Embed Size (px)
Citation preview
MOTORCYCLEAMBULANCESERVICE
UnderstandingEmergencyTransportinKigezi,UgandaandDevelopinganInnovativeSolution
StanfordUniversitySSLP2016UgandaMaternalHealthTeamSeptember16,2016
AbstractThisreportdetailsworkdonebytheSSLPUgandaMaternalHealthteamin2016.TheteamspentfiveweeksinKabale,UgandaworkingwithKigeziHealthcareFoundation
(KIHEFO)tolearnaboutmaternalhealthissuesanddevelopanengineeringsolutionforemergencytransportforexpectantmothers.Thisreportmaybeusedto(1)better
understandtransportationbarriersforexpectantmothers,(2)considermethodologiesforfieldinterviewsandstakeholderevaluation,(3)evaluatedatacollectedinuser
interviews,(4)gaugelocallyavailableprototypingresourcesandmaterialsinUganda,(5)reviewbusinessmodelsfordeliveringamotorcycleambulanceservice.
1
ContentsIntroduction.................................................................................................................................................2
Background..................................................................................................................................................2
HistoryofMaternalHealthinUganda.....................................................................................................2
IntroductiontoKabale.............................................................................................................................4
IntroductiontoKIHEFO............................................................................................................................5
NeedsIdentification.....................................................................................................................................5
ClinicalImmersion...................................................................................................................................6
MaternityWard&Clinic......................................................................................................................6
Outreaches:Cervical/BreastCancerScreening,GeneralHealth/HIVScreening.................................7
Workshop:NutritionClinic..................................................................................................................8
StakeholderInterviews............................................................................................................................8
NeedsIdentified.....................................................................................................................................11
ProblemStatement....................................................................................................................................11
Task1:UnderstandingTransportationBarriersforMaternalHealthcare.................................................12
Task2:EvaluatingMotorcycleAmbulancesasanEmergencyTransportSolution....................................13
MotorcycleAmbulanceDesignConsiderations.....................................................................................15
Pulse:LocallyAvailableMotorcycleAmbulance....................................................................................21
Task3:ImprovingMotorcycleAmbulancesforApplicationinKigezi,Uganda..........................................21
DesignRequirementsandConstraints...................................................................................................22
LocallyAvailableMaterialsandProduction...........................................................................................22
PrototypingandUserFeedback.............................................................................................................23
Design................................................................................................................................................24
Construction......................................................................................................................................24
ProspectiveCustomerFeedback........................................................................................................25
Task4:CreatingaBusinessModelforProvidingMotorcycleAmbulanceServiceinKigezi,Uganda........29
CustomerAcquisitionandRelations......................................................................................................30
ServiceComponents..............................................................................................................................30
FinancialModel......................................................................................................................................31
WillingnesstoPayStudy....................................................................................................................33
Conclusion.................................................................................................................................................37
MovingForward.........................................................................................................................................37
Stanford2016SSLPMaternalHealthTeam...............................................................................................38
Acknowledgements...................................................................................................................................39
Appendix....................................................................................................................................................40
2
Appendix1:MotorcycleandBicycleAmbulances.................................................................................40
Appendix2:WTPandPrototypeSurveyforServiceStakeholders........................................................43
Appendix3:FinancialModelDirectionsandScreenShot.....................................................................46
IntroductionThe2016StanfordSSLPMaternalHealthteamwastaskedwithimprovingmaternalhealthservicesatamaternitywardoperatedbyKigeziHealthcareFoundation(KIHEFO).HavingonlybeenrecentlyconstructedandopentopatientsinMarch2016,thematernitywardstillfacesmanyobstacleswithpatientrecruitment,outreachandaccessibility,identificationandtreatmentofhigh-riskbirths,organizationalandmanagementworkflow,workspacelayoutanddesign,andantenatalandpostnatalcareandeducation.Therefore,thepurposeoftheSSLPtripwastoevaluateandidentifyspecificneedsthatexistinKIHEFO'smaternalhealthcareservicesanddevelopsolutionsthatseektomitigatethem.
Thisreportprovidesanoverviewofthe2016SSLPMaternalHealthproject.Itarticulatestheprocesstheteamunderwentandtheworkthatresultedfromit.ThereportbeginswithanoverviewofthestateofmaternalhealthcareinUgandaandbackgroundinformationontheKabaleregionandhealthcareservicesprovided.Itdetailsourneedfindingprocess,includinginsightsfromclinicalimmersionandfieldinterviewswithstakeholdersinmaternalhealthandemergencytransportation.ThereportthendiscussescurrenttransportationoptionsandbarrierstoemergencytransportforwomeninKabale,Uganda,andapotentialsolutionthatcouldbeadoptedinthisregion:amotorcycleambulancesystem.Next,wedescribepredicatemotorcycleambulancesystemsandlistdesignrequirementsandconstraintsinselectingmotorcycleambulancecomponents.Wethendescribeourworkindesign,prototyping,andusageofpredicatesystemsinordertocollectmoreaccurateuserfeedback.Lastly,wediscusstheprocessbehindcreatinganoptimalbusinessmodelforKabale,Ugandaandthefinancialmodelanalysisandwillingnesstopayresearchthatcontributedtoitsselection.
Overthecomingmonths,weplantocontinueoureffortsinacquiringanemergencytransportsystemoutlinedinthisreportforKIHEFOtouseforitsmaternitywardandruralhealthoutreachservices.WehopetoobtainaninitialsystemtoconductfurthercompatibilitytestingandsensitizationinterviewsbeforeencouragingproductdeploymenttocommunitiesacrossKabale.
BackgroundThissectionprovidesthecontextthroughwhichtheproblemstatementwasinvestigated.ItincludesabriefhistoryofmaternalhealthinUganda,includingcurrentstatisticsonmaternalhealthinthecountryascomparedtotheglobalsetting;anoverviewoftheKigezi/Kabaleregion;andadescriptionofthelocalpartnerorganization,KIHEFO,andtheservicestheyprovide.
HistoryofMaternalHealthinUgandaMaternalmortality,definedbytheWorldHealthOrganization(WHO)asthe“deathofawomanwhilepregnantorwithin42daysofterminationofpregnancy…fromanycauserelatedtooraggravatedbythepregnancyoritsmanagement”,continuestobeaglobalconcern.iUgandahasoneofthehighestmaternalmortalityrates(MMR)intheworld,anditisestimatedthat16womendieperdayinchildbirth.iiThefourmostcommoncontributorstomaternaldeathsinUgandaarehemorrhages,sepsis,obstructedlabor,orcomplicationsarisingfromindirectcausessuchasHIVormalaria.iiCurrently,itisestimatedthatUgandahasanMMRofaround343deathsoutofevery100,000livebirths–areduction

3
fromitsMMRof687in1990.iiiHowever,thisnumberisnearlydoublethecountry’sMillenniumDevelopmentGoal5target:anMMRof131outofevery100,000livebirthsby2015.ii
Recently,theUgandangovernmentcreatedanumberofpoliciesinordertoincreasethenumberandcapacityofhealthfacilitiesandimprovethecareofferedinthesefacilities.Someoftheseprogramsarededicatedtoreducingthecountry’sMMR–however,thesehavebeen“minimallyimplemented”duetoalackofresourcesonalllevelsofgovernment.ivForinstance,thereductionoftheUgandaMMRhasgenerallybeenattributedtoanincreaseinthenumberofwomendeliveringinthepresenceofaskilledbirthattendant(SBA),ortrainedhealthworkerswhoareabletointerveneshouldcomplicationsariseduringthebirthingprocess,asopposedtotraditionalbirthattendants(TBAs),ormidwiveswhohavenotreceivedformalmedicaltrainingbuthadinsteadbeentrainedbyotherTBAs.Initially,thegovernmenthadtriedtopilotaprogramthatworkedtoprovideTBAswithmoreskills,withtheimplicationthatTBAswouldreferwomentolocalhospitalsiftherewerecomplicationsduringthebirthingprocess.However,in2010,thegovernmentinstitutedabanontraditionalbirthattendants,arguingthatTBAshadstrayedfromtheirmajorroleofreferring.vThisbanhasnotbeenveryeffective,asmanywomencontinuetoseekoutcarefromTBAsasanaffordableoptionfortheirdelivery.
However,publicawarenessofmaternalhealthissueshasgraduallybeenincreasing,andanumberofmaternalhealthadvocacygroupsinUgandahavegainedmomentuminthepastfewyears.In2011,apetitionwaslaunchedagainsttheUgandangovernmentbytheCentreforHealth,HumanRights,andDevelopment(CEHURD)afterthedeathsofSylviaNalubowaandJenniferAngukoinchildbirth.iiBecausetheUgandangovernmentfailedtoprovidesoundmaternalhealthcareservices,CEHURDarguedthatthegovernmentwasinviolationofthehumanrightslistedintheirconstitution,includingtherighttohealth.viThepetitionculminatedinthecaseConstitutionalPetitionNo.16of2011:CentreforHealth,HumanRightsandDevelopmentandothersvsAttorneyGeneralthatwaspresentedbeforetheUgandanConstitutionalCourt.InJune2012,theconstitutionalcourtdismissedthecase,statingthatithadnomandatetohearthiscase,asitdealtwith“politicalquestions”thatcouldnotbedeterminedbytheJudiciary.viiHowever,onOctober30,2015,theSupremeCourtoverruledtheconstitutionalcourt’sdecision,statingthattheConstitutionalCourtwasobligatedtohearthecaseasitconcernedhumanrightsissuesthatareoutlinedintheUgandanConstitution.viiiAsofSeptember1,2016,thecasehasbeenofficiallyreopened.ixThiscasehaslargeimplicationsforfuturematernalhealthpolicies,includingthoseregardingemergencyobstetricservices,asapproximately80%ofthepopulationresideinareaswithlittleornoaccesstothesetypesofservices.x
Despitethesecontroversies,thestateofmaternalhealthcareinthiscountryhasgreatlyimproved.Ingeneral,antenatalcareandmaternityservicesareofferedfree-of-chargetoallmothersinallpublicorgovernmentinstitutions,althoughexpectingmothersareoftenaskedtobringsupplies,suchasglovesorbasins,withthemwhentheydeliverinthesehealthcarefacilities.xiThemajorityofmothersinUgandaattendatleastoneantenatalcarevisit,withanestimatedonehalfofUgandansattendingmorethanfour.xMothersattendthesevisitsprimarilytoreceiveanantenatalcard,whichmakeiteasierforwomentobeadmittedinhospitalsshouldtheychoosetodeliverthere,butalsotoensurethehealthofthemotherandbaby.xiThereareanumberoffactorsthatinfluenceawoman’sdecisiontodeliverathomeoratahealthfacility,andgenerallyincludeculturalbeliefsorattitudestowardsbirth,socialinfluencesfromfamilymembers,costofcare,lackofaccesstotransportation,perceivedrudenessorabusivenessfromworkersatformalhealthcarefacilities,habit,orunexpected“quickness”oflabororlaboroccurringatnight.xi
4
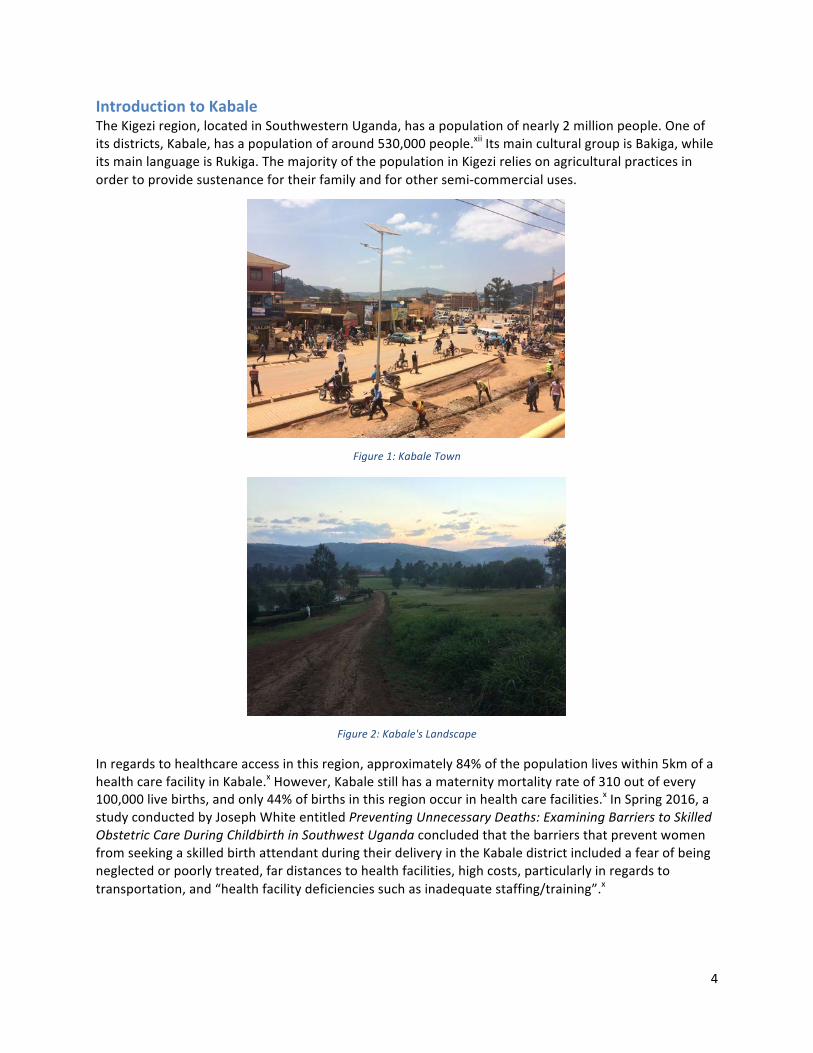
IntroductiontoKabaleTheKigeziregion,locatedinSouthwesternUganda,hasapopulationofnearly2millionpeople.Oneofitsdistricts,Kabale,hasapopulationofaround530,000people.xiiItsmainculturalgroupisBakiga,whileitsmainlanguageisRukiga.ThemajorityofthepopulationinKigezireliesonagriculturalpracticesinordertoprovidesustenancefortheirfamilyandforothersemi-commercialuses.
Figure1:KabaleTown
Figure2:Kabale'sLandscape
Inregardstohealthcareaccessinthisregion,approximately84%ofthepopulationliveswithin5kmofahealthcarefacilityinKabale.xHowever,Kabalestillhasamaternitymortalityrateof310outofevery100,000livebirths,andonly44%ofbirthsinthisregionoccurinhealthcarefacilities.xInSpring2016,astudyconductedbyJosephWhiteentitledPreventingUnnecessaryDeaths:ExaminingBarrierstoSkilledObstetricCareDuringChildbirthinSouthwestUgandaconcludedthatthebarriersthatpreventwomenfromseekingaskilledbirthattendantduringtheirdeliveryintheKabaledistrictincludedafearofbeingneglectedorpoorlytreated,fardistancestohealthfacilities,highcosts,particularlyinregardstotransportation,and“healthfacilitydeficienciessuchasinadequatestaffing/training”.x
5
IntroductiontoKIHEFOTheKigeziHealthcareFoundation(KIHEFO),foundedbyDr.GeoffreyAnguyo,isanon-profit,non-governmentalorganizationbasedinKabale,Uganda.Thisorganizationworksunderthebeliefthatissuessuchas“poverty,ignorance,anddisease”areintertwined;thus,theyworkinavarietyoffieldsregardingcommunitydevelopment,includingeducation,medicalservices,women'sempowerment,andeconomicdevelopment,inordertoreachfamiliesinKabale.xiiiTofacilitatethesustainabilityoftheirprograms,KIHEFOworkscloselywithcommunitiestocreateprogramsthatempowerindividualsandfamilies,ratherthansimply“handingout”resources.
Figure3:KIHEFO'sMainClinicinKabaleTown
KIHEFOoperatesfourseparateclinics:amedicalanddentalclinic,maternityward,HIV/AIDsclinic,andnutritioncenter.TheyalsoconductgeneralandHIV/AIDsoutreaches,workwithtraditionalhealersandTBAstoextendlocalreferralsystems,providevocationaltraining,andleadprojectsdesignedtomeetspecificcommunityneeds(e.g.,arabbitfarmtocombatmalnutritionandprovideeconomicopportunitiesforpoorerfamilies).
InMarch,KIHEFObuiltamaternitywardmeanttoprovidemothersandtheirfamilieswithasafespacetogivebirth.ThewardcurrentlyemploysfivemidwivesandholdsgeneralantenatalcarevisitseveryThursday.Duringthesevisits,themidwivescollectpatienthistories,conductphysicalexaminationsandbloodtests,andmonitorthegeneralhealthofthemotherduringherpregnancy.Additionally,themidwivesadvisethemotheronhowtoprepareforherupcomingdelivery,includinginformationonherdietandwhatmaterialstobringwhenshereturnstotheclinicforherdelivery.Incasesofextremecomplicationsduringthebirthingprocess,themidwivesrefermotherstoalocalhospitallocated1.5kmawayfromthematernityward,althoughthereferraltransportationisprovidedbyKIHEFO.Theclinicreliesonword-of-mouthadvertisingbytheircurrentpatientsinordertorecruitexpectingmothers.Thewardalsocaresformothersthatshowupbeforetheirexpectedduedateandprovidespostnatalcareandcheckupsforrecentlydeliveredmothersandtheirneonates.
NeedsIdentification Thissectiondescribestheprocesstheteamtooktoidentifyneedsinthelocalcommunityandageneralsummaryofourresults.Throughoutthisprocess,wehopedto(1)tofamiliarizeourselveswiththestateofmaternalhealthcareinsouthwestUganda,(2)toobserveproblemsregardingmaternalhealththatKIHEFOandthegreaterKabaleregionarefacing,and(3)toselectawell-scopedprojecttobeworkedon

6
withinthefiveweeksoftheprogram.TheMaternalHealthSSLPteamunderwentdifferentmethodsofneedsidentificationformaternalhealth,includingclinicalimmersionandinterviewswithnumerousstakeholders.Thefollowingsectionsoutlinetheprocedurebehindandinsightsgainedineachneed-findingmethod.
ClinicalImmersionWebeganourneedsidentificationbyobservingthevariouswaysKIHEFOdelivershealthcaretoitspatients.Throughoutthisprocess,weengagedinmaternitywardandclinicimmersionandattendedoutreachestoruralvillagesandcommunities,aswellasmonthlyworkshopsforhealtheducationandcheck-ups.
MaternityWard&ClinicKIHEFO'smaternitywardwasourfirstsourceofinformation.Wevisitedthematernitywardonseveraloccasionstospeakwithhealthcareworkerspresentandobservethedeliveryofcare.Thematernitywardstrivestoidentifymothersthatmayexperiencehigh-riskbirthsandrequireadditionalmedicalattentionorprocedures.Thematernitywardiscurrentlynotatthecapacitytoconfidentlyoverseecomplicateddeliveriesthatmayrequirespecialcare.Ifadeliveryisidentifiedashigh-riskattheonsetorinthemiddleoflabor,KIHEFOcurrentlyprovidesemergencytransportwithitsambulancevanfromthematernitywardtotheKabaleGeneralHospital,locatedapproximately1-2kilometersfromtheward.However,inthepresentsystem,patientsstillneedtofindtheirowntransportationtothematernitywardforcare,assistancewithdeliveries,ortransporttotheKabaleGeneralHospitalinhigh-riskcases.
Figure4:MaternalClinicInterior
Oneofthekeyconsiderationsformaternitywardstaffandadministratorsisthecarefulutilizationofresources.Asthewardhasonlybeenopenforhalfayear,theyhavebeenextremelycarefulnottooverextendtheward'scapacities.ThisiswhyANCvisitsareonlyacceptedonedayaweekandtheward'sserviceshavenotbeenbroadcastedtomorepeople.Additionally,therearecurrentlyonlyfivemidwivesandahealthpractitioneronstaff;thus,thewardiscautiousabouttakingintoomanypatientstopreventadropinthequalityofcare.Nonetheless,thewardispoisedtoseemorepatientsandgrowinitscapacityoverthenextyear.Inordertoaccomplishthis,KIHEFOishopingredesignthephysical

7
layoutofthewardinordertomaximizeitsphysicalspacetoseemorepatients,whilestillrespectingpatientprivacyandcomfort.
WealsolearnedaboutandvisitedKIHEFO'sotherhealthcareservices,suchasitsgeneralanddentalclinics.However,wespentlesstimeintheseclinicsaswewantedtofocusoureffortsonbetterunderstandingourtargetpopulationofstakeholdersinthematernityward.
Outreaches:Cervical/BreastCancerScreening,GeneralHealth/HIVScreeningKIHEFOalsoprovidesavarietyofcommunityoutreachservicesinordertoreachpopulationsinruralvillages.Theseservedasgoodopportunitiesforustoobservehealthcaredeliveryinruralsettingsandlearnaboutdailylifestyleforruralpopulations.Inthesecommunityoutreaches,KIHEFOstaff,volunteers,andservicesaretransportedtooneofthemanycommunitiesthathaveestablishedrelationshipswiththeorganization.Theseoutreachesareadvertisedthroughlocalchurches,savingsgroups,andcommunityleadersbeforehand.Eachmonth,therearethreeGeneralHealthExamination/HIVScreeningcamps.Twiceayear,largeGeneralHealthExaminationsarealsoheldforlargerpatientcapacity.KIHEFOhasalsolaunchedWomen'sHealthCamps,whichincludecervicalandbreastcancerscreeningandreferrals,antenatalcareservices,andfamilyplanning.
InordertoestablishsustainablerelationshipswiththelocalpopulationsandcontinuallyseepatientswhomaybeunabletotransportthemselvestoKIHEFO'sclinicsinKabale,thesecampsrecurinthesamecommunities-nonetheless,referralstolocalhealthcarefacilitiesandKIHEFO'sclinicsarestillmadeifadditionalmedicalattentionisdeemednecessary.
Duringtheprogram,wewereabletoattendanoutreachforcervicalandbreastcancerscreeningnearKabaleatKamukiraHealthCenterandanotherforgeneralhealthexaminationsandHIV,syphilis,typhoid,andmalariascreeninginRuhija(neartheImpenetrableForest).Theseoutreachesallowedustoobservetransportationmethods,alongwithlocalterrainandroadworkinruralcommunities.Throughshadowingandassistanceintheseoutreaches,wewerealsoabletolearnaboutthequestion,concerns,andinefficienciesthatplagueruralhealthcare.
