Embed Size (px)
Citation preview

http://nej.sagepub.com/Nursing Ethics
http://nej.sagepub.com/content/7/6/520The online version of this article can be found at:
DOI: 10.1177/096973300000700607
2000 7: 520Nurs EthicsKim Lützén, Agneta Johansson and Gun Nordström
Moral Sensitivity: some differences between nurses and physicians
Published by:
http://www.sagepublications.com
can be found at:Nursing EthicsAdditional services and information for
http://nej.sagepub.com/cgi/alertsEmail Alerts:
http://nej.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://nej.sagepub.com/content/7/6/520.refs.htmlCitations:
What is This?
- Nov 1, 2000Version of Record >>
at University Library Utrecht on June 2, 2014nej.sagepub.comDownloaded from at University Library Utrecht on June 2, 2014nej.sagepub.comDownloaded from

MORAL SENSITIVITY: SOMEDIFFERENCES BETWEEN NURSES
AND PHYSICIANS
Kim Lützén, Agneta Johansson and Gun Nordström
Key words: ethics; health care; moral sensitivity; professionals
We report the results of an investigation of nurses’ and physicians’ sensitivity to ethicaldimensions of clinical practice. The sample consisted of 113 physicians working ingeneral medical settings, 665 psychiatrists, 150 nurses working in general medicalsettings, and 145 nurses working in psychiatry. The instrument used was the MoralSensitivity Questionnaire (MSQ), a self-reporting Likert-type questionnaire consisting of30 assumptions related to moral sensitivity in health care practice. Each of these assump-tions was categorized into a theoretical dimension of moral sensitivity: relational orien-tation, structuring moral meaning, expressing benevolence, modifying autonomy,experiencing moral conflict, and following the rules. Significant differences in responseswere found between health care professionals from general medical settings and thoseworking in psychiatry. The former agreed to a greater extent with the assumptions inthe categories ‘meaning’ and ‘autonomy’ and to a lesser degree with the categories‘benevolence’ and ‘conflict’. Moreover, those from the psychiatric sector agreed to agreater extent to the use of coercion if necessary. Significant differences were also foundfor some of the MSQ categories, between physicians and nurses, and between males andfemales.
BackgroundThe theoretical approach to ethical problems in health care practice is today a sub-ject of much discussion. There is also a strong divergence of opinion in the liter-ature on differences in ethical reasoning between physicians and nurses. Onepredominant perspective is to associate nursing with the ‘caring’, subjective,approach, of which feelings and intuition are the modes of ethical reasoning, andphysicians with the ‘principle thinking’ and objective approach. Whether nursesare adopting this approach themselves in the process of professional develop-ment1 or whether there is a ‘true’ distinction between physicians and nurses isalso a subject engaging many scholars. Rickard et al.,1 for example, make a strong
Nursing Ethics 2000 7 (6) 0969-7330(00)NE375OA © 2000 Arnold
Address for correspondence: Kim Lützén, Dean, Department of Nursing, Ersta-SköndalUniversity College, Box 4619, 116 91 Stockholm, Sweden.
at University Library Utrecht on June 2, 2014nej.sagepub.comDownloaded from

Nursing Ethics 2000 7 (6)
Moral sensitivity: differences between nurses and physicians 521
case for the position that there are no significant differences between physiciansand nurses. In their study, they explored the extent to which nurses exhibited‘partialist’ ethical reasoning and physicians ‘impartialist’ reasoning. A structuredquestionnaire based on four hypothetical moral dilemmas was administered to agroup of randomly selected physicians and nurses. No significant differences werefound, yet both modes of ethical reasoning were evident in nurses as well as inphysicians.
Both nurses and physicians are expected to make decisions that are consistentwith their professional code of practice. The practical aspect of this mandate per-tains to ethical competency, specifically the ability to understand the ethical natureof individual contexts and to act in a responsible way. However, because nurses’and physicians’ relationship to the patient is different, they may also have dif-ferent ways of viewing their ethical responsibility. It is a fact that physicians arelegally responsible for patient treatment and nurses are responsible for patientcare, which should be consistent with the physician’s orders.
