Embed Size (px)
Citation preview
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
NCCN.org – For Clinicians │ NCCN.org/patients – For Patients
Monthly Oncology Tumor BoardsA Multidisciplinary Approach to Individualized Patient Care
Systemic Therapy Selection in Metastatic Castration-Resistant Prostate Cancer
Andrew J. Armstrong, MD, ScMDuke Cancer Institute
Joshua M. Lang, MD, MSUniversity of Wisconsin Carbone Cancer Center
Wednesday, July 21, 2021 | 3:00 – 4:00 PM [EDT]
Andrew J. Armstrong, MD, ScMDuke Cancer Institute
Andrew J. Armstrong, MD, ScM, is Professor of Medicine, Professor in Surgery, and Associate Professor in Pharmacology and Cancer Biology at Duke University School of Medicine. He is a medical oncologist at Duke Cancer Institute, and an internationally recognized expert in experimental therapeutics and biomarker development in genitourinary cancers, particularly prostate cancer.
Dr. Armstrong trained at Duke University as a biomedical engineer and received his medical degree at the University of Virginia School of Medicine. He completed a residency in internal medicine at the Hospital of the University of Pennsylvania and a fellowship at Johns Hopkins Hospital, followed by public health clinical investigation training at the Bloomberg School of Public Health. Dr. Armstrong joined Duke’s faculty in 2006, where he has subsequently remained.
As a clinical and translational investigator, Dr. Armstrong’s research examines experimental therapeutics for patients with advanced genitourinary malignancies, particularly with a focus on prostate cancer and the investigation of biomarkers of response and benefit. His reasearch for circulating tumor cell biology and epithelial plasticity is funded by the US Department of Defense, the Prostate Cancer Foundation and Movember, the NIH, and the American Cancer Society. He has developed a number of experimental agents in prostate and renal cell cancer, including completed or ongoing trials of mTOR inhibitors and PI3 kinase inhibitors, immunomodulatory agents, hormonal therapies, and anti-angiogenic agents. He is also heavily involoved in the leadersip of several phase 3 studies in advanced prostate cancer.
Dr. Armstrong is a member of the NCCN Prostate Cancer Panel and is co-chair of Prostate Cancer Working Group 3 which establishesguidelines for clinical investigation in men with advanced prostate cancer. He also contributes to the NCCN Oncology ResearchProgram (ORP) by serving on the Enzalutamide Scientific Review Committee and the Temsirolimus Scientific Advisory Board and Scientific Review Committee.
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
Joshua M. Lang, MD, MSUniversity of Wisconsin Carbone Cancer Center
Joshua M. Lang, MD, MS, is Associate Professor in the Department of Medicine at the University of Wisconsin School of Medicine and Public Health. He is the Co-Director of the internal medicine residency’s physician-scientist training program (IMPACT). He is the Director of UW Carbone Cancer Center’s circulating biomarker core and liquid biospecimen team, and co-leader of its tumor microenvironmental program, and the clinical co-chair of its precision medicine molecular tumor board.
Dr. Lang earned his medical degree from University of Illinois College of Medicine at Chicago. He completed a residency in internal medicine and fellowship in medical oncology at University of Wisconsin Hospital and Clinics.
Dr. Lang’s research interests are in developmental therapeutics for prostate cancer. He is the lead principal investigator on the multi-PI Department of Defense Prostate Cancer Research Program, and the PI of a Prostate Cancer Foundation-funded project to investigatetherapeutic targeting of AR-variant prostate cancer with a novel antibody drug conjugate. He also leads clinical trials that evaluate circulating tumor cells in solid tumor malignancies, efficacy of IMMU-132 in patients with metastatic castration-resistant prostate cancer and chemohormonal therapy in high-risk and oligo-metastatic prostate cancer.
Dr. Lang is a member of the American Society of Clinical Oncology (ASCO), the Society for Immunotherapy of Cancer, and the American Association of Cancer Research.
Dr. Lang is a Value Pathways Task Force Member of the NCCN Prostate Cancer Panel.
Case 1• 61 yo AAM presented at age 47 with a PSA of 8, found to have GG4 high
risk disease on biopsy
• After radical prostatectomy for pT3a high risk disease, PSA dropped to undetectable but rose 1 year later and he completed salvage RT and 2 years of ADT given prior + margins
• PSA rose despite ADT after 5 years, and he eventually progressed to nmCRPC and was treated with enzalutamide for 3 years
• Developed mCRPC in 2018 and progressed despite use of sipuleucel-T with pathologic adenopathy (RP, pelvic) and he was treated with docetaxel with a 6 mo response

© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
Case 1• 61 yo AAM presented at age 47 with a PSA of 8, found to have GG4 high
risk disease on biopsy
• After radical prostatectomy for pT3a high risk disease, PSA dropped to undetectable but rose 1 year later and he completed salvage RT and 2 years of ADT given prior + margins
• PSA rose despite ADT after 5 years, and he eventually progressed to nmCRPC and was treated with enzalutamide for 3 years
• Developed mCRPC in 2018 and progressed despite use of sipuleucel-T with pathologic adenopathy (RP, pelvic) and he was treated with docetaxel with a 6 mo response
• ctDNA profiling showed a BRCA2 mutation and germline testing confirmed this BRCA2 mutation
The most appropriate next step is:
a. Olaparibb. Radium-223c. Pembrolizumabd. Abiraterone acetate
• He was treated with olaparib 300 mg bid and disease responded with a partial soft tissue response, 50% PSA decline, and lack of bone metastasis
• However, he developed disease progression 9 mo later
• ctDNA analysis at that time showed a BRCA2 reversion mutation and TP53 mutation
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
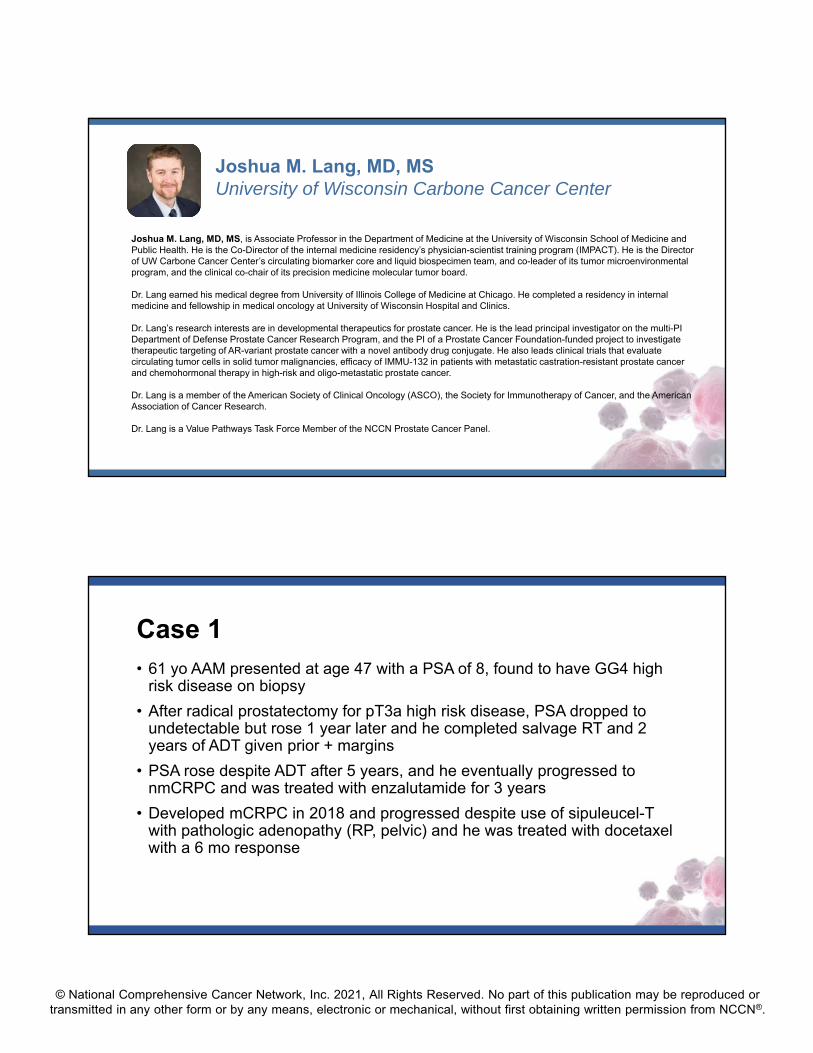
DNA Repair Gene Alterations (Somatic and Germline) are Common in Metastatic PCa1-3
• 23% of metastatic castration-resistant prostate cancers harbor DNA repair alterations
• The frequency of DNA repair alterations increases in metastatic disease vs. localized disease
12% of men with metastatic prostate cancer have a germline DNA repair defect
Somatic Germline
1. Robinson D, et al. Cell. 2015;161:1215-28; 2. Pritchard CC, et al. N Engl J Med. 2016;375:443-53; 3. Antonakaris ES, et al. Eur Urol. 2018;74(2):218-25.
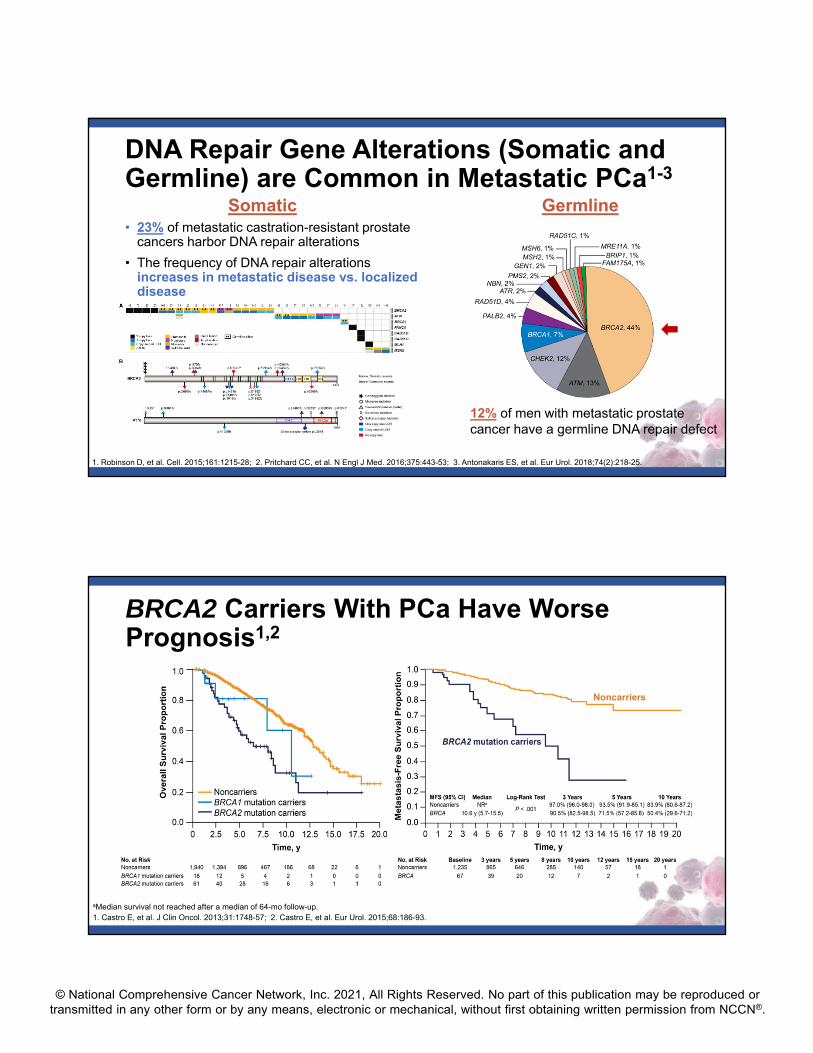
BRCA2 Carriers With PCa Have Worse Prognosis1,2
Noncarriers
aMedian survival not reached after a median of 64-mo follow-up.1. Castro E, et al. J Clin Oncol. 2013;31:1748-57; 2. Castro E, et al. Eur Urol. 2015;68:186-93.
