Embed Size (px)
Citation preview

1
International Journal of Radiation Biology, 2012; Early Online: 1–8© 2012 Informa UK, Ltd.ISSN 0955-3002 print / ISSN 1362-3095 onlineDOI: 10.3109/09553002.2012.666004
Correspondence: Dr Hooshang Nikjoo, PhD, Radiation Biophysics Group, Department of Oncology-Pathology, Karolinska Institutet, Box 260, SE-171 76 Stockholm, Sweden. E-mail: [email protected]
(Received 5 September 2011; revised 16 January 2012; accepted 7 February 2012)
Monte Carlo single-cell dosimetry of I-131, I-125 and I-123 for targeted radioimmunotherapy of B-cell lymphoma
Christos Bousis1, Dimitris Emfietzoglou1 & Hooshang Nikjoo2
1Medical Physics Laboratory, University of Ioannina Medical School, Ioannina, Greece, and 2Radiation Biophysics Group, Department of Oncology-Pathology, Karolinska Institute, Stockholm, Sweden
Introduction
Historically, targeted radionuclide therapy has been based almost exclusively on energetic electron irradiation from b-particle emitting isotopes (Kassis and Adelstein 2004). The heterogeneous activity distribution within tumors real-ized in most clinical cases may explain the extensive usage of b-emitters (e.g., 131I) since they are capable of cross-irradiating non-targeted tumor cells (a direct consequence of their long irradiation range), thus, negating the need to target each and every tumor cell (Kassis 2008). Although the crossfire effect is of great importance in the treatment of solid tumors, it can induce unacceptable radiotoxicity in surrounding normal tissues in hematologic or disseminated disease which may exhibit single cells in the circulation
(Brans et al. 2006). In such cases, Auger-electron emitting radionuclides that exhibit a high ionization density around the decay site, represent a better therapeutic alternative if they can be placed intracellularly and, especially, in close prox-imity to (or within) nuclear DNA (Feinendegen 1975, Humm et al. 1993, Kassis 2004, Buchegger et al. 2006, Howell 2008).
Contrary to Auger-emitters, it has been shown both in vivo (Narra et al. 1992, Behr et al. 2000) and in vitro (Chan et al. 1976) that the cytotoxicity of 131I is reasonably indepen-dent of its subcellular distribution, a fact that seems logical if one considers that its penetration range spans several cell diameters. However, Neti and Howell (2003) have shown that non-uniformities in the distribution of 131I can result in changes to the shape of the survival curve and the self-dose from 131I localized on the DNA can be very radiotoxic (Neti and Howell 2004). The cytotoxic effect of 131I can be similar (or higher) to that of Auger electron emitters in cases the radiopharmaceutical was not internalized or internalized but not bound to DNA (Govindan et al. 2000, Behr et al. 2000, Michel et al. 2003).
Absorbed dose calculations still constitutes a key consid-eration in assessing the efficacy of new radiopharmaceuticals, despite the fact that internal dosimetry protocols performed in patients receiving targeted radionuclide therapy are nowhere near the sophistication of external beam dosimetry protocols (Stabin 2003). Several approaches have been used for calcu-lating the absorbed dose from targeted radionuclides from the sub-cellular to the multi-cellular level. Early studies (e.g., Bardiès et al. 1990, Bardiès and Chatal 1994) made exten-sive use of Berger’s (1973) scaled dose point kernel data for monoenergetic electrons integrated over the electron emis-sion spectrum. Another popular semi-analytic technique is the convolution method that employs analytic range-energy expressions (Howell et al. 1989). This approach underlies the Medical Internal Radiation Dose (MIRD) cellular S-values calculations (Goddu et al. 1997). An alternative approach is based on the use of a Monte Carlo code to simulate electron tracks in a particular target medium (Nikjoo et al. 2006). Recent efforts on that front include the studies of Hindié
AbstractPurpose: To study the dosimetric characteristics of a non-internalizing and an internalizing monoclonal antibody (MAb) labeled with 131I, 125I or 123I, which targets a typical lymphoma B-cell. Materials and methods: Using our hybrid Monte Carlo (MC) code which combines detailed- and condensed-history electron track simulation we carry out transport calculations of Auger and beta electrons for different intracellular distributions of radioactivity. Results: Assuming permanent retention of the MAb in cells, 125I gave the highest absorbed dose and 123I the highest absorbed dose rate. Under the more realistic scenario of biologic excretion from the cells, 123I resulted in the highest absorbed dose and absorbed dose rate. Conclusion: The present dosimetric analysis shows that biological half-life, subcellular localization, and the proper account of low-energy electrons is critical in assessing the energy deposition inside the targeted cells from the three iodide radioisotopes examined. From a dosimetric point of view and under the present approximations 123I might be superior to the other two radioiodides in the treatment of microscopic disease in B-cell lymphoma patients.
Keywords: Auger electron, Monte Carlo, cellular dosimetry, targeted radiotherapy
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Gue
lph
on 1
0/01
/12
For
pers
onal
use
onl
y.

2 C. Bousis et al.
et al. (2009), Champion et al. (2008), Hindorf et al. (2007), Song et al. (2007), Spaic et al. (2007), Strigari et al. (2006), and Torres-García et al. (2006). However, differences in: (i) The cross-section models used for describing the interactions of electrons with water, which is the medium used to approxi-mate the cellular milieu, (ii) the algorithm used to simulate electron transport, and (iii) the employed electron emission spectrum, can lead to sizeable differences in the dosimetry.
In this work, we use our in-house Monte Carlo code (MC4) (Bousis et al. 2008a) to carry out dosimetric calcula-tions at the cellular and sub-cellular level for the case of non-internalizing (surface-bound) and internalizing monoclonal antibody (MAb) labeled with either 131I or the Auger-emitters 123I and 125I, which targets a typical lymphoma B-cell.
Materials and methods
Cell modelThe cell model used for the present calculations consists of two concentric homogeneous spheres of unit density ( 1 g cm23) water representing the cell and the cell nucleus. The radionuclides were assumed to be uniformly distributed in one of the following regions of the cell: Throughout the cell (C), the cytoplasm (Cy), the cell surface (CS), or the cell nucleus (N). This spherical model was applied to simulate a Raji cell with an average radius of 7.70 mm, which is often used to model a typical lymphoma B-cell (Griffiths et al. 1999). The radius of the Raji cell nucleus was assumed to be 75% of the cellular radius (Hindorf et al. 2007).
