Embed Size (px)
Citation preview

The Egyptian Journal of Radiology and Nuclear Medicine (2014) 45, 735–744
Egyptian Society of Radiology and Nuclear Medicine
The Egyptian Journal of Radiology andNuclearMedicine
www.elsevier.com/locate/ejrnmwww.sciencedirect.com
ORIGINAL ARTICLE
MRI evaluation of TMJ internal derangement:
Degree of anterior disc displacement correlated
with other TMJ soft tissue and osseous
abnormalities
* Corresponding author. Tel.: +20 1006892117; fax: +20 934602963.E-mail addresses: [email protected] (N.M.A. Hasan), tarekf-
[email protected] (T.E.F. Abdelrahman).
Peer review under responsibility of Egyptian Society of Radiology and
Nuclear Medicine.
0378-603X � 2014 Production and hosting by Elsevier B.V. on behalf of Egyptian Society of Radiology and Nuclear Medicine.
http://dx.doi.org/10.1016/j.ejrnm.2014.03.013Open access under CC BY-NC-ND license.
Nahla Mohamed Ali Hasan a,*, Tarek Elsayed Ftohy Abdelrahman b
a Department of Diagnostic Radiology, Sohag Faculty of Medicine, Sohag University, Egyptb Department of Maxillofacial Surgery. Sohag Faculty of Medicine, Sohag University, Egypt
Received 12 January 2014; accepted 24 March 2014Available online 21 April 2014
KEYWORDS
MRI;
TMJ dysfunction;
Anterior disc displacement
Abstract Objective: To evaluate the relationship between anterior disc displacement (ADD)
degree and other temporomandibular joint (TMJ) soft tissues and osseous abnormalities in symp-
tomatic TMJ dysfunction based on magnetic resonance imaging findings.
Patients and methods: MR images of 106 TMJs in 53 patients, presented with symptomatic TMJ
dysfunction were included. Degree of ADD was detected and its relationship to joint effusion, ret-
rodiscal layer integrity, thickness of lateral pterygoid muscle (LPM) attachments, degenerative
changes and condylar position and translation as well as clinical manifestations was studied.
Results: Compared with normal disc position, risk of joint effusion and degenerative changes were
significantly increased with increased degree of ADD (p< 0.05). LPM attachment thickening and
retrodiscal layer abnormalities are significantly associated with an advanced degree of ADD
(p< 0.05). Risk of ADD is significantly increased with posterior position of the condyle within
the fossa.
Conclusion: There is a direct relationship between the ADD degree and other TMJ soft tissues and
bone abnormalities as well as the severity of clinical manifestations, so early MRI detection and
reporting of ADD degree and other MRI findings might help clinicians in full assessment and deter-
mining strategy of management of TMJ dysfunction.� 2014 Production and hosting by Elsevier B.V. on behalf of Egyptian Society of Radiology and Nuclear
Medicine. Open access under CC BY-NC-ND license.
1. Introduction
Temporomandibular joint (TMJ) dysfunction is a commonproblem and affects up to one-third of all adults at some stage
in their life (1). The most frequent cause of TMJ dysfunction isinternal derangement which refers to an alteration in thenormal pathways of motion of the TMJ that largely involves

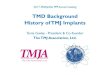
Fig. 1a Sagittal oblique spin-echo proton-density–weighted MR
image (closed-mouth position) shows the disc in its normal
position between the condyle and temporal bone and centred in
the intermediate zone (arrow).
736 N.M.A. Hasan, T.E.F. Abdelrahman
the function of the articular disc, therefore, these alterationshave been also referred to as disc derangement (2). Anteriordisc displacement (ADD) is one of the major findings in
TMJ internal derangement. Anterior disc displacement withreduction (ADDWR) and anterior disc displacement withoutreduction (ADDWOR) are the two most common forms of
TMJ disc displacement (3), while posterior displacement is rare(4). State-of-the-art magnetic resonance imaging (MRI) tech-niques allow analysis of disc position in both sagittal and coro-
nal planes, dynamic assessment of condylar translation anddisc movement during opening and closing the mouth (5).Other MRI signs that can suggest a diagnosis of TMJ dysfunc-tion include thickening of lateral pterygoid muscle (LPM)
attachment, rupture of retrodiscal layers or joint effusion (6).Relationship between ADD and joint effusion and degener-
ative changes have been discussed frequently in previous stud-
ies (7–9), while ADD relationship to LPM thickness andretrodiscal layer integrity as well as condylar position withinthe glenoid fossa and condylar translation has not been fre-
quently covered.The purpose of this study was to evaluate ADD in cases of
symptomatic TMJ dysfunction and to investigate the relation-
ship between its degree and other TMJ soft tissues and osseousabnormalities. Also in this study we tried to assess the correla-tion between the degree of disc displacement and the clinicalmanifestations of the patients.
