Embed Size (px)
Citation preview
Page 1 of 6
HygieneAdults
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution
Oral care is one of the most fundamental aspects of nursing care (NMC, 2015; DH, 2010). Evidence shows that there are inequalities in oral health across the UK, and attitudes towards it vary, even among healthcare professionals (Public Health England [PHE], 2017). Poor oral hygiene impacts upon the health, comfort and wellbeing of patients in hospital and in the community. Poor oral care can lead to stomatitis (inflammation of the mucous membranes of the mouth), dry mouth (xerostomia), halitosis, dental caries, dental abscesses and tooth loss. Patients with these problems may find it painful to chew, swallow or taste their food and they may be unable to swallow their medication. They may also be unable to communicate effectively, which may contribute to low self-confidence and self-esteem (Dougherty & Lister, 2015).
Advances in oral healthcare have resulted in people retaining their teeth into older age. They may have both natural teeth and dental appliances, but might not necessarily care for them (Humphreys et al., 2017). Smoking, alcohol, osteoporosis, diabetes, malnourishment and medication may contribute to poor dental and oral health (Humphreys et al., 2017; van der Putten, 2014). Inadequate mouth care can lead to local infection, and is also associated with cardiovascular risk and respiratory disease (Daly & Smith, 2015).
Other factors which may result in poor oral hygiene include impaired physical and cognitive function, such as following a cerebral vascular accident or a
stroke (Horne et al., 2014), dementia (Best & Hitchings, 2015) and learning disability (BSDOH, 2012). It is important to seek consent before carrying out mouth care (NMC, 2015; DH, 2010) and be alert to the risk of injury as a result of a bite, particularly if the patient is confused or uncooperative. Support may be required from relatives, carers or friends, with the patient’s permission. For those unable to understand the implications of refusing oral care, it may be helpful to refer to the Mental Capacity Act (2005).
Other important patient groups who need assistance with mouth care include those who are dying, as these patients commonly experience dry mouth and thirst regardless of whether they are well hydrated. Therefore, in palliative care, it is important to carry out mouth care as often as necessary to maintain a clean mouth in both conscious and unconscious patients (NICE, 2015). Other patients at risk of mouth problems include those receiving chemotherapy, steroids or other immunosuppressants and those taking antibiotics (NICE, 2018).
This procedure provides guidance on mouth care for patients who may need support to carry out effective mouth care due to their physical or cognitive impairment. The procedure described here is not appropriate for those who are unconscious or who have recently had oral surgery; in these cases, refer to local policy.
Mouth careEdited by Jackie Hunt, Senior Lecturer, Oxford Brookes University, Oxford
©2018 Clinical Skills Limited. All rights reserved
Surname..................................... NHS/Hospital No..................First Name.................................. Date of Birth.........................
Mouth Care Assessment Tool
Additional information
Signature
TonguePink and moistCoatedShiny/red/swollenBlistered/cracked
1234
Teeth/DenturesClean, no debrisLocalised debris/plaqueGeneralised debris/plaqueIll-fitting dentures/cariesImplants/bridges/crowns
1234
SalivaPresent/wateryThickDry mouthAbsent
1234
Mucous membranesPink and moistReddened and coatedWhite areasUlceration/bleeding
1234
LipsSmooth, pink and moistDry/crackedBleedingUlceration
1234
Capacity statusAlert/coherentApatheticSedatedUncooperative/unconscious
1234
PainPain freeAnticipated painIntermittentPain on movementUncontrolled
01234
Nutritional intakeGoodInadequate dietFluids onlyEnteralNo intake
01234
Other factorsNoneSteroid therapy/diabetesHaemorrhagic mucositis infection (viral/fungal)Oxygen therapy Mouth/breathing
012
34
Score 5–9Plan A
Score 10–17Plan B
Score 18–28Plan C
Score 29–31Plan D
Score 32–36Plan E
Assess the mouthExplain the procedure to the patient
It is important to assess the condition of a patient’s mouth with a structured assessment tool within 24 hours of hospital admission, then at least daily or more often, according to need, if the patient is unable to carry out appropriate mouth care independently (Health Education England [HEE], 2016; Huskinson & Lloyd, 2009; Bissett & Preshaw, 2011).