DosimetryWithin the MIRD formalism (e.g., Loevinger et al. 1991) the absorbed dose rate D
⋅ averaged over the target region rk from activity in the source region rh is given by:
D r r A S r rk h h k h
⋅←( ) = ←( ) ,
(1)
where Ah is the activity in the source region rh and S (the so-called S-value) is defined as the absorbed dose to the tar-get region rk per unit cumulative activity in the source region rh. The S-value is given by the following relation:
S r rn E r r
mk hi i i k h
ki←( ) =
←( )∑c
f,
(2)
where c is a proportionality constant, mk is the mass of the target region, ni and Ei are the number and the energy of the particles emitted in the i-th transition, and fi k hr r←( ) is the fraction of energy emitted from the source region rh that is absorbed in the target region rk in the i-th transition. Then, the total (over time) absorbed dose averaged over the target region rk from radioactive decay in the source region rh is given by:
D r r D r r dt S r r A dt A S r rk h k h k h h h k h←( ) = ←( ) = ←( ) = ←( )∫ ∫⋅
,
(3)where Ah
∼ is the cumulated activity in the source region rh.
The values of fi k hr r←( ) used to calculate the S-value in Equa-tion (3) are obtained here from MC simulation whereas the cumulative activity Ah
∼ will be estimated under various approx-
imations for the cellular biodistribution of the radioactivity.
Monte Carlo codeDosimetric calculations are performed using both the detailed- and condensed-history modules of our in-house MC code (Bousis et al. 2008a). All electrons (primary and secondaries) are followed down to 1 Ry ( 13.6 eV). The elec-tron energy for switching from event-by-event to condensed-history simulation is set at 10 keV. Since the physics models and transport approximations used in our MC code have been presented in detail elsewhere (Emfietzoglou et al. 2000, Bousis et al. 2008a, 2008b, 2009a), only a brief description is provided here. In the detailed-history simulation mode ( 10 keV), inelastic cross sections are calculated semi-empirically from the Born and Bethe theories (Inokuti 1971) using a parameterized oscillator strength for water for soft collisions and the binary-encounter-approximation-with-exchange (BEAX) for hard collisions. Elastic cross sections are obtained from the screened Rutherford formula replaced at low-energies by the Brenner-Zaider parameterization (Brenner and Zaider 1983). The ejection angle of secondary electrons is calculated using the angle-differential Bethe formula (Kim 1972). In the condensed-history scheme ( 10 keV) we adopt a hybrid approach whereby elastic collisions are simulated individually according to the relativistic Mott scat-tering cross sections as factorized by Berger (1963), whereas for inelastic collisions we distinguish between soft and hard events depending on whether the energy loss is, respectively, smaller or higher than 1 keV. Hard inelastic collisions are modeled individually through the relativistic version of the Möller formula modified to account for the binding energy of each shell in the water molecule (Kim et al. 2000). Regard-ing the soft inelastic collisions, we go beyond stopping power theory and account for straggling via the analytic distribu-tions of Salvat et al. (2003). These straggling distributions were here calculated specifically for water using our rela-tivistic inelastic cross sections for water as described above. For electron energies above 10 keV, the present condensed-history scheme provides cellular S-values that are within 5% of those of a detailed simulation (Bousis et al. 2009b). Fur-thermore, dose-point-kernels and depth-dose-distributions in water up to 1 MeV electron energies are in good agreement with those obtained by other general-purpose codes (Bousis et al. 2008a, 2008b, 2009a).
The energy of each primary electron is randomly selected based on the radionuclide decay spectrum. Specifically, the rejection sampling technique and a pseudo-random number generator are used to choose the energy from the continuous beta decay spectrum and the discrete Auger/Internal Con-version (IC) spectrum, respectively. The point of origin of the primary electron is selected randomly within the specified (source) volume and its initial direction is sampled isotropi-cally. To obtain reasonable statistics the results are average values over 1,000,000 decays. Regarding 131I, we consider the entire b-emission spectrum using Cross et al. (1983), as well as 21 Auger electrons and 108 IC electrons according to Champion et al. (2008). The Auger emission spectra (includ-ing Coster-Kronig and IC electrons) of 125I and 123I used in the present work were taken from the American Association of Physicists in Medicine (AAPM) Nuclear Medicine Task Group Report (Howell 1992). The absorbed energy for each
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Gue
lph
on 1
0/01
/12
For
pers
onal
use
onl
y.

Single cell dosimetry 3
decay was scored in spherical shells 1 nm thick and the dose rate was subsequently calculated from Equations (1) and (2). The emission of photons is ignored since they contrib-ute less than 1% to the total dose at the spatial scale and for the radionuclides examined in the present study (Stabin and Konijnenberg 2000).
Case study for iodines 131I, 125I and 123ICurrently, there exist in the market two Food and Drug Administration (FDA) approved radiopharmaceuticals (Zevalin and Bexxar) for the treatment of non-Hodgkin’s lymphoma (NHL). Both use cluster of differentiation (CD) 20-targeting MAb that are not internalized in the cell, labeled with the b-emitters 90Y (Zevalin) and 131I (Bexxar). A recent dosimetry study by Hindorf et al. (2007) showed that the Auger emitters 125I and 123I have greater potential than 131I for treatment of B-cell lymphoma patients. However, these dosimetric calculations were carried out using the mean energies per decay of the three radioiodines and a simple condensed-history scheme based on the continuous-slow-ing-down-approximation. In a latter work, we revisited and improved upon the dosimetric calculations of Hindorf et al. (2007) for 125I and 123I by using: (i) The full Auger spectrum of these radionuclides and, (ii) a more accurate MC transport scheme with full account of straggling which goes beyond the continuous-slowing-down-approximation (Bousis et al. 2010). Unfortunately, these studies (Hindorf et al. 2007, Bousis et al. (2010)) were performed under the oversimpli-fied assumption of permanent retention of the radionuclides once they were internalized. This assumption is certainly more critical for the long-lived 125I (physical half-time, Tp, of 60 days) and 131I (Tp 8.1 days) than for the short-lived 123I (Tp 13.2 hours). However, in vitro experiments (Hansen et al. 1996, Stein et al. 2003) indicate that a sizeable fraction (∼ 20–40%) of the initial surface-bound radioactivity can be eliminated from the cell within the first 2–3 days for a residu-alizing internalized MAb. Thus, in the present work, we fur-ther extend the previous studies by Hindorf et al. (2007) and Bousis (et al. 2010) by employing a typical — biologic half-time, Tb, of 48 hours (Stein et al. 2003) for the internalized radionuclides. Moreover, we perform calculations for 131I using its full emission spectrum and compare with the results of Hindorf et al. (2007). In addition, both a non-internalizing and an internalizing radiopharmaceutical was considered corresponding, for example, to the case of a CD20- and a CD22- (or CD74-) targeting MAb, respectively. The former antigen is being targeted by Zevalin and Bexxar whereas the latter antigens will be more suitable for Auger radionuclides. This is so because, by virtue of their short irradiation ranges, Auger radionuclides will tend to minimize the cross-dose to nearby normal cells the more they are internalized by the targeted cells. This is particularly important for hematologic tumors (or long circulating MAb) where collateral damage to marrow cells can lead to myelosuppression.