2. Patients and methods
This prospective study included MR images of 106 TMJs in 53
patients (17 males and 36 females, mean age was 25.9 years)were referred to the MRI unit in Diagnostic RadiologyDepartment at a teaching University Hospital from August
2010 to October 2012, presented by symptomatic unilateralor bilateral TMJ dysfunction (TMJ clicking, TMJ locking,restricted movement of the jaw or pain in the TMJ region).
Patients with TMJ fractures, or systemic diseases knownto affect the TMJ, such as rheumatoid arthritis wereexcluded. Also patients with posterior disc displacement were
excluded.
2.1. MRI technique
All MRIs had been obtained by using 1.5-T machine (Philips-
Acheiva), Netherlands using TMJ surface coli. Pulse sequencesincluded sagittal oblique T2-weighted images (T2WI) and pro-ton density (PD) weighted images in close- and open-mouth
positions (TR = 3000/3500 ms, TE = 120/30 ms respectively)and coronal PD weighted images in closed mouth position(TR= 3500 ms, TE = 30 ms). Section thickness was 2 mm
with a 0.2 mm intersection gap. The field of view was 12 cmfor sagittal images and 18 cm for coronal images.
2.2. Image analysis
2.2.1. ADD
The 1st step was evaluation of the disc location in both closed-
and open-mouth positions relative to the condyle and articulareminence.
ADD was assessed in sagittal oblique plane in both closed-
and open-mouth positions and coronal plane in closed mouth
position. According to the degree of ADD, our series was clas-sified into 4 categories.
2.2.2. Category 0
Normal disc position (the thin intermediate zone interposedbetween the condyle and the adjacent temporal bone, wher-ever the two bones are most closely apposed to one another
regardless of whether or not the mouth was open or closed)(Fig. 1) (10). Category I: Partial anterior disc displacementwith reduction (PADDWR); disc displaced anteriorly in
closed mouth up to the posterior band interposed betweenthe two most closely apposed cortical bone surfaces of thecondyle and eminence with disc reduction to normal loca-
tion in open mouth position (Fig. 2). Category II: Partialanterior disc displacement without reduction (PADDWOR);disc displaced anteriorly in closed mouth as described in cat-
egory I, that maintained displaced with mouth opening(Fig. 3). Category III: Complete anterior disc displacementwith reduction (CADDWR); disc displaced anteriorly inclosed mouth up to no disc substance interposed between
the two most closely apposed cortical bone surfaces of thecondyle and eminence with disc reduction to normal loca-tion in open mouth position (Fig. 4). Category IV: Complete
anterior disc displacement without reduction (CADDWOR);disc displaced anteriorly in closed mouth as described in cat-egory III, that maintained displaced with mouth opening
(Fig. 5).
2.2.3. Disc morphology
Normal disc morphology is biconcave structure in sagittal
images with homogenous low signal intensity. Disc deformitiesincluding thickening, irregularity, flattening, folded, degenera-tion, and perforation were reported (Fig. 6).
2.2.4. Joint effusion
Joint effusion was assessed on T2WI manifesting as area ofhyperintensity, which was divided into 3 grades (11). Grade

Fig. 1b Sagittal oblique spin-echo proton-density–weighted MR
image (open-mouth position) shows that the disc has maintained
its normal position during condylar movement (arrow).
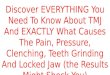
Fig. 2a Sagittal oblique spin-echo proton-density–weighted MR
image (closed-mouth position) shows partial anterior disc dis-
placement with intermediate signal of degeneration (large arrow)
and anterior osteophyte of the condyle (small arrow).
Fig. 2b Sagittal oblique spin-echo proton-density–weighted MR
image (open-mouth position) shows that the disc has maintained
its normal position during condylar movement (arrow).
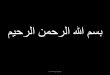
Fig. 3a Sagittal oblique spin-echo proton-density–weighted MR
image (closed-mouth position) shows (flattened shape) partial
anterior disc displacement (arrow).
