Embed Size (px)
Citation preview
Emerg Med Clin N Am
24 (2006) 797–808
Moral Moments at the End of Life
Terri A. Schmidt, MD, MSDepartment of Emergency Medicine, Center for Ethics in Health Care,
Oregon Health & Sciences University, CDW-EM, 3181 SW Sam Jackson Park Road,
Portland, OR 97239, USA
Decision making near the end of life can be complex and laden with emo-tion for families and health care providers. Families and patients can pre-pare themselves for these difficult moments by thinking ahead about thepatient’s wishes and preparing clear documents that express those wishes.Health care providers can prepare themselves by being familiar with thosedocuments, considering the goals of treatment, remembering the principleson which health care ethics are founded and knowing decision-makingmodels that will help them to think through treatment plans and the bestoptions for patient taking into consideration the goals of treatment.
Key concepts:
� Knowing the goals of treatment� Communicating and honoring patient wishes� Knowing the uses and limitations of advance directives and do not at-tempt resuscitation (DNAR) orders� Ethical decision making models� Role of futility
Three cases
The good
Eric arrives in an ambulance at 4:30 in the morning. He is a 27-year-oldman who is sitting upright on the gurney, leaning forward, and in obvioussevere respiratory distress. He has a Physicians Orders for Life-SustainingTreatment (POLST) form sitting on his lap that states, ‘‘Do Not AttemptResuscitation; Comfort Measures Only and this patient has end-stage cysticfibrosis’’ [1].
E-mail address: [email protected]
0733-8627/06/$ - see front matter � 2006 Elsevier Inc. All rights reserved.
doi:10.1016/j.emc.2006.05.011 emed.theclinics.com

798 SCHMIDT
The bad
A 78-year-old woman with profound Alzheimer’s dementia was admittedto the hospital with pneumonia. During a brief admission, her son and thedoctors determined that she would not want further intervention. A decisionwas made to transport her home in an ambulance for end-of-life care. Nowritten DNAR orders were provided to the emergency medical services(EMS) staff. Shortly after driving away from the hospital the patient wasfound to be without a pulse and not breathing.
The almost ugly
An 80-year-old man arrived in the emergency department with alteredmental status. No documents were sent with the patient. He was hypoten-sive and his heart rate was 50 beats per minute. He could not answer anyquestions and no family was initially with the patient. Over the next fewminutes his blood pressure continued to drop along with his oxygen satura-tion. Within a few minutes family arrived and were able to relay that thepatient had multiple serious medical conditions. He had been hospitalizeda few weeks earlier. At that time he was mentally alert and clearly expressedhis wishes for no aggressive interventions. The patient was kept comfortablein the ED with family at his bedside.
In emergency medicine and EMS, all patients are presumed to desireresuscitation and life-sustaining interventions unless there is explicit infor-mation to the contrary. However, many patients with advanced illnessesmay not want all interventions [2]. The emergency physician needs to de-termine which patients should have an attempt at cardiopulmonary resus-citation, as well as other life-sustaining interventions, and which shouldnot. These decisions are based on the goals and ethical principles of med-icine. The basic ethical principles on which modern medicine are foundedinclude respect for patient autonomy, beneficence, nonmaleficence, andjustice. Respect for patient autonomy leads to the understanding that pa-tients may choose to limit the interventions that they wish and thus sup-ports DNAR orders based on the patient’s preferences. Both beneficenceand nonmaleficence suggest that an intervention should not be performedif there is no chance that it will benefit the patient. This has been the ba-sis for consideration of DNAR orders based on futility.
The goal of this manuscript is to describe the framework for making eth-ical decisions when treating patients near the end of life. To achieve thosegoals, the manuscript includes further discussion of the ethical principlesof Western medicine, a description of methods for expressing patient pref-erences and two models for ethical decision making, as well as a brief dis-cussion of the role of futility. Finally, a few comments are included onpracticing procedures on the newly dead.

799MORAL MOMENTS AT THE END OF LIFE
Methods of expressing patient preferences
Emergency physicians are frequently faced with the need to make a rapiddecision about attempting resuscitation in a patient who arrives in extremis.Often the patient is unable to verbalize preferences about treatment and thephysician must make these time-critical decisions based on written instruc-tions, if available. These instructions can be either patient-initiated advancedirectives or health care provider–initiated DNAR orders and other treat-ment orders.
