evaluation of prognostic markers by assessing signs of structural damage, acute phase
reactants, number of swollen joints, rheumatoid factor, anti-CCP and disability level. Patients with
markers indicating severe and progressive disease should have the highest priority for early and
aggressive treatment with DMARDs.
Table 5: Prediction of outcome in RA
Prediction of future physical disability (HAQ-score)
Prediction of structural Damage
Prediction of increased mortality
HAQ score Age Acute phase reactants (?) Female gender (?) Level of education (?) Joint counts (?) Rheumatoid factor (?) Erosive disease (?)
Erosive disease Acute phase reactants Rheumatoid factor Anti-CCP Joint counts (?) Genetic markers (shared epitope) Female gender (?) Present HAQ score (?)
Age Level of education /coping Physical status Rheumatoid factor Comorbidities Extraarticular manifestations
Gender (?) Joint counts (?) Acute phase reactants (?) Structural damage (?) Use of corticosteroids (?)

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
29
Figure 10: Probability of radiographic progression – blue bars: males, red bars: females (from 79)
II – 3 Recent onset arthritis
Patients should be monitored frequently during the first years of the disease. It is assumed that tight
control of the patients in this period is important to achieve an acceptable disease state and to
prevent future damage and disability, since it seems to be an association between level of
inflammatory activity and future damage.
This concept has been supported by some recent studies, eg the TICORA study (80). Patients who
were followed by a tight control of disease activity had less radiographic progression than patients
followed by a regular follow-up regimen. Thus, it is recommended that patients should be followed
with assessment of disease activity (eg by DAS-28) and by a patient-reported outcome, e.g. HAQ.
The ideal situation is probably to predefine a targeted level of disease activity and to adjust therapy
until this target is achieved.
II – 4 Established disease The clinical challenge in patients with established disease is different from recent onset or early RA.
The joint involvement will often be dominated by deformities as a consequence of long-standing
inflammation and radiographic damage. However, active inflammation may still be present and should
be treated, also to prevent further radiographic damage, deformities and disability.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
30
In established disease, it is also particularly important to be aware of the possibility of involvement of
internal organs due to RA. Surgical procedures can be relevant for individual patients and a detailed
examination of joints with particular focus on functional consequences of deformities may be clinically
relevant.
II – 4 - 1 Involvement of Hands Involvement of the distal interphalangeal joint is infrequent and may rather indicate concurrent
osteoarthritis. MCP and PIP joints are frequently involved. Deformities of the PIP joints usually result
from lack of ligament support. Boutonnière deformity (Figure 11) describes a finger with flexion of the
PIP joint and hyperextension of the DIP joint. The similar deformity of the thumb is also called the 90-
90 thumb because both the flexion of the MCP and the hyperextension of the IP joint may be 90
degrees (Figure 12). A swan-neck deformity of the finger describes a hyperextension of the PIP joint
and a flexion of the DIP joint (Figure 13).
Deformities of the MCP joints include volar subluxation, which may be seen as a step, ulnar drift
(often in combination with radial deviation of the wrist) and flexion deformities.
Wrist deformities are common and include volar subluxation with a visible step opposite the
radiocarpal joint and radial deviation of the carpus from the axis of the wrist and hand.
Arthritis of the distal radioulnar joint results in instability and dorsal subluxation of the ulnar head with
a “piano key” movement on downward pressure. A dorsally subluxated ulnar head with erosive
abnormalities will often mechanically lead to rupture of neighbouring tendons (Figure 14).
II – 4 - 2 Elbow and Shoulder The elbow joint is frequently involved in established RA. Loss of extension is a typical early sign.
Functionally, loss of supination is disabling when eating and performing daily activities. The other
disabling limited motion is reduced flexion. This may lead to inability to reach hair, face etc. Thus,
maintenance of flexion and supination is functionally extremely important objectives.
Shoulder involvement in RA is not very frequent, but most patients with severe disabling RA also
have shoulder involvement. Shoulder symptoms will usually appear when joint destruction has
become advanced and will limit daily self-care activities. Synovitis leads to erosion and damage of
both the humeral head and glenoid fossa.
The long head of the biceps muscle may rupture. This can be detected as a biceps bulge when the
patient flexes the elbow against resistance. The rotator cuff can also frequently be involved with
inflammation and destruction. Involvement of the acromioclavicular joint is infrequent. The shoulder
pain is typically localized in the C4 region whereas pain developing from the humerogleoidal joint or
from the rotator cuff is typically in perceived in the C5 region including the upper arm.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
31
Figure 11: Boutonnière deformity of the finger -source http://www.lecofer.org-
Figure 12: Z-deformity or 90-90 deformity of the thumb -source http://www.lecofer.org-

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
32
Figure 13: Swan-neck deformity of the finger -source http://www.lecofer.org-
Figure 14: Rupture of the extensor tendons -source http://www.lecofer.org-
II – 4 - 3 Cervical Spine Involvement of the cervical spine is particularly important. The space between the odontoid process
from C2 and the arch of the atlas normally measures 3 mm or less. If this space exceeds 5 mm
(some clinicians will say 3 mm) the condition is defined as atlantoaxial subluxation. There is a
synovial articulation between the transverse ligament of the atlas of the posterior aspect of the
odontoid. This transverse ligament prevents a forward slip of C1 on C2 and continuing synovitis in
this articulation compromises the ligament and may produce erosions of the dens.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
33
Synovial involvement may also affect the apophyseal joints in the occiput atlantal area. The
consequence of the synovitis in this area may be an atlanto-axial subluxation.
This deformity is important and should be detected before general anaesthesia. When a patient with
RA requires surgery the presence of cervical subluxation presents a general anaesthetic risk. Routine
cervical radiographs with the head in flexed position is recommended before surgical procedures.
Special precautions are required preoperatively to prevent cervical cord damage when atlantoaxial
subluxation is detected.
