Embed Size (px)
Citation preview
doi:10.1093/brain/awh550 Brain (2005), 128, 1877–1886
Motor neuron pathology in experimentalautoimmune encephalomyelitis: studies inTHY1-YFP transgenic mice
P. G. Bannerman,1 A. Hahn,1 S. Ramirez,1 M. Morley,1 C. Bonnemann,1 S. Yu,2 G.-X. Zhang,2
A. Rostami2 and D. Pleasure1
1Neurology Research, Abramson Pediatric Research Center, Children’s Hospital of Philadelphia and 2Department ofNeurology, Thomas Jefferson Hospital, Philadelphia, Pennsylvannia, USA
Correspondence to: David Pleasure MD, Room 516H Abramson Research Building, The Children’s Hospital of Philadelphia,34th and Civic Center Blvd, Philadelphia, PA, USAE-mail: [email protected]
Using adult male C57BL/6 mice that express a yellow fluorescent protein transgene in their motor neurons,we induced experimental autoimmune encephalomyelitis (EAE) by immunization withmyelin oligodendrocyteglycoprotein peptide 35–55 (MOG peptide) in complete Freund’s adjuvant (CFA). Control mice of the sametransgenic strain received CFAwithout MOG peptide. Early in the course of their illness, the EAEmice showedlumbosacral spinal cord inflammation, demyelination and axonal fragmentation. By 14 weeks post-MOGpeptide, these abnormalities were much less prominent, but the mice remained weak and, as in patientswith progressive multiple sclerosis, spinal cord atrophy had developed. There was no significant loss of lumbarspinal cord motor neurons in the MOG peptide-EAE mice. However, early in the course of the illness, motorneuron dendrites were disrupted and motor neuron expression of hypophosphorylated neurofilament-H(hypoP-NF-H) immunoreactivity was diminished. By 14 weeks post-MOG peptide, hypoP-NF-H expressionhad returned to normal, but motor neuron dendritic abnormalities persisted and motor neuron perikaryalatrophy had appeared. We hypothesize that these motor neuron abnormalities contribute to weakness in thisform of EAE and speculate that similar motor neuron abnormalities are present in patients with progressivemultiple sclerosis.
Keywords: motor neuron; experimental autoimmune encephalomyelitis (EAE); dendrite; axonal degeneration;multiple sclerosis
Abbreviations: CFA = complete Freund’s adjuvant; EAE = experimental autoimmune encephalomyelitis; hypoP-NF-H =
hypophosphorylated neurofilament heavy; MAP2a = microtubule-associated protein 2a; MBP = myelin basic protein;MOG = myelin oligodendrocyte glycoprotein; PBS = phosphate-buffered saline; YFP = yellow fluorescent protein
Received February 11, 2005. Revised April 4, 2005. Accepted April 21, 2005. Advance Access publication May 18, 2005
IntroductionMultiple sclerosis is an immune-mediated disease character-
ized clinically by relapsing-remitting or progressive neurolo-
gical deficits, and pathologically by multiple plaques of CNS
inflammation and demyelination. While multiple sclerosis
was for many years considered to be primarily a myelin sheath
disorder, it is now clear that, as Charcot (1877) first observed,
axonal fragmentation is an important component of the dis-
ease (Trapp et al., 1998; Perry and Anthony, 1999; Bjartmar
et al., 2000, 2003). In vivo neuroimaging supports the concept
that loss of CNS axons contributes substantially to progressive
multiple sclerosis disability (De Stefano et al., 1998, 2001;
Edwards et al., 1999; Miller et al., 2002; Lin et al., 2003,
2004). Occasionally, neuronal perikarya are also lost in
multiple sclerosis (Peterson et al., 2001).
Experimental autoimmune encephalomyelitis (EAE) is
elicited in susceptible animal strains by immunization with
various myelin antigens. As in multiple sclerosis, pathological
features of EAE include foci of CNS inflammation, demy-
elination, and axonal blebbing, tortuosity and fragmenta-
tion (Slavin et al., 1998; Pitt et al., 2000; Kornek et al., 2001;
# The Author (2005). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: [email protected]
Dow
nloaded from https://academ
ic.oup.com/brain/article-abstract/128/8/1877/481392 by guest on 05 April 2019

Onuki et al., 2001). Reversible motor neuron dendritic
beading has also been observed during the acute phase of
myelin basic protein (MBP)-induced EAE in Lewis rats
(Zhu et al., 2003). Death of neurons has been documented
in greater detail in EAE than in multiple sclerosis. For
example, approximately one quarter of spinal cord ventral
horn neurons are lost in Lewis rats with MBP-induced
EAE (Smith et al., 2000) and neuronal apoptosis occurs in
the CNS of mice and rats with MBP- or myelin oligodendro-
cyte glycoprotein (MOG) peptide-induced EAE (Meyer et al.,
2001; Ahmed et al., 2002; Diem et al., 2003; Hobom et al.,
2004; Kanwar et al., 2004).
Our goal was to characterize motor neuron pathology in
EAE. To this end, we induced EAE in a transgenic line of
C57BL/6 mice expressing yellow fluorescent protein (YFP) in
the perikarya and processes of a variety of neurons, including
all motor neurons (Feng et al., 2000), by immunizing them
with a peptide homologous to residues 35–55 of rodent MOG
(MOG peptide) (Slavin et al., 1998; Onuki et al., 2001; Gran
et al., 2002; Zhang et al., 2003).
The intense perikaryal YFP fluorescence of spinal cord
motor neurons in these mice was helpful for motor neuron
counting and cell body size measurements, and facilitated
motor neuron localization of proteins of interest by dual
label fluorescence microscopy. Our results indicate that,
while these chronically weak MOG peptide-EAE mice do
not lose motor neurons, they do develop persistent motor
neuron dendritic abnormalities and late motor neuron
perikaryal atrophy.
MethodsThy1-YFP transgenic miceFounders for our colony of C57BL/6mice expressing a YFP transgene
driven by thy1 promoter elements (Feng et al., 2000) (thy1-YFP
mice) were obtained from Jackson Labs Bar Harbor, Maine, USA.
(B6.Cg-TgN(Thy1-YFPH)2Jrs).
MOG peptide-EAEWhile female mice are more susceptible than male mice to some
forms of EAE, preliminary observations demonstrated an approx-
imately equal clinical severity of MOG peptide-induced EAE in
female and male C57BL/6 thy1-YFP transgenic mice. Because it
was more efficient to generate males from our colony of these
mice, all our subsequent studies employed male thy1-YFP transgenic
mice. MOG peptide in complete Freund’s adjuvant (CFA) or CFA
withoutMOGpeptidewasadministered to thesemice at age3months.