An advance directive is a written document, completed by the patient, ex-pressing future wishes. It is designed to be used at a time when the patientcan no longer express his or her wishes. The two main types of advance di-rective are living wills and durable powers of attorney for health care. ThePatient Self-Determination Act, which became effective in 1991, requiresthat all hospitals that accept Medicare and Medicaid funds provide informa-tion about advance directives and develop policies for implementation ofadvance directives. There has been an increase in advance care planningsince then with more patients in long-term care settings having advance di-rectives but in many cases advance directives are still lacking when patientsare transferred to emergency departments [3–6]. These forms can be cumber-some to complete and calls have been made for states to simplify the process[7]. One study found that many emergency department patients have neverthought about an advance directive or prefer that families make the decisionat the time of an event [8].
One type of advance directive, the living will, expresses the wishes of pa-tients regarding life-sustaining procedures in the event of terminal illness.These documents have specific restrictions that state that the person wouldnot want resuscitation if he or she is terminally ill, death is imminent, andresuscitation would only prolong the dying process. Because of these restric-tive phrases, living wills are often of little value in the emergency and pre-hospital setting [9]. In many cases health care providers do not follow them[10] and in at least one state, they explicitly do not apply except in a hospitalor clinic setting [11]. However, when the applicability and circumstances areclear, the emergency physician should respect the living will and it does pro-vide valuable information about the patient’s preferences. Often, althoughthe document does not prevent a resuscitative effort in the emergency de-partment, it does facilitate later decisions about withdrawal of life supportin the intensive care unit.
Another form of patient-completed advance directive, the durable powerof attorney for health care, gives to another person the authority to makedecisions for a patient if he or she is unable to make decisions either tempo-rarily or permanently. Under those circumstances, the person designated inthe power of attorney becomes a legally recognized proxy decision makerfor the patient. When a durable power of attorney exists, the emergencyphysician should allow the designated person to participate in decisions
800 SCHMIDT
regarding the patient’s medical care. The proxy decision maker should notbase requests to initiate or withhold resuscitation on his or her own values,but make decisions according to the known wishes of the patient. Immunityis generally granted to the physician who carries out the proxy’s decision ingood faith. Some states allow surrogates without a specific health carepower of attorney to make decisions about resuscitation and end-of-lifecare for incapacitated patients and others do not. Emergency physiciansneed to be aware of their own state laws and regulations regarding healthcare proxies and living wills.
Unlike living wills and health care powers of attorney, DNAR orders arewritten by a health care provider to indicate that resuscitation should not bestarted. These orders are unique in that they are directions not to do some-thing, rather than orders that initiate a treatment. DNAR orders are one as-pect of respecting patient preferences but they only apply when the patient ispulseless and apneic. However, many primary care providers believe thatthey apply in other circumstances and that intubation and cardioversionare not appropriate in a patient with DNAR orders [12]. A 1997 reportfound that most emergency physicians are willing to honor written directivesregarding resuscitation but would not withhold resuscitation based on unof-ficial documents or verbal reports.