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
Family History is a Real Risk Factor
A father or brother with prostate cancer doubles a man’s risk of prostate cancer
A mother or sister with breast cancer diagnosed before age 50 significantly increases a woman’s risk of breast cancer
A mother or sister with breast cancer can affect a man’s risk of prostate cancer
Chen et al. Prostate. 2008. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2574825/; Colditz et al., 2012 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3387322/
Cascading Impact
~12% of men with prostate cancer carry an inherited DNA repair gene mutation
• Full family history is important to collect during the genetic evaluation
• In-person genetic counseling is the gold standard
• Patients’ psychosocial needs/preferences should dictate the mode of counseling

© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
© 2021 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN®. To view the most recent and complete version of the NCCN Guidelines, go online to NCCN.org.
• Pathogenic variants are those defined as mutations or alterations known to disrupt the function of the gene and confer disease risk.
• A Variant of Uncertain Significance (VUS) is a variation in a genetic sequence for which the association with disease risk is unclear. Most of these (>90%) are benign variants and do not require specific work up or counseling or treatment.
NCCN Guidelines: Recommendations for Genetic Testing1
1. NCCN Guidelines for Prostate Cancer, V.2.2021. 2. Giri VN et al. J Clin Oncol. 2020;38(24):2798-2811.
Germline Testing Somatic Tumor Testing
• Germline genetic testing is recommended for patients with prostate cancer and any of the following:– High‐risk, very high‐risk, regional, or metastatic
prostate cancer
– Intermediate‐risk with intraductal/cribriform histology
– Ashkenazi Jewish ancestry
– Family history of high‐risk germline mutations (eg, BRCA1/2, Lynch mutation)
– A positive family history of cancer*
• Recommend evaluating tumor for alterations in homologous recombination DNA repair genes, such as BRCA1, BRCA2, ATM, PALB2, FANCA, RAD51D, CHEK2, and CDK12, in patients with metastatic prostate cancer
• Can be considered in men with regional prostate cancer
• Testing for MSI‐H or dMMR is recommended in patients with metastatic CRPC, and should be considered in patients with regional or castration‐naïve metastatic prostate cancer
• The International Philadelphia Prostate Cancer Consensus Conference 2019 guidelines recommended a similar germline testing strategy2
*A strong family history of prostate cancer consists of: Brother or father or multiple family members who were diagnosed with prostate cancer (but not clinically localized Grade Group 1) at <60 years of age or who died from prostate cancerOR≥3 cancers on same side of family, especially diagnoses ≤50 years of age: bile duct, breast, colorectal, endometrial, gastric, kidney, melanoma, ovarian, pancreatic, prostate (but notclinically localized Grade Group 1), small bowel, or urothelial cancer
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
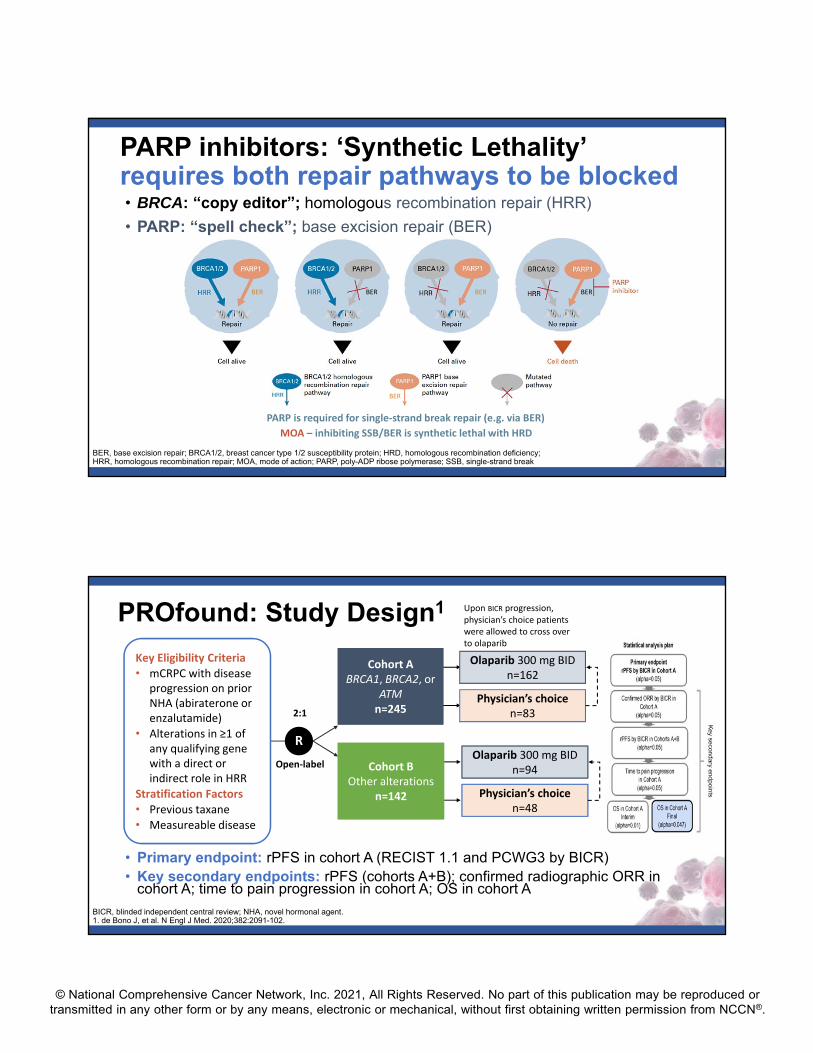
PARP is required for single‐strand break repair (e.g. via BER)
MOA – inhibiting SSB/BER is synthetic lethal with HRD
PARP inhibitors: ‘Synthetic Lethality’ requires both repair pathways to be blocked• BRCA: “copy editor”; homologous recombination repair (HRR)
• PARP: “spell check”; base excision repair (BER)
BER BERBER BER
BER
BER, base excision repair; BRCA1/2, breast cancer type 1/2 susceptibility protein; HRD, homologous recombination deficiency; HRR, homologous recombination repair; MOA, mode of action; PARP, poly-ADP ribose polymerase; SSB, single-strand break
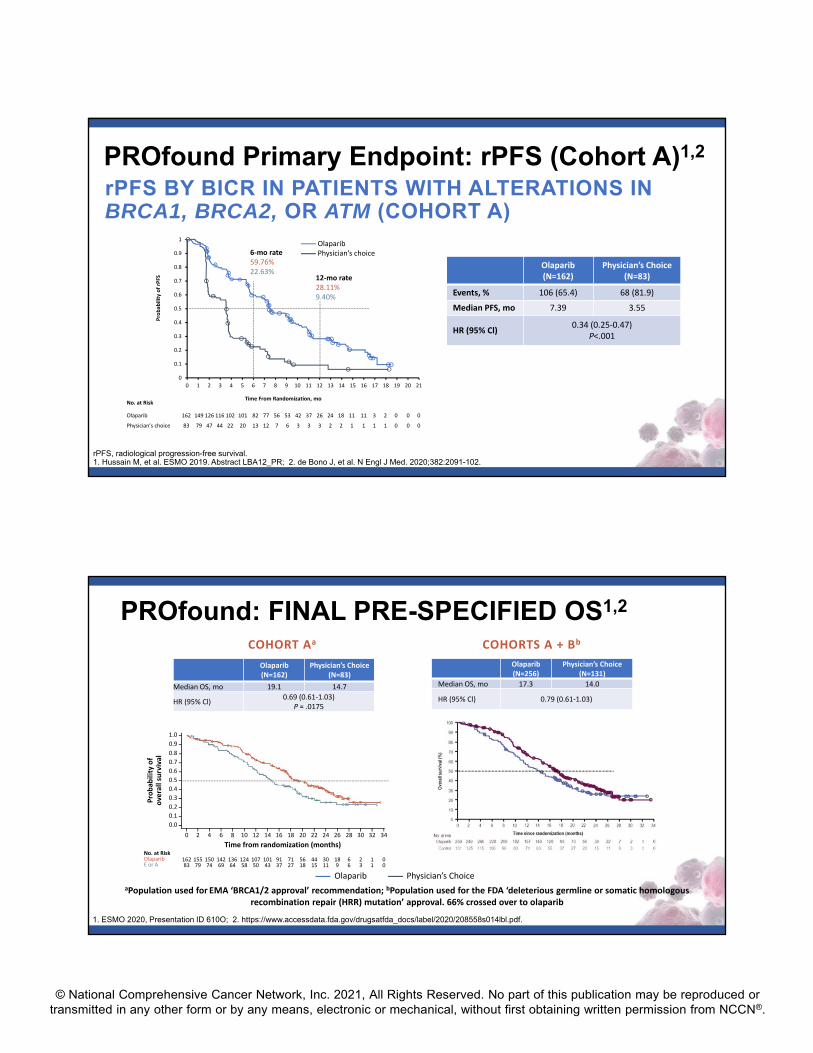
PROfound: Study Design1
• Primary endpoint: rPFS in cohort A (RECIST 1.1 and PCWG3 by BICR)• Key secondary endpoints: rPFS (cohorts A+B); confirmed radiographic ORR in
cohort A; time to pain progression in cohort A; OS in cohort A
Cohort ABRCA1, BRCA2, or
ATMn=245
Cohort ABRCA1, BRCA2, or
ATMn=245
Olaparib 300 mg BIDn=162
Cohort BOther alterations
n=142
Cohort BOther alterations
n=142
Olaparib 300 mg BIDn=94
R
2:1
Open‐label
Physician’s choicen=83
Physician’s choicen=48
Upon BICR progression, physician’s choice patients were allowed to cross over to olaparib
Key Eligibility Criteria
• mCRPC with disease progression on prior NHA (abiraterone or enzalutamide)
• Alterations in ≥1 of any qualifying gene with a direct or indirect role in HRR
Stratification Factors• Previous taxane
• Measureable disease
BICR, blinded independent central review; NHA, novel hormonal agent.1. de Bono J, et al. N Engl J Med. 2020;382:2091-102.

© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
PROfound: Patient Characteristics1
1. de Bono J, et al. N Engl J Med. 2020;382:2091-102.