Figure5:CervicalCancerOutreach
8
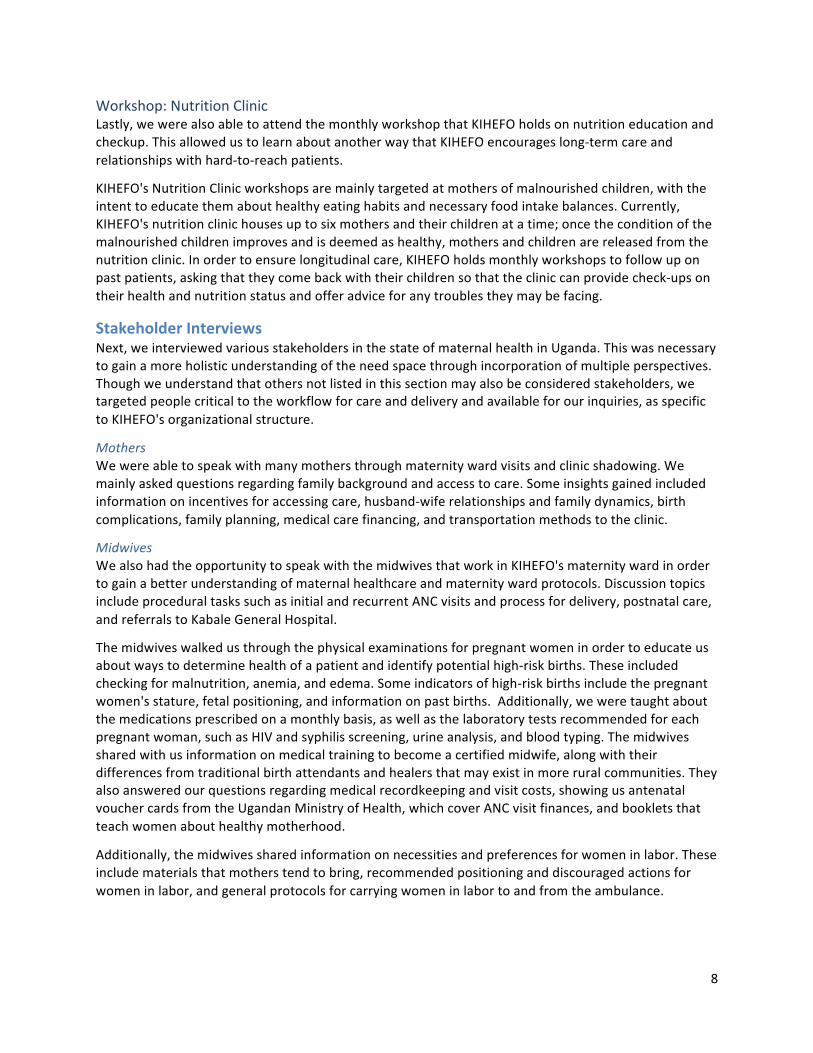
Workshop:NutritionClinicLastly,wewerealsoabletoattendthemonthlyworkshopthatKIHEFOholdsonnutritioneducationandcheckup.ThisallowedustolearnaboutanotherwaythatKIHEFOencourageslong-termcareandrelationshipswithhard-to-reachpatients.
KIHEFO'sNutritionClinicworkshopsaremainlytargetedatmothersofmalnourishedchildren,withtheintenttoeducatethemabouthealthyeatinghabitsandnecessaryfoodintakebalances.Currently,KIHEFO'snutritionclinichousesuptosixmothersandtheirchildrenatatime;oncetheconditionofthemalnourishedchildrenimprovesandisdeemedashealthy,mothersandchildrenarereleasedfromthenutritionclinic.Inordertoensurelongitudinalcare,KIHEFOholdsmonthlyworkshopstofollowuponpastpatients,askingthattheycomebackwiththeirchildrensothatthecliniccanprovidecheck-upsontheirhealthandnutritionstatusandofferadviceforanytroublestheymaybefacing.
StakeholderInterviewsNext,weinterviewedvariousstakeholdersinthestateofmaternalhealthinUganda.Thiswasnecessarytogainamoreholisticunderstandingoftheneedspacethroughincorporationofmultipleperspectives.Thoughweunderstandthatothersnotlistedinthissectionmayalsobeconsideredstakeholders,wetargetedpeoplecriticaltotheworkflowforcareanddeliveryandavailableforourinquiries,asspecifictoKIHEFO'sorganizationalstructure.
MothersWewereabletospeakwithmanymothersthroughmaternitywardvisitsandclinicshadowing.Wemainlyaskedquestionsregardingfamilybackgroundandaccesstocare.Someinsightsgainedincludedinformationonincentivesforaccessingcare,husband-wiferelationshipsandfamilydynamics,birthcomplications,familyplanning,medicalcarefinancing,andtransportationmethodstotheclinic.
MidwivesWealsohadtheopportunitytospeakwiththemidwivesthatworkinKIHEFO'smaternitywardinordertogainabetterunderstandingofmaternalhealthcareandmaternitywardprotocols.DiscussiontopicsincludeproceduraltaskssuchasinitialandrecurrentANCvisitsandprocessfordelivery,postnatalcare,andreferralstoKabaleGeneralHospital.
Themidwiveswalkedusthroughthephysicalexaminationsforpregnantwomeninordertoeducateusaboutwaystodeterminehealthofapatientandidentifypotentialhigh-riskbirths.Theseincludedcheckingformalnutrition,anemia,andedema.Someindicatorsofhigh-riskbirthsincludethepregnantwomen'sstature,fetalpositioning,andinformationonpastbirths.Additionally,weweretaughtaboutthemedicationsprescribedonamonthlybasis,aswellasthelaboratorytestsrecommendedforeachpregnantwoman,suchasHIVandsyphilisscreening,urineanalysis,andbloodtyping.Themidwivessharedwithusinformationonmedicaltrainingtobecomeacertifiedmidwife,alongwiththeirdifferencesfromtraditionalbirthattendantsandhealersthatmayexistinmoreruralcommunities.Theyalsoansweredourquestionsregardingmedicalrecordkeepingandvisitcosts,showingusantenatalvouchercardsfromtheUgandanMinistryofHealth,whichcoverANCvisitfinances,andbookletsthatteachwomenabouthealthymotherhood.
Additionally,themidwivessharedinformationonnecessitiesandpreferencesforwomeninlabor.Theseincludematerialsthatmotherstendtobring,recommendedpositioninganddiscouragedactionsforwomeninlabor,andgeneralprotocolsforcarryingwomeninlabortoandfromtheambulance.

9
TraditionalHealer/TraditionalBirthAttendantInordertobetterunderstandthepracticeoftraditionalmedicineinUganda,wealsovisitedatraditionalhealerandseveraltraditionalbirthattendantsinaruralvillageborderingLakeBunyonyiinsouthwestUganda.Thetraditionalhealerisaleaderinatraditionalmedicinenetwork,andservedasagreatresourceforourinquiriesonthedifferencesindeliveryofcareandpatientrelationships.Wefirstlearnedaboutthedifferenttypesoftraditionalhealers:herbalists,whoprovideherbstotreatmedicalproblems;witchdoctors,whousewitchcrafttocastoutevil;diviners,whopredictfuturehappenings;andtraditionalbirthattendants,whodealwithwomen'sissues,maternity,andpregnancy.Thetraditionalhealeralsoexplainedtousthecurrentpartnershipsthatexistbetweenthosewhopracticetraditionalmedicineandhospitalsandclinics,throughwhichpatientsmaybereferredtohealthcarefacilitiesforfurthercare.Herecognizedthatnotallconditionscanbetreatedorcuredbytraditionalmedicineandencouragedamixtureofthetwoformsofmedicine.Wealsolearnedaboutthemethodsinwhichpeoplereachtraditionalhealers,somecomingbyfootorstretcherfromnearbyruralcommunitiesandsomecomingbyboatormotorvehiclefromplacesasfarasRwanda,Tanzania,andBurundi.
Finally,welearnedabouttheproceduresforcarethattraditionalbirthattendantsfollow,whichincludemonthlycheckupswithphysicalexaminationsandmedicalhistorycollectionstartingfromthefourthmonthofpregnancy.Expectantmothersareencouragedtogotoahealthcenterforadditionalantenatalcaresothattheycanreceiveanantenatalcard,whichmakesiteasierforwomentobeadmittedtohospitalsinthecasethatcomplicationsariseduringtheirdelivery.Thetraditionalbirthattendantsexplainedthattheyalsoguidemothersonhealthynutritionhabits.Herbsareadministeredtomitigateandpreventcomplications.Afterbirth,thetraditionalbirthattendantsarecarefultocheckthatthebabyishealthyandwillrefertoahospitalifanyproblemsareidentified.
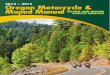
AmbulanceDriver(s)WeinterviewedKIHEFO'sambulancedrivertolearnmoreabouttheemergencytransportationservicesofferedbytheorganization.Hehadbeendrivingtheambulancevansinceearly2016andbeentrainedtonavigatethevansafelyandefficiently.Thoughhehasoccasionallydriventoruralcommunities,thevanismainlyusedwithintowntotransportpatientstoKabaleGeneralHospital-typicallywomeninhigh-risklaborfromthematernityward.Weaskedaboutthetrainingrequiredtodrivethevanandothergeneralinformationregardinghisday-to-dayschedule.HeisnotifiedofpatientstopickuponceaKIHEFOstaffmemberreacheshimbyaphonecall.Hetypicallydrivestheambulanceat80-90kilometersperhour,thoughhemaydriveat50kilometersperhourforrockierterrains.
10
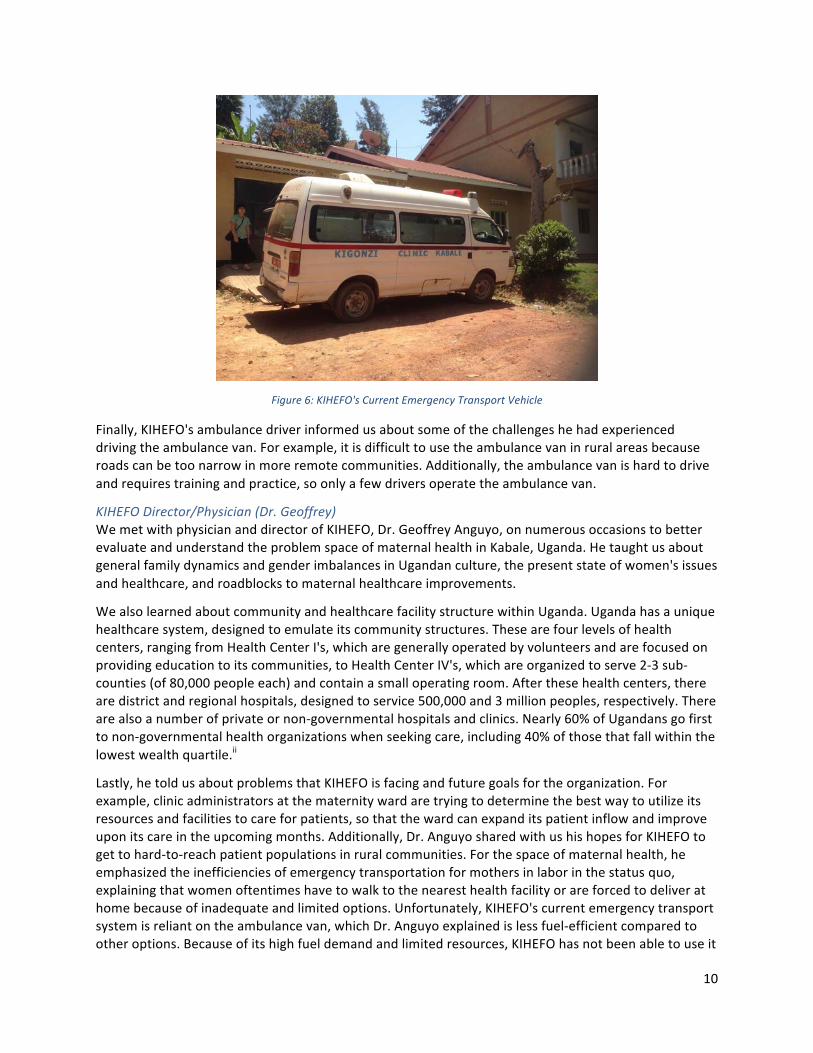
Figure6:KIHEFO'sCurrentEmergencyTransportVehicle
Finally,KIHEFO'sambulancedriverinformedusaboutsomeofthechallengeshehadexperienceddrivingtheambulancevan.Forexample,itisdifficulttousetheambulancevaninruralareasbecauseroadscanbetoonarrowinmoreremotecommunities.Additionally,theambulancevanishardtodriveandrequirestrainingandpractice,soonlyafewdriversoperatetheambulancevan.
KIHEFODirector/Physician(Dr.Geoffrey)WemetwithphysiciananddirectorofKIHEFO,Dr.GeoffreyAnguyo,onnumerousoccasionstobetterevaluateandunderstandtheproblemspaceofmaternalhealthinKabale,Uganda.HetaughtusaboutgeneralfamilydynamicsandgenderimbalancesinUgandanculture,thepresentstateofwomen'sissuesandhealthcare,androadblockstomaternalhealthcareimprovements.
WealsolearnedaboutcommunityandhealthcarefacilitystructurewithinUganda.Ugandahasauniquehealthcaresystem,designedtoemulateitscommunitystructures.Thesearefourlevelsofhealthcenters,rangingfromHealthCenterI's,whicharegenerallyoperatedbyvolunteersandarefocusedonprovidingeducationtoitscommunities,toHealthCenterIV's,whichareorganizedtoserve2-3sub-counties(of80,000peopleeach)andcontainasmalloperatingroom.Afterthesehealthcenters,therearedistrictandregionalhospitals,designedtoservice500,000and3millionpeoples,respectively.Therearealsoanumberofprivateornon-governmentalhospitalsandclinics.Nearly60%ofUgandansgofirsttonon-governmentalhealthorganizationswhenseekingcare,including40%ofthosethatfallwithinthelowestwealthquartile.ii
Lastly,hetoldusaboutproblemsthatKIHEFOisfacingandfuturegoalsfortheorganization.Forexample,clinicadministratorsatthematernitywardaretryingtodeterminethebestwaytoutilizeitsresourcesandfacilitiestocareforpatients,sothatthewardcanexpanditspatientinflowandimproveuponitscareintheupcomingmonths.Additionally,Dr.AnguyosharedwithushishopesforKIHEFOtogettohard-to-reachpatientpopulationsinruralcommunities.Forthespaceofmaternalhealth,heemphasizedtheinefficienciesofemergencytransportationformothersinlaborinthestatusquo,explainingthatwomenoftentimeshavetowalktothenearesthealthfacilityorareforcedtodeliverathomebecauseofinadequateandlimitedoptions.Unfortunately,KIHEFO'scurrentemergencytransportsystemisreliantontheambulancevan,whichDr.Anguyoexplainedislessfuel-efficientcomparedtootheroptions.Becauseofitshighfueldemandandlimitedresources,KIHEFOhasnotbeenabletouseit
11
frequentlytoreachruralcommunities.Inthefuture,KIHEFOhopestoincludethesepopulationsinitscare,astobestservethosethatmayneeditmost.
NeedsIdentifiedTheresultsofourclinicalimmersionandfieldinterviewsconfirmedandaddedcontexttoneedspreviouslyidentifiedinliteratureresearchandrevealedmanynewneedspreviouslyunidentified.Thefollowingaresomeoftheneedsthatweidentifiedfromthisprocess.Indeterminingthedirectionofourproject,wediscussedeachneed,takingintoconsiderationavailableresources,usefulnessforKIHEFO,timerestrictions,andteamcapabilities:
1. Increasecapacityforoutreachhealthservices2. Expandrecruitmentstrategies3. Redesignmaternitywardlayouttomaximizespaceutilizationwhileensuringprivacy4. Preparepostnatalpackets/pilotservicestoensurefollow-upattentionandeducation5. Seekbetteremergencytransportforoutreachtoruralcommunities6. Improveservicesforprematurebabies,suchasanincubatorsystem7. Providehealtheducationopportunitiesduringoutreachhealthservices8. Improvebirthpreparednesswithintegratedfamilyandfinancialplanning
ProblemStatementThoughmanyneedswereidentified,weultimatelyfocusedontheproblemthatwomenintheKigeziregionofUgandaexperiencesignificantchallengestransportingthemselvestohealthcarefacilitiesduringlaboranddelivery.AsthestateofmaternalhealthcareandemergencytransportationinUgandaismultifaceted,theproblemstatementourteamgeneratedisbrokendownintothreeparts.Ourproblemstatementisasfollows:
1. Toassessoptionsforemergencytransportationthroughdesignconsiderationsandanalysis.2. Toidentifyuserpainpointsandevaluateuserfeedbackfortargetedproductimprovement.3. Todevelopasustainablebusinessdistributionanduserprovisionmodelforthedeploymentof
animprovedemergencytransportsystem.
Inordertoaccomplisheachoftheseproblemstatementsubsections,weoutlinedaseriesoftasksthatwouldneedtobeachieved.
Task1:UnderstandingTransportationBarriersforMaternalHealthcareToassessoptionsforemergencytransportation,weconductedneed-findingthroughclinicalandcommunityimmersionandstakeholderinterviews,aswellasliteraturereviewofpastresearch.
Task2:EvaluatingMotorcycleAmbulancesasanEmergencyTransportSolutionWeevaluatedpredicateproducts,developedalistofmotorcycleambulancedesignconsiderations,andcollectedinformationonmanufacturingcapabilities,resources,andcosts.
Task3:ImprovingMotorcycleAmbulancesforApplicationinKigezi,UgandaWeconductedastudytounderstanduserpainpointsandpreferencestorecommendproductimprovements.Tobetterengageourinterviewsubjectsandsimulatethereal-lifeproduct,weprototypedcomponentsofamotorcycleambulancetoaidinourinterviewprocess.
12
Task4:CreatingaBusinessModelforProvidingMotorcycleAmbulanceServiceinKigezi,UgandaWeconductedawillingness-to-paystudytobetterunderstandtheusergroup.Additionally,wepreparedabusinessandfinancialmodeltodetermineKIHEFO'scurrentmodelforprogramsustainability.
Task1:UnderstandingTransportationBarriersforMaternalHealthcareThebarrierstomaternalhealthcareremainnumerous.OneofthelargestchallengesweidentifiedintheKigeziregion,however,wastheabsenceofanaffordable,comfortableandsafetransportationmethod,formothersinlabortravellingtohealthcentersfortheirdeliveries.Commonlyusedmodesoftransportarebymotorcars(cars),bodabodas(motorcyclesforhire),stretchers,andfoot(walking).
Transportationisamultiprongedissuethatreflectstheintricacyofmaternalhealthcare.Understandingthetopicfurtherrequiresknowledgeofthe‘ThreeDelaysModel’xiv,whichaddressesthreeparticularpillarsthatmayhinderaccesstomaternalhealthcare:
1. Delayindecisiontoseekcare:Thismayoccurduetoanumberoffactorssuchas,limitedawarenessandknowledgeabouthealthcenterservices,financialbarriers,familydynamics,culturalnormsandimplications,etc.
2. Delayinreachingcare:Thispertainsdirectlytothetopicoftransportwhileseekingmaternalhealthcareservices.Factorssuchastransportationcosts,roadconditions,distancetothehealthcenter,andtimeofday,amongothershavefar-reachingrepercussionsonmothers’abilityandwillingnesstopursueservicesathealthcenters(aswillbeexplainedfurtheron).
3. Delayinreceivingadequatehealthcare:Itisnotuncommonforhealthcenterstobeunderequippedorpoorlyresourced,especiallyinregionswhereitisdifficulttoacquireappropriateequipmentorhiremedicalserviceadministrators.
Financialbarriersserveasoneofthemostdauntingchallengestotransportationavailabilityandaccess.Thepricesvarydependingonthemodeoftransportaswellasthedistancetravelled.Additionally,manyvillagesareonlyconnectedtothetownbyroadswithroughterrain(oftennarrowandrocky),therebymakingitextremelydifficultforcertainkindsoftransporttopenetrateintothosecommunities.Othercommunitiesmaysimplynothavetransportationoptionsreadilyavailableatmothers’disposaliftheyaretoofarofffromtown,thereforepushingthewaitingtimefortransporttoacoupleofhours,ifnotmore.Timealsoplayedacriticalroleinseekingtransport.Oneofthemothersweinterviewedstatedthatshehadtoresorttoahomebirthbecausethechancesofherbeingabletofindtransportatnightwereextremelysmall.
BeforedelvingintothecurrenttransportspaceinsouthernUganda,wedecidedtoassesswhyconventionalambulanceshadnotmadetheirmarkintheregionyet.Duringourpreliminaryinvestigationintotransportationmodesforlabourtransits,wediscernedseveralshortcomingswithtraditionalambulancevehiclesandservices.Firstly,traditionalambulancevehiclescanonlybedrivenbycertifiedambulancedriverswhohaveacertainamountofmedicalexperienceandhavebeenlicensedtodrivelargevehicles(suchasthetraditionalambulance).Secondly,traditionalambulancevehiclescannotreachcertaincommunitiesandvillagesbecauseoftheirinabilitytonavigateonnarrow,unfriendlyterrain(suchasthenarrowdirt,rockyroads)whichareubiquitousintheKigeziregion.Additionally,thecostsofdrivingatraditionalambulancevehicleareveryhighandthistransportationoptionhasnotservedaseconomicallyfeasibleformostcommunitiesandvillages.Suchcostsnotonlyincludeinitialcapitalexpenditures,butalsoincludetherunningrepairandoperationexpensesofthesefuelinefficientvehiclesthatencountermanymaintenanceissueswhiletraversingtheroughterrainintheregion.Theaforementionedpointstherebyrenderthetraditionalambulanceunsustainableand
13
unaffordabletothevastmajorityofmothersseekingtransportationservicesfordelivery.Wethenmovedontoexaminingtheothertransportoptionsavailable,andcurrentlyinuse.
Carsarethemostexpensiveoption,butarelessprevalentindistantvillagesandcommunities.Theyhappentobethemostcomfortableoptioninuse,buttheirpriceovershadowsthebenefitsofcomforttomostpeopleintheregion.Carsarealsounabletotraveltocommunitiesthatcanonlybereachedbynarrowdirtroads.
Bodabodas(motorcycles)serveasanothertranportoptionandtendtobewidelyavailableforhire.Onefactorthatlargelydictatestheircommonuseistheirlowprices(theytendtobesubstantiallycheaperthancars).Itis,however,notuncommonforbodadriverstodemandhigherratesifpregnantorailingpeoplerequestthemtodriveslowerand‘morecautiously’,simplybecausedoingsoonamotorcycleisachallengingtask.Uponinterviewingmotherswhohadusedbodasduringtheirdeliverytransits,weconfirmedthatsittingonthebackofabodawasbothpainfulandstressfulformothersinlabour.Bumpyroadstendedtoexacerbatetheconditionofmothers(bothphysiologicallyandpsychologically),andsomemothersfearedthechancesofcomplications.
Itisalsoimportanttonotethatsomecommunitiesmakeuseofstretchers,whichareoftenprovidedthroughgroupinitatives.Fromourinterviewswithmothersincommunitygroups,welearntthatmemberscontributetothegroupinsomeformofafinancialway;mostgroupshaveamonthlyfeeinadditiontoaone-timeentryfee(valuesvaryquitesubstantially),andthemoneycollectedisusedtopayforpooledresources.TheNgozigroup,forexample,savesmoneytopayformembers’medicalbillsandemergencytransportationcosts(inadditiontoburialandfuneralcosts).Stretcherservicesareoftenofferedtothepregnantandthesick,asoneofthebenefitsofbeingapartofthecommunitygroup.Stretchers,however,byvirtueofbeingmanpowered,tendtobelargelyinefficientanditoftentakeshourstotransportapatienttoahealthcenterwhichmaybeonlyafewkilometersaway.Additionally,thismethodrequiresatleasttwopeople,ifnotmore,sinceitisquiteatiresomeandtaxingtaskanditiscommonforpeopletorotateshiftscarryingthestretcher.
Ifmothersdonothaveanyofthesetransportationmethodsavailable,theyeitherresorttowalking,whichcanbeaincrediblyarduousexperience,ortheydeliverintheirhomeswithwhateverminimalmeanstheymayhave.Bothofthesemayposeasgraverisks,particularlyifthemotherrequiresemergencycareanditistoofartobefound.
