Embed Size (px)
Citation preview
Molecular Epidemiology ofTuberculosis
Kathy DeRiemer, PhD, MPHSchool of Medicine
University of California, Davis
Overview
• TB transmission and pathogenesis• Genotyping methods• Genotyping for clinical management• Genotyping for TB Control Programs• Future applications of genotyping
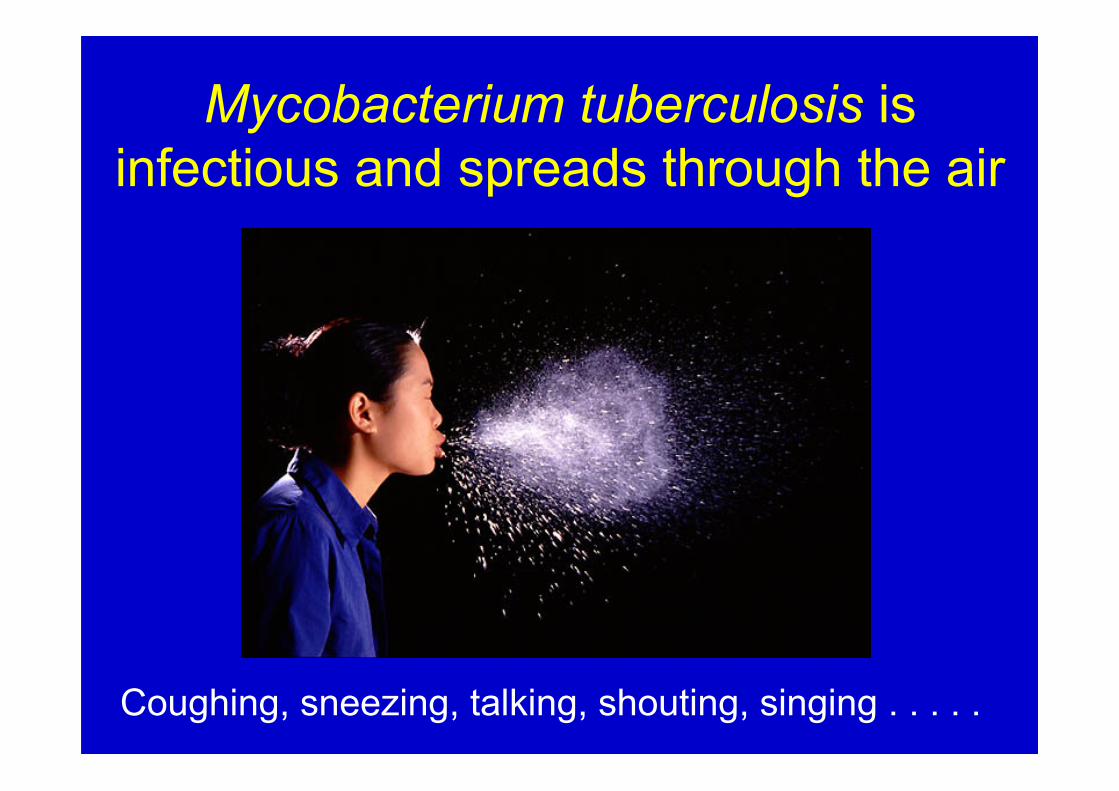
Mycobacterium tuberculosis isinfectious and spreads through the air
Coughing, sneezing, talking, shouting, singing . . . . .
Mycobacterium tuberculosis
Clonal organism, but some progeny lose chunks of DNA and become different
Thick, lipid-richcell wall and membrane
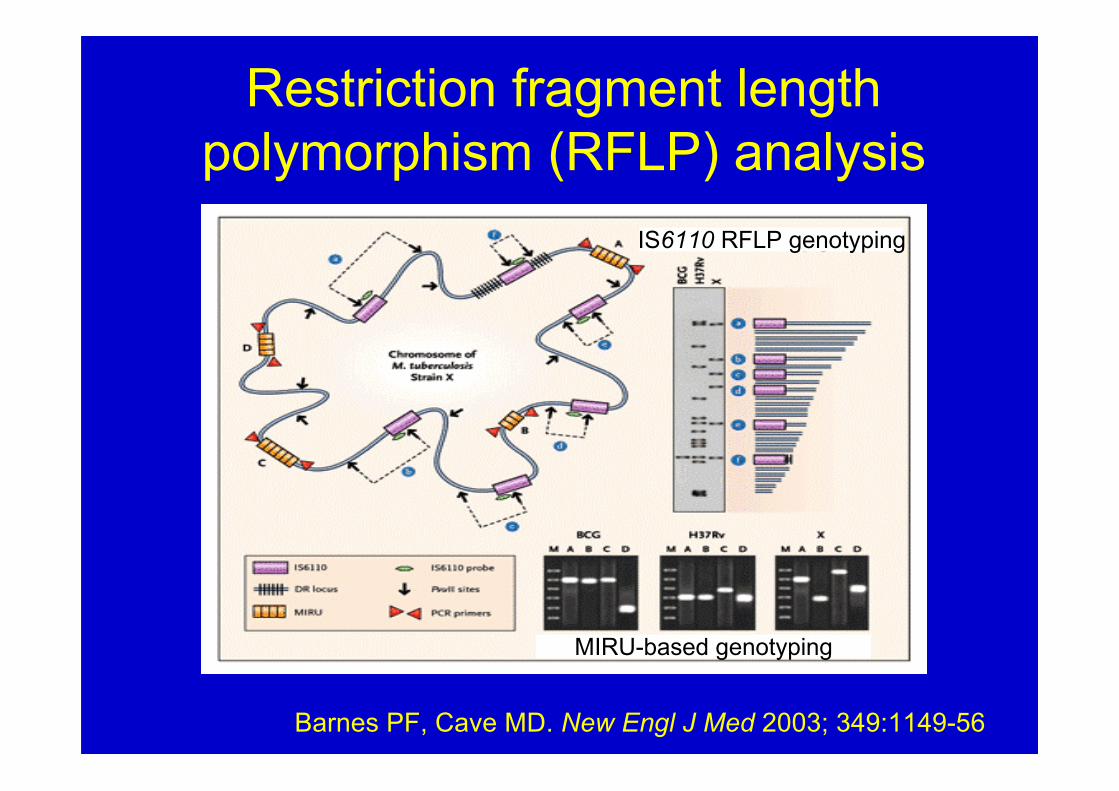
Restriction fragment lengthpolymorphism (RFLP) analysis
Barnes PF, Cave MD. New Engl J Med 2003; 349:1149-56