The main assumptions made in the present calculations can be summarized as follows: The non-internalizing radio-pharmaceutical was assumed to bind to 128,000 receptors on the cell surface (Press et al. 1989) immediately after the administration and remained bound. On the other hand, the
internalizing radiopharmaceutical was assumed to enter the cell instantaneously after its initial binding with cell surface receptors. The very rapid internalization rate of anti-CD74 was adopted, so that approximately 107 MAb molecules are taken up per cell per day (Hansen et al. 1996). For both cases we consider that, on average, 0.76 atoms of the radionuclide are bound to a MAb. This value is taken from Hindorf et al. (2007) where the number of atoms of the radionuclide per MAb for the radioimmunoconjugates was recalculated from the specific activity for the residualizing labeling method for 125I developed by Govindan et al. (1999). This corresponds to 45 GBq/mg MAb for 123I, 410 MBq/mg MAb for 125I and 3 GBq/mg MAb for 131I. Hence, the activity is given by the fol-lowing relation:
A N tp eff=
−( )0 76. ,atomsMAb
expλ λ
(4)
where N is the number of MAb per cell and λ λ λeff p b= + with λeff effT= ln /2 , λb bT= ln /2 and λp pT= ln /2 being the effective, physical, and biological decay constants, respec-tively. For the non-internalizing case N 128,000 and T Teff p= , whereas for the internalizing case N is a function of time given by the empirical relation (Hindorf et al. 2007) N t e et t( ) .= − +− − −
10 107 0 25 7 10 4, where t is in hours.
Calculations were also performed for the clinically rele-vant case where the whole body dose is constrained to 0.5 Gy which corresponds to a red marrow dose below the thresh-old for myelotoxicity (DeNardo et al. 2002, Siegel et al. 2003). For a whole-body dose of 0.5 Gy the administered activity, A/, is approximately 33 GBq for 123I, 590 MBq for 125I and 700 MBq for 131I (Hindorf et al. 2007). We should note that, in the present study, we neglect the fact that a large fraction of the administered radioactivity ends up non- specifically bound to other locations. More realistic scenar-ios regarding the kinetics of the radiopharmaceutical at the whole body level (including non-specific binding) is beyond the scope of this theoretical dosimetric study. Then, assum-ing 107 B-cells per 1 ml of blood and a total blood volume of 5 l, the activity in each B-cell for the non-internalizing radio-pharmaceutical is:
A
Atpnon int cells/mL ml− =
×
−( )/
( ) ( )exp ,
10 5 107 3λ
(5)
whereas for the internalizing radiopharmaceutical by:
A N t X tp effint ( ) exp=
−( )atomsMAb
l λ
(6)
The value of X is calculated from the ratio of the number of atoms of the radionuclide after one day (t 24 hours) to the number of MAbs taken up per cell per day, i.e.,:
XA tp eff=
−( )×
÷−/ exp
( )( )(
λ λ1
7 310 5 1010
24h
cells/mL ml77 MAbs/cell/day)
(7)
For simplicity, the activities calculated by Equations (4) and (5)–(6) will be denoted hereafter as maximum and constrained, respectively.
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Gue
lph
on 1
0/01
/12
For
pers
onal
use
onl
y.

4 C. Bousis et al.
et al. (1987), MIRD (Weber et al. 1989) and Howell (1992). We have extended here these semi-analytic calculations to 123I using the spectrum of Howell (1992). The percentage differ-ences between the MC and semi-analytic calculations range from 17–22% (125I) to 44–47% (123I).
Table III displays cellular S-values obtained by our MC code for 123I, 125I and 131I and for five source-target configura-tions, namely, cell to cell (C¬C), cell-surface to cell (C¬CS), nucleus to nucleus (N¬N), cytoplasm to nucleus (N¬Cy), and cell-surface to nucleus (N¬CS). Tabulations are for a typical lymphocyte cell of radius 5 mm with a concentric nucleus of radius 4 mm. Also quoted for comparison are the MIRD values (Goddu et al. 1997).
The absorbed dose to a Raji cell and its nucleus for both an internalizing and a non-internalizing radioiodine is pre-sented in Table IV. We have calculated the maximum and constrained absorbed dose using Equation (3) with the cumulated activity A
∼ obtained by integration of Equation
(4), (5) and (6), respectively. The values in the parentheses correspond to the case whereby the biologic excretion of the radionuclide from the cells is not taken into account.
In Figures 2a–c, we present the constrained absorbed dose rate in the nucleus of a Raji cell as a function of time for both an internalizing and non-internalizing radiopharmaceutical labeled to 123I, 125I and 131I. Calculations are performed using Equation (1) where the activity A is obtained by Equations (5) and (6). For the internalizing case, we present results
Results
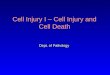
Table I displays the absorbed fraction, i.e., the fraction of the emitted energy that is retained in the sphere, for 131I uniformly distributed in spheres with radii varying from 0.01–100 mm. Comparison is made against the results of Bardiès and Chatal (1994) based on Berger’s scaled point kernel data for monoenergetic electrons, Goddu et al. (1997) based on analytic range-energy expressions for electrons, as well as Li et al. (2001) and Champion et al. (2008) based on the PARTRAC (PARticles TRACks) and CELLDOSE Monte-Carlo codes, respectively. The values in the parentheses are the percentage differences of the various calculations against our MC simulations. Note that for the smallest radii investi-gated (0.01 mm) we are not aware of any published values for the absorbed fraction. Figure 1 presents for each sphere the relative contribution to our MC-calculated absorbed frac-tion from beta particles and Auger/IC electrons of 131I. The published data of Champion et al. (2008) are also quoted for comparison. Differences between the two calculations for the relative contribution increase with decreasing sphere radius and should be ascribed solely to differences in the transport mechanics and physics models adopted by the two MC codes. However, deviations between the two calcu-lated contributions are within ∼10% for sphere radius larger than 0.1 mm.
