Embed Size (px)
Citation preview

1575HEPATIC IMAGING
Marcony Queiroz-Andrade, MD • Roberto Blasbalg, PhD, MD • Cinthia D. Ortega, MD • Marco A. M. Rodstein, MD • Ronaldo H. Baroni, PhD, MD • Manoel S. Rocha, PhD, MD • Giovanni G. Cerri, PhD, MD
Hemochromatosis can be classified as (a) primary, when it origi-nates from a genetic disturbance that promotes the increase of iron absorption, or (b) secondary, when it relates to chronic diseases or to multiple transfusions. The distribution of iron accumulation dif-fers between these two forms; therefore, they can be distinguished by using imaging methods in the majority of cases. Magnetic resonance (MR) imaging is the most sensitive and specific imaging modality in the diagnosis of hemochromatosis. The susceptibility effect caused by the accumulation of iron leads to signal loss in the affected tissues, particularly with the T2*-weighted sequences, which makes the diag-nosis of iron overload possible. By using MR imaging techniques, it is possible to estimate the hepatic iron concentration in a noninvasive way, thereby avoiding repeated biopsies. Hemochromatosis can lead to complications, such as a higher frequency of neoplasia, particularly the development of hepatocellular carcinoma. Other neoplasms, such as colorectal tumors, are also associated. Complications related to the treatment of chronic anemia include the appearance of peliosis hepatis and tumors, which can regress after the suspension of treatment with drugs. Knowledge of the disease and of the patterns of iron deposi-tion in patients with iron overload enables not only diagnosis, but also treatment, follow-up, and the detection of possible complications by using imaging methods.©RSNA, 2009 • radiographics.rsna.org
MR Imaging Findings of Iron Overload1
Abbreviations: GRE = gradient echo, SE = spin echo
RadioGraphics 2009; 29:1575–1589 • Published online 10.1148/rg.296095511 • Content Codes: 1From the Department of Radiology, Faculty of Medicine, University of São Paulo, Av Dr Eneas de Carvalho Aguiar 255, 05403-900 São Paulo, Brazil. Presented as an education exhibit at the 2008 RSNA Annual Meeting. Received March 17, 2009; revision requested May 5 and received June 6; accepted June 9. All authors have no financial relationships to disclose. Address correspondence to R.B. (e-mail: [email protected]).
©RSNA, 2009
See last page
TEACHING POINTS
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights.

1576 October Special Issue 2009 radiographics.rsna.org
IntroductionIron is found in the body particularly in the composition of certain structures, such as the cytochromes, hemoglobin, and myoglobin. After being absorbed by the mucosa of the small intes-tine, iron is transported by transferrin and stored in another complex known as ferritin (1).
Medullary erythropoiesis requires around 20 mg of iron daily. However, only 1–2 mg of dietary iron is absorbed, which corresponds to 10% of the total amount ingested. Approximately the same amount is lost each day because of epithe-lial desquamation, menstruation, and other forms of blood loss. There is a good recycling mecha-nism through the reuse of iron found in old erythrocytes. Thus, the absorption is physiologi-cally well controlled because there is no effective form of excretion (1,2).
Basically, iron is stored in the hepatic paren-chyma and in the reticuloendothelial system. Ex-cess iron can lead to toxicity because this element can catalyze the conversion of hydrogen peroxide into free radicals, causing damage to the cell membranes, proteins, and DNA (1).
The causes of iron accumulation in the body are numerous. The signs and symptoms of iron overload are highly nonspecific, which leads to (a) difficulty in developing a clinical suspicion that a patient has the condition and (b) a long period for correct diagnosis (3,4). The frequency of this disease varies according to the diagnostic methods used and the population studied (5).
The purpose of this article is to describe iron overload (hemochromatosis) and illustrate its appearance at magnetic resonance (MR) imag-ing, with an emphasis on detection, quantifica-tion, and related complications. After a general description of iron overload, the MR imaging methods and the patterns of iron deposition are presented, followed by the relationships of iron overload to other storage diseases and to various hepatic focal lesions.
HemochromatosisIron overload (hemochromatosis) can be classified as primary or secondary. Primary hemochroma-tosis is a recessive autosomal genetic disorder that alters a protein involved in the regulation of iron absorption. Most of these patients are homozy-
gous or heterozygous for this mutation and have iron absorption two or three times higher than that of the unaffected population (1,6). The results of studies indicate a global rate of occurrence of the gene of around 2%–5%, and primary hemochro-matosis is considered the most common genetic disease in the white population (rate of disease, 0.2%–0.5% for homozygous disease and as much as 10% for heterozygous disease) (1,5,7).
Any other nongenetic cause of iron accumula-tion in the organs is classified as secondary hemo-chromatosis. The causes of secondary hemochro-matosis include (a) another cause of increased absorption, such as cirrhosis, (b) myelodysplastic syndrome, (c) anemias related to ineffective eryth-ropoiesis (eg, thalassemia), and (d) exogenous increase by ingestion, parenteral infusion, or mul-tiple transfusions (2,3,8). The main differences between the primary and the secondary forms of hemochromatosis are shown in Table 1.
The disease is often clinically silent but can be diagnosed with imaging methods; therefore, radiologists should be aware of the MR imaging findings so that they can suggest the diagnosis. Moreover, the evaluation of the effects of clinical treatment can also be done in a noninvasive way.
Laboratory values used in the diagnosis of hemochromatosis include the ferritin level and the transferrin saturation index, both of which are generally increased in these patients. However, these tests have low sensitivity and specificity, with false-positive results found in alcohol abus-ers and with false-negative results found in young patients with hemochromatosis (1,9,10).
The genetic test can be done by using an inex-pensive blood examination. The test, which con-sists of the identification of the genes associated with primary hemochromatosis, is used primarily in the evaluation of populations at risk or to con-firm the diagnosis of primary hemochromatosis in patients with iron overload. However, the use of this test remains a topic of debate because identification of the defined mutations tests for only a subset of the patients with primary hemo-chromatosis and because other genetic mutations related to hemochromatosis have been identified. The overall costs and benefits of screening re-main unclear (5–7,11).
Hepatic biopsy is considered the reference standard method for diagnosis because biopsy has the capacity to be used to quantify iron overload, to determine the prognosis on the basis