MIRU-based genotyping
IS6110 RFLP genotyping
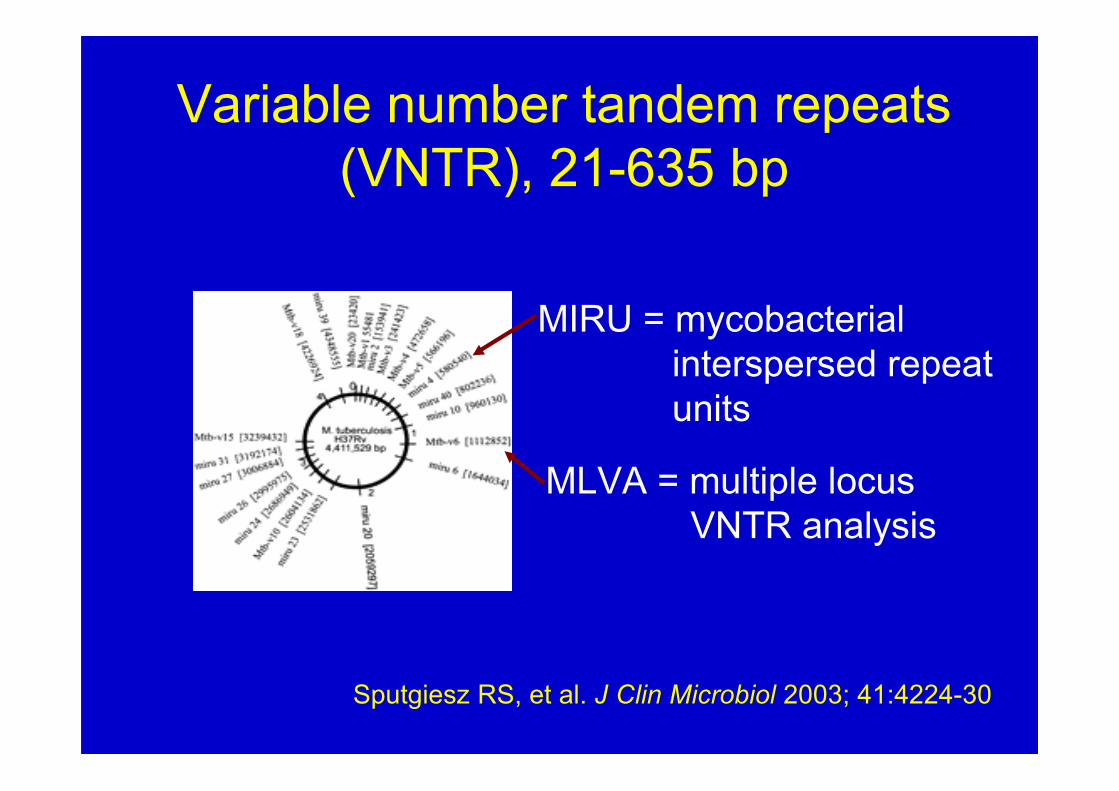
Variable number tandem repeats(VNTR), 21-635 bp
Sputgiesz RS, et al. J Clin Microbiol 2003; 41:4224-30
MIRU = mycobacterial interspersed repeat units
MLVA = multiple locus VNTR analysis
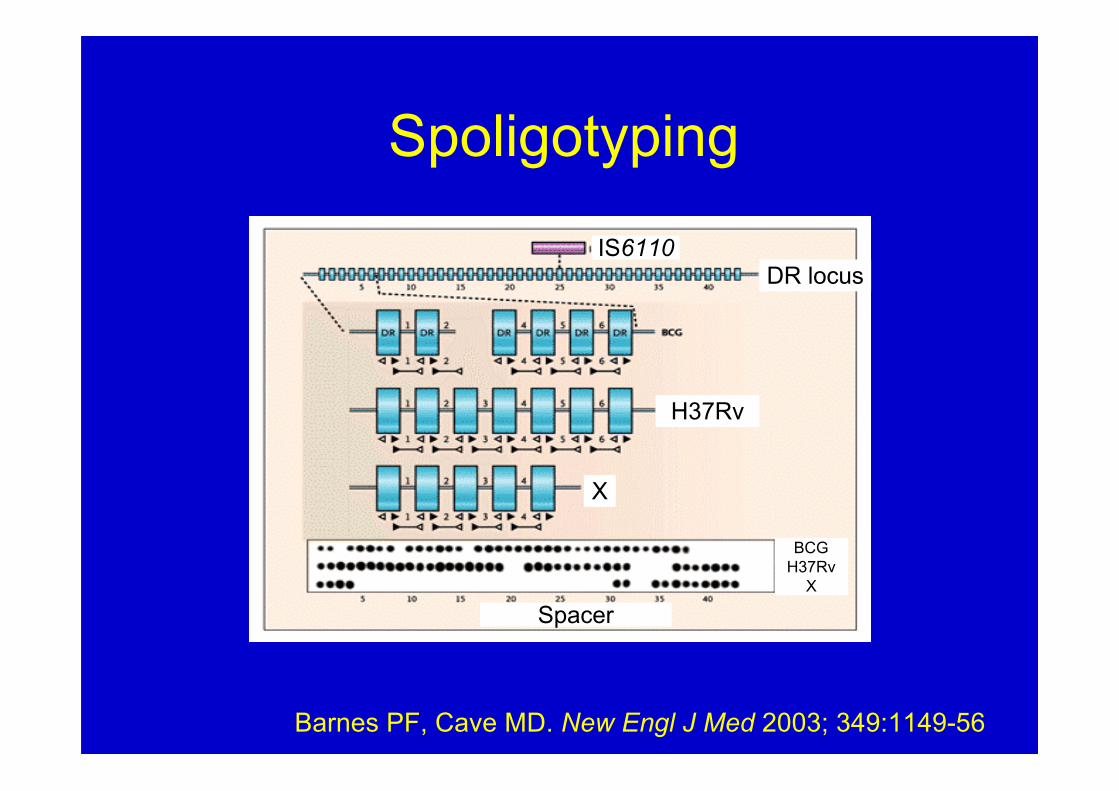
Spoligotyping
Spacer
H37Rv
IS6110DR locus
X
BCGH37Rv
X
Barnes PF, Cave MD. New Engl J Med 2003; 349:1149-56
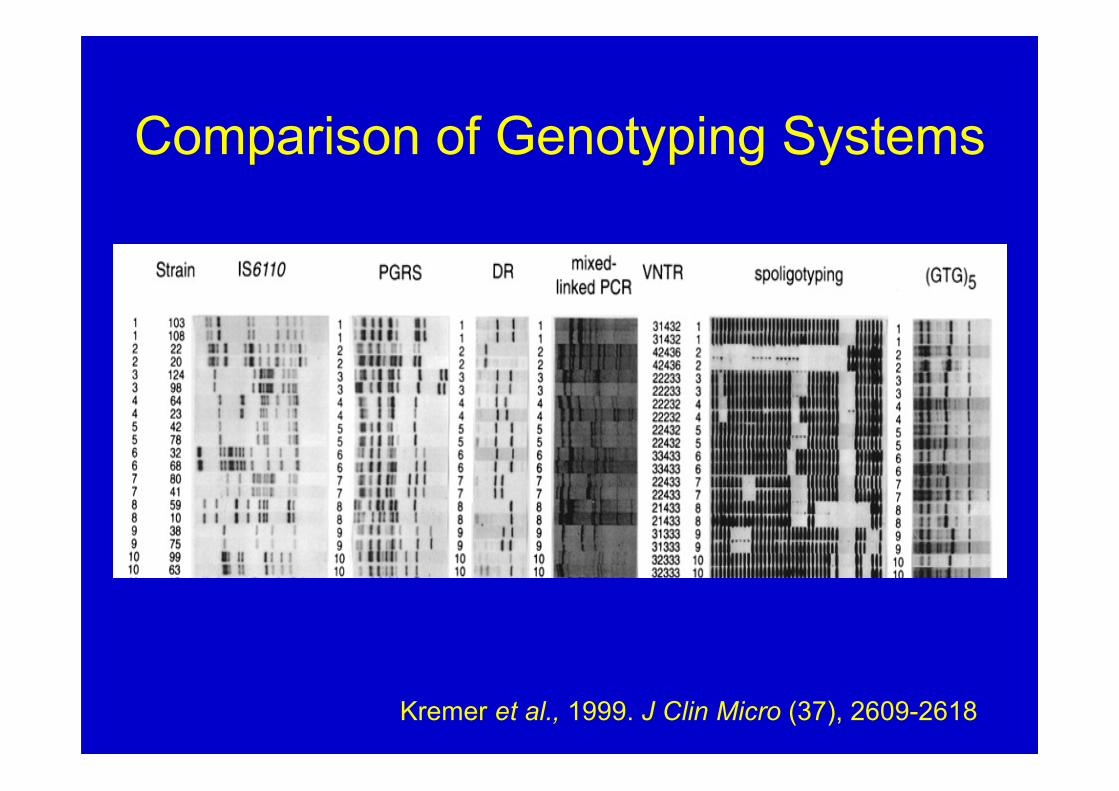
Comparison of Genotyping Systems
Kremer et al., 1999. J Clin Micro (37), 2609-2618
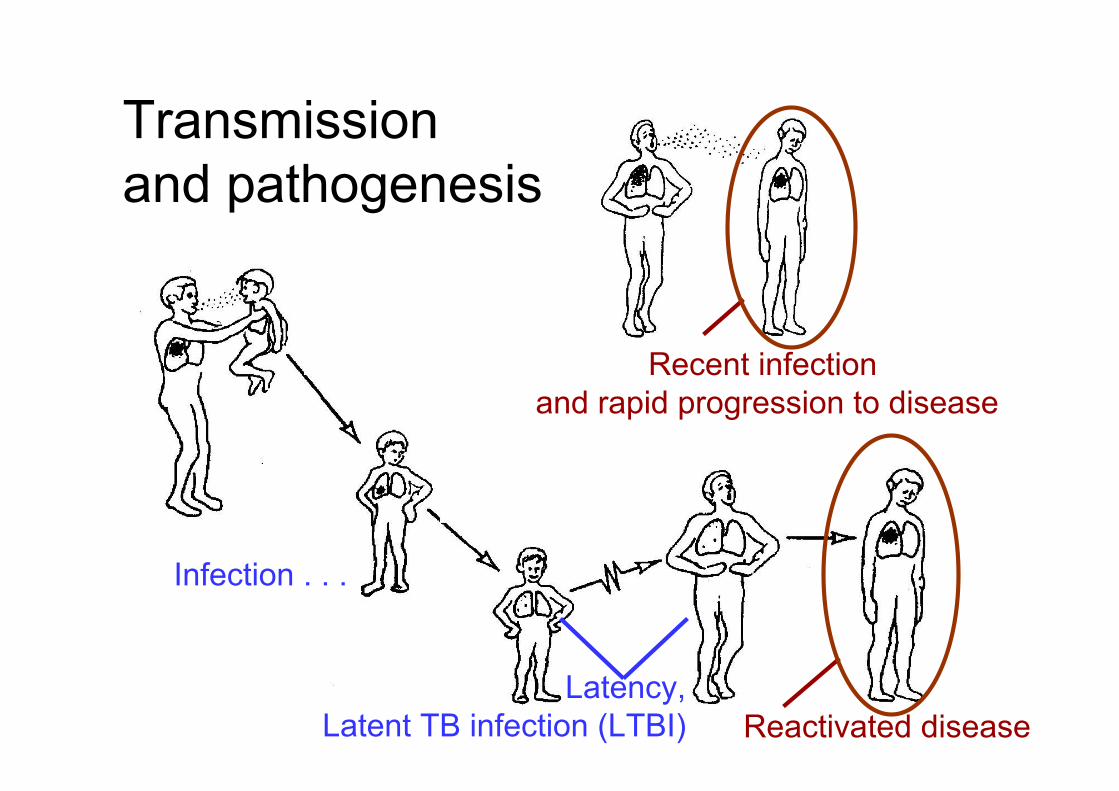
Recent infection and rapid progression to disease
Reactivated disease
Who is Infected and Diseased?
Latency,Latent TB infection (LTBI)
Infection . . .