Rodent MOG peptide (300 mg, amino acids 35–55, synthetic, reverse
phase chromatographically purified) in CFA containing 4 mg/ml of
killed Mycobacterium tuberculosis (Becton Dickinson Frankin Lakes,
NJ, USA) was administered by subcutaneous flank injection on
day 0, followed by tail vein administration of 75 ng of pertussis
toxin (List Biological Labs, Campbell, CA, USA) on days 0 and 2
post-immunization (Gran et al., 2002; Zhang et al., 2003). Control
mice received CFA and pertussis toxin, but no MOG peptide.
The mice were weighed and examined daily. Neurological deficits
were graded on a five-point scale (limp tail or waddling gait = 1; limp
tail and ataxia = 2; single limb paresis and ataxia = 2.5; single limb
paralysis = 3; single limb paralysis and paresis of second limb = 3.5;
full paralysis of two limbs = 4; moribund = 4.5; and death = 5) (Gran
et al., 2002; Zhang et al., 2003). MOG-EAE and control thy1-YFP
transgenic mice were sacrificed shortly after the onset of deficits
(14 days post-immunization), at peak mean clinical severity
(21 days post-immunization) and late in the course of their illness
(98 days post-immunization).
Spinal cord tissue fixation and processingMOG peptide-EAE and control thy1-YFP mice were anaesthetized
with ketamine/xylazine, then perfused via the heart with saline fol-
lowed by phosphate-buffered 4% (w/v) paraformaldehyde. Spinal
cords were removed, post-fixed at 25�C with phosphate-buffered
4% paraformaldehyde for 1 h, then transected in the mid-lumbar
region and processed for paraffin and cryostat sectioning. The par-
affin sections corresponded to spinal cord levels L5 and L6, whereas
the cryostat sections corresponded to spinal cord levels L5 and L4.
To prepare paraffin sections for fluorescence microscopy, spinal
cord was washed three times with phosphate-buffered saline (PBS)
post-fixation, dehydrated through ascending ethanol, cleared in
xylene, and infiltrated with Paraplast wax (Surgipath, Richmond,
IL, USA). Six mm transverse sections were collected on Superfrost/
Plus slides (Fisher Scientific Morris Plains, NJ, USA) and melted at
56�C for 20 min, then deparaffinized in xylene and rehydrated
through descending alcohols.
For cryostat sections, lumbar spinal cord was cryoprotected by
overnight immersion in 30% sucrose at 4�C prior to embedding in
OCT cryostat mounting medium (Miles Inc, Kankakee, IL, USA).
After freezing in 2-methylbutane cooled with liquid nitrogen, trans-
verse 10 mm cryostat sections were mounted on poly-L-lysine coated
slides.
Spinal cord immunohistologyThe primary antibodies used in this study are listed in Table 1.
Paraffin sections were deparaffinized and treated with 10% (v/v)
Triton X-100 in PBS for 30 min, then immunostained with
mouse monoclonal antibodies (mAbs) using a mouse-on-mouse
kit (Vector Labs Burlingane, CA, USA) as per the manufacturer’s
instructions. Binding of the biotinylated secondary layer to the prim-
ary antibody was detected with rhodamine-conjugated streptavidin
(diluted 1 : 100, Jackson Immunoresearch Labs, West Grove, PA,
USA). For combined detection of CD11b+ microglia/macrophages
or CD40+ lymphocytes and TUNEL (terminal deoxynucleotidyl
transferase-mediated dUTP nick end labelling) histochemistry for
intranuclear DNA nicking (Gavrieli et al., 1992; Ray et al., 2000),
frozen sections were incubated overnight with rat anti-CD11b or
goat anti-CD40 in block A [minimum essential medium containing
15 mM HEPES buffer, 10% foetal bovine serum (FBS) and 0.05%
sodium azide].
Detection of primary antibody binding was performed using
rhodamine-conjugated second antibodies. Then we applied a
minor modification of the TUNEL procedure (Gavrieli et al., 1992),
substituting Pacific blue-conjugated streptavidin for streptavidin
peroxidase (Yasuda et al., 1995). Following immunolabelling with
primary and secondary antibodies, all sections, both paraffin and
cryostat, were post-fixed with �20�C methanol, counterstained
(with the exception of the slides used for TUNEL) with the nuclear
1878 Brain (2005), 128, 1877–1886 P. G. Bannerman et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article-abstract/128/8/1877/481392 by guest on 05 April 2019

dye Hoechst 33258 (2 mg/ml in PBS, Sigma Chemical Co., St Louis,
MO, USA) for 3 min, and mounted in Vectashield.
Skeletal muscle immunohistologyCryostat sections (10 mm) of tibialis anterior obtained from anaes-
thetized mice prior to perfusion were fixed in 100% methanol for
20 s, pre-incubated in vehicle (10% FBS, 1· PBS, 0.1% Triton X-100)
for 1 h, and then incubated with primary antibodies diluted in vehicle
for 1 h, all at room temperature. Antibodies used were rabbit poly-
clonal AP5B3 (1 : 750) raised against alpha-actinin 3, which specif-
ically stains type 2B skeletal muscle fibres, and rabbit polyclonal
81864 raised against sacrospan to outline the sarcolemma of indi-
vidual muscle fibres (1 : 2500). The slides were then washed 3· for
20 min each with 1· PBS, and incubated with an Alexa fluor-labelled
secondary antibody at room temperature for 1 h in the dark. After
three additional washes, the slides were mounted in Vectashield.
Imaging and image analysisFluorescent images were captured with a Hamamatsu Orca-ER
digital camera mounted on a Leica DMR upright microscope or
by confocal microscopy with a Leica DM IRE2 HC fluo TCS 1-B-
UVmicroscope coupled to a Leica TCS SP2 spectral confocal system.
To evaluate numbers and sizes of motor neurons in EAE versus
control animals, laser scanning confocal microscopic scans were
performed on paraffin sections corresponding to spinal cord levels
L5 through L6. The areas of ventral horn YFP positive cell bodies
were measured using a Leica software program developed specifically
for the confocal system (Leica Microsystems, Heidelberg, Germany).
The area of ventral horn investigated mapped to motor neurons
innervating the following muscle groups: iliopsoas/sartorius,
quadriceps, adductors, hamstrings, gluteal and other proximal
muscles of the thigh, posterior compartment of the distal hind
limb (Vanderhorst and Holstege, 1997), i.e. the major muscle groups
controlling hind limb mobility. To standardize the measurements,
only perikarya in which the nucleus and nucleolus were in the plane
of the section were counted and measured (McPhail et al., 2004).
