Embed Size (px)
Citation preview
Moving towards Regulatory Harmonization
of in-vitro Diagnostics
Rosanna W Peeling Professor and Chair, Diagnostic Research
London School of Hygiene & Tropical Medicine United Kingdom
• Landscape of regulatory oversight of IVDs
• Why harmonization and why now?
• Overall goals and priorities
• Inter-regional collaboration
• Moving forward
Regulatory Harmonization for IVDs
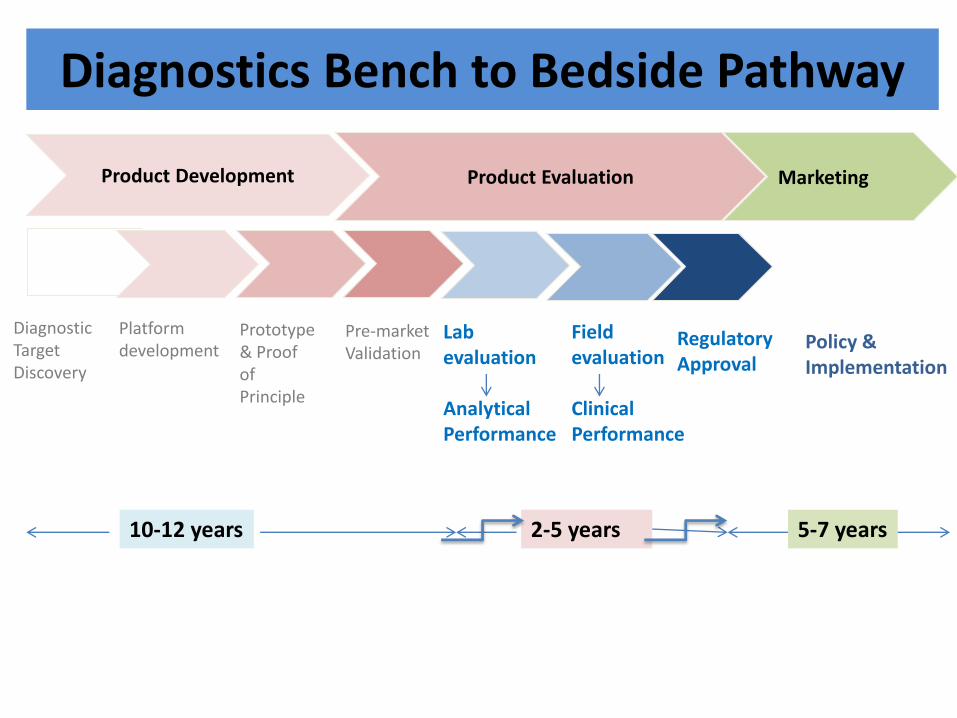
Diagnostics Bench to Bedside Pathway
Product Development
Product Evaluation
Marketing
Diagnostic Target Discovery
Platform development
Prototype & Proof of Principle
Pre-market Validation
Lab evaluation Analytical Performance
Policy & Implementation
Field evaluation Clinical Performance
Regulatory Approval
2-5 years 10-12 years 5-7 years
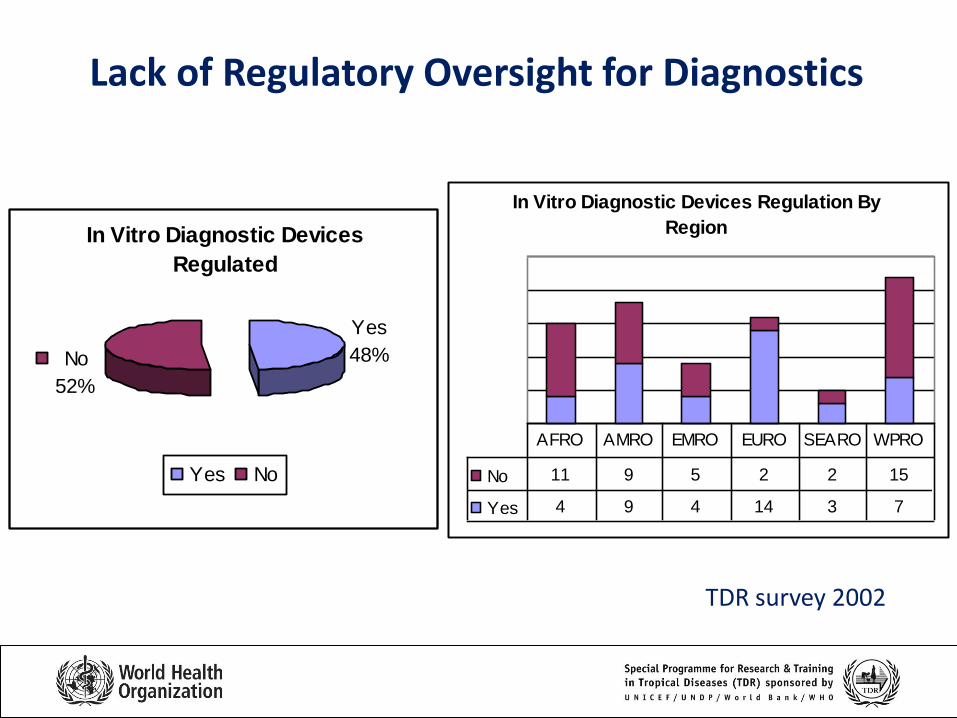
Lack of Regulatory Oversight for Diagnostics
In Vitro Diagnostic Devices
Regulated
No
52%
Yes
48%
Yes No
In Vitro Diagnostic Devices Regulation By
Region
No 11 9 5 2 2 15
Yes 4 9 4 14 3 7
AFRO AMRO EMRO EURO SEARO WPRO
TDR survey 2002
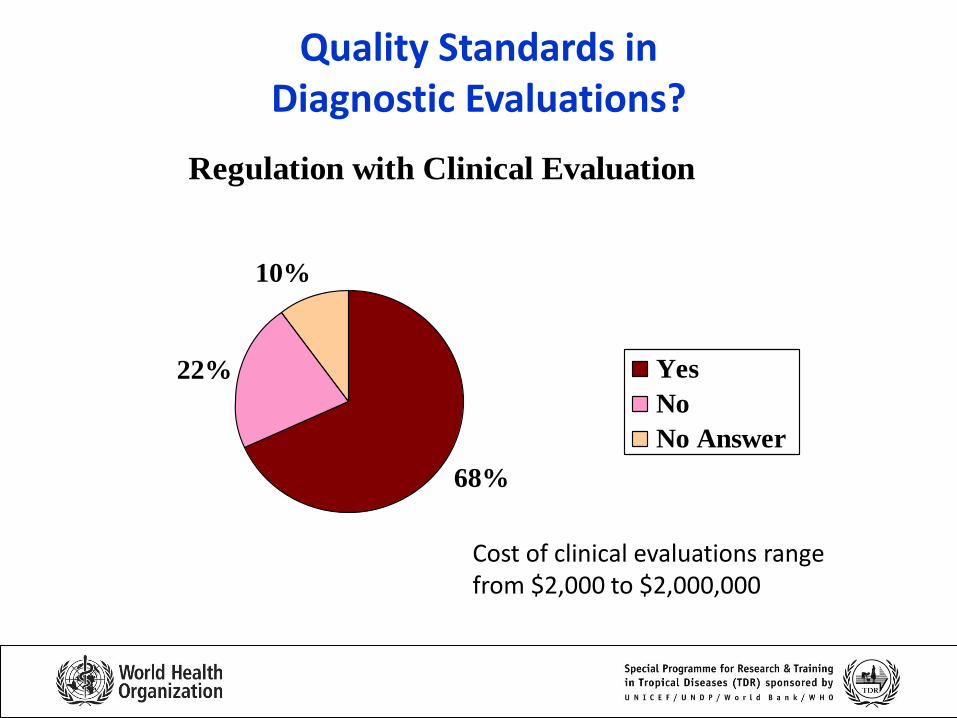
Quality Standards in Diagnostic Evaluations?
I. Diagnostics landscape
Regulation with Clinical Evaluation
68%
22%
10%
Yes
No
No Answer
Cost of clinical evaluations range from $2,000 to $2,000,000
Regulation of In-vitro Diagnostics: Top 10 Challenges
1. Regulatory landscape highly variable 2. Regulatory approval processes lengthy, especially for imported
tests 3. Most approval processes not transparent 4. Reviews often lack quality standards 5. Clinical performance studies often not required or lack rigour 6. Tests are sold and used in the developing world without