Characteristics
Cohort A Cohorts A and B
Olaparib(N=162)
Control(N=83)
Olaparib(N=256)
Control(N=131)
Median age at randomization, y (range) 68 (47‐86) 67 (49‐86) 69 (47‐91) 69 (49‐87)
Age ≥65 y at randomization, n (%) 108 (67) 60 (72) 174 (68) 97 (74)
Metastatic disease at initial diagnosis, n (%)Missing data
38 (23)7 (4)
19 (23)4 (5)
66 (26)11 (4)
25 (19)7 (5)
Gleason score ≥8, n/total n (%) 105/157 (67) 54/80 (67) 183/251 (73) 95/127 (75)
Patients with alterations in a single gene, n (%)BRCA1BRCA2ATMCDK12
8 (5)80 (49)60 (37)N/A
5 (6)47 (57)24 (29)N/A
8 (3)81 (32)62 (24)61 (24)
5 (4)47 (36)24 (18)28 (21)
Median PSA at baseline (IQR), mcg/L62.2
(21.9‐280.4)112.9
(34.3‐317.1)68.2
(24.1‐294.4)106.5
(37.2‐326.6)
Measurable disease at baseline, n (%) 95 (59) 46 (55) 149 (58) 72 (55)
Characteristic
Cohort A Cohorts A and B
Olaparib(N=162)
Control(N=83)
Olaparib(N=256)
Control(N=131)
Metastases at baseline, n (%)Bone onlyVisceral: lung or liverOther
57 (35)46 (28)49 (30)
23 (28)32 (39)23 (28)
86 (34)68 (27)88 (34)
38 (29)44 (34)41 (31)
ECOG performance status, n (%)012Missing data
84 (52)67 (41) 11 (7)0
34 (41)46 (55)3 (4)0
131 (51)112 (44)13 (5)0
55 (42)71 (54)4 (3)1 (1)
Previous new hormonal agent, n (%)Enzalutamide only Abiraterone onlyEnzalutamide and abiraterone
68 (42)62 (38)32 (20)
40 (48)29 (35)14 (17)
105 (41)100 (39)51 (20)
54 (41)54 (41)23 (18)
Previous taxane use, n (%)Docetaxel onlyCabazitaxel onlyDocetaxel and cabazitaxelPaclitaxel only
106 (65)74 (46)2 (1)
29 (18)1 (<1)
52 (63)32 (49)
020 (24)
0
170 (66)115 (45)3 (1)
51 (20)1 (<1)
84 (64)58 (44)
026 (20)
0
1. de Bono J, et al. N Engl J Med. 2020;382:2091-102.
PROfound: Patient Characteristics1
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
Probab
ility of rPFS
Time From Randomization, mo
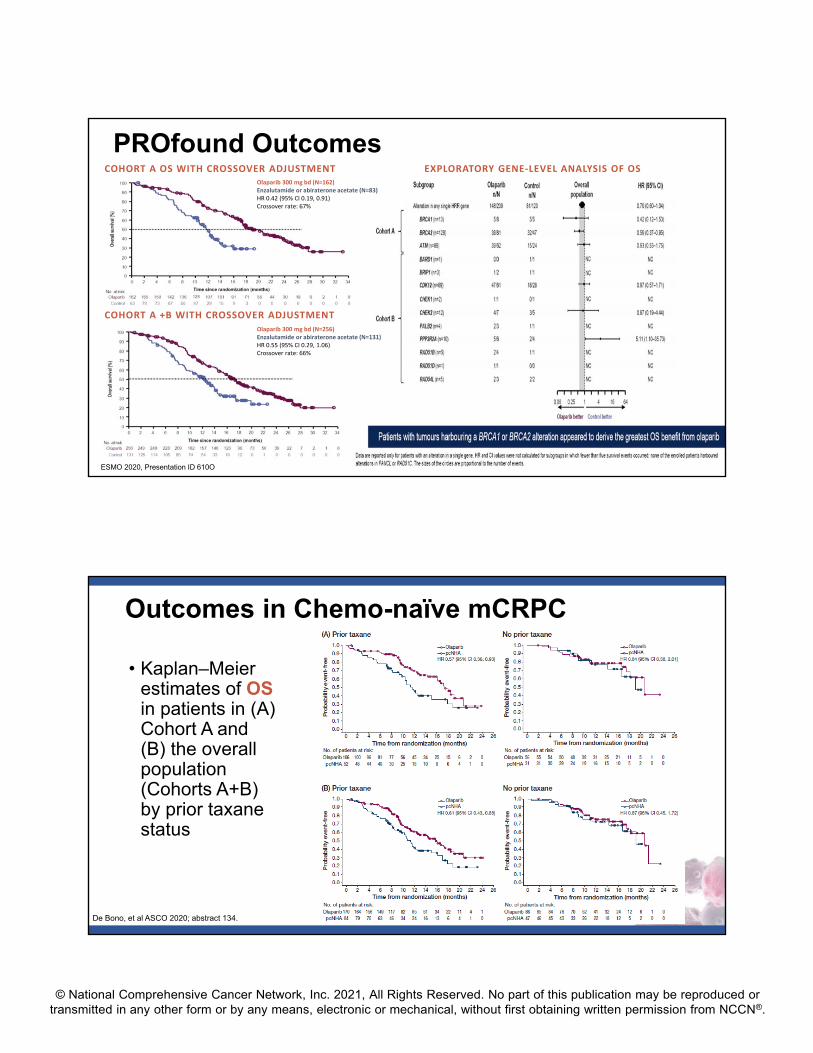
PROfound Primary Endpoint: rPFS (Cohort A)1,2
rPFS BY BICR IN PATIENTS WITH ALTERATIONS IN BRCA1, BRCA2, OR ATM (COHORT A)
rPFS, radiological progression-free survival.1. Hussain M, et al. ESMO 2019. Abstract LBA12_PR; 2. de Bono J, et al. N Engl J Med. 2020;382:2091-102.
No. at Risk
Olaparib 162 149 126 116 102 101 82 77 56 53 42 37 26 24 18 11 11 3 2 0 0 0
Physician’s choice 83 79 47 44 22 20 13 12 7 6 3 3 3 2 2 1 1 1 1 0 0 0
6‐mo rate59.76%22.63%
12‐mo rate28.11%9.40%
Olaparib(N=162)
Physician’s Choice(N=83)
Events, % 106 (65.4) 68 (81.9)
Median PFS, mo 7.39 3.55
HR (95% Cl)0.34 (0.25‐0.47)
P<.001
OlaparibPhysician’s choice
PROfound: FINAL PRE-SPECIFIED OS1,2
1. ESMO 2020, Presentation ID 610O; 2. https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/208558s014lbl.pdf.
Olaparib(N=162)
Physician’s Choice(N=83)
Median OS, mo 19.1 14.7
HR (95% Cl)0.69 (0.61‐1.03)
P = .0175
Olaparib(N=256)
Physician’s Choice(N=131)
Median OS, mo 17.3 14.0
HR (95% Cl) 0.79 (0.61‐1.03)
aPopulation used for EMA ‘BRCA1/2 approval’ recommendation; bPopulation used for the FDA ‘deleterious germline or somatic homologous recombination repair (HRR) mutation’ approval. 66% crossed over to olaparib
COHORT Aa COHORTS A + Bb
Olaparib Physician’s Choice
Probab
ility of
overall survival
Time from randomization (months)
0 2 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
0.0
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
4
No. at RiskOlaparibE or A
16283
15579
14269
13664
12458
10750
10143
9137
7127
5618
4415
3011
189
66
23
11
00
15074
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
PROfound Outcomes
ESMO 2020, Presentation ID 610O
COHORT A +B WITH CROSSOVER ADJUSTMENT
COHORT A OS WITH CROSSOVER ADJUSTMENT EXPLORATORY GENE‐LEVEL ANALYSIS OF OSOlaparib 300 mg bd (N=162)Enzalutamide or abiraterone acetate (N=83)HR 0.42 (95% CI 0.19, 0.91)Crossover rate: 67%
Olaparib 300 mg bd (N=256)Enzalutamide or abiraterone acetate (N=131)HR 0.55 (95% CI 0.29, 1.06)Crossover rate: 66%
Outcomes in Chemo-naïve mCRPC
De Bono, et al ASCO 2020; abstract 134.
• Kaplan–Meier estimates of OSin patients in (A) Cohort A and (B) the overall population (Cohorts A+B) by prior taxanestatus
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
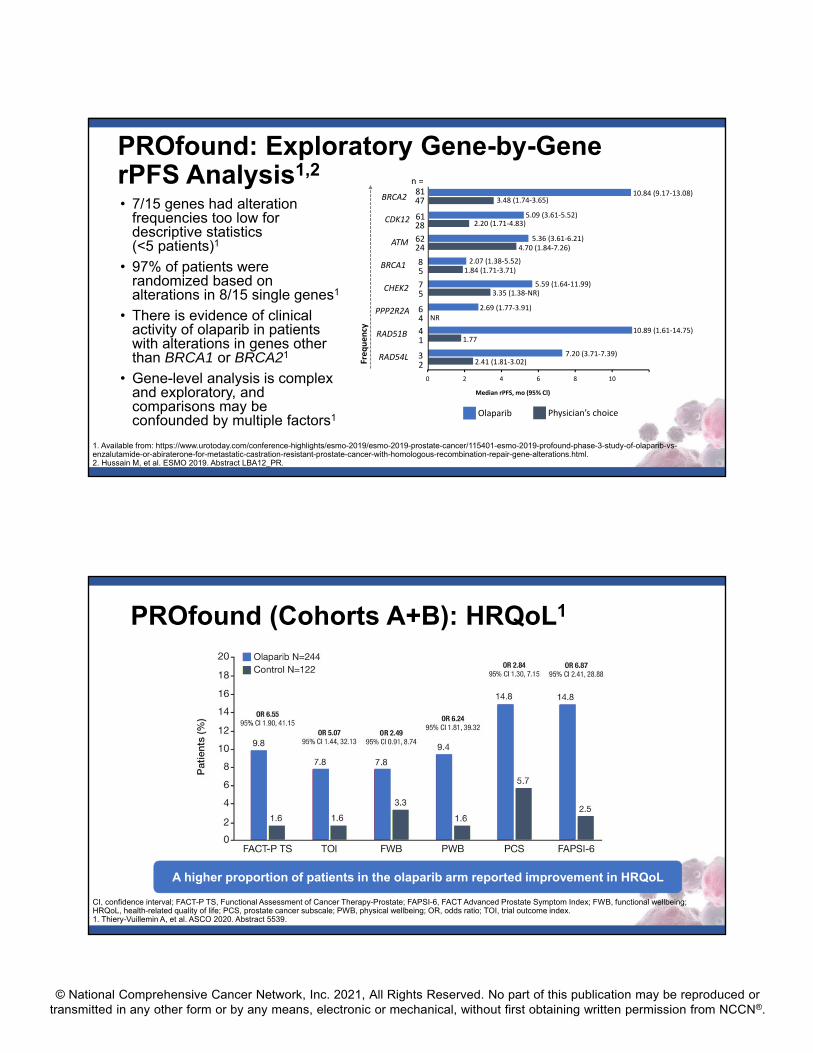
PROfound: Exploratory Gene-by-Gene rPFS Analysis1,2
• 7/15 genes had alteration frequencies too low for descriptive statistics (<5 patients)1
• 97% of patients were randomized based on alterations in 8/15 single genes1
• There is evidence of clinical activity of olaparib in patients with alterations in genes other than BRCA1 or BRCA21
• Gene-level analysis is complex and exploratory, and comparisons may be confounded by multiple factors1
1. Available from: https://www.urotoday.com/conference-highlights/esmo-2019/esmo-2019-prostate-cancer/115401-esmo-2019-profound-phase-3-study-of-olaparib-vs-enzalutamide-or-abiraterone-for-metastatic-castration-resistant-prostate-cancer-with-homologous-recombination-repair-gene-alterations.html.2. Hussain M, et al. ESMO 2019. Abstract LBA12_PR.