We devised a semi-quantitative scale to score the extent of motor
neuron dendritic pathology, employing microtubule-associated
protein 2a (MAP2a) immunostaining with the AP14 antibody.
The scorer was not provided with information as to whether a spe-
cimen was from an EAE or a control mouse; nor, in the EAE mice, as
to the duration and severity of EAE. A score of 0 (normal) was
assigned when most or all motor neuron dendrites were of normal
thickness and length. A score of + was assigned when the majority
of motor neuron dendrites were thinner than normal, a score
of ++ when the majority of motor neuron dendrites were shortened
or fragmented, and a score of +++ when the majority of motor
neuron dendrites were lost.
ResultsClinical features of MOG peptide-EAEControl thy1-YFP transgenic mice (n = 20) did not demon-
strate weight loss or neurological deficits at any point follow-
ing CFA injection. Thirty-four mice were immunized with
MOG peptide in CFA. Of these, four did not show weight loss
or neurological deficits at any point during the next 98 days;
these four were excluded from further analysis. In the remain-
ing 30 MOG peptide-injected mice, neurological deficits first
appeared 12–14 days post-immunization, preceded by 1 or
2 days of weight loss which averaged 10% of pre-symptomatic
body weight.
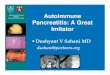
Five EAE mice and four CFA controls were sacrificed on
day 14 post-immunization. Clinical severity in the remaining
EAE mice peaked between days 19 and 21 post-immunization
(Fig. 1). Fifteen EAE mice and eight CFA controls were
sacrificed on day 21. In the remaining 10 EAE mice, clinical
deficits then subsided to a plateau level. However, in three of
these 10, a relapse occurred between day 21 and day 98 post-
immunization, defined as an increase in severity of neurolo-
gical deficits of one grade or more that persisted for �3 days.
Two of the 10 EAE mice had become entirely asymptomatic
by day 98 post-MOG peptide. These remaining 10 EAE mice
and eight CFA controls were sacrificed on day 98.
Lumbosacral spinal cord inflammation,demyelination and axonal fragmentation inMOG peptide-EAEAccumulations of inflammatory cells in spinal cord were
prominent on day 14 after administration of MOG peptide
in CFA, but were less apparent by days 21 and 98, and were
not present in CFA control mice. Combined immunofluor-
escence/TUNEL histochemistry demonstrated frequent
CD11b+ or CD40+ cells undergoing apoptosis on day 14
post-MOG peptide, as has previously been reported by
Ray et al. (2000). Demyelination, as visualized by MBP
immunoreactivity, was most evident in mice sacrificed
Table 1 Antibodies used in this study
Antibody specificity Name Titre used Source
Hypophosphorylated NF-H SMI-32 ascites 1 : 800 Sternberger Monoclonals Inc., Lutherville, MD, USAHypophosphorylated NF-H RMDO9.5 ascites 1 : 100 V.M-Y. Lee PhD, Pathology, University of Pennsylvania, PA, USAMyelin basic protein SMI-99 ascites 1 : 1000 Sternberger Monoclonals Inc.CD11b antigen M1/70 10 mg/ml Serotec, Raleigh, NC, USACD40 antigen sc-975 10 mg/ml Santa Cruz Biotechnology, Inc., Santa Cruz, California, USAMicrotubule-associated AP14 ascites 1 : 200 V.M-Y. Lee PhD, Pathology, University of PennsylvaniaProtein 2a (MAP2a) alpha-actinin 3 AP5B3 1 : 750 Dr A. BeggsSarcospan 81864 1 : 2500 Dr L. Kunkel
Motor neurons in EAE Brain (2005), 128, 1877–1886 1879
Dow
nloaded from https://academ
ic.oup.com/brain/article-abstract/128/8/1877/481392 by guest on 05 April 2019

21 days post-MOG peptide. Substantial remyelination had
occurred by day 98 post-MOG peptide. Disrupted and bal-
looned axons, visualized by hypophosphorylated neurofila-
ment heavy (hypoP-NF-H) immunohistology (Sternberger
and Sternberger, 1983; Lee et al., 1987), were present in spinal
cord white matter on day 14 post-MOG peptide, and had
become more prominent by day 21 (data not shown).
Spinal cord grey and white matteratrophy occur in MOG peptide-EAESpinal cord atrophy has been well documented in multiple
sclerosis (Edwards et al., 1999; Lin et al., 2003, 2004; Ukkonen
et al., 2003). To determine whether spinal cord atrophy also
occurs in MOG peptide-EAE, we compared the areas of grey
and white matter in paraffin-embedded cross sections of L5,6
spinal cord from 98-day post-MOG peptide and 98-day post-
CFA control mice. There were �20% smaller cross-sectional
areas of both greymatter (EAE= 0.9486 0.137mm2; control=
1.230 6 0.204 mm2, mean 6 SD, P < 0.01) and white matter
(EAE = 0.891 6 0.178 mm2; control = 1.106 6 0.206 mm2,
mean6SD; P < 0.05) in the MOG peptide-EAE mice.
Motor neurons survive in MOGpeptide-EAELoss of spinal cord ventral horn neurons has previously been
noted in rats with MBP-induced EAE (Smith et al., 2000).
Motor neurons of the thy1-YFP transgenic mice expressed
both cytoplasmic and nuclear YFP, with most intense fluor-
escence in the nucleus (Fig. 2). This intrinsic YFP fluorescence
facilitated visualization of motor neurons in these mice.
Three lines of evidence indicated that substantial numbers
of motor neurons were not lost as a consequence of MOG
peptide-EAE in these mice. First, we saw no TUNEL+ YFP+
neurons in any of the mice we examined on day 14, 21,
or 98 post-MOG peptide (data not shown). Secondly, there
were no significant differences between densities of YFP+
motor neurons in cross sections of L5,6 spinal cords of
MOG peptide-EAE and CFA control mice at day 98 post-
immunization (MOG peptide-EAE mice = 114 6 24; YFP
control mice = 132620; mean 6 SD, n = 8; P > 0.1). Thirdly,
examination of L5,6-innervated skeletal muscles using poly-
clonal anti-sarcospan antibodies, which outline skeletal mus-
cle sarcolemma, showed neither atrophic nor angulated
skeletal muscle fibres in the day 98 post-MOG peptide EAE
animals; and, using polyclonal anti-alpha-actinin 3 antibodies
which specifically label type 2b skeletal muscle fibres, there
was no fibre type-specific grouping (data not shown). These
immunohistological results indicated that skeletal muscle
fibres were neither denervated nor reinnervated by axonal
collateral sprouting at this late time-point in these mice.
