Embed Size (px)
Citation preview

Molecular Cytogenetics in Solid Tumors: LaboratorialTool for Diagnosis, Prognosis, and Therapy
MARILEILA VARELLA-GARCIA
Department of Medicine, Medical Oncology Division, University of Colorado Cancer Center, University ofColorado Health Sciences Center, Denver, Colorado, USA
Key Words. Cytogenetics · Fluorescence in situ hybridization (FISH) · Interphase FISH · Biomarker · Target therapy
ABSTRACT
The remarkable progress in the understanding ofleukemogenesis was soundly sustained by methodologicaldevelopments in the cytogenetic field. Nonrandom chro-mosomal abnormalities frequently associated with spe-cific types of hematological disease play a major role intheir diagnosis and have been demonstrated as indepen-dent prognostic indicators. Molecular pathways alteredby chimeric or deregulated proteins as a consequence ofchromosomal abnormalities have also significantly con-tributed to the development of targeted therapies, andcytogenetic assays are valuable for selecting patients for treatment and monitoring outcome. In solid tumors,significantly high levels of chromosome abnormalitieshave been detected, but distinction between critical and
irrelevant events has been a major challenge.Consequently, the application of cytogenetic technologyas diagnostic, prognostic, or therapeutic tools for thesemalignancies remains largely underappreciated. Theemergence of molecular-based techniques such as fluo-rescence in situ hybridization was particularly usefulfor solid malignancies, and the spectrum of their appli-cation is rapidly expanding to improve efficiency andsensitivity in cancer prevention, diagnosis, prognosis,and therapy selection, alone or in combination withother diagnostic methods. This overview illustrates cur-rent uses and outlines potential applications for molec-ular cytogenetics in clinical oncology. The Oncologist2003;8:45-58
The Oncologist 2003;8:45-58 www.TheOncologist.com
Correspondence: Marileila Varella-Garcia, Ph.D., University of Colorado Health Sciences Center, Campus Box B188,4200 East 9th Avenue, Denver, Colorado 80262, USA. Telephone: 303-315-3593; Fax: 303-315-3304; e-mail:[email protected] Received September 9, 2002; accepted for publication November 4, 2002. ©AlphaMed Press1083-7159/2003/$5.00/0
TheOncologist®
LEARNING OBJECTIVES
After completing this course, the reader will be able to:
1. Explain the basic principles supporting the FISH technology and list examples of methodology variants suitable foranalysis in metaphase and interphase cells.
2. Describe at least one advantageous and one limiting factor for the expansion of the applicability of FISH assays tosolid tumors.
3. Explain technical strategies for detection of chromosomal translocation in nondividing cells.
4. Illustrate applications of cytogenetic markers to solid malignancies for diagnosis, prognosis, selection of therapy, andmonitoring disease recurrence or response to treatment.
Access and take the CME test online and receive one hour of AMA PRA category 1 credit at CME.TheOncologist.comCMECME
by guest on April 13, 2018
http://theoncologist.alphamedpress.org/
Dow
nloaded from

INTRODUCTION
Early descriptions of mitotic and spindle aberrations inhuman tumors date from approximately a century ago;however, for many decades, the progress in cancer cyto-genetics was hampered by technical challenges in assessingthe nuclear chromosomal content. In the late 1950s and the1960s, significant methodological achievements regardingculture and mitotic arresting of cells made the detection ofchromosomal abnormalities possible, although without anaccurate identification of the occurring changes. The typi-cal example is the description in patients with chronicmyeloid leukemia, of the Philadelphia (Ph) chromosome,which initially was depicted as a deleted chromosome 21 or22 [1]. The flourish of chromosomal banding techniques(Q-, G-, R-banding) in the early 1970s has contributed tothe establishment of karyotype-phenotype correlations for arapidly increasing number of diseases. Characteristic recur-rent translocations were rapidly identified in hematopoieticand soft tissue neoplasias and have helped in the identifica-tion of chromosomal loci containing genes involved in thegenesis of these tumors [2]. Conversely, the impact of cyto-genetic technology on understanding molecular mecha-nisms involved in the initiation and progression of solidtumors has been less valuable. Solid tumors are commonly
associated with an array of orchestrated genetic changes,and the identification of changes causally related to the car-cinogenic process has been frustratingly slow, mainly as aconsequence of the enormous volume of secondary abnor-malities reflecting the phenomenon of genomic instability.
FLUORESCENCE IN SITU HYBRIDIZATION (FISH)AND INTERPHASE ANALYSIS
Classical cytogenetics represented by chromosomalbanding techniques was successful in correlating karyotypeabnormalities with diagnosis, prognosis, and response totherapy in hematological neoplasias. However, these tech-niques require a high rate of cell division and good chromo-somal morphology, which represent challenges for thecytogeneticists, and a long period for assaying and analyzing,which usually is a challenge for physicians (Table 1). Thus,it was not surprising that an outburst of progress in the can-cer cytogenetics field followed the advent of molecularcytogenetics, with the development and optimization ofFISH technology [3]. FISH technology initially focused onresearch issues, but soon was applied to clinical questionsand has proved sufficiently sensitive and reliable to fill inthe gap between classic karyotyping and highly sensitivemolecular techniques.
46 Molecular Cytogenetics in Clinical Oncology
Table 1. Cytogenetic techniques most commonly used, and advantages and limitations of their applications to human solid malignancies
Techniques Characteristics Applications Advantages Limitations
G-banding, R-banding Protein digestion and/or special dye Identification of numerical Genome-wise screening for Low resolution, dependent on generate banding pattern specific for and structural chromosomal chromosome-level abnormalities; chromosome condensation;each chromosome anomalies Low cost for reagents and Requires mitotic cells and well-
instrumentation; spread chromosomes;Simple and robust procedures Labor-intensive analysis;
Low efficacy in highly rearranged karyotypes
FISH A small, labeled DNA fragment is used Identification of the presence, Applicable to interphase cells; Conclusions limited to the tested as a probe to search for homologous number of copies per cell, Fast analysis and scoring; targets; target sequences in chromosome or and localization of probe Simple and robust procedures Scarceness of specific and reliable chromatin DNA DNA reagents
CGH Competitive hybridization of differentially Detection of variant DNA Applicable to fresh or preserved Dedicated instrument required forlabeled total genomic tumor DNA and copy numbers at the specimens; analysis;normal reference DNA to normal human chromosome level No need for cell culture; Low resolution, dependent on metaphases used as templates Genome-wise screening for chromosome condensation of
genomic imbalances normal template;Balanced rearrangements and imbalances present in low frequencies remain undetected
Multicolor karyotyping Hybridization with 24 differentially Detection of rearrangements Accurate origin identification of Requires mitotic cells and well-(M-FISH, SKY) labeled, chromosome-specific probes involving one or more all segments in complex spread chromosomes;
allows the painting of every human chromosomes within rearrangements; Limited accuracy in determination chromosome in a distinct color individual metaphase Clarification of marker of breakpoints;
spreads chromosomes Intrachromosomal changes remain undetected;Dedicated instrument required for analysis
by guest on April 13, 2018
http://theoncologist.alphamedpress.org/
Dow
nloaded from

The basis for the molecular cytogenetics technology isthe complementary double-stranded nature of DNA. A spe-cific DNA segment is converted into a probe through theattachment of a fluorescent tag or a reporter molecule thatlater in the procedure will be conjugated with a fluorescenttag. The probe is denatured, exposed to a similarly dena-tured target DNA, and, under proper hybridization condi-tions, recognizes and binds to the homologous sequences inthe target DNA. After hybridization, the copy number andlocation of the fluorescent tags, and consequently, of thetarget homologous regions, are recognized under fluores-cence microscopy both in chromosome spreads and in inter-phase nuclei (Fig. 1). FISH technology is simple and robust,and its phenomenal contribution to the cancer field largelyrelies on its applicability to interphase cells (Table 1).