0 2 4 6 8 10
Median rPFS, mo (95% Cl)
n =8147
6128
6224
85
57
46
14
23
BRCA2
CDK12
ATM
BRCA1
CHEK2
PPP2R2A
RAD51B
RAD54LFrequen
cy
Olaparib Physician’s choice
10.84 (9.17‐13.08)3.48 (1.74‐3.65)
5.09 (3.61‐5.52)2.20 (1.71‐4.83)
5.36 (3.61‐6.21)4.70 (1.84‐7.26)
2.07 (1.38‐5.52)1.84 (1.71‐3.71)
5.59 (1.64‐11.99)3.35 (1.38‐NR)
2.69 (1.77‐3.91)
NR
10.89 (1.61‐14.75)1.77
7.20 (3.71‐7.39)2.41 (1.81‐3.02)
PROfound (Cohorts A+B): HRQoL1
CI, confidence interval; FACT-P TS, Functional Assessment of Cancer Therapy-Prostate; FAPSI-6, FACT Advanced Prostate Symptom Index; FWB, functional wellbeing; HRQoL, health-related quality of life; PCS, prostate cancer subscale; PWB, physical wellbeing; OR, odds ratio; TOI, trial outcome index.1. Thiery-Vuillemin A, et al. ASCO 2020. Abstract 5539.
A higher proportion of patients in the olaparib arm reported improvement in HRQoL
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
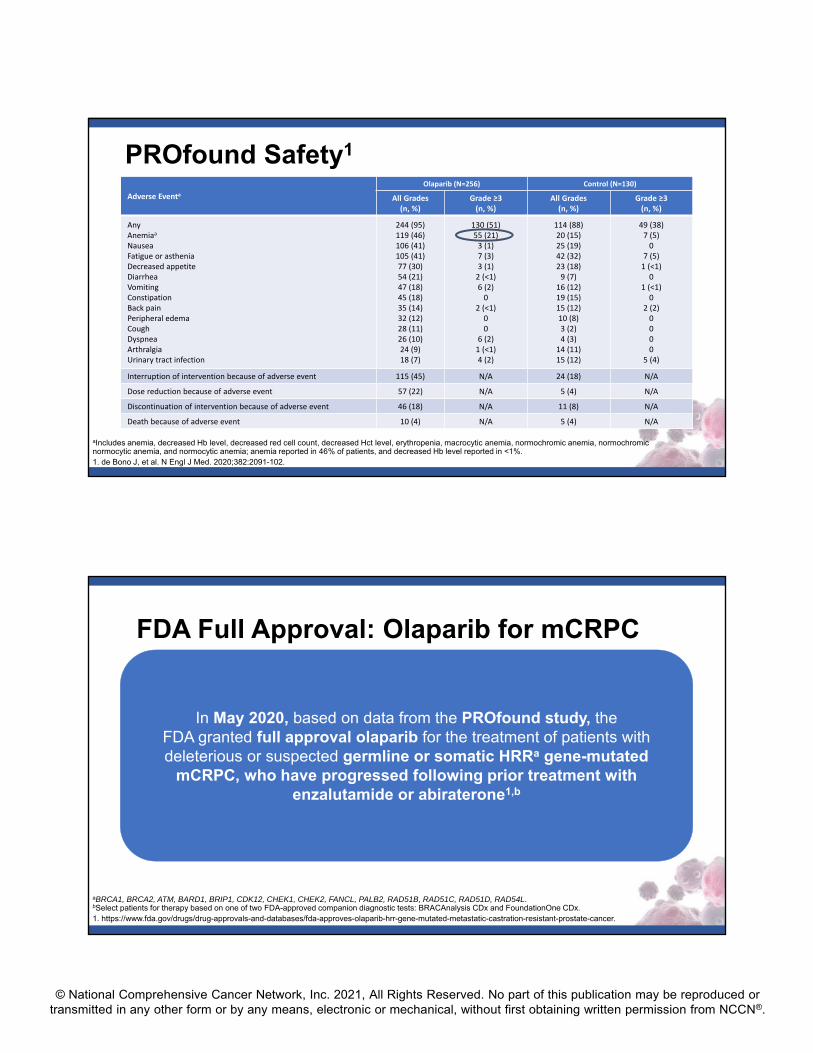
PROfound Safety1
aIncludes anemia, decreased Hb level, decreased red cell count, decreased Hct level, erythropenia, macrocytic anemia, normochromic anemia, normochromic normocytic anemia, and normocytic anemia; anemia reported in 46% of patients, and decreased Hb level reported in <1%.1. de Bono J, et al. N Engl J Med. 2020;382:2091-102.
Adverse EventaOlaparib (N=256) Control (N=130)
All Grades (n, %)
Grade ≥3 (n, %)
All Grades (n, %)
Grade ≥3 (n, %)
AnyAnemiaa
NauseaFatigue or astheniaDecreased appetiteDiarrheaVomitingConstipationBack pain Peripheral edemaCough DyspneaArthralgiaUrinary tract infection
244 (95)119 (46)106 (41)105 (41)77 (30)54 (21)47 (18)45 (18)35 (14)32 (12)28 (11)26 (10)24 (9)18 (7)
130 (51)55 (21)3 (1)7 (3)3 (1)2 (<1)6 (2)0
2 (<1)00
6 (2)1 (<1)4 (2)
114 (88)20 (15)25 (19)42 (32)23 (18)9 (7)
16 (12)19 (15)15 (12)10 (8)3 (2)4 (3)
14 (11)15 (12)
49 (38)7 (5)0
7 (5)1 (<1)0
1 (<1)0
2 (2)0000
5 (4)
Interruption of intervention because of adverse event 115 (45) N/A 24 (18) N/A
Dose reduction because of adverse event 57 (22) N/A 5 (4) N/A
Discontinuation of intervention because of adverse event 46 (18) N/A 11 (8) N/A
Death because of adverse event 10 (4) N/A 5 (4) N/A
FDA Full Approval: Olaparib for mCRPC
aBRCA1, BRCA2, ATM, BARD1, BRIP1, CDK12, CHEK1, CHEK2, FANCL, PALB2, RAD51B, RAD51C, RAD51D, RAD54L. bSelect patients for therapy based on one of two FDA-approved companion diagnostic tests: BRACAnalysis CDx and FoundationOne CDx.1. https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-olaparib-hrr-gene-mutated-metastatic-castration-resistant-prostate-cancer.
In May 2020, based on data from the PROfound study, the FDA granted full approval olaparib for the treatment of patients with deleterious or suspected germline or somatic HRRa gene-mutated
mCRPC, who have progressed following prior treatment with enzalutamide or abiraterone1,b
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
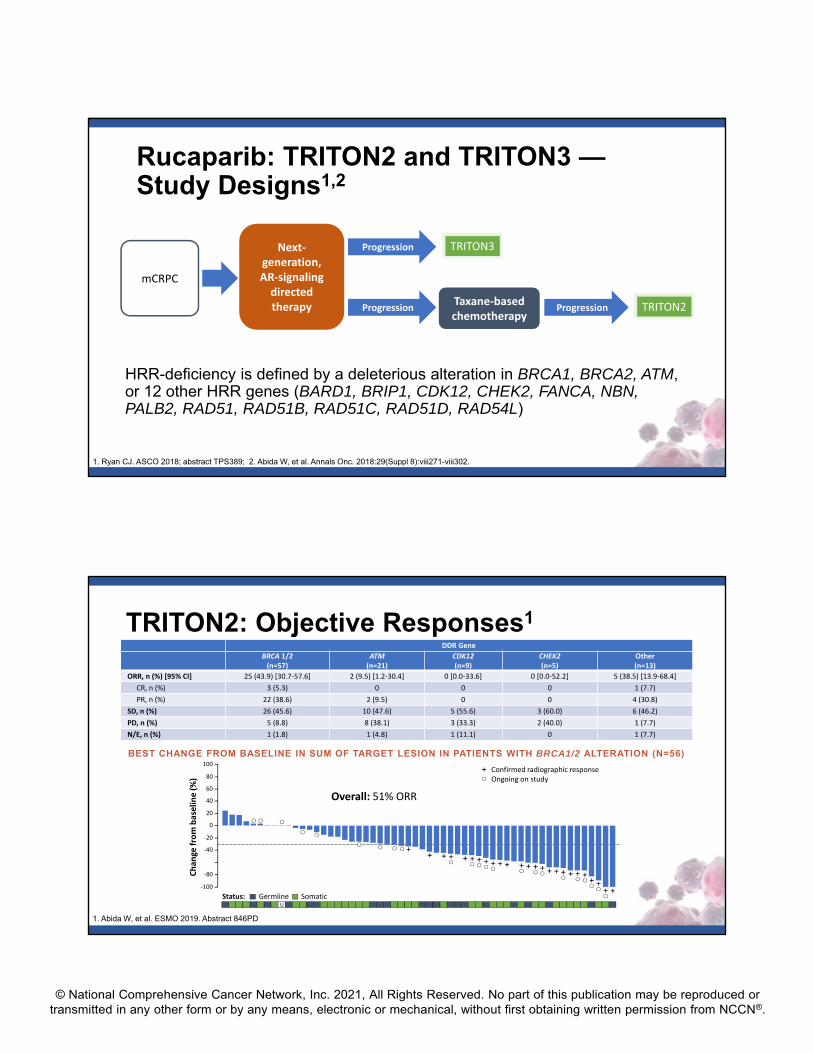
Rucaparib: TRITON2 and TRITON3 —Study Designs1,2
HRR-deficiency is defined by a deleterious alteration in BRCA1, BRCA2, ATM, or 12 other HRR genes (BARD1, BRIP1, CDK12, CHEK2, FANCA, NBN, PALB2, RAD51, RAD51B, RAD51C, RAD51D, RAD54L)
