Embed Size (px)
Citation preview

HEPATOBILIARY-PANCREAS
MR relaxometry of the liver: significant elevation of T1relaxation time in patients with liver cirrhosis
Tobias Heye & Schu-Ren Yang & Michael Bock &
Sylvia Brost & Kilian Weigand & Thomas Longerich &
Hans-Ulrich Kauczor & Waldemar Hosch
Received: 22 August 2011 /Revised: 6 December 2011 /Accepted: 15 December 2011 /Published online: 3 February 2012# European Society of Radiology 2012
AbstractObjectives To evaluate hepatic relaxation times T1, T2 andT2* in healthy subjects and patients with liver cirrhosisstratified by the Child-Pugh classification (CPC).Methods Sixty-one consecutive patients were stratified byCPC (class A026; B020; C015) and compared with age-matched controls (n031). Relaxometry measurements wereperformed at 1.5 T using six saturation recovery times (200–3,000 ms) to determine liver T1, six echo times (TE 14–113 ms) for T2 and eight TE (4.8–38 ms) for T2* assessment.Signal intensities in selected regions of interest in the liverparenchyma were fitted to theoretical models with leastsquares minimisation algorithms to determine T1, T2 and T2*.Results The most significant difference was the higherT1 values (852±132 ms) in cirrhotic livers compared withcontrols (678±45 ms, P<0.0001). A less significant
difference was seen for T2* (23±5 vs. 26±7 ms). Subdiffer-entiation showed a statistically significant difference be-tween control group and individual CPC classes as well asbetween class C and classes A or B for T1 relaxation times.Conclusion Measurement of T1 relaxation time can differ-entiate healthy subjects from patients with liver cirrhosis,and can distinguish between mild/moderate disease (CPC A/B) and advanced disease (CPC C).Key Points• Significantly elevated magnetic resonance T1 relaxationtimes are found in liver cirrhosis.
•T1 relaxation times can distinguish healthy subjects frompatients with liver cirrhosis.• T1 relaxation times can distinguish Child–Pugh classes Aand B from C.
Keywords MRI . Liver . Relaxation times . Liver cirrhosis .
Quantitative
Introduction
Chronic liver disease is a major public health problem. Thereare an estimated 800,000 cirrhosis-related deaths per yearworldwide [1]. A broad spectrum of hepatopathies can inducehepatic fibrosis, which may subsequently progress to livercirrhosis (LC). If detected at an early stage, liver fibrosismay be reversible and the incidence of late complications suchas end-stage liver disease or primary liver cancer can bedecreased [2–6]. Liver biopsy remains the best available di-agnostic procedure to provide a definite diagnosis despitelimitations such as its invasiveness, sampling error, and theinter- and intra-observer variation of interpretation [7, 8].Because liver biopsy is invasive, it is not suitable for use asa screening test for large segments of the population to detectsilent or significant liver disease or to evaluate the effect of
T. Heye : S.-R. Yang :H.-U. Kauczor :W. HoschDepartment of Diagnostic and Interventional Radiology,University Hospital,Heidelberg, Germany
M. BockDepartment of Medical Physics in Radiology,German Cancer Research Center (DKFZ),Heidelberg, Germany
S. Brost :K. WeigandDepartment of Gastroenterology, University Hospital Heidelberg,Heidelberg, Germany
T. LongerichInstitute of Pathology, University of Heidelberg,Heidelberg, Germany
T. Heye (*)Diagnostische und Interventionelle Radiologie,Radiologische Klinik, Universitätsklinikum Heidelberg,Im Neuenheimer Feld 110,69120 Heidelberg, Germanye-mail: [email protected]
Eur Radiol (2012) 22:1224–1232DOI 10.1007/s00330-012-2378-5

therapeutic interventions in apparent liver disease. There isthus an increasing need for a non-invasive, reproducible,quantitative and inexpensive test to identify liver disease [9].Non-invasive biomarkers and imaging techniques have re-cently been evaluated as methods for the detection and char-acterisation of liver disease [10, 11].
Serum tests [12–15] and various imaging methods such asultrasound elastography or magnetic resonance (MR) spec-troscopy, MR diffusion and MR elastography [16] have beeninvestigated for staging and diagnosing liver disease. Howev-er, MR relaxometry appears to be a promising tool for ana-lysing disease processes in other organ systems [17], and thereis evidence that indicates its usefulness in detecting liverdisease [18–21]. The relaxation times T1, T2 and T2* aretissue-specific parameters that are dependent on the physical,chemical and biological characteristics of the tissue. Relaxa-tion times may therefore change, in particular accompanyingparenchymal remodelling as in chronic liver disease [21]. Thepurpose of this study was to investigate whether T1, T2 andT2* relaxation times can be used as non-invasive, quantitativemeasures for diagnosing and stratifying liver cirrhosis.