RG ■ Volume 29 • Number 6 Queiroz-Andrade et al 1577
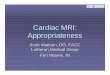
Figure 1. Appearance of the liver at CT. (a) Axial nonenhanced CT image of a normal liver (attenuation, 54–59 HU). (b) Axial nonenhanced CT image of a patient with secondary hemochromatosis shows increased liver attenua-tion (103–109 HU).
of the level of hepatopathy, and to monitor the evolution of the disease and the effects of treat-ment. However, biopsy is an invasive procedure with known potential risks and is susceptible to sampling error because of the tiny amount of tis-sue taken from the edge of the liver (9,10,12).
Imaging MethodsComputed tomography (CT) and MR imaging can be used to detect iron overload. Nonen-hanced CT shows a homogeneous increase in the attenuation of the hepatic parenchyma to 72 HU or more (13,14). CT has low sensitivity
(63%) and high specificity (96%) for the diag-nosis of iron overload.
Certain conditions, such as associated ste-atosis, can reduce the sensitivity still further by reducing the hepatic parenchymal attenuation. Other factors, such as Wilson disease, colloidal gold treatment, and long-term administration of amiodarone, also increase the hepatic parenchy-mal attenuation, which decreases the diagnostic specificity of CT (14–17) (Fig 1).
Table 1 Features of Primary and Secondary Hemochromatosis
Primary Hemochromatosis Secondary Hemochromatosis (Acquired)
Hereditary autosomal recessive disease Parenteral administration of iron (eg, repeated blood transfusions)
Increases intestinal absorption with normal dietary intake of iron
Dietary iron overload
Iron excess deposits in parenchymal cells, preferen-tially in the liver, pancreas, heart, pituitary gland, thyroid, and synovium
Iron is predominantly deposited in the reticuloendothelial system (spleen and Kupffer cells)
Leads to cellular damage, organ dysfunction, and malignancy
Less toxic
If untreated, may progress to cirrhosis, hepatocellu- lar carcinoma, diabetes, and cardiac dysfunction
Secondary increased absorption of normal dietary iron intake: liver diseases (alcoholic hepatitis and hepatitis C), myelodysplastic syndrome, anemias, other chronic and oncologic diseases