1. Ryan CJ. ASCO 2018; abstract TPS389; 2. Abida W, et al. Annals Onc. 2018:29(Suppl 8):viii271-viii302.
mCRPC
Progression
Progression
Next‐generation, AR‐signaling directed therapy
TRITON3
Taxane‐based chemotherapy
Progression TRITON2
TRITON2: Objective Responses1
1. Abida W, et al. ESMO 2019. Abstract 846PD
DDR Gene
BRCA 1/2 (n=57)
ATM (n=21)
CDK12(n=9)
CHEK2(n=5)
Other(n=13)
ORR, n (%) [95% CI] 25 (43.9) [30.7‐57.6] 2 (9.5) [1.2‐30.4] 0 [0.0‐33.6] 0 [0.0‐52.2] 5 (38.5) [13.9‐68.4]
CR, n (%) 3 (5.3) 0 0 0 1 (7.7)
PR, n (%) 22 (38.6) 2 (9.5) 0 0 4 (30.8)
SD, n (%) 26 (45.6) 10 (47.6) 5 (55.6) 3 (60.0) 6 (46.2)
PD, n (%) 5 (8.8) 8 (38.1) 3 (33.3) 2 (40.0) 1 (7.7)
N/E, n (%) 1 (1.8) 1 (4.8) 1 (11.1) 0 1 (7.7)
BEST CHANGE FROM BASELINE IN SUM OF TARGET LESION IN PATIENTS WITH BRCA1/2 ALTERATION (N=56)
‐100
Chan
ge from baselin
e (%)
40
0
‐20
‐40
‐80
Status:
20
60
100
80Confirmed radiographic responseOngoing on study
Germline SomaticU
Overall: 51% ORR
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
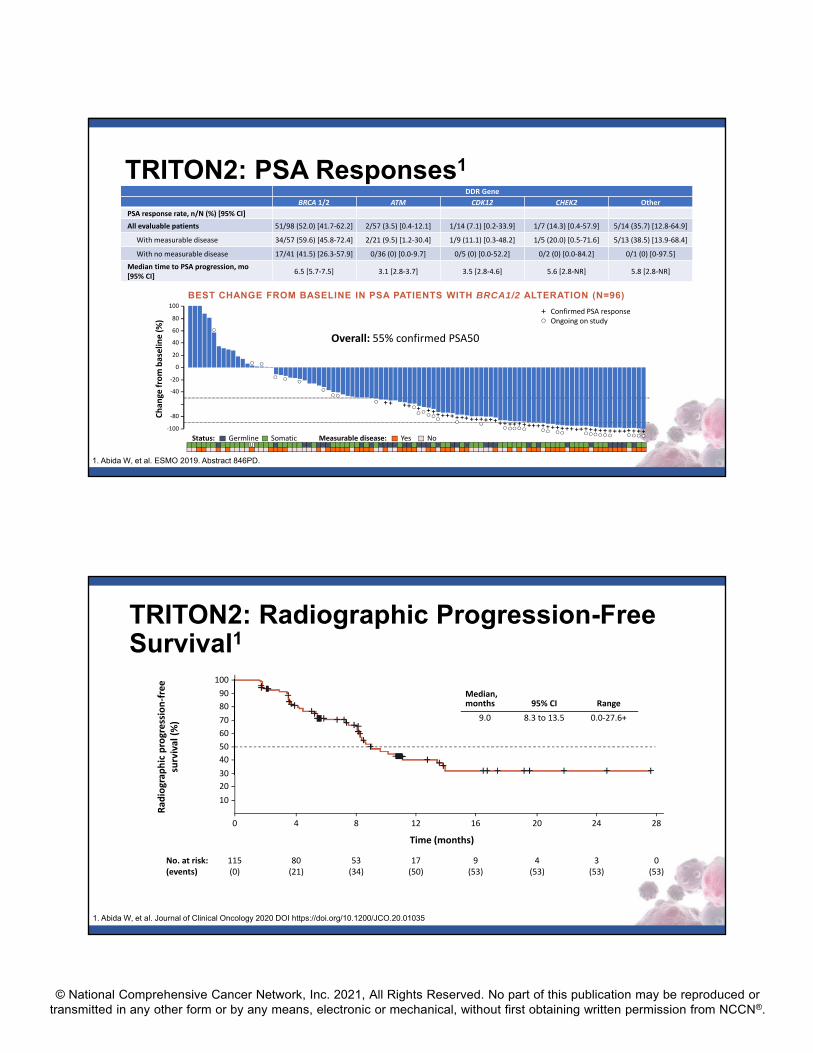
TRITON2: PSA Responses1
1. Abida W, et al. ESMO 2019. Abstract 846PD.
DDR Gene
BRCA 1/2 ATM CDK12 CHEK2 Other
PSA response rate, n/N (%) [95% CI]
All evaluable patients 51/98 (52.0) [41.7‐62.2] 2/57 (3.5) [0.4‐12.1] 1/14 (7.1) [0.2‐33.9] 1/7 (14.3) [0.4‐57.9] 5/14 (35.7) [12.8‐64.9]
With measurable disease 34/57 (59.6) [45.8‐72.4] 2/21 (9.5) [1.2‐30.4] 1/9 (11.1) [0.3‐48.2] 1/5 (20.0) [0.5‐71.6] 5/13 (38.5) [13.9‐68.4]
With no measurable disease 17/41 (41.5) [26.3‐57.9] 0/36 (0) [0.0‐9.7] 0/5 (0) [0.0‐52.2] 0/2 (0) [0.0‐84.2] 0/1 (0) [0‐97.5]
Median time to PSA progression, mo [95% CI]
6.5 [5.7‐7.5] 3.1 [2.8‐3.7] 3.5 [2.8‐4.6] 5.6 [2.8‐NR] 5.8 [2.8‐NR]
BEST CHANGE FROM BASELINE IN PSA PATIENTS WITH BRCA1/2 ALTERATION (N=96)
‐100
Chan
ge from baselin
e (%)
40
0
‐20
‐40
‐80
Status:
20
60
100
80Confirmed PSA responseOngoing on study
Germline Somatic Measurable disease: Yes NoU
Overall: 55% confirmed PSA50
TRITON2: Radiographic Progression-Free Survival1
1. Abida W, et al. Journal of Clinical Oncology 2020 DOI https://doi.org/10.1200/JCO.20.01035
20
Time (months)
10
30
40
50
60
70
80
90
100
40 8 12 16 20 24 28
80(21)
115(0)
53(34)
17(50)
9(53)
4(53)
3(53)
0(53)
No. at risk:(events)
Rad
iograp
hic progression‐free
survival (%)
Median,months 95% CI Range
9.0 8.3 to 13.5 0.0‐27.6+
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
Common Side Effects of Rucaparib
1. Abida W, et al. Clin Cancer Res. 2020 Feb 21 [Epub ahead of print]; 2. Rucabra. SmPC. May 2019.
Anemia
Fatigue, asthenia
Nausea/vomiting
Decreased appetite
Diarrhea or constipation
Thrombocytopenia
Increased AST/ALT and/or creatinine
Rash
Rare but serious: MDS/AML; fetal teratogenicity
The TRITON3 study is underway and recruiting patients withmCRPC and homologous recombination gene deficiency.2
FDA accelerated approval: Rucaparib for mCRPC
1. https://www.fda.gov/drugs/fda-grants-accelerated-approval-rucaparib-brca-mutated-metastatic-castration-resistant-prostate. 2. https://clinicaltrials.gov/ct2/show/NCT02975934.
In May 2020, based on data from the TRITON2 study, the FDAgranted accelerated approval to rucaparib for the treatment of patients with
deleterious BRCA1/2 (germline and/or somatic)-associated mCRPC, who have been treated with an androgen receptor-directed therapy and
a taxane-based chemotherapy.1

© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
© 2021 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN®. To view the most recent and complete version of the NCCN Guidelines, go online to NCCN.org.
• 74 yo WM presents with a PSA of 424 and back pain to his local urologist, biopsy shows GG5 disease pathologic RP nodes
• Treated initially for low volume mHSPC with ADT plus abiraterone acetate with a 9 mo response, PSA drops to 0.3, and adenopathy resolves
• Over subsequent year, PSA rises to 6.0 and he presents to local ER with a seizure and brief aphasia, found to have a new left frontal lobe metastasis, enlarging RP adenopathy
• Surgical resection of CNS metastasis confirms prostate adenocarcinoma, no evidence of NEPC. Profiling of tumor shows an MSH2 splice site pathogenic mutation, MSI-high disease, and TMB of 42/MB, multiple other mutations
• Treatment with CNS radiation postop
• He has significant baseline neuropathy (grade 2) from underlying diabetes
Case 2
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
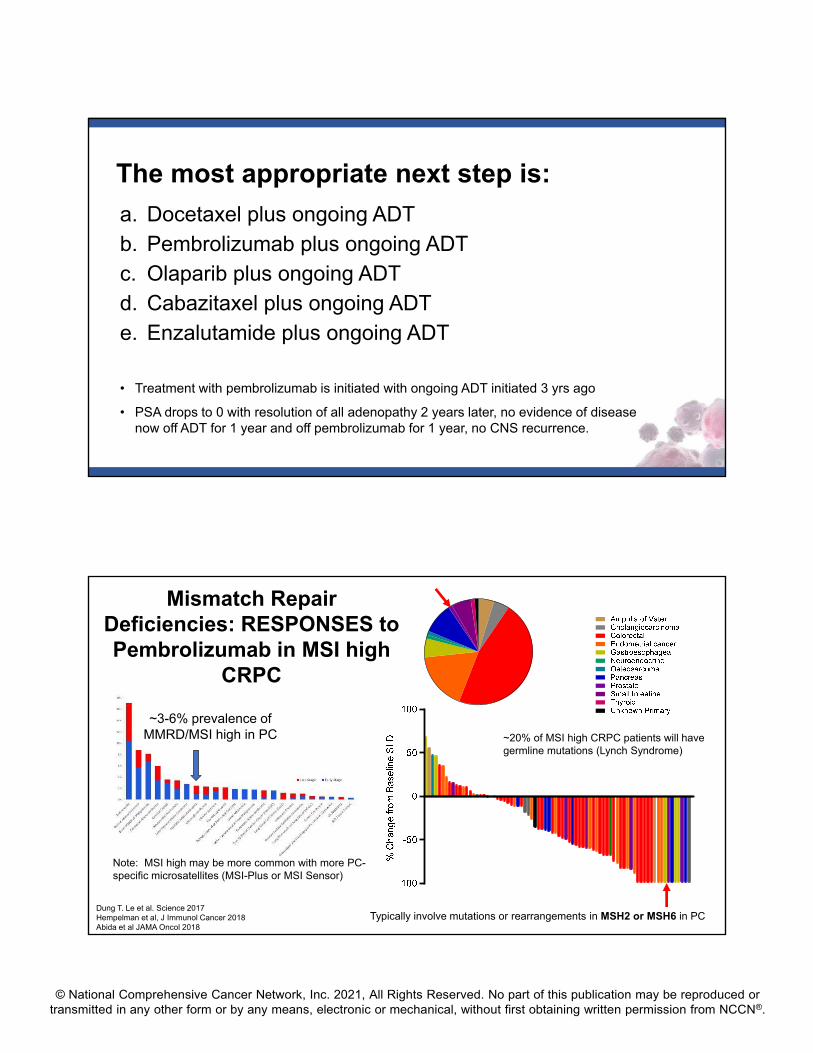
The most appropriate next step is:
a. Docetaxel plus ongoing ADTb. Pembrolizumab plus ongoing ADTc. Olaparib plus ongoing ADTd. Cabazitaxel plus ongoing ADTe. Enzalutamide plus ongoing ADT
• Treatment with pembrolizumab is initiated with ongoing ADT initiated 3 yrs ago
• PSA drops to 0 with resolution of all adenopathy 2 years later, no evidence of disease now off ADT for 1 year and off pembrolizumab for 1 year, no CNS recurrence.
