Embed Size (px)
Citation preview

234 Review Article DOI: 10.1111/j.1610-0387.2009.07219.x
JDDG | 4˙2010 (Band 8) © The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0804
JDDG; 2010 • 8:234–242 Submitted: 2.6.2009 | Accepted: 17.7.2009
Keywords• morgellons• delusional parasitosis• delusional infestation• skin
SummaryDelusional parasitosis (DP) is the most frequent delusional disorder in derma-tology. In DP there is a fixed belief of a usually skin-related invasion or infesta-tion by a number of alleged infectious species (usually parasites and bacteria),whose identity has varied over the decades. Since 2002 worldwide an increas-ing number of patients have complained of unverifiable fibers and filaments inor on the skin, associated with numerous nonspecific complaints (arthralgias,altered cognitive function and extreme fatigue). This entity has been named“Morgellons disease” by the patients themselves, although medical evidencefor its existence is lacking. As an example, we discuss a 55-year-old woman whocomplained of Morgellons disease and was treated as if she had DP. Currentlythe delusional assumption of infestation with Morgellons should be consid-ered as a new type of DP with some kind of inanimate material. We thereforerecommend in case of DP including Morgellons the use of the broader term“delusional infestation”.
Morgellons in dermatologyWolfgang Harth1, Barbara Hermes2, Roland W. Freudenmann3
(1) Department of Dermatology and Allergology, Vivantes Klinikum Berlin Spandau, Germany(2) Department of Dermatology and Phlebology, Vivantes Klinikum Berlin Friedrichshain, Germany(3) Ulm University Hospital, Department of Psychiatry and Psychotherapy III
IntroductionSomatic delusions are among the mostdifficult conditions to treat in dermatol-ogy, not in the least due to the fact thatmost patients refuse psychiatric help,falsely believing their disorder is the re-sult of somatic causes and thus demand-ing diagnosis and treatment of a somaticcause rather than accepting the psychi-atric nature of their symptoms [1]. Anexample is delusional parasitosis (DP), acondition in which patients are con-vinced they are infestated by a pathogen,parasite, or small organisms [2–4]. Thetype of medical advice sought by the pa-tient is based on the logic and actual con-tent of the delusion: patients who thinkthere is skin infestation may consult adermatologist, while those who think
their nose is asymmetrical may see a plas-tic surgeon. Only in more mild cases, orif the patient becomes more receptive,for instance under antipsychotic medica-tion, do patients accept a referral for psy-chiatric evaluation.Traditionally, delusions are defined ac-cording to the three criteria proposed byKarl Jaspers [5]:1. “extraordinary conviction” and “in-
comparable, subjective certainty”,2. “imperviousness to other experiences
and to compelling counter-argument”,3. “their content is impossible”.For clinical and psychiatric practice, thesecond criterion is the most helpful.Delusional disorders affecting the skin(Table 1) may be divided into threegroups [6]:
1. Delusions that strictly concern dermatology: delusional parasitosis,dysmorphic delusions, other body- related delusions such as an obsessionwith one’s own body odor withbromhidrosis or chromhidrosis, ortactile hallucinosis.
2. Delusions that are often seen by derma-tologists or other specialists: hypochon-driac delusions about syphilis, cancer,AIDS, or other disorders
3. Patients with chronic delusions whodevelop additional dermatologicalsymptoms.
Delusional disorders are rare, with an estimated annual incidence of 0.7–3.0 per100 000 inhabitants in the general pop-ulation [7]. The incidence of the mostcommon delusional disorder seen in

Morgellons disease Review Article 235
© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0804 JDDG | 4˙2010 (Band 8)
dermatology, delusional parasitosis, af-fects an estimated 2.37–17.0 per 1 mil-lion inhabitants per year [8, 9]. Delu-sional parasitosis usually affects womenbetween the ages of 50–80 years [9].In recent years, a growing number of pa-tients in the United States have reportedunproven infestation of the skin withsmall fibers. The source of the disorder isattributed to dermatological and infec-tious causes. Unlike traditional forms ofdelusional parasitosis, the patients be-lieve the disorder is caused by inorganicparticles. These they refer to as Morgel-lons, a term coined in 2002 by an Amer-ican biologist named Mary Leitao whobelieved that her young son was affectedby the disorder [10].We report a patient in Germany withMorgellons in order to bring this disorderto the attention of practicing dermatolo-gists, and because the advent of this phe-nomenon makes it advisable to changethe name “delusional parasitosis” whichdoes not properly cover Morgellons.
