Embed Size (px)
Citation preview

Monitoring health system performance - synthesis of some
experiences from low-income countries
Dina Balabanova, Tim Powell-Jackson, Richard Coker, Kara Hanson & Anne Mills
London School of Hygiene and Tropical Medicine
Health System Metrics, Glion sur Montreux, 28-29 September 2006

Overview
Background Complexity Objectives and methods Measurement Health financing Health care delivery Emerging issues Conclusions

Background Commitment to invest in health systems is unprecedented,
but will not last unless it is possible to show results Currently poor health information available but demand for
improved health system metrics (national / international)
Opportunities – Health System Metrics and other initiative seeking to strengthen HIS– Commitment to the health MDGs – need to measure progress– Growing consensus of importance of measurement strategies &
monitoring & evaluation built into programme planning cycles
Threats – Limited resources for health information and sustainability– Capacity constraints (in the health and social sectors)

Objectives & Methods Purpose of the study: a review of some low-income
countries’ experiences with health system performance monitoring and use of data
Case study countries:– Georgia– Rwanda– Uganda– West Bengal, India– Material from other countries
Selection criteria Analytical approaches:
– uses the WHO health system performance framework– synthesis around common themes and issues– identifying unique lessons in each type of context

Complexity How should health system performance be measured?
– Increasingly multiple contacts with the system, chronic diseases
– Outcomes determined by different care components, sectors
– Need for system-wide and inter-sectoral indicators
Tension between international (donor-driven) demands and country-level agendas and needs
Use of normative approaches imply causality
To what extent monitoring influences policy?
Impact of measurement on health systems, e.g. Indicators that are measured often improve
Monitoring information may be complex to interpret where a range of interventions co-exist.

Measurement
What approaches are taken to measure health system performance in the study
countries?

What is measured ?Data Georgia Rwanda Uganda West Bengal
Demographic Census (2002) Census (2002) Census (2002) Census (2001)
Health financing NHA (2004) NHA (2003)
NHA (2001), public expenditure reviews,
Tracking Study (2001) NHA (2001)
Health outcomes incl. births and deaths
RHS (2005) & MICS (2006), Vital
registration & HMISDHS (2005), HMIS
(facility) DHS (2004) DHS (2005)
Co-coverage of interventions
MICS (2006) & RHS (2005) DHS (2005) DHS (2004) DHS (2005)
Human resources HMIS HR inventory HR inventory HMIS
Service provisionHMIS & SAM (2005-
06)
HMIS, SAM (2004) & Service Provision
Assessment Survey (2001)
HMIS, SAM (2004), Area Team assessments HMIS
Quality n/a n/a Various / accreditation n/a
Vertical programme monitoring
Immunisation, TB, HIV/AIDS
Immunisation, malaria, HIV/AIDS, TB etc.
Immunisation, malaria, HIV/AIDS, TB etc.
Malaria, RCH, TB, Leprosy, Polio, HIV/AIDS
etc.
Disease surveillance IDRSSentinel sites (HIV), early
warning system, IDRS Sentinel sites (HIV) HMIS

Health financing
How has information been used?Where are the gaps?
What challenges remain?

Use of health financing information
Identification of financing gaps and advocacy for increased allocation of funds to health (Rwanda)
Health sector leadership and management of funds (Tanzania, Rwanda)
Equity of health financing in the health system (South Africa, Rwanda)
Protection against the financial burden of ill health (Mexico)
Resource allocation with the health sector (Rwanda)

Gaps in health financing information
Private health expenditures – difficult to collect compared to public and external health financing sources
Coverage of NHA relatively low in developing countries but expanding
Health financing data at decentralised levels for local decision-making
Financial burden of ill health and impact on impoverishment at the household level

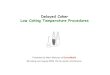
National Health Accounts in Africa
0 5 10 15 20 25 30
0
1
2
>2
NH
A R
ou
nd
s
Countries (N=46)
Number of NHA Rounds 1994 – 2004

Remaining challenges Institutionalisation of NHA into the routine activities of
Government
Underlying problems in Public Expenditure Management systems and data reliability
Timeliness of data (NHAs and household surveys)
Collection of private expenditure health financing data
Tension between disease expenditure and general health expenditure financial tracking
Addressing the needs of in-country policy makers vis-à-vis that of external agencies

Health care delivery
How has information been used?Where are the gaps?
What challenges remain?