Just as emergency physicians must consider patient preferences whendeciding when to attempt resuscitation, EMS systems and out-of-hospitalproviders face these same decisions [13]. Similarly to physicians in the emer-gency department, patient-initiated advance directives are difficult foremergency medical technicians (EMTs) to apply to decisions about specificlife-support measures [14]. Physician DNAR orders are often more success-ful. Most states now have out-of-hospital DNAR programs, consistent withthe American College of Emergency Physicians’ position that, ‘‘Each emer-gency medical services (EMS) system should have a well-defined, compre-hensive policy for dealing with out-of-hospital ‘do not attemptresuscitation’ (DNAR) directives’’ [15]. The number of states authorizingout-of-hospital DNR orders has increased from 11 states in 1992 [16] to42 states in 1999 [17]. A Canadian study found that nearly 10% of cardiacarrest calls were for patients with a terminal illness. In 63% of these cases,there was either a verbal (by family) or written request for no resuscitation[18]. A recent survey found that 89% of a national sample of EMTs werewilling to honor a state-approved DNR order and that 77% had localprotocols for termination of resuscitation in the prehospital setting [19].However, another study found that 21% of patients with DNAR ordersin long-term care facilities had resuscitation attempts when EMS was called.Thus, states have had success with their DNR programs [20] but problemsremain. For example, Connecticut has a DNR bracelet program requiringEMTs to honor these DNR orders and provides immunity from liabilityfor honoring the order [21]. However, one study suggests that braceletDNR programs are used infrequently [14]. In addition, advance directives
801MORAL MOMENTS AT THE END OF LIFE
and DNR orders may not be available when EMS arrives and often do notaccompany patients to the emergency department [4,22,23]. Further, out-of-hospital DNAR programs typically provide only orders about resuscita-tion with no guidance for patients who are breathing and have a pulse. It isoften harder for physicians and prehospital providers to know what inter-ventions are or are not appropriate for the seriously ill patient who is notin cardiopulmonary arrest but cannot speak for him or herself, and doesnot have a surrogate present to express the patient’s wishes.
Physician Orders for Life-Sustaining Treatment paradigm
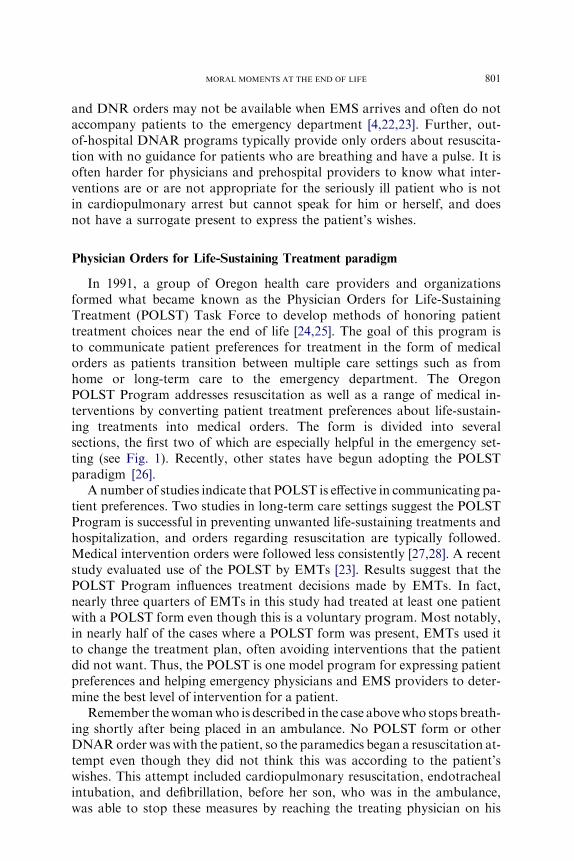
In 1991, a group of Oregon health care providers and organizationsformed what became known as the Physician Orders for Life-SustainingTreatment (POLST) Task Force to develop methods of honoring patienttreatment choices near the end of life [24,25]. The goal of this program isto communicate patient preferences for treatment in the form of medicalorders as patients transition between multiple care settings such as fromhome or long-term care to the emergency department. The OregonPOLST Program addresses resuscitation as well as a range of medical in-terventions by converting patient treatment preferences about life-sustain-ing treatments into medical orders. The form is divided into severalsections, the first two of which are especially helpful in the emergency set-ting (see Fig. 1). Recently, other states have begun adopting the POLSTparadigm [26].
A number of studies indicate that POLST is effective in communicating pa-tient preferences. Two studies in long-term care settings suggest the POLSTProgram is successful in preventing unwanted life-sustaining treatments andhospitalization, and orders regarding resuscitation are typically followed.Medical intervention orders were followed less consistently [27,28]. A recentstudy evaluated use of the POLST by EMTs [23]. Results suggest that thePOLST Program influences treatment decisions made by EMTs. In fact,nearly three quarters of EMTs in this study had treated at least one patientwith a POLST form even though this is a voluntary program. Most notably,in nearly half of the cases where a POLST form was present, EMTs used itto change the treatment plan, often avoiding interventions that the patientdid not want. Thus, the POLST is one model program for expressing patientpreferences and helping emergency physicians and EMS providers to deter-mine the best level of intervention for a patient.