Motor neuron phenotype is altered inMOG peptide-EAEWe documented alterations in motor neuron perikaryal size,
perikaryal cytoskeletal phosphorylation and dendrites in the
3.00
2.50
2.00
1.50
1.00
0.50
0.00
Clin
ical
EA
E S
core
8 11 14 17 20 23 26 29 32 35 38 41 44 47
47
50 53 56 59 62 65 68 71 74 77 80 83 86 89 92 95 98
Days post-MOG peptide
Fig. 1 Mice immunized with MOG peptide in CFA show prolonged neurological disability. Days post-MOG peptide administrationare plotted on the x-axis and neurological disability scores on the y-axis. Peak disability was on day 21 post-MOG peptide.Data shown are means 6 SD.
1880 Brain (2005), 128, 1877–1886 P. G. Bannerman et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article-abstract/128/8/1877/481392 by guest on 05 April 2019

MOG peptide-EAE mice. First, while the mean L5,6 spinal
cord motor neuron perikaryal cross-sectional area in these
mice was not significantly different from that in the CFA
control mice, the average transverse area of L5,6 motor neu-
ron perikarya in the 98-day post-MOG peptide mice was 15%
smaller than that in simultaneous CFA controls (427 6 75
versus 502 6 48 mm2, respectively, mean 6 SD, P < 0.02).
Secondly, we noted a widespread, but reversible, alteration
in motor neuron perikaryal neurofilament phosphorylation
in the EAE mice at day 21 post-MOG peptide immunization.
As previously reported (Carriedo et al., 1996; Tsang et al.,
2000), motor neurons of CFA control mice expressed abun-
dant perikaryal hypoP-NF-H immunoreactivity. Whereas
>80% of lumbar spinal cord motor neuron perikarya
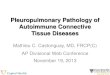
Fig. 2 Motor neuron perikaryal hypoP-NF-H immunoreactivity is depleted in MOG peptide-EAE. In these transversely orientedsections through L5,6 spinal cord anterior horns, Hoechst nuclear staining is shown in blue, hypoP-NF-H (SMI-32 mAb)immunostaining in red, and YFP fluorescence in green. Panels A, C and E are identical fields from a 21-day post-CFA control mouse. PanelsB, D and F are identical fields from a 21-day post-MOG peptide EAE mouse with a clinical disability score of 3.5. Note that YFPfluorescence was most intense in motor neuron nuclei in both control and EAE mice (A, B). Also note the co-localization of YFP andhypoP-NF-H in motor neuron perikarya of the CFA control (E), resulting in the yellow colour and the paucity of hypoP-NF-H in the YFP+motor neuron perikarya in the MOG peptide-EAE mouse (F). Magnifications are the same in the six panels; the size bar denotes 40 mm.
Motor neurons in EAE Brain (2005), 128, 1877–1886 1881
Dow
nloaded from https://academ
ic.oup.com/brain/article-abstract/128/8/1877/481392 by guest on 05 April 2019

expressed abundant hypoP-NF-H immunoreactivity in the
21-day post-CFA control mice (n = 8), this proportion had
fallen to <70% in 21-day post-MOG peptide EAE mice with
mild to moderate clinical deficits (deficit score 2.5 or lower, n
= 6), and to <60% in 21-day post-MOG peptide EAE mice
with severe clinical deficits (deficit score 3 or higher, n = 9) (P
< 0.01, x2 test).
An example of the depletion of hypoP-NF-H immuno-
staining in a mouse with grade 4 clinical deficits is shown
in Fig. 2. In the fields illustrated in this figure, average motor
neuron perikaryal size was larger in the CFA control mouse
than the MOG peptide-EAE mouse, but this was not a con-
sistent finding at this time-point. Even though clinical deficits
persisted beyond 21 days in most mice, motor neuron
perikaryal hypoP-NF-H immunoreactivity had returned to
normal by 98-day post-MOG peptide immunization (data
not shown).
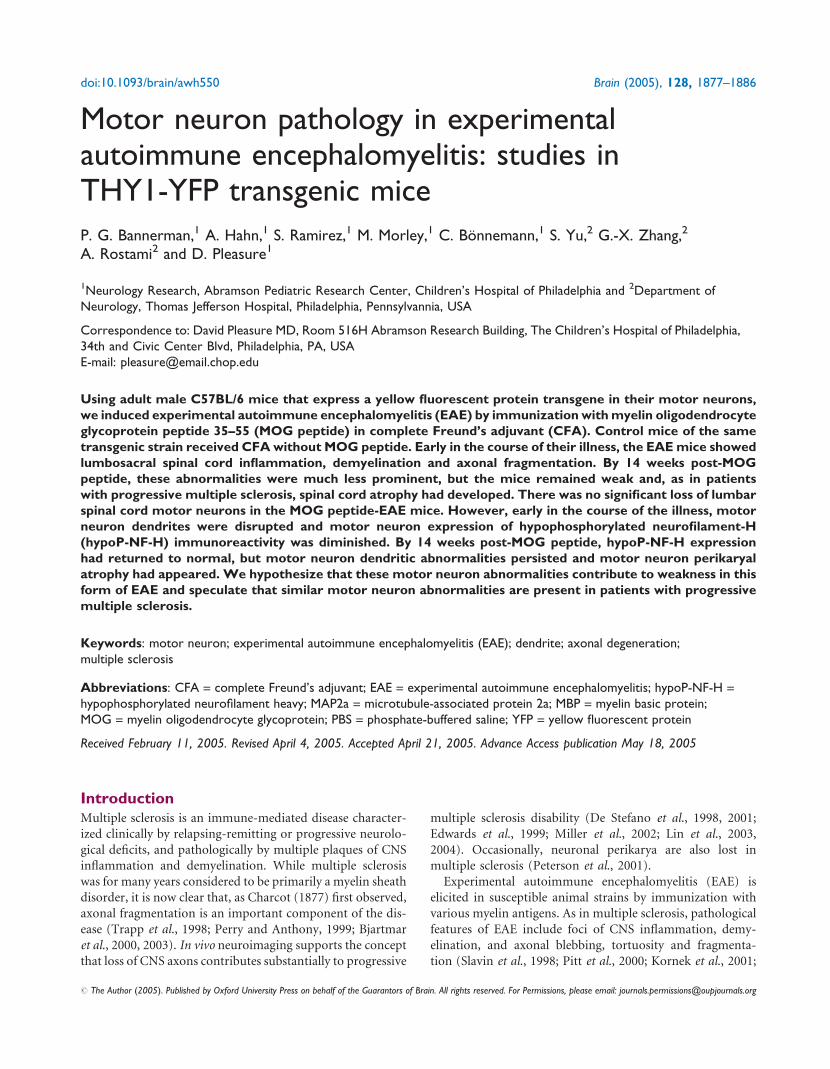
The third abnormality we observed in motor neurons
of the MOG peptide-EAE mice was dendritic thinning, short-
ening and fragmentation. This was evident from both YFP
fluorescence and MAP2a immunofluorescence microscopy
(Papandrikopoulou et al., 1989; Riederer et al., 1995)
(Fig. 3). Note the paucity of motor neuron dendrites in the
14-day post-MOG peptide EAE mouse (clinical deficit score
2.5) in Fig. 3C and D compared with those of the 14-day
CFA control mouse shown in Fig. 3A and B. MAP2a
immunostaining was particularly useful in highlighting this
dendritic abnormality.