Regarding 125I and 123I, an extensive dosimetric compari-son between our MC simulations with those of previous stud-ies at the cellular level was undertaken in our previous works (Bousis et al. 2010, Bousis 2011). For a uniform distribution of radioactivity throughout the examined spherical volumes, our results were in good agreement with those of previous studies with difference being less than 10%. However, the comparative studies of Emfietzoglou et al. (2007, 2008) for monoenergetic electrons revealed that differences between our MC simulations and those obtained by the convolution method that employs the analytic range-energy expression of Howell et al. (1989), increase rapidly as we approach the sub-cellular level. In Table II we present S-values calculated with our MC code for 10 and 20 nm diameter spheres of unit density water using the spectra of Howell (1992) for 125I and 123I. Also displayed for comparison are the corresponding values for 125I that were published by Howell (1992) and calculated using the semi-analytic method of Howell et al. (1989) for the spectra of Sastry and Rao (1984), Pomplun
Table I. Absorbed fractions for 131I uniformly distributed in spheres with radii varying from 0.01–100 mm: Comparison of our MC results with values reported by Bardiès and Chatal (1994), Goddu et al. (1994), Li et al. (2001) and Champion et al. (2008)*.
Sphere radius (mm)
Absorbed fraction
Bardiès and Chatal (1994) Goddu et al. (1994) Li et al. (2001) Champion et al. (2008) MC4
0.01 – – – – 1.09E–040.05 – – – 4.30E–04 (2 8.90%) 4.72E–040.1 – – – 6.81E–04 (2 4.22%) 7.11E–040.5 – – – 2.13E–04 (2 4.05%) 2.22E–041 – 3.57E–03 ( 2.88%) – 3.42E–03 (2 1.44%) 3.47E–035 – 1.14E–02 (2 5.00%) 1.20E–02 (0.00%) 1.18E–02 (2 1.67%) 1.20E–0210 2.23E–02 ( 0.45%) 2.01E–02 (2 9.46%) – 2.15E–02 (2 3.15%) 2.22E–0215 3.20E–02 (2 0.62%) – 3.33E–02 ( 3.42%) 3.02E–02 (2 6.21%) 3.22E–0250 9.24E–02 (2 1.28%) – 9.45E–02 ( 0.96%) 8.73E–02 (2 6.73%) 9.36E–02100 1.64E–01 (2 1.95%) 1.41E–01 (2 15.71%) – 1.53E–01 (2 8.53%) 1.67E–01
*The values in the parentheses are the percentage differences of the various calculations from our results.
Figure 1. MC simulations of the relative contribution of beta particles and Auger/IC electrons of 131I to the absorbed fraction. The published data of Champion et al. (2008) are also quoted for comparison.
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Gue
lph
on 1
0/01
/12
For
pers
onal
use
onl
y.

Single cell dosimetry 5
obtained with or without taking into account the biologic excretion of the radionuclide from the cells.
Discussion
The absorbed fraction represents a valuable dosimetric quantity for internally administered radionuclides. For 131I that, apart from beta-radiation, emits Auger electrons with short irradiation ranges, it is important to establish accurate absorbed fractions at the (sub)cellular level since the irra-diation pattern at this microscopic spatial scale might be non-uniform (Humm et al. 1994). Our MC simulations of the absorbed fractions for 131I uniformly distributed in spheres of various sizes (Table I) are in good agreement with those of previous studies (differences are less than 10–15%). Clearly, the absorbed fraction increases with increasing sphere size from ∼ 0.01% (0.01 mm radius) to ∼ 17% (100 mm radius). According to our calculations (Figure 1), the contribution of the beta electrons of 131I ranges from ∼ 9% (0.01 mm radius) to ∼90% (100 mm radius). In agreement with previous works (e.g., Sastry 1992, Unak and Cetinkaya 2005, Campos and Da Silva 2008, Champion et al. 2008), we have shown here that the contribution of the Auger/IC electrons becomes increas-ingly important with decreasing sphere size.
Several studies, which investigated the biophysical mech-anisms underlying the induction of cell death by the decay of beta- and/or Auger-emitting radionuclides in the presence of chemical radioprotectors, have shown that the lethal effect is enhanced when the radionuclides are incorporated in close proximity to (or within) the DNA. Interestingly, 5% dimethyl sulfoxide (DMSO) did not protect against lethality caused by DNA-incorporated 131I, but did protect against lethal-ity caused by unincorporated 32P and 3H2O (Howell et al. 1998). Elevating the concentration to 10% DMSO afforded protection against 131I; the dose modification factor (DMF)
was ∼ 2.3 (Bishayee et al. 2000a). In the same study Bishayee and co-workers also showed that DNA-incorporated 131I had a radiobiological effectiveness (RBE) equal to ∼ 3 compared to unincorporated 32P for cell killing (Bishayee et al. 2000a). A similar DMF was observed when cysteamine was used as the radioprotector (Bishayee et al. 2000b).
The comparison of our MC simulations of the cellular S-values for the three radioiodines against the MIRD values for various source-target configurations (Table III) shows that deviations are generally less than ∼ 15% except for the N¬CS combination where it reaches ∼ 54% (123I) and ∼ 65% (125I). The reason the largest deviations from MIRD are for the N¬CS combination is that, in this case, the target is at some distance from the source and, therefore, the results depend more strongly upon the transport scheme used which will essentially dictate the spectral distribution of electrons reaching the target region and their energy loss rate in it. Thus, one should expect that the discrepancies will also depend on the cytoplasm dimensions; generally decreasing for a thinner cytoplasm (note that in the limit of a vanishing cytoplasm the N¬CS com-bination approaches the C¬CS geometry). This finding is less pronounced in the case of 131I since, as expected, deviations decrease with increasing electron energy (Bousis et al. 2009b).
We have shown that under the present assumptions 125I delivers a much higher dose to the cell and the cell nucleus for all source distributions (Table IV) as also predicted by Hindorf et al. (2007). Specifically, the dose by 125I is 9–25 (5–15) times larger than 131I (123I) when the whole-body dose is constrained to 0.5 Gy, and 1.5–4 (1.5–2.3) times larger with respect to the maximum dose. Owing to the limited number of receptors on the cell surface, the maximum absorbed dose for a non-internalizing (C¬CS or N¬CS) radioiodine is by a factor of 100 smaller than for an internalizing (C¬Cy or N¬Cy).