While early FISH applications aimed at the detection ofnumerical abnormalities in mitotic or interphase cells, as wellas structural abnormalities in metaphase spreads, a milestonewas achieved in 1990 when Rowley et al. [4] and Tkachucket al. [5] developed strategies for identification of chromoso-mal translocations in interphase cells. Since then, variationsin probe design, and consequently, in the presentation of fluorescent signals in normal cells and in cells carrying chro-mosomal translocations have been developed for molecu-larly cloned rearrangements. In the standard approach forinterphase evaluation of chromosomal translocations [5], aDNA probe, comprising sequences mapped proximally to thebreakpoint in one of the chromosomes involved in the recip-rocal translocation, is combined with a differentially labeledDNA probe that includes sequences mapped distally to the
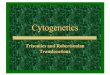
breakpoint in the other chromosome. Positive nuclei for thetranslocation display one dual-color fusion signal, represent-ing one of the derivative chromosomes generated by thetranslocation, and two single-color signals, one for each ofthe normal alleles (Fig. 2A). This standard FISH strategy haslargely been used for the diagnosis of leukemia and lym-phoma translocations at disease presentation or at clinicalrelapse, since patients at these stages usually show high fre-quencies of bone marrow cells with the chimeric gene.Nonetheless, for detection of residual disease, this approachlacks specificity, because cells with random spatial colocal-ization of normal signals with different colors, usually foundin frequencies ranging from 1%-5% of scored nuclei, areseen as false positives.
To minimize this problem, a dual-fusion FISH (D-FISH)approach was developed, with the probe set including DNAsequences that encompass proximally and distally thetranslocation breakpoints on both chromosomes involved inthe translocation.
As illustrated for the t(8;21)(q22;q22) in Figure 2B,sequences for each chromosome are labeled with a specificcolor, and the translocation generates fused signals in bothderivative chromosomes [6]. Using the D-FISH approach,nuclei carrying the reciprocal translocation show two copies ofthe fused signals and one copy of each of the single signalsrepresenting the normal alleles. It is doubtful that such a posi-tive pattern would be mimicked by artificial conditions; there-fore, the D-FISH approach shows a higher sensitivity thatfavors its application in patients in clinical remission who areexpected to present low frequencies of abnormal cells [7].
Varella-Garcia 47
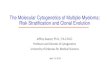
Figure 1. FISH technology uses alabeled DNA segment as a probe tosearch homologous sequences in inter-phase chromatin and metaphase chro-mosomes. On the right, nuclei ofejaculate suspension from a patient withprostate carcinoma were hybridizedwith centromeric probes for chromo-some 7 (labeled with SpectrumRed™ flu-orophore) and chromosome 8 (labeledwith SpectrumGreen™). Spermatozoidnuclei (small) show the expected singlecopy of each target because of theirhaploid chromosomal complement. Aprostate-derived nucleus (large) showsa gain in copy number for both targets,characterizing the cell as abnormal.On the left, a metaphase spread (par-tially illustrated) was hybridized withlocus-specific FISH probes for theHOXA (labeled with Spectrum-Green™) and HOX11L2 (labeled withSpectrumRed™) genes, which wererespectively mapped at 7p15 and5q34.
by guest on April 13, 2018
http://theoncologist.alphamedpress.org/
Dow
nloaded from

These two described FISHapproaches are adequate for analy-sis of recurrent reciprocal translo-cations, which comprise themajority of hematopoietic and softtissue-specific rearrangements, butare very rare in solid tumors.Presently, the sole example of sin-gle reciprocal translocation associ-ated with aggressive carcinomas isthe t(15;19), with breakpoints in19p13.1 and variant breakpoints in15q11-q15 [8, 9]; the molecularevents triggered by these rear-rangements have yet to be charac-terized. Conversely, solid tumorsusually present large numbers ofderivative chromosomes fromtranslocations involving two ormore chromosomes [10], suggest-ing that some critical cancer genesare promiscuous in the selection oftranslocation partners. Promiscuityin translocation partnership is wellknown for leukemia genes such asmixed-lineage leukemia and E2A[11], and a third FISH strategy wasdeveloped to address this particularcondition, namely, “break-apart”FISH. The break-apart probe com-prises DNA sequences mappedproximally and distally to the break-point within a critical gene labeledwith distinct fluorochromes [12].In this case, the fused fluorescentsignals represent a normal gene,whereas nuclei with disruptionswithin the target gene due totranslocations show one fusion sig-nal for the normal allele and two
48 Molecular Cytogenetics in Clinical Oncology
Figure 2. Detection of chromosomaltranslocations in interphase cells. A)Conventional FISH probe format wasproposed by Tkachuck et al. [5] and isillustrated for the t(9;22)(q34;q11),associated with chronic myeloidleukemia. B) Dual-fusion format isillustrated for the t(8;21)(q22;q22),characteristic of the AML-FAB M2[6]. C) Break-apart format for cancergenes with promiscuous partners isillustrated for the gene E2A [12].
by guest on April 13, 2018
http://theoncologist.alphamedpress.org/
Dow
nloaded from

Varella-Garcia 49
single-color signals, one for each of the derivative chromo-somes, regardless of which chromosome is the partner in thetranslocation (Fig. 2C).