When considering the cervical spine at the C1-C2 level it is helpful to divide the space through the
arch of the atlas into thirds, one third for the odontoid process, one third for the spinal cord and one
third free. If the C1-C2 slip exceeds 10 mm the free third is lost and cervical cord damage becomes a
risk. In these cases neurological assessment is required and an MRI examination may provide
important information about the space available for the neurological structures. Wearing a stiff collar
can be important for patients with atlanto-axial subluxation, especially in situations at risk for a neck
injury. Some patients will require surgical procedures to correct the subluxation of the cervical spine.
Sometimes even more severe deformities may occur, with the odontoid process moving upwards to
the foramen magnum with basilar invagination and a threat to the upper cervical cord and medulla.
II – 4 - 4 Joints of the Lower Limbs The hip is infrequently involved in RA, but may also be destroyed, even if this is more likely in patients
with ankylosing spondylitis.
Knee involvement is much more common in RA. Synovial effusion is the typical sign of inflammatory
activity of the knee. Patients with knee swelling have a tendency to assume a more comfortable
position with the knee flexed, and if this becomes a habit, a loss of full knee extension eventually
results.
Reduction of knee extension may be associated with a cyst of the popliteal region called Baker’s cyst.
This cyst can extend from its location in the gastrocnemius bursa down into the medial aspects of the
calf. This is best seen when patients are standing. The Baker’s popliteal cyst arises as an extension
from the joint cavity. Rupture of this cyst can give a general swelling of the calf and a clinical picture
which mimics deep vein thrombosis.
Destruction of the knee may lead to instability due to laxity of the collateral and cruciate ligaments.
This laxity is detected by stressing the knee joint for lateral and medial colateral stability. A special
problem arises in women with physiological valgus. This valgus increases the load on the lateral
compartment and as the valgus increases due to arthritis the loading will also increase so that a
vicious cycle is produced. Varus position is more common in osteoarthritis than in rheumatoid
arthritis.
Within the foot, the subtalar and mid-tarsal joints are more frequently involved than the ankle joint.
The ankle is usually quite stable, but reduced dorsal flexion may interfere with walking ability. The
subtalar and talonavicular joints are commonly affected in RA.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
34
Synovitis causes pain and stiffness and will sometimes lead to subtalar dislocation. As cartilage loss
and bone erosion develop, valgus deformity increases with progressive flattening of the longitudinal
arch.
Involvement of the MTP joints is extremely common in RA and causes much pain and disability.
Forefoot deformity starts with synovitis of the MTP-joints and the involvement of the flexor tendons.
This involvement is often followed by clawing of the toes and dorsal dislocation of the MTP-joints
(Figure 15). The metatarsal heads are destroyed due to the synovitis and can lead to extreme pain.
Figure 15: Toes with many claws -source http://www.lecofer.org-
II – 4 - 5 Other Joint Areas The temporal mandibular joint may be involved with tenderness and painful limitation of mouth
opening. Occasionally the cricoarytenoid joint may be involved and associated with hoarseness. The
ossicles of the ear may also be involved with hearing loss independent of medication-induced effects.
II – 4 - 6 Nodules, Tenosynovitis and Bursitis Subcutaneous nodules overlying the extensor aspects of the proximal ulna are present in about one
quarter of patients with RA. Subcutaneous nodules may form over other pressure locations such as
the occiput, palms of the hands and Achilles tendon (Figure 16).
Flexor tenosynovitis can lead to loss of active flexion. A trigger finger is a frequent feature of flexor
tenosynovitis. The pathology is a thickening of the tendon or may be stenosis of the tendon sheet. A
rupture of flexor tendons may occur but are much less common then extensor ruptures.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
35
Figure 16: Cutaneous nodules in rheumatoid arthritis -source http://www.lecofer.org-
Flexor tenosynovitis is often also accompanied by a tenosynovitis of the carpal tunnel, which may
lead to entrapment of the medial nerve and development of a carpal tunnel syndrome. The patients
will have weakness and finger tingling and sensory loss, especially in the index and middle finger.
Diagnosis can be established by neurographic examination or by ultrasonography.
Extensive tendon involvement is frequent as a swelling of the dorsum of the wrist, below the extensor
retinaculum. Asking the patients to extend the fingers will accentuate the swelling.
Bursae should not be overlooked in the evaluation of any joint region. The bursae are lined by a
synovial membrane that secrets synovial fluid and may develop rheumatoid synovitis. Involvement of
the olecranon bursa by rheumatoid arthritis is a typical example of bursitis. Other bursae that
frequently can be involved are the subacromial bursa, trochanteric and sub achilles bursa.
II – 4 - 7 Extra-articular Manifestations Articular manifestations are usually dominating when RA patients present to their doctors or when
therapeutic decisions are made in an effort to improve functional outcome. Non-articular
manifestations may include subcutaneous nodules, vasculitis, pericarditis, pulmonary nodules or
interstitial fibrosis, mononeuritis multiplex, episcleritis or scleritis. Some of the manifestations are
related to the inflammatory activity and should then be considered as markers of the disease process,
while others are to be considered as damage due to longstanding disease.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
36
II – 4 - 7 - 1 Secondary osteoporosis The skeleton is built of cortical and trabecular bone. It has been clearly demonstrated that RA is
associated with an increased generalized bone-loss, assessed by measures of bone mineral density
(BMD) (81). Increased occurrence of vertebral as well as non-vertebral fractures has also been
demonstrated. It is also been shown that RA in itself is directly associated to the increased
occurrence of vertebral fractures (82). There is a two-fold increase in the occurrence of osteoporosis
both in RA males and females. It is generally assumed that osteoporosis is due to inflammation (e.g.
cytokine release with osteoclast activation), use of glucocorticoids and immobility. It is important to
have focus on the bone health and to assess BMD in patients at risk. Preventive treatment (vitamin D
and calcium) should be considered, and in addition, anti-resorptive therapy when clinically indicated. II – 4 - 7 - 2 Muscles Muscle weakness and atrophy (Figure 17) is common in RA, often due to either neuropathy, use of
steroids, or less use due to joint involvement.
Figure 17: Interosseous muscle atrophy -source http://www.lecofer.org-

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
37
II – 4 - 7 - 3 Secondary Sjögren’s syndrome Secondary Sjögren’s syndrome is a typical manifestation of rheumatoid arthritis with sicca symptoms
from eyes and also dryness of the mouth.