Transmission and pathogenesis

IS6110 RFLP of M. tuberculosis
Identify unsuspected transmission
Strain 4 – Unsuspected transmission among Southeast Asian personsStrain 5 – Unsuspected transmission among US born persons
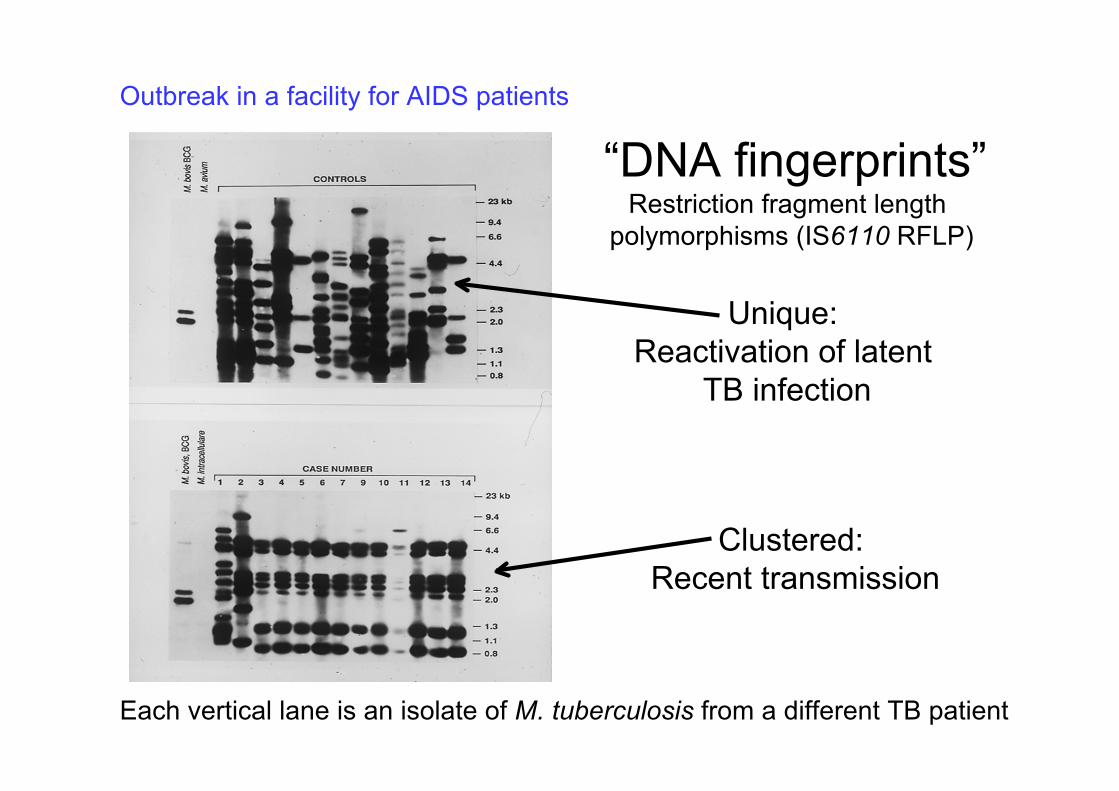
“DNA fingerprints”
Clustered: Recent transmission
Outbreak in a facility for AIDS patients
Restriction fragment length polymorphisms (IS6110 RFLP)
Each vertical lane is an isolate of M. tuberculosis from a different TB patient
Unique: Reactivation of latent
TB infection
MIRU-VNTR
Advantages• Almost as discriminatory as IS6110 RFLP• Automated high throughput analysis of many
isolates• Digital results, easy to establish and compare
databases• New loci identified for strains in specific
geographical regions
Genotyping for Clinical Management
1. Confirm cross-contamination in thelaboratory• ~ 3% of patients do not have TB• Cross contamination = sputum smears are negative and only one specimen is culture positive
Genotyping for Clinical Management
2. Evaluate recurrent tuberculosis• Relapse of disease, caused by the
same strain that caused the firstepisode