Fig. 3b Sagittal oblique spin-echo proton-density–weighted MR
image (open-mouth position) shows that the disc remains partially
displaced from its normal location (arrow), associated with Grade
I joint effusion.
MRI evaluation of TMJ internal derangement 737
0: None (no bright signal in either joint space). Grade I: Slighteffusion (a bright signal in either joint space that conforms to
the contours of the disc, fossa/articular eminence, and or con-dyle). Grade II: Frank effusion (a bright signal in either jointspace that extends beyond the osseous contours of fossa/artic-
ular eminence, and or condyle and has a convex configurationin the anterior or posterior recesses.
2.2.5. Degenerative changes
TMJ osteoarthritis was diagnosed when more than one of thefollowing changes were noted; fattening of the articular sur-face, subcortical sclerosis or cyst, surface erosion, osteophytes,
and generalized sclerosis for the condylar head and flatteningof the articular eminence, subcortical sclerosis, and surfaceerosions for the fossa (11).

Fig. 4a Sagittal oblique spin-echo proton-density–weighted MR
image (closed-mouth position) shows (thickened shape) complete
anterior disc displacement (arrow) and associated joint effusion in
both upper and lower joint recesses.
Fig. 4b Sagittal oblique spin-echo proton-density–weighted MR
image (open-mouth position) shows that the disc (arrow) has
maintained its normal position during condylar movement.
Fig. 5a Sagittal oblique spin-echo proton-density–weighted MR
image (closed-mouth position) shows complete anterior disc
displacement (arrow).
Fig. 5b Sagittal oblique spin-echo proton-density–weighted MR
image (open-mouth position) shows that the disc remains
displaced from its normal location (arrow) and cortical erosion
of the condyle (small arrow). Note the marked restricted mobility
of the condyle apex where it translates to less than the apex of the
articular eminence.
738 N.M.A. Hasan, T.E.F. Abdelrahman
2.2.6. Position of the condyle
Position of the condylar head in relation to the articular fossawas assessed in PD sagittal oblique images in closed mouthposition and was classified as concentric, anterior or posterior
position.
2.2.7. Translation of the condyle
Condyle translation was assessed in PD sagittal oblique imagesin open mouth position as follows; apex of the condyle trans-lates to less than the apex of the articular eminence, apex of thecondyle translates to the apex of the articular eminence, which
is a position many authors consider normal, or apex of thecondyle translates beyond the apex of the articular eminence(11) (Fig. 7).
2.2.8. Thickness of LPM attachments
Thickness of LPM attachments was assessed in closed mouthsagittal oblique PD weighted images and compared with theaverage thickness of LPM attachments in asymptomatic nor-
mal TMJ included in this study (Fig. 8).Integrity and thickness of retrodiscal layers: Integrity of
both superior and inferior retrodiscal layers was assessed in
open mouth sagittal oblique T2-weighted images. Images wereevaluated for thinning, thickening or rupture of either of supe-rior or inferior layer (Fig. 9).
2.2.9. Clinical evaluation
We divided patients into 3 groups according severity of clinicalmanifestation and we found that: Group I. EARLY cases who
presented with painless clicking with No restricted motion.Group II. INTERMEDIATE group who presented with

Fig. 6a Sagittal oblique spin-echo proton-density–weighted MR
images (closed-mouth position) show abnormal disc morphology:
(a) shows intermediate signal of degeneration within the disc
(arrow).
Fig. 6b Shows fattened, irregular disc with complete anterior
displacement (arrow) associated with osteoarthritic changes and
joint effusion.
Fig. 6c Shows ballooning of posterior disc band with complete
anterior displacement (arrow) associated with osteoarthritic
changes and joint effusion.
Fig. 6d Shows perforated disc with complete anterior displace-
ment (arrow) associated with osteoarthritic changes (cortical
erosion and irregular articular surface of the condyle and small
anterior osteophyte)
Fig. 7a Sagittal oblique spin-echo proton-density–weighted MR
images (open-mouth position) show the translation of the condyle
in relation to the articular eminence (a) the apex of the condyle
(arrow head) translates to the apex of the articular eminence
(asterisk), which is considered normal.
Fig. 7b Shows complete anterior disc displacement without
reduction and restricted mobility of the condyle i.e., the apex of
the condyle (arrow head) translates to less than the apex of the
articular eminence (asterisk).