Remember thewomanwho is described in the case abovewho stops breath-ing shortly after being placed in an ambulance. No POLST form or otherDNARorder was with the patient, so the paramedics began a resuscitation at-tempt even though they did not think this was according to the patient’swishes. This attempt included cardiopulmonary resuscitation, endotrachealintubation, and defibrillation, before her son, who was in the ambulance,was able to stop these measures by reaching the treating physician on his

802 SCHMIDT
cell phone. All of this could have been prevented by written orders such asa DNAR order or a POLST form.
Ethical decision making
Having clear documentation can help to prevent unwanted resuscitationand respect patient wishes but conflicts and dilemmas are likely to continue
Fig. 1. Physician Orders for Life-Sustaining Treatment (POLST) form.
803MORAL MOMENTS AT THE END OF LIFE
to arise. When faced with an ethical dilemma, the emergency physician (orEMT) needs to know how to determine the best course of action. Knowingthe goals of intervention and remembering the ethical principles on whichmedicine is founded are helpful but it is useful to have a framework in whichto think through the problem. Often decisions must be made quickly, withlimited information. Two models for ethical decision making will be pre-sented here.
First, Ken Iserson and colleagues [29] have developed an ethical decision-making model designed for the emergency setting. The first step in thismodel is to ask the question, ‘‘Is this a type of ethics problem for whichyou have already worked out a rule or is this at least similar enough sothat a rule could reasonably be extended to cover it?’’ If so, then followthe rule. The second step is to ask the question, ‘‘Is there an option thatwill buy time for deliberation without excessive risk to the patient?’’ Ifyes, buy time. Finally, if the first two steps do not yield a solution, testyour proposed action against the following three rules: (1) ImpartialitydWould you be willing to have this action performed if you were in the pa-tient’s place? (2) UniversalizabilitydWould you be willing to use the samesolution in all similar cases? (3) Interpersonal justifiabilitydWould you bewilling to defend the decision to others, to share the decision in public?One way to consider the problem is to ask yourself which action you wouldbe most willing to stand up and defend the next day.
What would happen if the emergency physician used this model to deter-mine what to do in the case above of an 80-year-old man who arrives withaltered mental status, hypotension, and bradycardia. Initially he has no ad-vance directives or information about his preferences for treatment. He ap-pears chronically ill but nothing is known about his quality of life or hisunderlying medical conditions. Using the first question, most emergencyphysicians agree that when no information is available about the patient’spreferences we need to err on the side of intervention and attempt resuscita-tion. This rule could be stated as, ‘‘When in doubt regarding the patient’swishes, resuscitative efforts should be initiated.’’ The decision to resuscitatemust be an immediate ‘‘yes’’ or ‘‘no’’ decision. ‘‘Slow codes,’’ suboptimal ef-fort, or delayed interventions are not medically or ethically justifiable. Atthe same time, consider the second question. In this case there are some in-terventions that can be employed to buy time until more information isavailable. The patient could be treated with atropine or external pacingalong with the use of a bag-valve mask for at least a few minutes. Thiswould allow the family to arrive and provide more information. When thephysician learns the patient’s preferences he or she could either continuethe resuscitation efforts or stop life-prolonging interventions. As it turnsout, the family arrives after a few minutes and is able to provide informationthat the patient has severe congestive heart failure along with other medicalproblems and has completed advance directives indicting that he does notwant life-sustaining treatments. Efforts at resuscitation are stopped; the

804 SCHMIDT
social worker provides support to the family; the family members spendtime with the patient in the emergency department; and he dies quietlywith them in attendance. The family is grateful that they were able to bethere with him when he died and that the emergency department stafftreated them and their loved one with respect and dignity.