Explain the procedure to the patient so that they understand why it is important and will assist. Wash your hands and put on personal protective equipment (PPE) before you start.
Hygiene
Adults
Mouth care Page 2
Page 2 of 6
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Name: GARNET Alfre
d
D
OB: 20-Aug-1941
S
ex: M
NHS No: 460 955 7867
6812
07
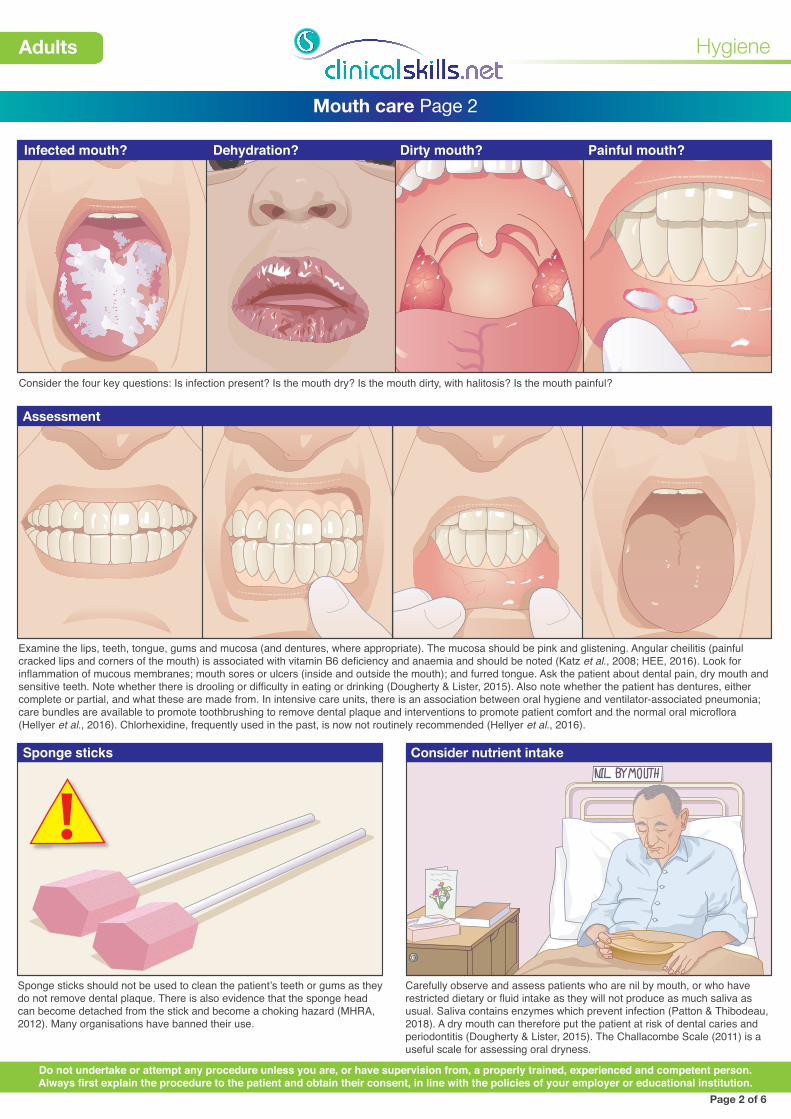
Sponge sticks Consider nutrient intake
Sponge sticks should not be used to clean the patient’s teeth or gums as they do not remove dental plaque. There is also evidence that the sponge head can become detached from the stick and become a choking hazard (MHRA, 2012). Many organisations have banned their use.
Carefully observe and assess patients who are nil by mouth, or who have restricted dietary or fluid intake as they will not produce as much saliva as usual. Saliva contains enzymes which prevent infection (Patton & Thibodeau, 2018). A dry mouth can therefore put the patient at risk of dental caries and periodontitis (Dougherty & Lister, 2015). The Challacombe Scale (2011) is a useful scale for assessing oral dryness.
