Embed Size (px)
DESCRIPTION
pschiatry
Citation preview
Mood Disorders
C. Baker-Burke
MScN, BScN, RN

Mood Disorders
Mood Disorders are mental disorders in which the prevailing symptoms are pathological mood changes of sadness/depression, elation/ mania or both.
Depressive disorders (DSM 5)
Major Depressive Disorder Persistent Depressive Disorder (Dysthymia)-
lasts more than 2 yrs. Premenstrual Dysphoric Disorder- symptoms
appear in final week before onset of most menses, then improve (eg. lability, irritability, anxiety, depressive mood)
Disruptive Mood Dysregulation Disorder –diagnosed before age 10 (temper tantrums, irritability, anger)
Depressive disorders (DSM 5)
Substance Medication-Induced Depressive Disorder
Other Specified Depressive Disorder-With Anxious distress-Peripartum onset (includes during/following
pregnancy) Unspecified Depressive Disorder-e.g.
insufficient information
Diagnostic criteria – Major Depressive Disorder
At least one of the following three abnormal moods that significantly interferes with the person's life:Depressed moodLoss of interest & pleasure Irritable mood (under 18 yrs)
Occurring most of the day, nearly every day, for at least 2 weeks
Diagnostic criteria
At least five of the following symptoms should have been present during the same 2 weeks as depressed mood: Loss of interest & pleasure Appetite/weight disturbance (gain/loss) Sleep disturbances Fatigue/loss of energy Guilt Poor concentration Morbid thoughts of death
Diagnostic criteria
The symptoms are not due toPhysical illness, alcohol,
medication, or drug use. Bipolar Disorder Delusional or Psychotic
Disorders
Bipolar disorder
Bipolar 1 Disorder -1 or more manic or mixed episodes
-Exclusions – physical, substance abuse, psychosis
Bipolar 11 -1 or more major depressive episodes accompanied by at least 1 manic episode
Cyclothymic Disorder
Mania
At least 5 of the foll. Increased physical & mental activity &
energy Heightened/ elevated mood, exag-
gerated optimism and self-confidence Excessive irritability, aggressive
behavior Decreased need for sleep without
experiencing fatigue
Mania
Grandiose delusions, inflated sense of self-importance
Racing speech & thoughts, flight of ideas
Impulsiveness, poor judgment, distractibility
Reckless behavior In severe cases, delusions &
hallucinations
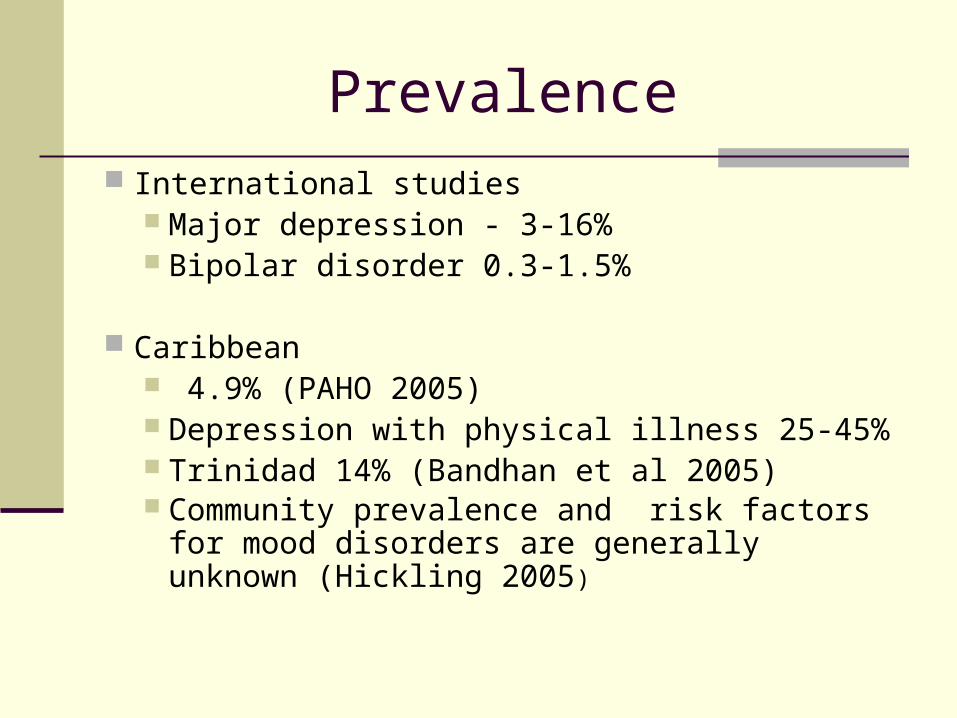
Prevalence International studies
Major depression - 3-16% Bipolar disorder 0.3-1.5%
Caribbean 4.9% (PAHO 2005) Depression with physical illness 25-45% Trinidad 14% (Bandhan et al 2005) Community prevalence and risk factors for
mood disorders are generally unknown (Hickling 2005)
Aetiology
Depression is often triggered by stressful life events
Contributing factors:Intensity and duration of these events
individual’s genetic endowmentcoping skills