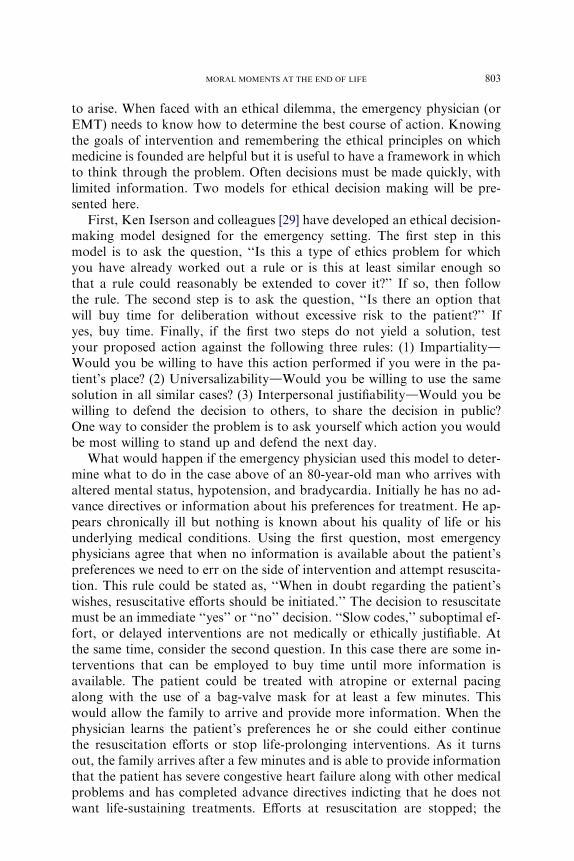
A second ethical decision-making model was developed by Jonson andcolleagues [30]. The model was designed to answer a medical ethics dilemmaby considering four domains: medical indications, patient preferences, qual-ity of life, and contextual features (see Fig. 2). By considering all four ofthese domains the health care provider attempts to ensure that no salientfeatures of the case are ignored.
Now, consider the story above of a man with cystic fibrosis who comes tothe emergency department in respiratory distress. The medical indicationsare straightforward: Eric is in severe respiratory failure and in need of intu-bation, airway management, and ventilation. Of course, with his seriouslung disease these efforts might be futile, but more on that later. In thiscase, his preferences are also known. He has a POLST form that indicatedthat he is DNAR and that he would want comfort measures only, no inter-ventions intended to prolong his life. In fact, a brief call to his foster momreveals that he has been very ill for the past year and his goal was to live tohis 27th birthday, now 3 weeks past. This conversation also confirms thatrecently he has been extremely short of breath even at rest and no longerwas satisfied with the quality of his life. Several of the nurses in the EDknow him from previous visits and describe him as a fun-loving man witha ‘‘wicked’’ sense of humor. On recent visits much of the love of life seemedto be waning. Contextual features encompass any other factors that mightinfluence a decision. Here one might consider family wishes, applicablelaws, or hospital policies that have an impact on the situation. In ourcase, the only available family is a foster mom who was unable to cometo the hospital because she was caring for others with cystic fibrosis in her
Contextual FeaturesPatient Preferences
Quality of LifeMedical Indications
Fig. 2. Jonsen model for ethical decision making.

805MORAL MOMENTS AT THE END OF LIFE
home, and clearly understood that Eric might die. Based on a brief analysis,considering the four domains, I was able to determine that no attemptshould be made to intubate Eric, although this meant that he was likelyto die of respiratory failure in a short time. He was made as comfortableas possible, with one of the nurses or me sitting at his side. After a shortwhile his breathing became labored and he seemed to be struggling so hewas given small doses of morphine and lorazepam to keep him comfortableand he quietly and peacefully died about sunrise. His foster mom, primaryphysician, and I believed that his wishes had been honored and the last mo-ments of his life were peaceful ones.