MRI evaluation of TMJ internal derangement 739

Fig. 7c Shows normal disc position with hypermobility of the
condyle i.e. the apex of the condyle (arrow head) translates beyond
the apex of the articular eminence (asterisk).
Fig. 8a Sagittal oblique spin-echo proton-density–weighted MR
image (closed-mouth position) shows normal disc position (large
arrow) and normal thickness of inferior LPM insertion (small
arrow).
Fig. 8b Sagittal oblique spin-echo proton-density–weighted MR
image (closed-mouth position) shows complete anterior disc
displacement (arrow) and thickened inferior LPM insertion (arrow
head), compared with (a).
Fig. 9a Sagittal oblique spin-echo proton-density–weighted MR
image (open-mouth position) shows normal intact superior (large
arrow) and inferior (small arrow) retrodiscal layers.
Fig. 9b Sagittal oblique T2-weighted MR image (open-mouth
position) shows thickening of superior retrodiscal layer (large
arrow) and normal inferior retrodiscal layer (small arrow).
740 N.M.A. Hasan, T.E.F. Abdelrahman
frequent pain, joint tenderness, headaches, locking restrictedmotion and painful chewing. Group III. LATE cases who pre-sented with trismus, joint crepitus and marked chronic pain.
Clinical manifestations were evaluated and registered andwere correlated to the degree of ADD in MRI.
2.2.10. Data analysis
Statistical analysis of the relationship between degree of ADDand other soft tissue and bone MRI findings was done usinglogistic regression analysis. Odds ratio with p-value <0.05
was considered significant and p-value <0.01 was consideredhighly significant.
3. Results
This study described a series of 106 TMJ in 53 patients, 17males and 36 females with male to female ratio 1:2.1. Their

Table 1 Basic clinical data.
No. of patients 53
Sex distribution No. (%)
Male 17 (32)
Female 36 (68)
Mean patient’s age (years) 25.9
No. of TMJ 106
Degree of ADD
Category 0 (normal disc position) 34 (32.1)
Category I (PADDWR) 37 (34.9)
Category II (PADDWOR) 5 (4.7)
Category III (CADDWR) 12 (11.3)
Category IV (CADDWOR) 18 (17)
TMJ, temporomandibular joint; PADDWR, partial anterior disc
displacement with reduction; PADDWOR, partial anterior disc
displacement without reduction; CADDWR, compete anterior disc
displacement with reduction; CADDWOR, complete anterior disc
displacement without reduction.
MRI evaluation of TMJ internal derangement 741
ages ranged between 19 and 43 years (mean age: 25.9 years). 34(32.1%) TMJs had normal disc position, while 72 (67.9%) had
ADD, Table 1.Disc deformity (thickening, irregularity, flattening) was
observed in 50% of joints with ADD, with increased frequency
with increasing degree of ADD, from 11% in PADDWR,reaching up to 100% in CADDWOR, while disc perforationwas reported only in 5 TMJs with complete ADD.
Table 2 Degree of ADD correlated to joint effusion grade and deg
Category 0 Category I
Joint effusion
Grade 0 29(85.3) 20(54.1)
Grade I 4(11.8) 10 (27)
Grade II 4 2 (5.9) 7 (18.9)
OR 4.9**
Degenerative changes No. (%)
Positive 10 (29.4) 16 (43.2)
Negative 24 (70.6) 21 (56.8)
OR 1.8
ADD, anterior disc displacement; OR, Odds ratio,* p< 0.05.** p< 0.01.
Table 3 Degree of ADD correlated to LPM and retrodiscal abnor
Category 0 Category I
LPM attachment
Normal 34 (100) 32 (86.5)
Thick – 5 (13.5)
Retrodiscal layers
Normal 34 (100) 37 (100)
Abnormal – –
Ruptured
Thin
Thick
ADD, anterior disc displacement; LPM, lateral pterygoid muscle.