On the other hand, when the whole-body dose is fixed to 0.5 Gy, the absorbed dose to the cell or its nucleus by a non-internalizing 125I or 131I is only a factor of 1.3–4.4 smaller than for the internalizing, while for 123I the situation is reversed, that is, the dose resulting from the non-internalizing 123I is higher than for the internalizing. This is because, for a fixed whole-body dose, a much smaller amount of radionuclide enters the cell which, for short-lived radionuclides (like 123I) is further limited by the physical decay during the uptake phase. Our findings confirm expectations that the more real-istic assumption of the biologic excretion from the cells has a greater influence on the long-lived 125I and 131I than on the short-lived 123I.
Interestingly, the constrained dose is reduced by a factor of ∼ 2, ∼ 7 and ∼ 40 for 123I, 131I and 125I, respectively, when
Table II. S-values calculated with our MC code for 10 and 20 nm diameter spheres of unit density water using the Howell (1992) spectra of 125I and 123I. Also displayed for comparison are the values calculated from the semi-analytic method of Howell et al. (1989) using the spectra of Sastry and Rao (1984), Pomplun et al. (1987), MIRD (Weber et al. 1989) and Howell (1992).
Spectrum
S-value (Gy/Bq s)125I 123I
10 nm 20 nm 10 nm 20 nm
Sastry and Rao (1984) 2.33E 05 4.42E 04 – –Pomplun et al. (1987) 4.83E 05 7.44E 04 – –MIRD (Weber et al. 1989) 0.64E 05 1.56E 04 – –Howell (1992) 2.38E 05 4.44E 04 1.14E 05 2.17E 04MC4 2.78E 05 5.42E 04 1.65E 05 3.19E 04
Table III. Cellular S-values obtained by our MC code for 123I, 125I and 131I and for five source-target configurations, namely, cell to cell (C¬C), cell-surface to cell (C¬CS), nucleus to nucleus (N¬N), cytoplasm to nucleus (N¬Cy), and cell-surface to nucleus (N¬CS). Tabulations are for a cell of radius 5 mm with a concentric nucleus of radius 4 mm. Also quoted for comparison are the MIRD values (Goddu et al. 1997)*.
S-value (Gy/Bq s)
123I 125I 131I
MIRD MC4 MIRD MC4 MIRD MC4
S(C¬C) 1.59E–03 1.65E–03 ( 3.77%) 3.54E–03 3.71E–03 ( 4.80%) 6.57E–04 6.86E–04 ( 4.41%)S(C¬CS) 8.50E–04 9.01E–04 ( 6.00%) 1.87E–03 2.01E–03 ( 7.49%) 4.19E–04 4.40E–04 ( 5.01%)S(N¬N) 2.98E–03 3.05E–03 ( 2.35%) 6.67E–03 6.87E–03 ( 3.00%) 1.07E–03 1.11E–03 ( 3.74%)S(N¬Cy) 2.90E–04 3.35E–04 ( 15.52%) 6.18E–04 6.94E–04 ( 12.30%) 4.00E–04 4.22E–04 ( 5.50%)S(N¬CS) 1.39E–04 2.14E–04 ( 53.96%) 2.53E–04 4.18E–04 ( 65.22%) 2.90E–04 3.11E–04 ( 7.24%)
*The values in the parentheses are the percentage differences of our MC simulations from MIRD values.
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Gue
lph
on 1
0/01
/12
For
pers
onal
use
onl
y.

6 C. Bousis et al.
non-internalizing radionuclide is larger than for the internal-izing for 125I and 131I.
With regard to the dose rate to the nucleus for a fixed whole-body dose of 0.5 Gy, 123I exhibits much larger values than 125I and 131I (Figure 2) by virtue of its shorter physical half-life, as also predicted by Hindorf et al. (2007). In par-ticular, for the non-internalizing case (N¬CS) the dose rate by 123I is an order of magnitude greater. Under the assump-tion of the permanent retention of radionuclides, 123I results in higher dose rates for the non-internalizing case (N¬CS) than for the internalizing case (N¬Cy) due to its very short physical half-life. The same is also true for the other two radioiodines when considering the biologic elimination of the radioactivity from the cells. Under this assumption, the dose rate profile exhibits a smaller maximum and a more
the biologic half-life is considered while the corresponding values in the case of maximum dose are ∼ 1.3, ∼ 5 and ∼ 28. The 123I delivers a higher dose to the cell (and its nucleus) in the internalized case than 125I and 131I. Specifically, the dose by 123I is 1.3–2 (2.3–6.5) times larger than 125I (131I) when the whole-body dose is restricted to 0.5 Gy, and 9.2–13.5 (2.4–7) times larger with respect to the maximum dose.
Also evident is that the smallest constrained and maxi-mum dose is observed for 131I and 125I, respectively. The maximum absorbed dose for a non-internalizing (C¬CS or N¬CS) radionuclide is by a factor of about 4, 20 and 80 smaller than for an internalizing (C¬Cy or N¬Cy) for 125I, 131I and 123I, respectively. Note that, contrary to the result pertaining to the assumption of permanent retention, the constrained absorbed dose to the cell (or its nucleus) by a
Table IV. Absorbed dose to a Raji cell (RC 7.70 mm) and its nucleus (RN 0.75 RC) from activity uniformly distributed in different cell compartments*.
Dose (Gy) 123I (constrained) 123I (maximum) 125I (constrained) 125I (maximum) 131I (constrained) 131I (maximum)
D(C¬C) 2.8E 00(5.3E 00) 2.4E 03 (3.2E 03) 2.1E 00 (8.2E 01) 2.6E 02 (7.2E 03) 5.0E–01 (3.5E 00) 3.8E 02 (2.0E 03)D(C¬Cy) 2.7E 00 (5.1E 00) 2.3E 03 (3.1E 03) 2.0E 00 (7.9E 01) 2.5E 02 (6.9E 03) 4.4E–01 (3.1E 00) 3.4E 02 (1.8E 03)D(C¬CS) 1.2E 01 2.7E 01 5.5E 01 6.1E 01 2.5E 00 1.7E 01D(N¬C) 3.7E 00 (6.9E 00) 3.1E 03 (4.2E 03) 1.8E 00 (7.0E 01) 2.3E 02 (6.2E 03) 5.7E–01 (4.0E 00) 4.4E 02 (2.3E 03)D(N¬Cy) 7.2E–01 (1.4E 00) 6.1E 02 (8.0E 02) 5.2E–01 (2.0E 01) 6.4E 01 (1.8E 03) 3.2E–01 (2.3E 00) 2.5E 02 (1.3E 03)D(N¬CS) 3.8E 00 8.2E 00 1.6E 01 1.8E 01 1.8E 00 1.2E 01*The values in the parentheses correspond to the case where the biological excretion of the radionuclide from the cells is not taken into account; this distinction applies only to the internalizing case, i.e. when the source region is either the whole cell (C) or the cytoplasm (Cy).