FISH VARIANTS: COMPARATIVE GENOMIC
HYBRIDIZATION AND MULTICOLOR KARYOTYPING
Two major variants of FISH technology, comparativegenomic hybridization (CGH) and multicolor karyotyping,have been extensively applied to solid tumors; their advan-tages and shortcomings are summarized in Table 1. CGH wasdeveloped by Kallioniemi et al. [13] and allows the visualiza-tion of gains and losses in the copy numbers of DNAsequences from specific chromosomal regions withoutinvolving cell culture, as illustrated in Figure 3A. Thegenomic DNA from the tumor specimen is isolated, frag-mented, and labeled with a given fluorophore, for instance,the green fluorophore fluorescein isothiocyanate (FITC). Asample of normal genomic DNA, taken as a reference, is sim-ilarly isolated and fragmented but is differentially labeled, forinstance, with the red fluorophore Texas Red. Subsequently,equal amounts of tumor and reference DNA are coprecipi-tated with an excess of repeat-rich DNA (Cot-1 DNA) for theblocking of the repetitive sequences, and this DNA mixture isallowed to hybridize to normal metaphase spreads. Sequencesof DNA from each specific chromosomal region recognizetheir homologous regions in the normal template metaphasesand hybridize to them according to the proportion in whichthey are represented in the DNA mixture. Comparative analy-sis of the proportion of each distinctly labeled tumor and ref-erence DNA that was incorporated into the templatemetaphase provides a ratio of tumor to normal signal againsta baseline of the metaphase chromosomes. Therefore, the nor-mal number of chromosome regions with copies in both thetumor and reference DNA of a chromosomal region will dis-play a balanced profile of Texas Red and FITC fluorophores,whereas regions deleted in the tumor will show a higher pro-file of Texas Red, and regions with gains in copy number inthe tumors will show a higher profile of FITC. Figure 3Billustrates the typical pattern for presentation of results gener-ated by CGH analysis. In the prostate carcinoma illustrated inFigure 3B, for instance, gene amplifications were found forthe oncogene MYC (at 8q24) and the vitamin D receptor gene(at 12q12-q14), which mediates growth inhibitory effects ofvitamin D in prostate cancer. The CGH technique has beenextensively used for solid tumor analysis since its inception,and a nonrandom pattern of genomic imbalances has emergedfrom these studies [14]. To this point, CGH has been the mosthelpful cytogenetics tool for identification of oncogenes andtumor suppressor genes involved in the initiation and pro-gression of solid tumors, guiding the more detailed geneticanalysis to specific chromosomal regions.
Two major multicolor karyotyping techniques are spec-tral karyotyping (SKY) and multiplex-FISH (M-FISH). Thesetechniques are similarly based on combinatorial probe-label-ing schemes with five spectrally discrete fluorochromes thatuniquely paint all 24 human chromosomes (Fig. 4) but differin their analytical procedures. SKY relies on a single digitalimage acquired with a charge-coupled device (CCD) in con-junction with a customized multiband optical filter, and onFourier spectroscopy [15]. An interferometer is used to accessthe spectrum of fluorescence wavelengths for each pixel ofthe image. A dedicated computer program identifies the com-ponents of the spectrum, applying a classification algorithm,and generates a composite image in which each chromosomeis pseudocolored based on its fluorochrome signature. Sinceeach chromosome is represented by one specific color,rearrangements involving different chromosomes are easilyrecognized (Fig. 5). On the other hand, the M-FISH techniquecombines monochrome CCD images acquired separately foreach of the five spectrally distinguishable fluorochromes (Fig.6) and has them subsequently analyzed by a dedicated soft-ware program that also builds a composite image by assign-ing a particular pseudocolor to each chromosome [16]. Thus,both multicolor karyotyping techniques are specially tailoredto identify and characterize the complex chromosomalrearrangements found in solid tumor cells. Nevertheless, thesemethodological approaches are unable to detect intrachromo-some rearrangements, such as inversions and deletions, sincethese specific abnormalities maintain the correct color forabnormal chromosomes. Consequently, multicolor karyotyp-ing cannot replace standard banding karyotyping; rather, bothtechniques should be used in conjunction for a comprehensiveevaluation of solid tumors.
Application of multicolor karyotyping technology to solidtumors faces most of the constraints of classic cytogeneticsregarding the need for dividing cells and long chromosomeswith good morphology in well-spread metaphases. These fea-tures are very difficult to achieve simultaneously in primarytumors, and both the SKY and M-FISH techniques have beenmore commonly applied to cell lines established from primarytumors. The immortal lines offer more suitable material forkaryotype analyses, and identification of chromosomalregions/genes involved in rearrangements provides interestingclues in the mechanisms of tumorigenesis [17].
CURRENT PROGRESS ON SOLID TUMORS: SLOWLY
BUT SURELY
The interphase FISH technology opened a new windowof research opportunities in solid tumors, largely due to theavailability of formalin-fixed, paraffin-embedded tumorblocks that could be used both for prospective and retro-spective studies. The ability to keep the tissue architecture
by guest on April 13, 2018
http://theoncologist.alphamedpress.org/
Dow
nloaded from

50 Molecular Cytogenetics in Clinical Oncology
Figure 3. Searching for genomic imbalances using CGH. A) Schematic representation of the procedure. B) Multiple imbalancedgenomic regions detected in the prostate adenocarcinoma cell line ALVA-31. Each human chromosome is represented by its ideogram onthe left and a graphic on the right. In the graphic, the black line represents the balanced hybridization, the red line on the left represents thethreshold for loss, and the green line on the right represents the threshold for gain. The blue line shows the CGH profile, i.e., the ratio oftumor/reference DNA along the chromosome. Chromosomal regions that are deleted or gained above the threshold are highlighted by, respec-tively, red and green bars at the sides of the chromosome ideograms. Gains in copy numbers were found for specific regions in chromosomes1, 3, 8, 10, 12, and 19 (green bars at right). Losses were found for regions in chromosomes 8, 10, 13, 17, 18, and 19 (red bars at left).Since DNA from a female donor was used as reference DNA, loss for chromosome X and gain for chromosome Y were not considered.
by guest on April 13, 2018
http://theoncologist.alphamedpress.org/
Dow
nloaded from

and, consequently, to reveal cell-to-cell heterogeneity anddetect small clones of genetically distinct cells is veryappealing and may be essential in achieving breakthroughsin current cancer therapy, as stressed by Kobayashi et al.[18]. Those authors established four sublines from a pri-mary pulmonary adenocarcinoma characterized by a poorprognosis. These sublines differed in morphological, bio-chemical, and genetic findings, and one of them exhibited a
12-fold amplification of the c-MYC oncogene and an increasedsensitivity to cytosine arabinoside.