Materials and methods
This prospective study was approved by the local institu-tional review board in accordance with the Declaration ofHelsinki. All study participants provided written informedconsent before the investigation.
Patients
The group of patients with liver cirrhosis consisted of 61consecutive patients (46 male, 15 female, mean age 61±8 years). Inclusion criteria were patients with biopsy-provenliver cirrhosis. Exclusion criteria were previous hepatic sur-gery or radiological interventions, liver malignancies orabscess, portal vein or bile obstruction, known iron deposi-tion or a contraindication for MRI. The time interval be-tween liver biopsy and MR relaxometry was 110±97 days.The causative agent for liver cirrhosis was chronic viralhepatitis B in 6, hepatitis C in 22, alcohol in 27, cryptogenicin 4 and autoimmune hepatitis in 2 cases.
A group of 31 consecutive healthy, age-matched patients(15 male, 16 female, mean age 60±10 years) without liverdisease served as the control group.
Clinical data
Laboratory results [i.e. serum albumin, bilirubin and inter-national normalised ratio (INR)] acquired within a mean of19±10 days of the MRI examination together with informa-tion on the severity of ascites and hepatic encephalopathy
were retrieved from the medical records to determine theChild-Pugh score [22]. Laboratory results of the healthycontrol group were within the normal range.
Magnetic resonance imaging
Magnetic resonance imaging was performed on a 1.5-Tsystem (Magnetom Avanto, Siemens, Erlangen, Germany)equipped with a 40 mT/m gradient system (slew rate: 170 T/ms). Two anterior six-element body phased-array coils andtwo three-element posterior spine-array coils were used forsignal reception. Patients were examined in a supine posi-tion, and all the images acquired were obtained during aninspiratory breath-hold.
MR relaxometry
T1 measurement
The T1 relaxation time of the liver parenchyma was deter-mined in a single breath-hold using a segmented saturation-recovery turboFLASH pulse sequence (SRTFL) with globalspin preparation [23]. The sequence uses a non-selectivesaturation pulse train to prepare the longitudinal magnet-isation. After the saturation recovery time TS, data areacquired with a segmented fast FLASH readout schemewith centric reordering to maintain the T1 contrast.
The following imaging parameters were used for theFLASH readout: TR05.5 ms; TE02.08 ms; flip angle015°;field of view 300×400 mm2; matrix 154×256 pixels; partialFourier 6/8; bandwidth 260 Hz/pixel; and a 5-mm slice thick-ness, resulting in an in-plane resolution of 1.9×1.6 mm2.During a single breath-hold it was possible for us to acquirea series of T1-weighted images with six different saturationrecovery times (TS0200, 400, 600, 800, 1,000, 3,000 ms) inaxial orientation in a total acquisition time of 18 s.
T2 measurement
A half-Fourier acquisition single-shot turbo spin-echo(HASTE) pulse sequence was repeated six times with dif-ferent echo times (TE) of 14, 32, 49, 67, 84, and 113 ms toquantify T2 relaxation times. Image parameters were asfollows: TR02,000 ms; flip angle 180°; field of view300×400 mm2; matrix 96×128; and a 6-mm slice thickness,resulting in an in-plane resolution of 3.1×3.1 mm2. Again,the six different contrasts were chosen because they couldbe acquired in axial orientation in a single breath-hold.
T2* measurement
To measure T2*, a set of eight gradient echoes was acquiredwith a spoiled gradient echo sequence (FLASH) with
Eur Radiol (2012) 22:1224–1232 1225

increasing TE of 4.8, 9.5, 14.3, 19.0, 23.8, 28.6, 33.3 and38.1 ms. Images were acquired in a single breath-hold in threeparallel slices. Additional sequence parameters were as fol-lows: TR0125 ms, flip angle 40°, field of view 325×400 mm2, matrix 187×256 pixels, and 6-mm slice thickness,resulting in an in-plane resolution of 1.7×1.6 mm2. To avoidodd-even echo artefacts, data were acquired with positivereadout gradient polarity only.