Risk of joint effusion significantly increased with thechange of the disc position, from normal to ADDWR (oddsratio 4.9 for PADDWR and 5.8 for CADDWR) to ADD-
WOR (odds ratio 8.7 for PADDWOR and 9.1 for CADD-WOR). Risk of degenerative changes increased significantlyin joints with ADD compared to joints with normal disc posi-
tion, and increased in frequency with increasing degree ofADD. Compared to normal joints, joints with PADDWR,PADDWOR, CADDWR and CADDWOR had 1.8, 3.6, 4.8
and 6.2 odds ratio, respectively Table 2.Thickening of LPM attachment was significantly observed
with increasing frequency from PADDWR to PADDWORto CADDWR then decreased in CADDWOR, 13.5%, 20%,
41.7%, and 33.3%. respectively. Morphological changes of ret-rodiscal layers were most frequently observed in CADDWOR,followed by PADDWOR, then CADDWR, 88.9%, 60% and
33.3%, respectively Table 3.ADD was observed more frequently in joints with posterior
position of the condyle within the glenoid fossa in closed
mouth position rather than concentric condyle position; witha significantly increased frequency from 27% in joints withPADDWR (3.8 odds ratio) to 72.2% in joints with CADD-
WOR (16.2 odds ratio). Restricted mobility of the condyle inopen mouth (apex of the condyle translates to less than theapex of the articular eminence) was significantly observedmore frequently in CADDWR and CADDWOR while hyper-
mobility (apex of the condyle translates beyond the apex of thearticular eminence) was significantly more detected in PADD-WOR Table 4.
enerative changes.
Category II Category III Category IV
2 (40) 6 (50) 7(38.9)
2 (40) 3 (25) 3(16.7)
1 (20) 3 (25) 8 (44.4)
8.7** 5.8** 9.1**
3 (60) 8 (66.7) 13 (72.2)
2 (40) 4 (33.3) 5 (27.8)
3.6 4.8* 6.2**
malities.
Category II Category III Category IV
4 (80) 7 (58.3) 12 (66.7)
1 (20) 5 (41.7) 6 (33.3)
2(40) 8 (66.7) 2 (11.1)
1 (20) - 2 (11.1)
2 (40) - 11 (61.1)
4 (33.3) 3 (16.7)

Table 4 Degree of ADD correlated to condylar position and translation.
Category 0 Category I Category II Category III Category IV
Condylar position No. (%)
Concentric 31 (91.2) 27 (73) 2 (40) 5 (41.7) 7 (38.9)
Posterior 3 (8.8) 10 (27) 3 (60) 7 (58.3) 11 (61.1)
OR 3.8 15.5* 14.5** 16.2**
Condylar translation
Less than the apex – 2 (5.4) 1 (20) 3 (25) 11 (61.1).
To the apex 30 (88.2) 30 (81.1) 4 (80) 9 (75) 7 (38.9) -
Beyond the apex 4 (11.8) 5(13.5) - - -
ADD, anterior disc displacement; OR, Odds ratio.* p< 0.05.** p < 0.01.
742 N.M.A. Hasan, T.E.F. Abdelrahman
As regards the clinical classification; 74 (70%) out of 106TMJs were symptomatic and we founded a positive correlation
between the severity of their clinical manifestations and degreeof anterior disc displacement detected in MR images. Group I(39 joints, 53%) had normal disc position or PADDWR,Group II had PADDWOR or CADDWR (17 joints, 23%)
and Group III had CADDWOR (18 joints, 24%).On the other hand, 32 (30%) out of 106 TMJs were asymp-
tomatic, 29 joints of them had normal disc position while 3
joints had PADDWR.
4. Discussion
ADD is considered a major cause of TMJ internal derange-ment and subsequently TMJ dysfunction. MRI has beenreported to be 95% accurate in assessment of disc position
and 93% accurate in assessment of osseous changes (12).Many authors defined normal disc position in closed mouth
by location of the posterior band at the superior or 12 o’clock
position relative to the condyle and the disc position is abnor-mal if the angle between the posterior band and vertical orien-tation of the condyle exceeds 10� (angle of displacement)(13,14). However, according to this definition, disc displace-
ment is detected in about 33% of asymptomatic volunteers(15,16). So, in this study, for assessment of disc position, weused the intermediate zone as a point of reference, emphasizing
its interpretation between the condyle and the temporal bone,not taking into account the angle of displacement of the pos-terior band (10). In this study, ADD was classified into 4
grades according to degree of displacement in closed mouthand the presence or absence of reduction in open mouth andpartial ADDWR was detected in 9% of asymptomatic TMJs.
It is now generally accepted and understood that joint effu-sion occurs with disc displacement (17,18). Changes in thecomposition of the synovial fluid may increase the intra-artic-ular friction, leading to unstable disc motion (19), these bio-
chemical changes may also affect the joint lubrication andnutritional requirements of the articular surfaces (2).