However, a serious caveat forthe broader application of FISHtechnology as a diagnostic tool forsolid tumors is the scarceness of spe-cific abnormalities associated withthem. Recent progress in the DNA-labeling strategies using new fluo-rophores has partially circumventedthis lack of specific targets, allow-ing the design of multicolor FISHprobes that simultaneously target atleast four different chromosomalregions in a single cell. The multi-color strategy is particularly usefulfor analysis of solid malignanciescharacterized by polyploidy orpolysomy for multiple chromo-somes, as addressed later in thisreview. In addition, among the lat-est publications, there is an emerg-ing variability in applications ofFISH as an adjunct diagnostic tool,which attests to the encouragingprogress recently achieved. Exam-ples are described below and summarized in Table 2.
Varella-Garcia 51
SKY (Spectral karyotyping) Schorck et al. [15]
M-FISH (Multiplex FISH) Speicher et al. [16]
Principle:• Combinatorial labeling scheme with 5 fluorochromes to• distinctly paint the 24 human chromosomes• Counterstaining with DAPI
Abs/Em
Abs/Em
M-FISH
SKY
nm700600500400
DAPI
SA SG
FITC
SGo SR
Rh TxR Cy5 Cy5.5
FR
367/452
433/480 497/524
495/525
530/555 592/612
550/570 596/620 650/670
655/675
675/694
Figure 4. Probe-labeling scheme used in each technique and fordiamidinophenylindolc (DAPI), used as counterstain. Fluorophoreslargely used for M-FISH are SpectrumAqua™ (SA), SpectrumGreen™
(SG), SpectrumGold™ (SGo), SpectrumRed™ (SR), and Spectrum-FarRed™ (FR). SKY uses the fluorophores fluorescein isothiocyanate(FITC), Rhodamine (Rh), Texas Red (TxR), Cy5, and Cy5.5
Figure 5. Spectral karyotype of a cellrepresentative of the small cell lungcarcinoma cell line UMC19. The toppanel shows the classified image, andthe bottom panel shows the invertedDAPI image. Chromosome derivativesfrom complex rearrangements involv-ing two to five chromosomes are shown.
by guest on April 13, 2018
http://theoncologist.alphamedpress.org/
Dow
nloaded from

Diagnosis and Follow-UpAn interesting illustration is the differential diagnosis
between teratoid/rhabdoid (AT/RT) and medulloblas-tomas/central primitive neuroectodermal (MB/PNET)tumors through the deletion of chromosome 22q11.2sequences. AT/RT is a rare intracranial neoplasm typicallyunresponsive to therapy and rapidly fatal, and approxi-mately 90% of patients present with a 22q deletion [19].Bruch et al. [20] have shown the diagnostic use of a
22q11.2 FISH probe in specimens with equivocal primitivecentral nervous system neoplasms. “Difficult to classify”tumors were assigned to AT/RT (when 22q deletion waspresent) or MB/PNET groups (when 22q deletion was notpresent), and after diagnosis reclassification, the study con-cluded that misdiagnosed cases of AT/RT had probablyaccounted for the worse prognosis associated withMB/PNET in younger infants.
An attempt has been made to use FISH to monitor sur-gical margins. The combination of multiple DNA probessuccessfully identified chromosome imbalances associatedwith malignancy in head and neck squamous cell carcino-mas that were also present in clinically normal adjacentcells, thereby detecting subclinical tumorigenesis [21]. Insome patients, aneusomy in surgical margins was found inspecimens for which the pathological evaluation was nega-tive; these patients relapsed and died within the 3-year fol-low-up [22]. Although a question remained regarding thepracticability of FISH as an intraoperative tool because, cur-rently, results cannot be provided within an intraoperativetime frame, the FISH results from these head and neck car-cinomas strongly reinforced the need for adjunct therapyfor patients with molecularly abnormal margins.
Additional examples are emerging regarding theapplicability of FISH assays to accurately monitor tumorresponse to therapy and to offer the clinician extra argu-ments for changing ineffective therapy at an earlier stage inthe course of treatment. The cytologic examination of cere-brospinal fluid (CSF) is the primary method for evaluationof response to therapy for metastatic spread to the lep-tomeninges; a diffuse and often multifocal infiltration of theleptomeninges is estimated to occur in up to 8% of patients
52 Molecular Cytogenetics in Clinical Oncology
Figure 6. Images captured for the M-FISH karyotyping analysis: DAPI (count-erstain) alone and combined with SpectrumAqua™, SpectrumGreen™,SpectrumGold™, SpectrumRed™, and SpectrumFarRed™. Distinct chromosomesfluoresce in distinct colors due to the combinatorial probe-labeling scheme.
Table 2. Strategies used for application of FISH technology to clinical oncology
Application Strategy Reference
Differential diagnosis of teratoid/rhabdoid (AT/RT) and Detection of 22q11.2 deletion as a Bruch et al. [20]medulloblastomas/central primitive ectodermal (MB/PNET) tumors marker for AT/RT
Monitoring of surgical margins in head and neck carcinomas Detection of chromosomal aneusomy Barrera et al. [21, 22]in adjacent margins
Monitoring response to therapy in metastatic cancer Detection of chromosomal aneusomy Van Oostenbrugge et al. [24]in cerebrospinal fluid
Selection of breast cancer patients for target therapy with Detection of HER-2 gene amplification Pauletti et al. [33] trastuzumab in tumor cells Kakar et al. [34]
Bartlett et al. [35]Tubbs et al. [36]
Early detection of bladder cancer recurrence Detection of aneusomic cells in Halling et al. [45]voided urine
Identification of patients at risk for carcinoma relapse Detection of aneusomic epithelial cells Engel et al. [49]in peripheral blood
Assessment of thyroid cancer risk in therapeutic exposure to Detection of TP53 loss as a marker for Ramirez et al. [51]radioactive iodine lack of cellular response to DNA damage
by guest on April 13, 2018
http://theoncologist.alphamedpress.org/
Dow
nloaded from

with systemic cancer [23]. However, this cytodiagnosis losesmuch of its sensitivity through the course of protracted ther-apy because CSF undergoes a decrease in cellularity,changes in cell morphology, and presentation of reactiveependymal cells. Van Oostenbrugge et al. [24] tested lep-tomeningeal metastases from three cases of non-Hodgkin’slymphoma, three cases of breast cancer, and one malignancywith unknown primary site using a single FISH probe (chro-mosome 1 centromere), and found a better correlationbetween FISH and treatment response than routine cytodiag-nosis. This study was performed retrospectively; however,the authors conceded that had the FISH results been takeninto account, the treatment would have changed for four ofthe seven patients with normal or suspicious cytology in theventricular CSF but aneusomic cells detected by FISH.Interestingly, in that study, the chromosome 1 probe wasselected as a nonspecific indicator of chromosome aneusomyrather than a specific marker for the patients’ diseases.