To permit semi-quantitation of dendritic alterations in the
30 MOG peptide-EAE mice and 20 CFA control mice that we
autopsied, we devised a semi-quantitative score that reflected
the aggregate severities of motor neuron dendritic shortening,
fragmentation and thinning, assigning grades varying between
normal (0) and very marked dendritic pathology (+++) (see
Methods). An example of each of these scores is shown in
Fig. 4; each panel is a Z-stack of 12 sequential 500-nm con-
focal optical slices through an L5,6 lumbar anterior horn. An
observer without knowledge of the history of individual mice
then scored the motor neuron dendritic pathology in L5,6
ventral horns in each of the 50mice, again using Z-stacks of 12
sequential 500-nm confocal optical sections. Only the red
(MAP2a) channel was viewed in order to avoid potential
bias introduced by the presence or absence of inflammatory
cells in the field. Results are summarized in Fig. 5.
Nineteen of the 20 CFA control mice, but only four of the
30MOG peptide-EAEmice, received a score of 0. Moderate to
severe dendritic pathology (++ or +++) was scored for 17 of
the 30 MOG peptide-EAE mice, but was not seen in any of the
CFA control mice. Dendritic abnormalities were observed in
the majority of theMOG peptide-EAEmice both early (day 14
post-immunization) and late (day 98 post-immunization)
in their illness. Interestingly, the two EAE mice with
Fig. 3 Motor neuron dendrites are disrupted in MOG peptide-EAE. In these transverse paraffin sections through L5,6 spinal cord,nuclear Hoechst staining is shown in blue, MAP2a (AP14) immunostaining in red, and YFP fluorescence in green. Co-localization of YFP(green) and MAP2a (red) in the cytoplasm of motor neurons in (A) and (C) results in the yellow coloration of portions of themotor neuron perikarya and dendrites. (A) and (B) are identical fields from a 14-day post-CFA control mouse, while (C) and (D) areidentical fields from a 14-day post-MOG peptide-EAE mouse with a clinical score of 2.5. Note the depletion of AP14+ dendrites in(C) and (D). Magnifications are the same in the four panels; the size bar denotes 50 mm.
1882 Brain (2005), 128, 1877–1886 P. G. Bannerman et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article-abstract/128/8/1877/481392 by guest on 05 April 2019

grade 0 (normal) L5,6 motor neuron dendrites on day 98
post-MOG peptide (see Fig. 5) were the only two in the
group of 10 EAE mice examined at that time-point which
had shown full clinical recovery from their clinical neurolo-
gical deficits.
DiscussionUntil 1998, most clinicians attributed all neurological deficits
in multiple sclerosis to demyelination, with permanent
deficits presumed to result from incomplete remyelination
and nerve action potential conduction block. But the redis-
covery of multiple sclerosis-associated axonal disruption by
confocal microscopy (Trapp et al., 1998), followed by longi-
tudinal in vivo imaging and magnetic resonance spectroscopic
evidences of axonal loss in patients with multiple sclerosis
(De Stefano et al., 1998, 2001; Edwards et al., 1999; Filippi
et al., 2003; Lin et al., 2003, 2004) have led to recognition that
axonopathy is a major cause of progressive and permanent
neurological disability in patients with multiple sclerosis
Fig. 4 Motor neuron dendrite disruption scoring system. In these transverse sections through L5,6 spinal cord, MAP2a (AP14)immunostaining is shown in red. Normal dendrites (0) are shown in a section prepared from a CFA control mouse. Progressively moresevere dendritic disruptions (+, ++ and +++) were prepared from MOG peptide-EAE mice. Each panel is a Z-stack of 12 successive500-nm confocal optical sections. Magnifications are the same in the four panels; the size bar denotes 50 mm.
Fig. 5 Scoring of motor neuron dendritic disruption as a functionof time post-immunization with MOG peptide in CFA or withCFA alone. X denotes results in MOG peptide-EAE mice, andsolid circles denote results in CFA control mice. Days post-immunization (D14, D21 and D98) are shown on the x-axis anddendritic disruption scoring (0, +, ++ or +++) on the y-axis.
Motor neurons in EAE Brain (2005), 128, 1877–1886 1883
Dow
nloaded from https://academ
ic.oup.com/brain/article-abstract/128/8/1877/481392 by guest on 05 April 2019

(Bjartmar et al., 2000, 2003). The causes of axonopathy in
multiple sclerosis and EAE have still not been fully established
(Kornek et al., 2001; Craner et al., 2004; Stys, 2004). However,
axonal disruption is most prevalent within plaques of demy-
elination (Trapp et al., 1998; Bjartmar et al., 2003), suggesting
that inflammatory processes centred in or bordering plaques
target axons as well as myelin or, alternatively, that a primary
loss of myelin within plaques causes secondary loss of axonal
integrity.
Most of the surviving mice with EAE in the present study
still demonstrated clinical neurological deficits 98 days after
receiving MOG peptide. At this late time-point, spinal
cord white matter atrophy had developed, presumably as
a consequence of depletion of myelinated axons. While we
are not aware of prior reports of spinal cord white matter
atrophy in EAE, autopsy and in vivoMRI studies have demon-
strated white matter atrophy in patients with progressive
multiple sclerosis (Charcot, 1877; Edwards et al., 1999; Lin
et al., 2003, 2004; Ukkonen et al., 2003).