Figure 2. The absorbed dose rate in the nucleus of a Raji cell as a function of time for both an internalizing and non-internalizing radiopharmaceutical labeled with (a) 123I, (b) 125I, and (c) 131I. The calculations are based on an administered activity that gives a whole-body dose of 0.5 Gy. For the internalizing case, the profiles are obtained with or without taking into account the biological elimination of the radionuclides from the cells. In the former case a typical biological half-time (Tb) of 48 hours was used in the calculations.
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Gue
lph
on 1
0/01
/12
For
pers
onal
use
onl
y.

Single cell dosimetry 7
ReferencesBardiès M, Chatal JF. 1994. Absorbed dose for internal radiotherapy
from 22 beta-emitting radionuclides: Beta dosimetry of small spheres. Physics in Medicine and Biology 39:961–981.
Bardiès M, Lamé J, Myers MJ, Simoen JP. 1990. A simplified approach to beta dosimetry for small spheres labelled on the surface. Physics in Medicine and Biology 35:1039–1050.
Behr TM, Béhé M, Löhr M. Sgouros G, Angerstein C, Wehrmann E, Nebendahl K, Becker W. 2000. Therapeutic advantages of Auger electron- over b-emitting radiometals or radioiodine when conju-gated to internalizing antibodies. European Journal of Nuclear Med-icine 27:753–765.
Berger MJ. 1973. Improved point kernels for electron and beta-ray dosimetry. NBSIR 73–107. Gaithersburg MD: National Bureau of Standards.
Berger MJ. 1963. Monte Carlo calculation of the penetration and dif-fusion of fast charged particles. In: Alder B, Fernbach S, Rotenberg M, editors. Methods in computational physics. New York: Academic Press. pp 135–215.
Bishayee A, Rao DV, Bouchet LG, Bolch WE, Howell RW. 2000a. Protection by DMSO against cell death caused by intracellularly localized Iodine-125, Iodine-131, and Polonium-210. Radiation Research 153:416–427.
Bishayee A, Rao DV, Howell RW. 2000b. Radiation protection by cysteamine against the lethal effects of intracellularly localized Auger electron, alpha-, and beta-particle emitting radionuclides. Acta Oncologica 39:713–720.
Bousis C, Emfietzoglou D, Hadjidoukas P, Nikjoo H. 2008a. A Monte Carlo study of absorbed dose distributions in water in the vapour and liquid phases by intermediate energy electrons based on differ-ent condensed-history transport schemes. Physics in Medicine and Biology 53:3739–3761.
Bousis C, Emfietzoglou D, Hadjidoukas P, Nikjoo H, Pathak A. 2008b. Electron ionization cross-section calculations for liquid water at high impact energies. Nuclear Instruments and Methods in Physics Research B: Beam Interactions with Materials & Atoms 266:1185–1192.
Bousis C, Emfietzoglou D, Nikjoo H, Hadjidoukas P, Pathak A. 2009a. The effects of energy-loss straggling and elastic scattering models on Monte Carlo calculations of dose distribution functions for 10 keV to 1 MeV incident electrons in water. Nuclear Instruments and Methods in Physics Research B: Beam Interactions with Materials & Atoms 267:1725–1732.
Bousis C, Emfietzoglou D, Hadjidoukas P, Nikjoo H. 2009b. A Monte Carlo study of cellular S-factors for 1 keV to 1 MeV electrons. Physics in Medicine and Biology 54:5023–5038.
Bousis C, Emfietzoglou D, Hadjidoukas P, Nikjoo H. 2010. Monte Carlo single-cell dosimetry of Auger-electron emitting radionuclides. Physics in Medicine and Biology 55:2555–2572.
Bousis C. 2011. Dosimetry on sub-cellular level for intracellular incor-porated Auger-electron-emitting radionuclides: A comparison of Monte Carlo simulations and analytic calculations. Radiation Pro-tection Dosimetry 143:33–41.
Brans B, Lindén O, Giammarile F, Tennvall J, Punt C. 2006. Clinical application of newer radionuclide therapies. European Journal of Cancer 42:994–1003.
Brenner DJ, Zaider M. 1983. A computationally convenient parametri-zation of experimental angular distributions of low energy electrons elastically scattered off water vapour. Physics in Medicine and Biol-ogy 29:443–447.
Buchegger F, Perillo-Adamer F, Dupertuis YM, Bischof Delaloye A. 2006. Auger radiation targeted into DNA: A therapy perspective. European Journal of Nuclear Medicine and Molecular Imaging 33:1352–1363.
Campos L, Da Silva F. 2008. Dosimetry in thyroid follicles due to low-energy electrons of iodine using the Monte Carlo method. Radio-logia Brasileira 41:403–407.
Champion C, Zanotti-Fregonara P, Hindié E. 2008. CELLDOSE: A Monte Carlo code to assess electron dose distribution-S values for 131I in spheres of various sizes. Journal of Nuclear Medicine 49:151–157.
Chan PC, Lisco E, Lisco H, Adelstein SJ. 1976. The radiotoxicity of iodine-125 in mammalian cells. A comparative study on cell survival and cytogenic responses to 125IUdR, 131IUdR and 3HTdR. Radia-tion Research 67:332–343.
Cross WG, Ing H, Freedman NO. 1983. A short atlas of beta-ray spectra. Physics in Medicine and Biology 28:1251–1260.
DeNardo SJ, Williams LE, Leigh BR, Wahl RL. 2002. Choosing an optimal radioimmunotherapy dose for clinical response. Cancer 94:1275–1286.
Emfietzoglou D, Papamichael G, Kostarelos K, Moschovitch M. 2000. A Monte Carlo track structure code for electrons (∼10 eV–10 keV)
rapid fall-off region. This is more pronounced for 125I and 131I due to their larger physical half-lives compared to the 123I.
Although the dose rate is known to influence various bio-logical processes (Wheldon and O’Donoghue 1990), its role in cell survival in the context of radioimmunotherapy is still not clear and, therefore, it is not presently included as input in dosimetric models. Sgouros et al. (2007) has reviewed the key experimental studies that have assessed the rela-tive effect of dose rate on both tumor and normal cells and found that the literature contains conflicting data regarding the role of dose rate in the dose-response relationship that may be dependent, in part, on tumor type and experimental model or design. In fact, the three examined radioiodines, and radionuclide targeted therapy in general, delivers very low dose rates compared to external radiotherapy. There-fore, it seems unlikely that the different dose rates found for the three examined radionuclides will affect the biological response relative to each other.