1578 October Special Issue 2009 radiographics.rsna.org
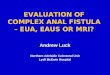
Figure 2. Dual-sequence MR imaging of the liver. (a, b) Hepatic steatosis. Axial GRE T1-weighted in-phase (a) and out-of-phase (b) MR images show a decrease in the signal intensity of the liver on the out-of-phase image (chemical shift). (c, d) Hemochromatosis. Axial GRE T1-weighted in-phase (c) and out-of-phase (d) MR images show a decrease in the signal intensity of the liver on the in-phase image (T2* effect).
verse relaxation time (T2), and particularly the transverse relaxation time as affected by magnetic field inhomogeneity (T2*). This effect causes a loss of signal intensity in the affected organs that is proportional to the iron deposition (17,21).
In the general protocol applied to an abdomi-nal study, it is not possible to estimate the hepatic iron concentration, although most of the time, it is possible to diagnose iron overload. This can be done by using “dual-sequence” (gradient in and out of phase) MR imaging, which demonstrates decreased signal intensity in the affected tissues on the in-phase images compared with the out-
MR imaging is the best noninvasive method for measuring the level of iron in the liver for the purposes of confirming the diagnosis, determin-ing the severity, and monitoring therapy with high sensitivity, specificity, and positive and nega-tive predictive values (12,18–20). The accumu-lation of iron ions in the tissues, because of the superparamagnetic properties of the ions, causes local distortion in the magnetic fields and relax-ation of the spins, which results in shortening of the longitudinal relaxation time (T1), the trans-
TeachingPoint
TeachingPoint
of-phase images. That effect is the opposite of the effect observed in patients with steatosis (Fig 2). This occurs because the echo time of the in-phase sequence is usually higher than that of the out-of-phase sequence; therefore, the in-phase pulse sequence is more sensitive to iron deposits because of the increased T2* effect (21).

RG ■ Volume 29 • Number 6 Queiroz-Andrade et al 1579
times are acquired. On the Web site of the Uni-versity of Rennes (http://www.radio.univ-rennes1 .fr/Sources/EN/Hemo.html), it is possible to cal-culate the estimated hepatic iron concentration by filling in the region of interest (ROI) values requested (24).
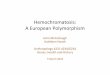
The results of examination of unaffected sub-jects show that the hepatic parenchyma dem-onstrates higher signal intensity than that of the paraspinal musculature with all sequences. Slight to moderate iron overload is better identified and evaluated on the GRE images obtained with lon-ger echo times, which demonstrate a decrease in the signal intensity of the liver parenchyma (Fig 3). When the hepatic iron concentration is high, MR sequences do not have good accuracy because
Iron Quantifi- cation with MR Imaging
The results of multiple studies have demon-strated that it is possible to estimate the amount of hepatic iron overload at MR imaging, with high correlation to the values found in speci-mens from biopsy (12,18–20,22,23). In our hospital, the method described by Gandon et al (18,19,24) is used to detect and quantify iron overload. Gradient-echo (GRE) sequences with T2* weighting and progressively longer echo
Figure 3. GRE T2*-weighted MR imaging performed in a dedicated study to investigate iron overload. (a) On an axial image of a healthy subject, the liver is hyperin-tense compared with paraspinal musculature. (b) Axial image of a subject with slight iron overload demonstrates a mild decrease in the signal intensity of the liver and spleen (darker than the paraspinal musculature). (c) Ax-ial image of a patient with severe iron overload demon-strates accentuated decrease in the liver signal intensity.
TeachingPoint

1580 October Special Issue 2009 radiographics.rsna.org
Figure 5. Secondary hemochromatosis and reticu-loendothelial pattern of iron overload. Axial GRE T2*-weighted MR image shows that the liver, spleen, and bone marrow demonstrate decreased signal intensity. The pancreas (arrow) has normal signal intensity.
Figure 4. Treatment follow-up of a patient with primary hemochromatosis. (a) Axial GRE T2*-weighted MR im-age shows the liver hypointensity that is due to iron overload. (b) Axial GRE T2*-weighted MR image obtained 1 year later, after phlebotomy, demonstrates a decrease in the liver hypointensity, which is caused by a decrease in the hepatic iron concentration.
of the complete loss of liver signal (12,18,19). Because of the capacity for quantitative and qualitative evaluation, MR imaging can be used noninvasively in the evolutionary and posttreat-ment control of hepatic iron overload, thereby avoiding multiple biopsies in these patients (19,23) (Fig 4).
Forms of Iron DepositionIn addition to the primary and secondary forms of hemochromatosis, iron overload can also be classified according to the deposition pat-terns. These patterns can help to differentiate among the possible causes of hemochromatosis (1,8,25–27) (Table 2).
Table 2 Patterns of Iron Deposition in Various Organs
Deposition Pattern Liver Spleen Bone Marrow Pancreas Kidney
Reticuloendothelial Yes Yes Yes No NoParenchymal Yes No No Yes* NoRenal No No No No YesMixed Yes Possibly Possibly Possibly Possibly
*Cannot be seen in a young patient with mild overload or in mild initial disease.
TeachingPoint