WithregardstoKIHEFO,theorganizationisonlyabletouseatraditionalambulancefortheshort(approximately3km)patientreferraljourneys(fromitsmaternitywardtooneofthelocalhospitals)inthecasethatbirthcomplicationsariseorifaproceduredemandsmoreresources(suchasacesaeriansection)thanwhatthewardcanprovide.Themothers,however,needtofindtheirowntransportfortheirinitialjourneytothematernityward.
Giventhedearthofanaffordable,comfortableandsustainabletransportoptionintheKigeziregion,webeganexploringthepossibilitiesofconvertingthemotorcycle,currentlythemostubiquitiousvehicle,intoamoresafetransportationoptionformothersgoingthroughlabour.Thiswaswhenweturnedourheadstowardsthenotionofthemotorcycleambulancecarriageattachment.
Task2:EvaluatingMotorcycleAmbulancesasanEmergencyTransportSolutionInordertoaddressthisneedstatement,wedecidedtofocusonmotorcycleambulancesforourproject.Thiswasduetomanyreasons,includingtheshortcomingsofothertypesoflocalemergencytransport
14
options.Thesehavebeendetailedaboveandprovidemotivationforlookingatotheremergencytransportoptions.Additionally,motorcycleambulancesareacheaperoption,cannavigateonroughterrain,andcapitalizeontheextensivemotorcycletaxiservice.
In1992,theUgandanmarketstartedtoincludemotorcycles(alsoknownasbodabodasorbodas),leadingtoagrowthinthemotorcyclemarketoverthenextseveralyears.Inpart,thiswasduetonewregulationsbytheUgandangovernmentthatbecamemorerelaxedonimportlawsregardingvehiclesolderthan5yearsold.Withinatowncenter,therearehundredsofpeopleinvolvedinthemotorcycletaxibusiness,includingthosewhoowntheirownmotorcycleandthosewhorentthemouttodriversonaweeklybasis.Themotorcycletaxidrivers(alsoknownasbodabodadrivers)offertheirservicestoindividualswhoneedtransportation.And,inregardstoemergencytransport,manywomencurrentlyusebodastotransportthemselvestoaccessmedicalservicecenters.
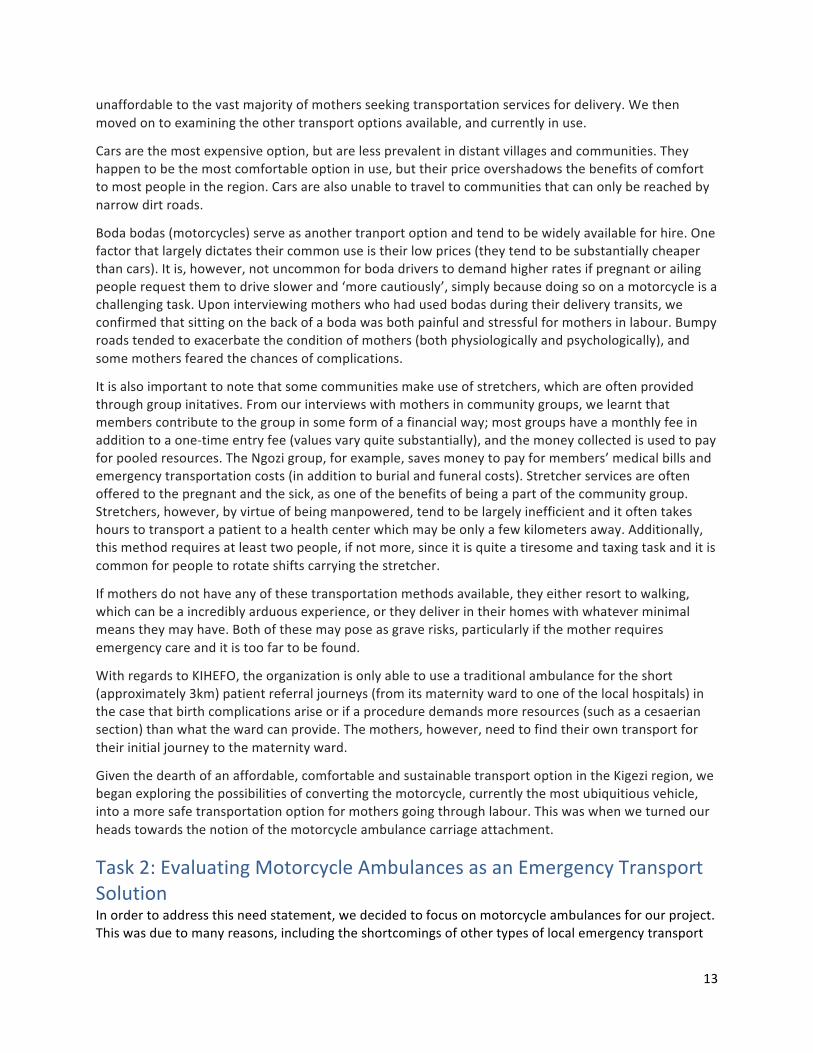
Inotherplacesaroundtheworld,therehavebeenmodificationstomotorcycleandbicycletransportoptionstofacilitateemergencytransportation.Theappendixdisplaysalistofbicycleandmotorcycleambulancesthathavebeenutilizedindevelopingcountriesaroundtheworld.BicycleambulanceshavebeendevelopedanddistributedwithinNigeria,Malawi,Uganda,Zambia,Nepal,andIndia.Thesesystemshavebeenbeneficialforcommunitieslocatedwithina5-10kmradiustomedicalservicecentersandaremoreeffectiveforshortertransportdistances.Theirpopularitycameinthe1990swhenlocalhealthepidemics,includingMalariaandHIV/AIDSoutbreaksputadditionalstressonhealthcareservices.
Figure7:BikecartBicycleAmbulancedeployedinZambia
However,becauseoftheterrainandlanduseoftheKigeziregion,bicycleambulancesarenotwellsuitedforemergencytransport.ThemajorityofthepopulationinKabalelivesinvillagesorhomeswithinthemountainousandhillyregions.Thiscreatesamuchmorecomplexproblem,asreachingmedicalservicecenterswiththeresourcestoaddressemergencycasesaredistantforamajorityofthepopulation.Unlikebicycleambulances,therearecurrentlylessemergencytransportationoptionsthatincorporateamotorcycle.Thesemotorcycleambulancesaremoreexpensivethantheirbicycleambulancecounterparts,butaremoreadepttotransportheavierloadsthroughdemandingterrains.
Regardlessofthetypeofmotorcycleambulance,thereareseveralconditionsthatmustbemetforthemotorcycleambulancetobeabletooperateandprovidesafetravelforpassengers.Mostoftheseconditionscomedowntomotorcyclerequirements.Thepowerofthemotorcyclehastobeableto
15
handlethetrailer’sweightandmomentumaswellasanyadditionalpassengersonthebackofthemotorcycle.Thereareseveralconditionsthatshouldbemet:fourstrokeengine(whichprovidesmoretorqueandfuelefficiency),near150-200cc(thougha125ccmotorcyclecouldworkifwell-maintained),minimum8kWattstopullnearly350kg,andaminimumof15bhp.xvInthecasethatthemotorcycledoesnotmeettheseconditions,therecouldbedamagetothemotorcycle,suchasdecreasedfuelefficiency,orinabilitytomeetitsexpectedfunctionality.Inpastreviewsofmotorcycleambulances,therehavebeendiscussionsofhowtheambulanceattachmentchangesthefuelconsumptionandoperationalcapacityofthemotorcycle.Ithasbeencitedthatfuelconsumptioncanincreasefrom5-8km/literto25-30km/literwhenthemotorcycleambulanceisdrivenonroughterrain.xv
MotorcycleAmbulanceDesignConsiderationsThemotorcycleambulancehasseveralkeytechnicalconsiderationstoensuresafetyandreliabilityforpatientemergencytransport.Thefollowingsectiondetailsseveraloftheseconsiderationsanddiscussestheirimportance,takingintoaccountthedesignrequirementsandlimitationsdetailedintheprevioussection.
AmbulanceOrientationTherearecurrentlythreetypesofmotorcycleambulancesonthemarket.Eachoftheseproductsprovidessomethingdifferentandisabletoaddressdifferentterrainsandenvironmentalconditions.Thisisbecauseofthechangeinbalanceofthevehicleandexpandedwidthofthesystem.
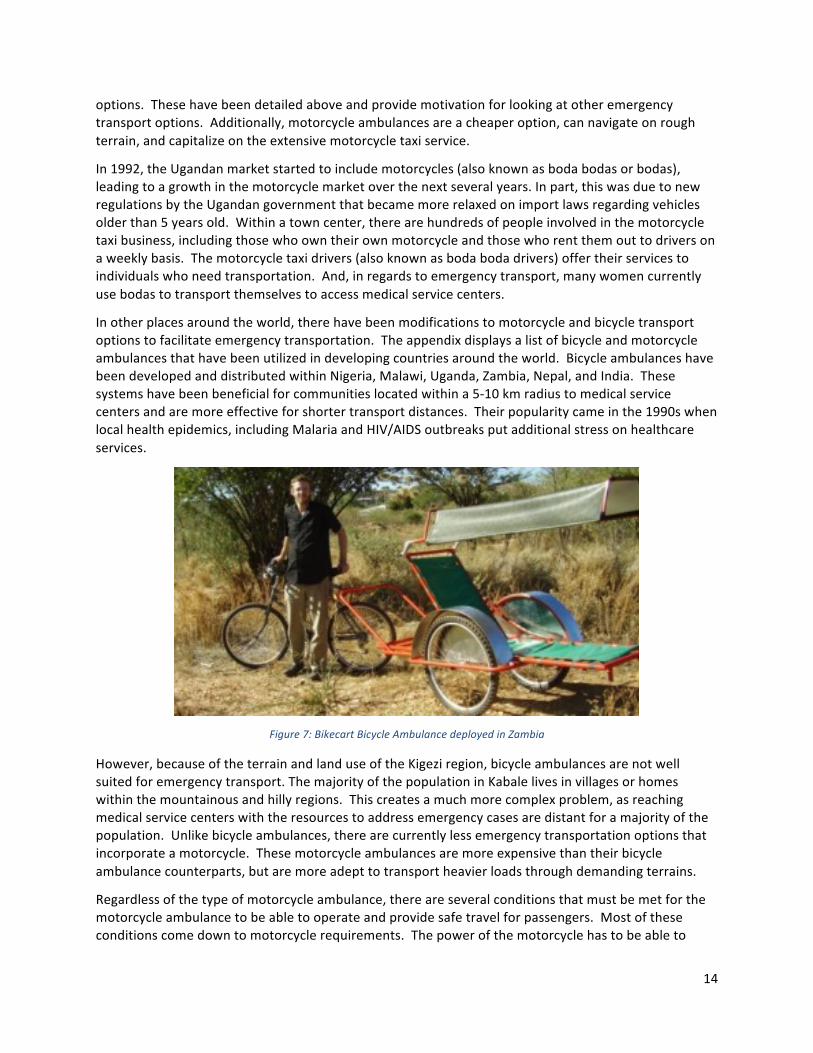
Table1:OrientationComparison
Name Description Comparisons Pictures
Backattachment
Attachmentlinkstotheback,similartoatrailerbedorwagon.Person’sorientationcanvaryfacingtowardsorawayfromthemotorcycle
Advantages:Thisbackattachmentishelpfulforthedriverbecauseitiseasiesttocontrolthemovementofthemotorcycle,astheambulanceisinlinewiththedirectionofthemotorcycle.
Disadvantages:Doesnotmovewiththemotorcycle
Sidecarattachment
Attachmenttothemotorcycleisonthesideoftheframe.
Advantages:Carriagemoveswiththemotorcycle
Disadvantages:Makesthemotorcyclemoredifficultfordriverstooperate;canapplyunduelateraltorsion
16
tothemotorcycle
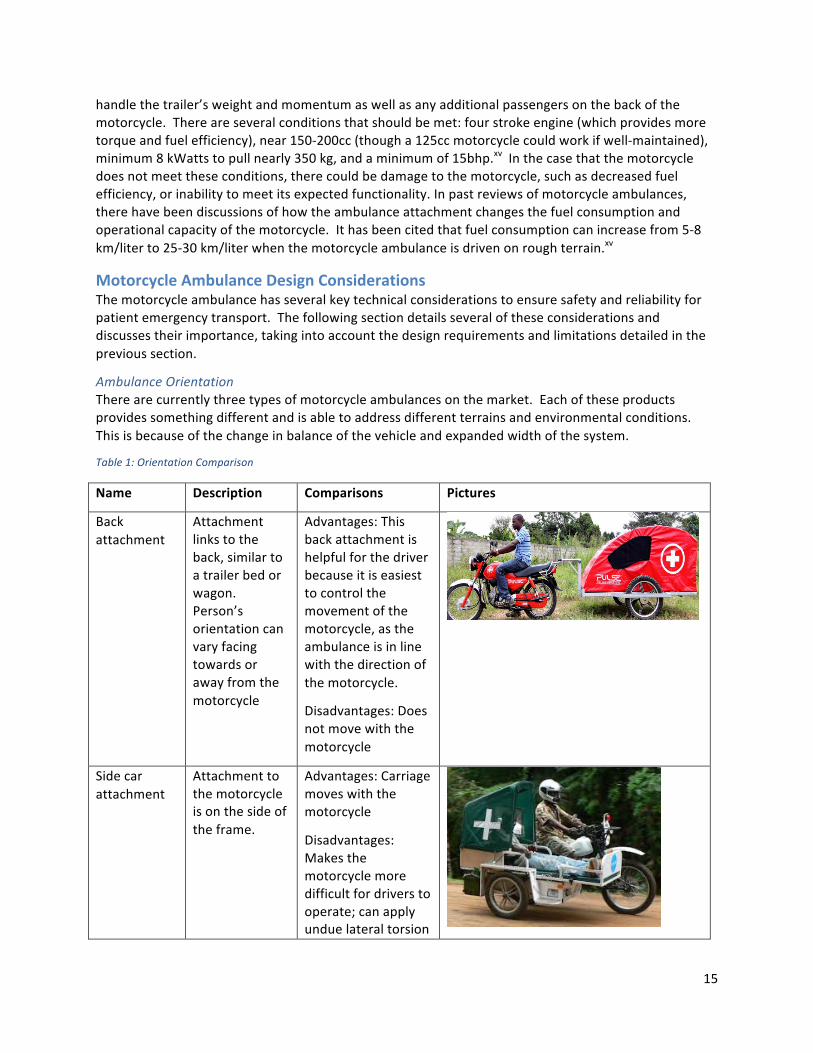
Threewheelmotorcycleambulance
Theback,typicallyusedforcarryingcargo,isconvertedintoacarriageforpatienttransport.
Advantages:Abletotransportheavyloads
Disadvantages:Moreexpensiveandlessreadilyavailable.Typicallyneedstobecustom-madetoorder.
Thedifferencesbetweenthesethreetypesofmotorcycleambulancesarenotjustrestrictedtotheirphysicaldesigns.Therearecriticalmanagement,ownership,andmaintenanceconsiderationsthatdifferbetweenthetypesofmotorcycleambulances.Thedifferencesaremostpronouncedbetweenthosedesignsthatcanbeeasilyattachedanddetachedtomotorcyclesandthosethatcannot,orthosewhichintegratethemotorcyclebodyinthecarriage(similartothethree-wheelmotorcycleambulance).Theambulanceattachmentmodelcapitalizesonthemotorcycletaxiserviceandthenetworkofmotorcycletaxidriversthatalreadyexists.Theattachmentcanbemovedbetweenmotorcyclesandallowsmoreflexibilityfordrivers,incasedriversneedabreakduetohours,experiencetheirownemergencysituations,orleavetheserviceandthereisaneedforanewdriver.Themotorcycleambulancethatdoesnotallowforambulancecarriagedetachmentrequirestheavailabilityofasingulardrivertoprovidetheservice.Iftheambulanceneedsmaintenance,thewholemodelcanbedecommissioned.Thisisnotthecasefortheattachmentmodel;ifthemotorcycleneedsmaintenance,theambulanceattachmentcanberemovedandtransferredtoanothermotorcycle.
AttachmentSelectionForanytrailersystem,theattachment,whichencompassesboththehitchonthetowingvehicleandthecouplingjoint,isincrediblyimportanttoconsider,asitaffectsthestabilityofthesystemaswellasthenavigationalcapacityoftheambulancecarriage.
HitchThehitchisthemechanismonamotorcycleontowhichtheambulancecarriageisattached.Thehitchitselfshouldbesturdyandconnectedtoatleastfournon-movingpointsalongthebike(i.e.,itcannotbeconnectedtothesuspensioncomponentsorshockabsorbers).Thehitchshouldbeclosetotheheightoftheaxleoftherearwheel–anyhigher,andtherear-wheelwilllightenduringbraking;anylower,andthefrontwheelwilllightenduringbraking,creatingawobble.xvi
CouplingJointThecouplingjointallowsforangulardisplacementbetweenthemotorcycleandthetrailerandisanintegralpartforthefunctionalityandnavigationalcapabilityoftheentiresystem.AstheroadsintheKigeziregionaregenerallyunpavedandrocky,commonoff-roadcouplingmechanismswereconsidered.Anoverviewofdifferentoff-roadcouplingjointsisincludedbelow.Inadditiontothecouplingjoint,thereshouldalsobeasafetychainbetweenthetrailerandthehitchinthecaseofattachmentfailure.
17
Table2:CouplingJointsComparison
Name Description Comparisons Pictures
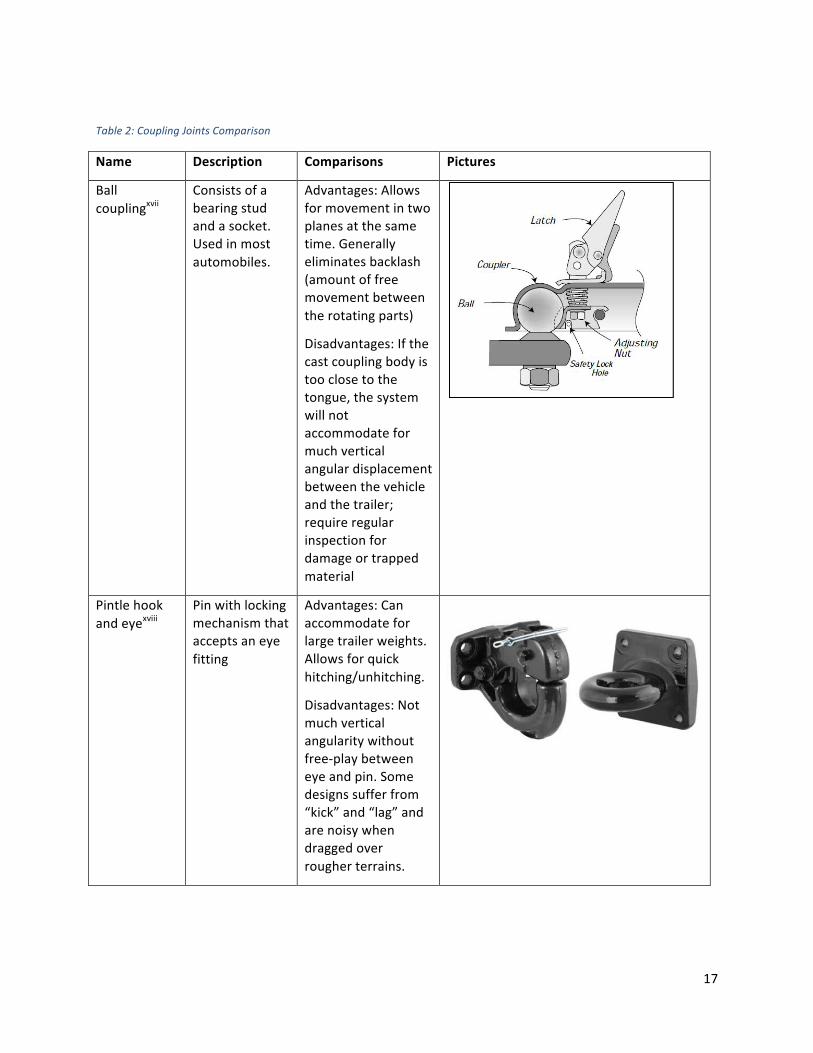
Ballcouplingxvii
Consistsofabearingstudandasocket.Usedinmostautomobiles.
Advantages:Allowsformovementintwoplanesatthesametime.Generallyeliminatesbacklash(amountoffreemovementbetweentherotatingparts)
Disadvantages:Ifthecastcouplingbodyistooclosetothetongue,thesystemwillnotaccommodateformuchverticalangulardisplacementbetweenthevehicleandthetrailer;requireregularinspectionfordamageortrappedmaterial
Pintlehookandeyexviii
Pinwithlockingmechanismthatacceptsaneyefitting
Advantages:Canaccommodateforlargetrailerweights.Allowsforquickhitching/unhitching.
Disadvantages:Notmuchverticalangularitywithoutfree-playbetweeneyeandpin.Somedesignssufferfrom“kick”and“lag”andarenoisywhendraggedoverrougherterrains.
18
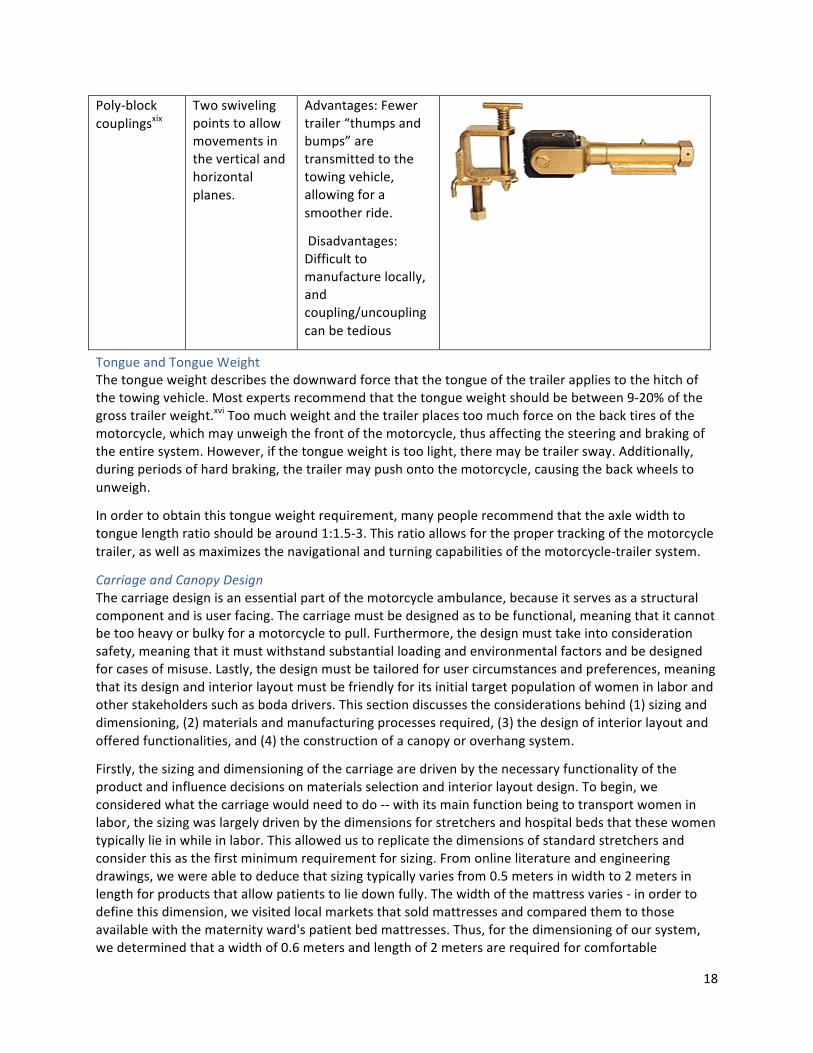
Poly-blockcouplingsxix
Twoswivelingpointstoallowmovementsintheverticalandhorizontalplanes.