Differences or similarities in how nurses and physicians view ethical issues inhealth care practice may be approached theoretically or empirically. Philosophicalenquiry, for example, typically starts from a commitment to a particular ethicaltheory in the analysis (and solution) of a particular problem. An example of anempirical approach is to describe real examples of difficult ethical problems in anattempt to identify the moral thinking or principles that are behind the decisionsthat are made.2
Each approach, characterized by the phenomenon of concern and its method-ology, makes a valuable contribution to health care ethics. However, there are lim-its to both of the above described approaches. Specifically, the philosophicalapproach to ethical enquiry may generate conceptual models that may not be truereplicas of the empirical world but, instead, abstract constructions of reality.Similarly, there is also a risk that the descriptive findings of empirical researchwill become uncritically accepted as the ‘norms’ of practice.
The phenomenon of concern in the study presented here is the interpersonalaspect of moral decision making, perceived to be a sensitizing factor in how eth-ical issues are identified in health care practice. More specifically, the aim of ourstudy was to describe nurses’ and physicians’ moral sensitivity, or attitudes con-cerning patient care. The term ‘attitude’ is usually defined as a quality of the indi-vidual and is known to be fairly stable over time.3 Thus, a person’s attitudetowards something is held to be ‘predictive’ of decisions that are made, or ofbehaviour in actual situations. In this study, the term attitude is used to mean anassimilation of ideas, feelings and values that influence a person’s moral sensi-tivity. We were particularly interested in comparing nurses and physicians in dif-ferent clinical settings, namely, general medical and psychiatric care.
The theoretical perspective builds on previous research that focuses on moralsensitivity, a personal predisposition guiding ethical decision making. In brief,moral sensitivity exhibited in health care practice is the ability to recognize amoral conflict, show a contextual and intuitive understanding of the patient’s vul-nerable situation, and have insight into the ethical consequences of decisionsmade on behalf of the person.4 A review of related studies shows that moral sen-sitivity is important as an affective component in the process of ethical decisionmaking. Carpenter,5 for example, explored the process by which nurses make eth-
at University Library Utrecht on June 2, 2014nej.sagepub.comDownloaded from

Nursing Ethics 2000 7 (6)
522 K Lützén, A Johansson and G Nordström
ical decisions in clinical practice. Twenty nurses participated in semistructuredinterviews in which they discussed ethical problems of their choice. Contentanalysis revealed that the process of making a decision begins with an emotionalresponse. Similarly, moral sensitivity can be seen as a type of emotional response,as a necessary component that activates the cognitive process of ethical decisionmaking.
In a phenomenological study by Smith,6 19 staff nurses were asked to describetheir experiences in making ethical decisions in practice. Two distinct componentsof the ethical decision-making process were identified: deliberation and integra-tion. The findings revealed that nurses need to: (1) recognize the ethical natureof their work; (2) discern which ethical decisions are theirs to make; and (3)acknowledge their authority to make ethical decisions in their practice.
The findings of other studies based on the concept of moral sensitivity7,8 indi-cate that the type of clinical setting influences how nurses and physicians per-ceive patient care. Another significant finding was that female nurses andphysicians experience moral conflicts in their practice to a greater extent thanmale nurses and physicians. Moreover, these conflicts often involve issues con-cerning patient autonomy. Other ethical issues in nursing practice concern team-work,9 and similarities and differences in the way that nurses and physicians viewethical problems.10
MethodInstrument
The Moral Sensitivity Questionnaire (MSQ), constructed from the qualitativeanalysis of moral sensitivity in psychiatric nursing practice,4,11 was used in thecollection of data. The MSQ is a self-administered questionnaire, designed as aseven-point scale that consists of 30 assumptions. An example of such an assump-tion is: ‘I believe that good care involves respecting the patient’s self-choice.’ Theanchors of each assumption are ‘I totally disagree’ and ‘I totally agree’. A scoreof 1–7 for each item indicates the extent of agreement or disagreement with theassumption. Twenty-nine assumptions are categorized according to the followingsix theoretical dimensions of moral sensitivity4,11:
• Relational orientation is reflected in the health care professional’s concern forhow actions will affect the relationship with the patient (category: relation).