Aetiology
Social support network – depression & many other mental disorders are described as the product of a complex interaction between biological and psychosocial factors
The importance of biological & psychosocial factors may vary across individuals & different types of depression.
AetiologyBiological factors
Alterations in brain function Abnormal concentrations of
neurotransmitters & their metabolites in urine, plasma, & cerebrospinal fluid
Overactivity of the HPA (hypothalamus-pituitary-adrenal) axis - stress
Major depression is associated with a dysfunction of the serotonergic activity and the hypothalamic-pituitary-adrenal (HPA) axis
AetiologyBiological factors
Dysfunction in 5-HT(1A) receptor activity could be due to a hypersecretion of cortisol
Antidepressants directly regulate HPA axis function.
HYDROXYTRYTAMINE- MODULATE NEUROTRANSMITTERS
Monoamine Hypothesis
Prevailing hypothesis - depression is caused by an absolute or relative deficiency of monoamine transmitters in the brain Evidence that reserpine used to treat
hypertension, caused depression by depleting the brain of both serotonin and the three principal catecholamines (dopamine, norepinephrine, and epinephrine).
monoamine hypothesis has been found insufficient to explain the complex etiology of depression. One problem is that many other neurotransmitter systems are altered in depression
Monoamine Hypothesis
monoamine hypothesis remains important for treatment purposes.
Many currently available pharmaco-therapies that relieve depression or mania, or both, enhance monoamine activity.
One of the foremost classes of drugs for depression, SSRIs, increase the level of serotonin in the brain.
Psychosocial and Genetic Factors in Depression
Social, psychological, and genetic factors act together to predispose to, or protect against, depression. Depression may be associated
with some sort of acute or chronic adversity
Psychosocial and Genetic Factors in Depression
Past parental neglect, physical and sexual abuse, and other forms of maltreatment impact on both adult emotional well-being and brain function
Early disruption of attachment bonds can lead to enduring problems in developing and maintaining interpersonal relationships and problems with depression and anxiety
Cognitive factors
How individuals view and interpret stressful events contributes to whether or not they become depressed.
The impact of a stressor is moderated by the personal meaning of the event or situation
Increased vulnerability to depression is linked to cognitive patterns that predispose to distorted interpretations of a stressful event
Genetic factors in depression & Bipolar Susceptibility to a depressive disorder is two to four
times greater among the first-degree relatives of patients with mood disorder
The risk among first-degree relatives of people with bipolar disorder is about 6 - 8 times greater. this does not prove a genetic connection. first-degree relatives typically live in the same
environment, share similar values and beliefs, and are subject to similar stressors, the vulnerability to depression could be due to nurture rather than nature
Management
50 to 70 percent of depressed patients who complete treatment respond to either antidepressants or psychotherapies
Surveys consistently show that a majority of individuals with depression receive no treatment
The acute phase for medication typically requires 6 to 8 weeks patients should be seen weekly or biweekly for
monitoring of symptoms, side effects, dosage adjustments, and support
Psychotherapies during the acute phase for depression typically consist of 6 to 20 weekly visits
Management
ECT Treatment in Depression 60 to 70 % response rate seen with ECT
effect of ECT occurs faster Proposed to be useful with poor response to
meds & depression is accompanied by potentially uncontrollable suicidal ideas and actions
The most common adverse effects are confusion and memory loss for events surrounding the period of ECT treatment.