evidence of effectiveness 7. Cost of regulatory approval pass onto end-users 8. Companies with quality tests unable or unwilling to compete
in market flooded with low quality tests 9. Limited success with standardisation and harmonization 10. Companies often do not bother filing in countries with small
markets

• Landscape of regulatory oversight of IVDs
• Why harmonization and why now?
• Overall goals and priorities
• Inter-regional collaboration
• Moving forward
Regulatory Harmonization for IVDs
Global Harmonization Task Force (GHTF)
• GHTF was conceived in 1992 in response to the growing need for international
harmonization in the regulation of medical devices to ensure the safety,
effectiveness and quality of medical devices
• In 2006, GHTF included 3 Liaison Body members: the Asian Harmonization
Working Party (AHWP), International Organization for Standardization (ISO), and
International Electro-technical Commission (IEC)
• GHTF published and disseminated harmonized documents on basic regulatory
practices and served as an information exchange forum. GHTF documents are
developed by 5 Study Groups (SG):
– SG1 - Premarket Evaluation
– SG 2 - Post-Market Surveillance/Vigilance
– SG 3 - Quality Systems
– SG 4 - Auditing
– SG 5 - Clinical Safety/Performance
• In 2012, GHTF transitioned to a purely regulatory body called the International
Medical Devices Regulatory Forum (IMDRF) which will continue to promote the
principles of harmonization.