Dung T. Le et al. Science 2017Hempelman et al, J Immunol Cancer 2018Abida et al JAMA Oncol 2018
~3-6% prevalence of MMRD/MSI high in PC
Typically involve mutations or rearrangements in MSH2 or MSH6 in PC
Mismatch Repair Deficiencies: RESPONSES to Pembrolizumab in MSI high
CRPC
Note: MSI high may be more common with more PC-specific microsatellites (MSI-Plus or MSI Sensor)
~20% of MSI high CRPC patients will have germline mutations (Lynch Syndrome)
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
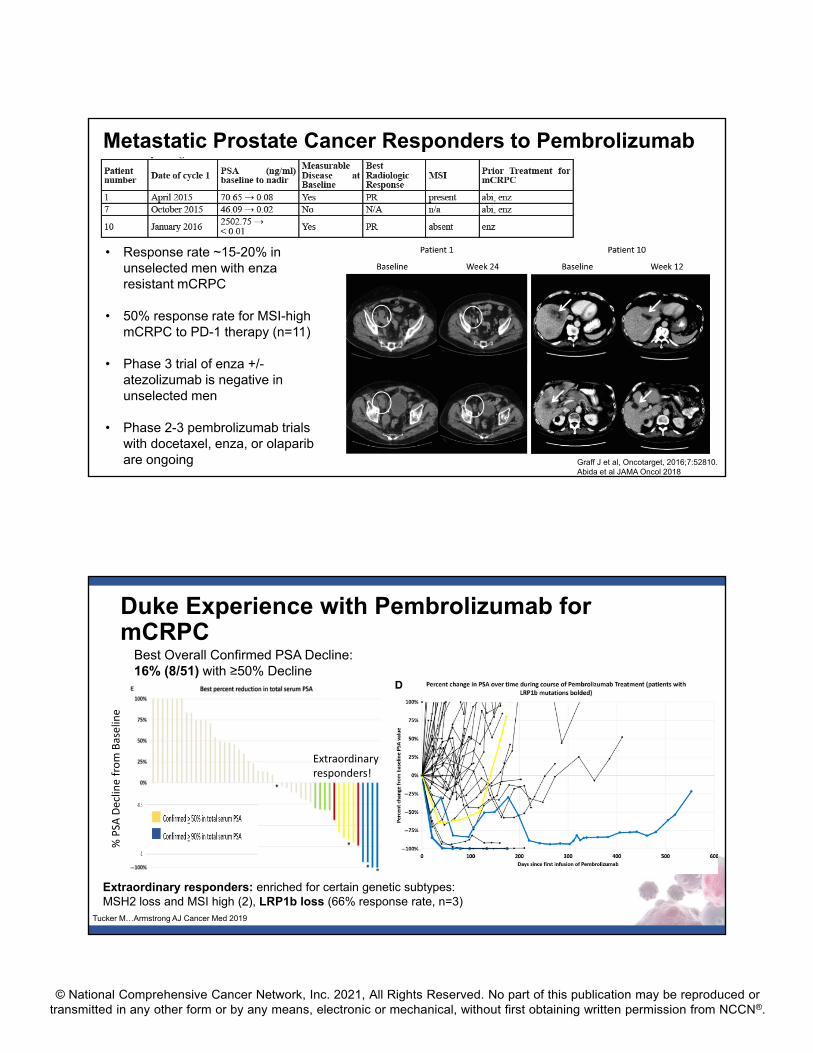
Metastatic Prostate Cancer Responders to Pembrolizumab
Graff J et al, Oncotarget, 2016;7:52810.Abida et al JAMA Oncol 2018
• Response rate ~15-20% in unselected men with enzaresistant mCRPC
• 50% response rate for MSI-high mCRPC to PD-1 therapy (n=11)
• Phase 3 trial of enza +/-atezolizumab is negative in unselected men
• Phase 2-3 pembrolizumab trials with docetaxel, enza, or olaparibare ongoing
Duke Experience with Pembrolizumab for mCRPC
Best Overall Confirmed PSA Decline: 16% (8/51) with ≥50% Decline
% PSA
Decline from Baselin
e
Extraordinary responders: enriched for certain genetic subtypes: MSH2 loss and MSI high (2), LRP1b loss (66% response rate, n=3)
Tucker M…Armstrong AJ Cancer Med 2019
Extraordinary responders!
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
Case 3: Symptomatic mCRPC post abiraterone
• 73 y/o male first diagnosed four years ago with a PSA of 9 ng/mL
• Prostatectomy identified a 3+4 adenocarcinoma pT2CN0
• Biochemical recurrence in 6 months and treated with salvage XRT
• Began ADT one year later due to rising PSA and increasing pelvic LAD
• Developed CRPC after 2 years with progressive bone metastases and enlarging LAD to 5cm
• Treated with abiraterone for 6 months before progression
• Patient received 6 cycles of docetaxel before taking an 8 week treatment break.
• Now with PSA progression and recurrent symptoms of bone pain.
• Imaging modalities performed• Bone Scan: 3 new lesions in femur, pelvis and T10
• CT Scan: Initial response in pelvic LAD no longer present with disease progression and increased size of dominant node to 5.3cm
Case 3: Symptomatic mCRPC post docetaxel
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
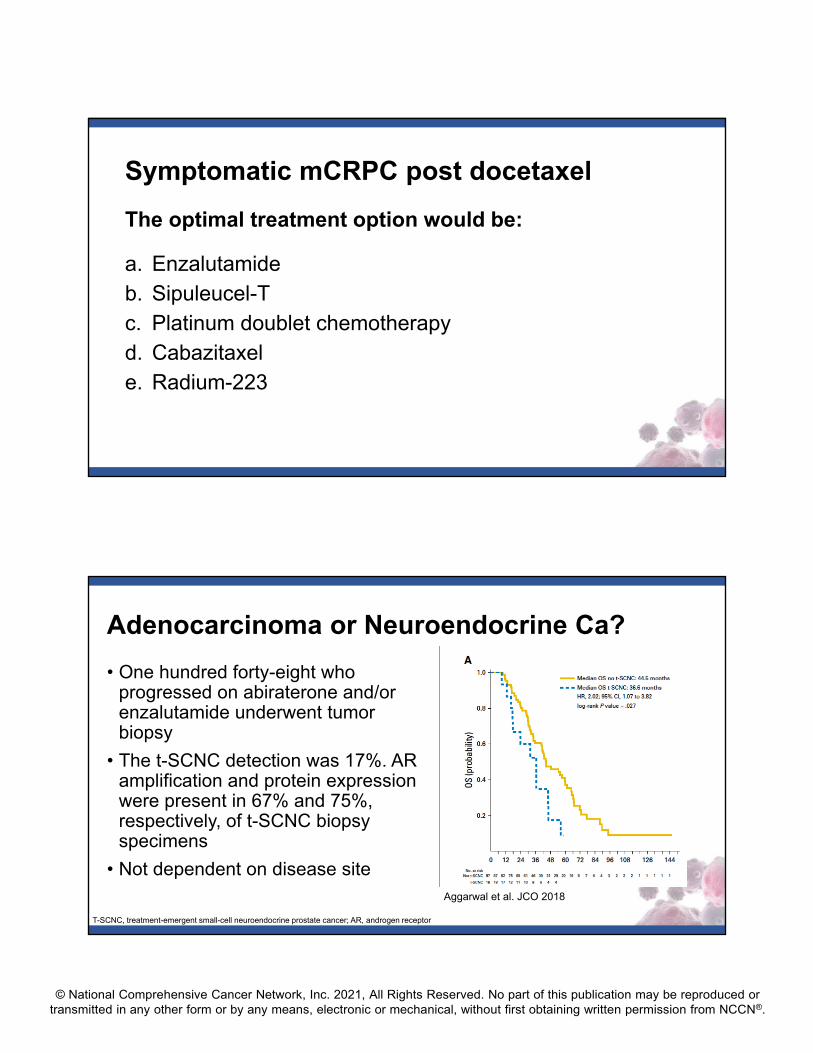
Symptomatic mCRPC post docetaxel
The optimal treatment option would be:
a. Enzalutamideb. Sipuleucel-Tc. Platinum doublet chemotherapyd. Cabazitaxele. Radium-223
Adenocarcinoma or Neuroendocrine Ca?
• One hundred forty-eight who progressed on abiraterone and/or enzalutamide underwent tumor biopsy
• The t-SCNC detection was 17%. AR amplification and protein expression were present in 67% and 75%, respectively, of t-SCNC biopsy specimens
• Not dependent on disease siteAggarwal et al. JCO 2018
T-SCNC, treatment-emergent small-cell neuroendocrine prostate cancer; AR, androgen receptor

© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
Cabazitaxel
• Semi-synthetic taxane
• Preclinical data• As potent as docetaxel against sensitive cell lines and tumor
models• Activity against tumor cells and tumor models that are
resistant to, or not sensitive to, currently available taxanes
• Clinical data• In Phase I trials, DLT was neutropenia • Antitumor activity in mCRPC in Phase I trials including
docetaxel-resistant disease
TROPIC: Phase III Study 146 Sites
Cabazitaxel 25 mg/m² q 3 wk+ prednisone* for 10 cycles
(n = 378)
Mitoxantrone 12 mg/m² q 3 wk+ prednisone* for 10 cycles
(n = 377)
*Oral prednisone/prednisolone: 10 mg daily.