Conclusion
We have presented MC simulations of the absorbed dose and dose rate in Raji cells for the three radioiodines 131I, 125I and 123I that have been widely studied in the context of targeted radiotherapy. Our dosimetric study demonstrated that by neglecting the biologic excretion of radioactivity from the cells (i.e., assuming permanent retention), 125I and 123I gave the highest absorbed dose and absorbed dose rate, respec-tively. Contrary to 123I, the isotopes 131I and 125I, resulted in higher dose rates for the internalizing (N¬Cy) than for the non-internalizing (N¬CS) case. However, under the more realistic scenario of biologic excretion from the cells, 123I led to the highest absorbed dose and absorbed dose rate while all three radioiodines resulted in higher dose rates for the non-internalizing (N¬CS) than for the internalizing (N¬Cy) case. Thus, from a dosimetric point of view, and under the present approximations, it was demonstrated that 123I might be superior to the other two radioiodides in the treatment of microscopic disease. However, for more realistic calculations with respect to their clinical application, the time-dependent biodistribution of the radionuclides within cells needs to be carefully addressed among, of course, several other factors such as, for example, the labeling efficiency and the extracel-lular pharmacokinetics (non-specific binding).
Acknowledgements
The authors thank Dr Cecilia Hindorf for valuable discus-sions during the course of this work and Dr Christophe Champion for providing raw data for the Auger and internal conversion spectra of 131I. CB and DE acknowledge financial support by the European Union FP7 ANTICARB (Monoclo-nal ANTIbody-targeted CARBon nanotubes against cancer) HEALTH-F2 - 2008–201587 research program.
Declaration of interest:
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Gue
lph
on 1
0/01
/12
For
pers
onal
use
onl
y.

8 C. Bousis et al.
Kim YK, Santos JP, Parente F. 2000. Extension of the binary-encoun-ter-dipole model to relativistic incident electrons. Physics Review A 62:1–14.
Li WB, Friedland W, Pomplun E, Jacob P, Paretzke HG, Lassmann M, Reiners C. 2001. Track structures and dose distributions from decays of 131I and 125I in and around water spheres simulating micrometasta-ses of differentiated thyroid cancer. Radiation Research 156:419–429.
Loevinger R, Budinger TF, Watson EE. 1991. MIRD primer for absorbed dose calculations, revised. New York: Society of Nuclear Medicine.
Michel RB, Brechbiel MW, Mattes MJ. 2003. A comparison of 4 radionu-clides conjugated to antibodies for single-cell kill. Journal of Nuclear Medicine 44:632–640.
Narra VR, Howell RW, Harapanhalli RS, Sastry KSR, Rao DV. 1992. Radiotoxicity of some iodine-123, iodine-125 and iodine-131- labeled compounds in mouse testes: Implications for radiopharma-ceutical design. Journal of Nuclear Medicine 33:2196–2201.
Neti PV, Howell RW. 2003. When may a nonuniform distribution of I131 be considered uniform? An experimental basis for multicellular dosimetry. Journal of Nuclear Medicine 44:2019–2026.
Neti PV, Howell RW. 2004. Isolating effects of microscopic nonuni-form distributions of I131 on labeled and unlabeled cells. Journal of Nuclear Medicine 45:1050–1058.
Nikjoo H, Uehara S, Emfietzoglou D, Cucinotta FA. 2006. Track-structure codes in radiation research. Radiation Measurements 41:1052–1074.
Pomplun E, Booz J, Charlton DE. 1987. A Monte Carlo simulation of Auger cascades. Radiation Research 111:533–552.
Press OW, Farr AG, Borroz KI, Anderson SK, Martin PJ. 1989. Endocy-tosis and degradation of monoclonal antibodies targeting human B-cell malignancies. Cancer Research 49:4906–4912.
Salvat F, Fernández-Varea JM, Sempau J. 2003. PENELOPE: A code sys-tem for Monte Carlo simulation of electron and photon transport. OECD/NEA Workshop Proceedings, Issy-les-Moulineaux, France. Available from http://www.nea.fr/html/dbprog/peneloperef.html
Sastry KSR, Rao DV. 1984. Dosimetry of low energy electrons. In: Rao DV, Chandra R, Graham M, editors. Physics of nuclear medicine: Recent advances. New York: American Institute of Physics. pp 169–208.
Sastry KSR. 1992. Biological effects of the Auger emitter 125I: A review. Report No. 1 of AAPM Nuclear Medicine Task Group No. Medical Physics. 6. 19:1361–1370.
Sgouros G. Knox SJ, Joiner MC, Morgan WF, Kassis AI. 2007. MIRD continuing education: Bystander and low-dose-rate effects: Are these relevant to radionuclide therapy? Journal of Nuclear Medicine 48:1683–1691.
Siegel JA, Stabin MG, Sparks RB. 2003. Total-body and red marrow dose estimates. Journal of Nuclear Medicine 44:320–321.
Song H, Du Y, Sgouros G, Prideaux A, Frey E, Wahl RL. 2007. Thera-peutic potential of 90Y- and 131I-labeled anti-CD20 monoclonal antibody in treating non-Hodgkin’s lymphoma with pulmonary involvement: A Monte Carlo-based dosimetric analysis. Journal of Nuclear Medicine 48:150–157.
Spaic R, Ilic R, Petrovic B, Toskovic F. 2007. Referent 3D solid tumour model and absorbed dose calculations at cellular level in radionu-clide therapy. World Journal of Nuclear Medicine 6:45–51.
Stabin M. 2003. Developments in the internal dosimetry of radiophar-maceuticals. Radiation Protection and Dosimetry 105:575–580.
Stabin M, Konijnenberg MW. 2000. Re-evaluation of absorbed frac-tions for photons and electrons in spheres of various sizes. Journal of Nuclear Medicine 41:149–160.
Stein R, Govindan SV, Mattes MJ, Chen S, Reed L, Newsome G, McBride BJ, Griffiths GL, Hansen HJ, Goldenberg DM. 2003. Improved iodine radiolabels for monoclonal antibody therapy. Cancer Research 63:111–118.
Strigari L, Menghi E, D’Andrea M, Benassi M. 2006. Monte Carlo dose voxel kernel calculations of beta-emitting and Auger-emitting radio-nuclides for internal dosimetry: A comparison between EGSnrcMP and EGS4. Medical Physics 33:3383–3389.
Torres-García E, Garnica-Garza HM, Ferro-Flores G. 2006. Monte Carlo microdosimetry of 188Re and 131I-labelled anti-CD20. Physics in Medicine and Biology 51:N349–356.