Assessment
Examine the lips, teeth, tongue, gums and mucosa (and dentures, where appropriate). The mucosa should be pink and glistening. Angular cheilitis (painful cracked lips and corners of the mouth) is associated with vitamin B6 deficiency and anaemia and should be noted (Katz et al., 2008; HEE, 2016). Look for inflammation of mucous membranes; mouth sores or ulcers (inside and outside the mouth); and furred tongue. Ask the patient about dental pain, dry mouth and sensitive teeth. Note whether there is drooling or difficulty in eating or drinking (Dougherty & Lister, 2015). Also note whether the patient has dentures, either complete or partial, and what these are made from. In intensive care units, there is an association between oral hygiene and ventilator-associated pneumonia; care bundles are available to promote toothbrushing to remove dental plaque and interventions to promote patient comfort and the normal oral microflora (Hellyer et al., 2016). Chlorhexidine, frequently used in the past, is now not routinely recommended (Hellyer et al., 2016).
Consider the four key questions: Is infection present? Is the mouth dry? Is the mouth dirty, with halitosis? Is the mouth painful?
Dehydration? Dirty mouth? Painful mouth?Infected mouth?

Spatula
Side-effects of medication
Hygiene
Adults
Mouth care Page 3
Page 3 of 6
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Impact of oxygen therapy
Oxygen therapy can dry the oral mucosa if high flows are used, especially if used for longer than one hour, so ask patients if their mouth feels dry or uncomfortable. The need for humidification of oxygen should be assessed, as humidification will help to keep the mouth, lips and tongue moist (Macintosh & Moore, 2011). Several moisturising products are available for patients with a dry mouth due to receiving oxygen. It is important to consider these rather than inflammable petroleum-based products such as soft paraffin (HEE, 2016).
Some drugs and treatments (e.g., radiotherapy and chemotherapy) can cause a painful inflammation of the oral mucosa called mucositis (Dauncey, 2012). Antibiotics and steroid inhalers can cause candidiasis (“thrush”), which produces white and red patches on the tongue and other areas of the oropharynx. This condition can slow recovery and may progress to more serious infection in immunocompromised patients. Candida albicans can be treated with fluconazole, nystatin, miconazole or itraconazole (NICE, 2018).
Other factorsPhysical factors
Patients who have impaired physical and/or cognitive function may find it difficult to maintain effective mouth care. Food and tablets can become lodged between teeth or under partial dentures, so these patients will need help several times a day in order to remove debris and maintain their oral hygiene (Daly & Smith, 2015). Patients with mental health problems may need reminding to clean their teeth, may be more receptive to being helped at particular times of the day and may respond better to family members or carers they know to help them with their oral hygiene (HEE, 2016).
Dehydration, some medicines, infection of the oral tract or upper respiratory tract, and smoking can all result in a “furred” tongue which can inhibit eating, appetite and speech. Eating encourages the production of saliva and therefore keeps the mouth clean. Frequent sips of cold water, sugar-free chewing gum and moisturing gels or sprays may also help to keep the mouth moist. It is important to encourage mouth care in those patients receiving enteral or parenteral nutrition, who are unable to eat normally (Baillie, 2009; Pattison & Thibodeau, 2018).
(b) Cleaning denturesDentures: (a)
Encourage the patient to remove any dentures, to allow you to make a full assessment of their mouth. Observe for signs of poorly fitting dentures such as ulcers or bleeding gums. If the patient has a partial denture, check the remaining teeth.
Clean dentures using a soft toothbrush and a fragrance-free soap to remove food and plaque. Toothpaste is not recommended as it is abrasive and can damage the denture. Clean the patient’s gums, either with a soft toothbrush or with mouthwash/water for rinsing.
If additional picture needed could split caption and add picture of patient sipping water or using moisturising spray/patient receiving parenteral nutrition
681207
681207
DATE O
F BIRTH.........
NAME....
.....
..........
.......
WARD....
.........
.............