Advantages:Fewertrailer“thumpsandbumps”aretransmittedtothetowingvehicle,allowingforasmootherride.
Disadvantages:Difficulttomanufacturelocally,andcoupling/uncouplingcanbetedious
TongueandTongueWeightThetongueweightdescribesthedownwardforcethatthetongueofthetrailerappliestothehitchofthetowingvehicle.Mostexpertsrecommendthatthetongueweightshouldbebetween9-20%ofthegrosstrailerweight.xviToomuchweightandthetrailerplacestoomuchforceonthebacktiresofthemotorcycle,whichmayunweighthefrontofthemotorcycle,thusaffectingthesteeringandbrakingoftheentiresystem.However,ifthetongueweightistoolight,theremaybetrailersway.Additionally,duringperiodsofhardbraking,thetrailermaypushontothemotorcycle,causingthebackwheelstounweigh.
Inordertoobtainthistongueweightrequirement,manypeoplerecommendthattheaxlewidthtotonguelengthratioshouldbearound1:1.5-3.Thisratioallowsforthepropertrackingofthemotorcycletrailer,aswellasmaximizesthenavigationalandturningcapabilitiesofthemotorcycle-trailersystem.
CarriageandCanopyDesignThecarriagedesignisanessentialpartofthemotorcycleambulance,becauseitservesasastructuralcomponentandisuserfacing.Thecarriagemustbedesignedastobefunctional,meaningthatitcannotbetooheavyorbulkyforamotorcycletopull.Furthermore,thedesignmusttakeintoconsiderationsafety,meaningthatitmustwithstandsubstantialloadingandenvironmentalfactorsandbedesignedforcasesofmisuse.Lastly,thedesignmustbetailoredforusercircumstancesandpreferences,meaningthatitsdesignandinteriorlayoutmustbefriendlyforitsinitialtargetpopulationofwomeninlaborandotherstakeholderssuchasbodadrivers.Thissectiondiscussestheconsiderationsbehind(1)sizinganddimensioning,(2)materialsandmanufacturingprocessesrequired,(3)thedesignofinteriorlayoutandofferedfunctionalities,and(4)theconstructionofacanopyoroverhangsystem.
Firstly,thesizinganddimensioningofthecarriagearedrivenbythenecessaryfunctionalityoftheproductandinfluencedecisionsonmaterialsselectionandinteriorlayoutdesign.Tobegin,weconsideredwhatthecarriagewouldneedtodo--withitsmainfunctionbeingtotransportwomeninlabor,thesizingwaslargelydrivenbythedimensionsforstretchersandhospitalbedsthatthesewomentypicallylieinwhileinlabor.Thisallowedustoreplicatethedimensionsofstandardstretchersandconsiderthisasthefirstminimumrequirementforsizing.Fromonlineliteratureandengineeringdrawings,wewereabletodeducethatsizingtypicallyvariesfrom0.5metersinwidthto2metersinlengthforproductsthatallowpatientstoliedownfully.Thewidthofthemattressvaries-inordertodefinethisdimension,wevisitedlocalmarketsthatsoldmattressesandcomparedthemtothoseavailablewiththematernityward'spatientbedmattresses.Thus,forthedimensioningofoursystem,wedeterminedthatawidthof0.6metersandlengthof2metersarerequiredforcomfortable
19
transportationofapatientwhileextendedandlyingdown.Wealsoconsideredtheoptionofallowingacaretakertoaccompanythepatientinthecarriage.Dependingonhowthecaretakerisoriented,thiswouldalsoinfluencethesizingofthecarriage.This,however,wouldrequiremorespaceinthecarriage,addingweighttothecarriageandoverextendingitfurtherinlengthorwidth.Werecognizedthatthismightnegativelyaffecttheproduct'sabilitytobepulledbyamotorcycleandobstructthebodadriver'sfieldofview.
Next,wehadtoconsiderthematerialsthatwouldcomposethecarriage,alongwiththemanufacturingthatwouldberequiredtoproduceandjoinindividualparts.Someoptionsincludedworkingwithsteelsheets,steelroundpiping,steelsquaretubing,andacombinationofeach.Wehadselectedmildsteelastherawmaterialforconstructionbecauseofitsavailability,strength,andmanufacturingabilityinUganda.Additionally,steelisafrequentmaterialselectionforautomobileandmotorvehiclecomponents.Inordertojoinpiecestogether,theideaofweldingmetaltogether,perhapswiththeaddedstrengthandsupportofanglebars,wassuggested.
Anotherfactorincarriagedesignwastheinteriorlayoutandfunctionalitiesthatwouldbeincorporatedintothesystem.Thiswasdrivenbyinformationprovidedbymidwivesandmothers,alongwithdecisionsandjustificationsmadeforpredicatesystems.Arecommendedfeaturewastocreatearecliningbedinordertooffermothersoptionsforpositioningwhiletravelingandinlabor.Additionally,motherstendtowalkorbecarriedbystretchertotheambulance;thus,wewantedtocreateasystemthatwouldbecompatiblewiththesedifferentoptionsandallowthewomantocomfortablyloadthecarriage.Someideasincludedbuildingastretcherintoourtransportsystemsuchthatitcanbeusedtopickupthewomananddropheroff.Webrainstormedandsketchedaseriesofstretcher-compatiblesystems,whichincludedslidingandlockingmechanismstoplacethestretcherintothecarriage.
Lastly,wediscussedoptionsforacanopyoroverhangsystem.Themainrequirementforthiswastokeeptheframeaslightaspossible,whilestilleffectiveinofferingpatientprivacyandprotectionfromenvironmentalfactorssuchasrainandsun.Tarpaulinwastherecommendedmaterialforcoverage,asitwascheap,effective,andlocallyavailable.Tosupportthetarpaulin,weconsideredsteeltubingextendinguprightalongtheedgesofthecarriageand/oratthefourcorners,alongwithcross-sectionsacrossthetopofthecanopytogivetheframestructure.Bamboowasanotheroptionwediscussedforthecanopyframebecauseofitslightweight,butdidnotfindnearlyaslocallyavailable,longlasting,orstrong.
WheelsThewheelselection,placement,andattachmenttotheframeareimportantforanumberofreasons.Firstly,theyprovidethemechanismthatwillallowtheambulancetotrailbehindthemotorcycleatthesamespeed.Secondly,theysupportthemajorityoftheweightoftheframeandcarriage.Lastly,theattachmentmechanism,whenconsideringsuspension,candampenthebouncingmovementscausedbyuneventerrain,whichisprevalentinruralUganda.Thissectiondiscussesthe(1)wheelspecificationsandloadcapacity,basedonthelocalavailablemotorcyclewheelmarketinKabale,Uganda,(2)thelocationofthewheelsontheframetoevenlyandeffectivelydistributetheloadoftheframeandcarriage(whenfullyloaded),and(3)themechanismforattachingthewheelstotheframe,includingthedesignsconsiderations.
Motorcyclewheelspecificationsconveyagreatdealofinformation.Thespecificationsincludethespeedrating,loadrating,rimdiameter,aspectratio,andsectionwidth.Basedonthesenumbers,itispossibletounderstandthelimitationsoftheambulanceandthedriverrestrictionstodrivingbehaviors/mechanisms.InKabale,Uganda,therefewoptionsformotorcycletires.TheBajajBoxer
20
motorcyclesthataremostcommonlyusedutilizea3.00x17,45P–100/90x17,55Pwhichconveysthatthewheelcapacityis165kgand218kg,respectively.xx
Theaxle,andthereforethewheel,locationontheframeshouldbeselectedtobalancetheloadeffectively.Inmanycases,expertsadvisethattheaxlelocationshouldbebehindthecenteroftheload.Thetongueoftheframeandhitchcombinationcanhandle15%ofthecarriageloadandthereforetheaxlelocationcanbefartheralongtheframelocation.xxi
Thewheelconnectionsnotonlydetailtheconnectionbetweenthewheelsandtheframe,butalsoservesasthesuspensionsystemoftheattachment.ThesuspensionsystemisespeciallyimportantforemergencytransportintheKigeziregionbecauseoftheunpavedroadsandthehillyterrain.Together,thesetwofactorscanincreasethediscomfortfortheambulancepassenger.Addingsuspensiontotheattachmentcandampenthevibrationsandmovementsoftheattachmentasitpassesoverroughterrain.
Table3:WheelConnectionComparisonxxii
Connection Description Comparisons Pictures
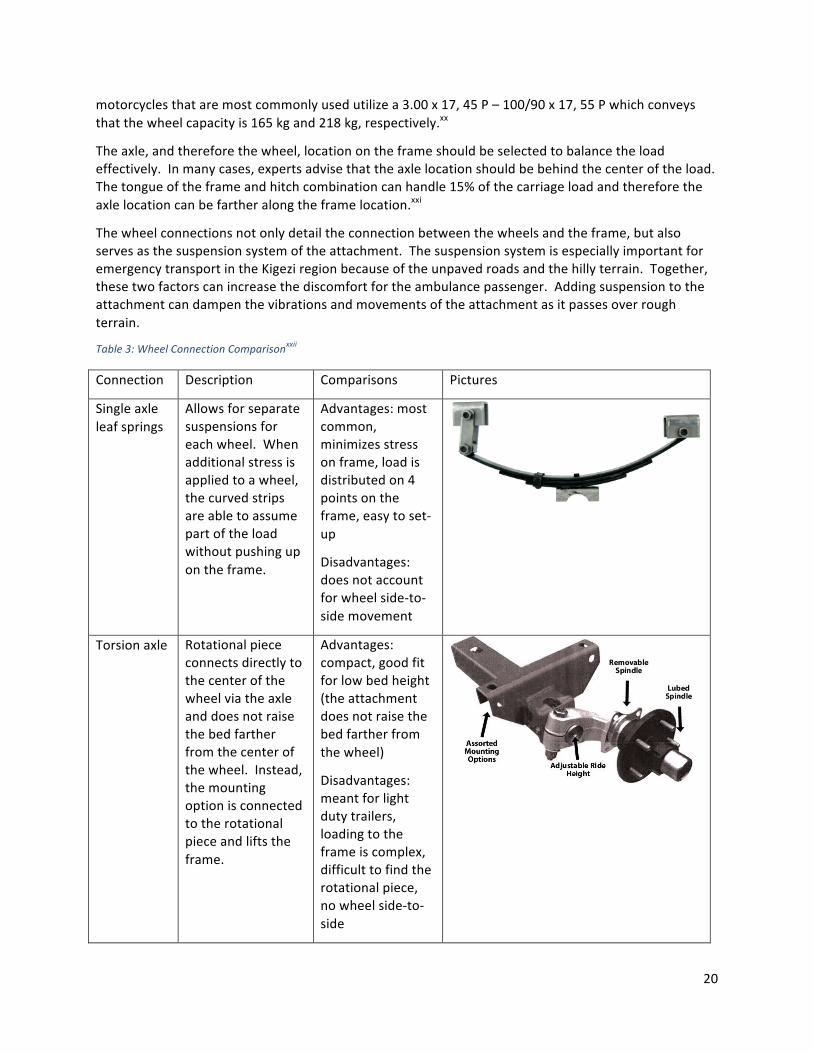
Singleaxleleafsprings
Allowsforseparatesuspensionsforeachwheel.Whenadditionalstressisappliedtoawheel,thecurvedstripsareabletoassumepartoftheloadwithoutpushingupontheframe.
Advantages:mostcommon,minimizesstressonframe,loadisdistributedon4pointsontheframe,easytoset-up
Disadvantages:doesnotaccountforwheelside-to-sidemovement
Torsionaxle Rotationalpiececonnectsdirectlytothecenterofthewheelviatheaxleanddoesnotraisethebedfartherfromthecenterofthewheel.Instead,themountingoptionisconnectedtotherotationalpieceandliftstheframe.
Advantages:compact,goodfitforlowbedheight(theattachmentdoesnotraisethebedfartherfromthewheel)
Disadvantages:meantforlightdutytrailers,loadingtotheframeiscomplex,difficulttofindtherotationalpiece,nowheelside-to-side
21
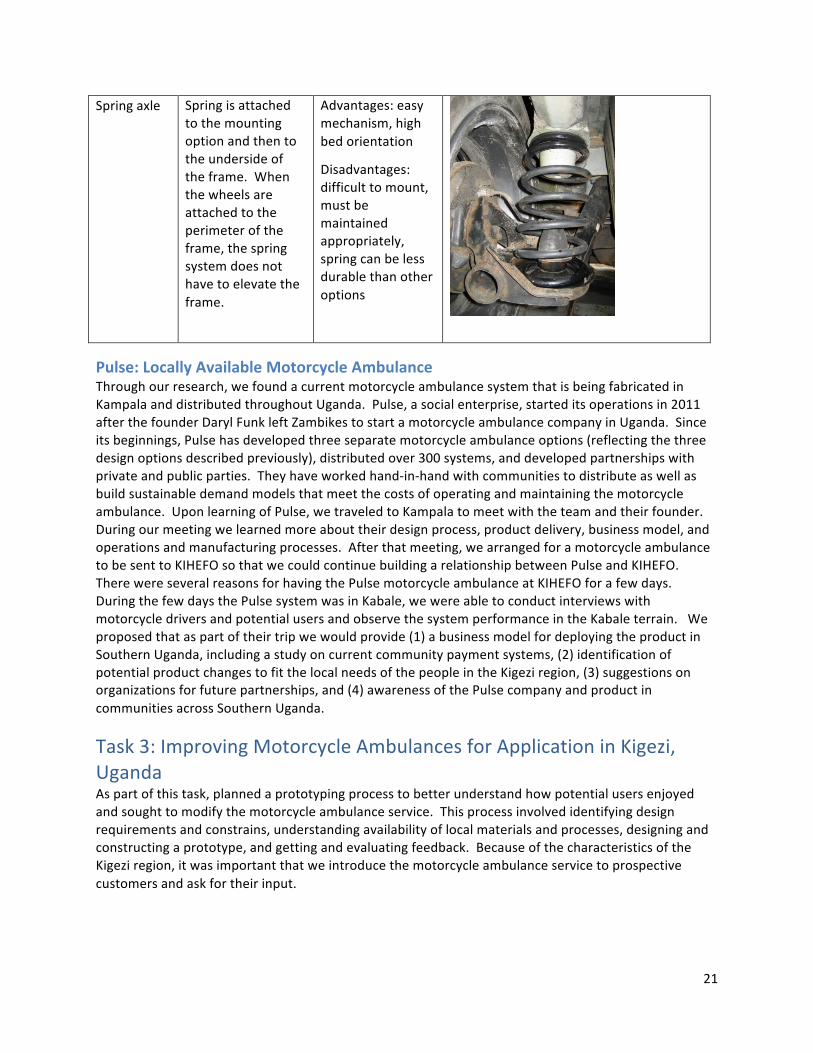
Springaxle Springisattachedtothemountingoptionandthentotheundersideoftheframe.Whenthewheelsareattachedtotheperimeteroftheframe,thespringsystemdoesnothavetoelevatetheframe.
Advantages:easymechanism,highbedorientation
Disadvantages:difficulttomount,mustbemaintainedappropriately,springcanbelessdurablethanotheroptions
Pulse:LocallyAvailableMotorcycleAmbulanceThroughourresearch,wefoundacurrentmotorcycleambulancesystemthatisbeingfabricatedinKampalaanddistributedthroughoutUganda.Pulse,asocialenterprise,starteditsoperationsin2011afterthefounderDarylFunkleftZambikestostartamotorcycleambulancecompanyinUganda.Sinceitsbeginnings,Pulsehasdevelopedthreeseparatemotorcycleambulanceoptions(reflectingthethreedesignoptionsdescribedpreviously),distributedover300systems,anddevelopedpartnershipswithprivateandpublicparties.Theyhaveworkedhand-in-handwithcommunitiestodistributeaswellasbuildsustainabledemandmodelsthatmeetthecostsofoperatingandmaintainingthemotorcycleambulance.UponlearningofPulse,wetraveledtoKampalatomeetwiththeteamandtheirfounder.Duringourmeetingwelearnedmoreabouttheirdesignprocess,productdelivery,businessmodel,andoperationsandmanufacturingprocesses.Afterthatmeeting,wearrangedforamotorcycleambulancetobesenttoKIHEFOsothatwecouldcontinuebuildingarelationshipbetweenPulseandKIHEFO.TherewereseveralreasonsforhavingthePulsemotorcycleambulanceatKIHEFOforafewdays.DuringthefewdaysthePulsesystemwasinKabale,wewereabletoconductinterviewswithmotorcycledriversandpotentialusersandobservethesystemperformanceintheKabaleterrain.Weproposedthataspartoftheirtripwewouldprovide(1)abusinessmodelfordeployingtheproductinSouthernUganda,includingastudyoncurrentcommunitypaymentsystems,(2)identificationofpotentialproductchangestofitthelocalneedsofthepeopleintheKigeziregion,(3)suggestionsonorganizationsforfuturepartnerships,and(4)awarenessofthePulsecompanyandproductincommunitiesacrossSouthernUganda.
Task3:ImprovingMotorcycleAmbulancesforApplicationinKigezi,UgandaAspartofthistask,plannedaprototypingprocesstobetterunderstandhowpotentialusersenjoyedandsoughttomodifythemotorcycleambulanceservice.Thisprocessinvolvedidentifyingdesignrequirementsandconstrains,understandingavailabilityoflocalmaterialsandprocesses,designingandconstructingaprototype,andgettingandevaluatingfeedback.BecauseofthecharacteristicsoftheKigeziregion,itwasimportantthatweintroducethemotorcycleambulanceservicetoprospectivecustomersandaskfortheirinput.
22
DesignRequirementsandConstraintsDefiningthedesignrequirementsandconstraintswereimportantforustosystematicallyevaluateimprovementstoexistingmotorcycleambulances.Thisalsoallowedustoformalizecriteriaforemergencytransportsystemsbaseduponourneedfindingresultsandpriorresearch.
Therequirementsareasfollows:
- Easilycleanable/hygienic- Vibrationsminimized- Horizontalmovements/effectsfromturns,brakes,andaccelerationminimized- Protectionfromenvironmentalelements(e.g.weather,motorcycleexhaust)- Balanced- Patientprivacy- Thereisspacefordriver,patient,andadditionalpassenger(s)- Lightweightdesign(topromotefuelefficiency)- Capitalcostisaffordable- Durablematerialsanddesign- Comfortableinteriordesign(bed,additionalmaterials)- Nosharpedges,points,orhazardouscomponents- Safeconnectionmechanisms
Theconstraintsareasfollows:
- Powerofmotorcycleengine- Dimensionsofmotorcycles/roads- Cost- Availabilityofmanufacturing,repairs,andparts- Driverskill- Teamskillsandknowledge
LocallyAvailableMaterialsandProductionOnemainconsiderationforanymotorcycleambulancedesignisfortheproduct'smaterialstobelocallyavailableandpartslocallyrepairable.Additionally,productionandmaintenanceshouldbecompatiblewithlocalmanufacturingprocesses.Inordertoensurethis,weconductedanassessmentoflocallyavailablematerialsandproductionmethodsinKabale,Ugandaandinterviewedlocalengineersandmechanics.
23
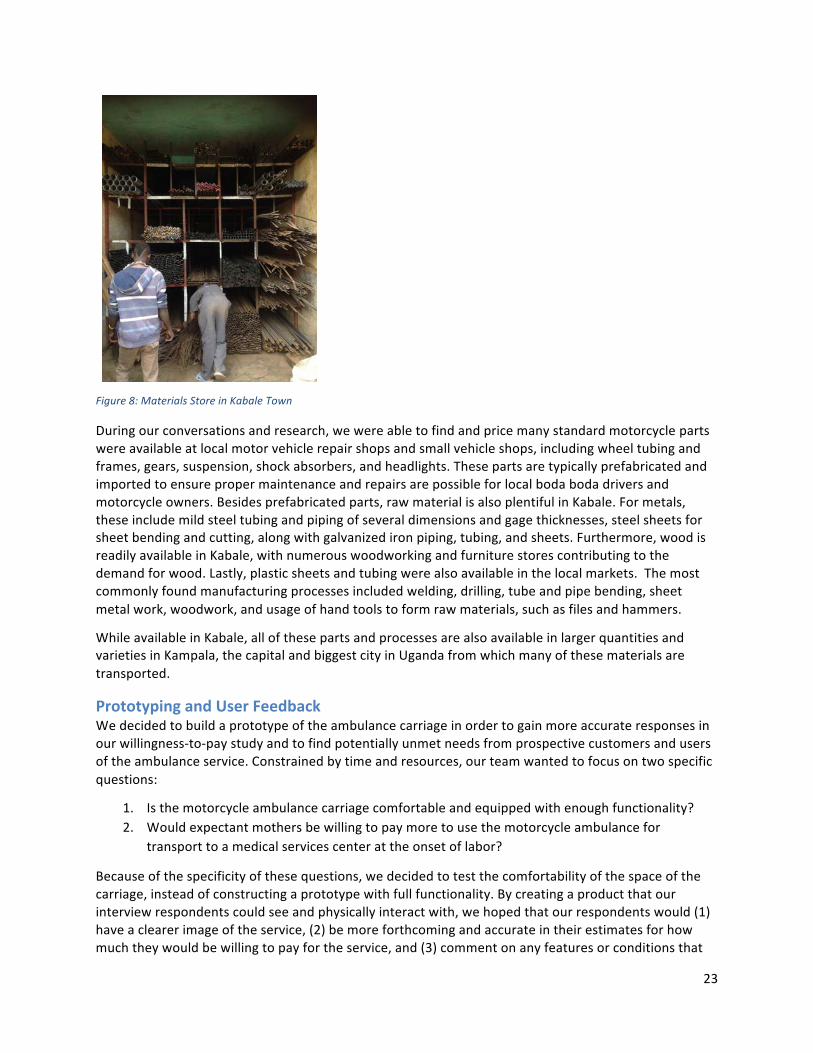
Figure8:MaterialsStoreinKabaleTown
Duringourconversationsandresearch,wewereabletofindandpricemanystandardmotorcyclepartswereavailableatlocalmotorvehiclerepairshopsandsmallvehicleshops,includingwheeltubingandframes,gears,suspension,shockabsorbers,andheadlights.Thesepartsaretypicallyprefabricatedandimportedtoensurepropermaintenanceandrepairsarepossibleforlocalbodabodadriversandmotorcycleowners.Besidesprefabricatedparts,rawmaterialisalsoplentifulinKabale.Formetals,theseincludemildsteeltubingandpipingofseveraldimensionsandgagethicknesses,steelsheetsforsheetbendingandcutting,alongwithgalvanizedironpiping,tubing,andsheets.Furthermore,woodisreadilyavailableinKabale,withnumerouswoodworkingandfurniturestorescontributingtothedemandforwood.Lastly,plasticsheetsandtubingwerealsoavailableinthelocalmarkets.Themostcommonlyfoundmanufacturingprocessesincludedwelding,drilling,tubeandpipebending,sheetmetalwork,woodwork,andusageofhandtoolstoformrawmaterials,suchasfilesandhammers.
WhileavailableinKabale,allofthesepartsandprocessesarealsoavailableinlargerquantitiesandvarietiesinKampala,thecapitalandbiggestcityinUgandafromwhichmanyofthesematerialsaretransported.