Stratification factorsECOG PS (0, 1 vs. 2) • Measurable vs. non-measurable disease
mCRPC patients who progressed during and after treatment with a docetaxel-
based regimen (N = 755)
de Bono JS, Oudard S, Ozguroglu M, et al. Lancet. 2010
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
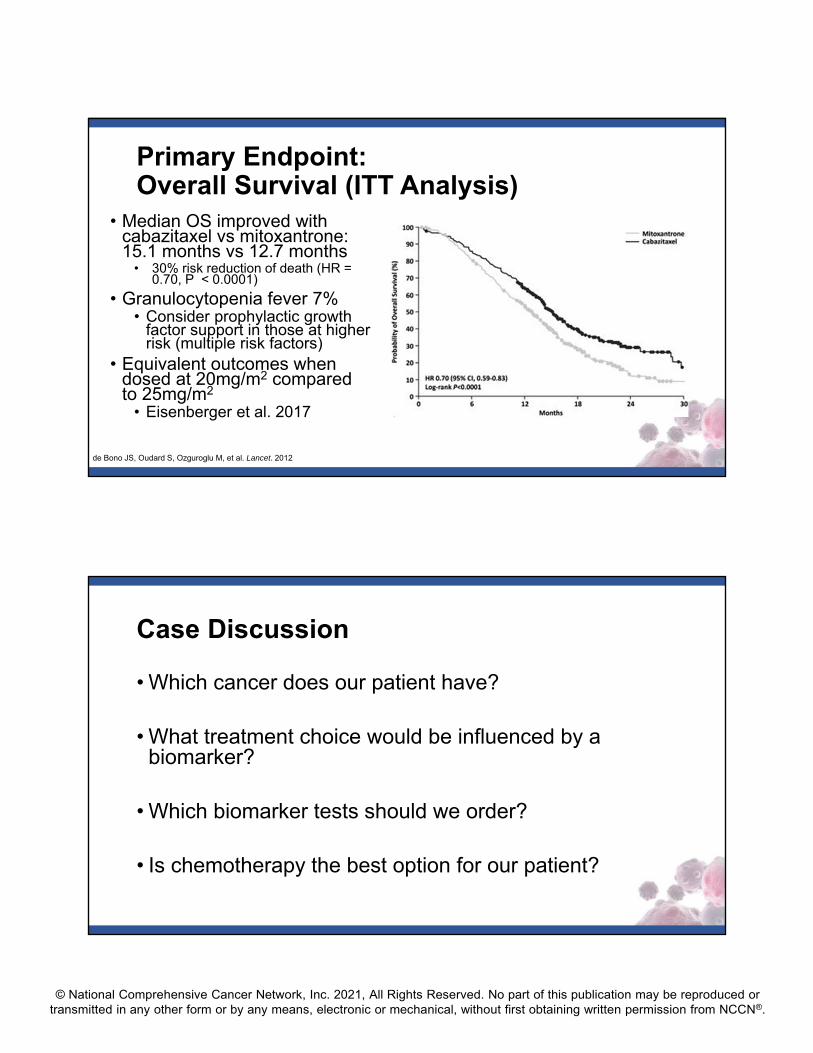
Primary Endpoint: Overall Survival (ITT Analysis)
• Median OS improved with cabazitaxel vs mitoxantrone: 15.1 months vs 12.7 months
• 30% risk reduction of death (HR = 0.70, P < 0.0001)
• Granulocytopenia fever 7%• Consider prophylactic growth
factor support in those at higher risk (multiple risk factors)
• Equivalent outcomes when dosed at 20mg/m2 compared to 25mg/m2
• Eisenberger et al. 2017
de Bono JS, Oudard S, Ozguroglu M, et al. Lancet. 2012
Case Discussion
• Which cancer does our patient have?
• What treatment choice would be influenced by a biomarker?
• Which biomarker tests should we order?
• Is chemotherapy the best option for our patient?
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
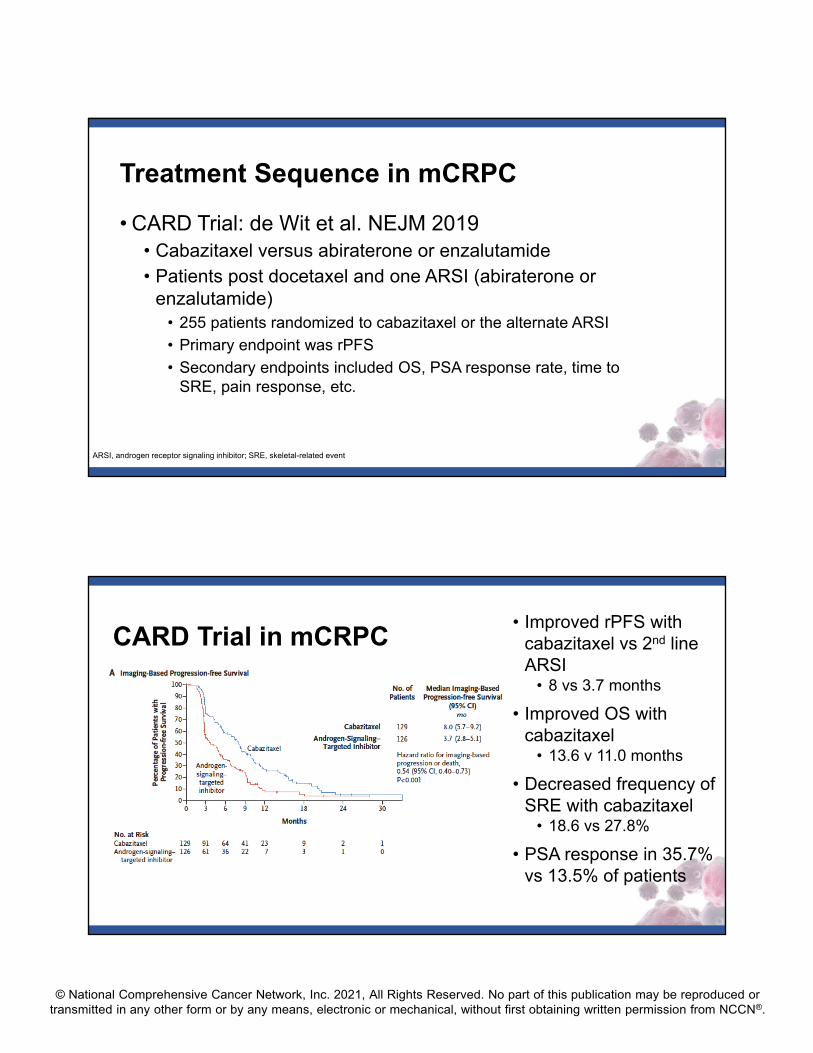
Treatment Sequence in mCRPC
• CARD Trial: de Wit et al. NEJM 2019• Cabazitaxel versus abiraterone or enzalutamide• Patients post docetaxel and one ARSI (abiraterone or
enzalutamide)• 255 patients randomized to cabazitaxel or the alternate ARSI
• Primary endpoint was rPFS
• Secondary endpoints included OS, PSA response rate, time to SRE, pain response, etc.
ARSI, androgen receptor signaling inhibitor; SRE, skeletal-related event
CARD Trial in mCRPC • Improved rPFS with
cabazitaxel vs 2nd line ARSI
• 8 vs 3.7 months
• Improved OS with cabazitaxel
• 13.6 v 11.0 months
• Decreased frequency of SRE with cabazitaxel
• 18.6 vs 27.8%
• PSA response in 35.7% vs 13.5% of patients
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
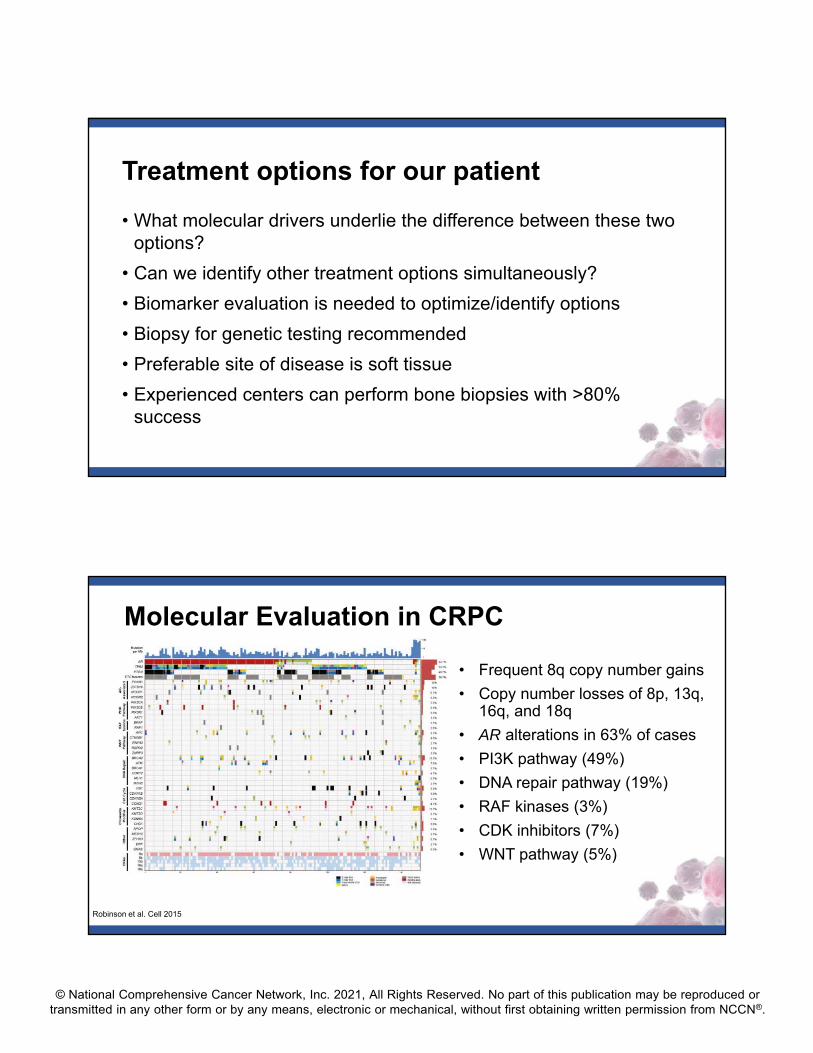
Treatment options for our patient
• What molecular drivers underlie the difference between these two options?
• Can we identify other treatment options simultaneously?