• Relapse represents treatment failure• Reinfection, with a different strain of M. tuberculosis
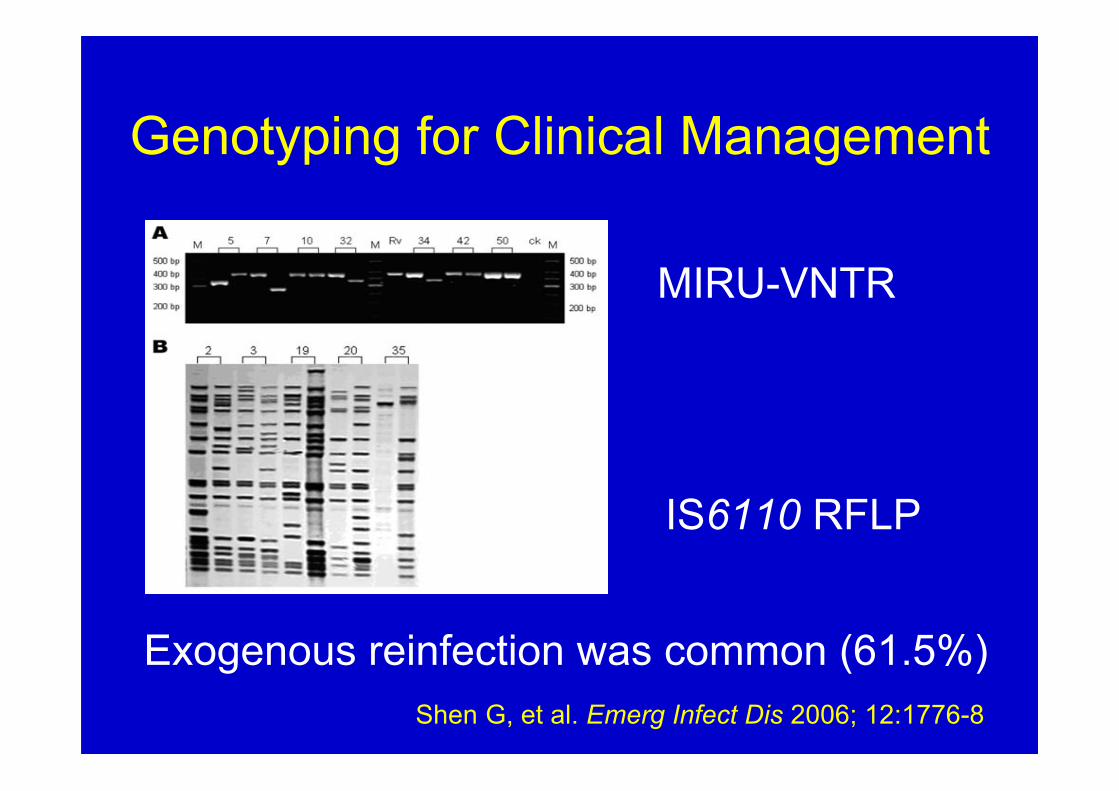
Genotyping for Clinical Management
MIRU-VNTR
IS6110 RFLP
Exogenous reinfection was common (61.5%) Shen G, et al. Emerg Infect Dis 2006; 12:1776-8
Genotyping for Clinical Management
3. Evaluate isolates with differentpatterns of drug susceptibility• Cross contamination• Original organism developed drug
resistance during or after anti-tuberculosis therapy
• Transmission of a drug-resistant strain
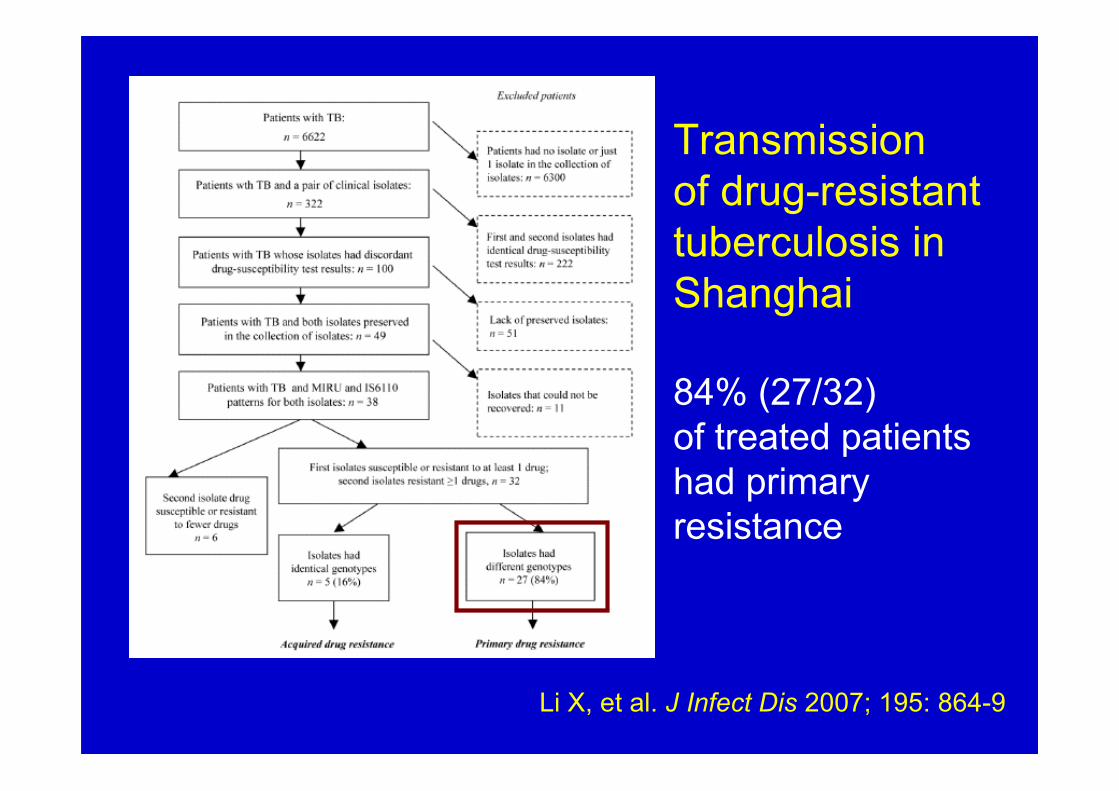
Li X, et al. J Infect Dis 2007; 195: 864-9
Transmissionof drug-resistanttuberculosis in Shanghai
84% (27/32)of treated patientshad primaryresistance
Genotyping for Clinical Management
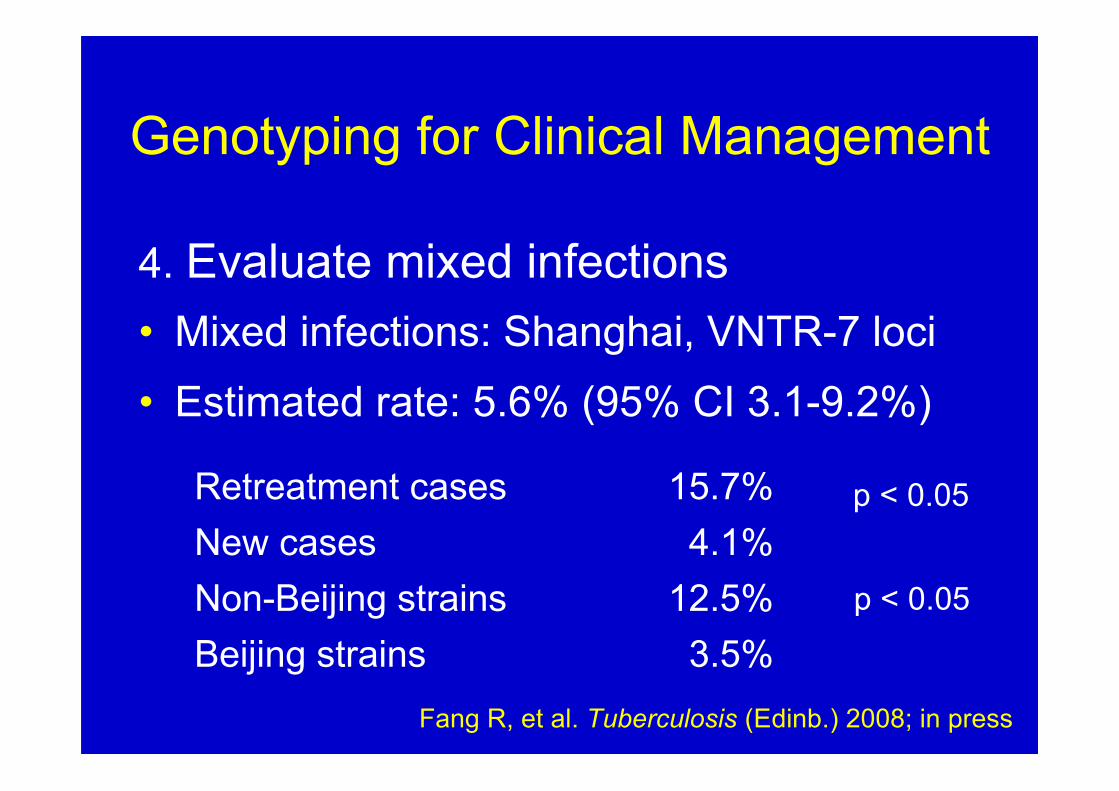
4. Evaluate mixed infections• Mixed infections: Shanghai, VNTR-7 loci• Estimated rate: 5.6% (95% CI 3.1-9.2%)
3.5%Beijing strains12.5%Non-Beijing strains4.1%New cases
15.7%Retreatment cases
Fang R, et al. Tuberculosis (Edinb.) 2008; in press
p < 0.05
p < 0.05
Genotyping for TB Control Programs
5. Evaluate chains of transmission