PrototypingandUserFeedbackWedecidedtobuildaprototypeoftheambulancecarriageinordertogainmoreaccurateresponsesinourwillingness-to-paystudyandtofindpotentiallyunmetneedsfromprospectivecustomersandusersoftheambulanceservice.Constrainedbytimeandresources,ourteamwantedtofocusontwospecificquestions:
1. Isthemotorcycleambulancecarriagecomfortableandequippedwithenoughfunctionality?2. Wouldexpectantmothersbewillingtopaymoretousethemotorcycleambulancefor
transporttoamedicalservicescenterattheonsetoflabor?
Becauseofthespecificityofthesequestions,wedecidedtotestthecomfortabilityofthespaceofthecarriage,insteadofconstructingaprototypewithfullfunctionality.Bycreatingaproductthatourinterviewrespondentscouldseeandphysicallyinteractwith,wehopedthatourrespondentswould(1)haveaclearerimageoftheservice,(2)bemoreforthcomingandaccurateintheirestimatesforhowmuchtheywouldbewillingtopayfortheservice,and(3)commentonanyfeaturesorconditionsthat
24
wereneededintermsofcomfortandoperations.Severaloftheprincipleswefollowedduringtheprototypingprocessincludeadaptability,localresources,flexibility,costeffective,andtemporal.Foraportionofthepotentialcustomerinterviews,wewereabletoprocureaPulsemotorcycleambulanceandreplacetheprototypewiththeactualmotorcycleambulance.
DesignOneofthepurposesoftheprototypewastotestthecomfortabilityandspaceoftheambulanceattachment.Therefore,ourteamdecidedtofocusoncreatingasetofproductsthatwouldapproximateanambulancecarriagethatiscurrentlyonthemarkettotestthesize,comfort,andeaseofentry.Totestthesefactors,wedecidedthattheprototypewouldconsistofthreemainparts–thebed,thecanopy,andaframetomodelasthe“reclining”featureofthemattress.
Anevaluationoflocalmaterialswasconductedtodeterminewhichmaterialswerewidelyavailableandcouldbeusedforourprototype.Basedontheavailabilityandcostsoflocallyavailablematerials,theteamdecidedtousewoodandPRRpipeforthebulkoftheprototype.Afoammattresswasobtainedfortheprototype.
Tocreatethecanopyandframeforthebed,22PRRtubeswerecuttovaryinglengths.Tentubeswereusedtocreatethebottomrectangularframe.Eighttubes(fouroneachlongsideoftherectangularframe)wereplacedverticallyonthelongersides.Thesepolesgraduallyincreasedinheight,creatingtheslopingcurveofthecanopy.Thelastfourtubeswereplacedonthetopofthestructure,heldupbytheeightverticalpieces,inordertoholdthestructuretogether.Finally,atarpwassecuredoverthestructureandgluedtothebottomframe,completingthecanopyimitation.
Therecliningfeature,ontheotherhand,wasdesignedsimplytoshowcasetherecliningfunctionofthesystem.Assuch,wedecidedoncreatingasimplewoodenrighttrianglefromasinglepieceof1inx4inx10ftwood,wherethemattresswouldrestonthehypotenuseoftheframe.
Theteamconsideredandrejectedanumberofideasforelevatingtheprototypeandmimickingtheheightoftheambulancecarriage.Forinstance,theteamdiscussedplacingtheprototypeontopofdiningroomtables,butthiswasrejectedastheyweredeemedtoohighformotherstoenterwithoutexcessstrain.Itwasalsosuggestedthatsidetables(approximately3ftby1ft)beused.However,theywereverysmall,somultipletableswouldhavetobeused,whichwouldbecumbersometotransport.Finally,theteamdiscussedcreatingasimplewoodenframe.Becauseofthelimitedtimeandresourcesdelegatedforprototypeconstruction,theelevationoftheprototypewascreatedbylayeringtwomedicalpurposemattresses.
ConstructionThefinalprototypeconsistedoffourparts(canopy,mattress,recliningstructure,andframe)andtooktwodaystoconstruct.Theconstructionprocessforeachpartisoutlinedbelow.
Canopy:Thefinalcanopydimensionswereapproximately1mx2mx1m.Thecanopywasconstructedusing0.5inchdiameterPRRpipes,T-joints,elbowjoints,PVCcement,ducttape,andasinglepieceof1x4metertarp.ThebottomrectangularframewasconstructedusingtenpiecesofPRRtubing,withtheeightsmallerpiecesusedtoconstructthelongersides.Thesideswereconnectedbyelbowjoints,whilethesidepieceswereconnectedwithT-joints.Initially,weattemptedtouseacombinationofPVCcementandducttapeinordertocreatestrongerandmorestablejoints–however,itwasfoundthatthecementdriedtooslowlyandwasnotsuitableforensuringstability.Therefore,ducttapewasusedexclusivelyontheremainingjoints.InordertomaximizethePRRwehadremaining,wedecidedtoconstructonlythreeheightsfortheverticalpiecesforatotalofsixPRRpiecestotal.Thetallestwas

25
attachedtheoneendoftheframe,thesecondtallestatthefirstT-jointfromthetallestend,andthesmallestpieceswereattachedatthethirdT-jointofthebottomframe.Wehadalsoplannedtosupergluethetarpontotheframe,butitwaslaterdecidedtheprototypewouldbeeasiertotransportifthetarpweredetachable.Therefore,thetarpwasattachedtotheframeusingtape.Wealsoaddedoneadditionalwoodenblockbehindthetallestsupportsinthecanopyframetoensurethetarpstayedtautthroughoutthetestingperiod.Finally,thesidesofthecanopystructurewereleftuncoveredbytarp,sothatinterviewparticipantscouldeasilygetinandoutofthestructure.
Mattress:AsimplefoammattresswasboughtintheKabalemarketplace.Theplasticwrapping(thatismeanttoprotectthefabricfromgettingdirty)waskeptonthemattresstoensureeaseofcleaning.Additionally,aclothcoveringwasaddedduringthetestingprocesstoensurecleanlinessofthesystem.
Recliningstructure:Therecliningstructurewasconstructedfrom6piecesofwood(1inchthickby1footwidth),threedifferentnailtypes,andafewpiecesofmetalsheetusedtobindwoodpiecestogether.Theangleatwhichtherecliningblockwasbuiltwasdeterminedbyassessingthecomfortabilityofthemattressinclinationatdifferentangles.Oncetheanglewasdetermined,thewoodenpieceswerefittotheangle.Thewoodenpieceswerenailedtogetherinatleasttwoplaces,withsomepiecesboundtogetherusingnailsandstripsofmetalsheet.Woodgluewasusedinitially,but,duetothedampnessofthewood,thiswasdeemedineffective.
Figure9:ConstructionoftheRecliningStructure
Frame:Uponarrivalatthematernityclinicontheveryfirstdayoftesting,werealizedthatthewardhadanumberofthickunusedmedicalmattresseswecouldusetocreateapseudo-frameinordertotesttheheightofthesystem.Westackedtwomattressesofapproximately20cmwidthandplacedtheentireprototypesystemontopofthetwomattresses.
ProspectiveCustomerFeedbackTheprototype,andlaterthePulsesystem,wasanintegralpartoftheinterviewingprocess.Participantswereinvitedtolookatandsitintheprototypeaspartofthewillingness-to-payinterview.Eachparticipantwasaskedanumberofquestionsregardingtheirthoughtsoftheprototype,thecomfortablenessofthespace,andanyfeaturestheywouldliketoseeaddedtothesystem.Fourseparatestakeholdergroups(mothers,bodadrivers,midwives,andcommunityleaders)were
26
interviewedaspartoftheprototypingtestingprocess.Eachstakeholdergroupapproachedthesystemwiththeirownbiasesandperceptions,andsubsequentlywasabletoprovideuniquefeedback.Thus,thefeedbackisgroupedaccordingtostakeholderclassification.Communityleadersarenotincludedinthisfeedbacksectionasthecommentstheygavewererelatedmoretocommunitypaymentsystems;assuch,theircommentsareincludedinalatersectionundertheresultsofthewillingness-to-paystudy.
Figure10:UsingthePrototypeduringInterviews
Figure11:UsingthePulsesystemduringInterviews
MothersMostmotherswerepleasedwiththesystem,findingthespacetobeverycomfortable.Despitethegeneralapprovaloftheprototype,themothersnotedseveralpotentialchangestothesystem:
• Roomforluggage:mostmothersbringitems,suchasbedsheets,extraclothes,abasin,andfood,withthemwhentheydeliver
27
• Extraguardrailsorgripbarsthattheycouldholdontoincasetheridewasbumpyortheywereinpain
• Anextrastepsothatshecouldgetintotheprototypemoreeasily.
Figure12:HouseholdInterviewswithMothers
Figure13:FieldInterviewswithMothers
BodabodadriversThelocalbodabodadriversweregenerallyveryreceptivetotheideaofthemotorcycleambulance.Thefeedbackwereceivedfromthisstakeholdergroupfellintotwomajorcategories:concernsorsuggestionsregardingeffectsoftheambulanceattachmentonthenavigationalefficiencyofthemotorcycle,andcommentsregardingpastemergencytransporttripstheyhadgiven.Duringthemajorityoftheinterviewswithbodabodadrivers,thePulsesystemwasavailable.Thisprovidedanaccuraterepresentationofthemotorcycleambulancesystemtobetestedbyattachingtoamotorcycle.
28
Figure14:InterviewswithBodaDriversinKabaleTown
AmbulanceandMotorcycleEfficiency:Nearlyallbodabodadriversweinterviewedwereconcernedwiththestabilityofthesystem,andmanyofthemaskedifPulse’sone-sidedattachmenttothemotorcycleaffectedbalanceduringtransport.Themajorityofthebodabodadriversweinterviewedexpressedabeliefthatthesystemwouldbeveryhardtobalance,particularlywhenturning,travelingoninclines/declines,startingthemotorcycle,ortransportingduringtherainyseason.ThelastconcernisveryvalidwithintheKigeziregionbecauseofthelengthandintensityoftherainseason.Thedriversspokeabouttheircurrentexperiencesdrivingintherain,inwhichtheysuspectedthatthebackattachmentmaybemorelikelytoslip.Onedriverpointedoutthatifthespeedofthemotorcyclewastoohigh,thecarriagemaybepulledfromsidetosidebythewind.Manyofthemaskedifthemotorcyclewouldbepowerfulenoughtopullthesystemupmountainousterrains,especiallyiftheywerecarryinganadditionalpassengeronthemotorcyclebehindthedriveraswellasapatientinthecarriage.Afewbodabodadriverswereconcernedthattheattachmentmayobstructtheirrearviewmirrors,andsuggestedthattherearviewmirrorsshouldbeextendedtobelonger.Almostallofthebodabodadriversweinterviewedwantedtoaddlightindicatorsatthebackofthecarriagetosignalbrakingandturning.Afewdriversalsowantedabrakingsysteminthecarriageforslopedareas.Manyaskedifsparepartscouldbeeasilyaccessedincasethecarriageattachmentneededextrarepairsormaintenance.
PatientExperience:Afewbodabodadriversexpressedconcernsaboutthepatientexperienceofthemotorcycleambulance.Onebodabodariderwashappytoseethattherewasenoughspaceforthecaretakertorideonthemotorcycle–however,hewasworriedthatthecaretakerwouldbelocatedtoofarawayfromthepatient,andthatthepatientmaybeisolatedduringthejourney.Shouldthepatient’sconditionworsenalongtheway,thedriverpointedout,thedriverandthecaretakermaynotrealizeorbeabletohelpuntiltheyarriveatthehealthfacility.Hesuggestedadoptingamethodofeasilymonitoringthepatient’sconditionfromthefrontofthemotorcycle.Onedriversuggestedthatwindowsbeadded,sothatthepatientcouldseewheretheywere,aswellasalightinsidethecarriagesothatitwouldnotbetoodark.Anotherrequestthatwasbroughtupintheseinterviewswasawayofholdingthecanopyup,sothatitdidnothavetobemanuallyheldinplaceaspatientsenteredorexitedthecarriageattachment(asthecanopycomponentismovedbyliftingthebottomframeofthecanopyanddoesnotremainuprightwithoutsupport,usuallyfromaperson).Onedriverinsistedthatthefoot

29
guard,locatedatthefootofthebedinthecarriage,shouldbehigher,sothatthepatientdoesnotslipforwardinthebedwhenthemotorcycleandambulancesystemaretravelingdownaslope.Othersmallsuggestionsincludedaddingmoresupportsonthesidesforthesafetyofthepatientaswellascreatingastrongercanopysothatitcouldwithstandharderrain.
MidwivesThemidwivesweregenerallyexcitedaboutthesystem,findingthespacetobemostcomfortable).However,afewmajorconcernswereraised,bothabouttheprototypeandthePulsesystem.Forinstance,oneofthemidwivespointedoutthatitwasrecommendedthatsomemotherslayontheirsideswhilebeingtransported,andthatthesafetystrapswereonlylongenoughtowraparoundwomenwholayontheirbacks.Therewerealsosomeconcernsthattherewasnotenoughspaceforacaretakertoalsobetransportedduringareferraljourney.Amidwifemustaccompanyawomantothehospitalafterbeingreferredfromtheclinicincaseanycomplicationsarise.Forexample,inthecaseofpreeclampsi,themother’svitalsmustbecheckedevery5minutesbyamidwife.Althoughthemidwivesagreedthesewererarecases,theyarguedthatthesecasesmuststillbeaccountedfor,andthatinthecurrentPulsesystemtherewasnotenoughroomforbothamidwifeandapatientinthecarriageareashouldtheambulancebeusedforthesespecificreferraljourneys.OtheradditionalfeaturesthemidwiveswishedforincludedahookforanIVdripbagandaspacetokeep“mamakits”,bagsthatcontainallofthenecessaryitemsshouldawomanneedtodeliveralongtheway.
HavingtheprototypeandthePulsemotorcycleambulanceavailableduringprospectivecustomerinterviewsprovidedvaluableinformation.Ingeneral,intervieweeswereenthusiasticabouttheproduct,althoughnearlyallofthemexpressedotherdesiresorconcernsregardingthecarriage.Mostmotherswantedmoreroomfortheirbagsiftheyweretousethisservicewhendelivering.Manybodabodadriverswereconcernedwiththestabilityofthesystem,andexpressedawishforattachmentsonbothsidesofthemotorcycleinordertoensurebalance.ThemidwivesoftheKIHEFOmaternitywardwereveryconcernedaboutthelocationofthecaretakershouldtheambulancebeusedforreferraljourneys.
Task4:CreatingaBusinessModelforProvidingMotorcycleAmbulanceServiceinKigezi,UgandaDespitetheundeniableneedforpromoting,developing,anddistributingthesesystemsthroughoutKabale,Uganda,andthedevelopingworld,itisimportanttounderstandthemanagementandbusinessofprovidingandrunningasuccessfulandsustainablemotorcycleambulanceservice.Inmanycases,thepopulationthatismostimpactedbypoor,inadequate,orinaccessiblemedicalservicesandmaternalhealthservices,isalsothepopulationthatisunabletoaffordtransportationfees.Therefore,developingamorecosteffective,safe,andqualitymotorcycleambulanceonlyaddresseshalfoftheproblem.TheprospectiveKIHEFOmotorcycleambulanceserviceprovidesexpectantmotherssafetransportationtoahospitalorclinicsettinginatimelyfashionsoastolimitpossiblecomplicationswithchilddelivery.TheKIHEFOmotorcycleambulanceserviceismeanttoserveasaproofofconceptandamarketingtoolforcommunitiesandvillagestobuyasystemandprovidetheservicefortheircommunitymembers.
Currently,itisdifficultforindividualcommunitiesandvillagestoprovideexpensivecommunalservicesfortheircommunitymembers.Despitethisbarrier,thereareseveralkeycommunityfactorsthatKIHEFOhastappedintothatcanbeutilizedinthedistributionmodel.Firstly,communitieshaveastrongpresenceofgroups,inwhichindividualsformcommunityorganizationsforaspecificpurpose.Someofthesegroups,suchasthengozigroup,provideatransportserviceforpregnantwomenviastretcherssothattheycanbesafelytransportedfromtheirhousestoaroad.Secondly,KIHEFO’s
30
relationshipswiththesecommunitiescanprovideabasisforhelpingtofundthecapitalexpensesfortheambulanceservice.Thirdly,KIHEFOhasareferralsystemwherewomenwhoareadmittedtothematernalclinicfordeliveryhavefreereferralservicestoalocalhospitaliftherearecomplicationswiththedelivery.WhiletheKIHEFOambulanceisabletoprovideservicebetweentheKIHEFOclinicsandthehospital,thereiscurrentlylimitedinfrastructuretoallowtheambulancetotravelbackandforthbetweencommunities/villages,theclinic,andthehospital.Thereareseveralreasonsforthis,asarticulatedintheNeedsIdentificationsection.
CustomerAcquisitionandRelationsThroughobservationsandextensiveinterviewswithmidwives,traditionalbirthattendants,andmothers,wehavefoundthereisaneedforreachingcustomersthroughavarietyofways.Currently,thereareseveralwaysthatKIHEFOreachespotentialcustomers:outreaches,in-patientservices,andrelationshipswithcommunitygroups(suchasreligiousgroups)andotherhealthserviceworkerssuchastraditionalhealersandtraditionalbirthattendants.Althoughexpectantmothersarethefirstcustomersegmentthatthisserviceismeanttoprovidefor,thereisgreatpotentialforusingthemotorcycleambulanceservicefortransportinginjuredandillindividuals.KIHEFOhasbuiltrelationshipswithatleast10communitiesthroughouttheKigeziregionandhascontinuedtofostertheserelationshipsthroughcontinuedcommunication.
KIHEFOhasestablishedanetworkofcommunitiesandvillagesinwhichtheycurrentlywork.AlongwithUSAID,KIHEFOwillberollingoutanewinsurancepolicyinthefallof2016inwhichthemotorcycleambulancewillbecomeapartoftheirincludedservices.KIHEFOwillbepartneringwith10communitieswithintheKigeziregiontoprovidehealthcareresources.Basicinsurance(UGX30,000perpersonperyear)willincludeoutpatientservicessuchasaccesstoweeklyoutreachesthatprovideHIV/AIDS,maternalhealth,generalhealthresourcesforindividuals,andregularvisitstotheclinicinKabaletownwhereindividualsarenotadmittedforovernightstays.Fullaccessinsurance(UGX50,000perpersonperyear)willincludebothoutpatientandinpatientservicesaswellastransportationexpensesforemergencysituationsandwomenindelivery.Aspartoftheinsuranceprogram,everyindividualinthehouseholdwouldberequiredtosubscribetotheinsurance.Therefore,afamilyof8wouldberequiredtopayUGX400,000inayearforfullaccessinsurance.BecauseKIHEFOcaterstolowincomeandpoorfamilieswithintheKigeziregion,theyunderstandthefinanciallimitationsoffamiliesinthearea.Assuch,KIHEFOprovidesanarrayofprogramsthataddresscommunitydevelopmentandfinancialdevelopment.Oneprogramthatisseenasawayforfamiliestoincreasetheirhouseholdincomesisthroughrabbitbreedinganddistribution.AscomparedtootherlivestockintheKigeziregion,rabbitsdonotrequirespecificfeedandreproduceatahigherrate.Itisestimatedthatapercentageofthetotalmonthlyinsurancerevenuewillbedirectedtowardsthemotorcycleambulanceservice.
ServiceComponentsToprovideamotorcycleambulanceservice,itisimportantthattherearekeyindividualsandinfrastructureinplace.Thedifferentpartsoftheserviceincludetheambulanceattachment,motorcycle,driver,andcallcenter.
1. Ambulanceattachment:Recently,KIHEFOhasestablishedarelationshipwithPulse,aKampala,Ugandabasedcompanythatmanufacturesanddistributesmotorcycleambulanceproducts.Pulsealsoprovidesmaintenancefortheirproductsandtrainingfordrivers.
2. Motorcycle:Themotorcycleisequallyasimportantastheambulanceattachment.MotorcycledetailshavepreviouslybeenaddressedinTask2.
3. Driver:Thedriverisacriticalpartoftheservice,astheyareresponsibleforsettingtheserviceprice,maintainingthemotorcycleandambulanceattachment,andprovidingsafeandefficient
31
transportforcustomers.Thislastpointbecomescrucialbecauseoftheadditionalskillittakestodriveamotorcyclewitha200kg(ormore)attachment.GiventhehillylandscapeandunpavedcommunityroadsinKabale,Uganda,thedrivermustbefamiliarwiththeterrainandbeabletoadjustquicklytoensurethatthecustomerhasasafejourney.Althoughmotorcycleambulanceattachmentsonthemarkethavebeentestedforalmostallconditionsandthesafetyratingsareusuallylistedatbelowthefailurelimitationsofthemotorcycleandambulanceattachments,thereisnosubstituteforagooddriverwhorespectsandmaintainshis/hermotorcycleandambulanceattachment.
4. Communicationnetwork:Therewillneedtobeanindividualwhoisabletoacceptcallsfromprospectivecustomers,detailtheircondition,anddispatchthedriverinatimelymanner.Incasesinwhichtheserviceissmall,itispossibleforthedrivertoactasthecallcenter,receivingcallsfrompatientsanddrivingtopickthemup.Incasesinwhichtheserviceislargeandexpandstomanydifferentcommunities,thereisagreaterneedtohaveacallcenterthatreceivescallsfrompatientsanddirectsthedriverwheretogoandwhentopickupthepatients.MobilephonesarecommonplaceinUganda,regardlessofsocioeconomicstatus.Therefore,itispossibleforthecallcentertobeamaincomponentofmanagingtheservice.Additionally,theavailabilityofmobilephonesamongstcustomersisanadvantagefortheservice.Inadditiontofacilitatingcommunicationsbetweenpatientsandthedriver(andthecallcenter),themobilephonescanbeusedtosendmobilemoneytothedriver(andthecallcenter).MobilemoneyiscommonplaceinUgandaandprovidesaneasywaytotransferfundstoandfromindividualsandaidwithaccountingpurposes,asthereisareceiptuponfinalizingeachtransaction.
FinancialModelInadditiontounderstandingthemotorcycleambulanceservicecomponents,thecustomeranalysisandpricingmodelsmustmakethisserviceaccessibleforthosewhoneeditmost.Aspartofourresearch,wesetouttounderstandthedemand,currentuse,andpricingofemergencytransportsystems.Thefollowingsectiondetailsseveraldifferentbusinessmodelsthatcanbeimplementedtoensurethatamotorcycleambulanceserviceissustainable.Asustainablebusinessmodelischaracterizedbyafinancialmodelinwhichtherevenuestreamisabletomeetorexceedsystemcosts.Thethreebasicmodelsbelowprovideafoundationforunderstandinghowtoestablishandmanageamotorcycleambulancesystem.Eachmodelisuniqueandwillbesuccessfulindifferentsituations.