Evaluation of MR relaxometry
The relaxation times T1, T2 and T2* were calculated offlineusing dedicated curve fitting software implemented in theInteractive Data Language software package (IDL 6.0,Creaso, Gilching, Germany). In the software a free-hand,polygonal region of interest (ROI) was placed manually toencompass as much liver parenchyma as possible whilecarefully avoiding major intrahepatic vessels or lesions,e.g. simple cysts. The mean ROI signal intensity was plottedas a function of TS (for T1 measurements) or TE (for T2 and
T2*) measurements, and the theoretical signal-time curvewas fitted to the data using least-squares minimisation algo-rithms. The measurement was repeated three times, and theaverage value of the three measurements was noted as therelaxation time.
In an SRTFL experiment, the T1 relaxation is describedby the following signal equation:
SðTS; T1Þ ¼ S0 � 1� e�TS=T1� �
where the fit parameter S0 denotes the signal intensity atinfinite TS. For the T2 (and T2*) relaxation the signalequation is given by:
SðTE; T2Þ ¼ S0 � e�TE=T2
From the signal intensities in the SRTFL time series, theT1 relaxation times were determined using a non-linearMarquardt-Levenberg fit procedure, whereas T2 and T2*times were calculated by applying a linear fit to the naturallogarithm of the signal intensities.
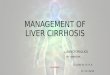
Fig. 1 A 50-year-old male patient with Child-Pugh class A livercirrhosis secondary to alcohol. Measurement of T1 relaxation time:axial segmented saturation-recovery single breath-hold turboFLASHpulse sequence (SRTFL) at six different saturation recovery time points(TS0200, 400, 600, 800, 1,000, 3,000 ms; left) were acquired. The
region of interest was placed in the liver parenchyma, carefully avoid-ing vessels (bottom right). T1 relaxation time was assessed from thesignal intensities in the SRTFL time series using a non-linearMarquardt-Levenberg fit (top right)
1226 Eur Radiol (2012) 22:1224–1232

Statistical analysis
Data are presented as mean values with standard deviation(SD) and 95% confidence interval (95% CI). Analysis ofvariance (one-way ANOVA) with Bonferroni correction formultiple comparisons was used to compare means. Thenormal distribution was assessed by the Shapiro-Wilk test.Student’s t-test was employed for normally distributed data(i.e. T1, T2 and T2* RT) and the Wilcoxon rank sum test,Mann-Whitney U-test and the Kruskal-Wallis test for data(e.g. age) not normally distributed. The χ2 test was used toanalyse nominal data (i.e. gender). Regression models [bi-nary logistic and ordinal regression (based on a generalisedlinear model)] were used to assess if T1, T2 and T2* candifferentiate between the groups (control group vs. livercirrhosis group) and between subgroups of the Child-Pughclassification [control group vs. class A (CA), class B (CB),or class C (CC)]. A receiver-operating characteristics anal-ysis was performed to identify a threshold value as a dis-criminator between study groups. An error probability ofP<0.05 was considered to be statistically significant. All
statistical analyses were calculated using commerciallyavailable software (PASW Statistics 18.0, SPSS, Chicago,IL, USA).
Results
The magnetic resonance examinations were well toleratedby all patients without any adverse reactions or prematuretermination of the examinations. There were no image arte-facts or technical failures that prohibited image analysis.Typical image data series of the T1, T2 and T2* measure-ments are shown in Figs. 1, 2 and 3 respectively. The imagesshow signal intensity changes according to increasing TStime points for T1 (TE for T2 and T2*) measurement andthe fit procedure.
Patient characteristics
There was no statistically significant difference in the agedistribution between the control group and the liver cirrhosis
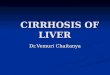
Fig. 2 A 50-year-old male patient with Child-Pugh class A livercirrhosis secondary to alcohol. Measurement of T2 relaxation time:axial half-Fourier acquisition single-shot turbo spin-echo (HASTE)pulse sequence repeated at six different echo times (TE014, 32, 49,
67, 84, 113 ms; left). The region of interest was placed in the liverparenchyma, excluding vessels (bottom right). T2 relaxation time wasdetermined by applying a linear fit to the natural logarithm of the signalintensities (top right)
Eur Radiol (2012) 22:1224–1232 1227

group (mean ± SD 60±10 vs. 61±8 years respectively; P00.605, Mann-Whitney U test). There was also no significantdifference in age between the liver cirrhosis patients strati-fied by Child-Pugh classification (CA: 62.1±8.3 years, CB:60.7±8.6 years, CC: 58.5±6.3 years) and the control group(P00.614 Kruskal-Wallis test). The gender distributionbetween the control group and the liver cirrhosis groupwas significantly different (control group: 15 male, 16female; liver cirrhosis: 46 male, 15 female; CA: 22 male,4 female; CB: 14 male, 6 female, CC: 10 male, 5 female;P00.01 χ2 test).