Potassium Chloride 0.15% w/v and Sodium Chloride 0.9% w/v Solution for Infusion BP
pH 4.5 -7.0 (approx) Hypertonic
Sodium Chloride 9.0g Potassium 20 Potassium Chloride 1.50g Sodium 154 Water for Injections qs Chloride 174
Osmolarity 388 m)sm/l (approx) Formula per 1000 ml mmol per 1000 ml (approx)
IV administration Read package leaflet before use
PL00116/0337 PA167/52/12 UN-35-01-531 1
POM 07 5 413760 137544 LOT EXP 12BO4E2B 01 / 2021
Keep out of reach and sight of children Do not remove from overwrap until ready for use Do not use unless solution is clear without visible particles and container undamaged Do not reconnect partially used bags
Contains UN-55 01 -069 20 mmol potassium 1000 ml
1000ml100
200
300
400
500
600
700
800
100
200
300
400
500
600
700
800
900 900
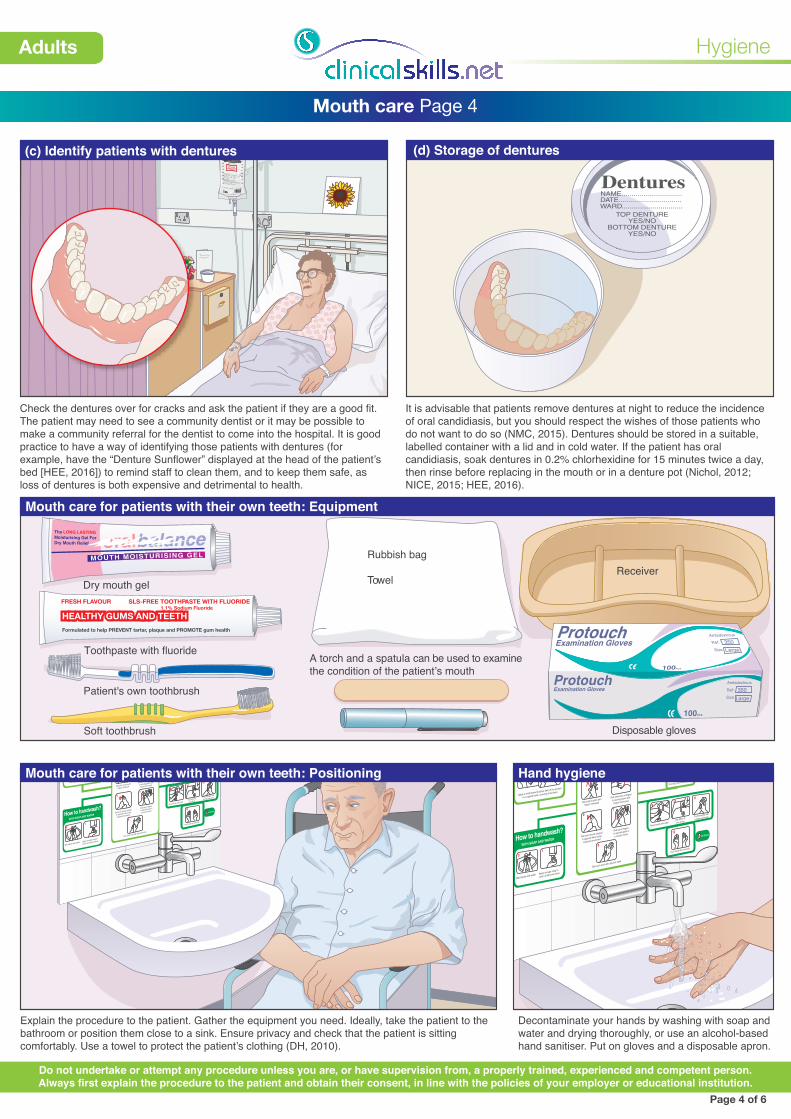
(d) Storage of dentures
Hygiene
Adults
Mouth care Page 4
Page 4 of 6
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Mouth care for patients with their own teeth: Positioning Hand hygiene
Explain the procedure to the patient. Gather the equipment you need. Ideally, take the patient to the bathroom or position them close to a sink. Ensure privacy and check that the patient is sitting comfortably. Use a towel to protect the patient’s clothing (DH, 2010).
Decontaminate your hands by washing with soap and water and drying thoroughly, or use an alcohol-based hand sanitiser. Put on gloves and a disposable apron.