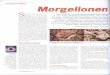
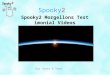
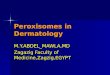
Case reportPatient historyA 55-year-old woman visited our derma-tology department for the first time inJune 2007 with severe ulcers on the face(Figure 1). At the time she stated thatthere were fibers and barbs emergingfrom the skin on the lesional area of theface and that these were causing the ul-cers. Symptoms had begun two years be-fore with fatigue, weakness, diminishedcoping ability, night sweats, dizziness,headache, earache, and pressure in theright paranasal sinus. These symptomswere followed by swelling, burning,stinging and itching, first affecting theface and then involving the throat andneckline. Two months later the patientdeveloped non-healing ulcers on thechin, upper lip, and nose, which thenspread over the entire face (Figure 1).The patient reported finding stinging,very thin barb-like and fiber-like ele-ments in the open sores. She also pro-vided samples for testing of the pre-
sumed cause (matchbox sign, Figure 2),explaining that she had collected the ma-terial from affected areas of the skin witha special pair of tweezers and with nee-dles (Figure 3). One year before she hadhad lower abdominal symptoms and in-fection of the genital area. After a stooltest was “positive” for Candida she wastreated with oral nystatin. Then, over thecourse of a year, she was treated continu-ously with fluconazole, itraconazole,ciprofloxacin, minocycline, moxi-floxacin, and acyclovir, although it is un-clear how she got the drugs. She hadconsulted 18 physicians in various fields,none of whom could help her.
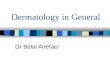
Clinical presentationClinical examination revealed linear ul-cerations with crusts on the face, neck,and upper chest (Figure 1).Bacteriology: Detection of Staphylococcusaureus. Mycological tests were negative.Histology: Mostly normal histological ap-pearances of the skin (Figure 4a).Laboratory values: Routine laboratorychemical and additional diagnostic stud-ies were normal with the exception of adrug-induced increase in transaminaseattributable to medication misuse (an-tibiotics, antifungal agents, antiviraldrugs), which was later addressed by thepatient during psychotherapy and psy-chiatric counselling.
Psychiatric symptoms There were no previous psychiatric prob-lems in the patient’s medical history. Shewas married and worked in an office.There were no indications of alcohol de-pendence or illicit drug use. Conscious-ness and orientation were normal andthere were no signs of dementia. Despitethe unshakable conviction that therewere fibers protruding from her skin(delusion), there were no major symp-toms of schizophrenia. The patient alsohad secondary depressive symptoms anda sleep disorder but no acute suicidal ten-dencies or dermatitis artefacta.
Therapy and courseGiven the large ulcerations on the face,the patient was admitted to the derma-tology unit in June 2007 for a 17-day-long hospital stay. After relapsing she wasadmitted to a dermatology day clinic forseveral weeks of therapy in the fall of2007. Initial inpatient treatment con-sisting of local therapy with a topical
Table 1: Psychiatric disorders with delusions in dermatology.
• Delusional parasitosis, F22.8 (coenaesthetic delusion/body hallucinations)
• Body odor delusion, F22.8 (odor hallucinations)
- Bromhidrosis (usually with presumed chromhidrosis: sweat discoloration)
• Hypochondriac delusions, F22.0 (delusion of syphilis, AIDS, cancer)
• Body dysmorphic disorder, F22.8 (delusional dysmorphophobia)
Figure 1: 55 year old female patient with delusional infestation in sense of Morgellons disease.