Markers for Prognosis and Targets to TherapyExamples of biomarkers that reliably predict responses
to chemotherapy for solid tumors are rare but nonethelessrapidly increasing, and FISH technology has expanded theavailability of molecular targets to be evaluated. The dual-color FISH assay for evaluation of HER-2 (erbB2) geneamplification in breast cancer is probably the utmost investigated FISH test that has proven to be effective as aprognostic marker and predictor for response to therapy insolid malignancies. Overexpression of HER-2 has beenfound in 20%-30% of breast cancers and has been associatedwith a poor overall survival [25, 26] and response to therapy[27, 28]. Trastuzumab, a humanized monoclonal antibodythat recognizes the HER-2 protein, produced objectiveresponses, alone or in combination with chemotherapy, inbreast cancer patients previously untreated and in the second-line setting [29-32]. Although it might be predicted that pro-tein expression would be more effective for assessingresponse to trastuzumab therapy, because the antibody binds
to the cell surface protein, results from a FISH assay usingHER-2 and chromosome 17 centromere sequences showedthat the presence of gene amplification (Fig. 7) correlatedbetter with survival, was more accurate and reliable forselecting patients eligible for treatment with trastuzumab,and was superior for predicting response to therapy [33-36].
The success of targeting HER-2 for therapy in breastcancer has yet to be validated in other epithelial tumors. Inlung and prostate carcinomas, it is clear that only a minorityof patients overexpress HER-2 due to gene amplification[37, 38]. Intriguingly, the expression patterns of HER-2 aredifferent in breast and lung carcinomas (Fig. 8), and mostlung tumors display gains in copy number of HER-2 geneper cell due to chromosomal aneusomy rather than geneamplification. Initial reports show that prostate adenocarci-noma patients without HER-2 amplification have notresponded to trastuzumab [39], while experiments in lungcancer cell lines indicate that trastuzumab was effective inreducing cell growth when multiple copies of the gene werepresent, even as a consequence of aneusomy [40]. Therefore,studies to determine the effectiveness of trastuzumab in rela-tion to the molecular profiling of patients regarding HER-2status are urged.
Another member of the HER family of receptors, the epi-dermal growth factor receptor (EGFR), has been postulated asa potential marker for prognosis and a target for therapy insolid malignancies. Recent studies have shown promisingresults with tyrosine kinase inhibitors of EGFR (ZD1839and OSI-774) in patients with esophageal [41] and lungcarcinomas. In non-small-cell lung carcinomas, ZD1839(Iressa®; AstraZeneca; London, UK) produced objectiveresponses in about 15%-20% of patients with advanceddisease who had failed one or two chemotherapy regi-mens (at least one platinum based) and in 10% of patientswho had failed two or more prior chemotherapy regimenscontaining platinum and docetaxel, with a favorableadverse event profile [42, 43]. These findings raised considerable excitement regarding the potential role of
Varella-Garcia 53
Figure 7. Dual-color FISH assay inbreast adenocarcinomas with sequen-ces for the HER-2 gene labeled in red(SpectrumOrange™) and the chromo-some 17 centromere labeled inSpectrumGreen™. A) Ideogram ofchromosome 17 with the location ofeach probe. B) Metaphase spread of cellline SKBr3 showing multiple chromo-somes with multiple copies of theHER-2 gene. C) Interphase nuclei of aprimary tumor with HER-2 geneamplification identified by clusters offluorescent red spots.
by guest on April 13, 2018
http://theoncologist.alphamedpress.org/
Dow
nloaded from

such therapies for lung cancerpatients with less advanced dis-ease and their potential toimprove survival. Nevertheless, there is little informationon how patients who might benefit from therapy withEGFR inhibitors should be selected. An interesting find-ing from the University of Colorado (Hirsch et al. sub-mitted for publication) was the positive correlationbetween the level EGFR protein expression and copynumber of the gene per cell, suggesting that an additiveeffect of gene copies is an important mechanism forEGFR protein expression in lung cancer cells.
Other key regulator genes for cell growth, proliferation,and differentiation processes, such as the MYC (8q24),MYCN (2p24.1), and CCND1 (cyclin D1, 11q13), havebeen less evaluated clinically in solid tumors. However,when these genes are erroneously expressed due to geneticrearrangements, such as translocation or gene amplifica-tion, neoplastic transformation is activated, and their mole-cular pathways are potential therapy targets. FISH probesare commercially available for these genes, and in thefuture, may be utilized similarly to the HER-2 probe.
Diagnosis of Recurrent DiseaseDetection of residual disease in patients with solid
malignancies is an essential goal in clinical oncology, andFISH technology has already been introduced as a tool inthis area. One of the promising applications of interphaseFISH is the detection of tumor cells in body fluids throughnoninvasive procedures, as illustrated by the detection oftumor cells in urine of patients with urothelial carcinomas.Urinary cytology has been the reference test for the evalua-tion of symptomatic patients, for the detection of lesions inhigh-risk patients, and for the follow-up of patients with aprior history of transitional cell carcinoma (TCC).
Although routine cytology has a relatively high level ofspecificity for the detection of high-grade in situ and inva-sive lesions, the sensitivity for patients with low-grade TCCis low, because these tumors may exfoliate cells that arecytologically indistinguishable from normal. Urine cytol-ogy is further limited by poor specificity for clinically sig-nificant lesions in cases that are classified as atypical on thebasis of cells with equivocal cytologic features. The cyto-logic diagnosis of atypia may result from degenerativechanges related to prior therapy or reactive changes that areof limited clinical significance. Therefore, the clinical out-comes for individual cases cannot be accurately determinedby cytologic examination alone. As a result, many patientsundergo unnecessary procedures to rule out malignancybased on limited specificity for clinically significantlesions. The U.S. Food and Drug Administration (FDA)recently approved the UroVysion™ Bladder RecurrenceCancer Test (Vysis; Downers Grove, IL) for the detectionof TCC in urine cells. The UroVysion™ test was designedfor interphase cell quantification of chromosomes 3, 7, 17,and 9p21 region (p16/CDKN2A gene), which were recog-nized as frequently involved in numerical anomalies inbladder cancer [44]. In a series of 265 patients, Halling etal. [45] demonstrated a significantly greater overall sensi-tivity of FISH over cytology for the detection of pTis, pT1-pT4, and grade 3 urothelial carcinoma. Validation of theUroVysion™ FISH assay as a screening tool for selection ofpatients with a history of bladder cancer who should be sub-mitted to cystoscopy has been performed in numerous insti-tutions, including the University of Colorado. Althoughfalse-negative FISH results can be expected in low-gradeTCC due to frequent diploid chromosomal content, in our
54 Molecular Cytogenetics in Clinical Oncology
Figure 8. Evaluation of HER-2 pro-tein staining by immunohistochem-istry and gene status by FISH inlung tumors [38]. Normal epithe-lium showing apical staining (A),well-differentiated tumor showingbasolateral staining (B), moderatelydifferentiated tumor scored as 2+
(C), and poorly differentiated tumorscored as 3+ (D). FISH assays showedthree major patterns: balanced dis-omy for HER-2 gene and chromosome17 (E), balanced gain for HER-2 geneand chromosome 17 (F), and HER-2gene amplification with a gene/chromosome ratio >2 (G).