• Structuring moral meaning refers to making sense of a patient’s limited auton-omy by finding that actions are meaningful, that is, they neither harm northreaten the patient’s integrity (category: meaning).
• Expressing benevolence refers to actions that are motivated by doing that whichis believed to be ‘good’ or in the best interest of the patient (category: benev-olence).
• Autonomy is reflected in views that the principle of patient autonomy, mean-ing self-choice, must be respected (category: autonomy).
• Experiencing moral conflict (category: conflict).• Following the ‘rules’ refers to actions that are instructed by routines and ward
policies (category: rules).
at University Library Utrecht on June 2, 2014nej.sagepub.comDownloaded from

Nursing Ethics 2000 7 (6)
Moral sensitivity: differences between nurses and physicians 523
Assumption no. 30: ‘It is sometimes justified to tell a patient that an injectionmay have to be given by force if he or she refuses the prescribed oral medica-tion’, explores the attitude to the threat of coercion and is analysed as a singleitem.
Respondents
The total sample in this study consisted of 1073 health care professionals whocompleted and returned the MSQ by post. The respondents comprised thefollowing professional groups:
Group A: physicians in general care settings (n = 113);Group B: psychiatrists (n = 665);Group C: nurses in general care settings (n = 150);Group D: nurses working in psychiatry (n = 145).
In group A, 240 questionnaires were distributed to physicians at a largeteaching hospital in Sweden. Of these, 113 were returned completed (47%). Theage range was 28–65 years (mean 46.8). A detailed description of the procedurefor the selection of groups B, C and D, as well as demographic data, has previ-ously been published.7,8 For the gender distribution in all groups, see Table 1.
The responses to the questionnaire in Group A were treated as new data andcompared with data collected in previous studies.7,8 The statistical method usedwas the t-test, which determines differences between two independent groups.The criterion for statistical significance was p < 0.05.
The Ethics Committee of Huddinge University Hospital approved the study.
FindingsDifferences between groups
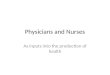
Significant differences in responses among the four groups A–D were foundfor the MSQ categories ‘meaning’, ‘benevolence’, ‘autonomy’ and ‘conflict’(Figure 1 and Table 2). No differences were found for the categories ‘relation’ and‘rules’.
Table 1 Gender distribution within groups A–D
Group Male Female Missinga Total(n=462) (n=577) (n=34) (n=1073)
A) Physicians, medical care 69 37 7 113B) Psychiatrists 365 288 12 665C) Nurses, general care 8 131 11 150D) Nurses, psychiatric care 20 121 4 145
a Gender not indicated.
at University Library Utrecht on June 2, 2014nej.sagepub.comDownloaded from

524 K Lützén, A Johansson and G Nordström
Nursing Ethics 2000 7 (6)
MEANING BENEVOLENCE
General nurse Psychiatric nurse
General physician Psychiatrist General physician Psychiatrist
General nurse Psychiatric nursep < 0.001
p < 0.001 p < 0.001
ns ns ns ns
p < 0.001
p < 0.001 p < 0.001p < 0.01p < 0.001
AUTONOMY CONFLICT
General nurse Psychiatric nurse
General physician Psychiatrist General physician Psychiatrist
General nurse Psychiatric nursens
p < 0.001 ns
ns ns ns
p<
0.0
01
p < 0.001
p < 0.001 p < 0.001nsns
Figure 1 Differences in responses between four groups of health careprofessionals in relation to four of the MSQ categories. ns, not significant
Table 2 Mean values for the MSQ categories for all groups
Category Physicians Psychiatrists Nurses, Nurses,general psychiatriccare care
Relation 16.8 17.4 17.3 17.3Meaning 25.8 23.9 23.1 25.6Benevolence 24.3 27.7 27.4 25.7Autonomy 17.8 16.5 16.8 16.9Conflict 16.0 16.5 18.1 15.4Rules 34.7 34.4 33.9 33.7
at University Library Utrecht on June 2, 2014nej.sagepub.comDownloaded from

Moral sensitivity: differences between nurses and physicians 525
Nursing Ethics 2000 7 (6)
Differences between general and psychiatric health careprofessionals
Significant differences in responses to the MSQ were found between health careprofessionals working in general and psychiatric care (Table 3). Nurses and doc-tors from general settings agreed to a greater extent than nurses and doctors frompsychiatric settings with the assumptions in the categories ‘meaning’ and ‘auton-omy’ and to a lesser extent with the assumptions in the categories ‘benevolence’and ‘conflict’. No significant differences were found in the categories ‘relations’and ‘rules’.