The exocrine function of tear glands and salivary glands may be altered in rheumatologic disorders
such as Sjögren’s syndrome, or secondary to RA and other connective tissue disorders. Some
studies had indicated such an affection in RA with secondary Sjögren’s syndrome may be common,
benign with subclinical manifestations, but with histological changes in salivary glands. Sicca
symptoms from eyes and mouth are frequent in RA, and about 10% of the patients seem to have
secondary Sjögren’s syndrome. Diagnoses can be established by applying tests for reduced saliva
and tear production.
Schirmer-I test is performed by placing a test strip in each eye between the medial and lateral parts of
the lower eyelid. After five minutes the strips are examined and a positive result is recorded if the
strips are wetted 5 mm or less in one or both eyes.
II – 4 - 7 - 4 Other eye complications Scleritis, episcleritis or both occur in some patients with RA, but are rather infrequent. In episcleritis
the eye becomes red within minutes. Unlike other inflammatory conditions of the eye, episcleritis
results in no discharge other than tearing in response to great discomfort. Loss of vision does not
occur as a direct result of episcleritis but cataracts may develop secondarily and cause visual loss.
Scleritis causes severe ocular pain and a dark red discolouration.
II – 4 - 7 - 5 Infections The incidence of infections as a complication of RA is increased partly due to the disease in itself,
partly due to use of glucocorticoids and other drugs with immuno-suppressive actions, in particular
the new anti-TNF-drugs. It is important to be aware that RA in itself also increases the risk for septic
arthritis. It can be extremely challenging to differentiate between an acute flare of arthritis or a septic
arthritis. The most important examination is to culture the synovial fluid.
II – 4 - 7 - 6 Cancer There is a slight increased risk of malignancy in RA patients, especially for lymphoma in certain
patient subsets. It has been clearly shown that this risk is related to the severity and inflammatory
activity of the disease (83). II – 4 - 7 - 7 Hematologic abnormalities The majority of patients with RA have a mild normocytic hypochromic anaemia that correlates with
ESR elevation and the activity of the disease. A few of these patients respond to iron therapy. Folate
and B12 deficiency may also be a cause of anaemia in RA. Thrombocytosis is frequent in RA and is
associated to disease activity.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
38
II – 4 - 7 - 8 Vasculitis One of the initial pathological changes in RA includes inflammatory changes in small blood vessels.
However, when talking about vasculitis as a complication, the focus is more on the arteries or
arterioles that lead to cutaneous ulceration (Figure 18) or peripheral neuropathy or involvement of
internal organs. Vasculitis is fortunately rather uncommon, but the presence of vasculitis is associated
with disease severity and activity. Neurovascular disease may be the only manifestation of vasculitis.
The two common clinical patterns are a mild distal sensory neuropathy and a severe sensory motor
neuropathy (mononeuritis multiplex). The latter form is characterized by severe arterial damage on
nerve biopsy specimens. Symptoms of the milder form may be parasthesia or burning feet in
association with decreased touch and pin sensation distally. Severe vasculitis must be managed
aggressively. Organ specific vasculitis can lead to organ infarctions.
Figure 18: Cutaneous vasculitis -source http://www.lecofer.org-
II – 4 - 7 - 9 Renal disease The kidney is rarely directly involved in RA but may be compromised by therapy. Both analgesics and
NSAIDs as well as some of the previously used DMARDs (e.g. gold preparation and penicillamine)
could lead to renal disease.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
39
II – 4 - 7 - 10 Pulmonary disease There are several forms of lung disease in RA. Pleuritis can be seen both at disease onset and during
the disease course and may be seen together with pericarditis. Interstitial pneumonitis and fibrosis is
rather common in long-standing RA. Nodular lunge disease can be seen but usually in patients who
also have rheumatic nodules in other parts of the body (Figure 19). Pulmonary hypertension may
also occasionally be seen.
Figure 19: Nodular lung disease -source http://www.lecofer.org-
II – 4 - 7 - 11 Cardiac complications Pericarditis can be seen as part of the inflammatory activity with RA and is often present concurrent
to pleuritis. Inflammation of the myocardium and endocardial inflammation may also be present.
Conduction defects are unusual. As are coronary arthritis.
II – 4 - 7 - 12 Arteriosclerosis Several studies have shown that patients with RA have an increased risk of clinical coronary heart
disease (CHD) compared with age- and sex-matched non-RA subjects, and that this risk is
maintained also after accounting for traditional CHD risk factors (diabetes mellitus, hypertension,
dyslipidemia, body mass index, smoking). One study suggests that the risk of CHD in RA patients
even precedes the ACR criteria-based diagnosis of RA (84). The understanding of atherosclerosis
has evolved from a passive process resulting in narrowing of the lumen and consequent myocardial
ischemia to a dynamic process that involves inflammation.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
40
Some studies support the view that atherosclerosis is correlated to the level of inflammatory activity
over time and that the inflammatory process impacts cardiovascular morbidity and mortality and
accelerated coronary and extra-coronary atherosclerosis (85). The therapeutic consequence is that
anti-inflammatory therapy then would reduce the risk, and some studies have supported that therapy
with methotrexate (86) and anti-TNF drugs (87) may reduce cardiovascular morbidity and mortality.
II – 4 - 7 - 13 Gastrointestinal manifestations The disease itself is not associated to any increased morbidity of the gastrointestinal tracts. Gastro-
duodenal ulcers are, however, rather frequent due to use of NSAIDs. Liver disease may also be
secondary to drugs commonly used in RA, e.g. methotrexate, diclofenac and other NSAIDs as well as
paracetamol.
II – 4 - 7 - 14. Secondary amyloidosis Secondary amyloidosis may complicate rheumatoid arthritis, causing nephropathy and various
internal manifestations. Amyloidosis results from the deposition in various organs of autologous
protein in an insoluble fibrillar form. In patients with RA, excess serum amyloid A protein production is
stimulated by the cytokines of the inflammatory response. In most clinical settings, secondary
amyloidosis is now a rare problem in clinical practice, probably due to more effective therapies with
intensive suppression of the inflammatory activity. Previously, renal amyloidosis was a rather frequent
complication leading to renal failure, dialysis and renal transplantation.