RG ■ Volume 29 • Number 6 Queiroz-Andrade et al 1581
Figure 7. Primary hemochromatosis and parenchy-mal pattern of iron overload. Axial GRE T2*-weighted MR image demonstrates that the liver and pancreas (arrow) show decreased signal intensity. The spleen and bone marrow have normal signal intensity.
Figure 6. Sickle cell disease. (a) Axial GRE T1-weighted in-phase MR image shows a decrease in the signal inten-sity of the spleen (arrow). Comparison with the GRE T1-weighted out-of-phase MR image (not shown) did not demonstrate the T2* effect, a finding consistent with calcium. (b) Axial nonenhanced CT image helps confirm that the MR appearance of the spleen is due to diffuse calcification (arrow) secondary to autosplenectomy.
Reticuloendo- thelial Deposition PatternIn iron overload secondary to multiple transfu-sions, deposition generally occurs in the cells of the reticuloendothelial system of the liver, spleen, and bone marrow. This type of accumulation is not associated with tissue damage (8,25).
The signal intensity of the spleen and bone marrow can be used to evaluate the type of deposition pattern because in two of the other forms of iron deposition (parenchymal and re-nal), we normally do not observe any effect on these structures (8,25,27) (Fig 5). One of the
diagnoses that is differentiated by the low signal intensity of the spleen is diffuse calcification secondary to autosplenectomy, which can be observed in cases of sickle cell anemia (Fig 6). In the reticuloendothelial deposition pattern, the signal intensity of the pancreas is generally preserved, except when the volume of blood infused goes beyond the storage capacity of the reticuloendothelial system, leading to parenchy-mal deposition (1,25,28).
Parenchymal Deposition PatternThis pattern occurs secondary to increased iron absorption. The pattern is observed mainly in pa-tients with primary hemochromatosis or in cases of chronic anemia with inefficient erythropoiesis (thalassemia syndromes, congenital dyserythro-poietic anemias, and sideroblastic anemias).
The excess iron accumulates initially in the periportal hepatocytes and then spreads to the rest of the liver, the pancreas, and the thyroid and leads to tissue damage (1,24–26). In this pattern of deposition, decreased signal intensity is observed in the liver and the pancreas, while in the spleen and the bone marrow, signal inten-sity is preserved (Fig 7).
In advanced forms of the disease, the myocar-dium and the hypophysis are affected. In young patients with mild overload, the signal intensity of the pancreas can be preserved (8,25).

1582 October Special Issue 2009 radiographics.rsna.org
Figures 8, 9. (8) Iron overload and cirrhosis. Axial fat-saturated fast spin-echo (SE) T2-weighted MR image shows nodularity of the liver outline, morphologic changes suggestive of cirrhosis, and a low signal intensity of the liver that is due to iron overload. (9) Iron overload and hepatocellular carcinoma. (a) Axial fast SE T2-weighted MR image demonstrates low signal intensity of the liver that is due to iron overload and also shows a slightly hyperin-tense nodule (arrow). (b, c) On axial dynamic fat-saturated GRE T1-weighted MR images obtained after adminis-tration of a gadolinium-based contrast agent, the nodule shows enhancement in the arterial phase (arrow in b) and washout in the portal venous phase (arrow in c). The findings from histologic analysis disclosed that the nodule was a hepatocellular carcinoma.
In addition to the decreased signal intensity of the liver, hepatomegaly, fibrosis, and cirrhosis are observed in advanced cases (1,8,25) (Fig 8). Investigators have also shown a considerable in-
crease in the rate of occurrence of hepatocellular carcinoma in these patients (1,29,30) (Fig 9).
Iron deposition in the heart may cause car-diomyopathy, pericarditis, and arrhythmias. Ac-cumulation of iron in the endocrine system may lead to diabetes mellitus, hypopituitarism, hypo-gonadism, and hypoparathyroidism (1,28).

RG ■ Volume 29 • Number 6 Queiroz-Andrade et al 1583
Figure 10. Intravascular hemolysis and iron deposition in the renal cortex. (a) Axial GRE T1-weighted MR image shows that the renal cortex is hypointense, with lower signal intensity than that of the medulla, causing reversed corticomedullary differentiation. (b) Coronal single-shot fast SE T2-weighted MR image shows the accentuated low signal intensity of the renal cortex.
observe patients with paroxysmal nocturnal he-moglobinuria or patients with anemias that are accompanied by intravascular hemolysis receiving multiple transfusions, resulting in renal and re-ticuloendothelial deposition (8,31,32).
Iron Overload and Other Storage Diseases
The association between deposition of fat and de-position of iron in the hepatic parenchyma is not infrequent. This association can make diagnosis challenging if the correct concepts and sequences are not used. The decrease in signal intensity occurs on the out-of-phase images in steatosis, while the decrease occurs on the in-phase images in hemochromatosis (21,38).
With CT, the diagnosis of combined steatosis and hemochromatosis can be difficult. Unlike CT, the MR imaging sequences used for quanti-fication of hepatic iron are not influenced by ste-atosis because with the selected echo times, the water and fat spins are in phase.
Renal Deposition PatternIron deposition in the kidneys is only seen in cases of intravascular hemolysis caused by mechani-cal stress in patients with heart valves, in patients with paroxysmal nocturnal hemoglobinuria, or in hemolytic crises of sickle cell disease (8,31–34). In these cases, hemosiderin is deposited in the proximal convoluted tubules, promoting inversion of the signal intensity of the renal cortex, which is hypointense in relation to the medulla on the T1-weighted images and demonstrates an accentuated decrease in the cortical signal intensity on the T2-weighted images (32–34). Despite the dramatic appearance of this type of accumulation, it is not believed that this accumulation affects renal func-tion (8,31,35) (Fig 10).
Mixed Deposition PatternsIn patients with advanced forms of the disease, an atypical distribution pattern of iron overload is observed (8,25,36,37). Patients with chronic anemias caused by ineffective erythropoiesis may require multiple transfusions, which can result in parenchymal and reticuloendothelial deposi-tion patterns (25,28). Similarly, it is possible to