MR relaxometry
T1 relaxation times were significantly increased for livercirrhosis patients compared with the age-matched controlgroup (P<0.0001). Comparison of the control group andthe liver cirrhosis group stratified by the Child-Pughclassification revealed that the T1 relaxation times in-creased for each class. Significantly different T1 valueswere found when the control group was compared witheach Child-Pugh class (P<0.0001), and, furthermore,these values were significantly different for CA and CB
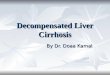
Fig. 3 A 50-year-old male patient with Child-Pugh class A livercirrhosis secondary to alcohol. Measurement of T2*: axial spoiledgradient echo sequence (FLASH) with increasing TE (4.8, 9.5, 14.3,19.0, 23.8, 28.6, 33.3, 38.1 ms, left). Carefully avoiding vessels, the
region of interest was placed in the liver parenchyma (bottom centre).By applying a linear fit to the natural logarithm of the signal intensities,the T2* relaxation time was defined (right)
Table 1 MR relaxometry. T1, T2 and T2* relaxation times of an age-matched healthy control group and patients with liver cirrhosis (LC) furtherstratified into subgroups class A (CA), B (CB) or C (CC) according to the Child-Pugh classification
Number T1 (ms) T2 (ms) T2* (ms)
Control 31 678±45 (661–694) 72±6 (68–76) 23±5 (21–24)
Liver cirrhosis (LC) 61 852±132 (818–886) 80±32 (72–88) 26±7 (25–28)
Child-Pugh classification of liver cirrhosis group
Class A (CA) 26 816±104 (774–858) 75±9 (71–78) 26±7 (23–29)
Class B (CB) 20 821±123 (764–879) 76±17 (68–84) 25±8 (21–28)
Class C (CC) 15 956±141 (878–1,034) 97±63 (59–135) 30±5 (27–32)
Data are presented as mean ± SD (95% confidence interval of the mean)
T1: P<0.0001 control vs. LC, vs. CA, vs. CB, vs. CC; P<0.0001 CA vs. CC; P<0.001 CB vs. CC
T2: P>0.05 for all group and Child-Pugh class comparisons
T2*: P00.005 control vs. LC; P00.002 control vs. CC
P calculated from one-way ANOVAwith Bonferroni correction for multiple comparisons
1228 Eur Radiol (2012) 22:1224–1232

compared with CC (CA: P<0.0001, CB: P<0.001). TheT1 differences between CA and CB were not statisticallydifferent. Data are displayed in Table 1 and Fig. 4.
T2 relaxation times were longer in liver cirrhosis patientsthan in the control group and increased with each Child-Pugh class. However, no statistically significant differenceswere observed (Table 1, Fig. 5).
For the T2* relaxation times, statistically significant differ-ences were present when the control group was compared withthe liver cirrhosis patients (P00.005) and with CC (P00.002).Statistical T2* data are summarised in Table 1 and Fig. 6.
Binary logistic regression was used to assess the contri-bution of variables such as age, gender, T1, T2 and T2* to amodel that assigns the study subjects either to the controlgroup or to the liver cirrhosis group. Essentially, only T1showed a significant contribution to the model (P<0.0001).Ordinal regression procedure using the same variables toclassify subjects into the control group or Child-Pugh clas-ses also identified T1 as the only significant parameter (P<0.0001). Using receiver-operating characteristics analysis,we calculated a T1 threshold of 748 ms, which discriminatesbetween control group and liver cirrhosis patients with asensitivity of 80% and specificity of 100% (true positives:49, false positives: 0, true negatives: 31, false negatives: 12,area under the curve: 0.91). A threshold of 877 ms was ableto differentiate CC from the other groups with a sensitivityof 80% and specificity of 86% (true positives: 12, falsepositives: 11, true negatives: 66, false negatives: 3, areaunder the curve: 0.87). No significant threshold wasobtained for T2 and T2*.