Regarding the single item referring to the threat of forced medication, a sig-nificant difference was found (p < 0.05). Health care professionals from psychi-atric settings agreed to a greater extent compared with those in general settings,indicating a more lenient attitude towards the use of coercion.
Differences between physicians and nurses
Significant differences in responses to the MSQ were found between all physi-cians (n = 778) and all nurses (n = 295) for the category ‘benevolence’ (p < 0.05).Physicians agreed with each other to a greater extent (mean 27.2, standard devi-ation (SD) 3.9) than nurses (mean 26.6, SD 4.4) with the assumptions in the cate-gory ‘benevolence’. No significant differences were found for the remainingcategories.
Regarding the single item referring to the threat of forced medication, a sig-nificant difference was found (p < 0.001). Physicians agreed to a greater extent(mean 3.3, SD 2.1) compared with nurses (mean 2.8, SD 1.9), indicating a morelenient attitude towards the use of coercion.
Table 3 Mean, SD and p-values for the MSQ categories for all general (groupsA and C) and all psychiatric (groups B and D) health care professionals
Category General care Psychiatric care p-value(n = 263) (n = 810)
Mean SD Mean SD
Relation 17.1 2.5 17.4 2.7 nsMeaning 25.7 6.4 23.7 5.7 <0.001Benevolence 25.1 4.7 27.6 3.6 <0.001Autonomy 17.3 2.7 16.5 3.1 <0.001Conflict 15.7 4.7 16.8 4.7 <0.001Rules 34.2 6.8 34.3 6.1 ns
ns, not significant.
at University Library Utrecht on June 2, 2014nej.sagepub.comDownloaded from

526 K Lützén, A Johansson and G Nordström
Nursing Ethics 2000 7 (6)
Differences between male and female professionals
Significant differences in responses to the MSQ were found between males andfemales regarding the category ‘meaning’ (p < 0.001). Female professionals agreedto a greater extent (mean 24.8, SD 6.1) compared with males (mean 23.4, SD 5.6)with the assumptions belonging to this category. No significant differences werefound for the remaining categories.
Regarding the single item about forced medication, a significant difference wasfound (p < 0.01) in the mean scores between male (mean 3.4, SD 2.1) and female(mean 3.0, SD 2.0) health care professionals. Females indicated a more negativeattitude towards the use of coercion than males.
DiscussionThe aim of this study was to describe nurses’ and physicians’ moral sensitivityconcerning patient care. We were also interested, if there were any differences,whether these could be explained by the ‘typical’ context of care and if theyoccurred between physicians and nurses employed in general medical wards com-pared with professionals in psychiatric care settings. A study of this kind has,however, some limitations, which should be taken into consideration in the inter-pretations of the findings. One of these is how the respondents conceptualizemoral dimensions, such as autonomy, in responding to the questionnaire.Nevertheless, there are typical contextual differences in the clinical settings rep-resented by the respondents that may account for the differences that were found.