1584 October Special Issue 2009 radiographics.rsna.org
parenchyma. Because of the decrease in the he-patic parenchymal signal intensity that is due to iron overload, some lesions may appear with relatively high signal intensity on the T2-weighted images, a finding that is generally seen in benign lesions (cysts and hemangiomas) (39). Thus, par-ticularly in this situation, the use of intravenous contrast agent injection is crucial for lesion char-acterization (Fig 13).
Figure 11. Diffuse form of hemochromatosis and steatosis. (a, b) In comparison with the axial GRE T1-weighted in-phase image (a), the axial GRE T1-weighted out-of-phase MR image (b) shows a decrease in the liver signal intensity that is due to steatosis. (c) Axial GRE T2*-weighted MR image demonstrates decreased liver signal intensity that is lower than that of the paraspinal musculature; the decrease is due to iron overload.
The diffuse forms of hemochromatosis and steatosis generally do not cause greater difficulties for diagnosis (Fig 11). However, the nodular form can simulate true lesions. These pseudonodules result from areas of focal steatosis or from areas of hepatic parenchyma that are spared from steatosis or iron overload. To differentiate these pseudonod-ules from true nodules, we need to observe the variations in signal intensity on the in-phase and out-of-phase images, together with the enhance-ment pattern, which should be similar to that of the normal liver, and the lack of expansive effect and the absence of vascular distortion (Fig 12).
Iron Overload and Hepatic Focal Lesions
Great care should be taken when evaluating the signal of focal lesions in relation to the hepatic

RG ■ Volume 29 • Number 6 Queiroz-Andrade et al 1585
Figure 12. Pseudonodules (arrows) and iron overload. (a) Ax- ial GRE T2-weighted MR image demonstrates the low signal in- tensity of the liver that is due to iron overload and also shows nod-ules without expansive effect or vascular distortion. (b, c) Axial GRE T1-weighted out-of-phase MR image (b) demonstrates a decrease in the signal intensity of the nodules compared with the signal intensity of the nodules on the axial GRE T1-weighted in-phase MR image (c), a finding suggestive of focal steatosis and spared areas of hemochromatosis. (d) Axial gadolinium-enhanced fat-saturated GRE T1-weighted MR image shows no different enhancement. (e) Ultrasonographic image demonstrates that this area is hyperechoic.

1586 October Special Issue 2009 radiographics.rsna.org
Figure 13. Focal hepatic lesion in iron overload. (a) Axial fat-saturated fast SE T2-weighted MR image shows low signal intensity of the liver that is due to iron overload and also shows relatively high signal intensity of the lesion (ar-row), simulating a benign lesion. (b) Axial gadolinium-enhanced fat-saturated GRE T1-weighted MR image shows peripheral enhancement of the lesion (arrow). The findings from histologic analysis showed that the lesion was a colon cancer metastasis.
Figure 14. Colon cancer, liver metastases, and iron overload in a young male patient. (a) Axial fast SE fat-saturated T2-weighted MR image demonstrates low signal intensity of the liver and secondary hyperintense liver nod-ules. (b) Axial GRE T1-weighted in-phase MR image dem-onstrates hypointense secondary liver nodules and slight iron overload. (c) Coronal single-shot fast SE T2-weighted MR image shows a tumor (arrow) of the descending colon.