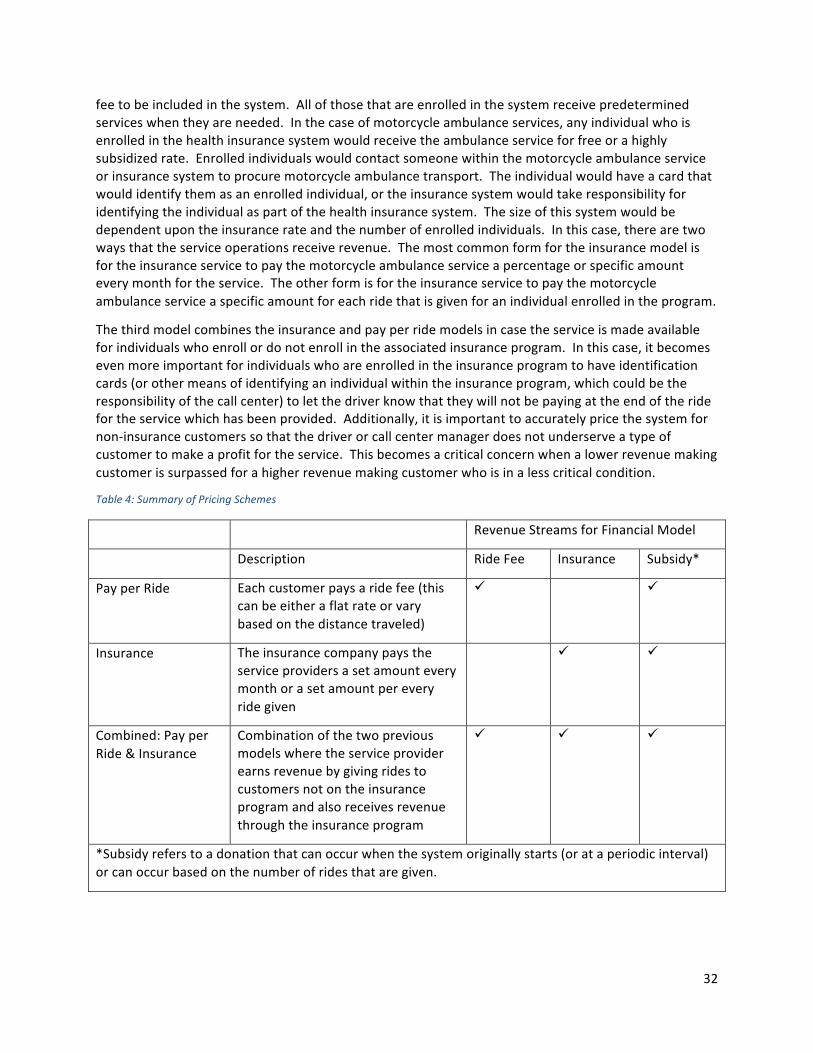
Thefirstmodelisapayperridemodel,inwhichacustomerpaysfortheserviceofthemotorcycleambulancewhentheyneedtousetheservice.ThisisverysimilartothetypeofservicethatiscurrentlyofferedbymotorcycletaxisinUganda.Whenanindividualrequeststransporttoacertainlocation,theyfindamotorcycletaxi,negotiateapricepriortoembarking,thedriverprovidestheservice,andthecustomerpaysthenegotiatedprice.Thepricefortheservice,basedonourconversationswithmotorcycletaxidrivers,variesdependinguponthetimeofday,distance,andincomeofthecustomer.Inthecaseofthemotorcycleambulance,thesameprocesswouldoccur.Theremaybeslightvariationsforthecustomer.Forexample,thecustomerwillhaveaccesstothedriver’sphonenumber(thismayinlaterstagesbecomeacallcenterthathandlesanetworkofmotorcycleambulances)andcallsthemotorcycleambulancewhentransportisneeded.Similartotraditionalmotorcycletaxiservice,themotorcycleambulance(attachment)mayberentedorownedbythedriver.Toaccountforthecapitalcostoftheattachment,theadditionalgasandmaintenanceexpenditures,themotorcycleambulancedrivermayincreasethepriceofthetransportservice.
Thesecondmodelisaninsurancemodelthattakesadvantageofcommunitygroupsavingsandcommunityhealthschemes.Theseprogramsoperatesimilarlytoahealthinsurancesysteminwhichmanyhouseholds,families,orindividualsenrollintheinsuranceprogramandpayamonthlyorannual
32
feetobeincludedinthesystem.Allofthosethatareenrolledinthesystemreceivepredeterminedserviceswhentheyareneeded.Inthecaseofmotorcycleambulanceservices,anyindividualwhoisenrolledinthehealthinsurancesystemwouldreceivetheambulanceserviceforfreeorahighlysubsidizedrate.Enrolledindividualswouldcontactsomeonewithinthemotorcycleambulanceserviceorinsurancesystemtoprocuremotorcycleambulancetransport.Theindividualwouldhaveacardthatwouldidentifythemasanenrolledindividual,ortheinsurancesystemwouldtakeresponsibilityforidentifyingtheindividualaspartofthehealthinsurancesystem.Thesizeofthissystemwouldbedependentupontheinsurancerateandthenumberofenrolledindividuals.Inthiscase,therearetwowaysthattheserviceoperationsreceiverevenue.Themostcommonformfortheinsurancemodelisfortheinsuranceservicetopaythemotorcycleambulanceserviceapercentageorspecificamounteverymonthfortheservice.Theotherformisfortheinsuranceservicetopaythemotorcycleambulanceserviceaspecificamountforeachridethatisgivenforanindividualenrolledintheprogram.
Thethirdmodelcombinestheinsuranceandpayperridemodelsincasetheserviceismadeavailableforindividualswhoenrollordonotenrollintheassociatedinsuranceprogram.Inthiscase,itbecomesevenmoreimportantforindividualswhoareenrolledintheinsuranceprogramtohaveidentificationcards(orothermeansofidentifyinganindividualwithintheinsuranceprogram,whichcouldbetheresponsibilityofthecallcenter)toletthedriverknowthattheywillnotbepayingattheendoftheridefortheservicewhichhasbeenprovided.Additionally,itisimportanttoaccuratelypricethesystemfornon-insurancecustomerssothatthedriverorcallcentermanagerdoesnotunderserveatypeofcustomertomakeaprofitfortheservice.Thisbecomesacriticalconcernwhenalowerrevenuemakingcustomerissurpassedforahigherrevenuemakingcustomerwhoisinalesscriticalcondition.
Table4:SummaryofPricingSchemes
RevenueStreamsforFinancialModel
Description RideFee Insurance Subsidy*
PayperRide Eachcustomerpaysaridefee(thiscanbeeitheraflatrateorvarybasedonthedistancetraveled)
ü ü
Insurance Theinsurancecompanypaystheserviceprovidersasetamounteverymonthorasetamountpereveryridegiven
ü ü
Combined:PayperRide&Insurance
Combinationofthetwopreviousmodelswheretheserviceproviderearnsrevenuebygivingridestocustomersnotontheinsuranceprogramandalsoreceivesrevenuethroughtheinsuranceprogram
ü ü ü
*Subsidyreferstoadonationthatcanoccurwhenthesystemoriginallystarts(orataperiodicinterval)orcanoccurbasedonthenumberofridesthataregiven.
33
WillingnesstoPayStudyInordertoestablishasustainablemodelforintegratingthemotorcycleambulancecarriageintocommunitiesfordeliverytransituse,itisessentialthatwegaugehowmuchcommunitiesareableandwillingtopayfortheseservices.Onewayinwhichwecanunderstandwhatanappropriatepricefortheambulanceserviceswouldbeisawillingnesstopaystudy.
WTPsurveydataallowusto‘estimatethenumberofclientswhowillpayagivenprice,theamountofrevenuethatwillbegeneratedbythatprice,andiftheappropriatequestionsareincludedinthequestionnaire,thecharacteristicsofindividualswhowillorwillnotpaythatprice’xxiii.Inotherwords,willingnesstopay(WTP)studiescanbeusedtounderstandhowmuchacommunityorsamplesetwouldbewillingtopayforagivenservice(keepinginminddifferentsocioeconomicstandingsexist)anddeterminedemandcurves(relatingthepercentageofpeopleinterviewedtothemaximumpricetheywouldbewillingtopay),amongotherthings.Inourcase,wecananalyzeWTPresponsestopredicttheoptimumpriceatwhichmotorcycleambulancecarriagescanbeofferedwhilebeingaffordabletoindividualmothersaswellassustainabletothecommunityasawhole.Afterall,itiscriticaltokeepinmindthat,thechallengeforsocialprogramsistosetpriceslowenoughtobeaffordabletothetargetclienteleandyethighenoughtoavoidcannibalizingself-supporting,fullycommercialbrandsandservices1.Additionally,theWTPsurveywillsupplementthefinancialandbusinessmodelsfortheambulancesystems,allowingformoreinformeddecisionswhenintegratedintocommunities.
DesignofStudyOurWTPstudywasbasedoninterviewing(bothcurrentandexpecting)mothers,arguablythemostimportantstakeholdersinthemotorcycleambulanceintegrationandimplementationprocesses.Communityleadersandbodadriverswerealsointerviewedtoobtainaholisticunderstandingofthepriceandsocietaldynamicsthatarelikelytoplayoutifamotorcycleambulanceweretobeintroducedtoacommunity.Ourinterviewswithcommunityleadershelpedusunderstanddifferentmechanismsforpoolingandsharingresources,oneoftheprimarymodelsbeingconsideredfortheambulanceintegrationprocess.Additionally,interviewingbodadriversprovideduswithcriticalinformationregardingtheanticipatedrunningcostsofusingthemotorcycle-poweredambulance,ageneralideaofhowthecarriageisperceived(withregardstofunctionalityandnavigationease)amongpeoplewhodrivemotorcycleseveryday,aswellasatheaveragecostsforhiringamotorcyclewithoutthecarriage.
ThequestionsfortheWTPsurveywerecreatedandfinalizedwithseveralnotesinmind.Theyserveseveralpurposes,suchashelpingustodeterminethesocioeconomicstandingofthemothers(whichwouldguideusinunderstandingtherationalebehindthepricequotestheygaveus),andtounderstandanysocial,culturaloreconomicbarrierstoseekingsupervisedmedicalcare(‘3Delaysmodel’,asexplainedinthetransportationbarriersection).Therewerenumeroussetsofsub-questionsthatvarieddependingonwhichofthethreetargetgroupswewereaddressing(Thequestionsarepresentintheappendix).
WithregardstothecoreoftheWTPsurvey,however,weposedquestionsaccordingtothefollowingcategories
1. Introduction:Thissectionencompassedthemother’sname,ageandhomelocation2. Abilityoffemaletomakedecisions:Thesequestionshelpedusunderstandhowmuchofasay
themotherhadinhouseholdmatters.Additionally,incomeandsavingvalueswereparticularlyusefulinunderstandingthefinancialcircumstancesofthemotherandherfamily,andbyextension,hereconomicstandinginhercommunity.
3. Availabilityoftransport:Thissectionhelpedusunderstandhowubiquitousdifferentbodas(andothertransportmeans)wereinthehomecommunityofthemother,herinclinationsand
34
disinclinationstobodas,howmuchsheusuallypaysforbodarides(tojuxtaposethepriceofregularcommutestoanambulancetransits),andherpreviousexperiencewithemergencytransportoptions(onceagain,forcomparisonpurposes).
4. Communitygroups:Thequestionsinthiscategorywereaimedatgagingthemother’ssocialstanding,whethershewasinacommunitysupportsystemofsomesortandwhatkindofreinforcementsthegroupprovided(forexample,whetheremergencytransportorhealthissues’chargeswerecovered).Theywerealsodirectedtoaidourunderstandingofhowinclusive(orexclusive)communitygroupswere(somethingcrucialtoknow,giventhatthemotorcycleambulancewouldbeasharedresourceifprocuredbyacommunity,andwouldneedtobeintegratedinaninclusivesystem).
5. Birthingexperience:Thiswasoneofthemoreimportantcategoriesgiventhatitdealtdirectlywiththebirthingprocessandthemothers’personalexperiencesandencounterswithproblems(ifany)withtransportationduringthedelivery/referraltransits.Thisservedastheproblemscopingspaceandpavedwayfortheintroductionofthemotorcyclecarriage.
6. Prototypecategories:Questionsherewereconcernedwithuserfeedback(withregardstotheprototypeandtheactualmotorcyclecarriage)andsuggestedrecommendations.Thethreemostimportantquestions,however,werethepricingquestionstrio:1.Howmuchwouldyoubewillingtopayforthismodeoftransporttothehealthcentreduringyourdeliverytransit?2.WouldyoubeabletopayforthismodeoftransportifthepricewereUGX10,000more(thanthepreviouslyrecordedanswer)?3.Whatisthemaximumamountyouwouldbewillingtopayforthisambulanceservice?Thesequestionsservedasthepillarsforthedemandcurve(thetwopriorquestionsculminatedintheaskingofthethirdquestion,whichwasusedtodrawgraph1below).
MethodologyInterviewsforthewillingness-to-paystudywereconductedbetweenSeptember8,2016andSeptember15,2016.Surveyquestionswerecreatedforeachpotential“stakeholder”,namely,mothers(boththoseexpectingandthosewhohadalreadydelivered),bodadrivers,andcommunityleaders.Atotalof46formalinterviewswereconducted,35ofthemwithlocalwomen,8withlocalbodadrivers,and3withcommunityleaders.Theinterviewswereconductedintown,atKIHEFO’smaternityward,andinthreevillagesintheKabaleregion.TheseinterviewswereconductedinRukiga,thelocallanguage,withsomepartiallyconductedinEnglish–KIHEFOstaffmembersprovidedtranslationsfortheStanfordteamandinterviewparticipants.Interviewsrangedfrom30to60minuteslongandweregenerallyconductedbytwoorthreeStanfordteammembers:onemembertoaskquestions,andatleastonemembertorecordresponses.Thesamelistofquestionswasposedtoallparticipantsoftheirrespective“stakeholder”classification,thoughtheStanfordteamwouldaskclarifyingorprobingquestionsaftersomeresponsesinordertogainabetterunderstandingoftheindividual’slifeexperience.Topicscoveredintheseinterviewsincludedoccupations,monthlyincomeandsavings,communitygroups,andexperienceswithbirth.Uponthecompletionofthesequestions,theparticipantwouldbeinvitedtositintheprototype/Pulsesystem.Iftheparticipantwasclassifiedasa“mother”,shewasthenaskedaseriesofquestionsabouttheprototype(e.g.,incomparisontoothertransportationoptions,oranyadditionalfeaturestheywantedtosee),aswellassomequestionsregardingthepriceshewouldbewillingtopayforthisservice.Iftheparticipantwasabodabodadriver,theywereaskedaboutanyconcernstheymayhaveabouttowingtheprototypebehindtheirmotorcycle,aswellashowmuchtheywouldchargepatientsiftheyweretoownoneoftheseambulanceattachments.Communityleaderswereaskedtoexplainthestepsthegroupmaytakeinordertoobtainoneofthesesystems,includingtheallocationofservicesamongstmembersafterpurchasingoneofthesesystems.
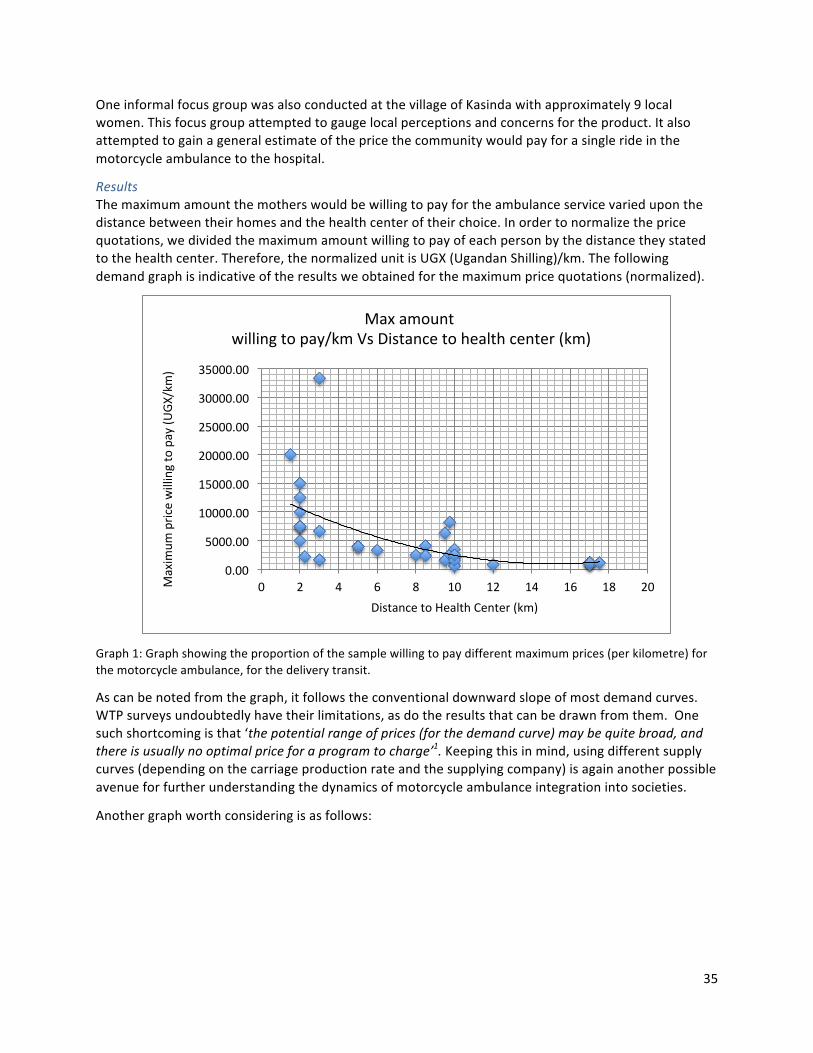
35
OneinformalfocusgroupwasalsoconductedatthevillageofKasindawithapproximately9localwomen.Thisfocusgroupattemptedtogaugelocalperceptionsandconcernsfortheproduct.Italsoattemptedtogainageneralestimateofthepricethecommunitywouldpayforasinglerideinthemotorcycleambulancetothehospital.
ResultsThemaximumamountthemotherswouldbewillingtopayfortheambulanceservicevarieduponthedistancebetweentheirhomesandthehealthcenteroftheirchoice.Inordertonormalizethepricequotations,wedividedthemaximumamountwillingtopayofeachpersonbythedistancetheystatedtothehealthcenter.Therefore,thenormalizedunitisUGX(UgandanShilling)/km.Thefollowingdemandgraphisindicativeoftheresultsweobtainedforthemaximumpricequotations(normalized).
Graph1:Graphshowingtheproportionofthesamplewillingtopaydifferentmaximumprices(perkilometre)forthemotorcycleambulance,forthedeliverytransit.
Ascanbenotedfromthegraph,itfollowstheconventionaldownwardslopeofmostdemandcurves.WTPsurveysundoubtedlyhavetheirlimitations,asdotheresultsthatcanbedrawnfromthem.Onesuchshortcomingisthat‘thepotentialrangeofprices(forthedemandcurve)maybequitebroad,andthereisusuallynooptimalpriceforaprogramtocharge’1.Keepingthisinmind,usingdifferentsupplycurves(dependingonthecarriageproductionrateandthesupplyingcompany)isagainanotherpossibleavenueforfurtherunderstandingthedynamicsofmotorcycleambulanceintegrationintosocieties.
Anothergraphworthconsideringisasfollows:
0.00
5000.00
10000.00
15000.00
20000.00
25000.00
30000.00
35000.00
0 2 4 6 8 10 12 14 16 18 20Maxim
umpricewillingtopay(U
GX/km)
DistancetoHealthCenter(km)
Maxamountwillingtopay/kmVsDistancetohealthcenter(km)
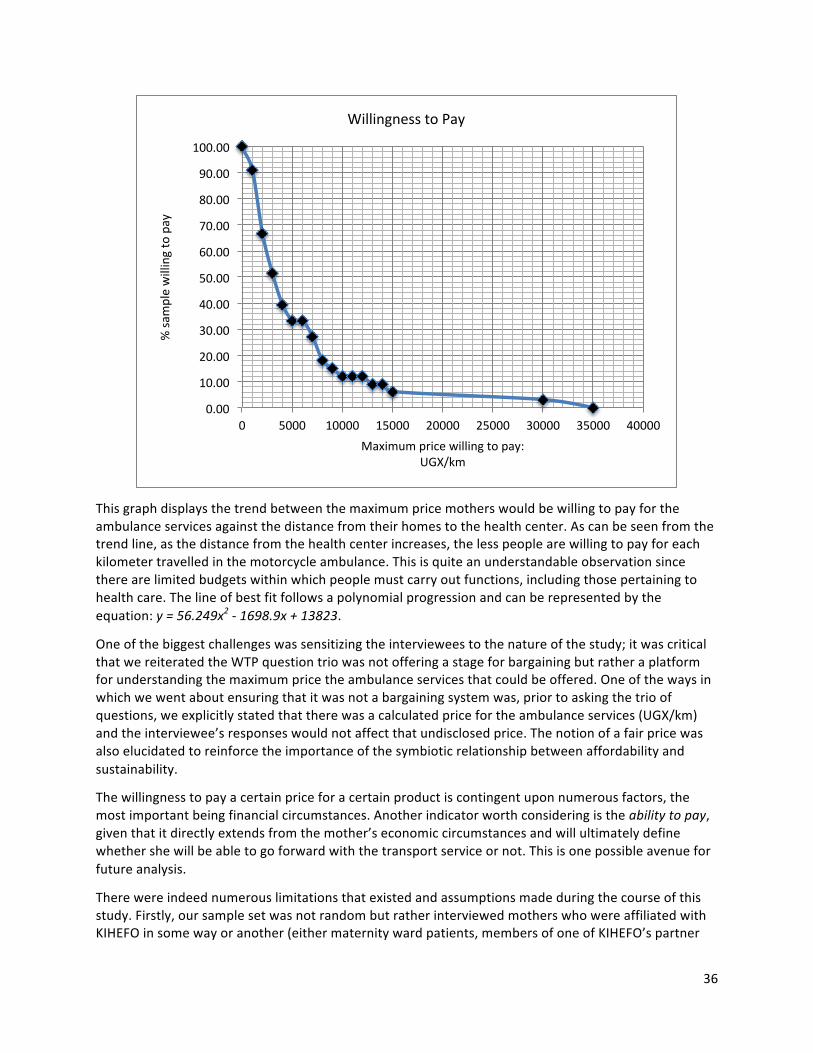
36
Thisgraphdisplaysthetrendbetweenthemaximumpricemotherswouldbewillingtopayfortheambulanceservicesagainstthedistancefromtheirhomestothehealthcenter.Ascanbeseenfromthetrendline,asthedistancefromthehealthcenterincreases,thelesspeoplearewillingtopayforeachkilometertravelledinthemotorcycleambulance.Thisisquiteanunderstandableobservationsincetherearelimitedbudgetswithinwhichpeoplemustcarryoutfunctions,includingthosepertainingtohealthcare.Thelineofbestfitfollowsapolynomialprogressionandcanberepresentedbytheequation:y=56.249x2-1698.9x+13823.
Oneofthebiggestchallengeswassensitizingtheintervieweestothenatureofthestudy;itwascriticalthatwereiteratedtheWTPquestiontriowasnotofferingastageforbargainingbutratheraplatformforunderstandingthemaximumpricetheambulanceservicesthatcouldbeoffered.Oneofthewaysinwhichwewentaboutensuringthatitwasnotabargainingsystemwas,priortoaskingthetrioofquestions,weexplicitlystatedthattherewasacalculatedpricefortheambulanceservices(UGX/km)andtheinterviewee’sresponseswouldnotaffectthatundisclosedprice.Thenotionofafairpricewasalsoelucidatedtoreinforcetheimportanceofthesymbioticrelationshipbetweenaffordabilityandsustainability.