It is well known that, in severe mental illness, psychiatric treatment is often ofan involuntary nature. The reason why psychiatric nurses and psychiatristsagreed to a lesser extent than those professionals working in general care toassumptions referring to patient autonomy could be explained in several ways.One interpretation, for example, is that psychiatric staff know by practical expe-rience what risks are involved if the principle of autonomy is strictly followed.Setting realistic limits to patient autonomy is (ideally) done in the best interest ofthe patient’s well-being. Patients with physical illness, compared with those withcognitive deficiencies, would be seen to be more able to participate in decisionsconcerning their care. Another explanation is that psychiatric nurses and physi-cians work in contexts that make it difficult to apply the principle of autonomyin an optimal way. When there is a shortage of staff, for example, strategies mayneed to be formulated to ensure the safety of all the patients on the ward. Suchmeasures need to be justified by defining autonomy in a more ‘flexible’ manner.
This way of ‘thinking contextually’ about autonomy has been demonstrated ina qualitative study of psychiatric nursing practice.12 The analysis of nurses’descriptions of the problems they faced and their reasoning about actions thatwere taken indicated that they defined the principle of autonomy in relation tocontextual demands. In order to ‘live with’ interventions that clearly limitedpatient autonomy, these nurses modified the principle of autonomy in order todefend and justify their actions. It is therefore likely that psychiatrists use thisprocess of thinking and justification, but from a medical point of view. Nursesreason from their experience of everyday situations concerning patient autonomy.
at University Library Utrecht on June 2, 2014nej.sagepub.comDownloaded from

Moral sensitivity: differences between nurses and physicians 527
Nursing Ethics 2000 7 (6)
In a study by Oddi et al.13 125 nurses were presented with situations involvingethical dilemmas. From the analysis it was concluded that these nurses generallyperceived that, in practice, ethical issues directly involve patients’ autonomy. Ifwe assume that ethical issues arise within the context of the professional andpatient relationship, we could also anticipate that nurses, who have a day to dayrelationship with patients, would view autonomy differently from physicians. Thefindings in our study indicate that the views on autonomy are shared by nursesand physicians but the problems or conflicts concerning patient autonomy aremore related to specific professional responsibility.
Compared with Rickard et al.,1 who did not find any differences between physi-cians and nurses in their study, we found that physicians were more in agree-ment than nurses were to assumptions belonging to the category ‘benevolence’.Our question is, what does it mean that physicians agree to a greater extent con-cerning these assumptions? Is the motivation that what is judged to be ‘good’ or‘best’ for the patient a stronger moral motivation for physicians than for nurses,or do nurses have other moral imperatives motivating their actions, such as doingthat which is delegated to them? In other words, although physicians may havemore of a professional informed choice in treatment regimens, nurses’ choices are,in part, determined by the physicians’ treatment orders.
Regarding differences between nurses and physicians in general settings, onlyin responses belonging to the category ‘benevolence’ was any dissimilarity iden-tified. Although there has been much theoretical debate on whether nurses andphysicians have different ways of looking at ethical problems,14 there are fewstudies that specify the nature of these variations. A study by Peter and Gallop15
examined whether ‘caring’ uniquely reflects the moral orientation of nursingstudents. Differences in moral orientation were subsequently found betweennursing and medical students. The authors concluded, however, that these dif-ferences appear to be related to gender, not to the professional roles of physiciansor nurses.
Whether it is the professional role, gender or the specific characteristics of thecontext of care that influences moral orientation is a difficult question to answer.Before the commencement of this study, we did not expect to find any differencesbetween nurses and psychiatrists employed in the same type of environment con-cerning the threat of coercion. Whether to use coercion or not, according to ourexperience, is an ethical problem for both nurses and physicians in psychiatriccare. The findings indicate, however, that, although health care professionals aregenerally not in favour of the threat of coercion, there was a difference betweenphysicians and nurses as well as between female and male professionals. Therewere no significant differences found between physicians and nurses regardingthe category ‘autonomy’, which may mean that physicians relate justification ofthe threat of coercion to the consequences of refusing medication in terms of treat-ment (i.e. the patient’s illness). Nurses, however, may talk about the threat of coer-cion in terms of how this may affect their relationship with the patient.