Asia Harmonization Working Party (AHWP)
Member Economies: (N=23) • Brunei, Cambodia, China, Hong Kong, India, Indonesia,
Korea, Laos, Malaysia, Myanmar, Pakistan, Philippines, Singapore, Taiwan, Thailand, Vietnam
• Abu Dhabi, Chile, Jordan, Kuwait, Saudi Arabia, South Africa, Yemen
• The Chair of AHWP for 2012-14 is Dr. Saleh S. Al-Tayyar
• Six working groups: – Work Group 1 (WG1) - Pre-Market Submission and CSDT
– Work Group 1a (WG1a) - IVDD
– Work Group 2 (WG2) - Post-Market Surveillance and Vigilance
– Work Group 3 (WG3) - Quality Management System
– Work Group 4 (WG4) - Quality System Audit
– Work Group 5 (WG5) - Clinical Safety/Performance
– Work Group 6 (WG6) - Capacity Building and Regulatory Training
– Special Task Group (STG - Nomenclature) - Medical Device Nomenclature
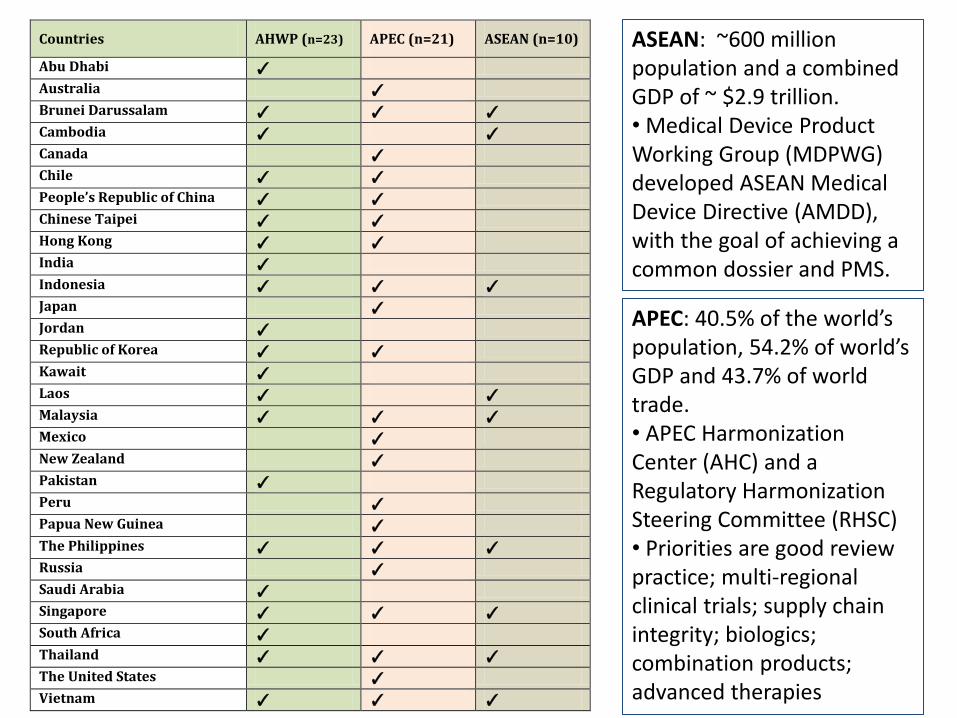
Countries AHWP (n=23) APEC (n=21) ASEAN (n=10)
Abu Dhabi ✓
Australia ✓
Brunei Darussalam ✓ ✓ ✓
Cambodia ✓ ✓ Canada ✓
Chile ✓ ✓
People’s Republic of China ✓ ✓
Chinese Taipei ✓ ✓
Hong Kong ✓ ✓
India ✓
Indonesia ✓ ✓ ✓
Japan ✓
Jordan ✓
Republic of Korea ✓ ✓
Kawait ✓
Laos ✓ ✓
Malaysia ✓ ✓ ✓
Mexico ✓
New Zealand ✓
Pakistan ✓
Peru ✓
Papua New Guinea ✓
The Philippines ✓ ✓ ✓
Russia ✓
Saudi Arabia ✓
Singapore ✓ ✓ ✓
South Africa ✓ Thailand ✓ ✓ ✓
The United States ✓
Vietnam ✓ ✓ ✓
ASEAN: ~600 million population and a combined GDP of ~ $2.9 trillion. • Medical Device Product Working Group (MDPWG) developed ASEAN Medical Device Directive (AMDD), with the goal of achieving a common dossier and PMS.
APEC: 40.5% of the world’s population, 54.2% of world’s GDP and 43.7% of world trade. • APEC Harmonization Center (AHC) and a Regulatory Harmonization Steering Committee (RHSC) • Priorities are good review practice; multi-regional clinical trials; supply chain integrity; biologics; combination products; advanced therapies
FY102 TFDA 推動新興市場國家之醫療器材法規科技研究及合作
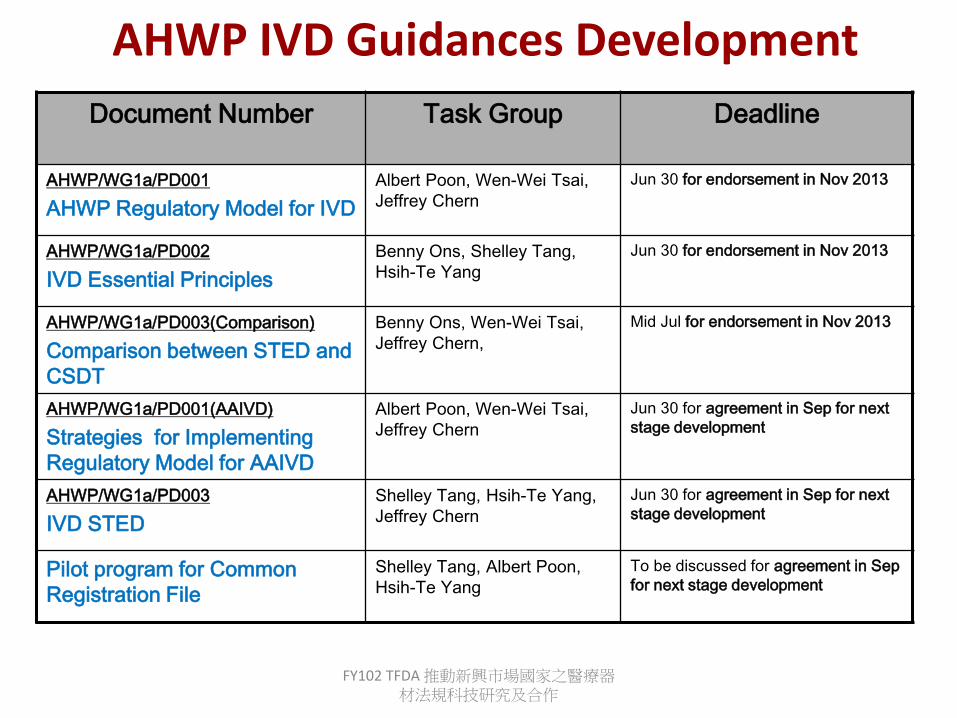
AHWP IVD Guidances Development
Document Number Task Group Deadline
AHWP/WG1a/PD001
AHWP Regulatory Model for IVD
Albert Poon, Wen-Wei Tsai,
Jeffrey Chern
Jun 30 for endorsement in Nov 2013
AHWP/WG1a/PD002
IVD Essential Principles