Futility
To this point, we have discussed making decisions based on patient pref-erences with a focus on respect for autonomy. Something needs to be saidabout futility in making decisions about resuscitation. Futility comes fromthe Latin, futiliz, meaning leaky or that which easily pours out [1,31]. Onereport found that a majority of emergency physicians had recently attemp-ted resuscitations despite expectations that they were futile. Nonetheless, itis generally agreed that physicians should not offer or provide treatments topatients that have no chance of benefiting a patient [32]. This is based onthe principles of beneficence and nonmaleficence [33,34]. To take this ideato its extreme, we would never offer surgery on the gall bladder as a treat-ment option for a patient who has appendicitis. The same is true of attemp-ted resuscitation. It should not be attempted on a patient who has nochance of benefit. The problem arises when we try to define ‘‘no chance’’and ‘‘benefit.’’ Further, many physicians report that they attempt resuscita-tion because of legal concerns. This might be somewhat mitigated by a re-port from Oregon, which found that only 2.4% of families reported thattoo little treatment was given to a deceased family member near the endof life.
Some ethicists have suggested a probabilistic approach to defining futil-ity. For example, if well-designed studies show a 1% or less chance of sur-vival the treatment can be defined as futile [30]. Using this approach in theprehospital setting, in the absence of obvious signs of death (dependent li-vidity, rigor mortis, decapitation) there are no absolute indicators that re-suscitation has no chance of success and unless there is information aboutpatient preferences, resuscitation should be attempted [35]. However, thereis a body of evidence that indicates that there have been no survivors ofadult medical arrest who are not in ventricular fibrillation if a full resuscita-tive effort including CPR, definitive airway management, medication admin-istration, defibrillation if necessary, and at least 20 minutes of treatmentfollowing Advanced Cardiac Life Support (ACLS) guidelines is performed[32,36,37]. In those circumstances, it is ethically justified to stop resuscita-tion attempts based on futility [38,39]. There is also evidence that families

806 SCHMIDT
are generally accepting of stopping efforts without transporting the personto a hospital [40].
Many authors have pointed out the importance of determining the goalswhen defining futility. Marco and Larkin [31] suggest using the term ‘‘clin-ically nonbeneficial interventions’’ instead of ‘‘futility’’ to help clarify the in-tent. This allows the clinician to consider the goals of treatment. A commonexample is the patient for which living for a few days might be a benefit be-cause it would allow her to say goodbye to family, or for out-of-town rela-tives to arrive. Thus, while some authors have argued that decisions aboutfutility should be made by physicians and that families do not need to beconsulted [41,42] to determine the goals of treatment, it makes sense to com-municate with patients and families when possible. It has been noted thatthe use of futility to justify unilateral decisions fosters conflict.
Procedures on the newly dead
Up to this point we have considered ethical decisions in patients near theend of life. One final ‘‘moral’’ moment arises when teachers and traineesmust make a decision on whether or not to practice procedures on the newlydead. In the past this may have been a common practice and few institutionshad policies regulating the practice that occurred behind closed doors. Stud-ies suggest that 47% to 63% of emergency programs allow the practice andthat consent is rarely obtained [43–47]. These same studies indicate that fewprograms have written policies surrounding the practice [44,46,47]. More re-cently, major medical organizations have begun to address this issue, gener-ally endorsing the need for written policies and the requirement for familyconsent before procedures are performed [9,48]. Recently, the Society forAcademic Emergency Medicine published a position that strongly encour-ages all emergency medicine training programs to develop a policy and rec-ommends that families be asked for consent before practicing procedures onthe newly dead [49].
Summary
Decision making near the end of life can be complex and laden with emo-tion for families and health care providers. Families and patients can pre-pare themselves for these difficult moments by thinking ahead about thepatient’s wishes and preparing clear documents that express those wishes.Health care providers can prepare themselves by being familiar with thosedocuments, considering the goals of treatment, remembering the principleson which health care ethics are founded and knowing decision-makingmodels that will help them to think through treatment plans and the bestoptions for patients taking into consideration the goals of treatment.

807MORAL MOMENTS AT THE END OF LIFE
References
[1] Schmidt T. Futility-futilis-the leaky vessel. Ann Emerg Med 2000;35:615–7.
[2] Innes G, Wanger K. Dignified death or legislated resuscitation? CMAJ 1999;161:1264–5.
[3] Teno JM, Branco KJ, Mor V, et al. Changes in advance care planning in nursing homes be-
fore and after the patient Self-Determination Act: report of a 10-state survey. J Am Geriatr
Soc 1997;45:939–44.