The more negative attitude to the use of coercion demonstrated by the womenin this study shows consistency with, for example, Gilligan´s theory of moralthinking. ‘Connectedness’, expressed by the question that women ask: ‘How shallI respond to the other?’, demonstrates a moral orientation of doing ‘good’ for the‘other’. According to Gilligan’s theory,16 because women’s moral orientation is
at University Library Utrecht on June 2, 2014nej.sagepub.comDownloaded from

528 K Lützén, A Johansson and G Nordström
Nursing Ethics 2000 7 (6)
towards the other, the main source of moral conflict for women arises in inter-personal relationships. Thus, the responses in this study may mean that otherstrategies, such as taking time to be with and to talk to patients, are more favouredby female professionals.
Significant differences were also found between female and male professionalsregarding the dimension concerned with structuring moral meaning. Female pro-fessionals agreed more than male professionals, for example, with the assump-tion: ‘If I should lose a patient’s trust I would feel that my work would lackmeaning.’ If moral meaning is primarily embedded in the interpersonal relation-ships, is this more of a concern for women?
One would expect that to experience meaning, especially in contacts withpatients who do not respond in a positive way, express gratitude or make theirown wishes known, is difficult for all health care professionals. The more demand-ing the interpersonal relationship becomes, the more a person needs to experi-ence moral meaning in order to feel that all that is done is not futile. In our study,nurses employed in general medical settings would find work meaningless (indi-cated by a higher score to questions in this category) if they never saw anyimprovement in their patients. In contrast, nurses in psychiatric settings agreedto a lesser extent. Is this because nurses in psychiatric care find meaning in theirwork because chronic mental illness is a reality that they have come to accept?Another way to phrase the question is: do nurses in general settings choose theirspecific field because of their need to feel moral meaning by experiencingimprovement in their patients?
In order to develop rigorous study designs and self-administered measure-ments, the conceptual underpinnings must be clearly formulated and attempt tocommunicate a common meaning. The different theories of ethics (e.g. quandaryethics, virtue ethics, principle-based ethics) are not easily operationalized becauseof the problem of definition of the terms associated with moral values. Moreover,attempts to identify gender differences are methodological as well as socially con-troversial, as the research of Gilligan and Attanuci16 has shown.
The theoretical and methodological problems that ethics research poses doesnot means that ethics should be rejected as a topic for empirical research. Rather,one goal of ethics research could be directed towards achieving an understand-ing of the variations in opinions or attitudes related to ethical issues in health carepractice, rather than evaluating what attitudes are right or wrong. Ethical enquiry,as a developing area of empirical research in health care, explores the basic moralnorms that underpin practice, research and education. However, whether femaleand male health care professionals respond to ethical problems according to con-text, gender or professional role is a complex question and needs to be related toits relevance for practice. Moreover, the consequences of agreeing on all ethicalissues needs to be reflected upon; for example, does team consensus foster criti-cal thinking and individual accountability in practice?
The research approach in this study was basically descriptive in its design (i.e.focusing on describing in general what persons think about ethical issues).However, the study’s limitations should not be ignored. The differences may notbe consistent in other populations, or in other social or cultural settings. Anotherapproach could be to focus on gaining in-depth knowledge about specific prob-lems that are experienced in health care practice and how the interaction between
at University Library Utrecht on June 2, 2014nej.sagepub.comDownloaded from

Moral sensitivity: differences between nurses and physicians 529
Nursing Ethics 2000 7 (6)
staff surrounding the patient influences decision making. For example, an ethno-graphic qualitative approach, using the strategy of participant observation in spe-cific health care settings, would be appropriate. Dialogue between researchers andpractitioners would give contextual depth and details of ethical problems that aquestionnaire cannot achieve. Nonetheless, the use of multiple research methodsshould be encouraged if the aim is to achieve a greater understanding of ethicalproblems in practice. This understanding is a priori to developing teaching andpractice interventions.