236 Review Article Morgellons disease
JDDG | 4˙2010 (Band 8) © The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0804
antiseptic (triclosan) and promograncovered with a polyurethane wounddressing. This led to rapid stabilizationof the patient’s condition.Using a simple behavioral therapy ap-proach, a good physician-patient rela-tionship was established and the patientagreed to keep a diary of manipulation ofthe skin lesions. The diary consisted ofthree columns with the date, length ofmanipulation in front of the mirror(minutes) and the related situation (e.g.,before going to bed at night) and emo-
tion (e.g., anger). The diary was thenevaluated during the next visit with thepatient. The diary showed that the pa-tient spent up to 3 hours a day trying toremove fibers from her skin with a pairof tweezers. She remained convincedthat subepidermal fibers were emergingfrom the skin and causing the ulcera-tions; upon further questioning she gavea highly detailed description of theprocess (Figure 4b–6). The patientagreed to continue to record the lengthof manipulation and to try to reduce the
time spent manipulating her skin. Shewas unsuccessful, however, and lateragreed to a psychiatric consultation. Shewas hospitalized for initial administra-tion of the necessary antipsychotic drugs.Therapy consisted of the sedating (anti-histaminergic) and antipruritic (anti-his-taminergic, anti-opioidergic) tricyclicantidepressant doxepin (50 mg daily) totreat restlessness, sleep disorder, and de-pressive mood, as well as clomipramine(50 mg daily) to treat the ritualized-ob-sessive behavior. A dosage increase wasnot possible due to adverse effects anddue to inadequate effectiveness. Giventhat the disorder was primarily delusional and failed to respond to anti-depressants, the local psychiatrist prescribed the atypical antipsychoticrisperidone (initial dose of 0.5 mg, increasing to 2 mg daily) which waseventually given in combination withparoxetine (20 mg daily). Under thiscombination therapy partial healing ofskin lesions was gradually achieved oversix weeks. The patient’s mood improvedand anxious/obsessive as well as delu-sional symptoms were diminished butdid not fully remit. The patient beganoutpatient behavioral therapy (25 hoursto start). After she was released from thehospital and had terminated day hospitalcare, the patient relapsed upon decidingto stop psychopharmacotherapy. Deepulcerations again developed which requiredlocal antiseptic treatment (Figure 7). At herlast visit at the end of 2008, the patientstill did not do well, in part due to hernon-adherence to the prescribed psychi-atric medication.
DiscussionIn 1938 the Swedish psychiatrist Karl-Axel Ekbom introduced the German term“Dermatozoenwahn” for a disorder whichhad been recognized since the end of the19th century [11]. In English it is usuallyreferred to as “delusions of parasitosis” (or “delusional parasitosis”) as coined byWilson & Miller [12]. The condition isalso refered to by various other names. Because the presentations of DP vary, thecurrent diagnostic system for psychiatricdisorders includes various diagnoses (puredelusional parasitosis which cannot be explained by any other known disease,disorder or intoxication is diagnosed as“persistent delusional disorder” ICD-10F22, while, for example, with an underly-ing organic brain disease such as vascular
Figure 2: Matchbox sign: Fibre of the skin presented by the patient as assumed cause of the disease.
Figure 3: Tweezers used to remove the fibers.

Morgellons disease Review Article 237
© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0804 JDDG | 4˙2010 (Band 8)
encephalopathy it is diagnosed as organichallucinosis F06.0) [13]. In all forms, patients believe their symp-toms are due to tiny organisms. Some aretruly incapable of believing otherwise(true delusion), but often patients aremerely unwilling (overly convinced oftheir belief ) to accept that there is no in-festation. Diagnosis is based on lackingevidence of a true infestation in derma-tological and parasitological investiga-tions [3]. Artificial lesions usually arisewhen the patient tires to eliminate theresponsible agent from the skin. A fur-ther diagnostic characteristic is that up to26 % of patients, including ours, bringthe “evidence” in a small box (matchboxsign) to the consultation [8]. In 2009 allof our patients who were diagnosed withthe disorder (9 out of 9) provided a sam-ple during the first visit or after beingasked to do so.