II – 4 - 8 Functional Disability and its Consequences
RA is associated with significant pain and joint destruction, and progressive loss of mobility and the
ability to care for oneself. Pain is the area of health where the majority of patients would like to see
improvement (88). Important correlates of functional disability in RA patients include female sex, age,
disease duration, and disease activity measures such as the Ritchie articular index and erythrocyte
sedimentation rate (ESR), which can be considered predictors of a poorer functional status. In
addition to indicating a requirement for more aggressive treatment, high levels of disability have a
negative impact on the psychological and social functioning of the patient, the consequences of which
include mental distress, depression and fatigue. Pain and disability are the two variables most
consistently related to mental distress, and high levels of disability with a consequent decreased
ability to cope are commonly associated with depression, even in the early stages of the illness. This
association of RA with depression has important implications for the overall health care burden of the
disease and points to the need to address depression as part of a patient’s comprehensive treatment
plan.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
41
Fatigue is also a significant and frequently debilitating problem for people with RA, as it contributes to
work difficulties, personal injury, reduced ability to participate in rehabilitation programs, and strained
relationships. Fatigue scores are significantly higher in patients with RA than in healthy individuals,
and RA patients with a history of affective disorder have higher levels of fatigue than those without
such a history.
II – 4 - 9 Mortality While RA has traditionally been regarded as a chronic, painful, disabling condition with an essentially
non-fatal outcome, numerous studies conducted over the last four decades have found that it is
associated with an increased mortality in comparison with the general population of the same age
and gender. However, the extent of the increased mortality risk has not been consistent, as
standardised mortality ratios (i.e. the ratio of deaths among RA patients compared with the age-
matched general population) have been reported to range from 1.16 to 3.0 in studies conducted in
various countries. Some studies show a more pronounced increase in mortality in females. Disease
severity, activity and disability are strongly linked to mortality in RA sufferers, and other independent
predictors include age, level of education, male sex, co-morbidity, and usage of prednisone.
However, whether prednisone usage is a marker of disease severity or is, in itself, deleterious is
unclear. The major contributing causes of death among RA patients are cardiovascular and
cerebrovascular diseases. Male sex and age at disease onset have been found to predict both the
occurrence of cardiovascular events and death.
However, it is uncertain whether the results from these previous studies correctly reflect the current
mortality risk. Some studies have indicated that RA currently is a milder disease than some years ago
and also that the disease on average starts later than before, It is also assumed that the advances in
treatment strategies and access to new therapies improves the health of patients with RA. However, it
is still important to consider RA as a severe disease with a potential reduction in life expectancy.
II – 4 - 10 Has the Disease Improved? Potential outcomes to examine changes in disease severity over time include survival, needs for joint
replacement surgery and health status.
Decreased disease mortality has been reported from Sweden. Data from 47,000 patients were
collected from the Swedish Hospital discharge register. The patients were followed up after five and
ten years and linked to the cause of death register. Compared to patients discharged in the 1960s
and early 1970s, the following decades had a reduced mortality which was statistically significant
(89). Mortality in RA was still doubled, mainly due to cardiovascular disease. Interestingly a
decreasing mortality for patients in the last two of the three decades was observed.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
42
The frequency and cumulative incidence of surgery at the Mayo clinic at Rochester, Minnesota has
been examined. Almost 30% of 609 RA cases followed, underwent at least one surgical procedure for
RA related joint disease. Patients diagnosed with RA after 1985 and until 1995 were clearly less likely
to require RA related joint surgery when adjusting for duration of follow-up (90).
A shift to an older age at RA incidence has been reported during the last few years. If patients
contract RA at an older age today than earlier – and if we assume that disease progression would be
the same, then the average RA patient of today would be spared of several years disease severity
compared to RA patients several decades ago. Documentation of improved long-term outcome
requires long-term observational data over 5-20 years. Repeated cross-sectional data from the Oslo
RA register in 1994 and 2004 suggest an improved overall health status. For example the average
MHAQ score improved from 1.68 in 2004 to 1.58 in 2001. Similar findings were obtained for other
dimensions of health status (91).

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
43
Summary Points:
• Rheumatoid arthritis is a heterogeneous disease which can, based on data combining genetic risk
factors and autoantibodies, be sub-classified in ACPA-positive and -negative RA.
• ACPA are highly specific for RA, whereas RF can also be found among healthy (elderly) individuals
and patients with other autoimmune diseases.
• The most important genetic risk factor for RA development, the shared epitope alleles, resides in
the MHC class II region. Shared epitope alleles only predispose to the development of ACPA-
positive RA.
• Smoking is thus far the most important environmental risk factor associated with the development of
RA. Similar to shared-epitope alleles, smoking is a risk factor only for ACPA-positive RA.
• The concept that RA is a Th1-mediated autoimmune disease is currently under revision. Th17 cells
might be more crucially involved, and efficacy of B cell depleting therapy and the ACPA response
indicate that B cells are more relevant than previously anticipated.
• Presence of ACPA and RF as well as rising CrP-levels years before onset of clinical symptoms
indicate that relevant immune responses for RA development are initiated very early.
• RA development requires several factors acting at different points in time in an orchestrated
manner.
• The joint involvement dominates the clinical picture, but extra-articular manifestations may be
present both at onset and in established disease.
• The current classification criteria include items which are rather late signs (eg nodules and
radiographic damage).
• Early diagnosis is essential. Patients with undifferentiated arthritis may progress into RA.
• Identification of prognostic markers are as important as the labelling of the disease. Elevated acute
phase reactants, anti-CCP level and presence of rheumatoid factor seem to predict persistent
erosive arthritis.
• Several differential diagnoses need to be considered. RA starts most frequently after the age of 50,
thus, generalized osteoarthritis with finger involvement will often be an important consideration. In
younger age groups, reactive arthritis and connective tissue diseases will be more frequently
considered.
• Several types of deformities may develop, both in fingers and feet, and also in middle-sized and
large joints.
• Osteoporosis and arteriosclerosis are important extra-articular manifestations and probably related
to the inflammatory activity. More data are needed to clarify whether active anti-inflammatory
treatment also prevents these manifestations.