Regardless of the theoretical and methodological difficulties that do not lendthemselves to generalizations, some conclusive statements can be made. The dif-ferences that were found may or may not be perceived as in the best interest ofpatients, depending on the perspective. Specifically, moral consensus and agree-ment about ethical principles is necessary in health care in order to optimizestability and just care for all patients. The findings in this study imply, to someextent, the opposite. The other perspective is that, as the results indicate, nursesand physicians are indeed sensitive to different aspects of patient care; they mayalso engage in critical moral reflection from these different aspects. To connectHekman’s claim of multiple moral voices17 to the concept of moral sensitivity,future investigations would benefit from an approach that does not place adisclaimer on different ways of thinking about ethical problems in health carepractice.
Kim Lützén, Karolinska Institutet, Stockholm, Sweden.Agneta Johansson, Karolinska Hospital, Stockholm, Sweden.Gun Nordström, Karolinska Institutet, Stockholm, Sweden.
References1 Rickard M, Kuhse H, Singer P. Caring and justice: a study of two approaches to health care
ethics. Nurs Ethics 1996; 3: 212–24.2 Jameton A, Fowler M. Ethical inquiry and the concept of research. ANS Adv Nurs Sci 1989;
11(3): 11–24.3 Charon J. Symbolic interactionism. Old Tappan, NJ: Prentice Hall, 1997.4 Lützén K. Moral sensitivity, a study of subjective aspects of moral decision making in nurs-
ing practice [Dissertation]. Stockholm: Karolinska Institute, 1993.5 Carpenter MA. The process of ethical decision making in psychiatric nursing practice. Issues
Ment Health Nurs 1991; 12(2): 179–91.6 Smith K. Ethical decision making in nursing: implications for continuing education. J Contin
Educ Nurs 1996; 27: 42–45.7 Lützén K, Evertson M, Nordin C. Moral sensitivity in psychiatric practice. Nurs Ethics 1997;
4: 472–82.8 Lützén K, Nordström G, Evertson M. Moral sensitivity in nursing practice. Scand J Caring
Sci 1995; 9: 131–38.9 Homenko DF. Overview of ethical issues perceived by allied health professionals in the
workplace. J Allied Health 1997; 26: 97–103, 10 Söderberg A, Norberg A. Intensive care: situations of ethical difficulty. J Adv Nurs 1993: 18:
2008–2014, 11 Lützén K, Nordin C. Conceptualisation and instrumentation of moral sensitivity in psychi-
atric nursing practice. Int J Methods Psychiatr Res 1994; 4: 241–48.12 Lützén K, Nordin C. Modifying autonomy, derived in a grounded theory study of
nurses’ experience of moral decision making in psychiatric settings. J Med Ethics 1994; 20:101–107.
at University Library Utrecht on June 2, 2014nej.sagepub.comDownloaded from

530 K Lützén, A Johansson and G Nordström
Nursing Ethics 2000 7 (6)
13 Oddi LF, Cassidy VR, Fisher C. Nurses’ sensitivity to the ethical aspects of clinical practice.Nurs Ethics 1995; 2: 197–209.
14 Grundstein-Amado R. Differences in ethical decision making processes among nurses anddoctors. J Adv Nurs 1992; 17: 129–37.
15 Peter E, Gallop R. The ethic of care: a comparison of nursing and medical students. IMAGEJ Nurs Schol 1994; 26: 1: 47–51.
16 Gilligan C, Attanuci J. Two moral orientations. In: Gilligan C, Ward J, Taylor J, eds. Mappingthe moral domain. Cambridge, MA: Harvard University Press, 1988.
17 Hekman SJ. Moral voices moral selves: Carol Gilligan and feminist moral theory. Cambridge:Polity Press, 1995.
Stop press
Professor Kim Lützén, member of the editorial board and Dean, Department ofNursing, Ersta-Sköndal University College, Stockholm, Sweden, has been elected asa Governor on the Board of the World Association for Medical Law. She is the firstnurse ever to be elected to that organization and did so with a huge majority.Congratulations and best wishes to Kim.Ed.
at University Library Utrecht on June 2, 2014nej.sagepub.comDownloaded from