Unak P, Cetinkaya B. 2005. Absorbed dose estimates at the cellular level for 131I. Applied Radiation and Isotopes 62:861–869.
Weber DA, Eckerman KF, Dillman LT, Ryman JC. 1989. MIRD: Radionulide data and decay schemes. New York: Society of Nuclear Medicine.
Wheldon TE, O’Donoghue JA. 1990. The radiobiology of targeted radiotherapy. International Journal of Radiation Biology 58:1–21.
and protons (∼ 0.3–10 MeV) in water: Partitioning of energy and collision events. Physics in Medicine and Biology 45:3171–3194.
Emfietzoglou D, Bousis C, Hindorf C, Fotopoulos A, Pathak A, Kostare-los K. 2007. A Monte Carlo study of energy deposition at the sub-cellular level for application to targeted radionuclide therapy with low-energy electron emitters. Nuclear Instruments and Methods in Physics Research B: Beam Interactions with Materials & Atoms 256:547–553.
Emfietzoglou D, Kostarelos K, Hadjidoukas P, Bousis C, Fotopoulos A, Pathak A, Nikjoo H. 2008. Subcellular S-factors for low-energy electrons: A comparison of Monte Carlo simulations and continu-ous-slowing-down calculations. International Journal of Radiation Biology 84:1034–1044.
Feinendegen LE. 1975. Biological damage from the Auger effect, possible benefits. Radiation Environmental Biophysics 12:85–99.
Goddu SM, Rao DV, Howell RW. 1994. Multicellular dosimetry for micrometastases: Dependence of self-dose versus cross-dose to cell nuclei on type and energy of radiation and subcellular distribution of radionuclides. Journal of Nuclear Medicine 35:521–530.
Goddu SM, Howell RW, Bouchet LG, Bolch WE, Rao DV. 1997. MIRD Cellular S values. Reston VA: Society of Nuclear Medicine.
Govindan SV, Mattes MJ, Stein R, McBride BJ, Karacay H, Goldenberg DM, Hansen HJ, Griffiths GL. 1999. Labeling of monoclonal antibod-ies with diethylenetriaminepentaacetic acid-appended radioiodi-nated peptides containing D-amino acids. Bioconjugate Chemistry 10:231–240.
Govindan SV, Goldenberg DM, Elsamra SE, Griffiths GL, Ong GL, Brechbiel MW, Burton J, Sgouros G, Mattes MJ. 2000. Radionu-clides linked to a CD74 antibody as therapeutic agents for B-cell lymphoma: Comparison of Auger electron emitters with b-particle emitters. Journal of Nuclear Medicine 41:2089–2097.
Griffiths GL, Govindan SV, Sgouros G, Ong GL, Goldenberg DM, Mattes MJ. 1999. Cytotoxicity with Auger electron-emitting radionuclides delivered by antibodies. International Journal of Cancer 81:985–992.
Hansen HJ, Ong GL, Diril H, Valdez A, Roche PA, Griffiths GL, Gold-enberg DM, Mattes MJ. 1996. Internalization and catabolism of radiolabeled antibodies to the MHC class-II invariant chain by B-cell lymphomas. Biochemistry Journal 320:293–300.
Hindié E, Champion C, Zanotti-Fregonara P, Rubello D, Colas-Linhart N, Ravasi L, Moretti JL. 2009. Calculation of electron dose to target cells in a complex environment by Monte Carlo code “CELLDOSE”. European Journal of Nuclear Medicine and Molecular Imaging 36:130–136.
Hindorf C, Emfietzoglou D, Lindén O, Bousis C, Fotopoulos A, Kostarelos K, Flux GD. 2007. Single-cell dosimetry for radioimmu-notherapy of B-cell lymphoma patients with special reference to leukemic spread. Cancer Biotherapy and Radiopharmaceuticals 22: 357–366.
Howell RW. 2008. Auger processes in the 21st century. International Journal of Radiation Biology 84:959–975.
Howell RW, Rao DV, Sastry KSR. 1989. Macroscopic dosimetry for radioimmunotherapy: Nonuniform activity distributions in solid tumors. Medical Physics 16:66–74.
Howell RW. 1992. Radiation spectra for Auger-electron emitting radio-nuclides: Report No.2 of AAPM Nuclear Medicine Task Group No. 6a). Medical Physics 19:1371–1383.
Howell RW, Goddu SM, Bishayee A, Rao DV. 1998. Radioprotection against lethal damage caused by chronic irradiation with radio-nuclides in vitro. Radiation Research 150:391–399.
Humm JL, Roeske JC, Fisher DR, Chen GTY. Howell RW, Rao DV. 1993. Microdosimetry concepts in radioimmunotherapy. Medical Physics 20:535–541.
Humm JL, Howell RW, Rao DV. 1994. Dosimetry of Auger-electron-emitting radionuclides: Report no.3 of AAPM Nuclear Medicine Task Group No. 6. Medical Physics 21:1901–1915.
Inokuti M. 1971. Inelastic collisions of fast charged particles with atoms and molecules – The Bethe theory revisited. Reviews of Modern Physics 43:297–347.
Kassis AI, Adelstein SJ. 2004. Radiobiologic principles in radionuclide therapy. Journal of Nuclear Medicine 46:4S–12S.
Kassis AI. 2008. Therapeutic radionuclides: Biophysical and radiobio-logic principles. Seminars in Nuclear Medicine 38:358–366.
Kassis AI. 2004. The amazing world of Auger electrons. International Journal of Radiation Biology 80:789–803.
Kim YK. 1972. Angular distribution of secondary electrons in the dipole approximation. Physics Review A 6:666–670.
Int J
Rad
iat B
iol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Gue
lph
on 1
0/01
/12
For
pers
onal
use
onl
y.
![Evaluation of CD146 as Target for Radioimmunotherapy against … · 2019. 3. 25. · ized antibody developed by Abgenix [29], entered a phase I study enrolling patients with malignant](https://img.pdfslide.net/doc/110x75/5fe45ba174c6bc0dc0101594/evaluation-of-cd146-as-target-for-radioimmunotherapy-against-2019-3-25-ized.jpg)





![A Phase I Study of [225Ac]-FPI-1434 Radioimmunotherapy in€¦ · Ac]-FPI-1434 is a radioimmunoconjugate consisting of a humanized monoclonal antibody (AVE1642) that binds to the](https://img.pdfslide.net/doc/110x75/5f20908268bba8344a7fcc5a/a-phase-i-study-of-225ac-fpi-1434-radioimmunotherapy-in-ac-fpi-1434-is-a-radioimmunoconjugate.jpg)