• The overall health and burden of disease has in many clinical settings improved over the last years,
most likely due to better treatment strategies and access to better diagnostic, monitoring and
treatment modalities.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
44
REFERENCES (key references are in bold)
1. Alamanos,Y., Voulgari,P.V., and Drosos,A.A. 2006. Incidence and prevalence of rheumatoid arthritis, based on the 1987 American College of Rheumatology criteria: a systematic review. Semin.Arthritis Rheum. 36:182-188.
2. Firestein,G.S. 2003. Evolving concepts of rheumatoid arthritis. Nature 423:356-361.
3. Brown,M.A., Newton,J.L., and Wordsworth,B.P. 2002. Genetics for Rheumatologists - The molecular genetic basis of rheumatological disorders. Remedica.
4. WITEBSKY,E., ROSE,N.R., TERPLAN,K., PAINE,J.R., and EGAN,R.W. 1957. Chronic thyroiditis and autoimmunization. J.Am.Med.Assoc. 164:1439-1447.
5. Waaler,E. 1940. On the occurrence of a factor in human serum activating the specific agglutination of sheep blood corpuscles. Acta Pathol Microbiol Scand 17:172-188.
6. FRANKLIN,E.C., HOLMAN,H.R., MULLER-EBERHARD,H.J., and KUNKEL,H.G. 1957. An unusual protein component of high molecular weight in the serum of certain patients with rheumatoid arthritis. J.Exp.Med. 105:425-438.
7. Zvaifler,N.J. 1973. The immunopathology of joint inflammation in rheumatoid arthritis. Adv.Immunol. 16:265-336.
8. Arnett,F.C., Edworthy,S.M., Bloch,D.A., McShane,D.J., Fries,J.F., Cooper,N.S., Healey,L.A., Kaplan,S.R., Liang,M.H., Luthra,H.S. et al. 1988. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 31:315-324.
9. NIENHUIS,R.L. and MANDEMA,E. 1964. A NEW SERUM FACTOR IN PATIENTS WITH RHEUMATOID ARTHRITIS; THE ANTIPERINUCLEAR FACTOR. Ann.Rheum.Dis. 23:302-305.
10. Young,B.J., Mallya,R.K., Leslie,R.D., Clark,C.J., and Hamblin,T.J. 1979. Anti-keratin antibodies in rheumatoid arthritis. Br.Med.J. 2:97-99.
11. Schellekens,G.A., de Jong,B.A., van den Hoogen,F.H., van de Putte,L.B., and van Venrooij,W.J. 1998. Citrulline is an essential constituent of antigenic determinants recognized by rheumatoid arthritis-specific autoantibodies. J.Clin.Invest 101:273-281.
12. Girbal-Neuhauser,E., Durieux,J.J., Arnaud,M., Dalbon,P., Sebbag,M., Vincent,C., Simon,M., Senshu,T., Masson-Bessiere,C., Jolivet-Reynaud,C. et al. 1999. The epitopes targeted by the rheumatoid arthritis-associated antifilaggrin autoantibodies are posttranslationally generated on various sites of (pro)filaggrin by deimination of arginine residues. J.Immunol. 162:585-594.
13. van Gaalen,F., Ioan-Facsinay,A., Huizinga,T.W., and Toes,R.E. 2005. The devil in the details: the emerging role of anticitrulline autoimmunity in rheumatoid arthritis. J.Immunol. 175:5575-5580.
14. Huizinga,T.W., Amos,C.I., van der Helm-van Mil AH, Chen,W., van Gaalen,F.A., Jawaheer,D., Schreuder,G.M., Wener,M., Breedveld,F.C., Ahmad,N. et al. 2005. Refining the complex

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
45
rheumatoid arthritis phenotype based on specificity of the HLA-DRB1 shared epitope for antibodies to citrullinated proteins. Arthritis Rheum. 52:3433-3438.
15. Hill,J.A., Southwood,S., Sette,A., Jevnikar,A.M., Bell,D.A., and Cairns,E. 2003. Cutting edge: the conversion of arginine to citrulline allows for a high-affinity peptide interaction with the rheumatoid arthritis-associated HLA-DRB1*0401 MHC class II molecule. J.Immunol. 171:538-541.
16. Kuhn,K.A., Kulik,L., Tomooka,B., Braschler,K.J., Arend,W.P., Robinson,W.H., and Holers,V.M. 2006. Antibodies against citrullinated proteins enhance tissue injury in experimental autoimmune arthritis. J.Clin.Invest 116:961-973.
17. Astorga,G.P. and Williams,R.C., Jr. 1969. Altered reactivity in mixed lymphocyte culture of lymphocytes from patients with rheumatoid arthritis. Arthritis Rheum. 12:547-554.
18. Stastny,P. 1976. Mixed lymphocyte cultures in rheumatoid arthritis. J.Clin.Invest 57:1148-1157.
19. Gregersen,P.K., Silver,J., and Winchester,R.J. 1987. The shared epitope hypothesis. An approach to understanding the molecular genetics of susceptibility to rheumatoid arthritis. Arthritis Rheum. 30:1205-1213.
20. Gourraud,P.A., Dieude,P., Boyer,J.F., Nogueira,L., Cambon-Thomsen,A., Mazieres,B., Cornelis,F., Serre,G., Cantagrel,A., and Constantin,A. 2007. A new classification of HLA-DRB1 alleles differentiates predisposing and protective alleles for autoantibody production in rheumatoid arthritis. Arthritis Res.Ther. 9:R27.
21. van der Helm-van Mil AH, Verpoort,K.N., Breedveld,F.C., Huizinga,T.W., Toes,R.E., and de Vries,R.R. 2006. The HLA-DRB1 shared epitope alleles are primarily a risk factor for anti-cyclic citrullinated peptide antibodies and are not an independent risk factor for development of rheumatoid arthritis. Arthritis Rheum. 54:1117-1121.
22. van der Helm-van Mil AH, Huizinga,T.W., de Vries,R.R., and Toes,R.E. 2007. Emerging patterns of risk factor make-up enable subclassification of rheumatoid arthritis. Arthritis Rheum. in press.