Fig. 4 Box plot of T1 relaxation times, reflecting patients with livercirrhosis stratified by the Child-Pugh classification and an age-matchedhealthy control group. Reference lines indicate thresholds as follows:748 ms separating healthy control and liver cirrhosis patients (sensi-tivity 80%; specificity 100%; true positives: 49, false positives: 0, truenegatives: 31, false negatives: 12, area under the curve: 0.91); 877 msdiscriminating Child-Pugh class C from all other groups (sensitivity80%; specificity 86%; true positives 12, false positives 11, true neg-atives 66, false negatives: 3, area under the curve: 0.87)
Fig. 5 Box plot of T2 relaxation times, reflecting patients with livercirrhosis stratified by Child-Pugh classification and an age-matchedhealthy control group. Circles indicate outliers; two outliers with T20136 ms (Child-Pugh class B) and 303 ms (Child-Pugh class C) are notshown
Fig. 6 Box plot of T2* relaxation times, reflecting patients with livercirrhosis stratified by Child-Pugh classification and an age-matchedhealthy control group. Circles indicate outliers
Eur Radiol (2012) 22:1224–1232 1229

Correlation analysis revealed a significant correlationamong variables only for T1 with r00.60 and r00.66 forstudy group classification, the control group vs. the livercirrhosis group and classification into Child-Pugh classes.No statistical difference was observed for T1, T2 and T2* ifthe groups examined (control, liver cirrhosis, CA, CB, CC)were stratified by gender (Table 2). The underlying aetiolo-gy had no effect on relaxation times as shown by the factthat further subdividing the groups according to the under-lying cause of cirrhosis did not reveal any statistical differ-ences (Table 2).
Discussion
The purpose of this study was to test the hypothesis that fibroticremodelling of the liver parenchyma in patients with livercirrhosis exerts an influence on relaxation times as measuredby MR relaxometry. The T1, T2 and T2* relaxation times aretissue parameters that are dependent on the physical, chemicaland biological characteristics of the tissue examined. Theresults of this study identified T1 relaxation times of liverparenchyma as a method of discriminating between healthysubjects and patients with liver cirrhosis. In addition, T1 relax-ation times also differentiated patients with Child-Pugh class Aor B from those with class C, separating mild or moderate fromsevere disease.
Although T2 relaxation times of the liver were higher inpatients with liver cirrhosis than in healthy subjects, wecould not find any significant differences in our study. T2*relaxation times were partially able to differentiate betweenthe control group and patients with liver cirrhosis, includingsubgroups, but not to reliably identify the stages of thedisease. Local mesoscopic incoherence in the magnetic field
contributes to T2*, so that structural changes on a cellularlevel should affect T2* significantly more than T2. Thestructural remodelling in cardiac disease has been shownto change the T2* values in the myocardium [24], and amathematical description has been found for calculating thelocal magnetic fields around the blood vessels in the heartmuscle to predict myocardial T2* [25]. For liver parenchy-ma, however, no mathematical models exist to predict thechange in T2* values, and thus a theoretical framework forT2* calculation still needs to be established.
Thomsen et al. reported a T1 relaxation time of 675±153 ms for healthy subjects and 931±192 ms for patientswith liver cirrhosis at 1.5 T [21]. Their work indicated thattissue remodelling in liver cirrhosis may be reflected in achange in relaxation times. In 1993 de Certaines and col-leagues [26] studied T1 and T2 relaxation times by measur-ing Eurospin TO5 test objects [27] and various organs,including the liver, in healthy subjects at different magneticfield strengths. They reported a mean T1 relaxation time of675±142 ms at 1.5 T by direct measurement of the liverparenchyma and 720±137 ms after correction according tophantom measurements. The quality of MR systems and thehomogeneity of the magnetic field strength have improvedsince that study was published in 1988 as T1 relaxation isstrongly dependent on the magnetic field [28]. The T1relaxation times of our study confirm the findings of thisearly study. The value of 678 ms for the healthy controlgroup with a threshold of 748 ms reliably separates healthysubjects from patients with liver cirrhosis. Mean T2 relaxa-tion times reported in 1993 by de Certaines (54 ms; 58 mscorrected) were lower than in the present study (72 ms),which may be due to a younger study population (range 20–60 years) than the mean age of 60 years in our study [26].The cited literature shows that although the variance in T1
Table 2 MR relaxometry liver cirrhosis subgroups. T1, T2 and T2* relaxation times of patients with liver cirrhosis (LC group) stratified by genderand causative agents
Number T1 (ms) T2 (ms) T2* (ms)
Gender
Male 46 842±139 (800–882) 80±36 (69–91) 25±7 (23–27)
Female 15 884±106 (825–942) 80±18 (69–90) 30±6 (26–33)
Cause
Viral hepatitis B 6 768±105 (657–879) 72±10 (61–83) 26±3 (23–29)
Viral hepatitis C 22 856±98 (812–900) 80±16 (73–87) 27±7 (24–30)
Alcohol 27 863±152 (800–926) 85±48 (65–106) 26±7 (23–29)
Cryptogenic 4 868±163 (731–1,004) 71±16 (59–83) 28±6 (18–35)
Autoimmune 2 776; 1,026 78; 81 25; 29
Data are presented as mean ± SD (95% confidence interval of the mean)
Student’s t-test for comparison by gender and one-way ANOVA with Bonferroni correction for multiple comparisons calculated for subgroups ofcauses with >5 patients showed no significant difference between the groups
1230 Eur Radiol (2012) 22:1224–1232

relaxation times between individual studies and individualsubjects is quite high, there seems to be a stable meanaround 675 [21, 26] to 678 ms (present study) for liverparenchyma in healthy subjects. In addition, comparison ofthe standard deviation measured in 1990 by Thomsen and in1993 by de Certaines (±153 and ±142 ms respectively) withthat in the present study (±45 ms) indicates there has beenimprovement in the accuracy of the method and the MRIequipment [21, 26].