• Outbreak versus coincidentaloccurrence of a large number ofcases
• Guide public health measures toreduce transmission of M.tuberculosis
Genotyping for TB Control Programs
6. Identification of groups at increasedrisk for tuberculosis
Homelessshelters
Genotyping for TB Control Programs
Prisoners
Genotyping for TB Control Programs
Schools and day care centers
Genotyping for TB Control Programs
Residences for the elderly
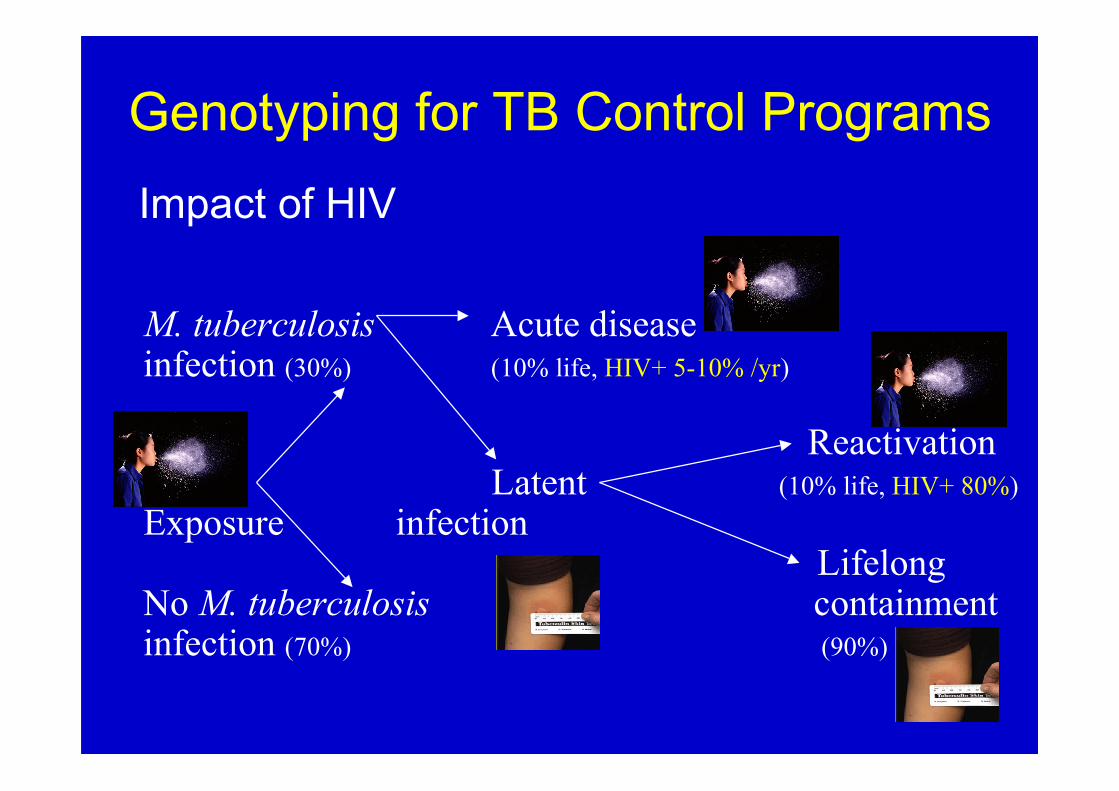
Genotyping for TB Control Programs
M. tuberculosis Acute diseaseinfection (30%) (10% life, HIV+ 5-10% /yr)
ReactivationLatent (10% life, HIV+ 80%)
Exposure infection Lifelong
No M. tuberculosis containmentinfection (70%) (90%)
Impact of HIV
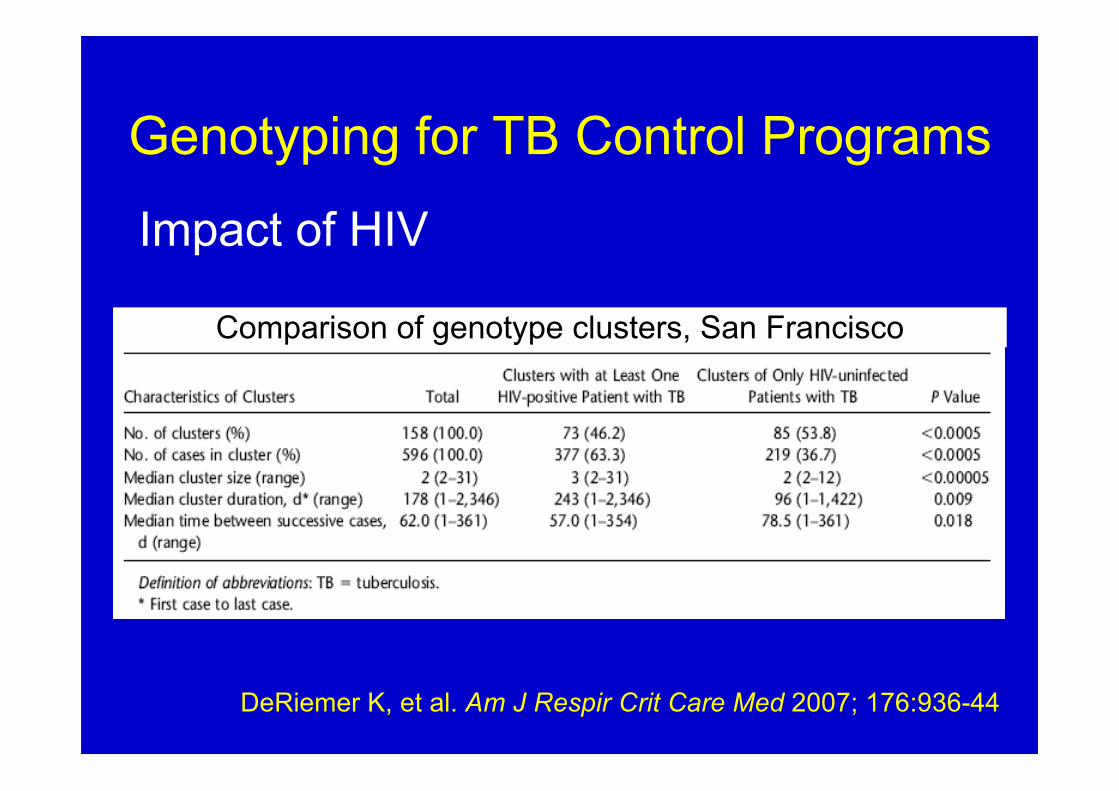
Genotyping for TB Control Programs
Impact of HIV
Comparison of genotype clusters, San Francisco
DeRiemer K, et al. Am J Respir Crit Care Med 2007; 176:936-44
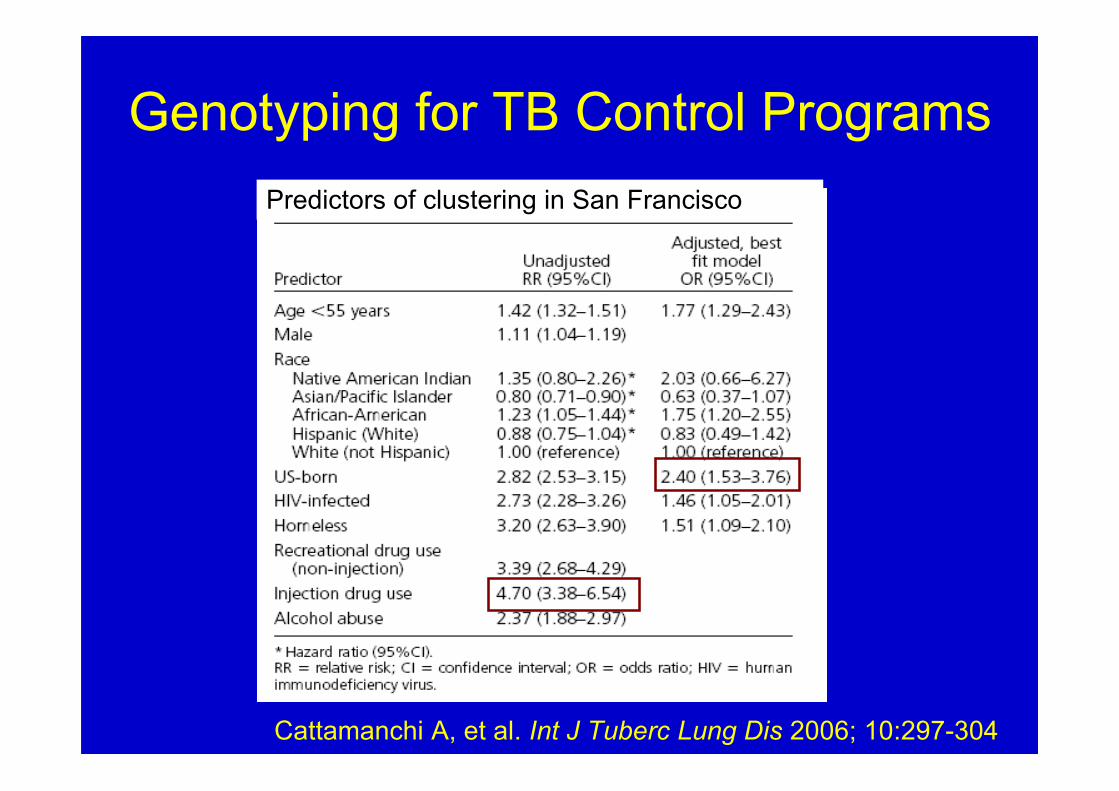
Genotyping for TB Control Programs
Cattamanchi A, et al. Int J Tuberc Lung Dis 2006; 10:297-304
Predictors of clustering in San Francisco
Genotyping for TB Control Programs