by guest on April 13, 2018
http://theoncologist.alphamedpress.org/
Dow
nloaded from

small series of 19 patients, urinespecimens from two patients withG1 tumors and one patient with aG2 tumor were classified as nega-tive by cytology but abnormal byFISH. Figure 9 illustrates an abnormal cell found in the G2TCC patient confirmed by cystoscopy in our series, show-ing multiple copies of each of the four DNA targetsincluded in the UroVysion™ probe set. Interestingly, theUroVysion™ test also was proven to be effective in detect-ing tumor recurrence before evidence of urothelial carci-noma was found on biopsy, likely due to the ability ofvoided urine to present the entire urothelium versus theregional evaluation of the biopsy [45]. A follow-up biopsyrevealed recurrent urothelial carcinoma in 7 out of 11patients identified by Halling at al. [45] as abnormal byFISH but with a negative initial biopsy. Therefore, patientswith positive FISH but negative biopsy should be carefullyfollowed, as they are at risk of harboring occult disease.
Other recently developed multicolor FISH probes weredemonstrated to be potentially useful laboratory tools in theeffort to reduce mortality from solid tumors, due to theirgreater ability to diagnosis early changes, and therefore,prevent disease progression. Examples include the analysisof cells collected through minimally invasive approaches,such as epithelial cells obtained in fine needle aspiratesfrom ductal carcinoma of the breast [46] and in bronchialbiopsies from smokers at risk for lung carcinoma [47]. Themulticolor probe used in the bronchial biopsies study,LAVysion™ (Vysis), addresses four chromosomal regionsor genes commonly involved in gains in lung carcinomas:5p15, 6 centromere, 7p12 (EGFR), and 8q24 (MYC), asillustrated in Figure 10. Normal bronchial cells are shownwith two copies of each of these DNA targets, and a nucleus
from a squamous cell carcinoma is shown with multiplecopies of each target.
The development of innovative technologies for unbiased recovery and enrichment of tumor cells from
Varella-Garcia 55
Figure 9. A highly aneusomic cellfound in voided urine using theUroVysion™ bladder cancer. The toppanel segmented images for each of thethree chromosome enumeration probes(CEP) including centromeric sequencesfor chromosomes 3 (CEP 3 labeled inSpectrumRed™), 7 (CEP 7 labeled inSpectrumGreen™), and 17 (CEP 17 inlabeled SpectrumAqua™) and the locus-specific indicator (LSI) probe for p16(9p21 labeled in SpectrumGold). Thebottom panel shows nuclei stained withDAPI and the multicolor image. Thelarge nucleus at the top left in eachimage of the top panel shows, respec-tively, 6, 11, 10, and 6 copies of the DNAtargets.
Figure 10. Multitarget probe set (LAVysion™; Vysis) for detection of aneusomyin lung tumors. A) Four chromosomal targets are addressed: 5p15 (labeled inSpectrumGreen™), chromosome 6 centromere (in SpectrumAqua™), EGFRsequences at 7p12 (in SpectrumRed™), and MYC sequences at 8q24 (inSpectrumGold™). B) Normal bronchial epithelial nuclei showing two copies ofeach probe. C) Highly aneusomic nucleus from a squamous cell lung carcinomashowing additional copies for all four DNA targets.
by guest on April 13, 2018
http://theoncologist.alphamedpress.org/
Dow
nloaded from

peripheral blood or bone marrow aspirates using magnetic-activated cell-sorting systems [48], coupled with accuratetests to characterize these cells, is expected to better moni-tor the response to cytotoxic or hormonal therapy and toidentify patients at risk for relapse. FISH has been proposedas an essential test to be combined with immunophenotyp-ing for evaluation of potential tumor cells selected fromblood or bone marrow. Engel et al. [49], in dilution assayswith the breast cancer cell line MCF7 and normal periph-eral lymphocytes, demonstrated the higher sensitivity ofFISH tests using centromeric probes compared with flowcytometry sorting using anticytokeratin and anti-CD45antibodies. In addition, these authors successfully identifiedcirculating tumor cells in the peripheral blood of 30 out of43 patients with breast or ovarian cancer using one locus-specific (17q11-12) and three centromeric probes (chromo-somes 7, 12, and 17) in combination with anticytokeratinand anti-CD45 antibodies.
Risk AssessmentThere are persisting concerns regarding the carcino-
genic risk to therapeutically irradiated patients, because it iswell known that ionizing radiation is a major aneugenic andclastogenic agent [50]. The application of emerging molec-ular cytogenetic methods to risk assessment may help toclarify the uncertainties of low-risk exposure to cancertreatments, such as radioactive iodine for thyroid disease.Ramirez et al. [51] tested a new FISH probe set, thatincluded the centromere of chromosome 17 and the p53locus (17p13.1), in buccal cells from patients with thyroidcancer before and after radioactive iodine treatment. Therationale for the selection of these probes was that the fail-ure to express a functional nuclear phosphoprotein p53plays a critical role in the cellular response to DNA dam-age, leads to aneuploidy in vitro and in vivo, and increasesthe incidence of spontaneous tumors [52, 53]. Inactivationof p53 is frequently associated with the loss or mutation ofits encoding gene, TP53. In that study, the radiation-induced chromosome breakage resulted in a significantincrease in 17p gains and losses in exposed individuals.Therefore, the 17cen/p53 FISH assay may be a potentialbiomarker for cancer risk in people therapeutically exposedto radiation.
CONCLUSIONS
The identification of specific chromosomal abnormali-ties in leukemias, lymphomas, and soft tissue tumors has pro-vided critical insight into the molecular changes that underliecarcinogenesis. In solid malignancies, the progress was lesssubstantial until the development of molecular cytogenetictechniques such as interphase FISH, CGH, and multicolorkaryotyping. SKY and M-FISH, the two major multicolorkaryotyping techniques, contribute to the identification ofcomplex chromosomal changes associated with solid tumors,and CGH has highlighted critical regions harboring onco-genes and tumor suppressor genes. Interphase FISH technol-ogy has been demonstrated to be specially suitable to bridgebasic research to clinical practice, and its applicability hasincreased substantially in a short time. These new method-ological strategies are rapidly expanding the application ofcytogenetic assays to critical areas in solid malignancies atboth the basic science and clinically applied levels.