Magnetic resonance relaxometry has been evaluated ear-lier in experimental ex vivo settings [29, 30]. Results ofthese studies show that MR relaxometry may fulfil therequirements of a non-invasive, quantitative and reproduc-ible test to identify liver cirrhosis. A recent study incorpo-rated T1 mapping before and after administration of contrastmaterial to compare and assess liver function in patientswith normal liver function and in patients with chronichepatitis and liver cirrhosis [31]. Although this work wasperformed at 3 T, the authors also showed that relaxometryis able to distinguish normal liver function from Child-Pughclasses A and B. Although the results presented there and inthe cited literature are promising, future investigationsshould assess the potential of MR relaxometry to identifyearly liver fibrosis, a condition of utmost clinical importancecurrently not sufficiently detected by non-invasive tests. MRrelaxometry may be incorporated into the clinical routine asa screening test in liver imaging to detect silent disease ordefine the stage of existing disease while extending theacquisition time of a liver MRI protocol by only 2–3 min.The accuracy of disease staging could be further improved ifMR T1 relaxometry were combined with a serum test [10,11, 32]. Further applications may be longitudinal studiesmonitoring patients with liver disease under therapy [10,33]. Ideally, a baseline relaxometry measurement used as ascreening test in conjunction with other clinical markerswould identify relevant liver disease, triggering either a liverbiopsy to confirm the findings or the initiation of therapy. IfMR relaxometry alone or in combination with other non-invasive tests proves to be sufficiently reliable in the dailyclinical routine, periodic MR relaxometry examinations maybe suitable for disease monitoring during therapy. In partic-ular, patients with viral hepatitis could benefit from thismethod; because imaging at regular intervals is necessaryto exclude hepatocellular carcinoma, the status of parenchy-mal remodelling could be quantitatively measured at thesame time. The possible role of MR relaxometry as a non-invasive test in a clinical concept of staging and diagnosingliver cirrhosis as well as monitoring disease in longitudinalstudies warrants further investigation, especially with regardto measurement reproducibility.
The study compares patients with liver cirrhosis classi-fied according to a clinical scoring system (Child-Pughscore) [22] and has certain limitations. Although the Child-
Pugh classification has been proven to correctly assessdisease stages as well as prognosis and has fulfilled itsclinical role to date [34, 35], the assumption of this studyis that disease progression into higher Child-Pugh classesalso reflects progressive parenchymal changes. Althoughthe time interval between laboratory data and MR relaxom-etry could be shorter, liver cirrhosis is a slowly progressingdisease, and none of the patients exhibited rapid deteriora-tion during the study. While there is some evidence thatclinical Child-Pugh scores are related to the histopatholog-ical fibrosis stage [36, 37], MR relaxometry needs to beevaluated in comparison to histopathology results in order toassess its potential as a non-invasive test. ROI placementmay be a source of variation due to a potential heteroge-neous distribution of parenchymal changes and limited re-producibility from patient to patient, but averaging threerepetitive measurements across a large area of liver paren-chyma should yield a representative value. The lack ofhistopathology for the control group is another potentiallimitation because early parenchymal changes such as stea-tosis may be present. However, liver biopsies in a controlgroup were not considered feasible for ethical reasons. Gen-der distribution was significantly different in the liver cir-rhosis group compared with the control group, with a 3:1male-to-female ratio in the former and an even distributionin the latter. However, this reflects the disease-specific gen-der frequency, and gender did not appear to be correlatedwith the study parameters or to contribute to the regressionmodel analysis. The time frame of 110±97 days betweenMR relaxometry and liver biopsy can be justified as thehistological disease progress in liver cirrhosis is relativelyslow.