Mouth care for patients with their own teeth: Equipment
HEALTHY GUMS AND TEETHFRESH FLAVOUR SLS-FREE TOOTHP
1.1% Sodium FluorideASTE WITH FLUORIDE
Formulated to help PREVENT tartar, plaque and PROMOTE gum health
Rubbish bag
Towel Receiver
Soft toothbrush
Patient's own toothbrush
Toothpaste with fluorideA torch and a spatula can be used to examinethe condition of the patient’s mouth
(c) Identify patients with dentures
Check the dentures over for cracks and ask the patient if they are a good fit. The patient may need to see a community dentist or it may be possible to make a community referral for the dentist to come into the hospital. It is good practice to have a way of identifying those patients with dentures (for example, have the “Denture Sunflower” displayed at the head of the patient’s bed [HEE, 2016]) to remind staff to clean them, and to keep them safe, as loss of dentures is both expensive and detrimental to health.
It is advisable that patients remove dentures at night to reduce the incidence of oral candidiasis, but you should respect the wishes of those patients who do not want to do so (NMC, 2015). Dentures should be stored in a suitable, labelled container with a lid and in cold water. If the patient has oral candidiasis, soak dentures in 0.2% chlorhexidine for 15 minutes twice a day, then rinse before replacing in the mouth or in a denture pot (Nichol, 2012; NICE, 2015; HEE, 2016).
Add picture of The Denture Sun�ower at end of someone’s bed and split caption below
oralbalanceThe LONG LASTINGMoisturising Gel ForDry Mouth Relief
MOUTH MOISTURISING GEL
Protouch
Protouch
Protouch350
AmbidextrousExamination Gloves
100PCS
Ref:
Size Large
350Ambidextrous
Examination Gloves Ref:
Size Large
100PCS
Disposable gloves
Dry mouth gel
45°
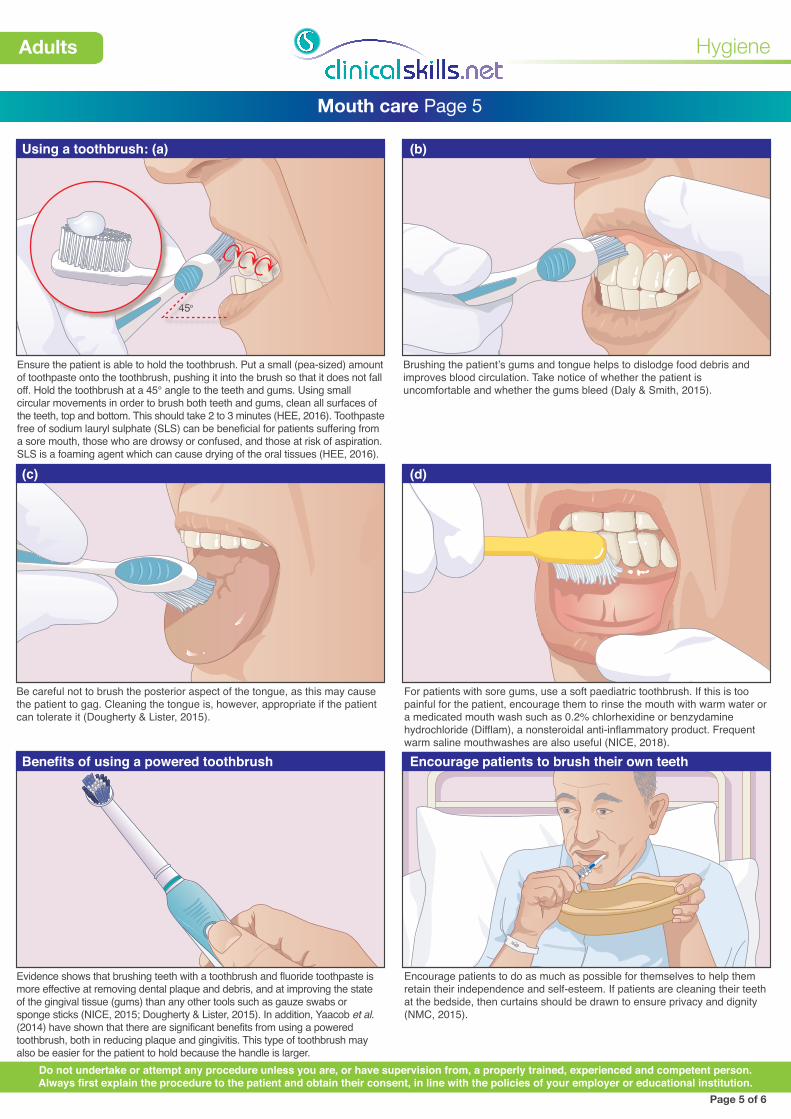
Using a toothbrush: (a) (b)
(c) (d)
Hygiene
Adults
Mouth care Page 5
Page 5 of 6
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Ensure the patient is able to hold the toothbrush. Put a small (pea-sized) amount of toothpaste onto the toothbrush, pushing it into the brush so that it does not fall off. Hold the toothbrush at a 45° angle to the teeth and gums. Using small circular movements in order to brush both teeth and gums, clean all surfaces of the teeth, top and bottom. This should take 2 to 3 minutes (HEE, 2016). Toothpaste free of sodium lauryl sulphate (SLS) can be beneficial for patients suffering from a sore mouth, those who are drowsy or confused, and those at risk of aspiration. SLS is a foaming agent which can cause drying of the oral tissues (HEE, 2016).