Thewillingnesstopayacertainpriceforacertainproductiscontingentuponnumerousfactors,themostimportantbeingfinancialcircumstances.Anotherindicatorworthconsideringistheabilitytopay,giventhatitdirectlyextendsfromthemother’seconomiccircumstancesandwillultimatelydefinewhethershewillbeabletogoforwardwiththetransportserviceornot.Thisisonepossibleavenueforfutureanalysis.
Therewereindeednumerouslimitationsthatexistedandassumptionsmadeduringthecourseofthisstudy.Firstly,oursamplesetwasnotrandombutratherinterviewedmotherswhowereaffiliatedwithKIHEFOinsomewayoranother(eithermaternitywardpatients,membersofoneofKIHEFO’spartner
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
90.00
100.00
0 5000 10000 15000 20000 25000 30000 35000 40000
%sa
mplewillingtopay
Maximumpricewillingtopay:UGX/km
WillingnesstoPay

37
communitiesetc.).Additionally,theinterviewsrequiredtranslatorsandasinanytranslationprocess,itisdifficulttoensurethattheoriginalnatureofthequestionremainsthroughtranslation.Furthermore,oursamplesetwasconfinedto33mothers(35wereinterviewed,2ofwhichwerenotabletoprovideampleinformationandcouldnotbeconsideredforanalysis),particularlyduetotimelimitations.Withregardstoassumptions,ifamotherwasunabletostateherearningsasdistinctfromherhousehold’sbutcontributedequally(withrespecttoherhusband)weassumedthatherindividualearningswouldbehalfofthatofthehousehold,forthesakeofsimplicity.
Keepingtheselimitationsaside,theinterviewsprovideduswithavastunderstandingofthecurrentstateofhealthcarebasedtransportationinandaroundtheKabaleregion.Theinterviewsweconductedenabledustoconversewithmothersfromdifferentbackgroundsanddifferentwalksoflife.Learningthathealthcareisgivengreatconsiderationamongstthevastmajorityofthemothersweinterviewedwasundoubtedlyoneofthehighlights,andtheirexcitementoverthemotorcycleambulancemadeourexperienceexponentiallymorefulfilling.
ConclusionThisreportdetailsourteamprocessforhelpingKIHEFOunderstand,consider,andimplementamotorcycleambulanceserviceforaddressingmaternalhealthcareintheKigeziregion.ThisreportisaccompaniedbyafinancialmodelthatwillhelpKIHEFOcontinuemovingtowardsamotorcycleambulanceservice.
AlthoughthisreportismeanttohelporganizationslikeKIHEFO,aswellascommunities,betterunderstandemergencytransportsolutions,wehopethatthisreportwillbeeducationalforotherstudentswhoareinterestedintacklingproblemsinglobaldevelopmentandsustainability.Asyoungengineers,thishasbeenanincredibleopportunityforustolearnaboutthepotentialforinnovationstoalleviateproblemsinaninternationalenvironment,alongwiththeconsiderationsthatmustcomealongwiththem.Westronglybelievethatotherstudents-engineeringorofotherdisciplines-willbeabletolearnfromourexperiencesandbuilduponandimproveourwork.
MovingForwardAspartoftheplanstobringamotorcycleambulancetoKIHEFOandtheKabaledistrict,theStanfordSSLPteamhascreatedacrowdfundingcampaignthatwillallowKIHEFOtoraisethenecessaryfundstoobtainamotorcycleambulancethroughPulseandbegintoprovideemergencytransporttoexpectingmothers.ThisservicewillfirstbeintroducedtotheKabaledistrictthroughKIHEFObeforelocalcommunitiesandvillagesobtaintheirownmotorcycleambulanceunitstomoreefficientlyprovideemergencytransporttocommunitymembers.Thecrowdfundingcampaigngoalencompassesanamountto(1)purchaseanambulanceattachment,(2)purchaseamotorcycle(bodaboda)strictlyforthepurposeofemergencytransport,(3)acanopythatwillprotectthemotorcycledriverfromtheelements(whichwillbeespeciallyusefulduringthewetseasons,whereraincanpreventdriversfromtakingcustomerslongdistances),(4)partofthemonthlysalaryforafulltimedriverandacallcenterthatwillreceiveemergencyphonecallsanddeploythemotorcycleambulanceasfit,and(5)trainingcostsforthemotorcycledriver.
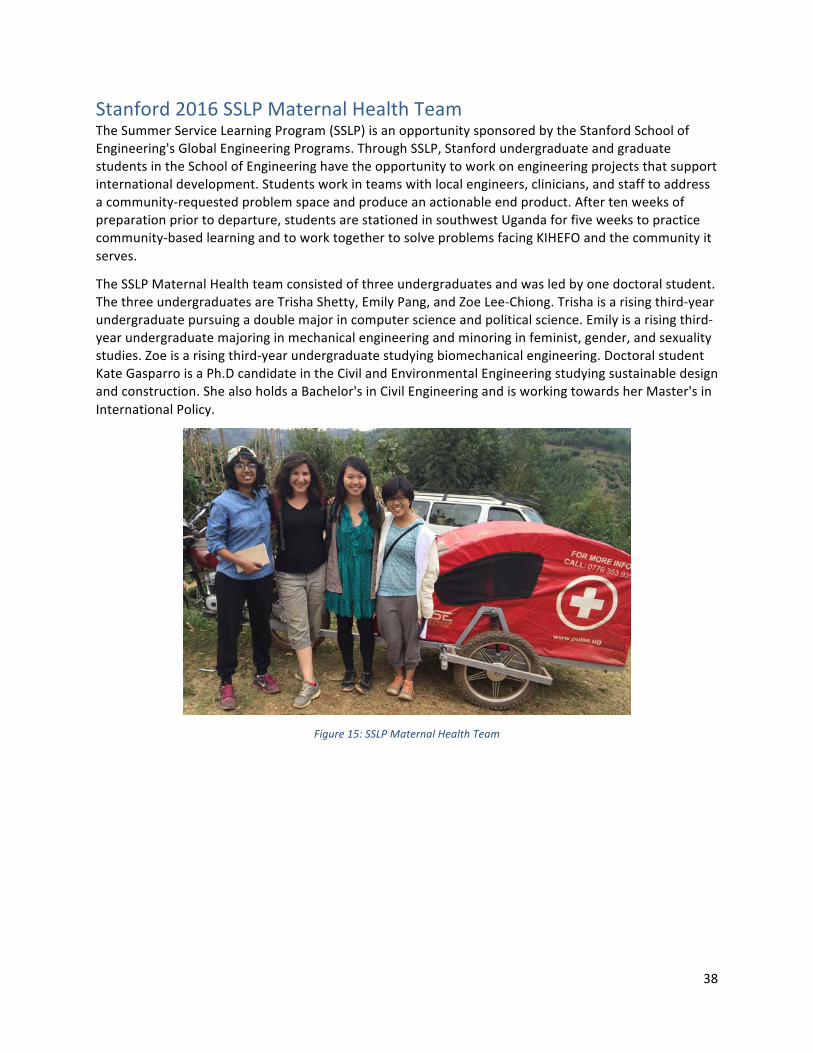
38
Stanford2016SSLPMaternalHealthTeamTheSummerServiceLearningProgram(SSLP)isanopportunitysponsoredbytheStanfordSchoolofEngineering'sGlobalEngineeringPrograms.ThroughSSLP,StanfordundergraduateandgraduatestudentsintheSchoolofEngineeringhavetheopportunitytoworkonengineeringprojectsthatsupportinternationaldevelopment.Studentsworkinteamswithlocalengineers,clinicians,andstafftoaddressacommunity-requestedproblemspaceandproduceanactionableendproduct.Aftertenweeksofpreparationpriortodeparture,studentsarestationedinsouthwestUgandaforfiveweekstopracticecommunity-basedlearningandtoworktogethertosolveproblemsfacingKIHEFOandthecommunityitserves.
TheSSLPMaternalHealthteamconsistedofthreeundergraduatesandwasledbyonedoctoralstudent.ThethreeundergraduatesareTrishaShetty,EmilyPang,andZoeLee-Chiong.Trishaisarisingthird-yearundergraduatepursuingadoublemajorincomputerscienceandpoliticalscience.Emilyisarisingthird-yearundergraduatemajoringinmechanicalengineeringandminoringinfeminist,gender,andsexualitystudies.Zoeisarisingthird-yearundergraduatestudyingbiomechanicalengineering.DoctoralstudentKateGasparroisaPh.DcandidateintheCivilandEnvironmentalEngineeringstudyingsustainabledesignandconstruction.ShealsoholdsaBachelor'sinCivilEngineeringandisworkingtowardsherMaster'sinInternationalPolicy.
Figure15:SSLPMaternalHealthTeam

39
AcknowledgementsTheprocessofcreatingthisdocumentandproceedingwithourprojectwasonlypossiblewiththehelpofmanygreatorganizationsandindividuals.
KigeziHealthcareFoundation(KIHEFO)servedasouron-the-groundsupportforthisproject.Theywereextremelyhelpfulwiththepreparationworkandtheneedsidentificationphaseofthisproject.KIHEFOprovidedroomandboardduringourfiveweekprojectandalsoprovidedaccesstotheirhealthcarefacilitiesandsupportstafftohelpwithtranslation.KIHEFOisalocalnot-for-profitNGOdedicatedtocommunitydevelopmentintheKabaleDistrictofsouthwestUganda.Itprovidesavarietyofservicessuchasmedicalcare,educationalservices,economicdevelopment,andcounseling.BesidesbeingstationedinKabale,KIHEFOalsoemphasizesitsoutreachservicesinordertoprovidecaretohard-to-reachcommunitiesinthegreaterKigeziRegion.KIHEFO’smissionistocombatpovertyandhealthissuesintheKigeziregionbyprovidingeducation,communityservices,andhealthcareforcommunities.Theirprogressiveandinnovativeperspectivewasveryhelpfulforguidingandinspiringourproject.AspecialthankyoutoDr.GeoffreyAnguyo.
ChildFamilyHealthInternational(CFHI)servedastheconnectionbetweenStanfordandKIHEFOandprovidedoff-the-groundsupportinavarietyofforms.CFHIisa501(c)3non-profitthatprovidesstudentswithservice-learningexperiencesaroundtheworld.Withmorethan30+programsintencountries,CFHI'sglobalhealtheducationprogramsfocusoncommunityengagement,asset-baseddevelopment,andcommitmenttosustainabilityandlong-termlocalempowerment.TheyprovidedpreparationmaterialsandinsuranceforuswhileweworkedinKabaleforthedurationoftheproject.AspecialthankyoutoRobinYoungwhopreparedourtripandworkedwiththeteamfromMarch2016toOctober2016.
StanfordUniversity’sGlobalEngineeringProgramwasinstrumentalinbringingtogetherthestudentgroupandprovidingtheresourcesfortheteam.StanfordUniversity'sGlobalEngineeringProgramsaimtoprovidestudentswithopportunitiestolearnfirst-handabouttheroleoftechnologyandengineeringinaninternationalandculturallydiverseenvironment.AspecialthankyoutoToriBianchiforhercontinuedsupportfortheSSLPprogramandguidancethroughoutourproject.
PulseisasocialenterprisethatmanufacturersanddistributesmotorcycleambulancesinUganda.PulsewasabletoprovideuswithfirsthandinsightsandworkedwithustobringaPulsemotorcycleambulancetoKabaletoconductinterviewsandgetfeedbackonimplementingamotorcycleambulancesystemintheKigeziDistrict.AspecialthankyoutoDarylFunkandFredKagara.
NabassaBarnabaswasresponsibleforplanningthemajorityofthefieldresearchandcoordinatingtheinterviewlogistics.Heservedasourculturalliaisonandworkedwithustodevelopaculturallyrelevantandrespectfulinterviewprocess.Additionally,Barnabasservedasthetranslatorforamajorityoftheinterviews.
HakimandJuliusspentseveraldayswithusasweinterviewedmothersandotherstakeholders.Theywereinstrumentalininterpretingtheinterviewsandmakingtheintervieweesfeelcomfortablethroughouttheinterviewprocess.
TheKIHEFOMaternityWardStaffworkedcloselywithusduringthefirststagesofourprojecttoensurethatourworkwasrelevantandnecessarytotheiroperations.Theywereapleasuretoworkwithandspentmanyhoursansweringourmedicallyrelatedquestionsasweworkedtobetterunderstandtheirprocesses.
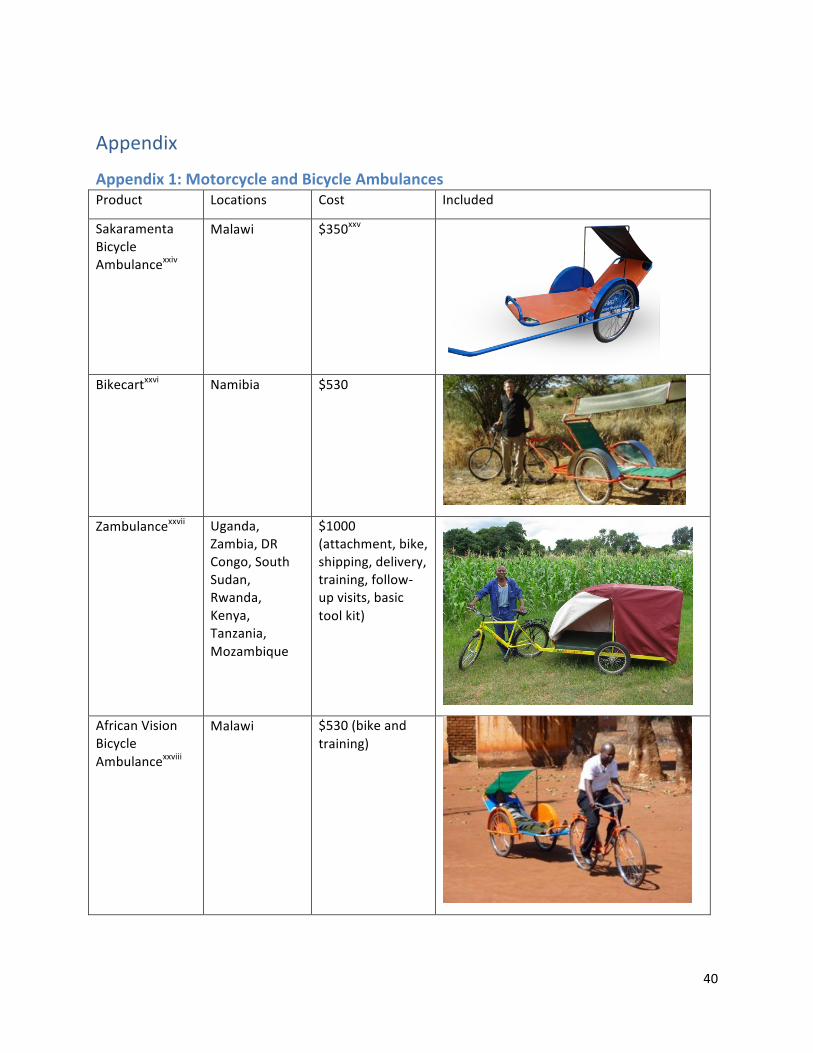
40
Appendix
Appendix1:MotorcycleandBicycleAmbulancesProduct Locations Cost Included
SakaramentaBicycleAmbulancexxiv
Malawi $350xxv
Bikecartxxvi Namibia $530
Zambulancexxvii Uganda,Zambia,DRCongo,SouthSudan,Rwanda,Kenya,Tanzania,Mozambique
$1000(attachment,bike,shipping,delivery,training,follow-upvisits,basictoolkit)
AfricanVisionBicycleAmbulancexxviii
Malawi $530(bikeandtraining)
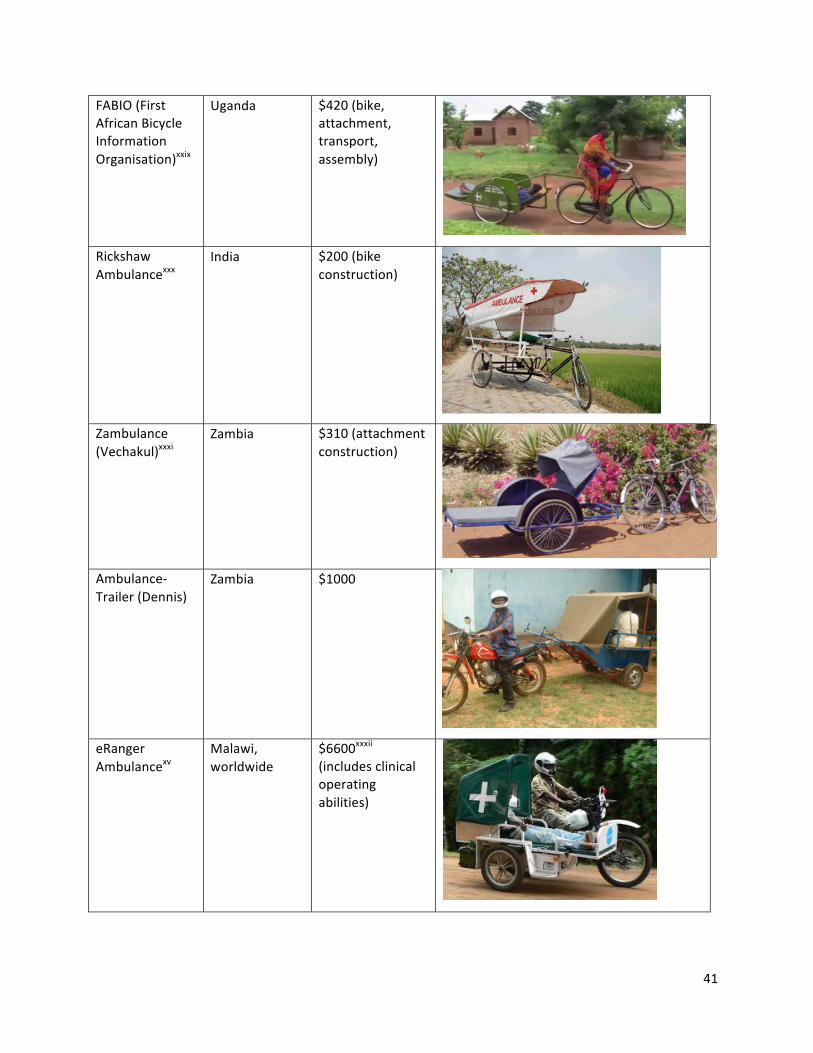
41
FABIO(FirstAfricanBicycleInformationOrganisation)xxix
Uganda $420(bike,attachment,transport,assembly)
RickshawAmbulancexxx
India $200(bikeconstruction)
Zambulance(Vechakul)xxxi
Zambia $310(attachmentconstruction)
Ambulance-Trailer(Dennis)
Zambia $1000
eRangerAmbulancexv
Malawi,worldwide
$6600xxxii(includesclinicaloperatingabilities)
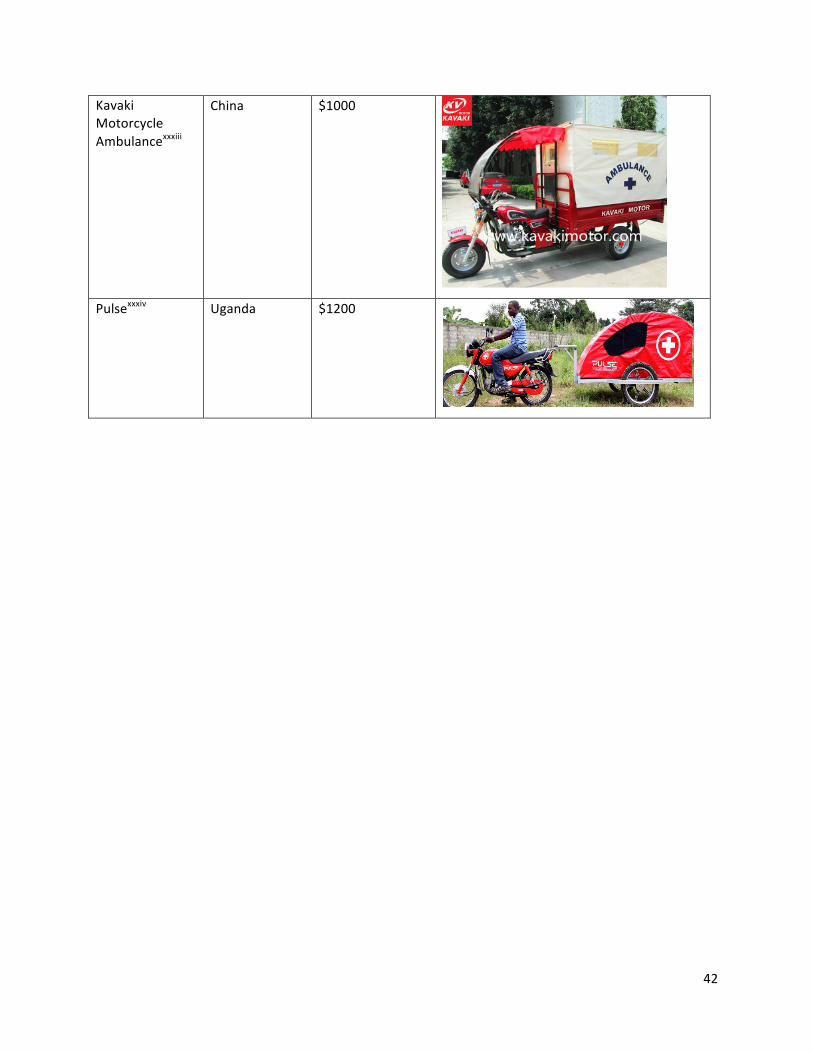
42
KavakiMotorcycleAmbulancexxxiii
China $1000
Pulsexxxiv Uganda $1200

43
Appendix2:WTPandPrototypeSurveyforServiceStakeholders
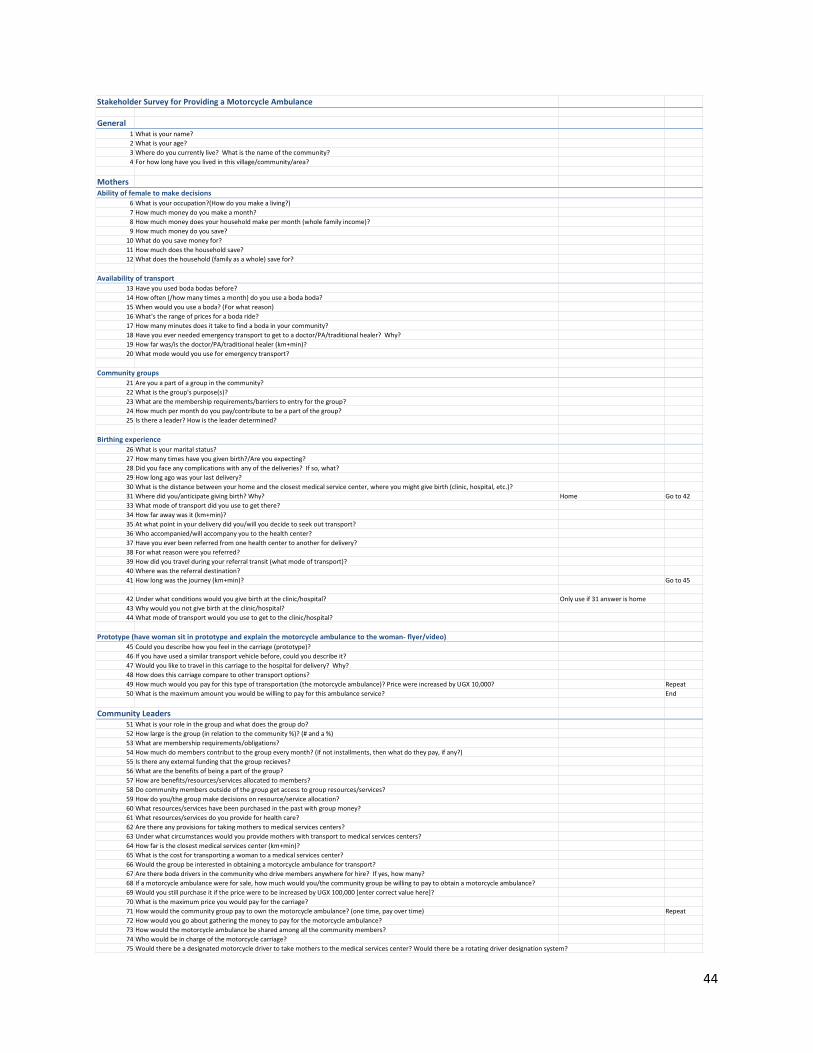
44
StakeholderSurveyforProvidingaMotorcycleAmbulance
General1 Whatisyourname?2 Whatisyourage?3 Wheredoyoucurrentlylive?Whatisthenameofthecommunity?4 Forhowlonghaveyoulivedinthisvillage/community/area?