Patients often complain of tactile skinsensations and dysesthesias such as itch-ing, burning, stinging, or crawling sensa-tions. These are interpreted as evidenceof organisms on the skin (which sting,eat, run, crawl, etc.). Sometimes theterm “chronic tactile hallucinosis” is usedinstead of “delusional parasitosis”, al-though this term is problematic from apsychopathological view [6]. Ratherthan stressing the delusion, it suggeststhat tactile dysesthesias may be the pri-mary symptom which, however, has notbeen found to be true in all cases [6].Retrospective studies show that into the1990s patients believed the disorder wascaused mainly by insects (63–84 %),worms (11–14 %), bacteria (2–20 %),fungi (1–6 %), viruses, or other parasites[8]. The cause continued to change withthe times, however, similar to other delu-sional disorders. At the end of the 19th
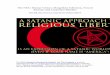
century, infestation was presumed to bewith “scabies.” Later patients believed itto be with insects, spiders, worms, orparasites, and ultimately with bacteria,fungi, and viral agents. In the past, imag-inary infestation was believed to be withsmall or microscopic living pathogens.There were also isolated reports of delu-sions of infestation with dead or anor-ganic material such as pigments, dust,sand or points [14] (Figure 8).There are now increasing reports ofsymptoms of presumed fibers, splinter-like elements, or particle infestation (or-ganic or anorganic) which are now beingreferred to by the patients as “Morgel-lons” [10] a term coined by Mary Leitaoand the patient-supported organization“Morgellons Research Foundation”(MRF, www.morgellons.org) which isactive politically and in the media (firstpublication on MRF in a dermatologyjournal was in 2006) [15] and which actsas a platform for the exchange betweenpatients. The MRF has succeeded ingenerating an immense amount of inter-est in the media for this “strange new dis-ease” as well as political pressure andcontributions for a significant amount ofresearch by the Centers for Disease Con-trol (www.CDC.gov) [10, 16, 17].There is also further evidence from theUnited States that the role of the mediaand Internet forums play a major role inspreading the delusion that Morgellonsis a disease. This phenomenon, also re-ferred to as a “socially transmitted dis-ease over the Internet”, or “cyberchon-dria”, or (less fittingly) “folie àInternet”, should be critically viewedand observed by physicians [17]. A visit to various Web sites is telling(www.morgellons.org, www.morgellons-research.org). People registered on theInternet (currently 13 600) are appar-ently convinced that they have a mysteri-ous new disease of unknown origin; theyfeel that the failure to diagnose it oridentify a cause is due to the incompe-tence of physicians. Despite lackingmedical or scientific confirmation of theexistence of Morgellons, the rapid dissemination of information via the In-ternet has fed an increase in the numberof patients, and the phenomenon hasspread to Great Britain and Europe [17].Morgellons is presently defined by affected patients and the MRF as infesta-tion of the body with unknown fibers,threads, or filaments associated with
Figure 4: Same patient: Regular picture of skin biopsy (a). Histological drawing of the patient withassumed pathogenesis of the ulcerations by fibers (b).

238 Review Article Morgellons disease
JDDG | 4˙2010 (Band 8) © The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0804
multiple symptoms affecting the entirebody, including arthralgia, fatigue, andconcentration disorders. The employeesof the MRF have also suggested connec-tions with various other organisms (including Borrelia) and some Internetpages also contain links to conspiracytheories. There is still no evidence sup-porting the theories of the MRF, andfrom a medical point of view, there is noevidence for any organic or infectiousdisease so far. Until there is no better ex-planation symptoms in Morgellons canbe considered to be delusional. TheCDC study on Morgellons patients,
which is searching for actual and system-atically detectable pathogens, is still un-derway [15].This new type of delusional disorder ispresumably much more common thanwas thought. In some patients the delu-sion may be identified only after carefulquestioning, while others are self-diag-nosed with Morgellons and refer to In-ternet pages to support their claim. In2009, of the nine patients seen at theDermatology Department in Berlin(Spandau) who were diagnosed withdelusional parasitosis, two (22.2 %) re-ported presumed particle infection upon
further questioning (splinter-like parti-cles, fibers).In the above, we have described a typicalpatient with primary DP who presentedwith a matchbox sign and severe skin le-sions, doctor-hopping, and self-treat-ment. As is often the case, her firm con-viction that her skin was infestated byfibers made treatment difficult and re-sulted in a lack of adherence to the treat-ment regime. A special feature of thiscase is the variation within the delusionaltheme “infestation”. Rather than an in-festation with parasites or other small liv-ing organisms, the patient believed thatthere was infestation with inanimatefibers and splinters, which could how-ever move like live organisms and causevarious moving tactile sensations.The term “delusional parasitosis”, whichis restricted to living pathogens such asparasites, is thus disadvantageous giventhese new developments as it does notinclude other forms of infestation (suchas fibers). Thus, based on psychopatho-logical, historical, and epidemiologicalfactors, the Morgellons phenomenonmay be viewed as a new variation on the delusional theme of “infestation”.The authors therefore suggest using thebroader term “delusional infestation” instead of “delusional parasitosis” be-cause the former includes infestation notonly with all forms of organic (mucous,discharge, organic structures, organicfibers) but also non-organic materialswhich are increasingly seen in recentyears (fibers, Morgellons, salts, metals,etc.) (Figure 8 and Table 2).