Neuronal apoptosis occurs in the spinal cord and retina in
EAE (Ahmed et al., 2002; Diem et al., 2003; Hobom et al.,
2004) and in multiple sclerosis plaques that involve cerebral
cortical grey matter (Peterson et al., 2001). The observation
that a substantial number of ventral horn neurons are lost
within 2 weeks after immunization of Lewis rats with myelin
basic protein (Smith et al., 2000), together with reports of
spinal cord motor neuron dysfunction, focal amyotrophy and
generalized weakness and fatigue in some patients with
multiple sclerosis (Petajan, 1982; Fisher et al., 1983; Shefner
et al., 1992; de Haan et al., 2000; Chaudhuri and Behan, 2004),
motivated us to evaluate whether neuronal perikarya are
targeted in MOG peptide-EAE. Based on the report by
Smith et al. (2000), we anticipated that YFP fluorescence
imaging might reveal substantial depletion of motor neurons
in the MOG peptide-EAE mice. In fact, however, these
mice did not show a statistically significant loss of motor
neurons.
In accord with this result, TUNEL histochemistry did not
demonstrate motor neuron apoptosis in the MOG peptide-
EAE mice and, 98 days after MOG peptide administration,
these mice did not show immunohistological evidences of
skeletal muscle fibre denervation or re-innervation. The dis-
crepancy between the observations of Smith et al. (2000) and
our own may reflect the divergent species and immunogens
used in the two studies, but differences in the neuron labelling
protocols may also have contributed. Smith et al. (2000)
counted all ventral horn neurons, including interneurons,
labelled by cresyl violet, a Nissl stain, whereas we determined
the density in L5,6 spinal cord of YFP+ motor neurons.
Thus, it is possible that either ventral horn interneurons
are selectively susceptible to death in EAE or the use by
Smith et al. (2000) of cresyl violet resulted in substantial
motor neuron undercounts in their EAE rats, as has been
reported when this stain has been used in other circumstances
where there is motor neuron perikaryal atrophy (McPhail
et al., 2004).
Late in the course of EAE in the thy1-YFP transgenic mice,
the mean cross-sectional area of lumbar spinal cord motor
neuron perikarya was 15% below that in CFA control mice
of the same strain and age. Motor neuron atrophy has not
previously been documented in EAE or multiple sclerosis, nor
has atrophy of this magnitude been reported in other neuronal
subsets in these disorders (Miller et al., 2002), though a
slight diminution in the size of parvocellular neurons in
the lateral geniculate body was noted in patients with multiple
sclerosis (Evangelou et al., 2001). Motor neuron perikaryal
atrophy in theMOGpeptide-EAEmice is unlikely to have been
a consequence of motor neuron axotomy (McPhail et al.,
2004), since there were no evidences in these mice of skeletal
muscle denervation or re-innervation. Other possible causes
for motor neuron shrinkage in these mice include a loss of
necessary trophic input owing to EAE-induced motor neuron
dendritic pathology (Zhu et al., 2003, and the present study)
or a deleterious effect of chronic exposure to pro-
inflammatory cytokines (Villarroya et al., 1997).
Much of the NF-H in normal motor neuron perikarya is
hypophosphorylated, and becomes hyperphosphorylated
only after transport into the axon (Carriedo et al., 1996;
Sun et al., 1996; Veeranna et al., 1998; Brownlees et al.,
2000; Tsang et al., 2000; Ackerley et al., 2004). In the
MOG peptide-EAE mice, the proportion of motor neurons
that displayed perikaryal hypoP-NF-P immunoreactivity had
fallen substantially by day 21 post-MOG peptide. This peri-
karyal cytoskeletal phosphorylation alteration was most
widespread in mice with the most severe clinical deficits.
Our studies do not shed light on the cause of this temporary
alteration in perikaryal neurofilament phosphorylation.
However, prior studies have shown that increased phos-
phorylation of neuronal perikaryal NF-H can be elicited by
raising the extracellular concentration of glutamate (Ackerley
et al., 2000) and perturbed CNS extracellular glutamate
homeostasis has been documented in EAE and multiple
sclerosis (Hardin-Pouzet et al., 1997; Matute et al., 2001;
Werner et al., 2001).
Using both YFP fluorescence and MAP2a immunofluores-
cence, we observed persistent alterations in the architecture
of motor neuron dendrites in the MOG peptide-EAE mice,
including proximal dendritic thinning, shortening and
fragmentation. Even by stacking multiple confocal optical
slices, we could not visualize all of the proximal dendrites
of individual motor neurons accurately; this would best be
achieved using in vivo cholera toxin or post-mortem DiI
retrograde tracing techniques (Snider and Palavali, 1990;
Ritz et al., 1992; Zhu et al., 2003). However, using a semi-
quantitative scoring system to grade abnormalities visualized
byMAP2a immunostaining, we were able to document motor
neuron dendritic abnormalities throughout the course of
MOG peptide-EAE. In addition, while the number of mice
with EAE we examined at day 98 was small (n = 10), our
observations suggested a correlation between full remission
of clinical illness and restoration of normal dendritic
architecture.
1884 Brain (2005), 128, 1877–1886 P. G. Bannerman et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article-abstract/128/8/1877/481392 by guest on 05 April 2019

We are not aware of prior reports of persistent dendritic
abnormalities in motor neurons in multiple sclerosis or EAE.
However, acute reversible beading of distal motor neuron
dendrites in spinal cord white matter has been documented
by both MAP2 immunostaining and in vivo cholera toxin
retrograde labelling techniques in Lewis rats with MBP-
induced EAE (Zhu et al., 2003).
In summary, we have documented perikaryal atrophy and
disruption of dendritic architecture in lumbosacral motor
neurons of mice with MOG peptide-induced EAE. Morpho-
metric studies will be required to determine the relative
extents to which motor neuron perikaryal atrophy and dend-
ritic disruption contribute to late spinal cord grey matter
atrophy in these mice. Further investigation is also needed
to evaluate whether similar motor neuron abnormalities
occur in multiple sclerosis.
AcknowledgementsWe wish to thank J. Golden, R. Kalb and J. Grinspan for their
critical reading of this manuscript. This work was supported
by the National Multiple Sclerosis Society, Muscular
Dystrophy Association, and NIH grant NS25044.
References
Ackerley S, Grierson AJ, Brownlees J, Thornhill P, Anderton BH, Leigh PN,
et al. Glutamate slows axonal transport of neurofilaments in transfected
neurons. J Cell Biol 2000; 150: 165–75.
Ackerley S, Grierson AJ, Banner S, PerkintonMS, Brownlees J, Byers HL, et al.
p38a stress-activated protein kinase phosphorylates neurofilaments and is
associated with neurofilament pathology in amyotrophic lateral sclerosis.
Mol Cell Neurosci 2004; 26: 354–64.