Results of this study showed that joint effusion was
observed more frequently in joints with ADD compared tojoints with normal disc position, moreover, its incidence pro-portionally increased from about 5 times in PADDWR to
about 9 times in CADDWOR. Roh et al. (20) after studying254 patients, have also reported that the incidence of joint effu-
sion was nearly twice as likely when there was ADDWR com-pared to normal discs and more than four times as likely in the
presence of ADDWOR.On the other hand, we observed that about 15% of TMJ
with normal disc position showed joint effusion. Similar resultsobtained by Roh et al. in a study included 508 TMJs of 254
patients (20). This could be explained in two ways, first;according to the hypothesis that the presence of synovial fluidis normal in the joint in small amount. Suenaga et al. (21)
reported joint effusion in up to 9% of asymptomatic individu-als. The second way is considering joint effusion is indicative ofsynovial tissue response to an inflammatory stimulus in TMJ
with normally positioned disc (22).In this study, degenerative changes were more frequently
observed in TMJ with ADD than TMJ with normal disc posi-
tion with its increased incidence from about twice in PAD-DWR to about six times in CADDWOR. These results weresupported with those of previous studies that consideredADD as an aetiological factor of osteoarthritis and/or to be
associated with osteoarthritis (23–25).The role of LPM in normal TMJ function is still controver-
sial. Results of this study showed significant incidence of
hypertrophy of inferior LPM attachment in TMJ with internalderangement compared to joints with normal disc position andthere was a parallel increased inferior LPM thickness with
respect to disc displacement degree.This was in agreement with the results of Tomas et al. (6)
and was supported with the results of electromyographic stud-ies, that showed in cases of TMJ internal derangement, inferior
LPM may become hyperactive in specific positions to help sta-bilize and position the condyle and the disc (26).
Other previous studies have demonstrated morphologic and
pathologic changes in LPM in cases of TMJ with internalderangement (27,28).
Retrodiscal layers play an important role in normal disc
displacement. Results of this study showed a significant corre-lation between ADD degree and morphological changes of ret-rodiscal layers, either thickening, thinning or even rupture.
Thinning of retrodiscal layers was identified in TMJ withADD without reduction. This sign may be due to retrodiscallayer atrophy in chronic stages of internal derangement causedby decreased disc vascularity and fibrous transformation
due to continuous compression and shear (29). Thickeningof retrodiscal layers was less frequently reported in thisseries. Thickening of the posterior meniscal attachment

MRI evaluation of TMJ internal derangement 743
(pseudo-meniscus sign) was identified byManzione et al. (30) insome cases of TMJ with ADD and was explained as a type ofTMJ protective reaction and affected patients may be less
symptomatic than those who do not have this thickening.Tomas et al. (6) described rupture of superior retrodiscal
layer in 2 patients with severe non-reduced disc displacement
and suggested that it may produce significant disc instabilityand in our study, this sign was identified in 3 TMJ with non-reduced ADD, one had partial displacement and two had com-
plete displacement.The correlation between signs and symptoms of tempro-
mandibular joint disorders and condylar position is controver-sial (31,32). Compared to TMJ with normal disc position, the
present study founded a significant association between poster-ior condyle position within the glenoid fossa in closed mouthand ADD, but no significant differences between variable
degrees of displacement. This could be explained as condylarposition posterior to the normal position may lead to deterio-ration in the disc ligaments, TMJ ligament and the disc itself
(33).Limitation of condylar translation in open mouth was
observed in this series only in joints with ADD and signifi-
cantly more frequent in cases of CADDWOR followed byCADDWR, which could be explained as the anteriorly posi-tioned disc may act as a mechanical interference to the anteriortranslation of the condyle to its normal position at the apex of
the articular eminence in open mouth. A previous studyassessed the degree of mandibular mobility in patients with aclinical diagnosis of temporomandibular disorder and healthy
individuals and found a significant difference in the groups ofpatients with muscle disorders and disc displacement withreduction regarding mandibular mobility when compared with
the control group. Nevertheless, the measurements of the 2groups were within the clinically normal values established inthe diagnostic criteria for temporomandibular disorders
(RDC/TMD) (34).
5. Conclusion
ADD is a common finding in TMJ internal derangement. Theresults show a direct relationship between the degree of ADDand MRI findings of other TMJ soft tissues and bone abnor-malities as well as the severity of clinical manifestations, so
early MRI detection and reporting of ADD degree and otherMRI findings might help clinicians in full assessment anddetermining the strategy of management of TMJ dysfunction.