Benny Ons, Shelley Tang,
Hsih-Te Yang
Jun 30 for endorsement in Nov 2013
AHWP/WG1a/PD003(Comparison)
Comparison between STED and
CSDT
Benny Ons, Wen-Wei Tsai,
Jeffrey Chern,
Mid Jul for endorsement in Nov 2013
AHWP/WG1a/PD001(AAIVD)
Strategies for Implementing
Regulatory Model for AAIVD
Albert Poon, Wen-Wei Tsai,
Jeffrey Chern
Jun 30 for agreement in Sep for next
stage development
AHWP/WG1a/PD003
IVD STED
Shelley Tang, Hsih-Te Yang,
Jeffrey Chern
Jun 30 for agreement in Sep for next
stage development
Pilot program for Common
Registration File
Shelley Tang, Albert Poon,
Hsih-Te Yang
To be discussed for agreement in Sep
for next stage development
HIV/AIDS Global Targets
• Place 15 million people on ART by 2015
• Eliminate new HIV infections in children
• Intensify HIV prevention
United Nations General Assembly High Level Meeting on AIDS, 2011
Investments of at least US$
22 billion are needed by 2015
As of 2012: 9 million HIV patients are on ART
Why pilot POC tests for CD4, Viral Load and Early Infant Diagnosis ?
• A CD4 test is used to determine eligibility to treatment (<500 CD4/ul of blood). It is estimated that millions of HIV infected patients do not have access to a CD4 test to determine whether they are eligible for life-saving treatments, e.g. in Malawi, <10% of HV service facilities offer CD4 tests
• for HIV patients already on treatment, less than 30% have access to a viral load assay to know if their treatment is still effective
• Most countries do not have access to tests that can diagnose HIV in babies born to HIV + mothers as babies carry their maternal antibodies up to 18 months of age. 53% of HIV+ babies are dead by 2 years of age, compared to a mortality rate of 7.6% for HIV- babies
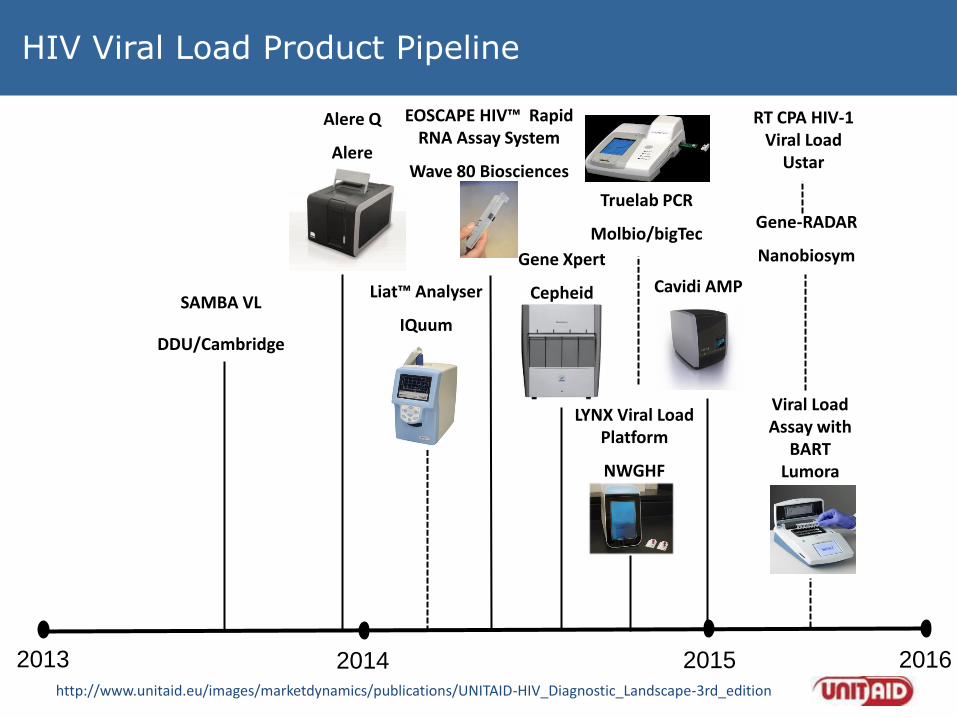
HIV Viral Load Product Pipeline
2015 2013 2014 2016
Alere Q
Alere
LYNX Viral Load Platform
NWGHF
SAMBA VL
DDU/Cambridge
Liat™ Analyser
IQuum
EOSCAPE HIV™ Rapid RNA Assay System
Wave 80 Biosciences
Gene Xpert
Cepheid Cavidi AMP
Viral Load Assay with
BART Lumora
Truelab PCR
Molbio/bigTec Gene-RADAR
Nanobiosym
RT CPA HIV-1 Viral Load
Ustar
http://www.unitaid.eu/images/marketdynamics/publications/UNITAID-HIV_Diagnostic_Landscape-3rd_edition