7. Improving case finding and contactinvestigations
• Identify locations TB patients use Household versus community sites• Determine who needs to be screened
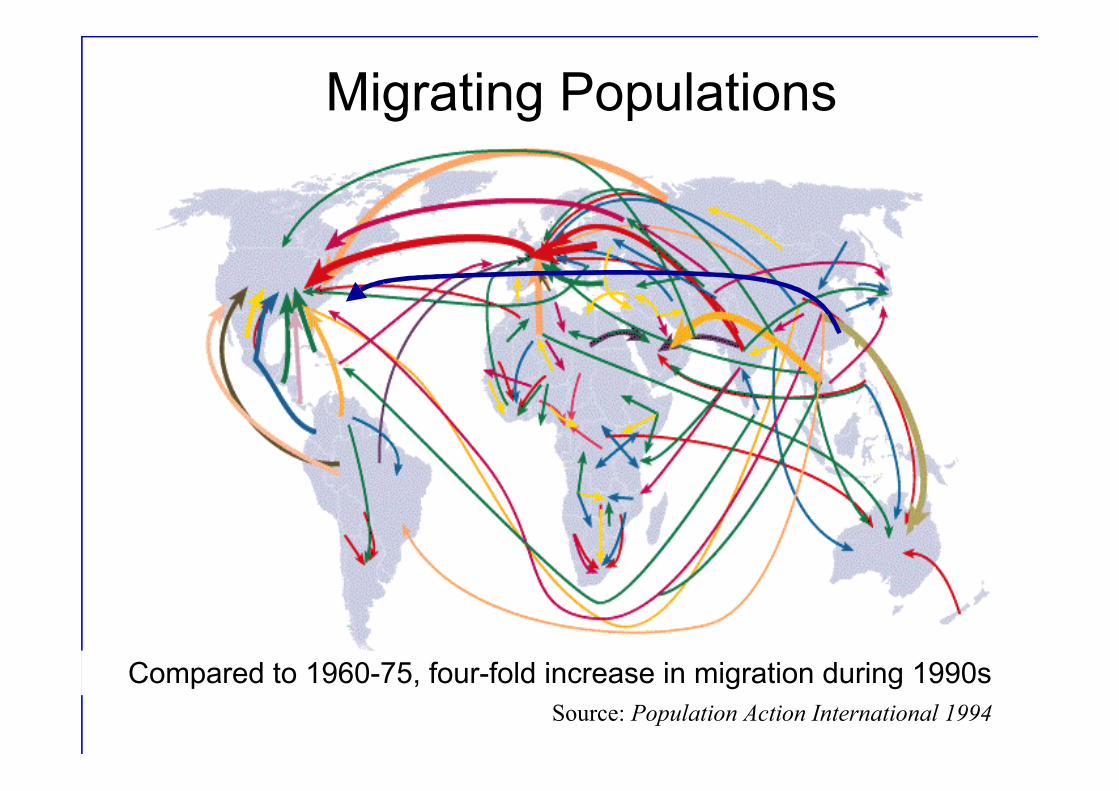
-75Source: Population Action International 1994
Migrating Populations
Compared to 1960-75, four-fold increase in migration during 1990s
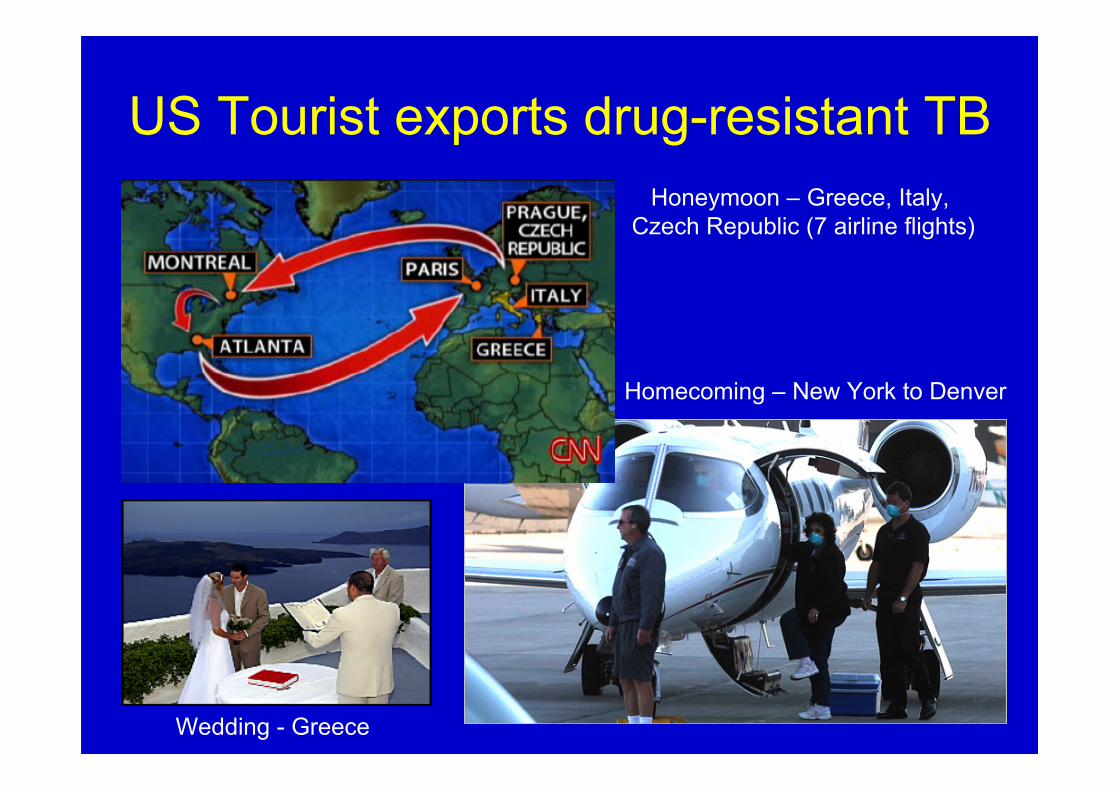
US Tourist exports drug-resistant TB
Wedding - Greece
Honeymoon – Greece, Italy, Czech Republic (7 airline flights)
Homecoming – New York to Denver
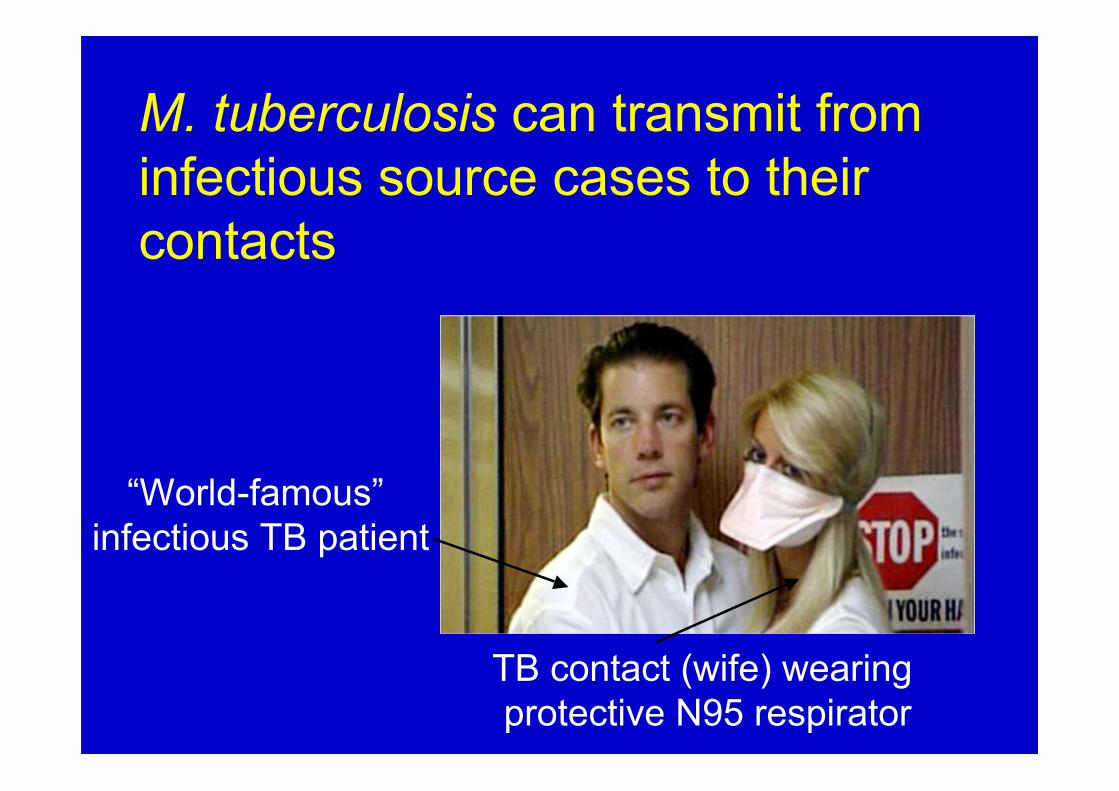
TB contact (wife) wearing protective N95 respirator
“World-famous” infectious TB patient
M. tuberculosis can transmit frominfectious source cases to theircontacts
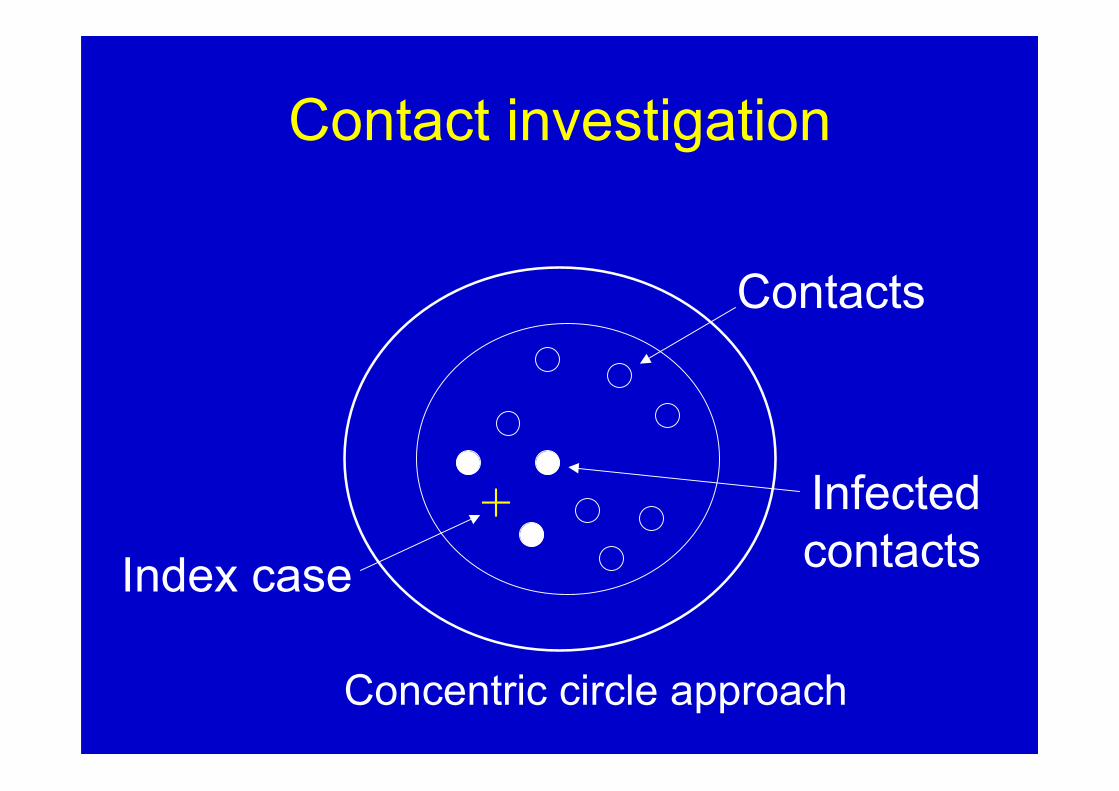
Contact investigation
Index case
Contacts
Infectedcontacts
+
Concentric circle approach
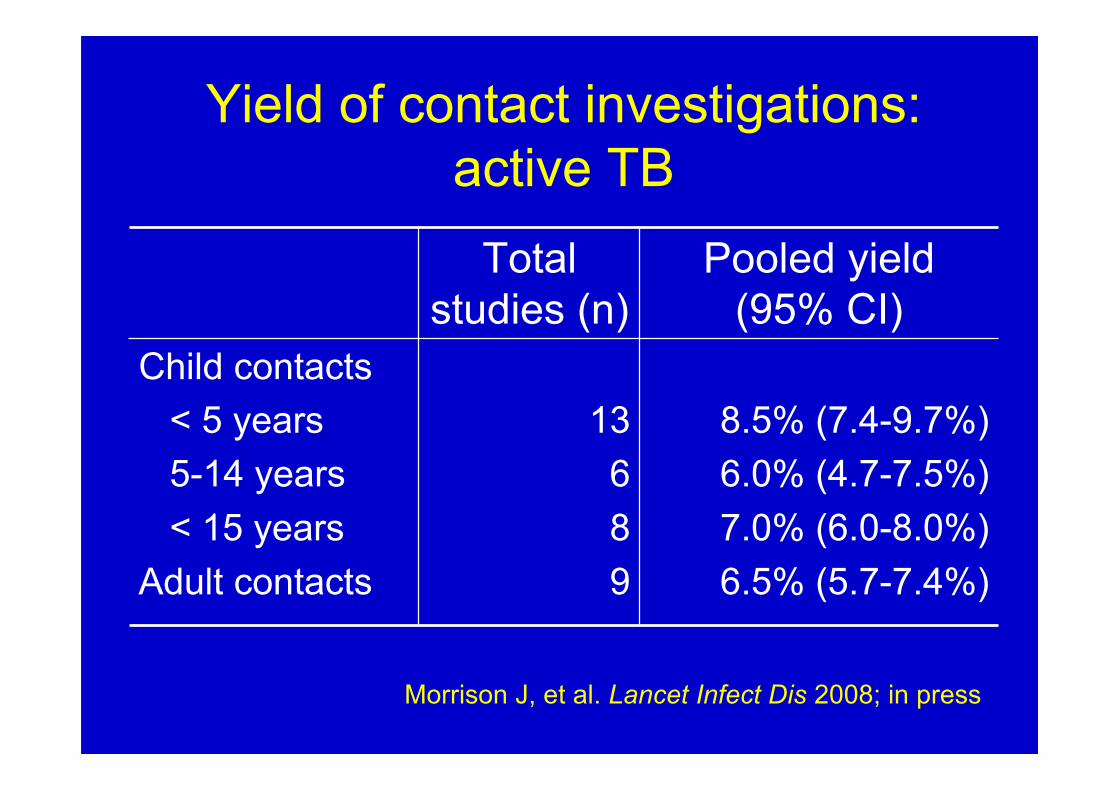
Yield of contact investigations:active TB
6.5% (5.7-7.4%)9Adult contacts
8.5% (7.4-9.7%)6.0% (4.7-7.5%)7.0% (6.0-8.0%)
1368
Child contacts < 5 years 5-14 years < 15 years
Pooled yield(95% CI)
Totalstudies (n)