[4] Lahn M, Friedman B, Bijur P, et al. Advance directives in skilled nursing facility residents
transferred to emergency departments. Acad Emerg Med 2001;8:1158–62.
[5] Jackson EA, Yarzebski JL, Goldberg RJ, et al. Do-not-resuscitate orders in patients hospi-
talized with acute myocardial infarction: the Worcester Heart Attack Study. Arch Intern
Med 2004;164:776–83.
[6] Llovera I, Mandel FS, Ryan JG, et al. Are emergency department patients thinking about
advance directives? Acad Emerg Med 1997;4:976–80.
[7] Lo B, Steinbrook R. Resuscitating advance directives. Arch Intern Med 2004;164:
1501–6.
[8] Llovera I, Ward MF, Ryan JG, et al. Why don’t emergency department patients have ad-
vance directives? Acad Emerg Med 1999;6:1054–60.
[9] AbramsonN, de VosR, FallatME, Finucane T, et al. Ethics in emergency cardiac care. Ann
Emerg Med 2001;37:s195–200.
[10] Danis M, Southerland LI, Garrett JM, et al. A prospective study of advance directives for
life-sustaining care. N Engl J Med 1991;324:882–8.
[11] SilveiraMJ, Buell RA, Deyo RA. Prehospital DNR orders: what do physicians inWashing-
ton know? J Am Geriatr Soc 2003;51:1435–8.
[12] Lerner EB, Billittier AJ, Hallinan K. Out-of-hospital do-not-resuscitate orders by primary
care physicians. J Emerg Med 2002;23:425–8.
[13] Becker LJ, Yeargin K, Rea TD, et al. Resuscitation of residents with do not resuscitate
orders in long-term care facilities. Prehosp Emerg Care 2003;7:303–6.
[14] Partridge RA, Virk A, Sayah A. Field experience with prehospital advance directives. Ann
Emerg Med 1998;32:589–93.
[15] American College of Emergency Physicians. ‘‘Do not attempt resuscitation’’ directives in the
out-of-hospital setting. Ann Emerg Med 1996;27:684.
[16] Adams J. Prehospital do-not-resuscitate orders: a survey of polices in the United States. Pre-
hospital Disaster Med 1993;8:317–22.
[17] Sabatino CP. Survey of state EMS-DNR laws and protocols. J Law Med Ethics 1999;27:
297–315.
[18] Guru V, Verbeek PR, Morrison LJ. Response of paramedics to terminally ill patients with
cardiac arrest: an ethical dilemma. CMAJ 1999;161:1251–4.
[19] Marco CA, Schears RM. Prehospital resuscitation practices: a survey of prehospital pro-
viders. J Emerg Med 2003;24:101–6.
[20] IsersonKV.A simplified prehospital advance directive law: Arizona’s approach.AnnEmerg
Med 1993;22:1703–10.
[21] Leon MD, Wilson EM. Development of a statewide protocol for the prehospital identifica-
tion of DNR patients in Connecticut including new DNR regulations. Ann Emerg Med
1999;34:263–74.
[22] Morrison RS, Olson E,Mertz KR, et al. The inaccessibility of advance directives on transfer
from ambulatory to acute care settings. JAMA 1995;274:478–82.
[23] Schmidt TA, Hickman S, Tolle SW, et al. The Physician Orders for Life-Sustaining Treat-
ment (POLST) Program: Oregon emergency medical technicians’ practical experiences
and attitudes. J Am Geriatr Soc 2004;52:1430–4.
[24] Dunn PM,Nelson CA, Tolle SW, et al. Communicating preferences for life-sustaining treat-
ment using a physician order form. J Gen Intern Med 1997;12(suppl):102.

808 SCHMIDT
[25] Dunn PM, Schmidt TA, Carley MM, et al. A method to communicate patient preferences
about medically indicated life-sustaining treatment in the out-of-hospital setting. J AmGer-
iatr Soc 1996;44:785–91.
[26] Available at: http://www.ohsu.edu/polst/national.shtml. Accessed June 16, 2006.
[27] Tolle SW, Tilden VP, Nelson CA, et al. A prospective study of the efficacy of the physician
order form for life-sustaining treatment. 1998;46:1097–102.