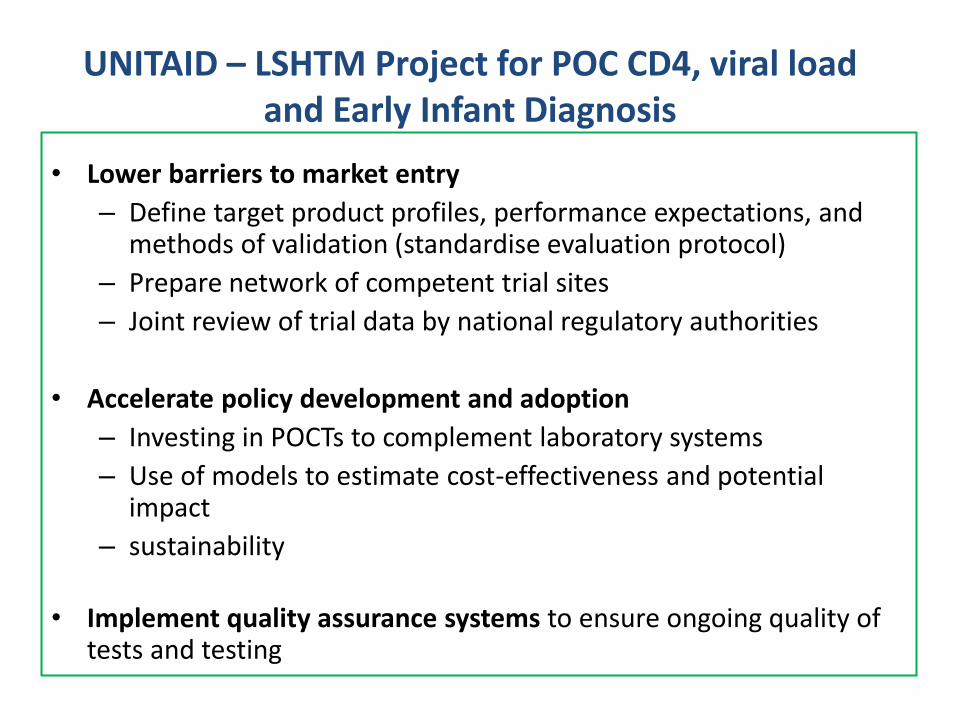
UNITAID – LSHTM Project for POC CD4, viral load and Early Infant Diagnosis
• Lower barriers to market entry
– Define target product profiles, performance expectations, and methods of validation (standardise evaluation protocol)
– Prepare network of competent trial sites
– Joint review of trial data by national regulatory authorities
• Accelerate policy development and adoption
– Investing in POCTs to complement laboratory systems
– Use of models to estimate cost-effectiveness and potential impact
– sustainability
• Implement quality assurance systems to ensure ongoing quality of tests and testing
• Landscape of regulatory oversight of IVDs
• Why harmonization and why now?
• Overall goals and priorities
• Inter-regional collaboration
• Moving forward
Regulatory Harmonization for IVDs

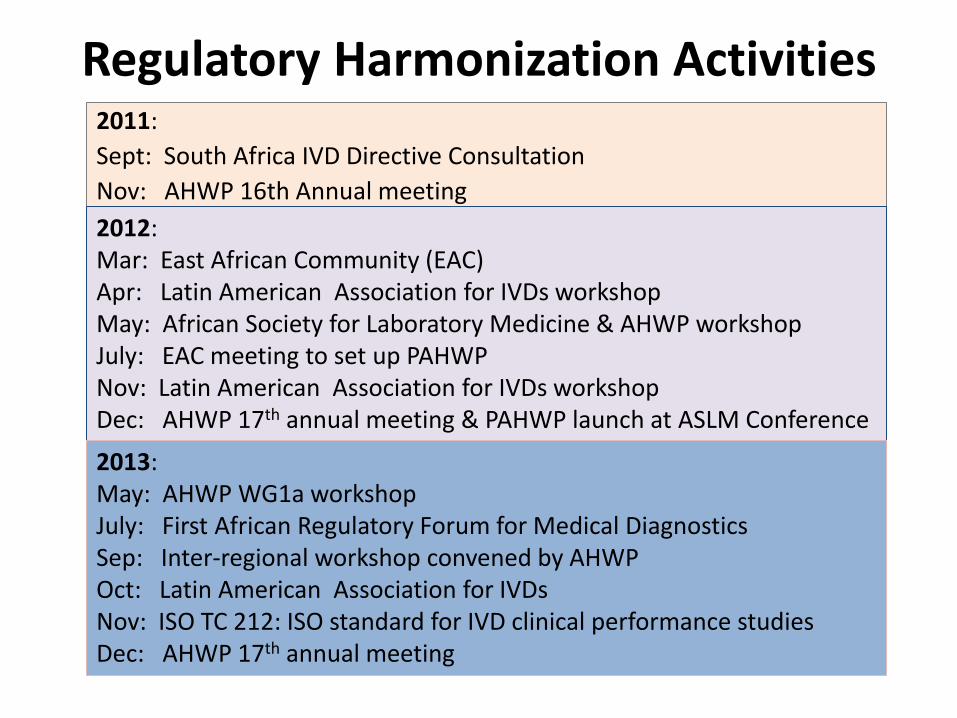
Regulatory Harmonization Activities 2011:
Sept: South Africa IVD Directive Consultation
Nov: AHWP 16th Annual meeting
2012: Mar: East African Community (EAC) workshop Apr: Latin American Association for IVD workshop May: African Society for Laboratory Medicine & AHWP workshops July: EAC meeting to set up PAHWP Nov: Latin American Association for IVDs workshops Dec: AHWP 17th annual meeting & PAHWP launch at ASLM Conference
2013: May: AHWP WG1a workshop July: First African Regulatory Forum for Medical Diagnostics Sep: Inter-regional workshop convened by AHWP Oct: Latin American Association for IVDs Nov: ISO TC 212: ISO standard for IVD clinical performance studies Dec: AHWP 17th annual meeting
East African Community (EAC)
• A regional intergovernmental organisation:
Kenya Uganda Tanzania Rwanda Burundi
• EAC was established in 1999, with a treaty ratified by the original 3 Partner
States – Kenya, Uganda and Tanzania. Rwanda and Burundi became full
Members in 2007. Its headquarters: Arusha, Tanzania
• Vision: a prosperous, competitive, secure, stable and politically united East Africa
• Mission: to widen and deepen Economic, Political, Social and Culture integration
in order to improve the quality of life of the people of East Africa through