Clinical appearanceSelf-inflicted skin damage is reported inup to two-thirds of patients with delu-sions of infestation (any type). Lesionsare produced by manipulation of theskin in an attempt to remove the para-sites [18].The clinical appearances of self-inflicteddamage vary and depend on the type ofmanipulation as well as any devices orsubstances used. Clinical examinationusually reveals excoriations or cuts orartefacts from tweezers. Aggressivechemicals are often used, sometimesfrom veterinary medicine; these are ap-plied to the skin to eliminate microbes[19]. The skin is usually severely dam-aged by frequent cleansing rituals andthe use of aggressive substances to fightthe parasites or pathogens, and it is often
Figure 5: Drawing of the patient with fiber and spike infestation of the epi- and subepidermal skin:Lump with inflammation; Pseudoskin surface formed by fibers, crusts, keratinization; Fluid-filled blis-ters, grape-like clusters, ca. 0.5–1 mm diameter; Hair loss due to pathologically changed skin surface;Circular arrangement, large lesion in the center with 5 smaller ones surrounding it; also overlappingdiameter 5 mm–2.5 cm; funnel-like depression in upper skin layers; Spikes, much thinner than a hair,needle point, stinging if pressure applied; fibers; swelling with inflammatory skin changes.

Morgellons disease Review Article 239
© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0804 JDDG | 4˙2010 (Band 8)
very dry with exsiccation eczema. Pa-tients usually consult numerous physi-cians and healthcare providers and oftenalso have elaborate disinfection habits.
Psychiatric symptomsDelusions are often a manifestation ofanother underlying psychiatric disorderand are hence referred to as “secondarydelusions.” Somatic delusions occur inparanoid disorders (20 %), depressive(50 %) disorders, brain disease, withdelirium and after toxic effects, but theycan also occur alone without an underly-ing disorder [20].Delusion is not a diagnosis, but a symp-tom. If symptoms occur alone, a “pure”or “primary” delusional disorder is present,fulfilling the ICD-10 diagnostic criteriaof a persistent delusional disorder (ICD-10 F22) [2].Three forms of delusional parasitosismay be distinguished based on researchby Musalek. These are divided by specificdelusional content:1. hypochondriac delusional parasitosis
as a monosymptomatic hypochon-driac psychosis,
2. parasitosis with symptoms of paranoia,3. mixed forms of 1 and 2 [21].These pathogenetic and psychopatho-logical differences between the variousforms of delusional parasitosis are important for the overall treatment approach and for targeted treatmentwith a psychopharmaceutical agent (antidepressant versus neuroleptic). In 5–15 % of patients with delusionalparasitosis an associated delusion is in-duced in a person close to the patient(folie à deux, folie à trois) [22, 23]. Pa-tients suffer considerably as a result ofthe delusion, and the quality of life of thepatient and family members is severelyimpaired.