Ahmed Z, Doward AI, Pryce G, Taylor DL, Pocock JM, Leonard JP, et al. A
role for caspase-1 and 3 in the pathology of experimental allergic encepha-
lomyelitis. Inflammation versus degeneration. Am J Pathol 2002; 161:
1577–86.
Bjartmar C, Kidd G, Mork S, Rudick R, Trapp BD. Neurological
disability correlates with spinal cord axonal loss and reduced N-acetyl
aspartate in chronic multiple sclerosis patients. Ann Neurol 2000; 48:
893–901.
Bjartmar C, Wujek JR, Trapp BD. Axonal loss in the pathology of multiple
sclerosis: consequences for understanding the progressive phase of the
disease. J Neurol Sci 2003; 206: 165–71.
Brownlees J, Yates A, Bajaj NP, Davis D, Anderton BH, Leigh PN, et al.
Phosphorylation of neurofilament heavy chain side-arms by stress
activated protein kinase-1b/Jun N-terminal kinase-3. J Cell Sci 2000;
113: 401–7.
Carriedo SG, Yin HZ, Weiss JH. Motor neurons are selectively vulnerable to
AMPA/kainate receptor-mediated injury in vitro. J Neurosci 1996; 16:
4069–79.
Charcot JM. Lectures on the diseases of the nervous system delivered at La
Salpetriere (translated by G. Sigerson). London: New Sydenham Society;
1877.
Chaudhuri A, Behan PO. Fatigue in neurological disorders. Lancet 2004;
363: 978–88.
Craner MJ, Hains BC, Lo AC, Black JA, Waxman SG. Co-localization of
sodium channel Nav1.6 and the sodium-calcium exchanger at sites of
axonal injury in the spinal cord in EAE. Brain 2004; 127: 294–303.
de Haan A, de Ruiter CJ, van der Woude, LHV, Jongen PJH. Contractile
properties and fatigue of quadriceps muscles in multiple sclerosis.
Muscle Nerve 2000; 23: 1534–41.
De Stefano N, Matthews PM, Fu L, Narayanan S, Stanley J, Francis GS, et al.
Axonal damage correlates with disability in patients with relapsing-
remitting multiple sclerosis. Results of a longitudinal magnetic resonance
spectroscopy study. Brain 1998; 121: 1469–77.
De Stefano N, Narayanan S, Francis GS, Arnaoutelis R, Tartaglia MC, Antel
JP, et al. Evidence of axonal damage in the early stages of multiple sclerosis
and its relevance to disability. Arch Neurol 2001; 58: 65–70.
Diem R, Hobom M, Maier K, Weissert R, Storch MK, Meyer R, Bahr M.
Methylprednisolone increases neuronal apoptosis during autoimmune
CNS inflammation by inhibition of an endogenous neuroprotective
pathway. J Neurosci 2003; 23: 6993–7000.
Edwards SG, Gong QY, Liu C, Zvartau ME, Jaspan T, Roberts N, Blumhardt
LD. Infratentorial atrophy on magnetic resonance imaging and disability
in multiple sclerosis. Brain 1999; 122: 291–301.
Evangelou N, Konz D, Esiri MM, Smith S, Palace J, Matthews PM. Size-
selective neuronal changes in the anterior optic pathways suggest a differ-
ential susceptibility to injury in multiple sclerosis. Brain 2001; 124:
1813–20.
Feng G,Mellor RH, BernsteinM, Keller-Peck C, Nguyen QT,WallaceM, et al.
Imaging neuronal subsets in transgenic mice expressing multiple spectral
variants of GFP. Neuron 2000; 28: 41–51.
Filippi M, Bozzali M, Rovaris M, Gonen O, Kesavadas C, Ghezzi A, et al.
Evidence for widespread axonal damage at the earliest clinical stage of
multiple sclerosis. Brain 2003; 126: 433–7.
Fisher M, Long RR, Drachman DA. Hand muscle atrophy in multiple
sclerosis. Arch Neurol 1983; 40: 811–5.
Gavrieli Y, Sherman Y, Ben-Sasson SA. Identification of programmed cell
death in situ via specific labeling of nuclear DNA fragmentation. J Cell
Biol 1992; 119: 493–501.
Gran B, Zhang G-X, Yu S, Li J, Chen X-H, Ventura ES, et al. IL-12p35-
deficient mice are susceptible to experimental autoimmune encephalo-
myelitis: evidence for redundancy in the IL-12 system in the induction
of central nervous system autoimmune demyelination. J Immunol 2002;
169: 7104–10.
Hardin-Pouzet H, Krakowski M, Bourbonniere L, Didier-Bazes M, Tran E,
Owens T. Glutamate metabolism is down-regulated in astrocytes during
experimental allergic encephalomyelitis. Glia 1997; 20: 79–85.
Hobom M, Storch MK, Weissert R, Maier K, Radhakrishnan A, Kramer B,
et al. Mechanisms and time course of neuronal degeneration in
experimental autoimmune encephalomyelitis. Brain Pathol 2004; 14:
148–57.
Kanwar JR, Kanwar RK, Krissansen GW. Simultaneous neuroprotection and
blockade of inflammation reverses autoimmune encephalomyelitis. Brain
2004; 127: 1313–31.
Kornek B, StorchMK, Bauer J, DjamshidianA,Weissert R,WallstroemE, et al.
Distribution of a calcium channel subunit in dystrophic axons in multiple
sclerosis and experimental autoimmune encephalomyelitis. Brain 2001;
124: 1114–24.
Lee VM-Y, Carden MJ, Schlaepfer WW, Trojanowski JQ. Monoclonal anti-
bodies distinguish several differentially phosphorylated states of the two
largest rat neurofilament subunits (NF-H and NF-M) and demonstrate
their existence in the normal nervous system of the adult rat. J Neurosci
1987; 7: 3474–88.
Lin X, Blumhardt LD, Constantinescu CS. The relationship of brain and
cervical cord volume to disability in clinical subtypes of multiple
sclerosis: a three-dimensional MRI study. Acta Neurol Scand 2003; 108:
401–6.
Lin X, Tench CR, Evangelou N, Jaspan T, Constantiescu CS. Measurement
of spinal cord atrophy in multiple sclerosis. J Neuroimaging 2004;
20S–26S.
Matute C, Alberdi E, DomercqM, Perez-Cerda F, Perez-Samartin A, Sanchez-
Gomez MV. The link between excitotoxic oligodendroglial death and
demyelinating diseases. Trends Neurosci 2001; 24: 224–30.
McPhail LT, Fernandes KJ, Chan CC, Vanderluit JL, Tetzlaff W. Axonal
reinjury reveals the survival and re-expression of regeneration-associated
genes in chronically axotomized adult motoneurons. ExpNeurol 2004; 188:
331–40.