23. van der Helm-van Mil AH, Huizinga,T.W., Schreuder,G.M., Breedveld,F.C., de Vries,R.R., and Toes,R.E. 2005. An independent role of protective HLA class II alleles in rheumatoid arthritis severity and susceptibility. Arthritis Rheum. 52:2637-2644.
24. Wesoly,J., van der Helm-van Mil AH, Toes,R.E., Chokkalingam,A.P., Carlton,V.E., Begovich,A.B., and Huizinga,T.W. 2005. Association of the PTPN22 C1858T single-nucleotide polymorphism with rheumatoid arthritis phenotypes in an inception cohort. Arthritis Rheum. 52:2948-2950.
25. van der Helm-van Mil AH, Wesoly,J.Z., and Huizinga,T.W. 2005. Understanding the genetic contribution to rheumatoid arthritis. Curr.Opin.Rheumatol. 17:299-304.
26. Klareskog,L., Padyukov,L., Ronnelid,J., and Alfredsson,L. 2006. Genes, environment and immunity in the development of rheumatoid arthritis. Curr.Opin.Immunol. 18:650-655.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
46
27. Klareskog,L., Padyukov,L., and Alfredsson,L. 2007. Smoking as a trigger for inflammatory rheumatic diseases. Curr.Opin.Rheumatol. 19:49-54.
28. Klareskog,L., Stolt,P., Lundberg,K., Kallberg,H., Bengtsson,C., Grunewald,J., Ronnelid,J., Harris,H.E., Ulfgren,A.K., Rantapaa-Dahlqvist,S. et al. 2006. A new model for an etiology of rheumatoid arthritis: smoking may trigger HLA-DR (shared epitope)-restricted immune reactions to autoantigens modified by citrullination. Arthritis Rheum. 54:38-46.
29. Pedersen,M., Jacobsen,S., Klarlund,M., Pedersen,B.V., Wiik,A., Wohlfahrt,J., and Frisch,M. 2006. Environmental risk factors differ between rheumatoid arthritis with and without auto-antibodies against cyclic citrullinated peptides. Arthritis Res.Ther. 8:R133.
30. Bartfai,T., Waalen,J., and Buxbaum,J.N. 2007. Adipose tissue as a modulator of clinical inflammation: does obesity reduce the prevalence of rheumatoid arthritis? J.Rheumatol. 34:488-492.
31. Sverdrup,B., Kallberg,H., Bengtsson,C., Lundberg,I., Padyukov,L., Alfredsson,L., and Klareskog,L. 2005. Association between occupational exposure to mineral oil and rheumatoid arthritis: results from the Swedish EIRA case-control study. Arthritis Res.Ther. 7:R1296-R1303.
32. Jorgensen,C., Picot,M.C., Bologna,C., and Sany,J. 1996. Oral contraception, parity, breast feeding, and severity of rheumatoid arthritis. Ann.Rheum.Dis. 55:94-98.
33. Sakaguchi,S., Ono,M., Setoguchi,R., Yagi,H., Hori,S., Fehervari,Z., Shimizu,J., Takahashi,T., and Nomura,T. 2006. Foxp3+ CD25+ CD4+ natural regulatory T cells in dominant self-tolerance and autoimmune disease. Immunol.Rev. 212:8-27.
34. Toh,M.L. and Miossec,P. 2007. The role of T cells in rheumatoid arthritis: new subsets and new targets. Curr.Opin.Rheumatol. 19:284-288.
35. Murphy,C.A., Langrish,C.L., Chen,Y., Blumenschein,W., McClanahan,T., Kastelein,R.A., Sedgwick,J.D., and Cua,D.J. 2003. Divergent pro- and antiinflammatory roles for IL-23 and IL-12 in joint autoimmune inflammation. J.Exp.Med. 198:1951-1957.
36. Furuzawa-Carballeda,J., Vargas-Rojas,M.I., and Cabral,A.R. 2007. Autoimmune inflammation from the Th17 perspective. Autoimmun.Rev. 6:169-175.
37. Lundy,S.K., Sarkar,S., Tesmer,L.A., and Fox,D.A. 2007. Cells of the synovium in rheumatoid arthritis. T lymphocytes. Arthritis Res.Ther. 9:202.
38. van Amelsfort,J.M., Jacobs,K.M., Bijlsma,J.W., Lafeber,F.P., and Taams,L.S. 2004. CD4(+)CD25(+) regulatory T cells in rheumatoid arthritis: differences in the presence, phenotype, and function between peripheral blood and synovial fluid. Arthritis Rheum. 50:2775-2785.
39. Ehrenstein,M.R., Evans,J.G., Singh,A., Moore,S., Warnes,G., Isenberg,D.A., and Mauri,C. 2004. Compromised function of regulatory T cells in rheumatoid arthritis and reversal by anti-TNFalpha therapy. J.Exp.Med. 200:277-285.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
47
40. Nadkarni,S., Mauri,C., and Ehrenstein,M.R. 2007. Anti-TNF-alpha therapy induces a distinct regulatory T cell population in patients with rheumatoid arthritis via TGF-beta. J.Exp.Med. 204:33-39.
41. Valencia,X., Stephens,G., Goldbach-Mansky,R., Wilson,M., Shevach,E.M., and Lipsky,P.E. 2006. TNF downmodulates the function of human CD4+CD25hi T-regulatory cells. Blood 108:253-261.
42. Morgan,M.E., Flierman,R., van Duivenvoorde,L.M., Witteveen,H.J., van Ewijk,W., van Laar,J.M., de Vries,R.R., and Toes,R.E. 2005. Effective treatment of collagen-induced arthritis by adoptive transfer of CD25+ regulatory T cells. Arthritis Rheum. 52:2212-2221.
43. Dorner,T. 2006. Crossroads of B cell activation in autoimmunity: rationale of targeting B cells. J.Rheumatol.Suppl 77:3-11.
44. Mauri,C. and Ehrenstein,M.R. 2007. Cells of the synovium in rheumatoid arthritis. B cells. Arthritis Res.Ther. 9:205.