Conflict of interest
We have no conflict of interest to declare.
References
(1) Greene CS, Marbach JJ. Epidemiologic studies of mandibular
dysfunction. A critical review. J Prosthet Dent 1982;48:184–90.
(2) Molinari F, Manicone PF, Raffaelli L, Raffaelli R, Pirronti T,
Bonomo L. Temporomandibular joint soft-tissue pathology, I:
disc abnormalities. Semin Ultrasound CT MRI 2007;28:192–204.
(3) Bakke M, Moller E, Werdelin LM, Dalager T, Kitai N, Kreiborg
S. Treatment of severe temporomandibular joint clicking with
botulinum toxin in the lateral pterygoid muscle in two cases of
anterior disc displacement. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 2005;100:693–700.
(4) Okochi K, Ida M, Honda E, Kobayashi K, Kurabayashi T. MRI
and clinical findings of posterior disk displacement in the
temporomandibular joint. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 2008;105:644–8.
(5) Whyte AM, McNamara D, Rosenberg I. Magnetic resonance
imaging in the evaluation of temporomandibular joint disc
displacement––a review of 144 cases. Int J Oral Maxillofac Surg
2006;35:696–703.
(6) Tomas X, Pomes J, Berenguer J, Quinto L, Nicolau C, Mercader
JM, Castro V. MR imaging of temporomandibular joint dys-
function: a pictorial review. RadioGraphics 2006;26:765–81.
(7) Emshoff R, Rudisch A, Innerhofer K, Bosch R, Bertram S.
Temporomandibular joint internal derangement type III: rela-
tionship to magnetic resonance imaging findings of internal
derangement and osteoarthrosis. an intraindividual approach. Int
J Oral Maxillofac Surg 2001;30:390–6.
(8) Larheim TA, Katzberg RW, Westesson PL, Tallents RH, Moss
ME. MR evidence of temporomandibular joint fluid and condyle
marrow alterations: occurrence in asymptomatic volunteers and
symptomatic patients. Int J Oral Maxillofac Surg 2001;30:113–7.
(9) Segami N, Suzuki T, Sato J, Miyamaru M, Nishimura M,
Yoshimura H. Does joint effusion on T2 magnetic resonance
images reflect synovitis? Part 3. Comparison of histologic findings
of arthroscopically obtained synovium in internal derangements
of the temporomandibular joint. Oral Surg Oral Med Oral Pathol
Oral Radiol Endod 2003;95:761–6.
(10) Helms CA, Kaplan PA. Diagnostic imaging of the temporoman-
dibular joint: recommendations for use of the various techniques.
AJR Am J Roentgenol 1990;154:319–22.
(11) Ahmad M, Hollender L, Anderson Q, Kartha K, Ohrbach R,
Truelove EL, John MT, et al. Research diagnostic criteria for
temporomandibular disorders (RDC/TMD): development of
image analysis criteria and examiner reliability for image analysis.
Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;107:
844–60.
(12) Maizlin ZV, Nutiu N, Dent PB, Vos PM, Fenton DM, Kirby JM,
et al. Displacement of the temporomandibular joint disk: corre-
lation between clinical findings and MRI characteristics. J Can
Dent Assoc 2010;76:a3.
(13) Emshoff R, Gerhard S, Ennemoser T, Rudisch A. Magnetic
resonance imaging findings of internal derangement, osteoarthro-
sis, effusion, and bone marrow edema before and after perfor-
mance of arthrocentesis and hydraulic distension of the
temporomandibular joint. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 2006;101:784–90.
(14) Takebayashi S, Takama T, Okada S, Masuda G, Matsubara S.
MRI of the TMJ disc with intravenous administration of
gadopentetate dimeglumine. J Comput Assist Tomogr 1997;21:
209–15.
(15) Tallents RH, Katzberg RW, Murphy W, Proskin H. Magnetic
resonance imaging findings in asymptomatic volunteers and
symptomatic patients with temporomandibular disorders. J
Prosthet Dent 1996;75:529–33.
(16) Katzberg RW, Westesson PL, Tallents RH, Drake CM. Ana-
tomic disorders of the temporomandibular joint disc in asymp-
tomatic subjects. J Oral Maxillofac Surg 1996;54:147–53.
(17) Larheim TA, Westesson PL, Sano T. MR grading of temporo-
mandibular joint fluid: association with disk displacement cate-
gories, condyle marrow abnormalities and pain. Int J Oral
Maxillofac Surg 2001;30:104–12.