Motor neurons in EAE Brain (2005), 128, 1877–1886 1885
Dow
nloaded from https://academ
ic.oup.com/brain/article-abstract/128/8/1877/481392 by guest on 05 April 2019

Meyer R, Weissert R, Diem R, Storch MK, de Graaf KL, Kramer B, Bahr M.
Acute neuronal apoptosis in a rat model of multiple sclerosis. J Neurosci
2001; 21: 6214–20.
Miller DH, Barkhof F, Frank JA, Parker GJM, Thompson AJ. Measurement of
atrophy in multiple sclerosis: pathological basis, methodological aspects
and clinical relevance. Brain 2002; 125: 1676–95.
Onuki M, Ayers MM, Bernard CC, Orian JM. Axonal degeneration is an
early pathological feature in autoimmune-mediated demyelination in
mice. Microsc Res Tech 2001; 15: 731–9.
Papandrikopoulou A, Doll T, Tucker RP, Garner GC, Matus A. Embryonic
MAP2 lacks the cross-linking sidearm sequences and dendritic targeting
signal of adult MAP2. Nature 1989; 340: 650–2.
Perry VH, Anthony DC. Axon damage and repair in multiple sclerosis. Philos
Trans R Soc Lond B Biol Sci 1999; 354: 1641–7.
Petajan JH. Electromyographic findings in multiple sclerosis: remitting signs
of denervation. Muscle Nerve 1982; 5: S157–60.
Peterson JW, Bo L, Mork S, Chang A, Trapp BD. Transected neurites, apop-
totic neurons, and reduced inflammation in cortical multiple sclerosis
lesions. Ann Neurol 2001; 50: 389–400.
Pitt D, Werner P, Raine CS. Glutamate excitotoxicity in a model of multiple
sclerosis. Nature Med 2000; 6: 67–70.
Ray SK, Schaecher KE, Shields DC, Hogan EL, Banik NL. Combined TUNEL
and double immunofluorescent labeling for detection of apoptotic mono-
nuclear phagocytes in autoimmune demyelinating disease. Brain Res Brain
Res Protoc 2000; 5: 305–11.
Riederer BM, Draberova E, Viklicky V, Draber P. Changes of MAP2 phos-
phorylation during brain development. J Histochem Cytochem 1995; 43:
1269–84.
Ritz LA, Bailey SM, Murray CR, Sparkes ML. Organizational and morpho-
logical features of cat sacrocaudal motoneurons. J Comp Neurol 1992; 318:
209–21.
Shefner JM, Mackin GA, Dawson DM. Lower motor neuron dysfunction in
patients with multiple sclerosis. Muscle Nerve 1992; 15: 1265–70.
Slavin A, Ewing C, Liu J, Ichikawa M, Slavin J, Bernard CC. Induction of
a multiple sclerosis-like disease in mice with an immunodominant epitope
of myelin oligodendrocyte glycoprotein. Autoimmunity 1998; 28: 109–20.
Smith T, Groom A, Zhu B, Turski L. Autoimmune encephalomyelitis
ameliorated by AMPA antagonists. Nature Med 2000; 6: 62–6.
Snider WD, Palavali V. Early axon and dendritic outgrowth of spinal access-
ory motor neurons studied with DiI in fixed tissues. J Comp Neurol 1990;
297: 227–38.
Sternberger LA, Sternberger NH. Monoclonal antibodies distinguish phos-
phorylated and nonphosphorylated forms of neurofilaments in situ.
Proc Natl Acad Sci USA 1983; 80: 6126–30.
Stys PK. Axonal degeneration in multiple sclerosis: is it time for neuropro-
tective strategies? Ann Neurol 2004; 55: 601–3.
Sun D, Leung CL, Liem RKH. Phosphorylation of the high molecular weight
neurofilament protein (NF-H) by Cdk5 and p35. J Biol Chem 1996; 271:
14245–51.
Trapp BD, Peterson J, Ransohoff RM, Rudick R, Mork S, Bo L. Axonal
transection in the lesions of multiple sclerosis. New Engl J Med 1998;
338: 278–85.
Tsang YM, Chiong F, Kuznetsov D, Karaskis E, Geula C. Motor neurons are
rich in non-phosphorylated neurofilaments: cross-species comparison
and alterations in ALS. Brain Res 2000; 861: 45–58.
Ukkonen M, Dastidar P, Heinonen T, Laasonen E, Elovaara I. Volumetric
quantitation by MRI in primary progressive multiple sclerosis: volumes of
plaques and atrophy correlated with neurological disability. Eur J Neurol
2003; 10: 663–9.
Vanderhorst VG, Holstege G. Organization of lumbosacral motoneuronal cell
groups innervating hindlimb, pelvic floor and axial muscles in the cat.
J Comp Neurol 1997; 382: 46–76.
Veeranna, Amin ND, Ahn NG, Jaffe H, Winters CA, Grant P, Pant HC.
Mitogen-activated protein kinases (Erk1,2) phosphorylate Lys-Ser-Pro
(KSP) repeats in neurofilament proteins NF-H and NF-M. J Neurosci
1998; 18: 4008–21.
Villarroya H, Marie Y, Ouallet JC, Le Saux F, Tchelingerian JL, Baumann N.
Expression of TNF alpha in central neurons of Lewis rat spinal cord after
EAE induction. J Neurosci Res 1997; 49: 592–9.
Werner P, Pitt D, Raine CS. Multiple sclerosis: altered glutamate homeostasis
in lesions correlates with oligodendrocyte and axonal damage. Ann Neurol
2001; 50: 169–80.
Yasuda M, Umemura S, Osamura RY, Kenjo T, Tsutsumi Y. Apoptotic cells
in the human endometrium and placental villi: pitfalls in applying the
TUNEL method. Arch Histol Cytol 1995; 58: 185–90.
Zhang GX, Yu S, Gran B, Li J, Siglienti I, Chen X, et al. Role of IL-12
receptor beta 1 in regulation of T cell response by APC in
experimental autoimmune encephalomyelitis. J Immunol 2003; 171:
4485–92.
Zhu B, Luo L, Moore GR, Paty DW, Cynader MS. Dendritic and synaptic
pathology in experimental autoimmune encephalomyelitis. Am J Pathol
2003; 162: 1639–50.
1886 Brain (2005), 128, 1877–1886 P. G. Bannerman et al.
Dow
nloaded from https://academ
ic.oup.com/brain/article-abstract/128/8/1877/481392 by guest on 05 April 2019