MothersAbilityoffemaletomakedecisions
6 Whatisyouroccupation?(Howdoyoumakealiving?)7 Howmuchmoneydoyoumakeamonth?8 Howmuchmoneydoesyourhouseholdmakepermonth(wholefamilyincome)?9 Howmuchmoneydoyousave?10 Whatdoyousavemoneyfor?11 Howmuchdoesthehouseholdsave?12 Whatdoesthehousehold(familyasawhole)savefor?
Availabilityoftransport13 Haveyouusedbodabodasbefore?14 Howoften(/howmanytimesamonth)doyouuseabodaboda?15 Whenwouldyouuseaboda?(Forwhatreason)16 What'stherangeofpricesforabodaride?17 Howmanyminutesdoesittaketofindabodainyourcommunity?18 Haveyoueverneededemergencytransporttogettoadoctor/PA/traditionalhealer?Why?19 Howfarwas/isthedoctor/PA/traditionalhealer(km+min)?20 Whatmodewouldyouuseforemergencytransport?
Communitygroups21 Areyouapartofagroupinthecommunity?22 Whatisthegroup'spurpose(s)?23 Whatarethemembershiprequirements/barrierstoentryforthegroup?24 Howmuchpermonthdoyoupay/contributetobeapartofthegroup?25 Istherealeader?Howistheleaderdetermined?
Birthingexperience26 Whatisyourmaritalstatus?27 Howmanytimeshaveyougivenbirth?/Areyouexpecting?28 Didyoufaceanycomplicationswithanyofthedeliveries?Ifso,what?29 Howlongagowasyourlastdelivery?30 Whatisthedistancebetweenyourhomeandtheclosestmedicalservicecenter,whereyoumightgivebirth(clinic,hospital,etc.)?31 Wheredidyou/anticipategivingbirth?Why? Home Goto4233 Whatmodeoftransportdidyouusetogetthere?34 Howfarawaywasit(km+min)?35 Atwhatpointinyourdeliverydidyou/willyoudecidetoseekouttransport?36 Whoaccompanied/willaccompanyyoutothehealthcenter?37 Haveyoueverbeenreferredfromonehealthcentertoanotherfordelivery?38 Forwhatreasonwereyoureferred?39 Howdidyoutravelduringyourreferraltransit(whatmodeoftransport)?40 Wherewasthereferraldestination?41 Howlongwasthejourney(km+min)? Goto45
42 Underwhatconditionswouldyougivebirthattheclinic/hospital? Onlyuseif31answerishome43 Whywouldyounotgivebirthattheclinic/hospital?44 Whatmodeoftransportwouldyouusetogettotheclinic/hospital?
Prototype(havewomansitinprototypeandexplainthemotorcycleambulancetothewoman-flyer/video)45 Couldyoudescribehowyoufeelinthecarriage(prototype)?46 Ifyouhaveusedasimilartransportvehiclebefore,couldyoudescribeit?47 Wouldyouliketotravelinthiscarriagetothehospitalfordelivery?Why?48 Howdoesthiscarriagecomparetoothertransportoptions?49 Howmuchwouldyoupayforthistypeoftransportation(themotorcycleambulance)?PricewereincreasedbyUGX10,000? Repeat50 Whatisthemaximumamountyouwouldbewillingtopayforthisambulanceservice? End
CommunityLeaders51 Whatisyourroleinthegroupandwhatdoesthegroupdo?52 Howlargeisthegroup(inrelationtothecommunity%)?(#anda%)53 Whataremembershiprequirements/obligations?54 Howmuchdomemberscontributtothegroupeverymonth?(ifnotinstallments,thenwhatdotheypay,ifany?)55 Isthereanyexternalfundingthatthegrouprecieves?56 Whatarethebenefitsofbeingapartofthegroup?57 Howarebenefits/resources/servicesallocatedtomembers?58 Docommunitymembersoutsideofthegroupgetaccesstogroupresources/services?59 Howdoyou/thegroupmakedecisionsonresource/serviceallocation?60 Whatresources/serviceshavebeenpurchasedinthepastwithgroupmoney?61 Whatresources/servicesdoyouprovideforhealthcare?62 Arethereanyprovisionsfortakingmotherstomedicalservicescenters?63 Underwhatcircumstanceswouldyouprovidemotherswithtransporttomedicalservicescenters?64 Howfaristheclosestmedicalservicescenter(km+min)?65 Whatisthecostfortransportingawomantoamedicalservicescenter?66 Wouldthegroupbeinterestedinobtainingamotorcycleambulancefortransport?67 Aretherebodadriversinthecommunitywhodrivemembersanywhereforhire?Ifyes,howmany?68 Ifamotorcycleambulancewereforsale,howmuchwouldyou/thecommunitygroupbewillingtopaytoobtainamotorcycleambulance?69 WouldyoustillpurchaseitifthepriceweretobeincreasedbyUGX100,000[entercorrectvaluehere]?70 Whatisthemaximumpriceyouwouldpayforthecarriage?71 Howwouldthecommunitygrouppaytoownthemotorcycleambulance?(onetime,payovertime) Repeat72 Howwouldyougoaboutgatheringthemoneytopayforthemotorcycleambulance?73 Howwouldthemotorcycleambulancebesharedamongallthecommunitymembers?74 Whowouldbeinchargeofthemotorcyclecarriage?75 Wouldtherebeadesignatedmotorcycledrivertotakemotherstothemedicalservicescenter?Wouldtherebearotatingdriverdesignationsystem?
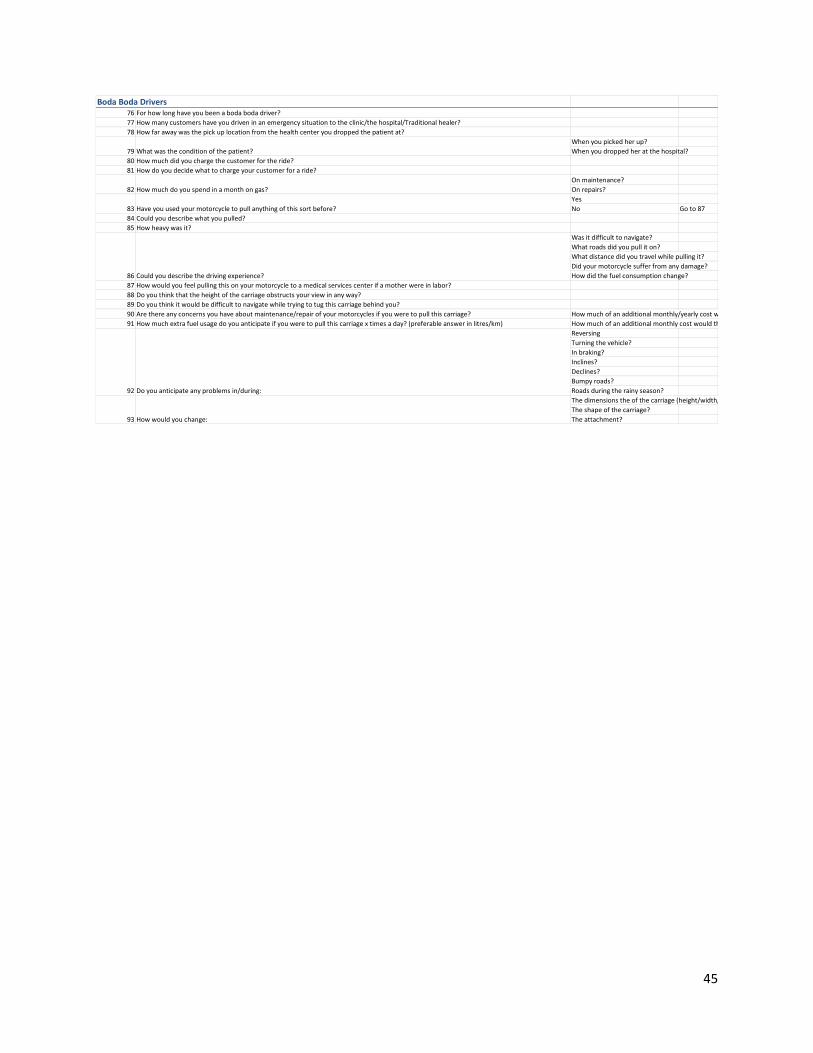
45
BodaBodaDrivers76 Forhowlonghaveyoubeenabodabodadriver?77 Howmanycustomershaveyoudriveninanemergencysituationtotheclinic/thehospital/Traditionalhealer?78 Howfarawaywasthepickuplocationfromthehealthcenteryoudroppedthepatientat?
Whenyoupickedherup?Whenyoudroppedheratthehospital?
80 Howmuchdidyouchargethecustomerfortheride?81 Howdoyoudecidewhattochargeyourcustomerforaride?
Onmaintenance?Onrepairs?YesNo Goto87
84 Couldyoudescribewhatyoupulled?85 Howheavywasit?
Wasitdifficulttonavigate?Whatroadsdidyoupulliton?Whatdistancedidyoutravelwhilepullingit?Didyourmotorcyclesufferfromanydamage?Howdidthefuelconsumptionchange?
87 Howwouldyoufeelpullingthisonyourmotorcycletoamedicalservicescenterifamotherwereinlabor?88 Doyouthinkthattheheightofthecarriageobstructsyourviewinanyway?89 Doyouthinkitwouldbedifficulttonavigatewhiletryingtotugthiscarriagebehindyou?90 Arethereanyconcernsyouhaveaboutmaintenance/repairofyourmotorcyclesifyouweretopullthiscarriage? Howmuchofanadditionalmonthly/yearlycostwouldthisbe?91 Howmuchextrafuelusagedoyouanticipateifyouweretopullthiscarriagextimesaday?(preferableanswerinlitres/km) Howmuchofanadditionalmonthlycostwouldthisbe?
ReversingTurningthevehicle?Inbraking?Inclines?Declines?Bumpyroads?Roadsduringtherainyseason?Thedimensionstheofthecarriage(height/width/length)?Theshapeofthecarriage?Theattachment?
Whatwastheconditionofthepatient?
Howmuchdoyouspendinamonthongas?
Howwouldyouchange:
79
82
83
93
Doyouanticipateanyproblemsin/during:92
Couldyoudescribethedrivingexperience?86
Haveyouusedyourmotorcycletopullanythingofthissortbefore?
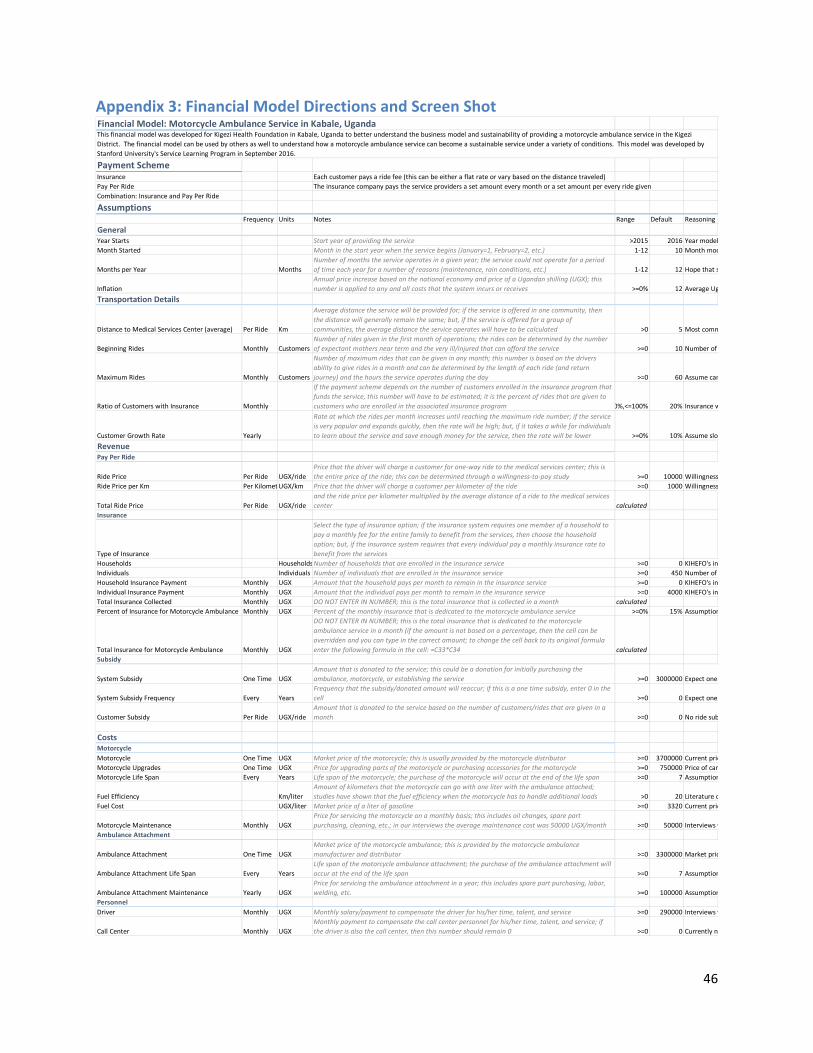
46
Appendix3:FinancialModelDirectionsandScreenShot
FinancialModel:MotorcycleAmbulanceServiceinKabale,Uganda
PaymentSchemeInsurance Eachcustomerpaysaridefee(thiscanbeeitheraflatrateorvarybasedonthedistancetraveled)PayPerRide TheinsurancecompanypaystheserviceprovidersasetamounteverymonthorasetamountpereveryridegivenCombination:InsuranceandPayPerRide
AssumptionsFrequency Units Notes Range Default Reasoning
GeneralYearStarts Startyearofprovidingtheservice >2015 2016 YearmodelwascreatedMonthStarted Monthinthestartyearwhentheservicebegins(January=1,February=2,etc.) 1-12 10 Monthmodelwascreated
MonthsperYear MonthsNumberofmonthstheserviceoperatesinagivenyear;theservicecouldnotoperateforaperiodoftimeeachyearforanumberofreasons(maintenance,rainconditions,etc.) 1-12 12 Hopethatserviceoperatesallyearlong
InflationAnnualpriceincreasebasedonthenationaleconomyandpriceofaUgandanshilling(UGX);thisnumberisappliedtoanyandallcoststhatthesystemincursorreceives >=0% 12 AverageUgandainflationbetween2005-2016
TransportationDetails
DistancetoMedicalServicesCenter(average) PerRide Km
Averagedistancetheservicewillbeprovidedfor;iftheserviceisofferedinonecommunity,thenthedistancewillgenerallyremainthesame;but,iftheserviceisofferedforagroupofcommunities,theaveragedistancetheserviceoperateswillhavetobecalculated >0 5 Mostcommondistancegivenininterviews
BeginningRides Monthly CustomersNumberofridesgiveninthefirstmonthofoperations;theridescanbedeterminedbythenumberofexpectantmothersneartermandtheveryill/injuredthatcanaffordtheservice >=0 10 NumberofcurrentreferraltripsgivenbyKIHEFOinamonth
MaximumRides Monthly Customers
Numberofmaximumridesthatcanbegiveninanymonth;thisnumberisbasedonthedriversabilitytogiveridesinamonthandcanbedeterminedbythelengthofeachride(andreturnjourney)andthehourstheserviceoperatesduringtheday >=0 60 Assumecanmake3tripsinadayfor20daysinamonth
RatioofCustomerswithInsurance Monthly
Ifthepaymentschemedependsonthenumberofcustomersenrolledintheinsuranceprogramthatfundstheservice,thisnumberwillhavetobeestimated;itisthepercentofridesthataregiventocustomerswhoareenrolledintheassociatedinsuranceprogram >=0%,<=100% 20% Insurancewillbegininthefall
CustomerGrowthRate Yearly
Rateatwhichtheridespermonthincreasesuntilreachingthemaximumridenumber;iftheserviceisverypopularandexpandsquickly,thentheratewillbehigh;but,ifittakesawhileforindividualstolearnabouttheserviceandsaveenoughmoneyfortheservice,thentheratewillbelower >=0% 10% Assumeslowcustomergrowth
RevenuePayPerRide
RidePrice PerRide UGX/ridePricethatthedriverwillchargeacustomerforone-wayridetothemedicalservicescenter;thisistheentirepriceoftheride;thiscanbedeterminedthroughawillingness-to-paystudy >=0 10000 Willingness-to-paystudyconductedforKIHEFO
RidePriceperKm PerKilometerUGX/km Pricethatthedriverwillchargeacustomerperkilometeroftheride >=0 1000 Willingness-to-paystudyconductedforKIHEFO
TotalRidePrice PerRide UGX/ride
DONOTENTERINNUMBER;thispriceisthemaximumridepricebetweentheridepriceperrideandtheridepriceperkilometermultipliedbytheaveragedistanceofaridetothemedicalservicescenter calculated
Insurance
TypeofInsurance
Selectthetypeofinsuranceoption;iftheinsurancesystemrequiresonememberofahouseholdtopayamonthlyfeefortheentirefamilytobenefitfromtheservices,thenchoosethehouseholdoption;but,iftheinsurancesystemrequiresthateveryindividualpayamonthlyinsuranceratetobenefitfromtheservices
Households HouseholdsNumberofhouseholdsthatareenrolledintheinsuranceservice >=0 0 KIHEFO'sinsurancemodelisbasedonindividualsIndividuals Individuals Numberofindividualsthatareenrolledintheinsuranceservice >=0 450 NumberofindividualsinonecommunityHouseholdInsurancePayment Monthly UGX Amountthatthehouseholdpayspermonthtoremainintheinsuranceservice >=0 0 KIHEFO'sinsurancemodelisbasedonindividualsIndividualInsurancePayment Monthly UGX Amountthattheindividualpayspermonthtoremainintheinsuranceservice >=0 4000 KIHEFO'sinsurancefeebasedon50000UGX/yearTotalInsuranceCollected Monthly UGX DONOTENTERINNUMBER;thisisthetotalinsurancethatiscollectedinamonth calculatedPercentofInsuranceforMotorcycleAmbulance Monthly UGX Percentofthemonthlyinsurancethatisdedicatedtothemotorcycleambulanceservice >=0% 15% AssumptionthatKIHEFOwoulddivert5%ofinsurancecollectedtogotoambulanceservice
TotalInsuranceforMotorcycleAmbulance Monthly UGX
DONOTENTERINNUMBER;thisisthetotalinsurancethatisdedicatedtothemotorcycleambulanceserviceinamonth(iftheamountisnotbasedonapercentage,thenthecellcanbeoverriddenandyoucantypeinthecorrectamount;tochangethecellbacktoitsoriginalformulaenterthefollowingformulainthecell:=C33*C34 calculated
Subsidy
SystemSubsidy OneTime UGXAmountthatisdonatedtotheservice;thiscouldbeadonationforinitiallypurchasingtheambulance,motorcycle,orestablishingtheservice >=0 3000000 Expectonetimedonationsforinitialsystempurchases(motorcycle,ambulanceattachment)
SystemSubsidyFrequency Every YearsFrequencythatthesubsidy/donatedamountwillreoccur;ifthisisaonetimesubsidy,enter0inthecell >=0 0 Expectonetimedonation
CustomerSubsidy PerRide UGX/rideAmountthatisdonatedtotheservicebasedonthenumberofcustomers/ridesthataregiveninamonth >=0 0 Noridesubsidyavailabe
CostsMotorcycleMotorcycle OneTime UGX Marketpriceofthemotorcycle;thisisusuallyprovidedbythemotorcycledistributor >=0 3700000 CurrentpriceofnewBajajBoxerinKabaleMotorcycleUpgrades OneTime UGX Priceforupgradingpartsofthemotorcycleorpurchasingaccessoriesforthemotorcycle >=0 750000 PriceofcanopysystemformotorcycledriverMotorcycleLifeSpan Every Years Lifespanofthemotorcycle;thepurchaseofthemotorcyclewilloccurattheendofthelifespan >=0 7 Assumptionthatmotorcyclewilllast7years
FuelEfficiency Km/literAmountofkilometersthatthemotorcyclecangowithoneliterwiththeambulanceattached;studieshaveshownthatthefuelefficiencywhenthemotorcyclehastohandleadditionalloads >0 20 Literatureoffuelefficiencyforloadedmotorcycle
FuelCost UGX/liter Marketpriceofaliterofgasoline >=0 3320 CurrentpriceofgasinKabale
MotorcycleMaintenance Monthly UGXPriceforservicingthemotorcycleonamonthlybasis;thisincludesoilchanges,sparepartpurchasing,cleaning,etc.;inourinterviewstheaveragemaintenancecostwas50000UGX/month >=0 50000 Interviewswithbodabodadriverswhogettwooilchanges/servicesduringamonth
AmbulanceAttachment
AmbulanceAttachment OneTime UGXMarketpriceofthemotorcycleambulance;thisisprovidedbythemotorcycleambulancemanufactureranddistributor >=0 3300000 Marketpriceofanambulanceattachment
AmbulanceAttachmentLifeSpan Every YearsLifespanofthemotorcycleambulanceattachment;thepurchaseoftheambulanceattachmentwilloccurattheendofthelifespan >=0 7 Assumptionthatattachmentwilllastatleast7years
AmbulanceAttachmentMaintenance Yearly UGXPriceforservicingtheambulanceattachmentinayear;thisincludessparepartpurchasing,labor,welding,etc. >=0 100000 Assumptionthatattachmentpartsreplacementandlaborforoneyear
PersonnelDriver Monthly UGX Monthlysalary/paymenttocompensatethedriverforhis/hertime,talent,andservice >=0 290000 Interviewswithbodabodadriversandneedtomake400000UGXinamonthtomaintainandbuygasformotorcycle
CallCenter Monthly UGXMonthlypaymenttocompensatethecallcenterpersonnelforhis/hertime,talent,andservice;ifthedriverisalsothecallcenter,thenthisnumbershouldremain0 >=0 0 Currentlynoneedforcallcenter
ThisfinancialmodelwasdevelopedforKigeziHealthFoundationinKabale,UgandatobetterunderstandthebusinessmodelandsustainabilityofprovidingamotorcycleambulanceserviceintheKigeziDistrict.Thefinancialmodelcanbeusedbyothersaswelltounderstandhowamotorcycleambulanceservicecanbecomeasustainableserviceunderavarietyofconditions.ThismodelwasdevelopedbyStanfordUniversity'sServiceLearningPrograminSeptember2016.