PathogenesisThe etiology of delusional disorders ismultifactorial and – as in the majority ofpsychological delusions – is primarily de-scribed using a biopsychosocial model ofdisease [24]. A possible disease model isthe vulnerability-stress model, in which asubclinical congenital or acquired multi-factorial predisposition to disease (prob-ability of developing the disorder) exists,and the disorder manifests when otheradditional factors (stress/conflict or bio-logical “stressors”) come into play [1].
Figure 6: Delusional step-by-step explanation of a perforating skin disease with exportation of spikesand fibers: Chin, right, hole since 3.6.07; Hole ca. 4 mm in diameter; Smooth skin on the sides withspikes – depressions in upper skin layers; Spikes ca. 1 mm or smaller, pus, grape-like encapsulated clus-ters; fluid-filled blisters, clusters of lesions; depression in upper skin layers, flattened out in 4.
Figure 7: Recurrent deep ulcer after dropping out therapy with Risperidone and Paroxetine.

240 Review Article Morgellons disease
JDDG | 4˙2010 (Band 8) © The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0804
Thus initial symptoms may arise after ac-tual parasite infection, media reports, orpersonal observation, such as pediculosisin a granddaughter, which then triggersthe delusion. Markus Huber suggestedthe hypothesis of a quantitative and/orqualitative disorder of the presynapticdopamine transporter (DaT), which isresponsible for the resorption ofdopamine in the presynaptic neuron[25]. If mediated by pathologically ele-vated dopamine availability, dysfunctionof DaT could presumably lead to psy-chotic symptoms.
Differential diagnosisSecondary delusional parasitosis must beexcluded which is due to another psychi-atric or organic brain disease or intoxica-tion, e.g., schizophrenia, organic psy-chosyndromes of the brain includingcerebral sclerosis and dementia.Differential diagnosis also includes so-matoform disorders such as sensory
symptoms with burning and itching,artefacts, and neurotic excoriations aswell as pruritic disease, which can alsohave delusional components. There is of-ten a combination of hypochondriacdelusion, especially in fungal infection;the idea can arise after media reports andinfections among friends or relatives orpets. Obsessive disorders must also beruled out – especially in compulsivewashing or compulsive manipulation ofthe skin. Pure artefacts such as self-harm-ing behavior are an important differen-tial diagnosis [26]. Mechanical injuriesoften occur as a result of squeezing, rub-bing, itching, cutting, or piercing or dueto related infection with delayed woundhealing.
TherapyAt the beginning of therapy, contact withthe patient should be made carefully andin a non-confrontational manner. To es-tablish a good therapeutic relationship,
physicians should not question the pa-tient’s belief in his or her disorder, even ifhe or she seems to be obviously mis-taken. Nor should the presence of thedisorder be accepted or confirmed. Ther-apy can commence with a non-irritatinglocal therapy for wound healing and forsymptomatic and bland treatment ofself-induced lesions. Samples providedby the patient should be carefully andthoroughly inspected and parasitologicaland microbiological testing should al-ways be performed in order to help gainthe trust of the patient. Premature con-frontation or embarrassing accusationsshould be avoided as these threaten toend the doctor-patient relationship andlead to a “physician odyssey.“ The needfor psychiatric or psychotherapeutictherapy should only be suggested afterthe patient’s trust has been gained. Treat-ment should continue until the patientcan be motivated to use a specific ther-apy, usually a combination psychi-atric/psychosomatic therapy. Treatmentof delusional parasitosis with initiationof a psychopharmacological therapy canbe particularly effective in a liaison con-sultation at the dermatology departmentincluding the dermatologist, psychia-trist, and patient.
Psychopharmaceutical agentsPsychopharmaceuticals have signifi-cantly improved the prognosis for pa-tients with delusional parasitosis [9].Treatment is usually multimodal (psy-chiatric, dermatological). The choice ofagent depends on the underlying psychi-atric disorder and symptoms. If depres-sion is the main symptom, an antide-pressant is given; for delusionalsymptoms a neuroleptic agent is thedrug of choice [27]. Only a few con-trolled studies are available and there areno large randomized placebo-controlledstudies [3], partly because patients canbarely adhere to the treatment protocolfor a clinical study. Most of what weknow is therefore based on case reports.The following medications are currentlyused in delusional disorders in dermato-logical patients, although none is ap-proved for such use: risperidone, olanza-pine, quetiapine and the olderpimozide. Pimozide has the longest his-tory of use in antipsychotic therapy ofdelusional parasitosis [28]. Yet due to itsrisk profile, including cardiac and ex-trapyramidal symptoms, it is no longer
Table 2: Broader delusional contents in delusion of parasitosis (delusionalinfestation).