Availability of reliable and specific markers for individ-ual diseases or stages is a critical shortcoming in the currentapplication of FISH to solid tumors, and the development ofa substantial number of DNA probes is warranted for a morepowerful use of the technology. In this regard, the massivevolume of molecular information that has been constantlyreleased in both the fields of genome databases and tumorprofiling is expected to minimize the current difficulties.Additionally, automated devices are currently under develop-ment to process and analyze interphase FISH assays, whichare expected to reduce the burden of the labor-intensive aspectof the molecular cytogenetics procedures. As a consequence,molecular cytogenetic technology is shortly expected toextend its contribution to more accurate tumor profiling;improved early detection, diagnosis, and prognosis; selectionof target therapeutic approaches, and monitoring clinical outcome in patients with solid malignancies.
ACKNOWLEDGMENTS
Supported in part by the following National CancerInstitute grants: Cancer Center Core Grant P30-CA46934,Specialized Program of Research Excellence P01-CA58187,and Early Detection Research Network U01-CA85070.Critical comments provided on this review by Dr. FredHirsch were deeply appreciated.
56 Molecular Cytogenetics in Clinical Oncology
REFERENCES
1 Nowell P, Hungerford D. A minute chromosome in humangranulocytic leukemia. Science 1960;132:1497.
2 Rowley JD. The role of chromosome translocations inleukemogenesis. Semin Hematol 1999;36(suppl 7):59-72.
3 Pinkel D, Straume T, Gray JW. Cytogenetic analysis usingquantitative, high-sensitivity, fluorescence hybridization. ProcNatl Acad Sci USA 1986;83:2934-2938.
4 Rowley JD, Diaz MO, Espinosa R et al. Mapping chromo-some band 11q23 in human acute leukemia with biotinylated
by guest on April 13, 2018
http://theoncologist.alphamedpress.org/
Dow
nloaded from

Varella-Garcia 57
probes: identification of 11q23 translocation breakpoints witha yeast artificial chromosome. Proc Natl Acad Sci USA1990;87:9358-9362.
5 Tkachuck DC, Westbrook C, Andreef M et al. Detection ofbcr-abl fusion in chronic myelogenous leukemia by in situhybridization. Science 1990;250:559-562.
6 Paskulin G, Philips G, Morgan R et al. A pre-clinical evalua-tion of probes to detect t(8;21) AML minimal residual diseaseby fluorescence in situ hybridization. Genes ChromosomesCancer 1998;21:144-152.
7 Varella-Garcia M, Murata-Collins JL, Ai H et al. Interphasecytogenetic analysis of minimal residual disease in t(8;21)AML and enrichment using CD34 selection. Leukemia2001;15:1408-1414.
8 Dang TP, Gazdar AF, Virmani AK et al. Chromosome 19translocation, overexpression of notch3 and human lung cancer. J Natl Cancer Inst 2000;92:1355-1357.
9 French C, Miyoshi I, Aster JC et al. BRD4 bromodomain generearrangement in aggressive carcinoma with translocationt(15;19). Am J Pathol 2001;159:1987-1992.
10 Saunders WS, Shuster M, Huang X et al. Chromosomal insta-bility and cytoskeletal defects in oral cancer cells. Proc NatlAcad Sci USA 2000;97:303-308.
11 Hayashi Y. The molecular genetics of recurrent chromosomeabnormalities in acute myeloid leukemia. Semin Hematol2000;37:368-380.
12 Boomer T, Varella-Garcia M, McGavran L et al. Detection of E2A translocations in leukemias via fluorescence in situhybridization. Leukemia 2001;15:95-102.
13 Kallioniemi A, Kallioniemi OP, Sudar D et al. Comparativegenomic hybridization for molecular cytogenetic analysis ofsolid tumors. Science 1992;258:818-821.
14 Struski S, Doco-Fenzy M, Cornillet-Lefebvre P. Compilationof published comparative genomic hybridization studies.Cancer Genet Cytogenet 2002;135:63-90.
15 Schrock E, du Manoir S, Veldman T et al. Multicolor spectralkaryotyping of human chromosomes. Science 1996;273:494-497.
16 Speicher MR, Ballard SG, Ward DC. Karyotyping humanchromosomes by combinatorial multi-fluor FISH. Nat Genet1996;12:368-375.
17 Schrock E, Padilla-Nash H. Spectral karyotyping and multicolorfluorescence in situ hybridization reveal new tumor-specificchromosomal aberrations. Semin Hematol 2000;37:334-347.
18 Kobayashi S, Noda M, Isogami K et al. c-MYC amplificationand enhancement of sensitivity to cytosine arabinoside: an invitro and in vivo study on four sublines established from apulmonary adenocarcinoma. Surg Today 2002;32:608-617.
19 Biegel JA, Allen CS, Kawasaki K et al. Narrowing the criti-cal region for a rhabdoid tumor locus in 22q11. GenesChromosomes Cancer 1996;16:94-105.
20 Bruch LA, Hill DA, Cai DX et al. A role for fluorescence insitu hybridization detection of chromosome 22q dosage indistinguishing atypical teratoid/rhabdoid tumors from
medulloblastomas/central primitive neuroectodermal tumors.Hum Pathol 2001;32:156-162.
21 Barrera JE, Hong Ai, Pan X et al. Malignancy detection bymolecular cytogenetics in clinically normal mucosa adjacentto head and neck tumors. Arch Otolaryngol Head Neck Surg1998;124:847-851.
22 Barrera JE, Varella-Garcia M. Chromosomal aneuploidy as apredictor for poor outcome in patients with head and neck can-cer. Arch Otolaryngol Head Neck Surg 2001;127:1519-1520.
23 Posner JB. Neurologic Complication of Cancer. OxfordUniversity Press USA, New York, NY, 1995.
24 Van Oostenbrugge RJ, Hopman AH, Arends JW et al. Treat-ment of leptomeningeal metastases evaluated by interphasecytogenetics. J Clin Oncol 2000;18:2053-2158.
25 Slamon DJ, Clark GM, Wong SG et al. Human breast cancer:correlation of relapse and survival with amplification of theHER-2/neu oncogene. Science 1987;235:177-182.
26 Slamon DJ, Godolphin W, Jones LA et al. Studies of theHER-2/neu proto-oncogene in human and ovarian cancer.Science 1989;244:707-712.
27 Muss HB, Thor AD, Berry DA et al. C-erb-B2 expression andresponse to adjuvant therapy in women with node-positiveearly breast cancer. N Engl J Med 1994;330:1260-1266.