45. Leadbetter,E.A., Rifkin,I.R., Hohlbaum,A.M., Beaudette,B.C., Shlomchik,M.J., and Marshak-Rothstein,A. 2002. Chromatin-IgG complexes activate B cells by dual engagement of IgM and Toll-like receptors. Nature 416:603-607.
46. Lau,C.M., Broughton,C., Tabor,A.S., Akira,S., Flavell,R.A., Mamula,M.J., Christensen,S.R., Shlomchik,M.J., Viglianti,G.A., Rifkin,I.R. et al. 2005. RNA-associated autoantigens activate B cells by combined B cell antigen receptor/Toll-like receptor 7 engagement. J.Exp.Med. 202:1171-1177.
47. He,B., Qiao,X., and Cerutti,A. 2004. CpG DNA induces IgG class switch DNA recombination by activating human B cells through an innate pathway that requires TLR9 and cooperates with IL-10. J.Immunol. 173:4479-4491.
48. Dorner,T., Egerer,K., Feist,E., and Burmester,G.R. 2004. Rheumatoid factor revisited. Curr.Opin.Rheumatol. 16:246-253.
49. Lee,D.M., Friend,D.S., Gurish,M.F., Benoist,C., Mathis,D., and Brenner,M.B. 2002. Mast cells: a cellular link between autoantibodies and inflammatory arthritis. Science 297:1689-1692.
50. Bischoff,S.C. 2007. Role of mast cells in allergic and non-allergic immune responses: comparison of human and murine data. Nat.Rev.Immunol. 7:93-104.
51. Maruotti,N., Crivellato,E., Cantatore,F.P., Vacca,A., and Ribatti,D. 2007. Mast cells in rheumatoid arthritis. Clin.Rheumatol. 26:1-4.
52. Kinne,R.W., Stuhlmueller,B., Palombo-Kinne,E., and Burmester,G.R. 2007. The pathogenetic importance of macrophages in rheumatoid arthritis. Arthritis Res.Ther. manuscript in preparation.
53. Chomarat,P., Rissoan,M.C., Pin,J.J., Banchereau,J., and Miossec,P. 1995. Contribution of IL-1, CD14, and CD13 in the increased IL-6 production induced by in vitro monocyte-synoviocyte interactions. J.Immunol. 155:3645-3652.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
48
54. Szekanecz,Z. and Koch,A.E. 2007. Macrophages and their products in rheumatoid arthritis. Curr.Opin.Rheumatol. 19:289-295.
55. Cutolo,M. and Lahita,R.G. 2005. Estrogens and arthritis. Rheum.Dis.Clin.North Am. 31:19-27, vii.
56. Padyukov,L., Hytonen,A.M., Smolnikova,M., Hahn-Zoric,M., Nilsson,N., Hanson,L.A., Tarkowski,A., and Klareskog,L. 2004. Polymorphism in promoter region of IL10 gene is associated with rheumatoid arthritis in women. J.Rheumatol. 31:422-425.
57. Eskdale,J., McNicholl,J., Wordsworth,P., Jonas,B., Huizinga,T., Field,M., and Gallagher,G. 1998. Interleukin-10 microsatellite polymorphisms and IL-10 locus alleles in rheumatoid arthritis susceptibility. Lancet 352:1282-1283.
58. Raza,K., Falciani,F., Curnow,S.J., Ross,E.J., Lee,C.Y., Akbar,A.N., Lord,J.M., Gordon,C., Buckley,C.D., and Salmon,M. 2005. Early rheumatoid arthritis is characterized by a distinct and transient synovial fluid cytokine profile of T cell and stromal cell origin. Arthritis Res.Ther. 7:R784-R795.
59. Klimiuk,P.A., Goronzy,J.J., Bjor,n.J., Beckenbaugh,R.D., and Weyand,C.M. 1997. Tissue cytokine patterns distinguish variants of rheumatoid synovitis. Am.J.Pathol. 151:1311-1319.
60. Bresnihan,B., Roux-Lombard,P., Murphy,E., Kane,D., FitzGerald,O., and Dayer,J.M. 2002. Serum interleukin 18 and interleukin 18 binding protein in rheumatoid arthritis. Ann.Rheum.Dis. 61:726-729.
61. Brennan,F. and Beech,J. 2007. Update on cytokines in rheumatoid arthritis. Curr.Opin.Rheumatol. 19:296-301.
62. Karouzakis,E., Neidhart,M., Gay,R.E., and Gay,S. 2006. Molecular and cellular basis of rheumatoid joint destruction. Immunol.Lett. 106:8-13.
63. Sato,K. and Takayanagi,H. 2006. Osteoclasts, rheumatoid arthritis, and osteoimmunology. Curr.Opin.Rheumatol. 18:419-426.
64. Poubelle,P.E., Chakravarti,A., Fernandes,M.J., Doiron,K., and Marceau,A.A. 2007. Differential expression of RANK, RANK-L, and osteoprotegerin by synovial fluid neutrophils from patients with rheumatoid arthritis and by healthy human blood neutrophils. Arthritis Res.Ther. 9:R25.
65. Kvien TK, Uhlig T, Ødegård S, Heiberg MS. Epidemiological Aspects of Rheumatoid Arthritis. The Sex Ratio. Ann N Y Acad Sci 2006:1069:212-22.
66. Uhlig T, Kvien TK. Is rheumatoid arthritis disappearing? Ann Rheum Dis 2005 Jan;64(1):7-10.
67. Symmons DP, Barrett EM, Bankhead CR, Scott DG, Silman AJ. The incidence of rheumatoid
arthritis in the United Kingdom: results from the Norfolk Arthritis Register. Br J Rheumatol 1994;33:735-9.
68. van der Heijde D. How to read radiographs according to the Sharp/van der Heijde method. J
Rheumatol 2000;27:261-3

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
49
69. Ostergaard M, Hansen M, Jensen KE, Szkudlarek M, Pedersen-Zbinden B, Lorenzen I. New radiographic bone erosions in the wrists of patients with rheumatoid arthritis are detectable with magnetic resonance imaging a median of two years earlier. Arthritis Rheum 2003; 48(8):2128-31.