Pathogen• Parasites: mites, ticks, worms• Infections: bacteria, fungi, viruses
Particles• Organic discharge, fibers, splinters, objects, particles• Anorganic substancces: splinters, spikes, sand, salts, metal pigments
Figure 8: Another patient with Morgellons-Disease presenting salt crystals as assumed pathogeneticcause coming out of the skin.

Morgellons disease Review Article 241
© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0804 JDDG | 4˙2010 (Band 8)
considered a first-line antipsychoticagent in general (not only in delusionalparasitosis) and should only be used as asecond-line option. Safer first genera-tion antipsychotic drugs includehaloperidol, perphenazine, andsulpiride. Second generation antipsy-chotic agents (“atypicals”) are often bet-ter tolerated, especially with regard toextrapyramidal motor symptoms, buthave other specific risks (e.g., metabolicdysfunction). In primary and secondarydelusional parasitosis (with the excep-tion of dementia-associated psychoses)risperidone has the most positive reportsand the best chances of success [29].Even if treated effectively and some in-sight into the nature of the conditioncan be achieved, however, the majorityof patients does not completely acceptthe diagnosis. Symptoms can neverthe-less almost always be alleviated to suchan etxtent that the patient can again fo-cus on other thoughts and lead a life notonly dominated by the imagined infesta-tion and the fight against it. Treatmentmay be considered successful if the delu-sion has been “quieted” and “if the topicof infestation does not preoccupy thepatient as much.” Complete remissionof the delusional belief is achieved inonly 33.5–51.9 % of patients with delu-sional parasitosis (minimum of threemonths without or with minimal symp-toms) [9]. Partial remission (the criteriaof the disorder are no longer fulfilled,but more than mild symptoms remain)or complete remission can be achievedusing second generation antipsychoticdrugs (risperidone, olanzapine, etc.) inup to 75 % of patients with delusionalparasitosis [29].
ConclusionPatients with delusional disorders, inparticular delusional parasitosis, may ini-tially consult a dermatologist given so-matic symptoms and denial of any psy-chopathological cause. Morgellons,which is widely discussed on the Internetby self-diagnosed patients, involves theinfestation with fibers and other non-or-ganic or organic particles, and can beconsidered to be a new manifestation ofdelusional parasitosis or, better, delu-sional infestation. It is a new phenome-non that has received little attention inthe medical until now. It will present cli-nicians in various fields with new chal-
lenges. The media as well as various In-ternet forums may help spread specificdelusions and should be watched care-fully in the future. <<<
Conflict of interestNone.
Correspondence to
Priv.-Doz. Dr. med. Wolfgang HarthKlinik für Dermatologie und AllergologieVivantes Klinikum, Berlin SpandauNeue Bergstraße 6D-13585 BerlinTel.: +49-30-130-13-1551E-mail: [email protected]
References1 Harth W, Gieler U, Kusnir D, Tausk F.
Clinical Management in Psychoderma-tology, Springer, New York, 2009.
2 Freudenmann RW. Der Dermatozoen-wahn. Eine aktuelle Übersicht. Fort-schr Neurol Psychiatr 2002; 70:531–41.
3 Lepping P, Russell I, FreudenmannRW. Antipsychotic treatment of delusional parasitosis: a systematic review. Br J Psychiatry 2007; 191:198–205.
4 Lepping P, Freudenmann RW. Delusio-nal parasitosis: a new pathway for dia-gnosis and treatment. Clin Exp Derm2008; 33:113–7.