Management
Medication – Depression
Antidepressants -Drugs that elevate mood by increasing the levels of serotonin and noradrenaline in the synaptic cleft
-antidepressant should be followed by at least 6 months of continued treatment)
SSRI - Fluoxetine 20mg daily
-Sertraline 50mg daily
-Paroxetine 20mg daily
Selective serotonin re-uptake inhibitor
Management
Medication – Depression (cont’d)
SNRI - Venlafaxine 37.5 mg daily (serotonin & norepinephrine reuptake inhibitor)
Bupropion / Wellbutrin
TCAs - Amytryptilline 75mg daily
- Imipramine 75 mg daily St John’s Wort
Tricyclic antidepressant
Management
Medication – Bipolar Disorder
Antipsychotic
Some atypical antipsychotics are also used to help control manic episodes (olanzapine, aripiprazole and quetiapine
Olanzapine & aripiprazole affect dopamine and serotonin.
Olanzapine prevents excessive activity of dopamine.
Quetiapine treats both manic and depressive episodes.
Management
Antimanic /mood stabilizers are drugs used in the long-term management of bipolar disorder.
They are used to maintain a person's mood at a reasonable level and help prevent future episodes of low or high mood (mania).
There are three types of mood stabiliser: The oldest and most widely used is lithium
(LiCO3) .
Management
Some anticonvulsants proved to be effective mood stabilisers ( valproate, carbamazepine and lamotrigine
Lithium 200mg tid PO (Monitor lithium levels)
Carbamazepine 300mg tid PO
Valproic acid 250 mg tid PO (monitor liver function)
Management
Anticonvulsants are thought to work on the brain by: increasing the amount of a natural nerve-calming chemical called GABA
reducing the amount of a natural nerve-exciting chemical called glutamate

Management
Issues to consider when taking lithium includes: regular blood tests to monitor the level of
lithium in your blood (0.6 -1.2 is normal; >1.5 is toxic)
maintaining an adequate fluid intake & avoiding dietary changes that suddenly increase or reduce salt intake
potential problems of using other medications at the same time (e.g. Diuretics).
Management - Side effects
Nausea, vomiting, and diarrhea. Trembling. Increased thirst & the need to urinate. Weight gain in the first few months of use. Drowsiness. A metallic taste in the mouth (lithium) With Carbamazepine and Lamotigine a major
side effect is Stevens-Johnson Syndrome (rash, sore throat, fever, lesions skin & mm)
Psychosocial interventions
NICE Guidelines Mild depression – psychological
Moderate depression – Medication or Psychological
Severe depression – CBT & medication
(CBT is best established treatment for depressive mood disorders)
Nursing Management using Nursing Process: Assessment
CC., HPI, PPH, PMH, SH, physical & mental health status
attitudes, feelings, knowledge of pt. & family re; illness
Degree & intensity of suicidal thinking Issues of powerlessness, hopelessness,
social isolation Sleeplessness, hyperactivity, risky
behaviours

Nursing diagnoses
Specific nursing diagnoses in depressed individuals include:
chronic low self-esteem, powerlessness, hopelessness Risk for suicideRisk for self directed violence
Planning & outcome identification
Outcomes are pt. & family oriented
Planning – develop written care plan, establish short term & long term goals

Implementation
Identify appropriate nursing Interventions with rationale to address problems/ needs
Develop nurse- patient relationship
-therapeutic use of self
-apply roles of nurse in psychiatric setting Administer medication Educate Pt. & family re: illness, meds.,
adherence to treatment, follow up care, lifestyle changes, stress reduction, activity, recreation
Evaluation
Formative – achievement of short term goals during care process
Summative at discharge- pt’s. ability to establish long term goals and continue therapy, referrals, follow up care, re-integration into family & community.
References
1. American Psychiatric Association (2013) Diagnostic Statistical Manual 5th edition Arlington VA APA
2. Carson, V.B.(2000) Mental health nursing: the nurse-patient journey 2nd ed. Philadelphia: W.B. Saunders company
3. Kaplan, H.I., Sadock, B.J. (1996) Concise textbook of clinical psychiatry 7th ed. Pennsylvania: Lippincott Williams & Wilkins