RG ■ Volume 29 • Number 6 Queiroz-Andrade et al 1587
Hemochroma- tosis and Neoplasias
Although no consensus exists in the literature, some investigators have demonstrated links among iron overload, the genes of hemochroma-tosis, and neoplasias other than hepatocellular carcinoma, particularly those of the colon (ad-enoma and adenocarcinoma). Also, an increased rate of occurrence of these tumors is seen in a younger age group (Fig 14) (40–42).
Other Findings Associ- ated with Iron Overload
Patients with anemias that are accompanied by inefficient erythropoiesis, as well as iron overload signal intensity, can also show other evidence of long-term anemia, such as foci of extramedul-lary erythropoiesis in the paravertebral regions and, less frequently, in the hepatic parenchyma, leading to a differential diagnosis with neoplastic lesions (Fig 15).
Some types of anemia, such as Fanconi anemia, benefit from treatment with steroids (oxymetholone, methyltestosterone, or danazol) to stimulate erythropoietin production. However, these drugs can induce the development of hepatic
Figure 15. Iron overload secondary to thalassemia and extramedullary erythropoiesis. (a, b) Axial GRE T1-weighted in-phase MR image (a) shows a decrease in the signal intensity of the liver, compared with the axial GRE T1-weighted out-of-phase MR image (b), and also shows hepatic nodules (arrow). (c) Axial gadolinium-enhanced fat-saturated GRE T1-weighted MR image demonstrates a paravertebral mass (arrow). The findings from histologic analysis disclosed extramedullary eryth-ropoiesis, both in the liver and the paravertebral region.
tumors, including hepatocellular carcinoma and adenoma (43), as well as peliosis hepatis (44–46)
TeachingPoint

1588 October Special Issue 2009 radiographics.rsna.org
Figure 16. Fanconi anemia treated with oxymetholone. Axial fat-saturated fast SE T2-weighted MR image (a) and gadolinium-enhanced fat-saturated GRE T1-weighted MR image (b) show low signal intensity of the liver and spleen that is due to secondary hemochromatosis. Multiple small (1–3-mm) blood-filled lacunar spaces seen in a are suggestive of peliosis hepatis. Multiple enhancing nodules (arrows) seen in b were confirmed as adenomas at percutaneous biopsy.
(Fig 16). Suspension of administration of those drugs can lead to regression of the lesions.
ConclusionsIron overload is a relatively common disease with various causes. Making a clinical diagnosis is often difficult. Knowledge of the imaging find-ings, the patterns of distribution, and associated diseases can facilitate diagnosis. MR imaging has a fundamental role because it can contribute, in a noninvasive way, to the diagnosis, the estimation of liver iron concentration, and the follow-up of these patients.
References 1. Andrews NC. Disorders of iron metabolism. N Engl
J Med 1999;341:1986–1995. 2. Siah CW, Ombiga J, Adams LA, Trinder D, Olynyk
JK. Normal iron metabolism and the pathophysiol-ogy of iron overload disorders. Clin Biochem Rev 2006;27:5–16.
3. Pietrangelo A. Haemochromatosis. Gut 2003;52 (suppl 2):ii23–ii30.
4. Jensen PS. Hemochromatosis: a disease often silent but not invisible. AJR Am J Roentgenol 1976;126: 343–351.
5. Adams PC, Reboussin DM, Barton JC, et al. Hemochromatosis and iron overload screening in a racially diverse population. N Engl J Med 2005;352: 1769–1778.
6. Njajou OT, Alizadeh BZ, van Duijn CM. Is genetic screening for hemochromatosis worthwhile? Eur J Epidemiol 2004;19:101–108.
7. Merryweather-Clarke AT, Pointon JJ, Shearman JD, Robson KJ. Global prevalence of putative haemo-chromatosis mutation. J Med Genet 1997;34:275– 278.
8. Siegelman ES, Mitchel DG, Semelka RC. Abdomi-nal iron deposition: metabolism, MR findings, and clinical importance. Radiology 1996;199:13–22.
9. Adams P, Brissot P, Powell LW. EASL International Consensus Conference on Haemochromatosis. J Hepatol 2000;33:485–504.
10. Brissot P, Bourel M, Herry D, et al. Assessment of liver iron content in 271 patients: a reevaluation of direct and indirect methods. Gastroenterology 1981; 80:557–565.
11. Crawford DH, Jazwinska EC, Cullen LM, Powell LW. Expression of HLA-linked hemochromatosis in subjects homozygous or heterozygous for the C28Y mutation. Gastroenterology 1998;114:1003–1008.
12. Alústiza JM, Artetxe J, Castiella A, et al. MR quan-tification of hepatic iron concentration. Radiology 2004;230:479–484.
13. Guyader D, Gandon Y, Deugnier Y, et al. Evaluation of computed tomography in the assessment of liver iron overload: a study of 46 cases of idiopathic hemo-chromatosis. Gastroenterology 1989;97:737–743.