28 Paik S, Bryant J, Park C et al. c-erb-B2 and response to dox-orubicin in patients with axillary lymph node-positive, hor-mone receptor-negative breast cancer. J Natl Cancer Inst1998;90:1361-1370.
29 Baselga J, Trupathy D, Mendelsohn J et al. Efficacy and safetyof weekly intravenous recombinant humanized anti-p185HER2monoclonal antibody in patients with HER2/neu overexpress-ing metastatic breast cancer. J Clin Oncol 1996;14:737-744.
30 Baselga J, Norton L, Albanell J et al. Recombinant human-ized anti-HER antibody (Herceptin) enhances the antitumoractivity of paclitaxel and doxorubicin against HER2/neuoverexpressing human breast cancer xenografts. Cancer Res1998;58:2825-2831.
31 Cobleigh MA, Vogle CL, Tripathy D et al. Efficacy and safetyof Herceptin (humanized anti-HER2 antibody) as a singleagent in 222 women with HER2 overexpression who relapsedfollowing chemotherapy for metastatic breast cancer. ProcAm Soc Clin Oncol 1998;17:97a.
32 Slamon D, Leyland-Jones B, Shak S et al. Addition ofHerceptin (humanized anti-HER2 antibody) to first linechemotherapy for HER2 overexpressing metastatic breastcancer (HER2+/MBC) markedly increases anticancer activity:a randomized, multinational controlled phase III trial. ProcAm Soc Clin Oncol 1998;17:98a.
33 Pauletti G, Dandekar S, Rong HM et al. Assessment of meth-ods for tissue-based detection of the HER2/neu alteration inhuman breast cancer: a direct comparison of fluorescence insitu hybridization and immunohistochemistry. J Clin Oncol2000;18:3651-3664.
34 Kakar S, Puangsuvan N, Stevens JM et al. HER-2/neu assess-ment in breast cancer by immunohistochemistry and fluores-
by guest on April 13, 2018
http://theoncologist.alphamedpress.org/
Dow
nloaded from

cence in situ hybridization: comparison of results and corre-lation with survival. Mol Diagn 2000;5:199-207.
35 Bartlett JM, Going JJ, Mallon EA et al. Evaluating HER2amplification and overexpression in breast cancer. J Pathol2001;195:422-428.
36 Tubbs RR, Pettay JD, Roche PC et al. Discrepancies in clini-cal laboratory testing of eligibility for trastuzumab therapy:apparent immunohistochemical false-positives do not get themessage. J Clin Oncol 2001;19:2714-2721.
37 Bubendorf L, Kononen J, Koivisto P et al. Survey of geneamplifications during prostate cancer progression by high-throughput fluorescence in situ hybridization on tissuemicroarrays. Cancer Res 1999;59:803-806.
38 Hirsch FR, Varella-Garcia M, Franklin WA et al. Evaluation ofHER-2/neu gene amplification and protein expression in non-small cell lung carcinomas. Br J Cancer 2002;86:1449-1456.
39 Morris MJ, Reuter VE, Kelly WK et al. HER-2 profiling andtargeting in prostate carcinoma. Cancer 2002;94:980-986.
40 Bunn Jr PA, Helfrich B, Soriano A et al. Expression of Her-2/neu in human lung cancer cell lines by immunohistochem-istry and fluorescence in situ hybridization and relationship toin vitro cytotoxicity by trastuzumab and chemotherapeuticagents. Clin Cancer Res 2001;7:3239-3250.
41 Cohen EEW, Rosen F, Dekker A et al. Phase II study ofZD1839 (Iressa) in recurrent or metastatic squamous cell car-cinoma of the head and neck (SCCHN). Proc Am Soc ClinOncol 2002;21:225a.
42 Fukuoka M, Yano S, Giaccone G et al. Final results from aphase II trial of ZD1839 (Iressa) for patients with advancednon-small cell lung carcinoma (IDEAL 1). Proc Am Soc ClinOncol 2002;21:298a.
43 Kris R, Natale B, Herbst RS et al. A phase II trial of ZD1839(Iressa) in advanced non-small cell lung carcinoma (NSCLC)who had failed platinum- and docetaxel-based regimens(IDEAL 2). Proc Am Soc Clin Oncol 2002;21:292a.
44 Sokolova IA, Halling KC, Jenkins RB et al. The developmentof a multitarget, multicolor fluorescence in situ hybridization
assay for the detection of urothelial carcinoma in urine. J MolDiag 2000;2:116-123.
45 Halling KC, King W, Sokolova IA et al. A comparison of cytol-ogy and fluorescence in situ hybridization for the detection ofurothelial carcinoma. J Urol 2000;164:1768-1775.
46 Heselmeyer-Haddad K, Chaudhri N, Stoltzfus P et al.Detection of chromosomal aneuploidies and gene copy num-ber changes in fine needle aspirates is a specific, sensitive,and objective genetic test for the diagnosis of breast cancer.Cancer Res 2002;62:2365-2369.
47 Romeo M, Sokolova IA, Morrison LE et al. Chromosomalabnormalities in non-small cell lung carcinomas and inbronchial epithelium of high risk smokers detected by multi-target interphase fluorescence in situ hybridization. J MolDiagn (in press).
48 Franklin W, Shpall EJ, Archer P et al. Immunocytochemicaldetection of breast cancer cells in marrow and peripheral bloodof patients undergoing high dose chemotherapy with autolo-gous stem cell support. Breast Cancer Res Treat 1996;41:1-13.
49 Engel H, Kleespies C, Friedrich J et al.. Detection of circu-lating tumour cells in patients with breast or ovarian cancerby molecular cytogenetics. Br J Cancer 1999;81:1165-1173.
50 Natarajan AT, Vyas RC, Wiegant K et al. A cytogenetic fol-low up study of the victims of a radiation accident in Goiania(Brazil). Mutat Res 1991;247:103-111.
51 Ramirez MJ, Puerto S, Galofre P et al. Multicolour FISHdetection of radioactive iodine-induced 17cen-p53 chromoso-mal breakage in buccal cells from therapeutically exposedpatients. Carcinogenesis 2000;8:1581-1586.
52 Chen LC, Neubauer A, Kurisu W et al. Loss of heterozygos-ity on the short arm of chromosome 17 is associated with highproliferative capacity and DNA aneuploidy in primary humanbreast cancer. Proc Natl Acad Sci USA 1991;88:3847-3851.
53 Livingstone LR, White A, Sprouse J et al. Altered cell cyclearrest and gene amplification potential accompany loss ofwild-type p53. Cell 1992;70:923-936.
58 Molecular Cytogenetics in Clinical Oncology
by guest on April 13, 2018
http://theoncologist.alphamedpress.org/
Dow
nloaded from