70. Wiles N, Symmons DP, Harrison B, Barrett E, Barrett JH, Scott DG, et al. Estimating the incidence of rheumatoid arthritis: trying to hit a moving target? Arthritis Rheum 1999;42(7):1339-46.
71. Van Dongen H, Van Aken J, Lard LR, Visser K, Ronday HK, Hulsmans HMJ, et al. Efficacy of methotrexate treatment in patients with probable rheumatoid arthritis: A double-blind, randomized, placebo-controlled trial. Arthritis Rheum 2007;56(5):1424-32.
72. Soderlin MK, Borjesson O, Kautianen H, Skogh T, Leirisalo-Repo M. Annual incidence of inflammatory joint diseases in a population based study in southern Sweden. Ann Rheum Dis 2002;61(10):911-5.
73. Savolainen E, Kaipiainen-Seppanen O, Kroger L, Luosujarvi R. Total incidence and distribution of inflammatory joint diseases in a defined population: results from the Kuopio 2000 arthritis survey. J Rheumatol 2003;30(10):911-5.
74. Van Gestel AM., Prevoo ML, Van 'T Hof MA, Van Rijswijk MH, Van de Putte LB, Van Riel PL. Development and validation of the European League Against Rheumatism response criteria for rheumatoid arthritis. Comparison with the preliminary American College of Rheumatology and the World Health Organization/International League Against Rheumatism Criteria. Arthritis Rheum 1996;39:34-40.
75. Smolen JS, Breedveld FC, Schiff MH, Kalden JR, Emery P, Eberl G, et al. A simplified disease activity index for rheumatoid arthritis for use in clinical practice. Rheumatology (Oxford) 2003;42:244-57.
76. Aletaha D, Nell VP, Stamm T, Uffmann M, Pflugbeil S, Machold K, et al. Acute phase reactants add little to composite disease activity indices for rheumatoid arthritis: validation of a clinical activity score. Arthritis Res Ther. 2005;7: R796-R806.
77. Zijlstra TR, Bernelot Moens HJ, Bukhari MA. The rheumatoid arthritis articular damage score: first steps in developing a clinical index of long term damage in RA. Ann Rheum Dis 2002;61(1):20-3.
78. Ødegård S, Landewé R, van der Heijde D; Kvien TK, Mowinckel P, Uhlig T. Association
of Early Radiographic Damage With Impaired Physical Function in Rheumatoid Arthritis. A Ten-Year, Longitudinal Observational Study in 238 Patients. Arthritis Rheum 2006;54:68-75.
79. Syversen SW, Gaarder PI, Goll GL, Ødegård S, Haavardsholm EA, Mowinckel P, et al.
High anti-CCP levels and an algorithm of four variables predict radiographic progression in patients with rheumatoid arthritis: results from a 10-year longitudinal study. Ann Rheum Dis 2007;May 25; [Epub ahead of print]
80. Grigor C, Capell H, Stirling A, McMahon AD, Lock P, Vallance R, et al. Effect of a
treatment strategy of tight control for rheumatoid arthritis (the TICORA study): a single-blind randomised controlled trial. Lancet 2004;364(9430):263-9.
81. Haugeberg G, Uhlig T, Falch JA, Halse JI, Kvien TK. Bone mineral density and frequency of
osteoporosis, in female patients with rheumatoid arthritis. Results from 394 patients in the Oslo County Rheumatoid Arthritis Register. Arthritis Rheum 2000;43:522-30.

Eular On-line Course on Rheumatic Diseases – module n°5 Prof. Tore K Kvien, Dr. Hans Ulrich Scherer and Prof. Gerd-Rüdiger Burmester
50
82. Ørstavik RE, Haugeberg G, Mowinckel P, Hoiseth A, Uhlig T, Falch JA Halse JI, McCloskey E, Kvien TK. Vertebral deformities in rheumatoid arthritis: A comparison with population-based controls. Arch Intern Med 2004;164(4):420-5.
83. Baecklund E, Iliadou A, Askling J, Ekbom A, Backlin C, Granath F, et al. Association of
chronic inflammation, not its treatment, with increased lymphoma risk in rheumatoid arthritis. Arthritis Rheum 2006;54(3):692-701.
84. Maradit-Kremers H, Crowson CS, Nicola PJ, Ballman KV, Roger VL, Jacobsen SJ, et al.
Increased unrecognized coronary heart disease and sudden deaths in rheumatoid arthritis: a population-based cohort study. Arthritis Rheum 2005;52(2):402-11.
85. Chung CP, Avalos I, Raggi P, Stein CM. Arterosclerosis and inflammation: insights from
rheumatoid arthritis. Clin Rheumatol 2007 Feb 2 [Epub ahead of print].
86. Choi HK, Hernan MA, Seeger JD, Robins JM, Wolfe F. Methotrexate and mortality in patients with rheumatoid arthritis: a prospective study. Lancet 2002;359(9313):1173-7.
87. Jacobsson LT, Turesson C, Gulfe A, Kapetanovic MC, Petersson IF, Saxne T, et al.
Treatment with tumor necrosis factor blockers is associated with a lower incidence of first cardiovascular events in patients with rheumatoid arthritis. J Rheumatol 2005;32(7):1213-8.
88. Heiberg T, Kvien TK. Preferences for improved health examined in 1024 patients with
rheumatoid arthritis: Pain has highest priority. Arthritis Rheum 2002;47:391-7
89. Bjornadal L, Baecklund E, Yin L, Granath F, Klareskog L, Ekbom A. Decreasing mortality in patients with rheumatoid arthritis: results from a large population based cohort in Sweden, 1964-95. J Rheumatol 2002;29(5):906-12.
90. Da Silva E, Doran MF, Crowson CS, O'Fallon WM, Matteson EL. Declining use of orthopedic
surgery in patients with rheumatoid arthritis? Results of a long-term, population-based assessment. Arthritis Rheum 2003;49(2):216-20.
91. Heiberg T, Kvien TK, Uhlig T, Finset A. Seven year changes in health status and priorities for
improvement of health in patients with rheumatoid arthritis. Ann Rheum Dis 2005 Feb;64(2):191-5.