RG ■ Volume 29 • Number 6 Queiroz-Andrade et al 1589
tion in the cirrhotic liver at MR imaging. Radiology 1999;212:235–240.
31. Roubidoux MA. MR imaging of hemorrhage and iron deposition in the kidney. RadioGraphics 1994; 14:1033–1044.
32. Jeong JY, Kim SH, Lee HJ, Sim JS. Atypical low-sig-nal-intensity renal parenchyma: causes and patterns. RadioGraphics 2002;22:833–846.
33. Lee JW, Kim SH, Yoon CJ. Hemosiderin deposition on the renal cortex by mechanical hemolysis due to malfunctioning prosthetic cardiac valve: report of MR findings in two cases. J Comput Assist Tomogr 1999;23:445–447.
34. Roubidoux MA. MR of kidney, liver, and spleen in paroxysmal nocturnal hemoglobinuria. Abdom Im-aging 1994;19:168–173.
35. Leonardi P, Ruol A. Renal hemosiderosis in the hemolytic anemias: diagnosis by means of needle biopsy. Blood 1960;16:1029–1038.
36. Stark DD. Hepatic iron overload: paramagnetic pa-thology. Radiology 1991;179:333–335.
37. Yoon DY, Choi BI, Han JK, Han MC, Park MO, Suh SJ. MR findings of secondary hemochromato-sis: transfusional vs erythropoietic. J Comput Assist Tomogr 1994;18:416–419.
38. Levenson H, Greensite F, Hoefs J, et al. Fatty infil- tration of the liver: quantification with phase-contrast MR imaging at 1.5 T vs biopsy. AJR Am J Roent-genol 1991;156:307–312.
39. Horton KM, Bluemke DA, Hruban RH, Soyer P, Fishman EK. CT and MR imaging of benign hepatic and biliary tumors. RadioGraphics 1999;19:431–451.
40. Chan AT, Ma J, Tranah GJ, et al. Hemochromatosis gene mutations, body iron stores, dietary iron, and risk of colorectal adenoma in women. J Natl Cancer Inst 2005;97:917–926.
41. Shaheen NJ, Silverman LM, Keku T, et al. Associa-tion between hemochromatosis (HFE) gene muta-tion carrier status and the risk of colon cancer. J Natl Cancer Inst 2003;95:154–159.
42. Stevens RG, Jones DY, Micozzi MS, Taylor PR. Body iron stores and the risk of cancer. N Engl J Med 1988;319:1047–1052.
43. Velazquez I, Alter BP. Androgens and liver tumors: Fanconi’s anemia and non-Fanconi’s conditions. Am J Hematol 2004;77:257–267.
44. Maves CK, Caron KH, Bisset GS 3rd, et al. Splenic and hepatic peliosis: MR findings. AJR Am J Roent-genol 1992;158:75–76.
45. Elsayes KM, Narra VR, Yin Y, Mukundan G, Lammle M, Brown JJ. Focal hepatic lesions: diag-nostic value of enhancement pattern approach with contrast-enhanced 3D gradient-echo MR imaging. RadioGraphics 2005;25:1299–1320.
46. Bagheri SA, Boyer JL. Peliosis hepatis associated with androgenic-anabolic steroid therapy: a severe form of hepatic injury. Ann Intern Med 1974;81: 610–618.
14. Howard JM, Ghent CN, Carey LS, Flanagan PR, Valberg LS. Diagnostic efficacy of hepatic computed tomography in the detection of body iron overload. Gastroenterology 1983;84:209–215.
15. Goldman IS, Winkler ML, Raper SE, et al. Increased hepatic density and phospholipidosis due to amio-darone. AJR Am J Roentgenol 1985;144:541–546.
16. De Maria M, De Simone G, Laconi A, Mercadante G, Pavone P, Rossi P. Gold storage in the liver: ap-pearance on CT scans. Radiology 1986;159:355–356.
17. Gomori JM, Horev G, Tamary H, et al. Hepatic iron overload: quantitative MR imaging. Radiology 1991; 179:367–369.
18. Gandon Y, Guyader D, Heautot JF, et al. Hemo-chromatosis: diagnosis and quantification of liver iron with gradient-echo MR imaging. Radiology 1994;193:533–538.
19. Gandon Y, Olivié D, Guyader D, et al. Non-invasive assessment of hepatic iron stores by MRI. Lancet 2004;363:357–362.
20. Alústiza JM, Castiella A, De Juan MD, Emparanza JI, Artetxe J, Uranga M. Iron overload in the liver diagnostic and quantification. Eur J Radiol 2007; 61:499–506.
21. Westphalen AC, Qayyum A, Yeh BM, et al. Liver fat: effect of hepatic iron deposition on evaluation with opposed-phase MR imaging. Radiology 2007;242: 450–455.
22. Ernst O, Sergent G, Bonvarlet P, Canva-Oelcambre V, Paris JC, L’Hermin C. Hepatic iron overload: di-agnosis and quantification with MR imaging. AJR Am J Roentgenol 1997;168:1205–1208.
23. Bonkovsky HL, Rubin RB, Cable EE, Davidoff A, Rijcken TH, Stark DD. Hepatic iron concentration: noninvasive estimation by means of MR imaging. Radiology 1999;212:227–234.
24. Gandon Y. Iron, liver and MRI. University of Rennes Web site. http://www.radio.univ-rennes1.fr /Sources/EN/Hemo.html. Updated June 10, 2001. Accessed January 25, 2009.
25. Siegelman ES, Mitchel DG, Rubin R, et al. Paren-chymal versus reticuloendothelial iron overload in the liver: distinction with MR imaging. Radiology 1991;179:361–366.
26. Siegelman ES, Mitchell RG, Outwater E, Munoz SJ, Rubin R. Idiopathic hemochromatosis: MR imaging findings in cirrhotic and precirrhotic patients. Radi-ology 1993;188:637–641.
27. Ben Salem D, Cercueil JP, Ricolfi F, Krausé D. Case 75: erythropoietic hemochromatosis. Radiology 2004;233:116–119.
28. Midiri M, Lo Casto A, Sparacia G, et al. MR imag-ing of pancreatic changes in patients with transfu-sion-dependent beta-thalassemia major. AJR Am J Roentgenol 1999;173:187–192.
29. Hann HW, Kim CY, London WT, Blumberg BS. Increased serum ferritin in chronic liver disease: a risk factor for primary hepatocellular carcinoma. Int J Cancer 1989;43:376–379.
30. Ito K, Mitchell DG, Gabata T, et al. Hepatocellular carcinoma: association with increased iron deposi-