Morrison J, et al. Lancet Infect Dis 2008; in press
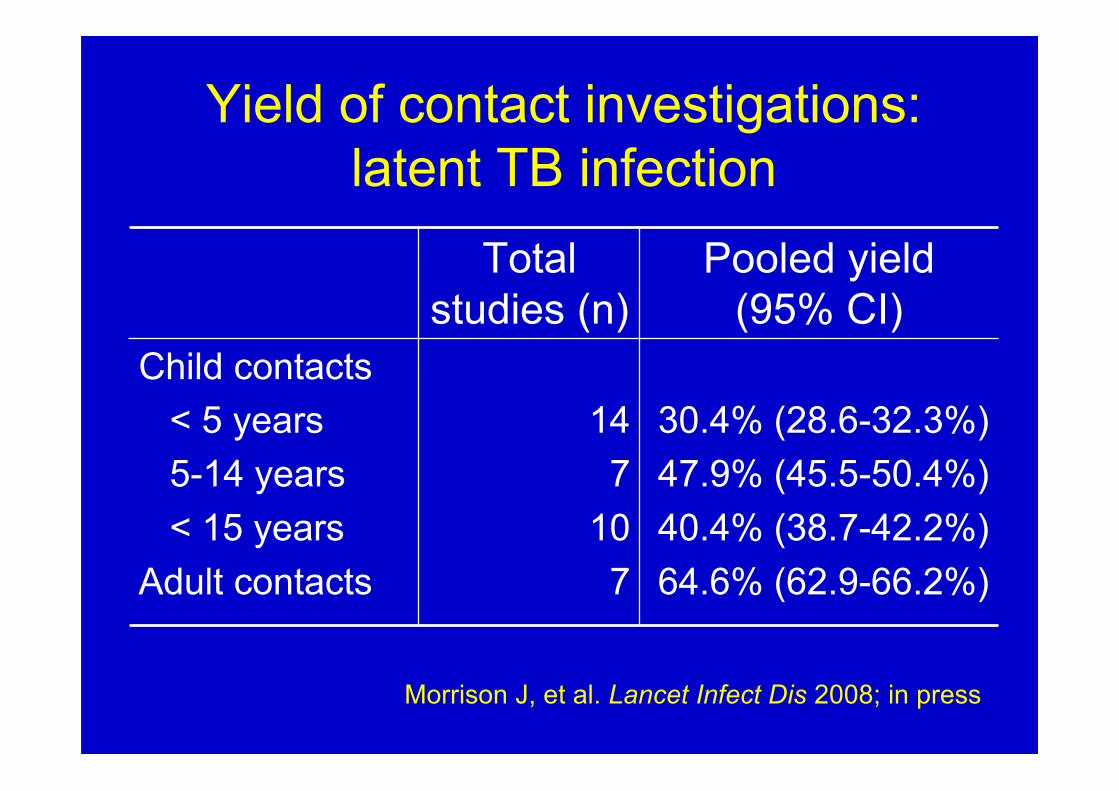
Yield of contact investigations:latent TB infection
64.6% (62.9-66.2%)7Adult contacts
30.4% (28.6-32.3%)47.9% (45.5-50.4%)40.4% (38.7-42.2%)
147
10
Child contacts < 5 years 5-14 years < 15 years
Pooled yield(95% CI)
Totalstudies (n)
Morrison J, et al. Lancet Infect Dis 2008; in press
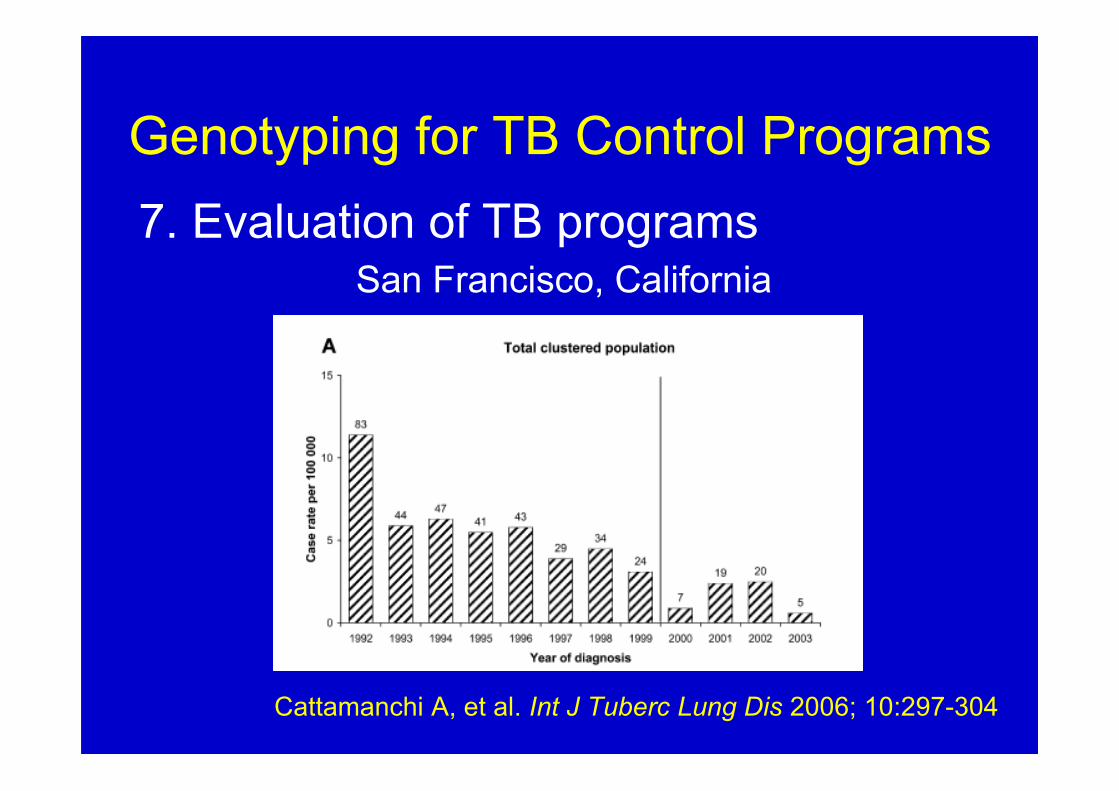
Genotyping for TB Control Programs7. Evaluation of TB programs
Cattamanchi A, et al. Int J Tuberc Lung Dis 2006; 10:297-304
San Francisco, California
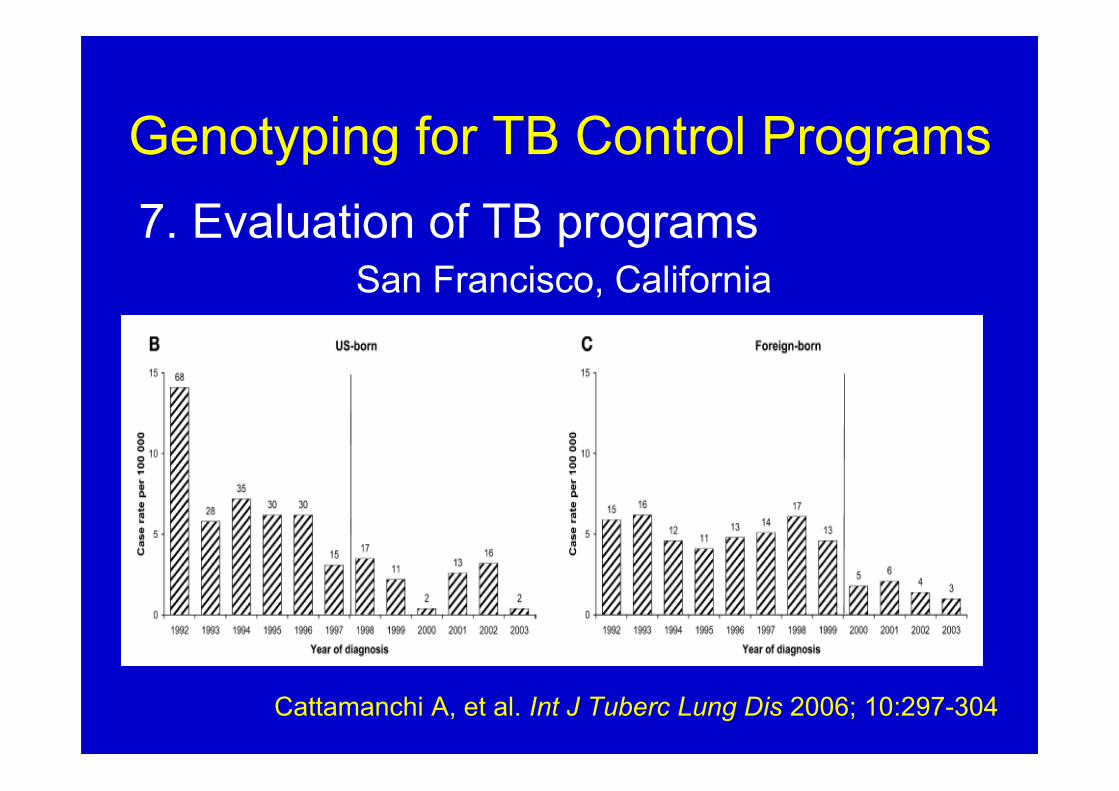
Genotyping for TB Control Programs7. Evaluation of TB programs
Cattamanchi A, et al. Int J Tuberc Lung Dis 2006; 10:297-304
San Francisco, California
Future Applications of Genotyping
• Surveillance genotyping: Real-timegenotyping
• Rapid identification of outbreaks• Evaluation of social networks
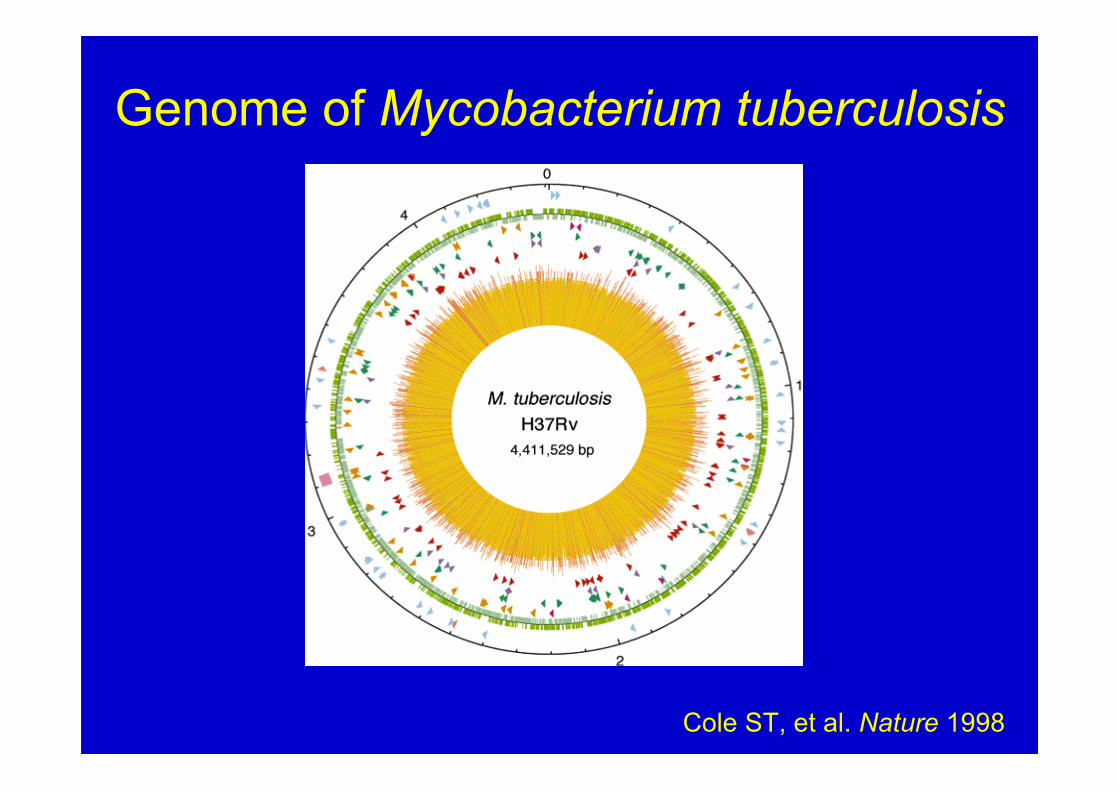
Genome of Mycobacterium tuberculosis
Cole ST, et al. Nature 1998
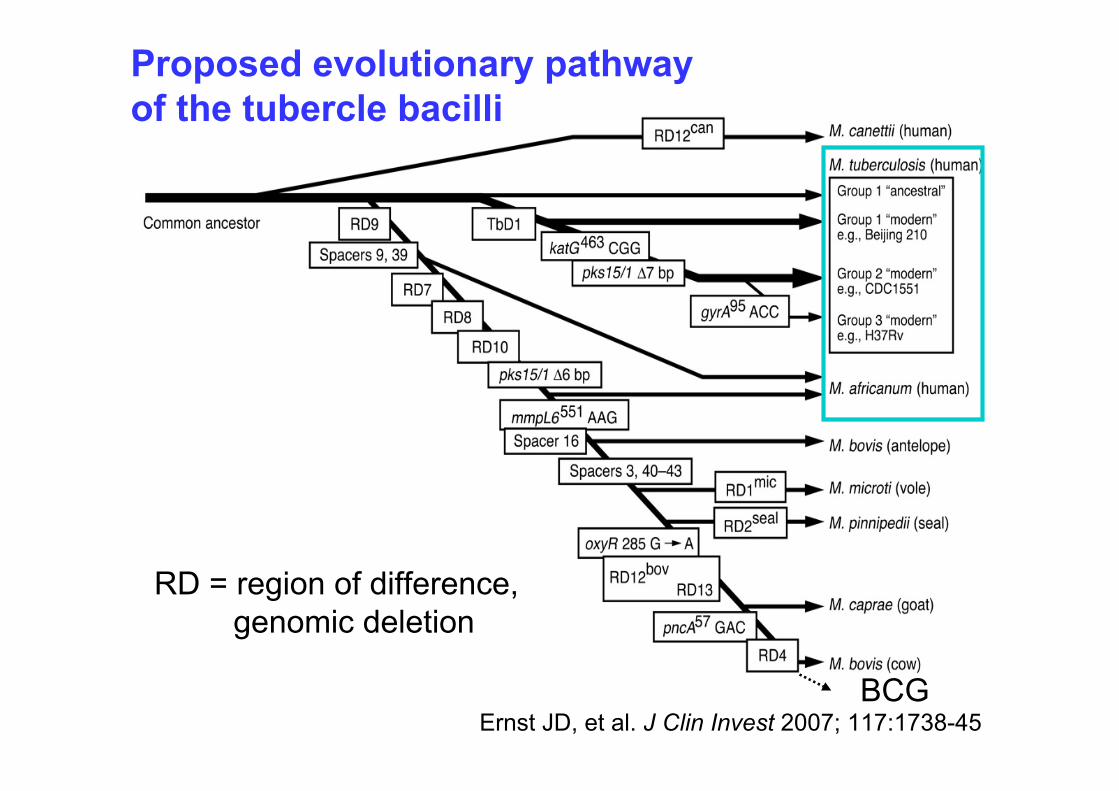
Ernst JD, et al. J Clin Invest 2007; 117:1738-45
RD = region of difference, genomic deletion