increased competitiveness, value added production, trade and investments
• Launched the EAC Medicines Registration Harmonization Project on 30 March 2012, Arusha, Tanzania with support from New Partnerships for African Development (NEPAD), WHO, Wold Bank, BMGF, Clinton Health Access Initiative, DFID, GIZ and others. EAC Secretariat has agreed to discuss harmonization of diagnostics at its next meeting in September
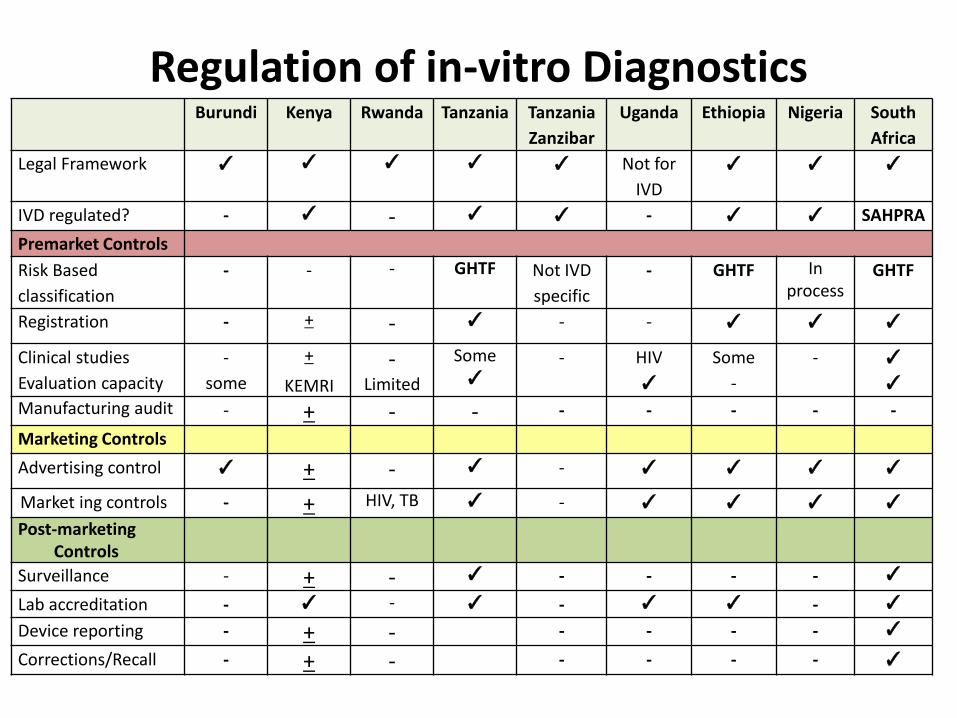
Regulation of in-vitro Diagnostics Burundi Kenya Rwanda Tanzania Tanzania
Zanzibar
Uganda Ethiopia Nigeria South
Africa
Legal Framework ✓ ✓ ✓ ✓ ✓ Not for
IVD
✓ ✓ ✓
IVD regulated? - ✓ - ✓ ✓ - ✓ ✓ SAHPRA
Premarket Controls
Risk Based
classification
- - - GHTF Not IVD
specific
- GHTF In process
GHTF
Registration - + - ✓ - - ✓ ✓ ✓
Clinical studies
Evaluation capacity
-
some
+
KEMRI
- Limited
Some ✓
- HIV
✓
Some
-
- ✓
✓
Manufacturing audit - + - - - - - - -
Marketing Controls
Advertising control ✓ + - ✓ - ✓ ✓ ✓ ✓
Market ing controls - + HIV, TB ✓ - ✓ ✓ ✓ ✓
Post-marketing Controls
Surveillance - + - ✓ - - - - ✓
Lab accreditation - ✓ - ✓ - ✓ ✓ - ✓
Device reporting - + - - - - - ✓
Corrections/Recall - + - - - - - ✓
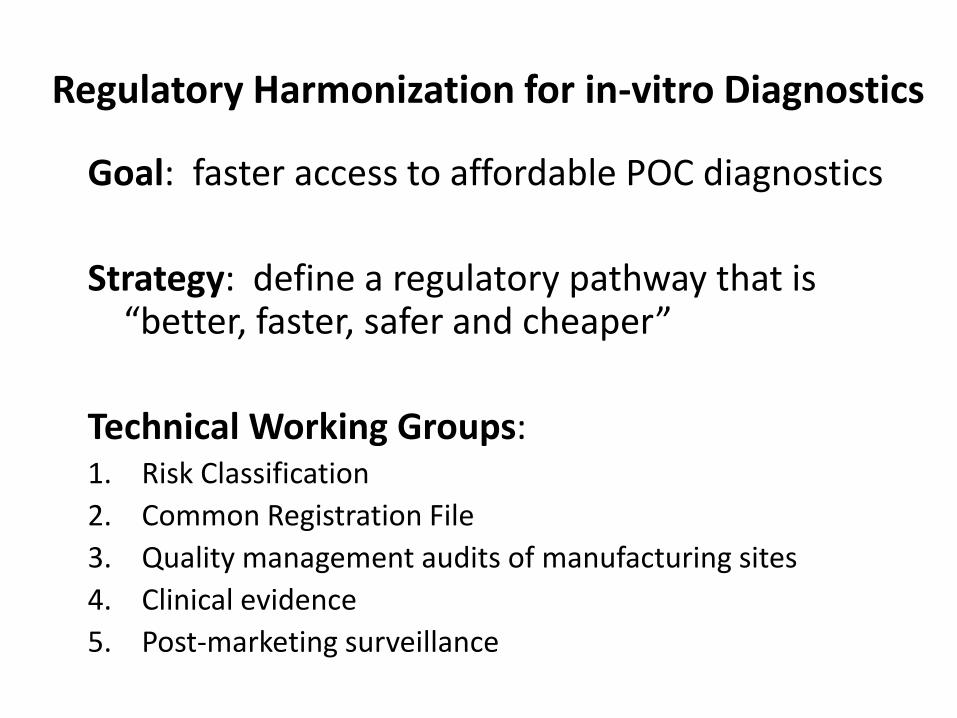
Regulatory Harmonization for in-vitro Diagnostics
Goal: faster access to affordable POC diagnostics
Strategy: define a regulatory pathway that is “better, faster, safer and cheaper”
Technical Working Groups: 1. Risk Classification
2. Common Registration File
3. Quality management audits of manufacturing sites
4. Clinical evidence
5. Post-marketing surveillance
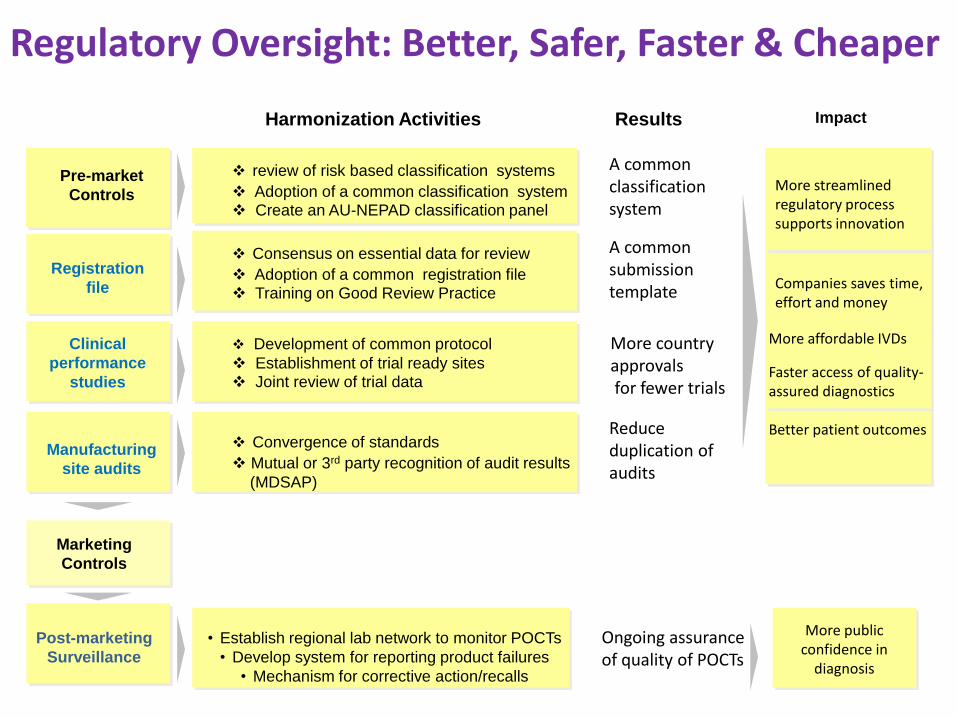
Pre-market
Controls
Pilot Implementation
Plan
Harmonization Activities
Impact
Training Registration
file
Quality
Assurance
Clinical
performance
studies
• Establish regional lab network to monitor POCTs
• Develop system for reporting product failures
• Mechanism for corrective action/recalls
Regulatory Oversight: Better, Safer, Faster & Cheaper
Marketing
Controls
Post-marketing
Surveillance
More public confidence in
diagnosis
Manufacturing
site audits
Consensus on essential data for review