Brushing the patient’s gums and tongue helps to dislodge food debris and improves blood circulation. Take notice of whether the patient is uncomfortable and whether the gums bleed (Daly & Smith, 2015).
Be careful not to brush the posterior aspect of the tongue, as this may cause the patient to gag. Cleaning the tongue is, however, appropriate if the patient can tolerate it (Dougherty & Lister, 2015).
681207
Benefits of using a powered toothbrush Encourage patients to brush their own teeth
Evidence shows that brushing teeth with a toothbrush and fluoride toothpaste is more effective at removing dental plaque and debris, and at improving the state of the gingival tissue (gums) than any other tools such as gauze swabs or sponge sticks (NICE, 2015; Dougherty & Lister, 2015). In addition, Yaacob et al. (2014) have shown that there are significant benefits from using a powered toothbrush, both in reducing plaque and gingivitis. This type of toothbrush may also be easier for the patient to hold because the handle is larger.
Encourage patients to do as much as possible for themselves to help them retain their independence and self-esteem. If patients are cleaning their teeth at the bedside, then curtains should be drawn to ensure privacy and dignity (NMC, 2015).
BD added Jackie Hunt’s revisions 29 March 2018Added Almas Altai comments 9 April 18
For patients with sore gums, use a soft paediatric toothbrush. If this is too painful for the patient, encourage them to rinse the mouth with warm water or a medicated mouth wash such as 0.2% chlorhexidine or benzydamine hydrochloride (Difflam), a nonsteroidal anti-inflammatory product. Frequent warm saline mouthwashes are also useful (NICE, 2018).
CORSODYL MOUTHWASH
TREATS GUM PROBLEMS
ORIGINAL PEROXYL Mouthwash Hydrogen Peroxide RELIEVES MINOR MOUTH AND GUM IRRITATIONS Medicated mouthwash ultra DEX DAILY ORAL RINSE ActiveOxi
DEEPER CLEAN
LISTERINE COOL MINT A N T I S E P T I C Reduces Plaque and Left Behind After brushing
Removes up to 97% of germs
CORSODYL MOUTHWASH
TREATS GUM PROBLEMS
ORIGINAL PEROXYL Mouthwash Hydrogen Peroxide RELIEVES MINOR MOUTH AND GUM IRRITATIONS Medicated mouthwash
ultra DEX DAILY ORAL RINSE ActiveOxi
DEEPER CLEAN