5 Jaspers K. Allgemeine Psychopatholo-gie, 9. Auflage, Springer, Heidelberg,1973.
6 Musalek M. Der Dermatozoenwahn.Thieme, Stuttgart, New York, 1991.
7 Manschreck TC. Delusional disorder:the recognition and management of pa-ranoia. J Clin Psychiatry 1996;57(Suppl 3): 32-8; discussion 49.
8 Trabert W. Der Dermatozoenwahn.Untersuchungen zur Häufigkeit, Klas-sifikation und Prognose, Habilitations-
schrift, Universität des Saarlandes,Homburg/Saar, 1993.
9 Trabert W. 100 years of delusional parasitosis. Meta-analysis of 1,223 casereports. Psychopathology 1995; 28:238–46.
10 Accordino RE, Engler DI, Ginsburg H,Koo J. Morgellons disease? DermatolTher 2008; 21: 8-12.
11 Ekbom KA. Der praesenile Dermato-zoenwahn. Acta Psychiatr NeurolScand 1938; 13: 227–59.
12 Wilson JW, Miller HE. Delusions ofparasitosis (acarophobia). Arch Derma-tol 1946; 54: 39–56.
13 Weltgesundheitsorganisation. ICD-10– Internationale statistische Klassifika-tion der Krankheiten und verwandterGesundheitsprobleme, 10.Revision,Band 1, Deutscher Ärzte Verlag GmbH,Köln, 1995.
14 Harbauer H. Das Syndrom des Derma-tozoenwahns (Ekbom). Nervenarzt1949; 20: 254–8.
15 Savely VR, Leitao MM, Stricker RB.The mystery of Morgellons disease: in-fection or delusion? Am J Clin Derma-tol 2006; 7: 1–5.
16 Koblenzer CS. The challenge of Mor-gellons disease. J Am Acad Dermatol2006; 55: 920–2.
17 Paquette M. Morgellons: disease or de-lusions? Perspect Psychiatr Care 2007;43: 67–8.
18 Hillert A, Gieler U, Niemeier V, BrosigB. Delusional Parasitosis. DermatoloPsychosom 2004; 5: 33–5.
19 Harth W, Gieler U. PsychosomatischeDermatologie, Lehrbuch und Bildatlas,Springer Medizinbuchverlag, Heidel-berg, Berlin, 2006.
20 Hornstein OP, Hofmann P, Joraschky P. Delusions of parasitic skin infesta-tion in elderly dermatologic patients. Z Hautkr 1989; 15; 64: 981–2, 985–9.
21 Musalek M. Wahnsyndrome in der Dermatologie. In: Gieler U, BosseKA (Hrsg.): Seelische Faktoren bei Hautkrankheiten. Bern: Huber, 1996.
22 Gieler U, Knoll M. Delusional parasi-tosis as folie a trois. Dermatologica1990; 181: 122–5.
23 Evans P, Merskey H. Shared beliefs ofdermal parasitosis: folie partagee. Br JMed Psychol 1972; 45: 19–26.
24 Koo J, Lee CS. Delusions of parasitosis.A dermatologist’s guide to diagnosis

242 Review Article Morgellons disease
JDDG | 4˙2010 (Band 8) © The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0804
and treatment. Am J Clin Dermatol2001; 2: 285–90.
25 Huber M, Kirchler E, Karner M, PychaR. Delusional parasitosis and the dopa-mine transporter. A new insight of etiology?Med Hypotheses 2006; 68: 1351–8.
26 Oostendorp I, Rakoski J. Mün-chausen’s Syndrom. Artefakte in der
Dermatologie. Hautarzt 1993; 44:86–90.
27 Harth W, Seikowski K, Gieler U, Niemeier V, Hillert A. Psychopharma-kologische Behandlung dermatologi-scher Patienten – wenn reden alleinnicht hilft. J Dtsch Dermatol Ges2007; 5: 1101–6.
28 Damiani JT, Flowers FP, Pierce DK. Pi-mozide in delusions of parasitosis. J AmAcad Dermatol 1990; 22: 312–3.
29 Freudenmann RW, Lepping P. Second-generation antipsychotics in primaryand secondary delusional parasitosis:outcome and efficacy. J Clin Psycho-pharmacol 2008; 28: 500–8.