• Biomarker evaluation is needed to optimize/identify options
• Biopsy for genetic testing recommended
• Preferable site of disease is soft tissue
• Experienced centers can perform bone biopsies with >80% success
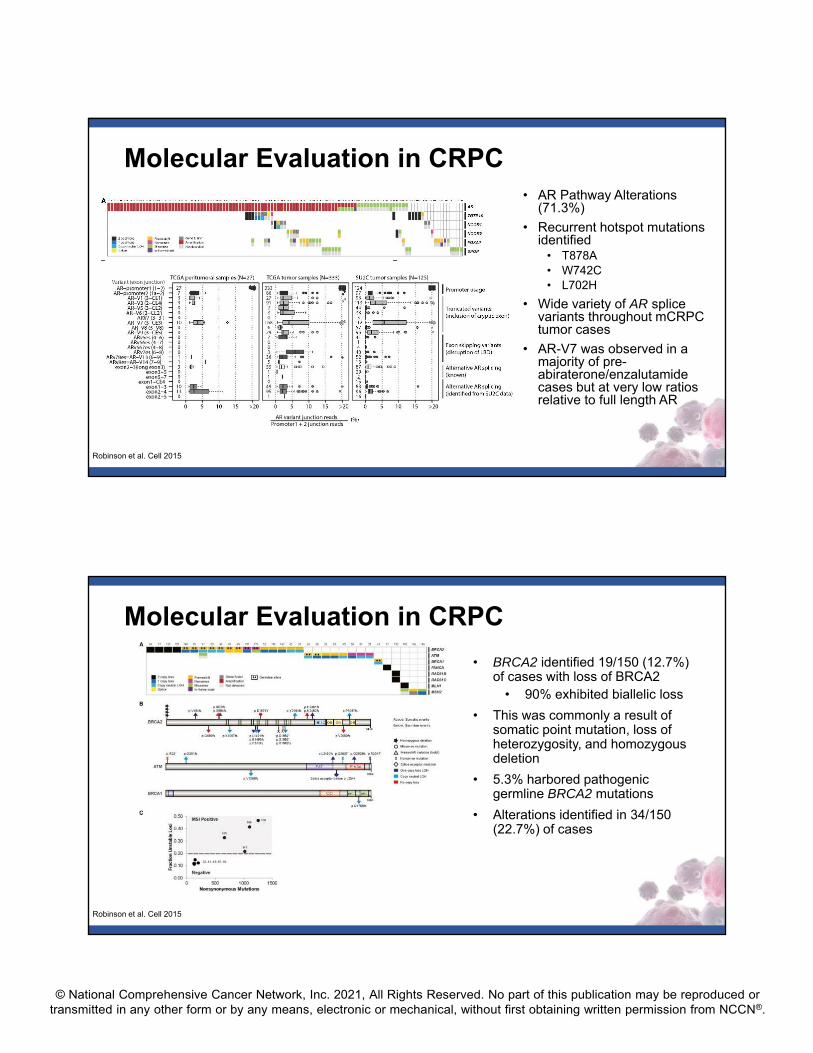
Robinson et al. Cell 2015
• Frequent 8q copy number gains
• Copy number losses of 8p, 13q, 16q, and 18q
• AR alterations in 63% of cases
• PI3K pathway (49%)
• DNA repair pathway (19%)
• RAF kinases (3%)
• CDK inhibitors (7%)
• WNT pathway (5%)
Molecular Evaluation in CRPC
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
• AR Pathway Alterations (71.3%)
• Recurrent hotspot mutations identified
• T878A• W742C• L702H
• Wide variety of AR splice variants throughout mCRPCtumor cases
• AR-V7 was observed in a majority of pre-abiraterone/enzalutamide cases but at very low ratios relative to full length AR
Molecular Evaluation in CRPC
Robinson et al. Cell 2015
• BRCA2 identified 19/150 (12.7%) of cases with loss of BRCA2
• 90% exhibited biallelic loss
• This was commonly a result of somatic point mutation, loss of heterozygosity, and homozygous deletion
• 5.3% harbored pathogenic germline BRCA2 mutations
• Alterations identified in 34/150 (22.7%) of cases
Molecular Evaluation in CRPC
Robinson et al. Cell 2015
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
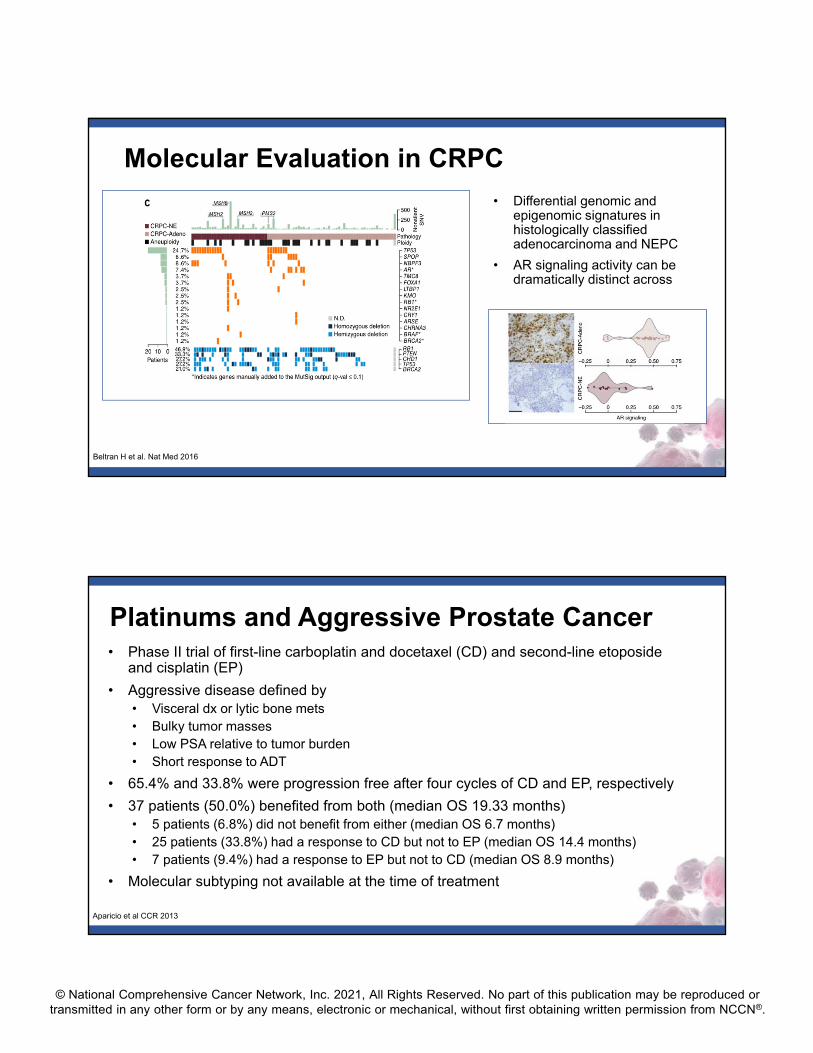
• Differential genomic and epigenomic signatures in histologically classified adenocarcinoma and NEPC
• AR signaling activity can be dramatically distinct across
Beltran H et al. Nat Med 2016
Molecular Evaluation in CRPC
• Phase II trial of first-line carboplatin and docetaxel (CD) and second-line etoposide and cisplatin (EP)
• Aggressive disease defined by • Visceral dx or lytic bone mets• Bulky tumor masses• Low PSA relative to tumor burden• Short response to ADT
• 65.4% and 33.8% were progression free after four cycles of CD and EP, respectively
• 37 patients (50.0%) benefited from both (median OS 19.33 months) • 5 patients (6.8%) did not benefit from either (median OS 6.7 months)• 25 patients (33.8%) had a response to CD but not to EP (median OS 14.4 months)• 7 patients (9.4%) had a response to EP but not to CD (median OS 8.9 months)
• Molecular subtyping not available at the time of treatment
Platinums and Aggressive Prostate Cancer
Aparicio et al CCR 2013
© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
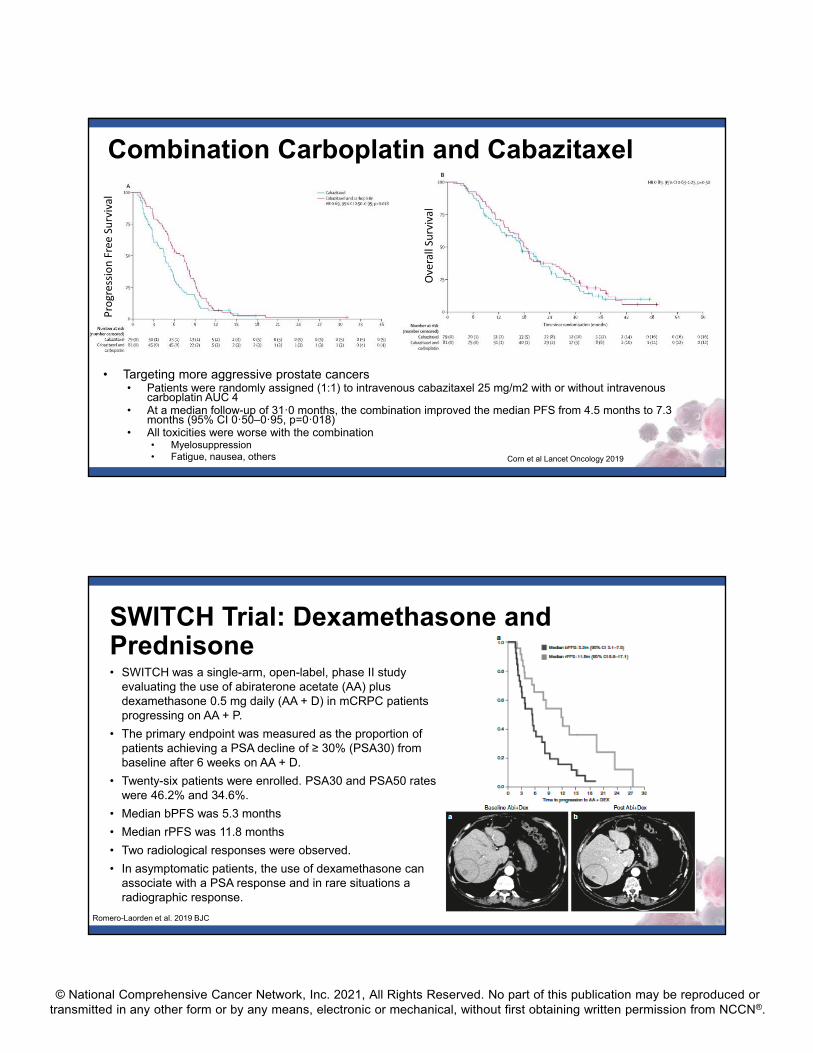
• Targeting more aggressive prostate cancers• Patients were randomly assigned (1:1) to intravenous cabazitaxel 25 mg/m2 with or without intravenous
carboplatin AUC 4• At a median follow-up of 31ꞏ0 months, the combination improved the median PFS from 4.5 months to 7.3
months (95% CI 0ꞏ50–0ꞏ95, p=0ꞏ018)• All toxicities were worse with the combination
• Myelosuppression• Fatigue, nausea, others
Combination Carboplatin and Cabazitaxel
Progression Free Su
rvival
Overall Su
rvival
Corn et al Lancet Oncology 2019
SWITCH Trial: Dexamethasone and Prednisone• SWITCH was a single-arm, open-label, phase II study
evaluating the use of abiraterone acetate (AA) plus dexamethasone 0.5 mg daily (AA + D) in mCRPC patients progressing on AA + P.
• The primary endpoint was measured as the proportion of patients achieving a PSA decline of ≥ 30% (PSA30) from baseline after 6 weeks on AA + D.
• Twenty-six patients were enrolled. PSA30 and PSA50 rates were 46.2% and 34.6%.
• Median bPFS was 5.3 months
• Median rPFS was 11.8 months
• Two radiological responses were observed.
• In asymptomatic patients, the use of dexamethasone can associate with a PSA response and in rare situations a radiographic response.
Romero-Laorden et al. 2019 BJC

© National Comprehensive Cancer Network, Inc. 2021, All Rights Reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN®.
© 2021 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN®. To view the most recent and complete version of the NCCN Guidelines, go online to NCCN.org.
© 2021 National Comprehensive Cancer Network, Inc. All rights reserved. These guidelines and this illustration may not be reproduced in any form without the express written permission of NCCN®. To view the most recent and complete version of the NCCN Guidelines, go online to NCCN.org.













![Tumor Mutational Burden Immuno-Oncology Scientific Updates · Title: Tumor Mutational Burden Immuno-Oncology Scientific Updates Author: Ritterhouse, Lauren [BSD] - PTH Created Date:](https://img.pdfslide.net/doc/110x75/5fc25b7302cd4e75fc4563dd/tumor-mutational-burden-immuno-oncology-scientific-updates-title-tumor-mutational.jpg)