To conclude, MRT1 relaxometry of the liver parenchymadifferentiated healthy subjects from patients with histologi-cally confirmed liver cirrhosis. Furthermore, patients withmild and moderate disease, corresponding to Child-Pughclasses A and B, were distinguished from severe disease, i.e. Child-Pugh class C. MR relaxometry may be incorporatedas a fast non-invasive test to identify liver cirrhosis. Whetherit may serve as an objective, quantitative method in longi-tudinal studies for monitoring patients with liver diseaseneeds to be evaluated in further studies.
Acknowledgements H.U. Kauczor is a consultant for the GeneralElectric Company and received funding for this research from SiemensAG and Boehringer Ingelheim GmbH.
References
1. World Health Organization (2004) The global burden of disease:2004 update. WHO Press, Geneva
Eur Radiol (2012) 22:1224–1232 1231

2. Bolanos-Meade J, Lopez-Arvizu C (2000) Histologic improve-ment of fibrosis in patients with hepatitis C and sustained responseto interferon therapy. Ann Intern Med 133:312
3. Dixon JB, Bhathal PS, Hughes NR, O’Brien PE (2004) Nonalcoholicfatty liver disease: improvement in liver histological analysis withweight loss. Hepatology 39:1647–1654
4. Farci P, Roskams T, Chessa L et al (2004) Long-term benefit ofinterferon alpha therapy of chronic hepatitis D: regression ofadvanced hepatic fibrosis. Gastroenterology 126:1740–1749
5. Friedman SL, Bansal MB (2006) Reversal of hepatic fibrosis – factor fantasy? Hepatology 43:S82–S88
6. Davis GL, Roberts WL (2010) The healthcare burden imposed byliver disease in aging Baby Boomers. Curr Gastroenterol Rep12:1–6
7. Strauss E (2010) Usefulness of liver biopsy in chronic hepatitis C.Ann Hepatol 9(Suppl):39–42
8. Rockey DC, Caldwell SH, Goodman ZD, Nelson RC, Smith AD(2009) Liver biopsy. Hepatology 49:1017–1044
9. PinzaniM, Rombouts K, Colagrande S (2005) Fibrosis in chronic liverdiseases: diagnosis and management. J Hepatol 42(Suppl):S22–S36
10. Castera L, Pinzani M (2010) Non-invasive assessment of liverfibrosis: are we ready? Lancet 375:1419–1420
11. Castera L, Pinzani M (2010) Biopsy and non-invasive methods forthe diagnosis of liver fibrosis: does it take two to tango? Gut59:861–866
12. Parkes J, Roderick P, Harris S et al (2010) Enhanced liver fibrosistest can predict clinical outcomes in patients with chronic liverdisease. Gut 59:1245–1251
13. McPherson S, Stewart SF, Henderson E, Burt AD, Day CP (2010)Simple non-invasive fibrosis scoring systems can reliably excludeadvanced fibrosis in patients with non-alcoholic fatty liver disease.Gut 59:1265–1269
14. Vizzutti F, ArenaU, Nobili Vet al (2009) Non-invasive assessment offibrosis in non-alcoholic fatty liver disease. Ann Hepatol 8:89–94
15. Molleken C, Sitek B, Henkel C et al (2009) Detection of novelbiomarkers of liver cirrhosis by proteomic analysis. Hepatology49:1257–1266
16. Bonekamp S, Kamel I, Solga S, Clark J (2009) Can imagingmodalities diagnose and stage hepatic fibrosis and cirrhosis accu-rately? J Hepatol 50:17–35
17. Hosch W, Bock M, Libicher M et al (2007) MR-relaxometry ofmyocardial tissue: significant elevation of T1 and T2 relaxationtimes in cardiac amyloidosis. Invest Radiol 42:636–642
18. Wang YX, Yuan J, Chu ES et al (2011) T1rho MR imaging issensitive to evaluate liver fibrosis: an experimental study in a ratbiliary duct ligation model. Radiology 259:712–719
19. Lee MJ, Kim MJ, Yoon CS, Han SJ, Park YN (2011) Evaluation ofliver fibrosis with T2 relaxation time in infants with cholestasis:comparison with normal controls. Pediatr Radiol 41:350–354