Proposed evolutionary pathwayof the tubercle bacilli
BCG
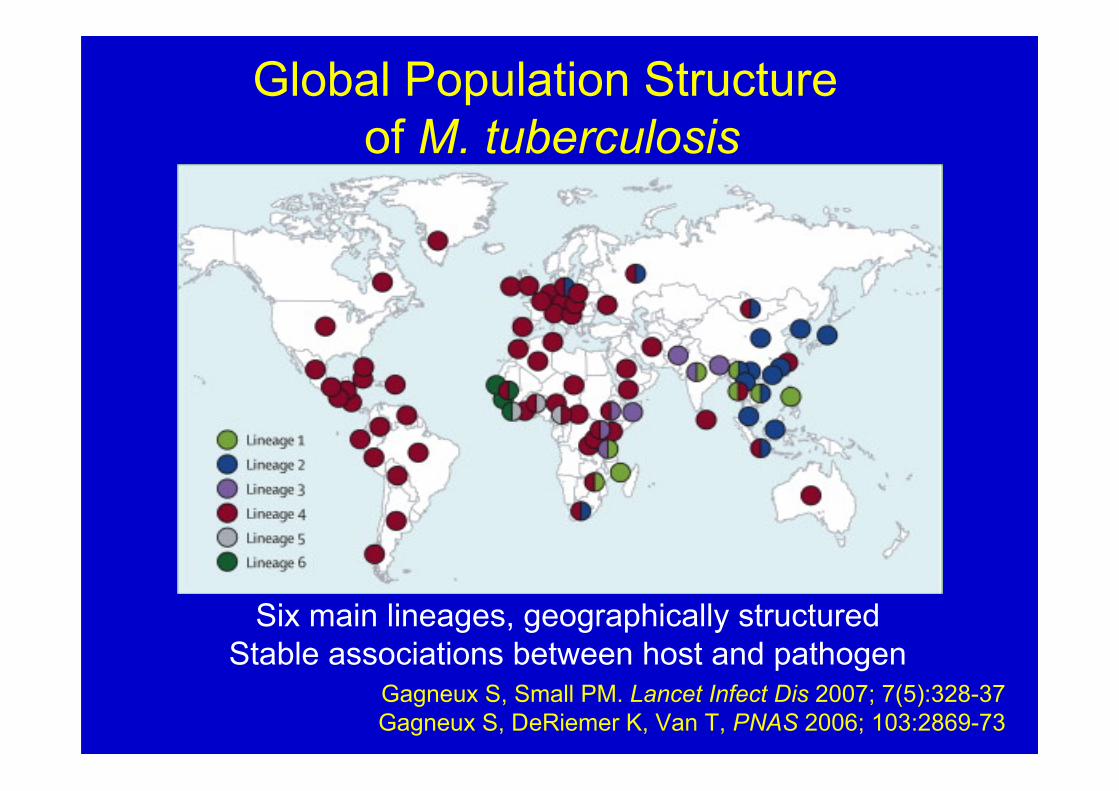
Global Population Structure of M. tuberculosis
Six main lineages, geographically structuredStable associations between host and pathogen
Gagneux S, Small PM. Lancet Infect Dis 2007; 7(5):328-37Gagneux S, DeRiemer K, Van T, PNAS 2006; 103:2869-73
New Paradigms:Interface of Several Fields
Molecular epidemiology
Microbial Pathogenesis
Functional Genomics

Acknowledgments• Shanghai CDC and Fudan University Dr. Jian Mei, Xin Shen, Dr. Qian Gao and many more
• Key Project of Chinese National Programsfor Fundamental Research & Development(973 Program 2005CB523102, 2002CB51284)
• Chinese National Programs B63(2006AA027423, 2006AA022328)
• Shanghai Key Medical Foundation(grant 5III029)
• Shanghai Municipal Sciences & TechnologyCommission (grants 05PJ14025, 05DZ22320)
Acknowledgments• Stanford University Peter Small Sebastien Gagneux Qian Gao Bouke de Jong Anthony Tsolaki
• University of California, Davis and San Francisco Phillip Hopewell, Charles Daley• National Institutes of Health• Wellcome Trust