Use of information: country examples
West Bengal, India
Aim: to monitor the performance of public sector programmes. Improve accountability and planning at national level
Standard service use indicators & regular meetings in PHC facilities
Uganda
Aim: to link health system performance monitoring to SWAPs and national policy process. Allows policy adjustment.
Data used in the annual health sector review process and to inform the development of annual plans
District league tables to rank performance of districts & motivate districts to improve indicators.
Tracking surveys – at the start of SWAP, 2001- to assess Govt systems (financial procedures, drug distribution, HR deployment)

Major gaps in measurement
Private sector – service use, service availability (infrastructure, human resources, services offered)
Vital events
Efficiency of health system
Quality of health care
Effective coverage

Remaining challenges
Low capacity and motivation to use data:
– Locally
– For decision-making or for policy initiatives
Lack of ownership by health providers, who are not involved in designing of monitoring procedure and indicators
Capacity for analysis concentrated at central level
Feedback to lower levels is limited, poor internal feedback
HMIS is often mistrusted
Selection of indicators often creates distortions
Information systems do not reflect move from project to system performance
– India: ‘critical milestones’ & vertical project indicators

Emerging issues

Data quality and reliability
Existing information systems, but data inaccessible or inappropriate to needs and policy process
Developing parallel monitoring frameworks rather than adapting & use of existing data: concerns for complexity and data reliability
HIS not always reflecting reform developments
Limited external data audit and reliance on single data sources (Rwanda, Uganda)
Technology involved in data collection, analysis and use often rely on bespoke software.

Parallel systems Donor agenda regarding data collection,
unsustainable
Data collection, analysis and use for policy is fragmented– Uganda/Nepal: lack of unified data linked to SWAPs– Private sector is often not covered (India/Uganda)
Multiple reporting requirements (Rwanda/India).
Lack of inter-sectoral information systems and unified quality standards. (Uganda/ Rwanda)
Vertical donors-supported programmes often function well in the short-term but may distort wider systems (e.g. Georgia & Angola)

Information flows & level of use
One-way traffic for information
– Disaggregated data not available at sub-national level
– Information intended to be used locally, is used at national level, or for different purpose reflecting governance & aid coordination
Information that is not aggregated nationally, less useful internationally
Governance and stewardship at local level needs to be able to draw effectively on aggregate & disaggregate data
– Disaggregated data feeds effectively into local planning when linked to decentralised decision-making (TEHIP)
Peer comparisons at district level – productive vs unhelpful

Factors facilitating measurement & use of data
Health system monitoring embedded within reform process– SWAPs/ PRSP in Uganda, Rwanda; district autonomy (TEHIP)
Unintended consequences (Afghanistan)– Selective use of data internationally (user fees/HIV, in Uganda)
In post-conflict settings, the aid influx promotes monitoring health systems & early warning systems. Possible inefficiencies.
The importance of governance– Channels for policy exist (annual reviews, SWAPs meetings) &
comparable timelines.
– Communities and non-health system stakeholders involved
Large-scale data collection exercises are resource-intensive and not synchronised with the policy process (some In-DEPTH/ LSMS).
Technology, appropriate to context

Conclusions
Effective health systems monitoring requires:
Capacity: to collect or use existing data, analyse, inform policy
Ownership
Coherence between domestic and external demands
Coherence between external agencies
Coherence between system-wide monitoring and vertical programmes performance measurement
Coherence between assessing the performance of different system elements
Domestic governance
Impact measurement to ensure sustainability/reform (scaling up)
Foster partnership between stakeholders

Acknowledgements
Georgia George GotsadzeIndia Barun KanjilalRwanda Vianney NizeyimanaTanzania Graham Reid Uganda Valeria Oliveira-Cruz
Freddy Ssengoba