Adoption of a common registration file Training on Good Review Practice
Development of common protocol
Establishment of trial ready sites Joint review of trial data
Convergence of standards
Mutual or 3rd party recognition of audit results
(MDSAP)
More country approvals for fewer trials
Reduce duplication of audits
A common submission template
Results
More affordable IVDs
Faster access of quality- assured diagnostics Better patient outcomes
Companies saves time, effort and money
Ongoing assurance of quality of POCTs
review of risk based classification systems
Adoption of a common classification system Create an AU-NEPAD classification panel
A common classification system
More streamlined regulatory process supports innovation
Regulatory Harmonization Activities 2011:
Sept: South Africa IVD Directive Consultation
Nov: AHWP 16th Annual meeting
2012: Mar: East African Community (EAC) Apr: Latin American Association for IVDs workshop May: African Society for Laboratory Medicine & AHWP workshop July: EAC meeting to set up PAHWP Nov: Latin American Association for IVDs workshop Dec: AHWP 17th annual meeting & PAHWP launch at ASLM Conference
2013: May: AHWP WG1a workshop July: First African Regulatory Forum for Medical Diagnostics Sep: Inter-regional workshop convened by AHWP Oct: Latin American Association for IVDs Nov: ISO TC 212: ISO standard for IVD clinical performance studies Dec: AHWP 17th annual meeting
24
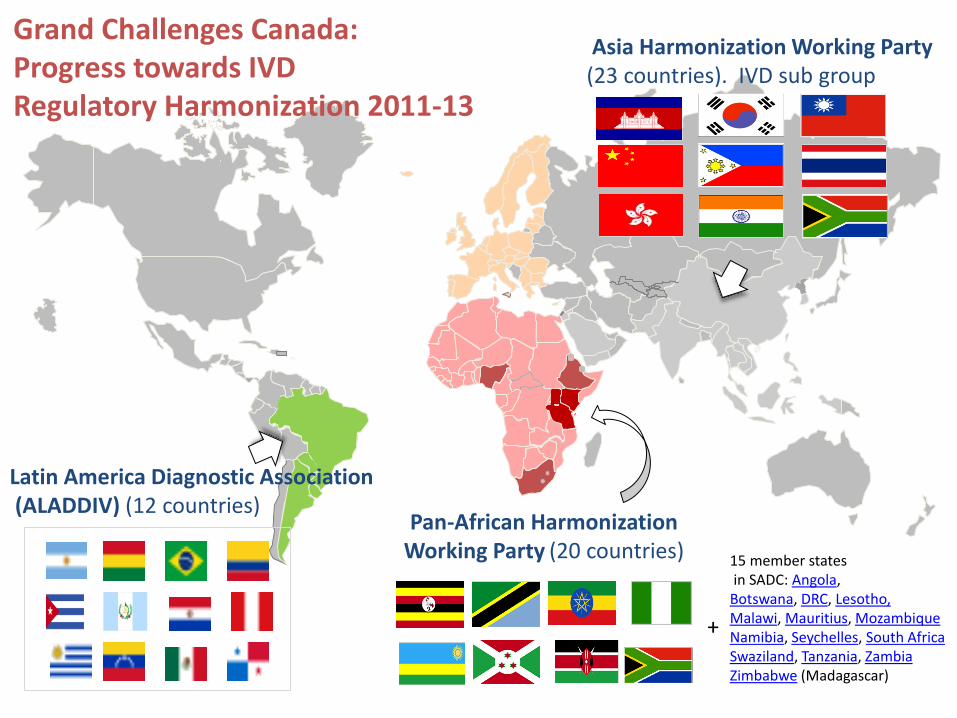
Grand Challenges Canada: Progress towards IVD Regulatory Harmonization 2011-13
. .
Asia Harmonization Working Party (23 countries). IVD sub group
Latin America Diagnostic Association (ALADDIV) (12 countries)
Pan-African Harmonization Working Party (20 countries)
+
15 member states in SADC: Angola, Botswana, DRC, Lesotho, Malawi, Mauritius, Mozambique Namibia, Seychelles, South Africa Swaziland, Tanzania, Zambia Zimbabwe (Madagascar)

• Landscape of regulatory oversight of IVDs
• Why harmonization and why now?
• Overall goals and priorities
• Inter-regional collaboration
• Moving forward
Regulatory Harmonization for IVDs
Moving Forward: least burdensome approach to:
Reduce Costs
Faster Access
Save Lives