20. Keevil SF, Alstead EM, Dolke G, Brooks AP, Armstrong P, FarthingMJ (1994) Non-invasive assessment of diffuse liver disease by invivo measurement of proton nuclear magnetic resonance relaxationtimes at 0.08T. Br J Radiol 67:1083–1087
21. Thomsen C, Christoffersen P, Henriksen O, Juhl E (1990) Pro-longed T1 in patients with liver cirrhosis: an in vivo MRI study.Magn Reson Imaging 8:599–604
22. Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni McWilliams R(1973) Transection of the oesophagus for bleeding oesophagealvarices. Br J Surg 60:646–649
23. Bock M, Schulz J, Ueltzhoeffer S, Giesel F, Voth M, Essig M(2008) Intravascular contrast agent T1 shortening: fast T1 relax-ometry in a carotid volunteer study. MAGMA 21:363–368
24. Wacker CM, Bock M, Hartlep AW et al (1999) Changes in myo-cardial oxygenation and perfusion under pharmacological stresswith dipyridamole: assessment using T*2 and T1 measurements.Magn Reson Med 41:686–695
25. Bauer WR, Nadler W, Bock M et al (1999) Theory of coherent andincoherent nuclear spin dephasing in the heart. Phys Rev Lett83:4215–4218
26. de Certaines JD, Henriksen O, Spisni A, Cortsen M, Ring PB(1993) In vivo measurements of proton relaxation times in humanbrain, liver, and skeletal muscle: a multicenter MRI study. MagnReson Imaging 11:841–850
27. Lerski RA, McRobbie DW, Straughan K, Walker PM, de CertainesJD, Bernard AM (1988) Multi-center trial with protocols andprototype test objects for the assessment of MRI equipment. EECConcerted Research Project. Magn Reson Imaging 6:201–214
28. Henriksen O, de Certaines JD, Spisni A, Cortsen M, Muller RN,Ring PB (1993) In vivo field dependence of proton relaxationtimes in human brain, liver and skeletal muscle: a multicenterstudy. Magn Reson Imaging 11:851–856
29. Bernardino ME, Small W, Goldstein J et al (1983) Multiple NMRT2 relaxation values in human liver tissue. AJR Am J Roentgenol141:1203–1208
30. Chamuleau RA, Creyghton JH, De Nie I, Moerland MA, Van derLende OR, Smidt J (1988) Is the magnetic resonance imagingproton spin-lattice relaxation time a reliable noninvasive parameterof developing liver fibrosis? Hepatology 8:217–221
31. Katsube T, Okada M, Kumano S et al (2011) Estimation of liverfunction using T1 mapping on Gd-EOB-DTPA-enhanced magneticresonance imaging. Invest Radiol 46:277–283
32. Castera L, Sebastiani G, Le Bail B, de Ledinghen V, Couzigou P,Alberti A (2010) Prospective comparison of two algorithms com-bining non-invasive methods for staging liver fibrosis in chronichepatitis C. J Hepatol 52:191–198
33. Kim SU, Han KH, Ahn SH (2010) Non-invasive assessment ofliver fibrosis: time to move from cross-sectional studies to longi-tudinal ones. J Gastroenterol Hepatol 25:1472–1473
34. Boursier J, Cesbron E, Tropet AL, Pilette C (2009) Comparisonand improvement of MELD and Child-Pugh score accuracies forthe prediction of 6-month mortality in cirrhotic patients. J ClinGastroenterol 43:580–585
35. Shaikh S, Ghani H, Memon S, Baloch GH, Jaffery M, Shaikh K(2010) MELD era: is this time to replace the original Child-Pughscore in patients with decompensated cirrhosis of liver. J CollPhysicians Surg Pak 20:432–435
36. Foucher J, Chanteloup E, Vergniol J et al (2006) Diagnosis ofcirrhosis by transient elastography (FibroScan): a prospectivestudy. Gut 55:403–408
37. Hashimoto K, Murakami T, Dono K et al (2006) Assessment of theseverity of liver disease and fibrotic change: the usefulness ofhepatic CT perfusion imaging. Oncol Rep 16:677–683
1232 Eur Radiol (2012) 22:1224–1232