LISTERINE COOL MINT A N T I S E P T I C Reduces Plaque and Left Behind After brushing Removes up to 97% of germs
Hygiene
Adults
Mouth care Page 6
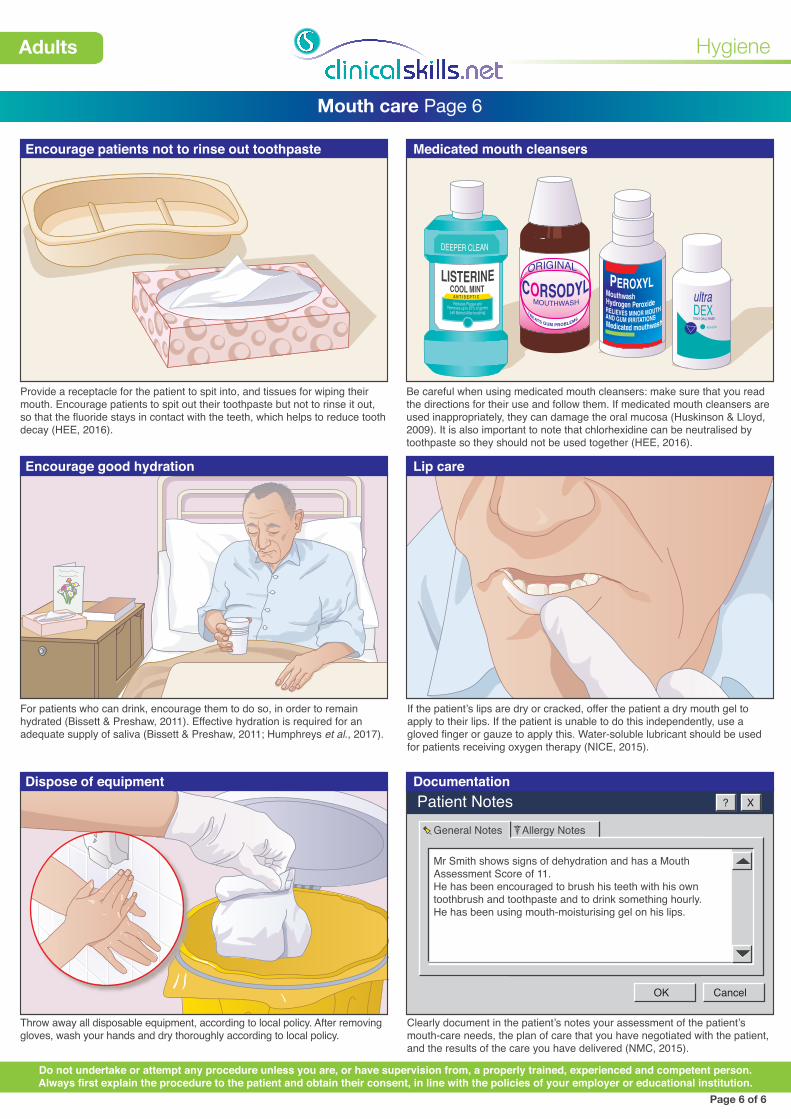
Encourage patients not to rinse out toothpaste Medicated mouth cleansers
Provide a receptacle for the patient to spit into, and tissues for wiping their mouth. Encourage patients to spit out their toothpaste but not to rinse it out, so that the fluoride stays in contact with the teeth, which helps to reduce tooth decay (HEE, 2016).
Be careful when using medicated mouth cleansers: make sure that you read the directions for their use and follow them. If medicated mouth cleansers are used inappropriately, they can damage the oral mucosa (Huskinson & Lloyd, 2009). It is also important to note that chlorhexidine can be neutralised by toothpaste so they should not be used together (HEE, 2016).
Encourage good hydration Lip care
For patients who can drink, encourage them to do so, in order to remain hydrated (Bissett & Preshaw, 2011). Effective hydration is required for an adequate supply of saliva (Bissett & Preshaw, 2011; Humphreys et al., 2017).
If the patient’s lips are dry or cracked, offer the patient a dry mouth gel to apply to their lips. If the patient is unable to do this independently, use a gloved finger or gauze to apply this. Water-soluble lubricant should be used for patients receiving oxygen therapy (NICE, 2015).
Patient Notes ? X
OK Cancel
General Notes
Mr Smith shows signs of dehydration and has a Mouth Assessment Score of 11. He has been encouraged to brush his teeth with his own toothbrush and toothpaste and to drink something hourly. He has been using mouth-moisturising gel on his lips.
Allergy Notes
Dispose of equipment Documentation
Throw away all disposable equipment, according to local policy. After removing gloves, wash your hands and dry thoroughly according to local policy.
Clearly document in the patient’s notes your assessment of the patient’s mouth-care needs, the plan of care that you have negotiated with the patient, and the results of the care you have delivered (NMC, 2015).
Page 6 of 6
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.





