Support Innovation
Regulatory Issues
• In countries where NRAs do not exist or have no capacity to regulatory diagnostics, evaluation of the performance of diagnostics is often carried out by laboratories for their own procurement purposes or by the national reference laboratory at the request of disease control programmes
• there is growing tension between newly empowered NRAs and laboratories who have been conducting test evaluations.
• NRAs have the overall legal mandate to ensure safety, quality and effectiveness of in-vitro diagnostics
• Laboratories are technical bodies who can supply evidence of test effectiveness and post-marketing surveillance data on quality of tests
• Inter-regional collaboration on regulatory harmonization: Mar 2014: AHWP workshop Mar 2014: IMDRF on medical device single audit programme (MDSAP) Jul 2014: 3rd African Regulatory Forum on Medical Diagnostics
• Need to create new models of public-private collaboration to: support innovation create an enabling environment for accelerating market entry and patient access to quality-assured diagnostics
• Need to build regulatory capacity in countries within the context of harmonization and efficiency • Need to brainstorm on how regulatory science can keep pace with technological advances
Moving Forward
Thank you • LSHTM: Ruth McNerney, Kim Sollis, Rhosyn Tuta, Beth Downe • AU: Paul Tanui • EAC: Stanley Sonoiya, Jane Masingia, Louisa Kosimbei • WHO: Jean-Bosco Ndihokubwayo, Willie Urassa, Robyn Meurant • ASLM: Trevor Peter, Tsehaynesh Messele • GIZ: Wesley Ronoh, Thomas Walter • PAHWP: Issac Kadowa, Ilonze Chinyere, Sagie Pillay, Sarvashi Moodliar,
Patience Dabula, Agnes Kijo • AHWP: Liling Liu, Albert Poon, Jeffrey Chern, Jack Wong, Benny Ons • ALADDIV: Carlos Gouvea • National regulatory authority representatives • Consultants: Maurine Murtagh, Ben Cheng, Elliott Cowan, Albert
Poon, Simon Rugera, Skating Panda Ltd • Many companies who have given us advice • Funding:
- Grand Challenges Canada: Peter Singer, Ken Simiyu, Rebecca Lackman - Bill & Melinda Gates Foundation: Gene Walther, Christine Rousseau,
Vincent Ahonkhai, Samuel Martins - UNITAID: Brenda Waning