[28] Lee MA, Brummel-Smith K, Meyer J, et al. Physician orders for life-sustaining treatment
(POLST): outcomes in a PACE program. Program of All-Inclusive Care for the Elderly.
J Am Geriatr Soc 2000;48:1343–4.
[29] Iserson KV, Sanders AB, Mathieu D. Ethics in emergency medicine. 2nd ed. Tuscon, AZ:
Galen Press, Ltd; 1995.
[30] JonsenAR, SieglerM,WinsladeWJ. Clinical ethics. 4th ed. NewYork:McGraw-Hill; 1998.
[31] Marco CA, Larkin GL. Ethics seminars: case studies in ‘‘futility’’dchallenges for academic
emergency medicine. Acad Emerg Med 2000;7:1147–51.
[32] American Heart Association. Part 2: Ethical aspects of CPR and ECC. Resuscitation 2000;
102:17–27.
[33] Levack P. Live and let die? A structured approach to decision-making about resuscitation.
Br J Anaesth 2002;89:684–5.
[34] HilbermanM, Kutner J, Parsons D, et al. Marginally effective medical care: ethical analysis
of issues in cardiopulmonary resuscitation (CPR). J Med Ethics 1997;23:361–7.
[35] Pepe PE, Swor RA, Ornato JP, et al. Resuscitation in the out-of-hospital setting: medical fu-
tility criteria for on-scene pronouncement of death. Prehosp Emerg Care 2001;5:79–87.
[36] Bailey ED,WydroGC, ConeDC. Termination of resuscitation in the prehospital setting for
adult patients suffering nontraumatic cardiac arrest. National Association of EMS Physi-
cians Standards and Clinical Practice Committee. Prehosp Emerg Care 2000;4:190–5.
[37] BonninMJ, Pepe PE, Kimball KT, et al. Distinct criteria for termination of resuscitation in
the out-of-hospital setting. JAMA 1993;270:1457–1462.
[38] Kellerman AL, Staves DR, Hackman BB. In-hospital resuscitation following unsuccessful
prehospital advanced cardiac life support: ‘‘heroic efforts’’ or an exercise in futility. Ann
Emerg Med 1988;17:589–94.
[39] GrayWA, Capone RJ,Most AS. Unsuccessful emergencymedical resuscitation: are contin-
ued efforts in the emergency department justified? N Eng J Med 1991;1991:1393–8.
[40] Schmidt TA, Harrahill MA. Family response to out-of-hospital death. Acad Emerg Med
1995;2:513–8.
[41] SchneidermanLJ, JeckerNS, JonsenAR.Medical futility: response to critiques. Arch Intern
M 1996;125:669–74.
[42] Jecker NS, Pearlman RA.Medical futility: who decides? Arch InternMed 1992;152:1140–4.
[43] Burns JP, ReardonFE, TruogRD.Using newly deceased patients to teach resuscitation pro-
cedures. N Engl J Med 1994;331:1652–5.
[44] Morhaim DK, Heller MB. The practice of teaching endotracheal intubation on recently de-
ceased patients. J Emerg Med 1991;9(6):515–8.
[45] Ginifer C, Kelly AM. Teaching resuscitation skills using newly deceased. Med J Aust 1996;
165:445–7.
[46] FourreMW. Performance of procedures on the recently deceased. Acad EmergMed 2003;9:
595–8.
[47] Knopp RK. Practicing cricothyrotomy on the newly dead. Ann Emerg Med 1995;25:694–6.
[48] The Council on Ethical and Judicial Affairs of the AmericanMedical Association. Perform-
ing procedures on the newly dead. Acad Med 2002;77:1212–6.
[49] Schmidt TA, Abbott JT, Geiderman JM, et al. Ethics seminars: the ethical debate on prac-
ticing procedures on the newly dead. Acad Emerg Med 2004;11:962–6.























![Moral Realism, Moral Relativism, Moral Rules [Oddie]](https://img.pdfslide.net/doc/110x75/577cd1091a28ab9e78937559/moral-realism-moral-relativism-moral-rules-oddie.jpg)