(18) Sener S, Akganlu F. MRI characteristics of anterior disc
displacement with and without reduction. Dentomaxillofac
Radiol 2004;33(4):245–52.
(19) Nitzan DW. The process of lubrication impairment and its
involvement in temporomandibular joint disc displacement: a
theoretical concept. J Oral Maxillofac Surg 2001;59:36–45.

744 N.M.A. Hasan, T.E.F. Abdelrahman
(20) Roh HS, Kim W, Kim YK, Lee JY. Relationships between disk
displacement, joint effusion, and degenerative changes of the TMJ
in TMD patients based on MRI findings. J Craniomaxillofac Surg
2012;40:283–6.
(21) Suenaga S, Abeyama K, Hamasaki A, Mimura T, Noikura T.
Temporomandibular disorders: relationship between joint pain
and effusion and nitric oxide concentration in the joint fluid.
Dentomaxillofac Radiol 2001;30(4):214–8.
(22) Poveda-Roda R, Dıaz-Fernandez JM, Hernandez-Bazan S,
Jimenez- Soriano Y, Margaix M, Sarrion G. A review of
temporomandibular joint disease (TMJD) Part II: clinical and
radiological semiology morbidity processes. Med Oral Patol Oral
Cir Bucal 2008;13(2):102–9.
(23) Campos MI, Campos PS, Cangussu MC, Guimaraes RC, Line
SR. Analysis of magnetic resonance imaging characteristics and
pain in temporomandibular joints with and without degenerative
changes of the condyle. Int J Oral Maxillofac Surg 2008;37:
529–34.
(24) Emshoff R, Brandlmaier I, Gerhard S, Strobl H, Bertram S,
Rudisch A. Magnetic resonance imaging predictors of temporo-
mandibular joint pain. J Am Dent Assoc 2003;134:705–14.
(25) Honda K, Natsumi Y, Urade M. Correlation between MRI
evidence of degenerative condylar surface changes, induction of
articular disc displacement and pathological joint sounds in the
temporomandibular joint. Gerodontology 2008;25:251–7.
(26) Lafreniere CM, Lamontagne M, el-Sawy R. The role of the lateral
pterygoid muscles in TMJ disorders during static conditions.
Cranio 1997;15:38–52.
(27) Liu ZJ, Yamagata K, Kuroe K, Suenaga S, Noikura T, Ito G.
Morphological and positional assessments of TMJ components
and lateral pterygoid muscle in relation to symptoms and
occlusion of patients with temporomandibular disorders. J Oral
Rehabil 2000;27:860–74.
(28) Yang X, Pernu H, Pyhtinen J, Tiilikainen PA, Oikarinen KS,
Raustia AM. MR abnormalities of the lateral pterygoid muscle in
patients with non-reducing disk displacement of the TMJ. Cranio
2002;20:209–21.
(29) Bjornland T, Refsum SB. Histopathologic changes of the tempo-
romandibular joint disk in patients with chronic arthritic disease.
A comparison with internal derangement. Oral Surg Oral Med
Oral Pathol 1994;77:572–8.
(30) Manzione JV et al. Head and neck radiology RSNA meeting
notes [abstr]. Radiology 1993:186, 607(P).
(31) Vasconcelos Filho JO, Menezes AV, Freitas DQ, Manzi FR,
Boscolo FM, De Almeida SM. Condylar and disk position and
signs and symptoms of temporomandibular disorders in stressfree
subjects. J Am Dent Assoc 2007;138:251–5.
(32) Pereira LJ, Gaviao M, Bonjardim LR, Castelo PM. Ultrasound
and tomographic evaluation of temporomandibular joints in
adolescents with and without signs and symptoms of temporo-
mandibular disorders:a pilot study. Dentomaxillofac Radiol
2007;36:402–8.
(33) de Senna BR, Marques LS, Franca JP, Ramos-Jorge ML, Pereira
LJ, Coracoes T. Condyle-disk-fossa position and relationship to
clinical signs and symptoms of temporomandibular disorders in
women. Oral Surg Oral Med Oral Pathol Oral Radiol Endod
2009;108:117–24.
(34) Celic R, Jerolimov V, Zlataric KD, Klaic B. Measurement of
mandibular movements in patients with temporomandibular
disorders and in asymptomatic subjects. Coll Antropol 2003;
27(Suppl 2):43–9.