RG Volume 29 • October Special Issue 2009 Queiroz-Andade et al
MR Imaging Findings of Iron Overload Marcony Queiroz-Andrade, MD, et al
Page 1578 MR imaging is the best noninvasive method for measuring the level of iron in the liver for the purposes of confirming the diagnosis, determining the severity, and monitoring therapy with high sensitivity, specificity, and positive and negative predictive values (12,18–20). The accumulation of iron ions in the tissues, because of the superparamagnetic properties of the ions, causes local distortion in the magnetic fields and relaxation of the spins, which results in shortening of the longitudinal relaxation time (T1), the transverse relaxation time (T2), and particularly the transverse relaxation time as affected by magnetic field inhomogeneity (T2*). This effect causes a loss of signal intensity in the affected organs that is proportional to the iron deposition (17,21). Page 1578 In the general protocol applied to an abdominal study, it is not possible to estimate the hepatic iron concentration, although most of the time, it is possible to diagnose iron overload. This can be done by using “dual-sequence” (gradient in and out of phase) MR imaging, which demonstrates decreased signal intensity in the affected tissues on the in-phase images compared with the out-of-phase images. That effect is the opposite of the effect observed in patients with steatosis (Fig 2). This occurs because the echo time of the in-phase sequence is usually higher than that of the out-of-phase sequence; therefore, the in-phase pulse sequence is more sensitive to iron deposits because of the increased T2* effect (21). Page 1579 The results of examination of unaffected subjects show that the hepatic parenchyma demonstrates higher signal intensity than that of the paraspinal musculature with all sequences. Slight to moderate iron overload is better identified and evaluated on the GRE images obtained with longer echo times, which demonstrate a decrease in the signal intensity of the liver parenchyma (Fig 3). Page 1580 In addition to the primary and secondary forms of hemochromatosis, iron overload can also be classified according to the deposition patterns. These patterns can help to differentiate among the possible causes of hemochromatosis (1,8,25–27) (Table 2). Page 1587 Patients with anemias that are accompanied by inefficient erythropoiesis, as well as iron overload signal intensity, can also show other evidence of long-term anemia, such as foci of extramedullary erythropoiesis in the paravertebral regions and, less frequently, in the hepatic parenchyma, leading to a differential diagnosis with neoplastic lesions (Fig 15). Some types of anemia, such as Fanconi anemia, benefit from treatment with steroids (oxymetholone, methyltestosterone, or danazol) to stimulate erythropoietin production. However, these drugs can induce the development of hepatic tumors, including hepatocellular carcinoma and adenoma (43), as well as peliosis hepatis (44–46).
RadioGraphics 2009; 29:1575–1589 • Published online 10.1148/rg.296095511 • Content Codes: